User login
Dermatologists lack training about skin of color
a small study in JAMA Dermatology suggests.

Lead author Kristina Gorbatenko-Roth, PhD, of the department of psychology at University of Wisconsin-Stout, Menomonie, Wis., and colleagues analyzed the perceptions of 19 black, adult patients who had received treatment in a skin of color clinic (SOCC). Patients were asked about their perspectives and experiences inside and outside of the clinic as it pertained to dermatologists’ interaction style, cultural awareness, and overall treatment. Two focus groups consisted of patients seen by a race-concordant dermatologist, and two focus groups consisted of patients seen by a race-discordant dermatologist. The patients also responded to a survey.
Of 19 adult black patients who participated in the study, 18 respondents were women, and the mean age was 50 years. Compared with non-SOCC dermatology treatment experiences, patients experienced higher levels of overall satisfaction with SOCC dermatologists, reporting that SOCC dermatologists were better trained to care for black patients, showed greater respect and dignity, and were more trustworthy, according to the study published Aug 21.
Care satisfaction appeared most related to doctors’ interpersonal style and specialized knowledge of black skin and hair, according to the study. Investigators gleaned nine major themes during the analysis, five of which included dermatologist behaviors: interaction style, knowledge, partnering with patients in focusing on outcomes, economic sensitivity, and shared life experiences. Four themes were specific to patients: comfort, confidence, education, and concordance preference. Across all participants, a dermatologist’s interaction style was identified as the most important factor, elements of which included oral communication, body language, and physical examination performance.
Regarding experiences outside the SOCC, participants reported that some providers performed only a cursory skin examination and appeared to avoid physical contact, which some patients interpreted as a sign of disrespect and a lack of racial sensitivity. Participants also expressed frustration with dermatologists outside the clinic who seemed to lack knowledge about black skin and hair disorders. Of all respondents, 71% reported they would prefer a black (or race concordant) dermatologist, including 91% of the race-concordant group and 33% of the race-discordant group.
The investigators wrote the findings underscore a number of needed changes to enhance the care of black dermatology patients, including enhanced dermatology residency and workforce education about treatment of skin of color and more training on culturally aware communication skills. Perceptions of racial and cost-of-care insensitivities identified by the study population also suggest the need for training in cultural competency and implicit bias, delivery of cost conscious care, and the social determinants of health.
As far as they know, the authors noted that, before this study, “little was known regarding black patients’ perceptions of their dermatology care, either within or external to an SOCC,” and that the study “appears to be the first to investigate and provide preliminary findings for addressing this knowledge gap.”
SOURCE: Gorbatenko-Roth K et al. JAMA Dermatol. 2019 Aug 21. doi: 10.1001/jamadermatol.2019.2063.
The study by Gorbatenko-Roth et al. will hopefully serve as a spring board for the field of dermatology to improve physicians’ cultural competence and eliminate persistent knowledge gaps that exist in the treatment of black skin and hair, according to Susan C. Taylor, MD, of the department of dermatology at the University of Pennsylvania, Philadelphia.

In an accompanying editorial in JAMA Dermatology (2019 Aug 21. doi: 10.1001/jamadermatol.2019.1963), Dr. Taylor wrote that the analysis yields insight into the importance of recognizing and understanding that differences exist in the skin and hair of black patients, compared with those of white patients.
“Implicit in this statement is that black skin color, biology, disease, reactions, presentation, diagnosis, and treatment as well as hair types, texture, tensile strength, shape, diameter, growth pattern, follicular configuration, diseases, and treatments are different than those of whites and require the dermatologist to have an expanded knowledge base and cultural sensitivity when evaluating and treating black patients,” Dr. Taylor wrote.
Another important finding is the overall preference by black patients for a race-concordant dermatologist, Dr. Taylor wrote, noting that the ability to fulfill these preferences is limited. In 2016, black dermatologists constituted only 3% of all dermatologists in the United States, while the overall black population in the United States at the time was 12.8%.
“Although this was a small study, the authors have demonstrated the great need for improvement and opportunities for the field of dermatology, including enhanced residency training, lifelong education in skin of color, culturally sensitive and competent care, and greater diversity in the dermatology workforce,” Dr. Taylor wrote. “Let us use this article as a call to action to serve all patients, regardless of race or ethnicity, with equal excellence.”
Dr. Taylor is an associate professor of dermatology at the University of Pennsylvania, Philadelphia, and creator and inaugural director of the Skin of Color Center, St. Luke’s Roosevelt Hospital Center, New York (currently Mount Sinai St Luke’s Medical Center). She reported no disclosures other than her association with the Skin of Color Center.
The study by Gorbatenko-Roth et al. will hopefully serve as a spring board for the field of dermatology to improve physicians’ cultural competence and eliminate persistent knowledge gaps that exist in the treatment of black skin and hair, according to Susan C. Taylor, MD, of the department of dermatology at the University of Pennsylvania, Philadelphia.
In an accompanying editorial in JAMA Dermatology (2019 Aug 21. doi: 10.1001/jamadermatol.2019.1963), Dr. Taylor wrote that the analysis yields insight into the importance of recognizing and understanding that differences exist in the skin and hair of black patients, compared with those of white patients.
“Implicit in this statement is that black skin color, biology, disease, reactions, presentation, diagnosis, and treatment as well as hair types, texture, tensile strength, shape, diameter, growth pattern, follicular configuration, diseases, and treatments are different than those of whites and require the dermatologist to have an expanded knowledge base and cultural sensitivity when evaluating and treating black patients,” Dr. Taylor wrote.
Another important finding is the overall preference by black patients for a race-concordant dermatologist, Dr. Taylor wrote, noting that the ability to fulfill these preferences is limited. In 2016, black dermatologists constituted only 3% of all dermatologists in the United States, while the overall black population in the United States at the time was 12.8%.
“Although this was a small study, the authors have demonstrated the great need for improvement and opportunities for the field of dermatology, including enhanced residency training, lifelong education in skin of color, culturally sensitive and competent care, and greater diversity in the dermatology workforce,” Dr. Taylor wrote. “Let us use this article as a call to action to serve all patients, regardless of race or ethnicity, with equal excellence.”
Dr. Taylor is an associate professor of dermatology at the University of Pennsylvania, Philadelphia, and creator and inaugural director of the Skin of Color Center, St. Luke’s Roosevelt Hospital Center, New York (currently Mount Sinai St Luke’s Medical Center). She reported no disclosures other than her association with the Skin of Color Center.
The study by Gorbatenko-Roth et al. will hopefully serve as a spring board for the field of dermatology to improve physicians’ cultural competence and eliminate persistent knowledge gaps that exist in the treatment of black skin and hair, according to Susan C. Taylor, MD, of the department of dermatology at the University of Pennsylvania, Philadelphia.
In an accompanying editorial in JAMA Dermatology (2019 Aug 21. doi: 10.1001/jamadermatol.2019.1963), Dr. Taylor wrote that the analysis yields insight into the importance of recognizing and understanding that differences exist in the skin and hair of black patients, compared with those of white patients.
“Implicit in this statement is that black skin color, biology, disease, reactions, presentation, diagnosis, and treatment as well as hair types, texture, tensile strength, shape, diameter, growth pattern, follicular configuration, diseases, and treatments are different than those of whites and require the dermatologist to have an expanded knowledge base and cultural sensitivity when evaluating and treating black patients,” Dr. Taylor wrote.
Another important finding is the overall preference by black patients for a race-concordant dermatologist, Dr. Taylor wrote, noting that the ability to fulfill these preferences is limited. In 2016, black dermatologists constituted only 3% of all dermatologists in the United States, while the overall black population in the United States at the time was 12.8%.
“Although this was a small study, the authors have demonstrated the great need for improvement and opportunities for the field of dermatology, including enhanced residency training, lifelong education in skin of color, culturally sensitive and competent care, and greater diversity in the dermatology workforce,” Dr. Taylor wrote. “Let us use this article as a call to action to serve all patients, regardless of race or ethnicity, with equal excellence.”
Dr. Taylor is an associate professor of dermatology at the University of Pennsylvania, Philadelphia, and creator and inaugural director of the Skin of Color Center, St. Luke’s Roosevelt Hospital Center, New York (currently Mount Sinai St Luke’s Medical Center). She reported no disclosures other than her association with the Skin of Color Center.
a small study in JAMA Dermatology suggests.
Lead author Kristina Gorbatenko-Roth, PhD, of the department of psychology at University of Wisconsin-Stout, Menomonie, Wis., and colleagues analyzed the perceptions of 19 black, adult patients who had received treatment in a skin of color clinic (SOCC). Patients were asked about their perspectives and experiences inside and outside of the clinic as it pertained to dermatologists’ interaction style, cultural awareness, and overall treatment. Two focus groups consisted of patients seen by a race-concordant dermatologist, and two focus groups consisted of patients seen by a race-discordant dermatologist. The patients also responded to a survey.
Of 19 adult black patients who participated in the study, 18 respondents were women, and the mean age was 50 years. Compared with non-SOCC dermatology treatment experiences, patients experienced higher levels of overall satisfaction with SOCC dermatologists, reporting that SOCC dermatologists were better trained to care for black patients, showed greater respect and dignity, and were more trustworthy, according to the study published Aug 21.
Care satisfaction appeared most related to doctors’ interpersonal style and specialized knowledge of black skin and hair, according to the study. Investigators gleaned nine major themes during the analysis, five of which included dermatologist behaviors: interaction style, knowledge, partnering with patients in focusing on outcomes, economic sensitivity, and shared life experiences. Four themes were specific to patients: comfort, confidence, education, and concordance preference. Across all participants, a dermatologist’s interaction style was identified as the most important factor, elements of which included oral communication, body language, and physical examination performance.
Regarding experiences outside the SOCC, participants reported that some providers performed only a cursory skin examination and appeared to avoid physical contact, which some patients interpreted as a sign of disrespect and a lack of racial sensitivity. Participants also expressed frustration with dermatologists outside the clinic who seemed to lack knowledge about black skin and hair disorders. Of all respondents, 71% reported they would prefer a black (or race concordant) dermatologist, including 91% of the race-concordant group and 33% of the race-discordant group.
The investigators wrote the findings underscore a number of needed changes to enhance the care of black dermatology patients, including enhanced dermatology residency and workforce education about treatment of skin of color and more training on culturally aware communication skills. Perceptions of racial and cost-of-care insensitivities identified by the study population also suggest the need for training in cultural competency and implicit bias, delivery of cost conscious care, and the social determinants of health.
As far as they know, the authors noted that, before this study, “little was known regarding black patients’ perceptions of their dermatology care, either within or external to an SOCC,” and that the study “appears to be the first to investigate and provide preliminary findings for addressing this knowledge gap.”
SOURCE: Gorbatenko-Roth K et al. JAMA Dermatol. 2019 Aug 21. doi: 10.1001/jamadermatol.2019.2063.
a small study in JAMA Dermatology suggests.
Lead author Kristina Gorbatenko-Roth, PhD, of the department of psychology at University of Wisconsin-Stout, Menomonie, Wis., and colleagues analyzed the perceptions of 19 black, adult patients who had received treatment in a skin of color clinic (SOCC). Patients were asked about their perspectives and experiences inside and outside of the clinic as it pertained to dermatologists’ interaction style, cultural awareness, and overall treatment. Two focus groups consisted of patients seen by a race-concordant dermatologist, and two focus groups consisted of patients seen by a race-discordant dermatologist. The patients also responded to a survey.
Of 19 adult black patients who participated in the study, 18 respondents were women, and the mean age was 50 years. Compared with non-SOCC dermatology treatment experiences, patients experienced higher levels of overall satisfaction with SOCC dermatologists, reporting that SOCC dermatologists were better trained to care for black patients, showed greater respect and dignity, and were more trustworthy, according to the study published Aug 21.
Care satisfaction appeared most related to doctors’ interpersonal style and specialized knowledge of black skin and hair, according to the study. Investigators gleaned nine major themes during the analysis, five of which included dermatologist behaviors: interaction style, knowledge, partnering with patients in focusing on outcomes, economic sensitivity, and shared life experiences. Four themes were specific to patients: comfort, confidence, education, and concordance preference. Across all participants, a dermatologist’s interaction style was identified as the most important factor, elements of which included oral communication, body language, and physical examination performance.
Regarding experiences outside the SOCC, participants reported that some providers performed only a cursory skin examination and appeared to avoid physical contact, which some patients interpreted as a sign of disrespect and a lack of racial sensitivity. Participants also expressed frustration with dermatologists outside the clinic who seemed to lack knowledge about black skin and hair disorders. Of all respondents, 71% reported they would prefer a black (or race concordant) dermatologist, including 91% of the race-concordant group and 33% of the race-discordant group.
The investigators wrote the findings underscore a number of needed changes to enhance the care of black dermatology patients, including enhanced dermatology residency and workforce education about treatment of skin of color and more training on culturally aware communication skills. Perceptions of racial and cost-of-care insensitivities identified by the study population also suggest the need for training in cultural competency and implicit bias, delivery of cost conscious care, and the social determinants of health.
As far as they know, the authors noted that, before this study, “little was known regarding black patients’ perceptions of their dermatology care, either within or external to an SOCC,” and that the study “appears to be the first to investigate and provide preliminary findings for addressing this knowledge gap.”
SOURCE: Gorbatenko-Roth K et al. JAMA Dermatol. 2019 Aug 21. doi: 10.1001/jamadermatol.2019.2063.
FROM JAMA DERMATOLOGY
Key clinical point: Dermatologists need more training about the treatment of skin of color.
Major finding: Compared with a non–skin of color clinic (non-SOCC), patients experienced higher levels of overall satisfaction with SOCC dermatologists, reporting that SOCC dermatologists were better trained to care for black patients.
Study details: A study of 19 black, adult patients through focus groups and a survey.
Disclosures: No disclosures were reported.
Source: Gorbatenko-Roth K et al. JAMA Dermatol. 2019 Aug 21. doi: 10.1001/jamadermatol.2019.2063.
FRAX with BMD may not be accurate for women with diabetes
according to data from 566 women aged 40-90 years.
In a study published in Bone Reports, Lelia L.F. de Abreu, MD, of Deakin University, Geelong, Australia, and colleagues investigated the accuracy of FRAX scores and the role of impaired fasting glucose (IFG) and bone mineral density (BMD) on fracture risk by comparing FRAX scores for 252 normoglycemic women, 247 women with IFG, and 67 women with diabetes.
When BMD was not included, women with diabetes had a higher median FRAX score for major osteoporotic fractures of the hip, clinical spine, forearm, and wrist than women without diabetes or women with IFG (7.1, 4.3, and 5.1, respectively). In the diabetes group, 11 major osteoporotic fractures were observed versus 5 predicted by FRAX. In the normoglycemic group, 28 fractures were observed versus 15 predicted, and in the IFG group 31 fractures were observed versus 16 predicted.
When BMD was included, major osteoporotic fractures and hip fractures also were underestimated in the diabetes group (11 observed vs. 4 observed; 6 observed vs. 1 predicted, respectively), but the difference in observed versus predicted fractures trended toward statistical significance but was not significant (P = .055; P = .52, respectively). FRAX with BMD increased the underestimation of major osteoporotic fractures in the normoglycemic and IFG groups (28 observed vs. 13 predicted; 31 observed vs. 13 predicted).
The study findings were limited by several factors including the inability to determine the impact of specific types of diabetes on fracture risk, lack of data on the duration of diabetes in study participants, the use of self-reports, and a relatively small and homogeneous sample size, the researchers noted.
However, the results support data from previous studies showing an increased fracture risk in diabetes patients regardless of BMD, and suggest that FRAX may be unreliable as a predictor of fractures in the diabetes population, they concluded.
The study was supported in part by the Victorian Health Promotion Foundation, National Health and Medical Research Council Australia, and the Geelong Region Medical Research Foundation. Two researchers were supported by university postgraduate rewards and one researcher was supported by a university postdoctoral research fellowship. The remaining coauthors reported no relevant financial conflicts.
SOURCE: de Abreu LLF et al. Bone Reports. 2019 Aug 13. doi: 10.1016/j.bonr.2019.100223.
according to data from 566 women aged 40-90 years.
In a study published in Bone Reports, Lelia L.F. de Abreu, MD, of Deakin University, Geelong, Australia, and colleagues investigated the accuracy of FRAX scores and the role of impaired fasting glucose (IFG) and bone mineral density (BMD) on fracture risk by comparing FRAX scores for 252 normoglycemic women, 247 women with IFG, and 67 women with diabetes.
When BMD was not included, women with diabetes had a higher median FRAX score for major osteoporotic fractures of the hip, clinical spine, forearm, and wrist than women without diabetes or women with IFG (7.1, 4.3, and 5.1, respectively). In the diabetes group, 11 major osteoporotic fractures were observed versus 5 predicted by FRAX. In the normoglycemic group, 28 fractures were observed versus 15 predicted, and in the IFG group 31 fractures were observed versus 16 predicted.
When BMD was included, major osteoporotic fractures and hip fractures also were underestimated in the diabetes group (11 observed vs. 4 observed; 6 observed vs. 1 predicted, respectively), but the difference in observed versus predicted fractures trended toward statistical significance but was not significant (P = .055; P = .52, respectively). FRAX with BMD increased the underestimation of major osteoporotic fractures in the normoglycemic and IFG groups (28 observed vs. 13 predicted; 31 observed vs. 13 predicted).
The study findings were limited by several factors including the inability to determine the impact of specific types of diabetes on fracture risk, lack of data on the duration of diabetes in study participants, the use of self-reports, and a relatively small and homogeneous sample size, the researchers noted.
However, the results support data from previous studies showing an increased fracture risk in diabetes patients regardless of BMD, and suggest that FRAX may be unreliable as a predictor of fractures in the diabetes population, they concluded.
The study was supported in part by the Victorian Health Promotion Foundation, National Health and Medical Research Council Australia, and the Geelong Region Medical Research Foundation. Two researchers were supported by university postgraduate rewards and one researcher was supported by a university postdoctoral research fellowship. The remaining coauthors reported no relevant financial conflicts.
SOURCE: de Abreu LLF et al. Bone Reports. 2019 Aug 13. doi: 10.1016/j.bonr.2019.100223.
according to data from 566 women aged 40-90 years.
In a study published in Bone Reports, Lelia L.F. de Abreu, MD, of Deakin University, Geelong, Australia, and colleagues investigated the accuracy of FRAX scores and the role of impaired fasting glucose (IFG) and bone mineral density (BMD) on fracture risk by comparing FRAX scores for 252 normoglycemic women, 247 women with IFG, and 67 women with diabetes.
When BMD was not included, women with diabetes had a higher median FRAX score for major osteoporotic fractures of the hip, clinical spine, forearm, and wrist than women without diabetes or women with IFG (7.1, 4.3, and 5.1, respectively). In the diabetes group, 11 major osteoporotic fractures were observed versus 5 predicted by FRAX. In the normoglycemic group, 28 fractures were observed versus 15 predicted, and in the IFG group 31 fractures were observed versus 16 predicted.
When BMD was included, major osteoporotic fractures and hip fractures also were underestimated in the diabetes group (11 observed vs. 4 observed; 6 observed vs. 1 predicted, respectively), but the difference in observed versus predicted fractures trended toward statistical significance but was not significant (P = .055; P = .52, respectively). FRAX with BMD increased the underestimation of major osteoporotic fractures in the normoglycemic and IFG groups (28 observed vs. 13 predicted; 31 observed vs. 13 predicted).
The study findings were limited by several factors including the inability to determine the impact of specific types of diabetes on fracture risk, lack of data on the duration of diabetes in study participants, the use of self-reports, and a relatively small and homogeneous sample size, the researchers noted.
However, the results support data from previous studies showing an increased fracture risk in diabetes patients regardless of BMD, and suggest that FRAX may be unreliable as a predictor of fractures in the diabetes population, they concluded.
The study was supported in part by the Victorian Health Promotion Foundation, National Health and Medical Research Council Australia, and the Geelong Region Medical Research Foundation. Two researchers were supported by university postgraduate rewards and one researcher was supported by a university postdoctoral research fellowship. The remaining coauthors reported no relevant financial conflicts.
SOURCE: de Abreu LLF et al. Bone Reports. 2019 Aug 13. doi: 10.1016/j.bonr.2019.100223.
FROM BONE REPORTS
‘Pot’ is still hot for Dravet, Lennox-Gastaut
BANGKOK – Interim results of long-term, open-label extension trials of add-on prescription cannabidiol in patients with Dravet syndrome or Lennox-Gastaut syndrome show sustained, clinically meaningful seizure reductions with no new safety concerns, Anup D. Patel, MD, reported at the International Epilepsy Congress.

“Overall, this is a very promising and sustainable result that we were happy to see,” said Dr. Patel, chief of child neurology at Nationwide Children’s Hospital in Columbus, Ohio.
Epidiolex is the brand name for the plant-derived, highly purified cannabidiol (CBD) in an oil-based oral solution at 100 mg/mL. Dr. Patel has been involved in the medication’s development program since the earliest open-label compassionate use study, which was followed by rigorous phase 3, double-blind, placebo-controlled randomized trials, eventually leading to Food and Drug Administration marketing approval for the treatment of Dravet syndrome and Lennox-Gastaut syndrome in patients 2 years of age or older.
“On June 25th, 2018, history was made: for the first time in United States history, a plant-based derivative of marijuana was approved for use as a medication, and it was also the first FDA-approved treatment for Dravet syndrome,” Dr. Patel noted at the congress sponsored by the International League Against Epilepsy.
A total of 96% of the 289 children with Dravet syndrome who completed the 14-week, double-blind, controlled randomized trials enrolled in the open-label, long-term extension study, during which they were on a median of three concurrent antiepileptic drugs along with a mean modal dose of CBD at 22 mg/kg/day. Although the target maintenance dose of CBD was 20 mg/kg/day, as advised in the product labeling, physicians could reduce or increase the dose up to 30 mg/kg/day.
“In the initial compassionate-use study, our site could go up to 50 mg/kg/day,” according to Dr. Patel. “We have plenty of data showing efficacy and continued safety beyond the FDA-recommended dose.”
In the open-label extension study, the median reduction from baseline in monthly seizure frequency assessed in 12-week intervals up to a maximum of week 72 was 44%-57% for convulsive seizures and 49%-67% for total seizures. More than 80% of patients and/or caregivers reported improvement in the patient’s overall condition as assessed on the Subject/Caregiver Global Impression of Change scale.
The pattern of adverse events associated with CBD has been consistent across all of the studies. The most common side effects are diarrhea in about one-third of patients, sleepiness in one-quarter, and decreased appetite in about one-quarter. Seven percent of patients discontinued the long-term extension trial because of adverse events.
Seventy percent of patients remained in the long-term extension study at 1 year.
Twenty-six patients developed liver transaminase levels greater than three times the upper limit of normal, and of note, 23 of the 26 were on concomitant valproic acid. None met criteria for severe drug-induced liver injury, and all recovered either spontaneously or after a reduction in the dose of CBD or valproic acid. But this association between CBD, valproic acid, and increased risk of mild liver injury has been a consistent finding across the clinical trials program.
“This is a very important clinical pearl to take away,” commented Dr. Patel, who is also a pediatric neurologist at Ohio State University.
The interim results of the long-term, open-label extension study of add-on CBD in patients with Lennox-Gastaut syndrome are similar to the Dravet syndrome study. Overall, 99% of the 368 patients with Lennox-Gastaut syndrome who completed the 14-week, double-blind, randomized trials signed up for the open-label extension. During a median follow-up of 61 weeks, the median percent reduction in seizure frequency as assessed in serial 12-week windows was 48%-70% for drop seizures and 48%-63% for total seizures. Twenty-four percent of patients withdrew from the study. Eighty-eight percent of patients or caregivers reported an improvement in overall condition when assessed at weeks 24 and 48. Forty-seven patients developed elevated transaminase levels – typically within the first 2 months on CBD – and 35 of them were on concomitant valproic acid.
More on drug-drug interactions
Elsewhere at IEC 2019, Gilmour Morrison of GW Pharmaceuticals, the Cambridge, England, company that markets Epidiolex, presented the findings of a series of drug-drug interaction studies involving coadministration of their CBD with clobazam (Sympazan and Onfi), valproate, stiripentol (Diacomit), or midazolam (Versed) in adult epilepsy patients and healthy volunteers. The researchers reported a bidirectional drug-drug interaction between Epidiolex and clobazam resulting in increased levels of the active metabolites of both drugs. The mechanism is believed to involve inhibition of cytochrome P450 2C19. However, there were no interactions with midazolam or valproate, and the slight bump in stiripentol levels when given with CBD didn’t reach the level of a clinically meaningful drug-drug interaction, according to the investigators.
On the horizon, Canadian researchers are investigating the possibility that since both the tetrahydrocannabinol (THC) and CBD components of marijuana have been shown to have anticonvulsant effects, adding a bit of THC to CBD will result in even better seizure control than with pure CBD in patients with Dravet syndrome. Investigators at Toronto’s Hospital for Sick Children have conducted a prospective, open-label study of a product containing CBD and THC in a 50:1 ratio as add-on therapy in 20 children with Dravet syndrome. The dose was 2-16 mg/kg/day of CBD and 0.04-0.32 mg/kg/day of THC. The cannabis plant extract used in the study was produced by Tilray, a Canadian pharmaceutical company.
Nineteen of the 20 patients completed the 20-week study. The sole noncompleter died of SUDEP (sudden unexpected death in epilepsy) deemed treatment unrelated. Patients experienced a median 71% reduction in motor seizures, compared with baseline. Sixty-three percent of patients had at least a 50% reduction in seizure frequency. Elevated liver transaminases occurred in patients on concomitant valproic acid, as did platelet abnormalities, which have not been seen in the Epidiolex studies, noted Dr. Patel, who was not involved in the Canadian study (Ann Clin Transl Neurol. 2018 Aug 1;5[9]:1077-88).
Dr. Patel reported serving as a consultant to Greenwich Biosciences, a U.S. offshoot of GW Pharmaceuticals. He receives research grants from that company as well as from the National Institutes of Health and the Pediatric Epilepsy Research Foundation.
BANGKOK – Interim results of long-term, open-label extension trials of add-on prescription cannabidiol in patients with Dravet syndrome or Lennox-Gastaut syndrome show sustained, clinically meaningful seizure reductions with no new safety concerns, Anup D. Patel, MD, reported at the International Epilepsy Congress.
“Overall, this is a very promising and sustainable result that we were happy to see,” said Dr. Patel, chief of child neurology at Nationwide Children’s Hospital in Columbus, Ohio.
Epidiolex is the brand name for the plant-derived, highly purified cannabidiol (CBD) in an oil-based oral solution at 100 mg/mL. Dr. Patel has been involved in the medication’s development program since the earliest open-label compassionate use study, which was followed by rigorous phase 3, double-blind, placebo-controlled randomized trials, eventually leading to Food and Drug Administration marketing approval for the treatment of Dravet syndrome and Lennox-Gastaut syndrome in patients 2 years of age or older.
“On June 25th, 2018, history was made: for the first time in United States history, a plant-based derivative of marijuana was approved for use as a medication, and it was also the first FDA-approved treatment for Dravet syndrome,” Dr. Patel noted at the congress sponsored by the International League Against Epilepsy.
A total of 96% of the 289 children with Dravet syndrome who completed the 14-week, double-blind, controlled randomized trials enrolled in the open-label, long-term extension study, during which they were on a median of three concurrent antiepileptic drugs along with a mean modal dose of CBD at 22 mg/kg/day. Although the target maintenance dose of CBD was 20 mg/kg/day, as advised in the product labeling, physicians could reduce or increase the dose up to 30 mg/kg/day.
“In the initial compassionate-use study, our site could go up to 50 mg/kg/day,” according to Dr. Patel. “We have plenty of data showing efficacy and continued safety beyond the FDA-recommended dose.”
In the open-label extension study, the median reduction from baseline in monthly seizure frequency assessed in 12-week intervals up to a maximum of week 72 was 44%-57% for convulsive seizures and 49%-67% for total seizures. More than 80% of patients and/or caregivers reported improvement in the patient’s overall condition as assessed on the Subject/Caregiver Global Impression of Change scale.
The pattern of adverse events associated with CBD has been consistent across all of the studies. The most common side effects are diarrhea in about one-third of patients, sleepiness in one-quarter, and decreased appetite in about one-quarter. Seven percent of patients discontinued the long-term extension trial because of adverse events.
Seventy percent of patients remained in the long-term extension study at 1 year.
Twenty-six patients developed liver transaminase levels greater than three times the upper limit of normal, and of note, 23 of the 26 were on concomitant valproic acid. None met criteria for severe drug-induced liver injury, and all recovered either spontaneously or after a reduction in the dose of CBD or valproic acid. But this association between CBD, valproic acid, and increased risk of mild liver injury has been a consistent finding across the clinical trials program.
“This is a very important clinical pearl to take away,” commented Dr. Patel, who is also a pediatric neurologist at Ohio State University.
The interim results of the long-term, open-label extension study of add-on CBD in patients with Lennox-Gastaut syndrome are similar to the Dravet syndrome study. Overall, 99% of the 368 patients with Lennox-Gastaut syndrome who completed the 14-week, double-blind, randomized trials signed up for the open-label extension. During a median follow-up of 61 weeks, the median percent reduction in seizure frequency as assessed in serial 12-week windows was 48%-70% for drop seizures and 48%-63% for total seizures. Twenty-four percent of patients withdrew from the study. Eighty-eight percent of patients or caregivers reported an improvement in overall condition when assessed at weeks 24 and 48. Forty-seven patients developed elevated transaminase levels – typically within the first 2 months on CBD – and 35 of them were on concomitant valproic acid.
More on drug-drug interactions
Elsewhere at IEC 2019, Gilmour Morrison of GW Pharmaceuticals, the Cambridge, England, company that markets Epidiolex, presented the findings of a series of drug-drug interaction studies involving coadministration of their CBD with clobazam (Sympazan and Onfi), valproate, stiripentol (Diacomit), or midazolam (Versed) in adult epilepsy patients and healthy volunteers. The researchers reported a bidirectional drug-drug interaction between Epidiolex and clobazam resulting in increased levels of the active metabolites of both drugs. The mechanism is believed to involve inhibition of cytochrome P450 2C19. However, there were no interactions with midazolam or valproate, and the slight bump in stiripentol levels when given with CBD didn’t reach the level of a clinically meaningful drug-drug interaction, according to the investigators.
On the horizon, Canadian researchers are investigating the possibility that since both the tetrahydrocannabinol (THC) and CBD components of marijuana have been shown to have anticonvulsant effects, adding a bit of THC to CBD will result in even better seizure control than with pure CBD in patients with Dravet syndrome. Investigators at Toronto’s Hospital for Sick Children have conducted a prospective, open-label study of a product containing CBD and THC in a 50:1 ratio as add-on therapy in 20 children with Dravet syndrome. The dose was 2-16 mg/kg/day of CBD and 0.04-0.32 mg/kg/day of THC. The cannabis plant extract used in the study was produced by Tilray, a Canadian pharmaceutical company.
Nineteen of the 20 patients completed the 20-week study. The sole noncompleter died of SUDEP (sudden unexpected death in epilepsy) deemed treatment unrelated. Patients experienced a median 71% reduction in motor seizures, compared with baseline. Sixty-three percent of patients had at least a 50% reduction in seizure frequency. Elevated liver transaminases occurred in patients on concomitant valproic acid, as did platelet abnormalities, which have not been seen in the Epidiolex studies, noted Dr. Patel, who was not involved in the Canadian study (Ann Clin Transl Neurol. 2018 Aug 1;5[9]:1077-88).
Dr. Patel reported serving as a consultant to Greenwich Biosciences, a U.S. offshoot of GW Pharmaceuticals. He receives research grants from that company as well as from the National Institutes of Health and the Pediatric Epilepsy Research Foundation.
BANGKOK – Interim results of long-term, open-label extension trials of add-on prescription cannabidiol in patients with Dravet syndrome or Lennox-Gastaut syndrome show sustained, clinically meaningful seizure reductions with no new safety concerns, Anup D. Patel, MD, reported at the International Epilepsy Congress.
“Overall, this is a very promising and sustainable result that we were happy to see,” said Dr. Patel, chief of child neurology at Nationwide Children’s Hospital in Columbus, Ohio.
Epidiolex is the brand name for the plant-derived, highly purified cannabidiol (CBD) in an oil-based oral solution at 100 mg/mL. Dr. Patel has been involved in the medication’s development program since the earliest open-label compassionate use study, which was followed by rigorous phase 3, double-blind, placebo-controlled randomized trials, eventually leading to Food and Drug Administration marketing approval for the treatment of Dravet syndrome and Lennox-Gastaut syndrome in patients 2 years of age or older.
“On June 25th, 2018, history was made: for the first time in United States history, a plant-based derivative of marijuana was approved for use as a medication, and it was also the first FDA-approved treatment for Dravet syndrome,” Dr. Patel noted at the congress sponsored by the International League Against Epilepsy.
A total of 96% of the 289 children with Dravet syndrome who completed the 14-week, double-blind, controlled randomized trials enrolled in the open-label, long-term extension study, during which they were on a median of three concurrent antiepileptic drugs along with a mean modal dose of CBD at 22 mg/kg/day. Although the target maintenance dose of CBD was 20 mg/kg/day, as advised in the product labeling, physicians could reduce or increase the dose up to 30 mg/kg/day.
“In the initial compassionate-use study, our site could go up to 50 mg/kg/day,” according to Dr. Patel. “We have plenty of data showing efficacy and continued safety beyond the FDA-recommended dose.”
In the open-label extension study, the median reduction from baseline in monthly seizure frequency assessed in 12-week intervals up to a maximum of week 72 was 44%-57% for convulsive seizures and 49%-67% for total seizures. More than 80% of patients and/or caregivers reported improvement in the patient’s overall condition as assessed on the Subject/Caregiver Global Impression of Change scale.
The pattern of adverse events associated with CBD has been consistent across all of the studies. The most common side effects are diarrhea in about one-third of patients, sleepiness in one-quarter, and decreased appetite in about one-quarter. Seven percent of patients discontinued the long-term extension trial because of adverse events.
Seventy percent of patients remained in the long-term extension study at 1 year.
Twenty-six patients developed liver transaminase levels greater than three times the upper limit of normal, and of note, 23 of the 26 were on concomitant valproic acid. None met criteria for severe drug-induced liver injury, and all recovered either spontaneously or after a reduction in the dose of CBD or valproic acid. But this association between CBD, valproic acid, and increased risk of mild liver injury has been a consistent finding across the clinical trials program.
“This is a very important clinical pearl to take away,” commented Dr. Patel, who is also a pediatric neurologist at Ohio State University.
The interim results of the long-term, open-label extension study of add-on CBD in patients with Lennox-Gastaut syndrome are similar to the Dravet syndrome study. Overall, 99% of the 368 patients with Lennox-Gastaut syndrome who completed the 14-week, double-blind, randomized trials signed up for the open-label extension. During a median follow-up of 61 weeks, the median percent reduction in seizure frequency as assessed in serial 12-week windows was 48%-70% for drop seizures and 48%-63% for total seizures. Twenty-four percent of patients withdrew from the study. Eighty-eight percent of patients or caregivers reported an improvement in overall condition when assessed at weeks 24 and 48. Forty-seven patients developed elevated transaminase levels – typically within the first 2 months on CBD – and 35 of them were on concomitant valproic acid.
More on drug-drug interactions
Elsewhere at IEC 2019, Gilmour Morrison of GW Pharmaceuticals, the Cambridge, England, company that markets Epidiolex, presented the findings of a series of drug-drug interaction studies involving coadministration of their CBD with clobazam (Sympazan and Onfi), valproate, stiripentol (Diacomit), or midazolam (Versed) in adult epilepsy patients and healthy volunteers. The researchers reported a bidirectional drug-drug interaction between Epidiolex and clobazam resulting in increased levels of the active metabolites of both drugs. The mechanism is believed to involve inhibition of cytochrome P450 2C19. However, there were no interactions with midazolam or valproate, and the slight bump in stiripentol levels when given with CBD didn’t reach the level of a clinically meaningful drug-drug interaction, according to the investigators.
On the horizon, Canadian researchers are investigating the possibility that since both the tetrahydrocannabinol (THC) and CBD components of marijuana have been shown to have anticonvulsant effects, adding a bit of THC to CBD will result in even better seizure control than with pure CBD in patients with Dravet syndrome. Investigators at Toronto’s Hospital for Sick Children have conducted a prospective, open-label study of a product containing CBD and THC in a 50:1 ratio as add-on therapy in 20 children with Dravet syndrome. The dose was 2-16 mg/kg/day of CBD and 0.04-0.32 mg/kg/day of THC. The cannabis plant extract used in the study was produced by Tilray, a Canadian pharmaceutical company.
Nineteen of the 20 patients completed the 20-week study. The sole noncompleter died of SUDEP (sudden unexpected death in epilepsy) deemed treatment unrelated. Patients experienced a median 71% reduction in motor seizures, compared with baseline. Sixty-three percent of patients had at least a 50% reduction in seizure frequency. Elevated liver transaminases occurred in patients on concomitant valproic acid, as did platelet abnormalities, which have not been seen in the Epidiolex studies, noted Dr. Patel, who was not involved in the Canadian study (Ann Clin Transl Neurol. 2018 Aug 1;5[9]:1077-88).
Dr. Patel reported serving as a consultant to Greenwich Biosciences, a U.S. offshoot of GW Pharmaceuticals. He receives research grants from that company as well as from the National Institutes of Health and the Pediatric Epilepsy Research Foundation.
REPORTING FROM IEC 2019
Dermatologists urged to take ownership of preventable AEs
NEW YORK – according to Galen T. Foulke, MD, who discussed avoidable clinical disasters in practice at the American Academy of Dermatology summer meeting.
Of a list of known and predictable risks that “fall under the purview of ‘You Should Have Known Better,’ ” Dr. Foulke focused on glucocorticoid-associated osteoporosis and infections associated with biologics.
Prior to delivering advice about preventing osteoporosis in patients taking glucocorticoids, he polled the audience about what they considered appropriate prophylaxis in this setting. The vast majority opted for vitamin D and calcium supplementation.
“This is a common answer, but it is the wrong answer,” said Dr. Foulke, a dermatologist affiliated with Penn State Milton S. Hershey Medical Center in Hershey, Pennsylvania.
The available data show that patients on vitamin D and calcium supplementation will continue to lose bone density on therapeutic doses of steroids, according to Dr. Foulke. This is true even when the daily doses for these supplements exceed 800 units and 900 mg, respectively. Moreover, calcium supplementation is associated with an increased risk of heart disease in patients without a calcium deficiency, he noted.
The correct answer is a bisphosphonate, said Dr. Foulke. Of the bisphosphonates, he recommended alendronate as one that is particularly well tolerated and readily reimbursed.
He believes that dermatologists prescribing glucocorticoids should not overlook the substantial risk of osteoporosis or their responsibility to discuss strategies for risk mitigation. Moreover, he believes dermatologists should consider prescribing alendronate in the appropriate candidates, not just refer to another specialist.
“In the first year of steroid use, substantial bone loss is a risk even at doses below 5 mg,” Dr. Foulke warned. At higher doses, patients can lose up to 25% of their bone density, he added.
Of preventable risks of biologics, Dr. Foulke focused on infection. In particular, he urged dermatologists who prescribe these drugs to routinely inform patients about the role and safety of vaccines in infection prevention.
“An immunosuppressant suppresses the immune system, increasing the risk of infection. It is our responsibility to protect patients from the known risks of the therapies we offer them,” he said.
Several organizations recommend the pneumococcal vaccine series and the annual influenza vaccine for patients taking biologics. Although Dr. Foulke was unable to find reliable data on vaccination rates among patients prescribed a biologic for a dermatologic indication, he cited rheumatology practice data to suggest that less than half of patients receive this protection.
A major reason for the low rate of vaccination was failure of the biologic prescriber to assume responsibility for this recommended step, according to Dr. Foulke. Although he does not believe that biologic prescribers need to administer the vaccine, and he acknowledged that he does not stock vaccines in his clinic, he does believe they should inform patients when vaccination is safe and appropriate.
Live attenuated vaccines, in his opinion, are not safe. Although he reported that this is an area of controversy, he takes a conservative approach, advising candidates for a live attenuated vaccine to undergo vaccination prior to starting the biologic or during a break from biologic therapy.
When he polled the audience about which vaccines are live attenuated vaccines, several failed to recognize that the MMR vaccine falls into this category. However, he also noted that the majority of vaccines are not live attenuated and should be considered. He specifically singled out the recombinant herpes zoster as a vaccine recommended by the American College of Rheumatology in patients on biologics.
“We do not have to give the shots, but we should be the ones who start the discussion,” said Dr. Foulke, referring to vaccines in patients on a biologic. He called these important steps “to protect patients from preventable disasters.”
Dr. Foulke reported no potential conflicts of interest.
SOURCE: Summer AAD 2019, Session F02.
NEW YORK – according to Galen T. Foulke, MD, who discussed avoidable clinical disasters in practice at the American Academy of Dermatology summer meeting.
Of a list of known and predictable risks that “fall under the purview of ‘You Should Have Known Better,’ ” Dr. Foulke focused on glucocorticoid-associated osteoporosis and infections associated with biologics.
Prior to delivering advice about preventing osteoporosis in patients taking glucocorticoids, he polled the audience about what they considered appropriate prophylaxis in this setting. The vast majority opted for vitamin D and calcium supplementation.
“This is a common answer, but it is the wrong answer,” said Dr. Foulke, a dermatologist affiliated with Penn State Milton S. Hershey Medical Center in Hershey, Pennsylvania.
The available data show that patients on vitamin D and calcium supplementation will continue to lose bone density on therapeutic doses of steroids, according to Dr. Foulke. This is true even when the daily doses for these supplements exceed 800 units and 900 mg, respectively. Moreover, calcium supplementation is associated with an increased risk of heart disease in patients without a calcium deficiency, he noted.
The correct answer is a bisphosphonate, said Dr. Foulke. Of the bisphosphonates, he recommended alendronate as one that is particularly well tolerated and readily reimbursed.
He believes that dermatologists prescribing glucocorticoids should not overlook the substantial risk of osteoporosis or their responsibility to discuss strategies for risk mitigation. Moreover, he believes dermatologists should consider prescribing alendronate in the appropriate candidates, not just refer to another specialist.
“In the first year of steroid use, substantial bone loss is a risk even at doses below 5 mg,” Dr. Foulke warned. At higher doses, patients can lose up to 25% of their bone density, he added.
Of preventable risks of biologics, Dr. Foulke focused on infection. In particular, he urged dermatologists who prescribe these drugs to routinely inform patients about the role and safety of vaccines in infection prevention.
“An immunosuppressant suppresses the immune system, increasing the risk of infection. It is our responsibility to protect patients from the known risks of the therapies we offer them,” he said.
Several organizations recommend the pneumococcal vaccine series and the annual influenza vaccine for patients taking biologics. Although Dr. Foulke was unable to find reliable data on vaccination rates among patients prescribed a biologic for a dermatologic indication, he cited rheumatology practice data to suggest that less than half of patients receive this protection.
A major reason for the low rate of vaccination was failure of the biologic prescriber to assume responsibility for this recommended step, according to Dr. Foulke. Although he does not believe that biologic prescribers need to administer the vaccine, and he acknowledged that he does not stock vaccines in his clinic, he does believe they should inform patients when vaccination is safe and appropriate.
Live attenuated vaccines, in his opinion, are not safe. Although he reported that this is an area of controversy, he takes a conservative approach, advising candidates for a live attenuated vaccine to undergo vaccination prior to starting the biologic or during a break from biologic therapy.
When he polled the audience about which vaccines are live attenuated vaccines, several failed to recognize that the MMR vaccine falls into this category. However, he also noted that the majority of vaccines are not live attenuated and should be considered. He specifically singled out the recombinant herpes zoster as a vaccine recommended by the American College of Rheumatology in patients on biologics.
“We do not have to give the shots, but we should be the ones who start the discussion,” said Dr. Foulke, referring to vaccines in patients on a biologic. He called these important steps “to protect patients from preventable disasters.”
Dr. Foulke reported no potential conflicts of interest.
SOURCE: Summer AAD 2019, Session F02.
NEW YORK – according to Galen T. Foulke, MD, who discussed avoidable clinical disasters in practice at the American Academy of Dermatology summer meeting.
Of a list of known and predictable risks that “fall under the purview of ‘You Should Have Known Better,’ ” Dr. Foulke focused on glucocorticoid-associated osteoporosis and infections associated with biologics.
Prior to delivering advice about preventing osteoporosis in patients taking glucocorticoids, he polled the audience about what they considered appropriate prophylaxis in this setting. The vast majority opted for vitamin D and calcium supplementation.
“This is a common answer, but it is the wrong answer,” said Dr. Foulke, a dermatologist affiliated with Penn State Milton S. Hershey Medical Center in Hershey, Pennsylvania.
The available data show that patients on vitamin D and calcium supplementation will continue to lose bone density on therapeutic doses of steroids, according to Dr. Foulke. This is true even when the daily doses for these supplements exceed 800 units and 900 mg, respectively. Moreover, calcium supplementation is associated with an increased risk of heart disease in patients without a calcium deficiency, he noted.
The correct answer is a bisphosphonate, said Dr. Foulke. Of the bisphosphonates, he recommended alendronate as one that is particularly well tolerated and readily reimbursed.
He believes that dermatologists prescribing glucocorticoids should not overlook the substantial risk of osteoporosis or their responsibility to discuss strategies for risk mitigation. Moreover, he believes dermatologists should consider prescribing alendronate in the appropriate candidates, not just refer to another specialist.
“In the first year of steroid use, substantial bone loss is a risk even at doses below 5 mg,” Dr. Foulke warned. At higher doses, patients can lose up to 25% of their bone density, he added.
Of preventable risks of biologics, Dr. Foulke focused on infection. In particular, he urged dermatologists who prescribe these drugs to routinely inform patients about the role and safety of vaccines in infection prevention.
“An immunosuppressant suppresses the immune system, increasing the risk of infection. It is our responsibility to protect patients from the known risks of the therapies we offer them,” he said.
Several organizations recommend the pneumococcal vaccine series and the annual influenza vaccine for patients taking biologics. Although Dr. Foulke was unable to find reliable data on vaccination rates among patients prescribed a biologic for a dermatologic indication, he cited rheumatology practice data to suggest that less than half of patients receive this protection.
A major reason for the low rate of vaccination was failure of the biologic prescriber to assume responsibility for this recommended step, according to Dr. Foulke. Although he does not believe that biologic prescribers need to administer the vaccine, and he acknowledged that he does not stock vaccines in his clinic, he does believe they should inform patients when vaccination is safe and appropriate.
Live attenuated vaccines, in his opinion, are not safe. Although he reported that this is an area of controversy, he takes a conservative approach, advising candidates for a live attenuated vaccine to undergo vaccination prior to starting the biologic or during a break from biologic therapy.
When he polled the audience about which vaccines are live attenuated vaccines, several failed to recognize that the MMR vaccine falls into this category. However, he also noted that the majority of vaccines are not live attenuated and should be considered. He specifically singled out the recombinant herpes zoster as a vaccine recommended by the American College of Rheumatology in patients on biologics.
“We do not have to give the shots, but we should be the ones who start the discussion,” said Dr. Foulke, referring to vaccines in patients on a biologic. He called these important steps “to protect patients from preventable disasters.”
Dr. Foulke reported no potential conflicts of interest.
SOURCE: Summer AAD 2019, Session F02.
EXPERT ANALYSIS FROM SUMMER AAD 2019
Class I recall issued for Sapien 3 balloon
The Food and Drug Administration has issued a class I correction recall for Edward Lifescience’s Sapien 3 balloon system, which is used to deploy transcatheter aortic valve replacements, according to a release from the agency. A class I recall is the most serious the agency issues and indicates risk of severe injury or even death.

Rather than indicate removal of the device from market, this recall provides details on how to use the device cautiously and safely and instructs physicians on proper technique to safely retract the delivery system into the sheath in cases of a suspected balloon burst. Failure to observe these recommendations can result in vascular injury, bleeding, or surgical intervention.
These recommendations and instructions reiterate those issued in an Urgent Field Safety Notice that was provided by Edward Lifesciences on July 9, 2019. Edward Lifesciences could not be reached for comment.
The Food and Drug Administration has issued a class I correction recall for Edward Lifescience’s Sapien 3 balloon system, which is used to deploy transcatheter aortic valve replacements, according to a release from the agency. A class I recall is the most serious the agency issues and indicates risk of severe injury or even death.
Rather than indicate removal of the device from market, this recall provides details on how to use the device cautiously and safely and instructs physicians on proper technique to safely retract the delivery system into the sheath in cases of a suspected balloon burst. Failure to observe these recommendations can result in vascular injury, bleeding, or surgical intervention.
These recommendations and instructions reiterate those issued in an Urgent Field Safety Notice that was provided by Edward Lifesciences on July 9, 2019. Edward Lifesciences could not be reached for comment.
The Food and Drug Administration has issued a class I correction recall for Edward Lifescience’s Sapien 3 balloon system, which is used to deploy transcatheter aortic valve replacements, according to a release from the agency. A class I recall is the most serious the agency issues and indicates risk of severe injury or even death.
Rather than indicate removal of the device from market, this recall provides details on how to use the device cautiously and safely and instructs physicians on proper technique to safely retract the delivery system into the sheath in cases of a suspected balloon burst. Failure to observe these recommendations can result in vascular injury, bleeding, or surgical intervention.
These recommendations and instructions reiterate those issued in an Urgent Field Safety Notice that was provided by Edward Lifesciences on July 9, 2019. Edward Lifesciences could not be reached for comment.
Fifty-one percent of U.S. adolescents fully vaccinated against HPV
according to a report published in Morbidity and Mortality Weekly Report.

Researchers analyzed data from 18,700 adolescents aged 13-17 years – 48% of whom were female – in the 2018 National Immunization Survey–Teen to discover that 51% of adolescents were up to date with the human papillomavirus (HPV) vaccine, and 68% had received at least one dose of the vaccine.
There was an increase in HPV vaccination coverage from 2017 to 2018, but this was attributable to a 4.4 percentage point increase in males who were up to date, compared with a 0.6 percentage point increase in females.
“Although HPV vaccination coverage improved, increases among all adolescents were modest compared with increases in previous years and were observed only among males,” wrote Tanja Y. Walker of the National Center for Immunization and Respiratory Diseases at the Centers for Disease Control and Prevention, and coauthors.![]()
The number of adolescents who had at least one dose of the quadrivalent meningococcal conjugate (4MenB) vaccine increased by 1.5 percentage points to 86.6%, while among individuals aged 17 years, coverage with two or more doses of 4MenB vaccine increased by 6.5 percentage points to 50.8%. Tdap coverage remained the same at 89% (MMWR 2019;68(33):718-23).
However, the study saw no significant increases in coverage with three or more hepatitis B vaccine doses, two or more MMR vaccine doses, or with one or more varicella vaccine doses in adolescents without a history of varicella disease.
Adolescents with Medicaid had higher HPV vaccination coverage than did adolescents with private health insurance. Uninsured adolescents had lower coverage overall, ranging from 4 percentage points lower for one or more varicella vaccine doses to 19 percentage points lower for two or more 4MenB vaccines, compared with adolescents with private health insurance.
Vaccination rates were lower among adolescents outside metropolitan areas, particularly when it came to being up to date with HPV vaccination, where there was a 15 percentage point difference, and with two or more doses of the quadrivalent meningococcal conjugate vaccine, where there was a 20 percentage point difference.
Provider recommendations to parents were associated with a higher rate of coverage with one or more doses of the HPV vaccine, but the prevalence of provider recommendations varied significantly from state to state. Overall, 78% of parents said they received a provider recommendation for the adolescent HPV vaccine, but that figure was as low as 60% in Mississippi and as high as 91% in Massachusetts.
Parents living in nonmetropolitan areas were less likely to report receiving a provider recommendation than were those in metropolitan principal cities.
“Equipping providers with the tools they need to give strong recommendations that emphasize the importance of HPV vaccination in preventing cancer and effectively address parental concerns is a priority, especially in states where provider recommendations were less commonly reported,” Ms. Walker and associates said.
No conflicts of interest were declared.
according to a report published in Morbidity and Mortality Weekly Report.
Researchers analyzed data from 18,700 adolescents aged 13-17 years – 48% of whom were female – in the 2018 National Immunization Survey–Teen to discover that 51% of adolescents were up to date with the human papillomavirus (HPV) vaccine, and 68% had received at least one dose of the vaccine.
There was an increase in HPV vaccination coverage from 2017 to 2018, but this was attributable to a 4.4 percentage point increase in males who were up to date, compared with a 0.6 percentage point increase in females.
“Although HPV vaccination coverage improved, increases among all adolescents were modest compared with increases in previous years and were observed only among males,” wrote Tanja Y. Walker of the National Center for Immunization and Respiratory Diseases at the Centers for Disease Control and Prevention, and coauthors.![]()
The number of adolescents who had at least one dose of the quadrivalent meningococcal conjugate (4MenB) vaccine increased by 1.5 percentage points to 86.6%, while among individuals aged 17 years, coverage with two or more doses of 4MenB vaccine increased by 6.5 percentage points to 50.8%. Tdap coverage remained the same at 89% (MMWR 2019;68(33):718-23).
However, the study saw no significant increases in coverage with three or more hepatitis B vaccine doses, two or more MMR vaccine doses, or with one or more varicella vaccine doses in adolescents without a history of varicella disease.
Adolescents with Medicaid had higher HPV vaccination coverage than did adolescents with private health insurance. Uninsured adolescents had lower coverage overall, ranging from 4 percentage points lower for one or more varicella vaccine doses to 19 percentage points lower for two or more 4MenB vaccines, compared with adolescents with private health insurance.
Vaccination rates were lower among adolescents outside metropolitan areas, particularly when it came to being up to date with HPV vaccination, where there was a 15 percentage point difference, and with two or more doses of the quadrivalent meningococcal conjugate vaccine, where there was a 20 percentage point difference.
Provider recommendations to parents were associated with a higher rate of coverage with one or more doses of the HPV vaccine, but the prevalence of provider recommendations varied significantly from state to state. Overall, 78% of parents said they received a provider recommendation for the adolescent HPV vaccine, but that figure was as low as 60% in Mississippi and as high as 91% in Massachusetts.
Parents living in nonmetropolitan areas were less likely to report receiving a provider recommendation than were those in metropolitan principal cities.
“Equipping providers with the tools they need to give strong recommendations that emphasize the importance of HPV vaccination in preventing cancer and effectively address parental concerns is a priority, especially in states where provider recommendations were less commonly reported,” Ms. Walker and associates said.
No conflicts of interest were declared.
according to a report published in Morbidity and Mortality Weekly Report.
Researchers analyzed data from 18,700 adolescents aged 13-17 years – 48% of whom were female – in the 2018 National Immunization Survey–Teen to discover that 51% of adolescents were up to date with the human papillomavirus (HPV) vaccine, and 68% had received at least one dose of the vaccine.
There was an increase in HPV vaccination coverage from 2017 to 2018, but this was attributable to a 4.4 percentage point increase in males who were up to date, compared with a 0.6 percentage point increase in females.
“Although HPV vaccination coverage improved, increases among all adolescents were modest compared with increases in previous years and were observed only among males,” wrote Tanja Y. Walker of the National Center for Immunization and Respiratory Diseases at the Centers for Disease Control and Prevention, and coauthors.![]()
The number of adolescents who had at least one dose of the quadrivalent meningococcal conjugate (4MenB) vaccine increased by 1.5 percentage points to 86.6%, while among individuals aged 17 years, coverage with two or more doses of 4MenB vaccine increased by 6.5 percentage points to 50.8%. Tdap coverage remained the same at 89% (MMWR 2019;68(33):718-23).
However, the study saw no significant increases in coverage with three or more hepatitis B vaccine doses, two or more MMR vaccine doses, or with one or more varicella vaccine doses in adolescents without a history of varicella disease.
Adolescents with Medicaid had higher HPV vaccination coverage than did adolescents with private health insurance. Uninsured adolescents had lower coverage overall, ranging from 4 percentage points lower for one or more varicella vaccine doses to 19 percentage points lower for two or more 4MenB vaccines, compared with adolescents with private health insurance.
Vaccination rates were lower among adolescents outside metropolitan areas, particularly when it came to being up to date with HPV vaccination, where there was a 15 percentage point difference, and with two or more doses of the quadrivalent meningococcal conjugate vaccine, where there was a 20 percentage point difference.
Provider recommendations to parents were associated with a higher rate of coverage with one or more doses of the HPV vaccine, but the prevalence of provider recommendations varied significantly from state to state. Overall, 78% of parents said they received a provider recommendation for the adolescent HPV vaccine, but that figure was as low as 60% in Mississippi and as high as 91% in Massachusetts.
Parents living in nonmetropolitan areas were less likely to report receiving a provider recommendation than were those in metropolitan principal cities.
“Equipping providers with the tools they need to give strong recommendations that emphasize the importance of HPV vaccination in preventing cancer and effectively address parental concerns is a priority, especially in states where provider recommendations were less commonly reported,” Ms. Walker and associates said.
No conflicts of interest were declared.
FROM MMWR
Key clinical point: Slightly more than half of adolescents in the United States are fully vaccinated with the HPV vaccine.
Major finding: Rates of full HPV vaccination are 51% among adolescents aged 13-17 years.
Study details: Analysis of data from 18,700 adolescents aged 13-17 years in the 2018 National Immunization Survey–Teen.
Disclosures: No conflicts of interest were declared.
Source: Walker T et al. MMWR 2019 Aug 23;68(33):718-23.
EULAR updates vaccination recommendations for autoimmune inflammatory rheumatic disease patients
Vaccination status should be reviewed annually for patients with autoimmune inflammatory rheumatic diseases, according to updated recommendations from the European League Against Rheumatism.

Patients with autoimmune inflammatory rheumatic diseases (AIIRD) are at increased risk for infections, and vaccination has been shown to reduce risk by “potentially translating into a lower rate of hospital admissions due to infections, emergency room visits, and the rate of invasive infectious diseases,” wrote Victoria Furer, MD, of Tel Aviv Sourasky Medical Center, and members of the task force that updated the recommendations, which were published in Annals of the Rheumatic Diseases.
However, AIIRD patients often go unvaccinated because of a lack of awareness or concerns about vaccine safety and efficacy, they said (Ann Rheum Dis. 2019 Aug 14. doi: 10.1136/annrheumdis-2019-215882).
The task force consisted of 21 experts, including patients, rheumatologists, immunologists, an infectious disease specialist, and health professionals in rheumatology representing eight countries. They evaluated data from four systematic literature reviews and developed nine recommendations based on six key principles.
“For each recommendation, the level of evidence for the incidence/prevalence of vaccine preventable infection in AIIRD, and efficacy/immunogenicity/safety of vaccination were stated, when available, followed by the strength of recommendation and the level of agreement,” the task force wrote.
These overarching principles start with an annual assessment of vaccination status by the AIIRD patient’s rheumatology team. Other principles include explanation of an individualized vaccination program to the patient as a foundation for joint decision-making, vaccinating patients during quiescent disease periods, vaccinating in advance of planned immunosuppression when possible, considering non-live vaccines for AIIRD patients also treated with systemic glucocorticoids and DMARDs, and considering live-attenuated vaccines with caution.
Several of the nine recommendations developed by the task force are modified from the previous recommendations issued in 2011. The task force made its recommendations with an eye toward optimizing individual risk stratification and avoiding “unnecessary” vaccination in AIIRD patients with low risk of infection as part of the update process. A notable change from the 2011 guidelines is the recommendation of both influenza and pneumococcal vaccinations for the majority of patients with AIIRD as opposed to all patients to emphasize the importance of individualized risk assessment, the task force noted.
The recommendations state that influenza vaccination and pneumococcal vaccination should be “strongly considered” for patients with AIIRD, and patients also should receive tetanus toxoid vaccination according to recommendations for the general population. However, clinicians should consider passive immunization for patients treated with B-cell depleting therapy, the task force wrote.
AIIRD patients at risk for hepatitis A and B should receive vaccinations for those diseases, with boosters or passive immunization if indicated, and high-risk patients may consider herpes zoster vaccination, according to the recommendations.
In addition, AIIRD patients – especially patients with systemic lupus erythematosus – should receive human papilloma virus vaccination according to recommendations for the general population, but AIIRD patients should avoid yellow fever vaccination, the task force stated. However, for AIIRD patients traveling to areas of yellow fever risk, “withholding immunosuppressive therapy to allow a safe vaccination or measuring serology in previously exposed patients may be considered.”
Finally, mothers treated with biologics during the second half of pregnancy should avoid live-attenuated vaccines for their newborns, and immunocompetent household members of AIIRD patients should be encouraged to follow national guidelines for routine vaccination with the exception of the oral polio vaccine, the task force concluded.
Vaccination status should be reviewed annually for patients with autoimmune inflammatory rheumatic diseases, according to updated recommendations from the European League Against Rheumatism.
Patients with autoimmune inflammatory rheumatic diseases (AIIRD) are at increased risk for infections, and vaccination has been shown to reduce risk by “potentially translating into a lower rate of hospital admissions due to infections, emergency room visits, and the rate of invasive infectious diseases,” wrote Victoria Furer, MD, of Tel Aviv Sourasky Medical Center, and members of the task force that updated the recommendations, which were published in Annals of the Rheumatic Diseases.
However, AIIRD patients often go unvaccinated because of a lack of awareness or concerns about vaccine safety and efficacy, they said (Ann Rheum Dis. 2019 Aug 14. doi: 10.1136/annrheumdis-2019-215882).
The task force consisted of 21 experts, including patients, rheumatologists, immunologists, an infectious disease specialist, and health professionals in rheumatology representing eight countries. They evaluated data from four systematic literature reviews and developed nine recommendations based on six key principles.
“For each recommendation, the level of evidence for the incidence/prevalence of vaccine preventable infection in AIIRD, and efficacy/immunogenicity/safety of vaccination were stated, when available, followed by the strength of recommendation and the level of agreement,” the task force wrote.
These overarching principles start with an annual assessment of vaccination status by the AIIRD patient’s rheumatology team. Other principles include explanation of an individualized vaccination program to the patient as a foundation for joint decision-making, vaccinating patients during quiescent disease periods, vaccinating in advance of planned immunosuppression when possible, considering non-live vaccines for AIIRD patients also treated with systemic glucocorticoids and DMARDs, and considering live-attenuated vaccines with caution.
Several of the nine recommendations developed by the task force are modified from the previous recommendations issued in 2011. The task force made its recommendations with an eye toward optimizing individual risk stratification and avoiding “unnecessary” vaccination in AIIRD patients with low risk of infection as part of the update process. A notable change from the 2011 guidelines is the recommendation of both influenza and pneumococcal vaccinations for the majority of patients with AIIRD as opposed to all patients to emphasize the importance of individualized risk assessment, the task force noted.
The recommendations state that influenza vaccination and pneumococcal vaccination should be “strongly considered” for patients with AIIRD, and patients also should receive tetanus toxoid vaccination according to recommendations for the general population. However, clinicians should consider passive immunization for patients treated with B-cell depleting therapy, the task force wrote.
AIIRD patients at risk for hepatitis A and B should receive vaccinations for those diseases, with boosters or passive immunization if indicated, and high-risk patients may consider herpes zoster vaccination, according to the recommendations.
In addition, AIIRD patients – especially patients with systemic lupus erythematosus – should receive human papilloma virus vaccination according to recommendations for the general population, but AIIRD patients should avoid yellow fever vaccination, the task force stated. However, for AIIRD patients traveling to areas of yellow fever risk, “withholding immunosuppressive therapy to allow a safe vaccination or measuring serology in previously exposed patients may be considered.”
Finally, mothers treated with biologics during the second half of pregnancy should avoid live-attenuated vaccines for their newborns, and immunocompetent household members of AIIRD patients should be encouraged to follow national guidelines for routine vaccination with the exception of the oral polio vaccine, the task force concluded.
Vaccination status should be reviewed annually for patients with autoimmune inflammatory rheumatic diseases, according to updated recommendations from the European League Against Rheumatism.
Patients with autoimmune inflammatory rheumatic diseases (AIIRD) are at increased risk for infections, and vaccination has been shown to reduce risk by “potentially translating into a lower rate of hospital admissions due to infections, emergency room visits, and the rate of invasive infectious diseases,” wrote Victoria Furer, MD, of Tel Aviv Sourasky Medical Center, and members of the task force that updated the recommendations, which were published in Annals of the Rheumatic Diseases.
However, AIIRD patients often go unvaccinated because of a lack of awareness or concerns about vaccine safety and efficacy, they said (Ann Rheum Dis. 2019 Aug 14. doi: 10.1136/annrheumdis-2019-215882).
The task force consisted of 21 experts, including patients, rheumatologists, immunologists, an infectious disease specialist, and health professionals in rheumatology representing eight countries. They evaluated data from four systematic literature reviews and developed nine recommendations based on six key principles.
“For each recommendation, the level of evidence for the incidence/prevalence of vaccine preventable infection in AIIRD, and efficacy/immunogenicity/safety of vaccination were stated, when available, followed by the strength of recommendation and the level of agreement,” the task force wrote.
These overarching principles start with an annual assessment of vaccination status by the AIIRD patient’s rheumatology team. Other principles include explanation of an individualized vaccination program to the patient as a foundation for joint decision-making, vaccinating patients during quiescent disease periods, vaccinating in advance of planned immunosuppression when possible, considering non-live vaccines for AIIRD patients also treated with systemic glucocorticoids and DMARDs, and considering live-attenuated vaccines with caution.
Several of the nine recommendations developed by the task force are modified from the previous recommendations issued in 2011. The task force made its recommendations with an eye toward optimizing individual risk stratification and avoiding “unnecessary” vaccination in AIIRD patients with low risk of infection as part of the update process. A notable change from the 2011 guidelines is the recommendation of both influenza and pneumococcal vaccinations for the majority of patients with AIIRD as opposed to all patients to emphasize the importance of individualized risk assessment, the task force noted.
The recommendations state that influenza vaccination and pneumococcal vaccination should be “strongly considered” for patients with AIIRD, and patients also should receive tetanus toxoid vaccination according to recommendations for the general population. However, clinicians should consider passive immunization for patients treated with B-cell depleting therapy, the task force wrote.
AIIRD patients at risk for hepatitis A and B should receive vaccinations for those diseases, with boosters or passive immunization if indicated, and high-risk patients may consider herpes zoster vaccination, according to the recommendations.
In addition, AIIRD patients – especially patients with systemic lupus erythematosus – should receive human papilloma virus vaccination according to recommendations for the general population, but AIIRD patients should avoid yellow fever vaccination, the task force stated. However, for AIIRD patients traveling to areas of yellow fever risk, “withholding immunosuppressive therapy to allow a safe vaccination or measuring serology in previously exposed patients may be considered.”
Finally, mothers treated with biologics during the second half of pregnancy should avoid live-attenuated vaccines for their newborns, and immunocompetent household members of AIIRD patients should be encouraged to follow national guidelines for routine vaccination with the exception of the oral polio vaccine, the task force concluded.
FROM ANNALS OF THE RHEUMATIC DISEASES
FUO, pneumonia often distinguishes influenza from RSV in hospitalized young children
LJUBLJANA, SLOVENIA – as the cause of hospitalization in infants and young children, Cihan Papan, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.

Dr. Papan, a pediatrician at University Children’s Hospital Mannheim (Germany) and Heidelberg (Germany) University, presented a retrospective single-center study of all 573 children aged under 2 years hospitalized over the course of several seasons for respiratory syncytial virus (RSV) or influenza as confirmed by rapid antigen testing. Even though these are two of the leading causes of hospitalization among young children, there is surprisingly sparse data comparing the two in terms of disease severity and hospital resource utilization, including antibiotic consumption. That information gap provided the basis for this study.
There were 476 children with confirmed RSV, 96 with influenza, and 1 RSV/influenza coinfection. Notably, even though the RSV group had lower temperatures and C-reactive protein levels, they were nevertheless more likely to be treated with antibiotics, by a margin of 29% to 23%.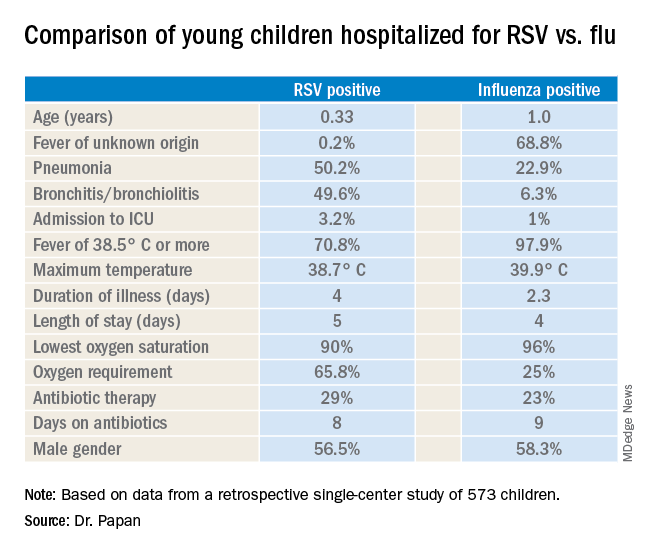
“These findings open new possibilities for antimicrobial stewardship in these groups of virally infected children,” observed Dr. Papan.
Fever of unknown origin was present in 68.8% of the influenza-positive patients, compared with just 0.2% of the RSV-positive children. In contrast, 50.2% of the RSV group had pneumonia and 49.6% had bronchitis or bronchiolitis, versus just 22.9% and 6.3% of the influenza patients, respectively. A larger proportion of the young children with RSV infection presented in a severely ill–looking condition. Children with RSV infection also were significantly younger.
Dr. Papan reported having no financial conflicts regarding his study.
LJUBLJANA, SLOVENIA – as the cause of hospitalization in infants and young children, Cihan Papan, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
Dr. Papan, a pediatrician at University Children’s Hospital Mannheim (Germany) and Heidelberg (Germany) University, presented a retrospective single-center study of all 573 children aged under 2 years hospitalized over the course of several seasons for respiratory syncytial virus (RSV) or influenza as confirmed by rapid antigen testing. Even though these are two of the leading causes of hospitalization among young children, there is surprisingly sparse data comparing the two in terms of disease severity and hospital resource utilization, including antibiotic consumption. That information gap provided the basis for this study.
There were 476 children with confirmed RSV, 96 with influenza, and 1 RSV/influenza coinfection. Notably, even though the RSV group had lower temperatures and C-reactive protein levels, they were nevertheless more likely to be treated with antibiotics, by a margin of 29% to 23%.
“These findings open new possibilities for antimicrobial stewardship in these groups of virally infected children,” observed Dr. Papan.
Fever of unknown origin was present in 68.8% of the influenza-positive patients, compared with just 0.2% of the RSV-positive children. In contrast, 50.2% of the RSV group had pneumonia and 49.6% had bronchitis or bronchiolitis, versus just 22.9% and 6.3% of the influenza patients, respectively. A larger proportion of the young children with RSV infection presented in a severely ill–looking condition. Children with RSV infection also were significantly younger.
Dr. Papan reported having no financial conflicts regarding his study.
LJUBLJANA, SLOVENIA – as the cause of hospitalization in infants and young children, Cihan Papan, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
Dr. Papan, a pediatrician at University Children’s Hospital Mannheim (Germany) and Heidelberg (Germany) University, presented a retrospective single-center study of all 573 children aged under 2 years hospitalized over the course of several seasons for respiratory syncytial virus (RSV) or influenza as confirmed by rapid antigen testing. Even though these are two of the leading causes of hospitalization among young children, there is surprisingly sparse data comparing the two in terms of disease severity and hospital resource utilization, including antibiotic consumption. That information gap provided the basis for this study.
There were 476 children with confirmed RSV, 96 with influenza, and 1 RSV/influenza coinfection. Notably, even though the RSV group had lower temperatures and C-reactive protein levels, they were nevertheless more likely to be treated with antibiotics, by a margin of 29% to 23%.
“These findings open new possibilities for antimicrobial stewardship in these groups of virally infected children,” observed Dr. Papan.
Fever of unknown origin was present in 68.8% of the influenza-positive patients, compared with just 0.2% of the RSV-positive children. In contrast, 50.2% of the RSV group had pneumonia and 49.6% had bronchitis or bronchiolitis, versus just 22.9% and 6.3% of the influenza patients, respectively. A larger proportion of the young children with RSV infection presented in a severely ill–looking condition. Children with RSV infection also were significantly younger.
Dr. Papan reported having no financial conflicts regarding his study.
REPORTING FROM ESPID 2019
Treating children with Kawasaki disease and coronary enlargement
IVIG plus steroids or infliximab, or IVIG alone?
Clinical question
Does use of corticosteroids or infliximab in addition to intravenous immunoglobulin improve cardiac outcomes in children with Kawasaki disease and enlarged coronary arteries?
Background
Kawasaki disease is a medium-vessel vasculitis primarily of young children. While the underlying cause remains unknown, treatment with intravenous immunoglobulin (IVIG) substantially lowers the risk of coronary artery aneurysms (CAA), the most serious sequelae of Kawasaki disease. Recent studies have suggested that – in cases of high-risk or treatment-resistant Kawasaki disease – using an immunomodulator, such as a corticosteroid or a TNF-alpha blocker, may improve outcomes, though these studies involved relatively small and homogeneous patient populations. It is unknown if these medications could prevent progression of CAA.
Study design
Retrospective multicenter study.
Setting
Two freestanding children’s hospitals and one mother-child hospital.
Synopsis
The study identified 121 children diagnosed with Kawasaki disease with CAA (z score 2.5-10) from 2008 through 2017 treated at the three study hospitals. Children with giant CAA at the time of diagnosis (z score greater than 10) or significant preexisting congenital heart disease were excluded.
All study hospitals had protocols for treatment of Kawasaki disease: Center 1 used IVIG and corticosteroids, Center 2 used IVIG and infliximab, and Center 3 used IVIG alone. Patients at all centers also received aspirin. Center 1 used methylprednisolone IV initially, changing to oral prednisolone after clinical improvement. The researchers reviewed the charts of each patient and classified them as having complete or incomplete Kawasaki disease. They assigned z scores for CAA size based on both initial and follow-up echocardiograms. The primary outcome was change in z score of CAA over the first year.
The population of patients treated at each center was significantly different. Center 1 reported older patients (median age 2.6 vs. 2.0 and 1.1), as well as a higher rate of male patients (83% vs. 77% and 58%). However, there was no difference in baseline z scores between centers. Patients who initially received IVIG and corticosteroids were less likely to require additional therapy because of persistent fever versus those receiving IVIG only, or IVIG and infliximab (0% vs. 21% vs. 14%, P = .03).
Patients receiving IVIG and corticosteroids, or IVIG and infliximab, were less likely to have progression of CAA size, with 23% and 24% having an increase in z score of more than 1 versus 58% of those who received IVIG alone. No group had significant differences in maximum z score, the rate of giant aneurysms, or the rate of regression of CAA.
Bottom line
Using IVIG + corticosteroids or IVIG + infliximab versus IVIG alone for children with Kawasaki disease with coronary artery aneurysms decreases the rate of aneurysm enlargement.
Citation
Dionne A et al. Treatment intensification in patients with Kawasaki disease and coronary aneurysm at diagnosis. Pediatrics. May 2019:e20183341. doi: 10.1542/peds.2018-3341.
Dr. Stubblefield is a pediatric hospitalist at Nemours/Alfred I. duPont Hospital for Children in Wilmington, Del., and clinical assistant professor of pediatrics at Sidney Kimmel Medical College at Thomas Jefferson University in Philadelphia.
IVIG plus steroids or infliximab, or IVIG alone?
IVIG plus steroids or infliximab, or IVIG alone?
Clinical question
Does use of corticosteroids or infliximab in addition to intravenous immunoglobulin improve cardiac outcomes in children with Kawasaki disease and enlarged coronary arteries?
Background
Kawasaki disease is a medium-vessel vasculitis primarily of young children. While the underlying cause remains unknown, treatment with intravenous immunoglobulin (IVIG) substantially lowers the risk of coronary artery aneurysms (CAA), the most serious sequelae of Kawasaki disease. Recent studies have suggested that – in cases of high-risk or treatment-resistant Kawasaki disease – using an immunomodulator, such as a corticosteroid or a TNF-alpha blocker, may improve outcomes, though these studies involved relatively small and homogeneous patient populations. It is unknown if these medications could prevent progression of CAA.
Study design
Retrospective multicenter study.
Setting
Two freestanding children’s hospitals and one mother-child hospital.
Synopsis
The study identified 121 children diagnosed with Kawasaki disease with CAA (z score 2.5-10) from 2008 through 2017 treated at the three study hospitals. Children with giant CAA at the time of diagnosis (z score greater than 10) or significant preexisting congenital heart disease were excluded.
All study hospitals had protocols for treatment of Kawasaki disease: Center 1 used IVIG and corticosteroids, Center 2 used IVIG and infliximab, and Center 3 used IVIG alone. Patients at all centers also received aspirin. Center 1 used methylprednisolone IV initially, changing to oral prednisolone after clinical improvement. The researchers reviewed the charts of each patient and classified them as having complete or incomplete Kawasaki disease. They assigned z scores for CAA size based on both initial and follow-up echocardiograms. The primary outcome was change in z score of CAA over the first year.
The population of patients treated at each center was significantly different. Center 1 reported older patients (median age 2.6 vs. 2.0 and 1.1), as well as a higher rate of male patients (83% vs. 77% and 58%). However, there was no difference in baseline z scores between centers. Patients who initially received IVIG and corticosteroids were less likely to require additional therapy because of persistent fever versus those receiving IVIG only, or IVIG and infliximab (0% vs. 21% vs. 14%, P = .03).
Patients receiving IVIG and corticosteroids, or IVIG and infliximab, were less likely to have progression of CAA size, with 23% and 24% having an increase in z score of more than 1 versus 58% of those who received IVIG alone. No group had significant differences in maximum z score, the rate of giant aneurysms, or the rate of regression of CAA.
Bottom line
Using IVIG + corticosteroids or IVIG + infliximab versus IVIG alone for children with Kawasaki disease with coronary artery aneurysms decreases the rate of aneurysm enlargement.
Citation
Dionne A et al. Treatment intensification in patients with Kawasaki disease and coronary aneurysm at diagnosis. Pediatrics. May 2019:e20183341. doi: 10.1542/peds.2018-3341.
Dr. Stubblefield is a pediatric hospitalist at Nemours/Alfred I. duPont Hospital for Children in Wilmington, Del., and clinical assistant professor of pediatrics at Sidney Kimmel Medical College at Thomas Jefferson University in Philadelphia.
Clinical question
Does use of corticosteroids or infliximab in addition to intravenous immunoglobulin improve cardiac outcomes in children with Kawasaki disease and enlarged coronary arteries?
Background
Kawasaki disease is a medium-vessel vasculitis primarily of young children. While the underlying cause remains unknown, treatment with intravenous immunoglobulin (IVIG) substantially lowers the risk of coronary artery aneurysms (CAA), the most serious sequelae of Kawasaki disease. Recent studies have suggested that – in cases of high-risk or treatment-resistant Kawasaki disease – using an immunomodulator, such as a corticosteroid or a TNF-alpha blocker, may improve outcomes, though these studies involved relatively small and homogeneous patient populations. It is unknown if these medications could prevent progression of CAA.
Study design
Retrospective multicenter study.
Setting
Two freestanding children’s hospitals and one mother-child hospital.
Synopsis
The study identified 121 children diagnosed with Kawasaki disease with CAA (z score 2.5-10) from 2008 through 2017 treated at the three study hospitals. Children with giant CAA at the time of diagnosis (z score greater than 10) or significant preexisting congenital heart disease were excluded.
All study hospitals had protocols for treatment of Kawasaki disease: Center 1 used IVIG and corticosteroids, Center 2 used IVIG and infliximab, and Center 3 used IVIG alone. Patients at all centers also received aspirin. Center 1 used methylprednisolone IV initially, changing to oral prednisolone after clinical improvement. The researchers reviewed the charts of each patient and classified them as having complete or incomplete Kawasaki disease. They assigned z scores for CAA size based on both initial and follow-up echocardiograms. The primary outcome was change in z score of CAA over the first year.
The population of patients treated at each center was significantly different. Center 1 reported older patients (median age 2.6 vs. 2.0 and 1.1), as well as a higher rate of male patients (83% vs. 77% and 58%). However, there was no difference in baseline z scores between centers. Patients who initially received IVIG and corticosteroids were less likely to require additional therapy because of persistent fever versus those receiving IVIG only, or IVIG and infliximab (0% vs. 21% vs. 14%, P = .03).
Patients receiving IVIG and corticosteroids, or IVIG and infliximab, were less likely to have progression of CAA size, with 23% and 24% having an increase in z score of more than 1 versus 58% of those who received IVIG alone. No group had significant differences in maximum z score, the rate of giant aneurysms, or the rate of regression of CAA.
Bottom line
Using IVIG + corticosteroids or IVIG + infliximab versus IVIG alone for children with Kawasaki disease with coronary artery aneurysms decreases the rate of aneurysm enlargement.
Citation
Dionne A et al. Treatment intensification in patients with Kawasaki disease and coronary aneurysm at diagnosis. Pediatrics. May 2019:e20183341. doi: 10.1542/peds.2018-3341.
Dr. Stubblefield is a pediatric hospitalist at Nemours/Alfred I. duPont Hospital for Children in Wilmington, Del., and clinical assistant professor of pediatrics at Sidney Kimmel Medical College at Thomas Jefferson University in Philadelphia.
Oncologists agree with AI treatment decisions about half the time
When it comes to treatment recommendations for high-risk breast cancer, oncologists agree with a leading artificial intelligence platform about half the time, according to investigators.
In the first study of its kind, involving 10 Chinese oncologists, recommendation concordance with the Watson for Oncology treatment advisory tool (WfO) was generally lower for hormone receptor–positive and metastatic cancers than hormone receptor–negative and nonmetastatic cases, reported Fengrui Xu, MD, of the Academy of Military Medical Sciences in Beijing, and colleagues. Refinement could enable broad use of Watson, not to dictate treatment decisions, but instead to propose alternate treatment approaches and offer point-of-care access to relevant evidence.
“[WfO] is an example of a quantitative oncology clinical decision support that leverages the clinical expertise of oncologists at Memorial Sloan Kettering Cancer Center [MSKCC],” the investigators wrote in JCO Clinical Cancer Informatics. The platform uses machine-learning software to interpret patient scenarios in light from MSKCC training cases, MSKCC treatment guidelines, and more than 300 medical textbooks and journals.
To compare WfO with real-world decision makers, the investigators recruited three chief physicians, four attending physicians, and three fellows to provide treatment recommendations for 1,977 patients with complex breast cancer who were treated at 10 hospitals in China. Participating physicians shared the workload; each evaluated an average of 198 different cases.
On average, oncologists and WfO made the same treatment recommendations 56% of the time. Out of the different types of physicians, fellows were most likely to agree with WfO, based on a 68% concordance rate, compared with 54% for chief physicians and 49% for attending physicians. Including all physicians, concordance was lowest for hormone receptor–positive/HER2-positive disease (48%) and highest for triple-negative cases (71%). Adjuvant and metastatic therapies were also evaluated, with high concordance for adjuvant endocrine (78%) and targeted therapy (100%), compared with moderate concordance for first- (52%) and second-line metastatic therapy (50%). The investigators described concordance results as generally “modest;” however, they noted that such levels are promising.
“This degree of concordance is encouraging because therapeutic decisions in these cases are often difficult as a result of the current limits of medical knowledge for treating complex breast cancers and the presence of local contextual factors that affect physician treatment choices,” the investigators wrote. “It is important to note that nonconcordance does not imply that one treatment is correct for a given patient and another is not, nor does it necessarily diminish the potential value of a decision support system that provides access to supporting evidence and insight into its reasoning process.”
The study was funded by Zefei Jiang. The investigators reported affiliations with IBM Watson Health, Pharmaceutical Manufacturer Institution, Merck, and others.
SOURCE: Xu F et al. JCO Clin Cancer Inform. 2019 Aug 16. doi: 10.1200/CCI.18.00159.
When it comes to treatment recommendations for high-risk breast cancer, oncologists agree with a leading artificial intelligence platform about half the time, according to investigators.
In the first study of its kind, involving 10 Chinese oncologists, recommendation concordance with the Watson for Oncology treatment advisory tool (WfO) was generally lower for hormone receptor–positive and metastatic cancers than hormone receptor–negative and nonmetastatic cases, reported Fengrui Xu, MD, of the Academy of Military Medical Sciences in Beijing, and colleagues. Refinement could enable broad use of Watson, not to dictate treatment decisions, but instead to propose alternate treatment approaches and offer point-of-care access to relevant evidence.
“[WfO] is an example of a quantitative oncology clinical decision support that leverages the clinical expertise of oncologists at Memorial Sloan Kettering Cancer Center [MSKCC],” the investigators wrote in JCO Clinical Cancer Informatics. The platform uses machine-learning software to interpret patient scenarios in light from MSKCC training cases, MSKCC treatment guidelines, and more than 300 medical textbooks and journals.
To compare WfO with real-world decision makers, the investigators recruited three chief physicians, four attending physicians, and three fellows to provide treatment recommendations for 1,977 patients with complex breast cancer who were treated at 10 hospitals in China. Participating physicians shared the workload; each evaluated an average of 198 different cases.
On average, oncologists and WfO made the same treatment recommendations 56% of the time. Out of the different types of physicians, fellows were most likely to agree with WfO, based on a 68% concordance rate, compared with 54% for chief physicians and 49% for attending physicians. Including all physicians, concordance was lowest for hormone receptor–positive/HER2-positive disease (48%) and highest for triple-negative cases (71%). Adjuvant and metastatic therapies were also evaluated, with high concordance for adjuvant endocrine (78%) and targeted therapy (100%), compared with moderate concordance for first- (52%) and second-line metastatic therapy (50%). The investigators described concordance results as generally “modest;” however, they noted that such levels are promising.
“This degree of concordance is encouraging because therapeutic decisions in these cases are often difficult as a result of the current limits of medical knowledge for treating complex breast cancers and the presence of local contextual factors that affect physician treatment choices,” the investigators wrote. “It is important to note that nonconcordance does not imply that one treatment is correct for a given patient and another is not, nor does it necessarily diminish the potential value of a decision support system that provides access to supporting evidence and insight into its reasoning process.”
The study was funded by Zefei Jiang. The investigators reported affiliations with IBM Watson Health, Pharmaceutical Manufacturer Institution, Merck, and others.
SOURCE: Xu F et al. JCO Clin Cancer Inform. 2019 Aug 16. doi: 10.1200/CCI.18.00159.
When it comes to treatment recommendations for high-risk breast cancer, oncologists agree with a leading artificial intelligence platform about half the time, according to investigators.
In the first study of its kind, involving 10 Chinese oncologists, recommendation concordance with the Watson for Oncology treatment advisory tool (WfO) was generally lower for hormone receptor–positive and metastatic cancers than hormone receptor–negative and nonmetastatic cases, reported Fengrui Xu, MD, of the Academy of Military Medical Sciences in Beijing, and colleagues. Refinement could enable broad use of Watson, not to dictate treatment decisions, but instead to propose alternate treatment approaches and offer point-of-care access to relevant evidence.
“[WfO] is an example of a quantitative oncology clinical decision support that leverages the clinical expertise of oncologists at Memorial Sloan Kettering Cancer Center [MSKCC],” the investigators wrote in JCO Clinical Cancer Informatics. The platform uses machine-learning software to interpret patient scenarios in light from MSKCC training cases, MSKCC treatment guidelines, and more than 300 medical textbooks and journals.
To compare WfO with real-world decision makers, the investigators recruited three chief physicians, four attending physicians, and three fellows to provide treatment recommendations for 1,977 patients with complex breast cancer who were treated at 10 hospitals in China. Participating physicians shared the workload; each evaluated an average of 198 different cases.
On average, oncologists and WfO made the same treatment recommendations 56% of the time. Out of the different types of physicians, fellows were most likely to agree with WfO, based on a 68% concordance rate, compared with 54% for chief physicians and 49% for attending physicians. Including all physicians, concordance was lowest for hormone receptor–positive/HER2-positive disease (48%) and highest for triple-negative cases (71%). Adjuvant and metastatic therapies were also evaluated, with high concordance for adjuvant endocrine (78%) and targeted therapy (100%), compared with moderate concordance for first- (52%) and second-line metastatic therapy (50%). The investigators described concordance results as generally “modest;” however, they noted that such levels are promising.
“This degree of concordance is encouraging because therapeutic decisions in these cases are often difficult as a result of the current limits of medical knowledge for treating complex breast cancers and the presence of local contextual factors that affect physician treatment choices,” the investigators wrote. “It is important to note that nonconcordance does not imply that one treatment is correct for a given patient and another is not, nor does it necessarily diminish the potential value of a decision support system that provides access to supporting evidence and insight into its reasoning process.”
The study was funded by Zefei Jiang. The investigators reported affiliations with IBM Watson Health, Pharmaceutical Manufacturer Institution, Merck, and others.
SOURCE: Xu F et al. JCO Clin Cancer Inform. 2019 Aug 16. doi: 10.1200/CCI.18.00159.
FROM JCO CLINICAL CANCER INFORMATICS