User login
ICYMI: Andexanet alfa reduces anti–factor Xa activity from apixaban, rivaroxaban
Patients with acute major bleeding associated with factor Xa inhibitor usage who received andexanet alfa experienced a significant decrease in anti–factor Xa activity, with more than three-quarters of patients experiencing good or excellent hemostatic efficiency after 12 hours. That finding emerged from the multicenter, prospective, open-label, single-group ANNEXA-4 trial published in the New England Journal of Medicine (2019 Feb 11. doi: 10.1056/NEJMoa1814051).
We reported this story at the annual meeting of the American College of Cardiology before it was published in the journal. Find our coverage at the link below.
Patients with acute major bleeding associated with factor Xa inhibitor usage who received andexanet alfa experienced a significant decrease in anti–factor Xa activity, with more than three-quarters of patients experiencing good or excellent hemostatic efficiency after 12 hours. That finding emerged from the multicenter, prospective, open-label, single-group ANNEXA-4 trial published in the New England Journal of Medicine (2019 Feb 11. doi: 10.1056/NEJMoa1814051).
We reported this story at the annual meeting of the American College of Cardiology before it was published in the journal. Find our coverage at the link below.
Patients with acute major bleeding associated with factor Xa inhibitor usage who received andexanet alfa experienced a significant decrease in anti–factor Xa activity, with more than three-quarters of patients experiencing good or excellent hemostatic efficiency after 12 hours. That finding emerged from the multicenter, prospective, open-label, single-group ANNEXA-4 trial published in the New England Journal of Medicine (2019 Feb 11. doi: 10.1056/NEJMoa1814051).
We reported this story at the annual meeting of the American College of Cardiology before it was published in the journal. Find our coverage at the link below.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
FDA approves first interoperable insulin infusion pump
, for insulin delivery in children and adults with diabetes.

The pump delivers insulin under the skin at a variable or fixed rate. It can function on its own, or it can be digitally connected to automatically communicate with and receive drug-dosing commands from other diabetes management devices, such as automated insulin-dosing systems, the agency announced.
The approval was based on a review of performance data demonstrating that the device can deliver insulin accurately and reliably and at the rates and volumes programmed by the user. The agency also assessed the pump’s ability to connect reliably with other devices, as well as its cybersecurity and fail-safe modes.
Risks associated with the device were similar to those of other infusion pumps and include infection, bleeding, pain, or skin irritations. Blockages and air bubbles can occur in the tubing, which will affect drug delivery. Risks associated with incorrect drug delivery include hypo- and hyperglycemia as well as diabetic ketoacidosis.
“The marketing authorization of the [pump] has the potential to aid patients who seek more individualized diabetes therapy systems and opens the door for developers of future connected diabetes devices to get other safe and effective products to patients more efficiently,” FDA Commissioner Scott Gottlieb, MD, said in the announcement.
, for insulin delivery in children and adults with diabetes.
The pump delivers insulin under the skin at a variable or fixed rate. It can function on its own, or it can be digitally connected to automatically communicate with and receive drug-dosing commands from other diabetes management devices, such as automated insulin-dosing systems, the agency announced.
The approval was based on a review of performance data demonstrating that the device can deliver insulin accurately and reliably and at the rates and volumes programmed by the user. The agency also assessed the pump’s ability to connect reliably with other devices, as well as its cybersecurity and fail-safe modes.
Risks associated with the device were similar to those of other infusion pumps and include infection, bleeding, pain, or skin irritations. Blockages and air bubbles can occur in the tubing, which will affect drug delivery. Risks associated with incorrect drug delivery include hypo- and hyperglycemia as well as diabetic ketoacidosis.
“The marketing authorization of the [pump] has the potential to aid patients who seek more individualized diabetes therapy systems and opens the door for developers of future connected diabetes devices to get other safe and effective products to patients more efficiently,” FDA Commissioner Scott Gottlieb, MD, said in the announcement.
, for insulin delivery in children and adults with diabetes.
The pump delivers insulin under the skin at a variable or fixed rate. It can function on its own, or it can be digitally connected to automatically communicate with and receive drug-dosing commands from other diabetes management devices, such as automated insulin-dosing systems, the agency announced.
The approval was based on a review of performance data demonstrating that the device can deliver insulin accurately and reliably and at the rates and volumes programmed by the user. The agency also assessed the pump’s ability to connect reliably with other devices, as well as its cybersecurity and fail-safe modes.
Risks associated with the device were similar to those of other infusion pumps and include infection, bleeding, pain, or skin irritations. Blockages and air bubbles can occur in the tubing, which will affect drug delivery. Risks associated with incorrect drug delivery include hypo- and hyperglycemia as well as diabetic ketoacidosis.
“The marketing authorization of the [pump] has the potential to aid patients who seek more individualized diabetes therapy systems and opens the door for developers of future connected diabetes devices to get other safe and effective products to patients more efficiently,” FDA Commissioner Scott Gottlieb, MD, said in the announcement.
Flu season showing its staying power
Like an unwelcome guest, the 2018-2019 flu season seems to be settling in for a lengthy stay as three more states have reached the highest level of influenza-like illness (ILI) activity, according to the Centers for Disease Control and Prevention.
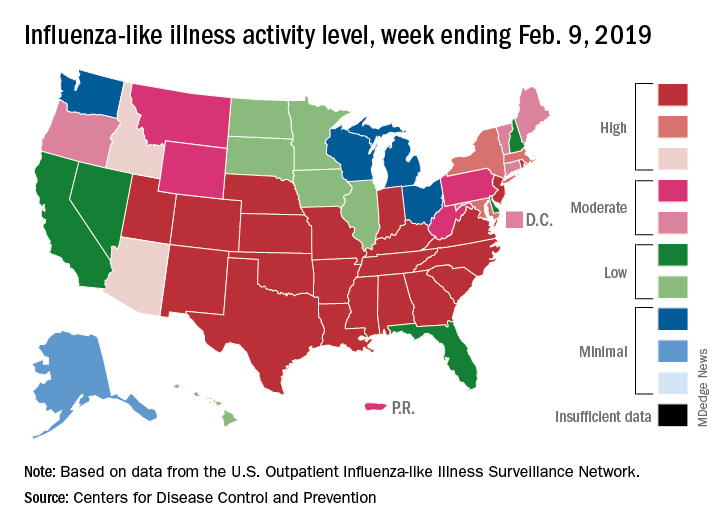
There are now 21 states at level 10 on the CDC’s 1-10 scale, with the South showing up almost solidly red on the flu activity map for the week ending Feb. 9. Another five states are at levels 8 and 9, bringing the total in the high range to 26 for the week, compared with 24 the previous week, the CDC’s influenza division reported Feb. 15.
National activity, reflected in the proportion of outpatient visits involving ILI, took a step up from 4.3% the week before to 4.8% for the week ending Feb. 9. The national baseline rate is 2.2% for ILI, which the CDC defines “as fever (temperature of 100°F [37.8°C] or greater) and cough and/or sore throat.”
Two flu-related pediatric deaths occurred during the week ending Feb. 9, and another four were reported from earlier weeks, which brings the total for the 2018-2019 season to 34, the CDC said. At the same point in last year’s flu season, there had been 84 flu-related deaths in children.
In a separate report, the CDC said that, based on data collected from Nov. 23, 2018 to Feb. 2, 2019, “the influenza vaccine has been 47% effective in preventing medically attended acute respiratory virus infection across all age groups and specifically was 46% effective in preventing medical visits associated with influenza A(H1N1)pdm09.” The effectiveness of the vaccine was 61% for children aged 6 months to 17 years, the CDC said (MMWR. 2019 Feb 15;68[6];135-9).
Flu vaccination during the 2017-2018 season prevented 7.1 million illnesses, 3.7 million medical visits, 109,000 hospitalizations, and 8,000 flu-related deaths, the CDC said, adding that “vaccination has been found to reduce deaths, intensive care unit admissions and length of stay, and overall duration of hospitalization among hospitalized influenza patients.”
Forecasts for the rest of the 2018-2019 season “predict that elevated influenza activity in parts of the United States will continue for several more weeks,” the CDC said.
Like an unwelcome guest, the 2018-2019 flu season seems to be settling in for a lengthy stay as three more states have reached the highest level of influenza-like illness (ILI) activity, according to the Centers for Disease Control and Prevention.
There are now 21 states at level 10 on the CDC’s 1-10 scale, with the South showing up almost solidly red on the flu activity map for the week ending Feb. 9. Another five states are at levels 8 and 9, bringing the total in the high range to 26 for the week, compared with 24 the previous week, the CDC’s influenza division reported Feb. 15.
National activity, reflected in the proportion of outpatient visits involving ILI, took a step up from 4.3% the week before to 4.8% for the week ending Feb. 9. The national baseline rate is 2.2% for ILI, which the CDC defines “as fever (temperature of 100°F [37.8°C] or greater) and cough and/or sore throat.”
Two flu-related pediatric deaths occurred during the week ending Feb. 9, and another four were reported from earlier weeks, which brings the total for the 2018-2019 season to 34, the CDC said. At the same point in last year’s flu season, there had been 84 flu-related deaths in children.
In a separate report, the CDC said that, based on data collected from Nov. 23, 2018 to Feb. 2, 2019, “the influenza vaccine has been 47% effective in preventing medically attended acute respiratory virus infection across all age groups and specifically was 46% effective in preventing medical visits associated with influenza A(H1N1)pdm09.” The effectiveness of the vaccine was 61% for children aged 6 months to 17 years, the CDC said (MMWR. 2019 Feb 15;68[6];135-9).
Flu vaccination during the 2017-2018 season prevented 7.1 million illnesses, 3.7 million medical visits, 109,000 hospitalizations, and 8,000 flu-related deaths, the CDC said, adding that “vaccination has been found to reduce deaths, intensive care unit admissions and length of stay, and overall duration of hospitalization among hospitalized influenza patients.”
Forecasts for the rest of the 2018-2019 season “predict that elevated influenza activity in parts of the United States will continue for several more weeks,” the CDC said.
Like an unwelcome guest, the 2018-2019 flu season seems to be settling in for a lengthy stay as three more states have reached the highest level of influenza-like illness (ILI) activity, according to the Centers for Disease Control and Prevention.
There are now 21 states at level 10 on the CDC’s 1-10 scale, with the South showing up almost solidly red on the flu activity map for the week ending Feb. 9. Another five states are at levels 8 and 9, bringing the total in the high range to 26 for the week, compared with 24 the previous week, the CDC’s influenza division reported Feb. 15.
National activity, reflected in the proportion of outpatient visits involving ILI, took a step up from 4.3% the week before to 4.8% for the week ending Feb. 9. The national baseline rate is 2.2% for ILI, which the CDC defines “as fever (temperature of 100°F [37.8°C] or greater) and cough and/or sore throat.”
Two flu-related pediatric deaths occurred during the week ending Feb. 9, and another four were reported from earlier weeks, which brings the total for the 2018-2019 season to 34, the CDC said. At the same point in last year’s flu season, there had been 84 flu-related deaths in children.
In a separate report, the CDC said that, based on data collected from Nov. 23, 2018 to Feb. 2, 2019, “the influenza vaccine has been 47% effective in preventing medically attended acute respiratory virus infection across all age groups and specifically was 46% effective in preventing medical visits associated with influenza A(H1N1)pdm09.” The effectiveness of the vaccine was 61% for children aged 6 months to 17 years, the CDC said (MMWR. 2019 Feb 15;68[6];135-9).
Flu vaccination during the 2017-2018 season prevented 7.1 million illnesses, 3.7 million medical visits, 109,000 hospitalizations, and 8,000 flu-related deaths, the CDC said, adding that “vaccination has been found to reduce deaths, intensive care unit admissions and length of stay, and overall duration of hospitalization among hospitalized influenza patients.”
Forecasts for the rest of the 2018-2019 season “predict that elevated influenza activity in parts of the United States will continue for several more weeks,” the CDC said.
CMS proposes coverage of CAR T-cell therapy in trials
The Centers for Medicare & Medicaid Services has proposed to cover chimeric antigen receptor (CAR) T-cell therapy for cancer patients participating in clinical trials that study the treatment’s effectiveness, according to a Feb. 15 announcement.

The proposed national coverage determination would require CMS to cover CAR T-cell therapies nationwide when the treatment is offered in CMS-approved registries or clinical studies in which patients are monitored for 2 or more years following treatment.
Results from the studies would help CMS identify which patients benefit most from CAR T-cell therapies and inform future coverage decisions, CMS Administrator Seema Verma said.
“CAR T-cell therapy was the first FDA-approved gene therapy, marking the beginning of an entirely new approach to treating serious and even life-threatening diseases,” Ms. Verma said in a statement. “Today’s proposed coverage decision would improve access to this therapy while deepening CMS’s understanding of how patients in Medicare respond to it, so the agency can ensure that it is paying for CAR T-cell therapy for cases in which the benefits outweigh the risks.”
As part of the proposal, CMS would cover autologous treatment with T cells expressing at least one chimeric antigen receptor (CAR) through coverage with evidence development when prescribed by a treating oncologist and performed in a hospital, according to a summary of the proposal.
The patient and hospital must meet specific criteria to be eligible for coverage, including that patients have relapsed or refractory cancer and do not have a comorbidity that would otherwise preclude patient benefit.
Hospitals, meanwhile, must have a cellular therapy program consisting of an integrated medical team that includes a clinical program director, a quality manager, and at least one physician experienced in cellular therapy, among other requirements.
CMS also would require that treatment is an FDA-approved biologic, providing targeted therapy for a known antigen expressed in the patient’s cancer according to an FDA indication. Repeat treatment would be covered only when a new primary cancer diagnosis is made by the treating oncologist and certain patient conditions are met.
Both inpatient and outpatient settings for the CAR T-cell therapy treatment are acceptable under the proposal. In either case, the patient and the hospital must be participating in a prospective, national, audited registry that consecutively enrolls patients, accepts all manufactured products, follows the patient for at least 2 years, and addresses a set of approved evidence-development questions. Additionally, all registries must be reviewed and approved by CMS.
The proposed national coverage determination was the result of an Aug. 22, 2018 meeting of the Medicare Evidence Development & Coverage Advisory Committee. The committee provides CMS with an external assessment of the appropriateness of therapies under review.
Public comments about the CAR T-cell therapy proposal will be accepted online here until March 15. A final decision on the proposal is expected by May 2019.
The agency’s proposal follows an Aug. 17 final rule by CMS that sets a new payment scheme for inpatient administration of two CAR T-cell therapies. The rule categorizes CAR T-cell therapies under the umbrella of the renamed Medicare Severity–Diagnosis Related Groups 016 – Autologous Bone Marrow Transplant with CC/MCC or T-cell Immunotherapy – and assigns ICD-10 PCS procedure codes XW033C3 and XW043C3 to the use of axicabtagene ciloleucel (Yescarta) and tisagenlecleucel (Kymriah) in the inpatient setting for fiscal year 2019, which began in October 2018. CMS also approved a temporary New Technology Add-On Payment for use of the therapies with a maximum threshold of $186,500.
In April 2018, CMS announced payment rates for outpatient administration of the two drugs, settling on $395,380 for axicabtagene ciloleucel and $500,839 for tisagenlecleucel. The two medications have list prices of $373,000 and $475,000, respectively.
The Centers for Medicare & Medicaid Services has proposed to cover chimeric antigen receptor (CAR) T-cell therapy for cancer patients participating in clinical trials that study the treatment’s effectiveness, according to a Feb. 15 announcement.
The proposed national coverage determination would require CMS to cover CAR T-cell therapies nationwide when the treatment is offered in CMS-approved registries or clinical studies in which patients are monitored for 2 or more years following treatment.
Results from the studies would help CMS identify which patients benefit most from CAR T-cell therapies and inform future coverage decisions, CMS Administrator Seema Verma said.
“CAR T-cell therapy was the first FDA-approved gene therapy, marking the beginning of an entirely new approach to treating serious and even life-threatening diseases,” Ms. Verma said in a statement. “Today’s proposed coverage decision would improve access to this therapy while deepening CMS’s understanding of how patients in Medicare respond to it, so the agency can ensure that it is paying for CAR T-cell therapy for cases in which the benefits outweigh the risks.”
As part of the proposal, CMS would cover autologous treatment with T cells expressing at least one chimeric antigen receptor (CAR) through coverage with evidence development when prescribed by a treating oncologist and performed in a hospital, according to a summary of the proposal.
The patient and hospital must meet specific criteria to be eligible for coverage, including that patients have relapsed or refractory cancer and do not have a comorbidity that would otherwise preclude patient benefit.
Hospitals, meanwhile, must have a cellular therapy program consisting of an integrated medical team that includes a clinical program director, a quality manager, and at least one physician experienced in cellular therapy, among other requirements.
CMS also would require that treatment is an FDA-approved biologic, providing targeted therapy for a known antigen expressed in the patient’s cancer according to an FDA indication. Repeat treatment would be covered only when a new primary cancer diagnosis is made by the treating oncologist and certain patient conditions are met.
Both inpatient and outpatient settings for the CAR T-cell therapy treatment are acceptable under the proposal. In either case, the patient and the hospital must be participating in a prospective, national, audited registry that consecutively enrolls patients, accepts all manufactured products, follows the patient for at least 2 years, and addresses a set of approved evidence-development questions. Additionally, all registries must be reviewed and approved by CMS.
The proposed national coverage determination was the result of an Aug. 22, 2018 meeting of the Medicare Evidence Development & Coverage Advisory Committee. The committee provides CMS with an external assessment of the appropriateness of therapies under review.
Public comments about the CAR T-cell therapy proposal will be accepted online here until March 15. A final decision on the proposal is expected by May 2019.
The agency’s proposal follows an Aug. 17 final rule by CMS that sets a new payment scheme for inpatient administration of two CAR T-cell therapies. The rule categorizes CAR T-cell therapies under the umbrella of the renamed Medicare Severity–Diagnosis Related Groups 016 – Autologous Bone Marrow Transplant with CC/MCC or T-cell Immunotherapy – and assigns ICD-10 PCS procedure codes XW033C3 and XW043C3 to the use of axicabtagene ciloleucel (Yescarta) and tisagenlecleucel (Kymriah) in the inpatient setting for fiscal year 2019, which began in October 2018. CMS also approved a temporary New Technology Add-On Payment for use of the therapies with a maximum threshold of $186,500.
In April 2018, CMS announced payment rates for outpatient administration of the two drugs, settling on $395,380 for axicabtagene ciloleucel and $500,839 for tisagenlecleucel. The two medications have list prices of $373,000 and $475,000, respectively.
The Centers for Medicare & Medicaid Services has proposed to cover chimeric antigen receptor (CAR) T-cell therapy for cancer patients participating in clinical trials that study the treatment’s effectiveness, according to a Feb. 15 announcement.
The proposed national coverage determination would require CMS to cover CAR T-cell therapies nationwide when the treatment is offered in CMS-approved registries or clinical studies in which patients are monitored for 2 or more years following treatment.
Results from the studies would help CMS identify which patients benefit most from CAR T-cell therapies and inform future coverage decisions, CMS Administrator Seema Verma said.
“CAR T-cell therapy was the first FDA-approved gene therapy, marking the beginning of an entirely new approach to treating serious and even life-threatening diseases,” Ms. Verma said in a statement. “Today’s proposed coverage decision would improve access to this therapy while deepening CMS’s understanding of how patients in Medicare respond to it, so the agency can ensure that it is paying for CAR T-cell therapy for cases in which the benefits outweigh the risks.”
As part of the proposal, CMS would cover autologous treatment with T cells expressing at least one chimeric antigen receptor (CAR) through coverage with evidence development when prescribed by a treating oncologist and performed in a hospital, according to a summary of the proposal.
The patient and hospital must meet specific criteria to be eligible for coverage, including that patients have relapsed or refractory cancer and do not have a comorbidity that would otherwise preclude patient benefit.
Hospitals, meanwhile, must have a cellular therapy program consisting of an integrated medical team that includes a clinical program director, a quality manager, and at least one physician experienced in cellular therapy, among other requirements.
CMS also would require that treatment is an FDA-approved biologic, providing targeted therapy for a known antigen expressed in the patient’s cancer according to an FDA indication. Repeat treatment would be covered only when a new primary cancer diagnosis is made by the treating oncologist and certain patient conditions are met.
Both inpatient and outpatient settings for the CAR T-cell therapy treatment are acceptable under the proposal. In either case, the patient and the hospital must be participating in a prospective, national, audited registry that consecutively enrolls patients, accepts all manufactured products, follows the patient for at least 2 years, and addresses a set of approved evidence-development questions. Additionally, all registries must be reviewed and approved by CMS.
The proposed national coverage determination was the result of an Aug. 22, 2018 meeting of the Medicare Evidence Development & Coverage Advisory Committee. The committee provides CMS with an external assessment of the appropriateness of therapies under review.
Public comments about the CAR T-cell therapy proposal will be accepted online here until March 15. A final decision on the proposal is expected by May 2019.
The agency’s proposal follows an Aug. 17 final rule by CMS that sets a new payment scheme for inpatient administration of two CAR T-cell therapies. The rule categorizes CAR T-cell therapies under the umbrella of the renamed Medicare Severity–Diagnosis Related Groups 016 – Autologous Bone Marrow Transplant with CC/MCC or T-cell Immunotherapy – and assigns ICD-10 PCS procedure codes XW033C3 and XW043C3 to the use of axicabtagene ciloleucel (Yescarta) and tisagenlecleucel (Kymriah) in the inpatient setting for fiscal year 2019, which began in October 2018. CMS also approved a temporary New Technology Add-On Payment for use of the therapies with a maximum threshold of $186,500.
In April 2018, CMS announced payment rates for outpatient administration of the two drugs, settling on $395,380 for axicabtagene ciloleucel and $500,839 for tisagenlecleucel. The two medications have list prices of $373,000 and $475,000, respectively.

What I learned from Navy SEALs about resilience
In 2017, the National Academy of Medicine recognized the urgent need to address burnout, wellness, and resilience in physicians. A consortium was subsequently put together comprising many cosponsoring organizations, including the Accreditation Council for Graduate Medical Education (ACGME), and the American Board of Medical Specialties (ABMS). One of many outputs of this consortium was a discussion paper, “A Journey to Construct an All-Encompassing Conceptual Model of Factors Affecting Clinician Well-Being and Resilience.”

The authors conceptually divided wellness and resilience drivers into external and individual factors. It turns out that a large portion of clinician well-being and resilience is related to individual factors that include personal factors, skills, and abilities. Taking personal responsibility and ownership of developing these individual factors is important, but many do not know where to begin.
My journey in this area began 5 years ago. This was a time when organizational resources were sparse and there was little local or national attention to addressing physician wellness. My life was horribly out of balance. While this should have been obvious, the “hit-on-the-head” moment was weighing myself one day and realizing that I was 30 pounds overweight. This was the ultimate sign to me that there was a problem because throughout my entire life, I was always very athletic, even during residency and fellowship training. I was using food as a reward system for several years which, in combination with a dramatic decrease in physical activity due to prioritizing everything related to work, led to this problem. A slowing metabolism that we all face as we age certainly accentuated it.
I was taking care of everybody else, but not myself. Many family members, friends, and even patients told me this over the years, which I conveniently ignored. For several years, my patients were asking me, “How are you doing?” at the end of their office visits. As a surgeon with a busy cancer practice, this should have been a signal for me – my cancer patients asking me how I am doing!
I started to think more about why this was happening. I realized that I was a victim of my own passions. In terms of my clinical practice, I cherished and absolutely loved every aspect of my practice and taking care of patients. I loved educating our next generation and thrived on conducting research, presenting at meetings, and publishing papers. And as I was accumulating more administrative roles and responsibilities at the department, hospital, and medical school levels, I realized I had a growing passion for administrative work. I found that the administrative work was uniquely challenging and allowed me to meaningfully serve others in a very special way.
In all of these areas for which I had a deep passion, I was committed to nothing short of excellence in everything I did. That is what I expected of myself. Self-compassion was almost absent. In addition, I have a people-pleasing personality and find it difficult to say no to people. As I have come to realize, this characteristic can be self-destructive.
I began to recognize that I fell into an acceptance (and almost expectation) that every 6-8 months I’d experience an episode of burnout that lasted 3-4 days. My burnout trigger was feeling a sense of helplessness. Everything seemed to come down all at once, and I felt helpless to dig out of it.
I realized I wanted to change, but I had no idea what resources were available or how to go about making a change. One day, I was talking to a colleague about these issues, and he asked, “Have you read the book, ‘Lone Survivor?’ ” I hadn’t heard of it, but I picked it up and started reading. Looking back, this was one of the most important decisions I made in my effort to help myself. “Lone Survivor” tells the the story of Marcus Luttrell, a retired U.S. Navy SEAL who received the Navy Cross for his actions facing Taliban fighters during Operation Red Wings.
When I finished reading this book, I realized that this was a remarkable story of resilience. The entirety of his story really connected with me. I then began to think there might be something I could learn from the Navy SEAL community that I could apply to my own civilian life.
Candidates who enter training for Navy SEALs are physically fit to succeed, but only approximately 20% make it through Basic Underwater Demolition/SEAL (BUD/S). Many drop out on request, largely because they don’t have the mental toughness and emotional resilience to tolerate intense stress continuously over a prolonged period of time. The ones who succeed have a deep meaning to their “Why” to become a SEAL.
I then learned about a retired Navy SEAL Commander, Mark Devine, who had a program intended to train civilians in physical fitness, mental toughness, emotional resilience, intuitional awareness, and spiritual consciousness in a manner similar to that of preparing prospective candidates for BUD/S training. The website stated that the defining attribute for enrollees was “a burning desire to better oneself.” I connected with that. After resolving my self-doubts and uncomfortable feelings about doing this, I signed up for the 3-day Fundamentals immersion program.
My 3 days with Coach Divine and his team were truly transformative. This was definitely not a “Navy SEAL Fantasy Camp,” and perhaps were the 3 most difficult days of my life in many regards.
When I got back from this program, I had a framework and toolbox for developing resilience to avoid burnout and improve my personal wellness. I immediately changed several things in my life, in an enduring way for the past 5 years. I started to train regularly. While I could not find a predictable time to do this during the week, I prioritized training during weekends. I improved my nutrition, stopped using food as a reward system, and started getting more sleep. Within 6 months after completing the program, I dropped the 30 pounds by being disciplined, not motivated, to make these changes. I also developed a morning ritual upon awakening. This consists of drinking a glass of water, doing box-breathing exercises, positive self-talk, thinking through my day, prioritizing what needs to be done, doing an ethos check-in to make sure that the priorities of the day correlate with my “Why,” engaging in further positive self-talk, and then engaging in positive visualization. I think this mindfulness activity has been critically important.
With the enduring changes I made, my regular schedule of burnout episodes every 6-8 months stopped, despite some very stressful events in my life. Go figure. My productivity was not affected, and my happiness was certainly improved. I had a definite sense that the changes I made were real and effective. One day a few years later while rounding with an intern, one of my patients said to the resident, “I remember Dr. Nussenbaum when he was fat.” The intern looked at me with a puzzled expression.
Based on my own journey, what advice can I give you to improve your own personal wellness and resilience? Most importantly, know your “Why” and your “3 Ps” (passion, purpose, and principles in life). What’s your personal ethos? Make sure that the job you do and the activities you perform tie into your ethos as much and as often as possible. Engage in mindfulness activities. There are many possibilities. For me, the mindfulness activity is my morning ritual. Talking about failures with trusted friends and colleagues rather than hiding them can also increase your resilience.
Developing and maintaining resilience is still an evolving and ongoing process for me. I consider this a lifelong learning process, rather than a one-time deal. Most difficult has been becoming disciplined and patient to learn new things and incorporate them into my life, and along the way becoming comfortable with being uncomfortable. And taking the necessary time to define a personal ethos, which took much longer than I thought it would.
I’ve continued to learn from several resources available from the Harvard Business Review, and from reading several widely available books. I have taken an academic approach to supplement what I learned from Coach Divine and his team, which is not surprising to those that know me well. Societies also now have many resources, such as The American Medical Association’s Burnout Tip-of-the Week, as one example.
One of the four guiding principles from the recent article, “Charter on Physician Well-Being,” states that physician well-being is a shared responsibility. It’s shared among the organizations we work in, society and its regulatory agencies, and individuals. It’s important to remind ourselves that taking individual responsibility for your wellness and developing resilience will still be a key component even as resources from our organizations and society continue to expand and become more available. Improving physician well-being needs to be a team sport.
Dr. Brian Nussenbaum is executive director of the American Board of Otolaryngology–Head and Neck Surgery. He lives in Houston. These remarks were adapted from a presentation that Dr. Nussenbaum gave at the Triological Society’s Combined Sections Meeting in Coronado, Calif., which was jointly sponsored by the Triological Society and the American College of Surgeons.
In 2017, the National Academy of Medicine recognized the urgent need to address burnout, wellness, and resilience in physicians. A consortium was subsequently put together comprising many cosponsoring organizations, including the Accreditation Council for Graduate Medical Education (ACGME), and the American Board of Medical Specialties (ABMS). One of many outputs of this consortium was a discussion paper, “A Journey to Construct an All-Encompassing Conceptual Model of Factors Affecting Clinician Well-Being and Resilience.”
The authors conceptually divided wellness and resilience drivers into external and individual factors. It turns out that a large portion of clinician well-being and resilience is related to individual factors that include personal factors, skills, and abilities. Taking personal responsibility and ownership of developing these individual factors is important, but many do not know where to begin.
My journey in this area began 5 years ago. This was a time when organizational resources were sparse and there was little local or national attention to addressing physician wellness. My life was horribly out of balance. While this should have been obvious, the “hit-on-the-head” moment was weighing myself one day and realizing that I was 30 pounds overweight. This was the ultimate sign to me that there was a problem because throughout my entire life, I was always very athletic, even during residency and fellowship training. I was using food as a reward system for several years which, in combination with a dramatic decrease in physical activity due to prioritizing everything related to work, led to this problem. A slowing metabolism that we all face as we age certainly accentuated it.
I was taking care of everybody else, but not myself. Many family members, friends, and even patients told me this over the years, which I conveniently ignored. For several years, my patients were asking me, “How are you doing?” at the end of their office visits. As a surgeon with a busy cancer practice, this should have been a signal for me – my cancer patients asking me how I am doing!
I started to think more about why this was happening. I realized that I was a victim of my own passions. In terms of my clinical practice, I cherished and absolutely loved every aspect of my practice and taking care of patients. I loved educating our next generation and thrived on conducting research, presenting at meetings, and publishing papers. And as I was accumulating more administrative roles and responsibilities at the department, hospital, and medical school levels, I realized I had a growing passion for administrative work. I found that the administrative work was uniquely challenging and allowed me to meaningfully serve others in a very special way.
In all of these areas for which I had a deep passion, I was committed to nothing short of excellence in everything I did. That is what I expected of myself. Self-compassion was almost absent. In addition, I have a people-pleasing personality and find it difficult to say no to people. As I have come to realize, this characteristic can be self-destructive.
I began to recognize that I fell into an acceptance (and almost expectation) that every 6-8 months I’d experience an episode of burnout that lasted 3-4 days. My burnout trigger was feeling a sense of helplessness. Everything seemed to come down all at once, and I felt helpless to dig out of it.
I realized I wanted to change, but I had no idea what resources were available or how to go about making a change. One day, I was talking to a colleague about these issues, and he asked, “Have you read the book, ‘Lone Survivor?’ ” I hadn’t heard of it, but I picked it up and started reading. Looking back, this was one of the most important decisions I made in my effort to help myself. “Lone Survivor” tells the the story of Marcus Luttrell, a retired U.S. Navy SEAL who received the Navy Cross for his actions facing Taliban fighters during Operation Red Wings.
When I finished reading this book, I realized that this was a remarkable story of resilience. The entirety of his story really connected with me. I then began to think there might be something I could learn from the Navy SEAL community that I could apply to my own civilian life.
Candidates who enter training for Navy SEALs are physically fit to succeed, but only approximately 20% make it through Basic Underwater Demolition/SEAL (BUD/S). Many drop out on request, largely because they don’t have the mental toughness and emotional resilience to tolerate intense stress continuously over a prolonged period of time. The ones who succeed have a deep meaning to their “Why” to become a SEAL.
I then learned about a retired Navy SEAL Commander, Mark Devine, who had a program intended to train civilians in physical fitness, mental toughness, emotional resilience, intuitional awareness, and spiritual consciousness in a manner similar to that of preparing prospective candidates for BUD/S training. The website stated that the defining attribute for enrollees was “a burning desire to better oneself.” I connected with that. After resolving my self-doubts and uncomfortable feelings about doing this, I signed up for the 3-day Fundamentals immersion program.
My 3 days with Coach Divine and his team were truly transformative. This was definitely not a “Navy SEAL Fantasy Camp,” and perhaps were the 3 most difficult days of my life in many regards.
When I got back from this program, I had a framework and toolbox for developing resilience to avoid burnout and improve my personal wellness. I immediately changed several things in my life, in an enduring way for the past 5 years. I started to train regularly. While I could not find a predictable time to do this during the week, I prioritized training during weekends. I improved my nutrition, stopped using food as a reward system, and started getting more sleep. Within 6 months after completing the program, I dropped the 30 pounds by being disciplined, not motivated, to make these changes. I also developed a morning ritual upon awakening. This consists of drinking a glass of water, doing box-breathing exercises, positive self-talk, thinking through my day, prioritizing what needs to be done, doing an ethos check-in to make sure that the priorities of the day correlate with my “Why,” engaging in further positive self-talk, and then engaging in positive visualization. I think this mindfulness activity has been critically important.
With the enduring changes I made, my regular schedule of burnout episodes every 6-8 months stopped, despite some very stressful events in my life. Go figure. My productivity was not affected, and my happiness was certainly improved. I had a definite sense that the changes I made were real and effective. One day a few years later while rounding with an intern, one of my patients said to the resident, “I remember Dr. Nussenbaum when he was fat.” The intern looked at me with a puzzled expression.
Based on my own journey, what advice can I give you to improve your own personal wellness and resilience? Most importantly, know your “Why” and your “3 Ps” (passion, purpose, and principles in life). What’s your personal ethos? Make sure that the job you do and the activities you perform tie into your ethos as much and as often as possible. Engage in mindfulness activities. There are many possibilities. For me, the mindfulness activity is my morning ritual. Talking about failures with trusted friends and colleagues rather than hiding them can also increase your resilience.
Developing and maintaining resilience is still an evolving and ongoing process for me. I consider this a lifelong learning process, rather than a one-time deal. Most difficult has been becoming disciplined and patient to learn new things and incorporate them into my life, and along the way becoming comfortable with being uncomfortable. And taking the necessary time to define a personal ethos, which took much longer than I thought it would.
I’ve continued to learn from several resources available from the Harvard Business Review, and from reading several widely available books. I have taken an academic approach to supplement what I learned from Coach Divine and his team, which is not surprising to those that know me well. Societies also now have many resources, such as The American Medical Association’s Burnout Tip-of-the Week, as one example.
One of the four guiding principles from the recent article, “Charter on Physician Well-Being,” states that physician well-being is a shared responsibility. It’s shared among the organizations we work in, society and its regulatory agencies, and individuals. It’s important to remind ourselves that taking individual responsibility for your wellness and developing resilience will still be a key component even as resources from our organizations and society continue to expand and become more available. Improving physician well-being needs to be a team sport.
Dr. Brian Nussenbaum is executive director of the American Board of Otolaryngology–Head and Neck Surgery. He lives in Houston. These remarks were adapted from a presentation that Dr. Nussenbaum gave at the Triological Society’s Combined Sections Meeting in Coronado, Calif., which was jointly sponsored by the Triological Society and the American College of Surgeons.
In 2017, the National Academy of Medicine recognized the urgent need to address burnout, wellness, and resilience in physicians. A consortium was subsequently put together comprising many cosponsoring organizations, including the Accreditation Council for Graduate Medical Education (ACGME), and the American Board of Medical Specialties (ABMS). One of many outputs of this consortium was a discussion paper, “A Journey to Construct an All-Encompassing Conceptual Model of Factors Affecting Clinician Well-Being and Resilience.”
The authors conceptually divided wellness and resilience drivers into external and individual factors. It turns out that a large portion of clinician well-being and resilience is related to individual factors that include personal factors, skills, and abilities. Taking personal responsibility and ownership of developing these individual factors is important, but many do not know where to begin.
My journey in this area began 5 years ago. This was a time when organizational resources were sparse and there was little local or national attention to addressing physician wellness. My life was horribly out of balance. While this should have been obvious, the “hit-on-the-head” moment was weighing myself one day and realizing that I was 30 pounds overweight. This was the ultimate sign to me that there was a problem because throughout my entire life, I was always very athletic, even during residency and fellowship training. I was using food as a reward system for several years which, in combination with a dramatic decrease in physical activity due to prioritizing everything related to work, led to this problem. A slowing metabolism that we all face as we age certainly accentuated it.
I was taking care of everybody else, but not myself. Many family members, friends, and even patients told me this over the years, which I conveniently ignored. For several years, my patients were asking me, “How are you doing?” at the end of their office visits. As a surgeon with a busy cancer practice, this should have been a signal for me – my cancer patients asking me how I am doing!
I started to think more about why this was happening. I realized that I was a victim of my own passions. In terms of my clinical practice, I cherished and absolutely loved every aspect of my practice and taking care of patients. I loved educating our next generation and thrived on conducting research, presenting at meetings, and publishing papers. And as I was accumulating more administrative roles and responsibilities at the department, hospital, and medical school levels, I realized I had a growing passion for administrative work. I found that the administrative work was uniquely challenging and allowed me to meaningfully serve others in a very special way.
In all of these areas for which I had a deep passion, I was committed to nothing short of excellence in everything I did. That is what I expected of myself. Self-compassion was almost absent. In addition, I have a people-pleasing personality and find it difficult to say no to people. As I have come to realize, this characteristic can be self-destructive.
I began to recognize that I fell into an acceptance (and almost expectation) that every 6-8 months I’d experience an episode of burnout that lasted 3-4 days. My burnout trigger was feeling a sense of helplessness. Everything seemed to come down all at once, and I felt helpless to dig out of it.
I realized I wanted to change, but I had no idea what resources were available or how to go about making a change. One day, I was talking to a colleague about these issues, and he asked, “Have you read the book, ‘Lone Survivor?’ ” I hadn’t heard of it, but I picked it up and started reading. Looking back, this was one of the most important decisions I made in my effort to help myself. “Lone Survivor” tells the the story of Marcus Luttrell, a retired U.S. Navy SEAL who received the Navy Cross for his actions facing Taliban fighters during Operation Red Wings.
When I finished reading this book, I realized that this was a remarkable story of resilience. The entirety of his story really connected with me. I then began to think there might be something I could learn from the Navy SEAL community that I could apply to my own civilian life.
Candidates who enter training for Navy SEALs are physically fit to succeed, but only approximately 20% make it through Basic Underwater Demolition/SEAL (BUD/S). Many drop out on request, largely because they don’t have the mental toughness and emotional resilience to tolerate intense stress continuously over a prolonged period of time. The ones who succeed have a deep meaning to their “Why” to become a SEAL.
I then learned about a retired Navy SEAL Commander, Mark Devine, who had a program intended to train civilians in physical fitness, mental toughness, emotional resilience, intuitional awareness, and spiritual consciousness in a manner similar to that of preparing prospective candidates for BUD/S training. The website stated that the defining attribute for enrollees was “a burning desire to better oneself.” I connected with that. After resolving my self-doubts and uncomfortable feelings about doing this, I signed up for the 3-day Fundamentals immersion program.
My 3 days with Coach Divine and his team were truly transformative. This was definitely not a “Navy SEAL Fantasy Camp,” and perhaps were the 3 most difficult days of my life in many regards.
When I got back from this program, I had a framework and toolbox for developing resilience to avoid burnout and improve my personal wellness. I immediately changed several things in my life, in an enduring way for the past 5 years. I started to train regularly. While I could not find a predictable time to do this during the week, I prioritized training during weekends. I improved my nutrition, stopped using food as a reward system, and started getting more sleep. Within 6 months after completing the program, I dropped the 30 pounds by being disciplined, not motivated, to make these changes. I also developed a morning ritual upon awakening. This consists of drinking a glass of water, doing box-breathing exercises, positive self-talk, thinking through my day, prioritizing what needs to be done, doing an ethos check-in to make sure that the priorities of the day correlate with my “Why,” engaging in further positive self-talk, and then engaging in positive visualization. I think this mindfulness activity has been critically important.
With the enduring changes I made, my regular schedule of burnout episodes every 6-8 months stopped, despite some very stressful events in my life. Go figure. My productivity was not affected, and my happiness was certainly improved. I had a definite sense that the changes I made were real and effective. One day a few years later while rounding with an intern, one of my patients said to the resident, “I remember Dr. Nussenbaum when he was fat.” The intern looked at me with a puzzled expression.
Based on my own journey, what advice can I give you to improve your own personal wellness and resilience? Most importantly, know your “Why” and your “3 Ps” (passion, purpose, and principles in life). What’s your personal ethos? Make sure that the job you do and the activities you perform tie into your ethos as much and as often as possible. Engage in mindfulness activities. There are many possibilities. For me, the mindfulness activity is my morning ritual. Talking about failures with trusted friends and colleagues rather than hiding them can also increase your resilience.
Developing and maintaining resilience is still an evolving and ongoing process for me. I consider this a lifelong learning process, rather than a one-time deal. Most difficult has been becoming disciplined and patient to learn new things and incorporate them into my life, and along the way becoming comfortable with being uncomfortable. And taking the necessary time to define a personal ethos, which took much longer than I thought it would.
I’ve continued to learn from several resources available from the Harvard Business Review, and from reading several widely available books. I have taken an academic approach to supplement what I learned from Coach Divine and his team, which is not surprising to those that know me well. Societies also now have many resources, such as The American Medical Association’s Burnout Tip-of-the Week, as one example.
One of the four guiding principles from the recent article, “Charter on Physician Well-Being,” states that physician well-being is a shared responsibility. It’s shared among the organizations we work in, society and its regulatory agencies, and individuals. It’s important to remind ourselves that taking individual responsibility for your wellness and developing resilience will still be a key component even as resources from our organizations and society continue to expand and become more available. Improving physician well-being needs to be a team sport.
Dr. Brian Nussenbaum is executive director of the American Board of Otolaryngology–Head and Neck Surgery. He lives in Houston. These remarks were adapted from a presentation that Dr. Nussenbaum gave at the Triological Society’s Combined Sections Meeting in Coronado, Calif., which was jointly sponsored by the Triological Society and the American College of Surgeons.
Obstetric patients with opioid use disorder fare well with medication-assisted treatment
LAS VEGAS – A prospective study of pregnant women with opioid use disorder showed good success with tapering or discontinuation of medication-assisted treatment (MAT) for women who wished to reduce or eliminate opioids while pregnant.
In related work, naltrexone showed promise for MAT in pregnancy, with rapid fetal clearance and no neonatal abstinence syndrome (NAS) seen in women who were adherent to naltrexone.
Presenting early experiences from an obstetric clinic dedicated to care of women with opioid use disorder (OUD), Craig Towers, MD, said that the clinic began seeing patients in November, 2016. “Eastern Tennessee has a high rate of opioid use disorder,” so the clinic at the University of Tennessee, Knoxville, fills an unmet need, he said, speaking during a poster session at the meeting sponsored by the Society for Maternal-Fetal Medicine.
Women who enroll at the clinic are offered MAT; those who are stable on MAT and adherent to prenatal care also are offered the choice to taper from MAT and detoxify, said Dr. Towers, professor in the division of maternal-fetal medicine in the department of obstetrics and gynecology at the University of Tennessee – Knoxville.
The prospective observational cohort study found that, of a total of 367 compliant patients, 286 (78%) chose opioid tapering/detoxification, and of these, 152 (53%) did detoxify fully. Of these patients, 126 (83%) were taking no opioids at delivery, and their infants experienced no NAS.
At the time of delivery, 26 patients (17%) were taking opioids at delivery; 18 were back on MAT, and 8 were using illicit opioids. A total of 116 patients chose to continue MAT, whether they stayed on the regimen or converted back to stable MAT doses after beginning to taper.
Another option offered women at the OUD-dedicated obstetric clinic is the use of the Bridge device, a percutaneous nerve field stimulator, for OUD. Dr. Tower said that, in early use in 14 patients, the Bridge was successful in helping women transition off opioids completely in 10 (71%) patients.
About the larger study, Dr. Towers said, “This is the first study to prospectively report outcome data on a designated OUD clinic that offers detoxification during pregnancy.
“With a structured program that includes behavioral health and offers the option of detoxification, fetal risks are negligible, relapse rates by delivery are low, and NAS rates are greatly decreased,” wrote Dr. Towers and colleagues in the abstract accompanying the study.
In a related poster presentation, Dr. Towers reported outcomes for a subset of pregnant women with OUD who received naltrexone as MAT. Previously, said Dr. Towers, retrospective work showed no significant harm using naltrexone, which is one of the three approved options for MAT to manage OUD, along with buprenorphine and methadone. Naltrexone has the advantage of helping reduce cravings.
Of the 108 patients, 82 (76%) remained on naltrexone until delivery; in these pregnancies, there were no cases of NAS. However, among the 26 pregnancies in which women stopped taking naltrexone before delivery, there were 6 (23%) NAS cases.
Fifty-one patients were started on naltrexone before 24 weeks’ gestation, and of those patients, no changes were seen with fetal monitoring. There were no instances of spontaneous abortion or intrauterine demise in any participants.
The investigators tracked gestational age at the point of full detoxification and gestational age at the point naltrexone was started. Additionally, fetal response to naltrexone and maternal and neonatal outcomes were recorded.
“This is the first prospective study and largest to date on the use of naltrexone in pregnancy,” Dr. Towers and his colleagues wrote in the poster accompanying the presentation. “These data demonstrate that naltrexone MAT is a viable option for managing OUD in pregnancy.”
Dr. Towers reported no conflicts of interest and no outside sources of funding.
LAS VEGAS – A prospective study of pregnant women with opioid use disorder showed good success with tapering or discontinuation of medication-assisted treatment (MAT) for women who wished to reduce or eliminate opioids while pregnant.
In related work, naltrexone showed promise for MAT in pregnancy, with rapid fetal clearance and no neonatal abstinence syndrome (NAS) seen in women who were adherent to naltrexone.
Presenting early experiences from an obstetric clinic dedicated to care of women with opioid use disorder (OUD), Craig Towers, MD, said that the clinic began seeing patients in November, 2016. “Eastern Tennessee has a high rate of opioid use disorder,” so the clinic at the University of Tennessee, Knoxville, fills an unmet need, he said, speaking during a poster session at the meeting sponsored by the Society for Maternal-Fetal Medicine.
Women who enroll at the clinic are offered MAT; those who are stable on MAT and adherent to prenatal care also are offered the choice to taper from MAT and detoxify, said Dr. Towers, professor in the division of maternal-fetal medicine in the department of obstetrics and gynecology at the University of Tennessee – Knoxville.
The prospective observational cohort study found that, of a total of 367 compliant patients, 286 (78%) chose opioid tapering/detoxification, and of these, 152 (53%) did detoxify fully. Of these patients, 126 (83%) were taking no opioids at delivery, and their infants experienced no NAS.
At the time of delivery, 26 patients (17%) were taking opioids at delivery; 18 were back on MAT, and 8 were using illicit opioids. A total of 116 patients chose to continue MAT, whether they stayed on the regimen or converted back to stable MAT doses after beginning to taper.
Another option offered women at the OUD-dedicated obstetric clinic is the use of the Bridge device, a percutaneous nerve field stimulator, for OUD. Dr. Tower said that, in early use in 14 patients, the Bridge was successful in helping women transition off opioids completely in 10 (71%) patients.
About the larger study, Dr. Towers said, “This is the first study to prospectively report outcome data on a designated OUD clinic that offers detoxification during pregnancy.
“With a structured program that includes behavioral health and offers the option of detoxification, fetal risks are negligible, relapse rates by delivery are low, and NAS rates are greatly decreased,” wrote Dr. Towers and colleagues in the abstract accompanying the study.
In a related poster presentation, Dr. Towers reported outcomes for a subset of pregnant women with OUD who received naltrexone as MAT. Previously, said Dr. Towers, retrospective work showed no significant harm using naltrexone, which is one of the three approved options for MAT to manage OUD, along with buprenorphine and methadone. Naltrexone has the advantage of helping reduce cravings.
Of the 108 patients, 82 (76%) remained on naltrexone until delivery; in these pregnancies, there were no cases of NAS. However, among the 26 pregnancies in which women stopped taking naltrexone before delivery, there were 6 (23%) NAS cases.
Fifty-one patients were started on naltrexone before 24 weeks’ gestation, and of those patients, no changes were seen with fetal monitoring. There were no instances of spontaneous abortion or intrauterine demise in any participants.
The investigators tracked gestational age at the point of full detoxification and gestational age at the point naltrexone was started. Additionally, fetal response to naltrexone and maternal and neonatal outcomes were recorded.
“This is the first prospective study and largest to date on the use of naltrexone in pregnancy,” Dr. Towers and his colleagues wrote in the poster accompanying the presentation. “These data demonstrate that naltrexone MAT is a viable option for managing OUD in pregnancy.”
Dr. Towers reported no conflicts of interest and no outside sources of funding.
LAS VEGAS – A prospective study of pregnant women with opioid use disorder showed good success with tapering or discontinuation of medication-assisted treatment (MAT) for women who wished to reduce or eliminate opioids while pregnant.
In related work, naltrexone showed promise for MAT in pregnancy, with rapid fetal clearance and no neonatal abstinence syndrome (NAS) seen in women who were adherent to naltrexone.
Presenting early experiences from an obstetric clinic dedicated to care of women with opioid use disorder (OUD), Craig Towers, MD, said that the clinic began seeing patients in November, 2016. “Eastern Tennessee has a high rate of opioid use disorder,” so the clinic at the University of Tennessee, Knoxville, fills an unmet need, he said, speaking during a poster session at the meeting sponsored by the Society for Maternal-Fetal Medicine.
Women who enroll at the clinic are offered MAT; those who are stable on MAT and adherent to prenatal care also are offered the choice to taper from MAT and detoxify, said Dr. Towers, professor in the division of maternal-fetal medicine in the department of obstetrics and gynecology at the University of Tennessee – Knoxville.
The prospective observational cohort study found that, of a total of 367 compliant patients, 286 (78%) chose opioid tapering/detoxification, and of these, 152 (53%) did detoxify fully. Of these patients, 126 (83%) were taking no opioids at delivery, and their infants experienced no NAS.
At the time of delivery, 26 patients (17%) were taking opioids at delivery; 18 were back on MAT, and 8 were using illicit opioids. A total of 116 patients chose to continue MAT, whether they stayed on the regimen or converted back to stable MAT doses after beginning to taper.
Another option offered women at the OUD-dedicated obstetric clinic is the use of the Bridge device, a percutaneous nerve field stimulator, for OUD. Dr. Tower said that, in early use in 14 patients, the Bridge was successful in helping women transition off opioids completely in 10 (71%) patients.
About the larger study, Dr. Towers said, “This is the first study to prospectively report outcome data on a designated OUD clinic that offers detoxification during pregnancy.
“With a structured program that includes behavioral health and offers the option of detoxification, fetal risks are negligible, relapse rates by delivery are low, and NAS rates are greatly decreased,” wrote Dr. Towers and colleagues in the abstract accompanying the study.
In a related poster presentation, Dr. Towers reported outcomes for a subset of pregnant women with OUD who received naltrexone as MAT. Previously, said Dr. Towers, retrospective work showed no significant harm using naltrexone, which is one of the three approved options for MAT to manage OUD, along with buprenorphine and methadone. Naltrexone has the advantage of helping reduce cravings.
Of the 108 patients, 82 (76%) remained on naltrexone until delivery; in these pregnancies, there were no cases of NAS. However, among the 26 pregnancies in which women stopped taking naltrexone before delivery, there were 6 (23%) NAS cases.
Fifty-one patients were started on naltrexone before 24 weeks’ gestation, and of those patients, no changes were seen with fetal monitoring. There were no instances of spontaneous abortion or intrauterine demise in any participants.
The investigators tracked gestational age at the point of full detoxification and gestational age at the point naltrexone was started. Additionally, fetal response to naltrexone and maternal and neonatal outcomes were recorded.
“This is the first prospective study and largest to date on the use of naltrexone in pregnancy,” Dr. Towers and his colleagues wrote in the poster accompanying the presentation. “These data demonstrate that naltrexone MAT is a viable option for managing OUD in pregnancy.”
Dr. Towers reported no conflicts of interest and no outside sources of funding.
REPORTING FROM THE PREGNANCY MEETING
Key clinical point: Over two-thirds of MAT-adherent patients chose detoxification.
Major finding:
Study details: Prospective single-center cohort study of 367 pregnant women with opioid use disorder.
Disclosures: Dr. Towers reported no outside sources of funding and no relevant conflicts of interest.
Source: Towers C. et al. SMFM 2019, Posters 141 & 142.
Postpartum depression often tricky to diagnose
LAS VEGAS – Diagnosing postpartum depression can be tricky because of the wide range of body changes that occur during the postpartum period, but vigilance is warranted with mothers who express a lack of sleep and a lack of social support.

at an annual psychopharmacology update held by the Nevada Psychiatric Association. “This gives you information about depression and insomnia. Make sure to ask about anxiety symptoms. Also ask about any thoughts of suicide or harming the infant, and support from family and friends when she’s under stress and taking care of the baby.”
According to Dr. Friedman, a perinatal and forensic psychiatrist at Case Western Reserve University, Cleveland, social risk factors for postpartum depression (PPD) include being a victim of intimate partner violence and/or abuse, negative life events, decreased social support, relationship issues, and socioeconomic status. Psychological risk factors include anxiety/depression in pregnancy, personal or family history of PPD, and substance misuse. Biological risk factors include medical illness, multiple births, and having an infant with low birth weight/prematurity.
PPD affects 10%-20% of new mothers and peaks at 12 weeks. Postpartum psychosis, meanwhile, occurs in about 1-2 of every 1,000 deliveries. Anxiety comorbidity is common.
In the neonatal intensive care unit (NICU), PPD rates might increase from 28% to 70% depending on the study. Risk factors include personal or family history, disturbed relationships, unfavorable socioeconomic factors, and stressful life events. Obstetrical risk factors might include conception by assisted reproductive technologies and having a stillbirth in the year before conception. NICU-specific risk factors include less-effective coping strategies, greater perception of maternal role disruption, and decreased perception of nursing support. “A lot of mothers [in the NICU] talk to me about being on a roller roaster every day about what’s going to happen with their baby,” Dr. Friedman said.
The most widely used measure to screen for PPD is the 10-item self-rating Edinburgh Postnatal Depression Scale . A total score of 10 or more is considered a flag for the need to follow up for possible depressive symptoms. She advises clinicians to pay particular attention to how patients respond to item No. 10 on the scale, which reads, “The thought of harming myself has occurred to me.” (Optional answers range from “Yes, quite often” to “Never.”) She also recommends administering the screen at both pediatric and obstetrical office visits, “because mothers are more likely to attend a pediatrics appointment than her own [postpartum] follow-up.”
The differential diagnosis of PPD includes the baby blues, postpartum psychosis, postpartum anxiety/PTSD, medical causes, substance use disorder, and PPD in bipolar disorder. Baby blues is not synonymous with PPD. It affects the majority (50%-80%) of new mothers and is characterized by emotional sensitivity, mood lability, and irritability. It usually occurs within 5 days and resolves by the second week post partum.
Postpartum psychosis (PPP) occurs in about 1-2 of every 1,000 deliveries, typically in the first 2 weeks after delivery. The onset occurs rapidly, and PPP is most frequently correlated with bipolar disorder over time. PPP itself is characterized by grandiose bizarre delusions, mood lability, hallucinations, confusion, and disorganized behavior. “This can occur as a new onset of mental illness as well, so getting collateral information about her behaviors is important,” she said.
Dr. Friedman explained that those events occur post partum largely because of sleep deprivation and increasing stress as the woman adjusts to a mothering role. Hormonal shifts also occur, with a drop in estrogen levels. Obstetrical complications also might factor in.
Postpartum obsessive-compulsive disorder (OCD) is commonly comorbid with PPD and is distinguished by ego-dystonic intrusive thoughts. The mother might have intense distress that she is going to harm the infant and might start to avoid holding the baby out of concern. “Common things I’ve heard from women with postpartum OCD are: ‘I’m afraid I’m going to put the baby in the microwave or in the oven instead of dinner’ or ‘I’m afraid I’m going to leave the baby in the car overnight and she’ll freeze to death,’ ” she said.
Postpartum PTSD can be triggered by a traumatic event experience in the birthing process, such as an emergency C-section. Affected mothers avoid the infant and hospital, “reexperience” the trauma, are easily startled, irritable, and disconnected. Dr. Friedman also noted that early parental PTSD symptoms predict sleep and eating problems in childhood and less sensitive/more controlling maternal behaviors.
Medical conditions that mimic PPD include anemia, thyroid disease, hypoactive delirium, infections, and alcohol/substance use disorder.
The best available data show that mothers with PPD are more withdrawn, disengaged, display more hostility, and are more likely to have disrupted attachment with their babies, Dr. Friedman said. They also are less likely to employ healthy child development practices and to breastfeed. Untreated depression might lead to psychotic symptoms, suicide, or homicide. Paternal PPD also occurs in an estimated 10% of fathers and is moderately correlated with maternal PPD.
Potential risks of PPD include impaired bonding, attachment disturbance, language development, cognitive skills, and behavior problems.
Potential risks of untreated PPD include child neglect or abuse because of active symptoms, suicide, and psychotic or maltreatment-related infanticide. “If the mother is taking about harming herself, I often ask: ‘Have you thought of what would happen to your baby if you were to take your own life?’ ” Dr. Friedman offered. Peripartum suicide risk is lower than in the general female population, but it represents about 20% of peripartum deaths. Overdose is the most common method. “However, uncommon and dramatic methods are more common in this population,” she said. “Teens and stigmatized single mothers are at greater risk.”
Dr. Friedman noted that clinicians face risk of a malpractice lawsuit if they fail to treat, abandon the patient, fail to provide informed consent, and if there are bad outcomes. The best approach is to proactively communicate with the patient, partner, pediatrics, and obstetrics. “Conduct an individual risk-benefit assessment with the individual patient’s history,” she advised. “Don’t do anything knee jerk. Consult when needed, document, and consider lactation and future pregnancy possibility in women of reproductive age.”
Nonpharmacologic therapy might be the first line of treatment for mild to moderate symptoms. Options include cognitive-behavioral therapy, interpersonal psychotherapy, family therapy, psychodynamic psychotherapy, and supportive psychotherapy. She recommends close follow-up and conducting a careful medication history. Electroconvulsive therapy remains a possibility.
If medication use is warranted, “weigh the benefits of breastfeeding with the usually low drug exposure of the infant,” Dr. Friedman advised. “We want to use the least number of medications at an effective dose to optimize treatment. Newer medications have less perinatal data. Sertraline and paroxetine are usually the preferred selective serotonin reuptake inhibitors in lactation. However, fluoxetine or citalopram might be used depending on the patient’s response history/use in pregnancy.”
Dr. Friedman reported no disclosures.
LAS VEGAS – Diagnosing postpartum depression can be tricky because of the wide range of body changes that occur during the postpartum period, but vigilance is warranted with mothers who express a lack of sleep and a lack of social support.
at an annual psychopharmacology update held by the Nevada Psychiatric Association. “This gives you information about depression and insomnia. Make sure to ask about anxiety symptoms. Also ask about any thoughts of suicide or harming the infant, and support from family and friends when she’s under stress and taking care of the baby.”
According to Dr. Friedman, a perinatal and forensic psychiatrist at Case Western Reserve University, Cleveland, social risk factors for postpartum depression (PPD) include being a victim of intimate partner violence and/or abuse, negative life events, decreased social support, relationship issues, and socioeconomic status. Psychological risk factors include anxiety/depression in pregnancy, personal or family history of PPD, and substance misuse. Biological risk factors include medical illness, multiple births, and having an infant with low birth weight/prematurity.
PPD affects 10%-20% of new mothers and peaks at 12 weeks. Postpartum psychosis, meanwhile, occurs in about 1-2 of every 1,000 deliveries. Anxiety comorbidity is common.
In the neonatal intensive care unit (NICU), PPD rates might increase from 28% to 70% depending on the study. Risk factors include personal or family history, disturbed relationships, unfavorable socioeconomic factors, and stressful life events. Obstetrical risk factors might include conception by assisted reproductive technologies and having a stillbirth in the year before conception. NICU-specific risk factors include less-effective coping strategies, greater perception of maternal role disruption, and decreased perception of nursing support. “A lot of mothers [in the NICU] talk to me about being on a roller roaster every day about what’s going to happen with their baby,” Dr. Friedman said.
The most widely used measure to screen for PPD is the 10-item self-rating Edinburgh Postnatal Depression Scale . A total score of 10 or more is considered a flag for the need to follow up for possible depressive symptoms. She advises clinicians to pay particular attention to how patients respond to item No. 10 on the scale, which reads, “The thought of harming myself has occurred to me.” (Optional answers range from “Yes, quite often” to “Never.”) She also recommends administering the screen at both pediatric and obstetrical office visits, “because mothers are more likely to attend a pediatrics appointment than her own [postpartum] follow-up.”
The differential diagnosis of PPD includes the baby blues, postpartum psychosis, postpartum anxiety/PTSD, medical causes, substance use disorder, and PPD in bipolar disorder. Baby blues is not synonymous with PPD. It affects the majority (50%-80%) of new mothers and is characterized by emotional sensitivity, mood lability, and irritability. It usually occurs within 5 days and resolves by the second week post partum.
Postpartum psychosis (PPP) occurs in about 1-2 of every 1,000 deliveries, typically in the first 2 weeks after delivery. The onset occurs rapidly, and PPP is most frequently correlated with bipolar disorder over time. PPP itself is characterized by grandiose bizarre delusions, mood lability, hallucinations, confusion, and disorganized behavior. “This can occur as a new onset of mental illness as well, so getting collateral information about her behaviors is important,” she said.
Dr. Friedman explained that those events occur post partum largely because of sleep deprivation and increasing stress as the woman adjusts to a mothering role. Hormonal shifts also occur, with a drop in estrogen levels. Obstetrical complications also might factor in.
Postpartum obsessive-compulsive disorder (OCD) is commonly comorbid with PPD and is distinguished by ego-dystonic intrusive thoughts. The mother might have intense distress that she is going to harm the infant and might start to avoid holding the baby out of concern. “Common things I’ve heard from women with postpartum OCD are: ‘I’m afraid I’m going to put the baby in the microwave or in the oven instead of dinner’ or ‘I’m afraid I’m going to leave the baby in the car overnight and she’ll freeze to death,’ ” she said.
Postpartum PTSD can be triggered by a traumatic event experience in the birthing process, such as an emergency C-section. Affected mothers avoid the infant and hospital, “reexperience” the trauma, are easily startled, irritable, and disconnected. Dr. Friedman also noted that early parental PTSD symptoms predict sleep and eating problems in childhood and less sensitive/more controlling maternal behaviors.
Medical conditions that mimic PPD include anemia, thyroid disease, hypoactive delirium, infections, and alcohol/substance use disorder.
The best available data show that mothers with PPD are more withdrawn, disengaged, display more hostility, and are more likely to have disrupted attachment with their babies, Dr. Friedman said. They also are less likely to employ healthy child development practices and to breastfeed. Untreated depression might lead to psychotic symptoms, suicide, or homicide. Paternal PPD also occurs in an estimated 10% of fathers and is moderately correlated with maternal PPD.
Potential risks of PPD include impaired bonding, attachment disturbance, language development, cognitive skills, and behavior problems.
Potential risks of untreated PPD include child neglect or abuse because of active symptoms, suicide, and psychotic or maltreatment-related infanticide. “If the mother is taking about harming herself, I often ask: ‘Have you thought of what would happen to your baby if you were to take your own life?’ ” Dr. Friedman offered. Peripartum suicide risk is lower than in the general female population, but it represents about 20% of peripartum deaths. Overdose is the most common method. “However, uncommon and dramatic methods are more common in this population,” she said. “Teens and stigmatized single mothers are at greater risk.”
Dr. Friedman noted that clinicians face risk of a malpractice lawsuit if they fail to treat, abandon the patient, fail to provide informed consent, and if there are bad outcomes. The best approach is to proactively communicate with the patient, partner, pediatrics, and obstetrics. “Conduct an individual risk-benefit assessment with the individual patient’s history,” she advised. “Don’t do anything knee jerk. Consult when needed, document, and consider lactation and future pregnancy possibility in women of reproductive age.”
Nonpharmacologic therapy might be the first line of treatment for mild to moderate symptoms. Options include cognitive-behavioral therapy, interpersonal psychotherapy, family therapy, psychodynamic psychotherapy, and supportive psychotherapy. She recommends close follow-up and conducting a careful medication history. Electroconvulsive therapy remains a possibility.
If medication use is warranted, “weigh the benefits of breastfeeding with the usually low drug exposure of the infant,” Dr. Friedman advised. “We want to use the least number of medications at an effective dose to optimize treatment. Newer medications have less perinatal data. Sertraline and paroxetine are usually the preferred selective serotonin reuptake inhibitors in lactation. However, fluoxetine or citalopram might be used depending on the patient’s response history/use in pregnancy.”
Dr. Friedman reported no disclosures.
LAS VEGAS – Diagnosing postpartum depression can be tricky because of the wide range of body changes that occur during the postpartum period, but vigilance is warranted with mothers who express a lack of sleep and a lack of social support.
at an annual psychopharmacology update held by the Nevada Psychiatric Association. “This gives you information about depression and insomnia. Make sure to ask about anxiety symptoms. Also ask about any thoughts of suicide or harming the infant, and support from family and friends when she’s under stress and taking care of the baby.”
According to Dr. Friedman, a perinatal and forensic psychiatrist at Case Western Reserve University, Cleveland, social risk factors for postpartum depression (PPD) include being a victim of intimate partner violence and/or abuse, negative life events, decreased social support, relationship issues, and socioeconomic status. Psychological risk factors include anxiety/depression in pregnancy, personal or family history of PPD, and substance misuse. Biological risk factors include medical illness, multiple births, and having an infant with low birth weight/prematurity.
PPD affects 10%-20% of new mothers and peaks at 12 weeks. Postpartum psychosis, meanwhile, occurs in about 1-2 of every 1,000 deliveries. Anxiety comorbidity is common.
In the neonatal intensive care unit (NICU), PPD rates might increase from 28% to 70% depending on the study. Risk factors include personal or family history, disturbed relationships, unfavorable socioeconomic factors, and stressful life events. Obstetrical risk factors might include conception by assisted reproductive technologies and having a stillbirth in the year before conception. NICU-specific risk factors include less-effective coping strategies, greater perception of maternal role disruption, and decreased perception of nursing support. “A lot of mothers [in the NICU] talk to me about being on a roller roaster every day about what’s going to happen with their baby,” Dr. Friedman said.
The most widely used measure to screen for PPD is the 10-item self-rating Edinburgh Postnatal Depression Scale . A total score of 10 or more is considered a flag for the need to follow up for possible depressive symptoms. She advises clinicians to pay particular attention to how patients respond to item No. 10 on the scale, which reads, “The thought of harming myself has occurred to me.” (Optional answers range from “Yes, quite often” to “Never.”) She also recommends administering the screen at both pediatric and obstetrical office visits, “because mothers are more likely to attend a pediatrics appointment than her own [postpartum] follow-up.”
The differential diagnosis of PPD includes the baby blues, postpartum psychosis, postpartum anxiety/PTSD, medical causes, substance use disorder, and PPD in bipolar disorder. Baby blues is not synonymous with PPD. It affects the majority (50%-80%) of new mothers and is characterized by emotional sensitivity, mood lability, and irritability. It usually occurs within 5 days and resolves by the second week post partum.
Postpartum psychosis (PPP) occurs in about 1-2 of every 1,000 deliveries, typically in the first 2 weeks after delivery. The onset occurs rapidly, and PPP is most frequently correlated with bipolar disorder over time. PPP itself is characterized by grandiose bizarre delusions, mood lability, hallucinations, confusion, and disorganized behavior. “This can occur as a new onset of mental illness as well, so getting collateral information about her behaviors is important,” she said.
Dr. Friedman explained that those events occur post partum largely because of sleep deprivation and increasing stress as the woman adjusts to a mothering role. Hormonal shifts also occur, with a drop in estrogen levels. Obstetrical complications also might factor in.
Postpartum obsessive-compulsive disorder (OCD) is commonly comorbid with PPD and is distinguished by ego-dystonic intrusive thoughts. The mother might have intense distress that she is going to harm the infant and might start to avoid holding the baby out of concern. “Common things I’ve heard from women with postpartum OCD are: ‘I’m afraid I’m going to put the baby in the microwave or in the oven instead of dinner’ or ‘I’m afraid I’m going to leave the baby in the car overnight and she’ll freeze to death,’ ” she said.
Postpartum PTSD can be triggered by a traumatic event experience in the birthing process, such as an emergency C-section. Affected mothers avoid the infant and hospital, “reexperience” the trauma, are easily startled, irritable, and disconnected. Dr. Friedman also noted that early parental PTSD symptoms predict sleep and eating problems in childhood and less sensitive/more controlling maternal behaviors.
Medical conditions that mimic PPD include anemia, thyroid disease, hypoactive delirium, infections, and alcohol/substance use disorder.
The best available data show that mothers with PPD are more withdrawn, disengaged, display more hostility, and are more likely to have disrupted attachment with their babies, Dr. Friedman said. They also are less likely to employ healthy child development practices and to breastfeed. Untreated depression might lead to psychotic symptoms, suicide, or homicide. Paternal PPD also occurs in an estimated 10% of fathers and is moderately correlated with maternal PPD.
Potential risks of PPD include impaired bonding, attachment disturbance, language development, cognitive skills, and behavior problems.
Potential risks of untreated PPD include child neglect or abuse because of active symptoms, suicide, and psychotic or maltreatment-related infanticide. “If the mother is taking about harming herself, I often ask: ‘Have you thought of what would happen to your baby if you were to take your own life?’ ” Dr. Friedman offered. Peripartum suicide risk is lower than in the general female population, but it represents about 20% of peripartum deaths. Overdose is the most common method. “However, uncommon and dramatic methods are more common in this population,” she said. “Teens and stigmatized single mothers are at greater risk.”
Dr. Friedman noted that clinicians face risk of a malpractice lawsuit if they fail to treat, abandon the patient, fail to provide informed consent, and if there are bad outcomes. The best approach is to proactively communicate with the patient, partner, pediatrics, and obstetrics. “Conduct an individual risk-benefit assessment with the individual patient’s history,” she advised. “Don’t do anything knee jerk. Consult when needed, document, and consider lactation and future pregnancy possibility in women of reproductive age.”
Nonpharmacologic therapy might be the first line of treatment for mild to moderate symptoms. Options include cognitive-behavioral therapy, interpersonal psychotherapy, family therapy, psychodynamic psychotherapy, and supportive psychotherapy. She recommends close follow-up and conducting a careful medication history. Electroconvulsive therapy remains a possibility.
If medication use is warranted, “weigh the benefits of breastfeeding with the usually low drug exposure of the infant,” Dr. Friedman advised. “We want to use the least number of medications at an effective dose to optimize treatment. Newer medications have less perinatal data. Sertraline and paroxetine are usually the preferred selective serotonin reuptake inhibitors in lactation. However, fluoxetine or citalopram might be used depending on the patient’s response history/use in pregnancy.”
Dr. Friedman reported no disclosures.
EXPERT ANALYSIS FROM NPA 2019
When to suspect a severe skin reaction to an AED
NEW ORLEANS – Most skin eruptions in patients taking antiepileptic drugs (AEDs) are relatively benign. With close supervision, some patients with epilepsy may continue treatment despite having a benign drug rash, according to a lecture at the annual meeting of the American Epilepsy Society.

“When do you know that you’re not dealing with that kind of eruption?” said Jeanne M. Young, MD, assistant professor of dermatology at the University of Virginia in Charlottesville.
Signs and symptoms that raise concerns about severe cutaneous reactions include swelling of the face; lesions that are fluid-filled, dusky, or painful; mucus membrane involvement; and signs of systemic involvement.
Associations with anticonvulsants
Diffuse swelling of the face is a hallmark symptom of DRESS. Fluid-filled lesions such as pustules, vesicles, and bullae indicate a condition other than a benign drug eruption. Signs of systemic involvement may include fever, marked eosinophilia, transaminitis, and evidence of lymphocyte activation. “In general, I want to see systemic involvement that can’t be explained by the patient’s other systemic diseases,” Dr. Young said.
A 2018 study found that AEDs are associated with SJS and TEN, and the labels for lamotrigine and carbamazepine include black box warnings about the risk of severe cutaneous adverse events. Carbamazepine’s warning, which was added in 2007, notes that SJS and TEN are significantly more common in patients of Asian ancestry with the human leukocyte antigen allele HLA-B*1502 and that physicians should screen at-risk patients before starting treatment.
Benign drug rashes
Morbilliform drug eruptions, sometimes called benign exanthems, are “by far the most common drug rash that we see” and typically are “the rashes that people refer to as drug rashes,” Dr. Young said. The mechanisms appear to be primarily immune complex mediated and cell mediated. “When the drug is stopped, these rashes tend to go away quite predictably in 2-3 weeks.”
For any class of drug, about 1% of people taking that medication may have this type of reaction, Dr. Young said. “We expect to see erythematous papules and plaques that oftentimes become confluent on the skin.” These reactions generally occur 7-10 days after the first exposure to the medication, and most patients do not have other symptoms, although the rash may itch. In addition, patients may have erythroderma with desquamation. “I think it’s important to point out the difference between desquamation, which is loss of the stratum corneum, and epidermal sloughing, which is what you see in something like [SJS] or TEN, where you’re actually losing the entire epidermis,” Dr. Young said. Recovering from desquamation is “sort of like recovering from a sun burn, and it’s not particularly dangerous.” Management of morbilliform drug eruptions is largely symptomatic.
Treat through, taper, or rechallenge
In the case a benign drug rash, “if you feel like you … need to keep a patient on a drug, you do have that option with close supervision,” Dr. Young said. “Communicate that with the dermatologist. Say, ‘I have really struggled getting this patient stabilized. Can we keep them on this drug?’ ”
The dermatologist may not fully realize the implications of stopping an effective AED in a patient with seizures that have been difficult to control. If the drug rash is benign, treating through may be an option. Patients often resolve the rash while continuing the medication, which may be because of desensitization, Dr. Young said. If a patient’s symptoms are too great to continue the drug, neurologists have the option of slowly tapering the drug and reinitiating with a new drug, Dr. Young said. Neurologists also may choose to rechallenge.
If a patient is on several medications, making it difficult to elucidate a causative agent, after stopping those drugs and allowing the rash to resolve, “there is little danger in restarting a medication,” she said.
Benign rash or DRESS?
“When I see a morbilliform eruption, usually what’s on my mind is, ‘Is this just a drug rash or is this DRESS?’ ” Dr. Young said. DRESS often starts with a morbilliform eruption that is indistinguishable from a benign drug eruption.
“Timing is a major difference,” she said. “If a patient develops a morbilliform drug eruption much later than I would expect, then my suspicion [for DRESS] goes up.” Patients with DRESS often have fever and systemic symptoms. Proposed DRESS diagnostic criteria can be useful, but clinical judgment still plays a key role. If a patient does not satisfy diagnostic criteria but has some signs and is taking a drug that is associated with DRESS, “it is going to make me more suspicious and maybe make me recommend stopping that drug sooner,” she said. Anticonvulsants such as carbamazepine, lamotrigine, and phenobarbital are among the drugs most commonly associated with DRESS.
Toxic erythemas
Patients may present with toxic erythemas, such as fixed drug reactions, erythema multiforme, SJS, and TEN. These drug reactions appear similar on biopsy but have different courses.
A patient with a fixed drug reaction often has a single lesion, and the lesion will occur in the same location every time the patient is exposed to the drug. Patients may develop additional lesions with subsequent exposures. These lesions typically are large, erythematous, well-demarcated plaques with central duskiness. “They can be bullous in the center, and they typically will heal with pigmentation, which is unique to this particular drug reaction,” said Dr. Young. “When it gets more concerning and most important to differentiate is when you get generalized bullous fixed drug eruption.” Generalized bullous fixed drug eruptions mimic and are difficult to clinically distinguish from TEN, which has a much has a much poorer prognosis.
Patients with a fixed drug eruption are not as ill as patients with TEN and tend not to slough their skin to the extent seen with TEN. Interferon gamma, perforin, and Fas ligand have been implicated as mechanisms involved in fixed drug reactions. Unlike in TEN, regulatory T cells are abundant, which may explain why TEN and fixed drug reactions progress differently even though they appear to share pathologic mechanisms, Dr. Young said.
Erythema multiforme generally presents with classic target lesions and little mucosal involvement. Infections, most commonly herpes simplex virus (HSV) 1 and 2, may trigger erythema multiforme. Dr. Young recommends evaluating patients for HSV and checking serologies, even if patients have never had a herpes outbreak. “If you have no evidence for infection, you do have to consider discontinuing a medication,” she said.
Stevens–Johnson syndrome and TEN
SJS and TEN are “the rarest of the severe cutaneous adverse drug reactions” and have “the highest morbidity and mortality,” Dr. Young said. They appear to exist on a continuum where SJS may represent early TEN.
“This is a situation where you expect to see blistering of the skin [and] always mucosal involvement. You need to stop the drug immediately when you suspect this drug reaction,” Dr. Young said.
One reason to distinguish SJS or early TEN from later TEN is that high-dose steroids may play a role in the treatment of SJS or early TEN. “Once you get past about 10% total body surface area, there is good evidence that steroids actually increase morbidity and mortality,” she said.
If the eruption has occurred before, that factor suggests that a diagnosis of erythema multiforme or fixed drug reaction may be more likely than TEN.
An apparent lack of regulatory T cells in TEN could explain why patients with HIV infection are at much higher risk of developing SJS and TEN. Understanding the role that regulatory T cells play in severe drug eruptions may lead to new therapeutic options in the future, Dr. Young said.
Dr. Young had no disclosures.
NEW ORLEANS – Most skin eruptions in patients taking antiepileptic drugs (AEDs) are relatively benign. With close supervision, some patients with epilepsy may continue treatment despite having a benign drug rash, according to a lecture at the annual meeting of the American Epilepsy Society.
“When do you know that you’re not dealing with that kind of eruption?” said Jeanne M. Young, MD, assistant professor of dermatology at the University of Virginia in Charlottesville.
Signs and symptoms that raise concerns about severe cutaneous reactions include swelling of the face; lesions that are fluid-filled, dusky, or painful; mucus membrane involvement; and signs of systemic involvement.
Associations with anticonvulsants
Diffuse swelling of the face is a hallmark symptom of DRESS. Fluid-filled lesions such as pustules, vesicles, and bullae indicate a condition other than a benign drug eruption. Signs of systemic involvement may include fever, marked eosinophilia, transaminitis, and evidence of lymphocyte activation. “In general, I want to see systemic involvement that can’t be explained by the patient’s other systemic diseases,” Dr. Young said.
A 2018 study found that AEDs are associated with SJS and TEN, and the labels for lamotrigine and carbamazepine include black box warnings about the risk of severe cutaneous adverse events. Carbamazepine’s warning, which was added in 2007, notes that SJS and TEN are significantly more common in patients of Asian ancestry with the human leukocyte antigen allele HLA-B*1502 and that physicians should screen at-risk patients before starting treatment.
Benign drug rashes
Morbilliform drug eruptions, sometimes called benign exanthems, are “by far the most common drug rash that we see” and typically are “the rashes that people refer to as drug rashes,” Dr. Young said. The mechanisms appear to be primarily immune complex mediated and cell mediated. “When the drug is stopped, these rashes tend to go away quite predictably in 2-3 weeks.”
For any class of drug, about 1% of people taking that medication may have this type of reaction, Dr. Young said. “We expect to see erythematous papules and plaques that oftentimes become confluent on the skin.” These reactions generally occur 7-10 days after the first exposure to the medication, and most patients do not have other symptoms, although the rash may itch. In addition, patients may have erythroderma with desquamation. “I think it’s important to point out the difference between desquamation, which is loss of the stratum corneum, and epidermal sloughing, which is what you see in something like [SJS] or TEN, where you’re actually losing the entire epidermis,” Dr. Young said. Recovering from desquamation is “sort of like recovering from a sun burn, and it’s not particularly dangerous.” Management of morbilliform drug eruptions is largely symptomatic.
Treat through, taper, or rechallenge
In the case a benign drug rash, “if you feel like you … need to keep a patient on a drug, you do have that option with close supervision,” Dr. Young said. “Communicate that with the dermatologist. Say, ‘I have really struggled getting this patient stabilized. Can we keep them on this drug?’ ”
The dermatologist may not fully realize the implications of stopping an effective AED in a patient with seizures that have been difficult to control. If the drug rash is benign, treating through may be an option. Patients often resolve the rash while continuing the medication, which may be because of desensitization, Dr. Young said. If a patient’s symptoms are too great to continue the drug, neurologists have the option of slowly tapering the drug and reinitiating with a new drug, Dr. Young said. Neurologists also may choose to rechallenge.
If a patient is on several medications, making it difficult to elucidate a causative agent, after stopping those drugs and allowing the rash to resolve, “there is little danger in restarting a medication,” she said.
Benign rash or DRESS?
“When I see a morbilliform eruption, usually what’s on my mind is, ‘Is this just a drug rash or is this DRESS?’ ” Dr. Young said. DRESS often starts with a morbilliform eruption that is indistinguishable from a benign drug eruption.
“Timing is a major difference,” she said. “If a patient develops a morbilliform drug eruption much later than I would expect, then my suspicion [for DRESS] goes up.” Patients with DRESS often have fever and systemic symptoms. Proposed DRESS diagnostic criteria can be useful, but clinical judgment still plays a key role. If a patient does not satisfy diagnostic criteria but has some signs and is taking a drug that is associated with DRESS, “it is going to make me more suspicious and maybe make me recommend stopping that drug sooner,” she said. Anticonvulsants such as carbamazepine, lamotrigine, and phenobarbital are among the drugs most commonly associated with DRESS.
Toxic erythemas
Patients may present with toxic erythemas, such as fixed drug reactions, erythema multiforme, SJS, and TEN. These drug reactions appear similar on biopsy but have different courses.
A patient with a fixed drug reaction often has a single lesion, and the lesion will occur in the same location every time the patient is exposed to the drug. Patients may develop additional lesions with subsequent exposures. These lesions typically are large, erythematous, well-demarcated plaques with central duskiness. “They can be bullous in the center, and they typically will heal with pigmentation, which is unique to this particular drug reaction,” said Dr. Young. “When it gets more concerning and most important to differentiate is when you get generalized bullous fixed drug eruption.” Generalized bullous fixed drug eruptions mimic and are difficult to clinically distinguish from TEN, which has a much has a much poorer prognosis.
Patients with a fixed drug eruption are not as ill as patients with TEN and tend not to slough their skin to the extent seen with TEN. Interferon gamma, perforin, and Fas ligand have been implicated as mechanisms involved in fixed drug reactions. Unlike in TEN, regulatory T cells are abundant, which may explain why TEN and fixed drug reactions progress differently even though they appear to share pathologic mechanisms, Dr. Young said.
Erythema multiforme generally presents with classic target lesions and little mucosal involvement. Infections, most commonly herpes simplex virus (HSV) 1 and 2, may trigger erythema multiforme. Dr. Young recommends evaluating patients for HSV and checking serologies, even if patients have never had a herpes outbreak. “If you have no evidence for infection, you do have to consider discontinuing a medication,” she said.
Stevens–Johnson syndrome and TEN
SJS and TEN are “the rarest of the severe cutaneous adverse drug reactions” and have “the highest morbidity and mortality,” Dr. Young said. They appear to exist on a continuum where SJS may represent early TEN.
“This is a situation where you expect to see blistering of the skin [and] always mucosal involvement. You need to stop the drug immediately when you suspect this drug reaction,” Dr. Young said.
One reason to distinguish SJS or early TEN from later TEN is that high-dose steroids may play a role in the treatment of SJS or early TEN. “Once you get past about 10% total body surface area, there is good evidence that steroids actually increase morbidity and mortality,” she said.
If the eruption has occurred before, that factor suggests that a diagnosis of erythema multiforme or fixed drug reaction may be more likely than TEN.
An apparent lack of regulatory T cells in TEN could explain why patients with HIV infection are at much higher risk of developing SJS and TEN. Understanding the role that regulatory T cells play in severe drug eruptions may lead to new therapeutic options in the future, Dr. Young said.
Dr. Young had no disclosures.
NEW ORLEANS – Most skin eruptions in patients taking antiepileptic drugs (AEDs) are relatively benign. With close supervision, some patients with epilepsy may continue treatment despite having a benign drug rash, according to a lecture at the annual meeting of the American Epilepsy Society.
“When do you know that you’re not dealing with that kind of eruption?” said Jeanne M. Young, MD, assistant professor of dermatology at the University of Virginia in Charlottesville.
Signs and symptoms that raise concerns about severe cutaneous reactions include swelling of the face; lesions that are fluid-filled, dusky, or painful; mucus membrane involvement; and signs of systemic involvement.
Associations with anticonvulsants
Diffuse swelling of the face is a hallmark symptom of DRESS. Fluid-filled lesions such as pustules, vesicles, and bullae indicate a condition other than a benign drug eruption. Signs of systemic involvement may include fever, marked eosinophilia, transaminitis, and evidence of lymphocyte activation. “In general, I want to see systemic involvement that can’t be explained by the patient’s other systemic diseases,” Dr. Young said.
A 2018 study found that AEDs are associated with SJS and TEN, and the labels for lamotrigine and carbamazepine include black box warnings about the risk of severe cutaneous adverse events. Carbamazepine’s warning, which was added in 2007, notes that SJS and TEN are significantly more common in patients of Asian ancestry with the human leukocyte antigen allele HLA-B*1502 and that physicians should screen at-risk patients before starting treatment.
Benign drug rashes
Morbilliform drug eruptions, sometimes called benign exanthems, are “by far the most common drug rash that we see” and typically are “the rashes that people refer to as drug rashes,” Dr. Young said. The mechanisms appear to be primarily immune complex mediated and cell mediated. “When the drug is stopped, these rashes tend to go away quite predictably in 2-3 weeks.”
For any class of drug, about 1% of people taking that medication may have this type of reaction, Dr. Young said. “We expect to see erythematous papules and plaques that oftentimes become confluent on the skin.” These reactions generally occur 7-10 days after the first exposure to the medication, and most patients do not have other symptoms, although the rash may itch. In addition, patients may have erythroderma with desquamation. “I think it’s important to point out the difference between desquamation, which is loss of the stratum corneum, and epidermal sloughing, which is what you see in something like [SJS] or TEN, where you’re actually losing the entire epidermis,” Dr. Young said. Recovering from desquamation is “sort of like recovering from a sun burn, and it’s not particularly dangerous.” Management of morbilliform drug eruptions is largely symptomatic.
Treat through, taper, or rechallenge
In the case a benign drug rash, “if you feel like you … need to keep a patient on a drug, you do have that option with close supervision,” Dr. Young said. “Communicate that with the dermatologist. Say, ‘I have really struggled getting this patient stabilized. Can we keep them on this drug?’ ”
The dermatologist may not fully realize the implications of stopping an effective AED in a patient with seizures that have been difficult to control. If the drug rash is benign, treating through may be an option. Patients often resolve the rash while continuing the medication, which may be because of desensitization, Dr. Young said. If a patient’s symptoms are too great to continue the drug, neurologists have the option of slowly tapering the drug and reinitiating with a new drug, Dr. Young said. Neurologists also may choose to rechallenge.
If a patient is on several medications, making it difficult to elucidate a causative agent, after stopping those drugs and allowing the rash to resolve, “there is little danger in restarting a medication,” she said.
Benign rash or DRESS?
“When I see a morbilliform eruption, usually what’s on my mind is, ‘Is this just a drug rash or is this DRESS?’ ” Dr. Young said. DRESS often starts with a morbilliform eruption that is indistinguishable from a benign drug eruption.
“Timing is a major difference,” she said. “If a patient develops a morbilliform drug eruption much later than I would expect, then my suspicion [for DRESS] goes up.” Patients with DRESS often have fever and systemic symptoms. Proposed DRESS diagnostic criteria can be useful, but clinical judgment still plays a key role. If a patient does not satisfy diagnostic criteria but has some signs and is taking a drug that is associated with DRESS, “it is going to make me more suspicious and maybe make me recommend stopping that drug sooner,” she said. Anticonvulsants such as carbamazepine, lamotrigine, and phenobarbital are among the drugs most commonly associated with DRESS.
Toxic erythemas
Patients may present with toxic erythemas, such as fixed drug reactions, erythema multiforme, SJS, and TEN. These drug reactions appear similar on biopsy but have different courses.
A patient with a fixed drug reaction often has a single lesion, and the lesion will occur in the same location every time the patient is exposed to the drug. Patients may develop additional lesions with subsequent exposures. These lesions typically are large, erythematous, well-demarcated plaques with central duskiness. “They can be bullous in the center, and they typically will heal with pigmentation, which is unique to this particular drug reaction,” said Dr. Young. “When it gets more concerning and most important to differentiate is when you get generalized bullous fixed drug eruption.” Generalized bullous fixed drug eruptions mimic and are difficult to clinically distinguish from TEN, which has a much has a much poorer prognosis.
Patients with a fixed drug eruption are not as ill as patients with TEN and tend not to slough their skin to the extent seen with TEN. Interferon gamma, perforin, and Fas ligand have been implicated as mechanisms involved in fixed drug reactions. Unlike in TEN, regulatory T cells are abundant, which may explain why TEN and fixed drug reactions progress differently even though they appear to share pathologic mechanisms, Dr. Young said.
Erythema multiforme generally presents with classic target lesions and little mucosal involvement. Infections, most commonly herpes simplex virus (HSV) 1 and 2, may trigger erythema multiforme. Dr. Young recommends evaluating patients for HSV and checking serologies, even if patients have never had a herpes outbreak. “If you have no evidence for infection, you do have to consider discontinuing a medication,” she said.
Stevens–Johnson syndrome and TEN
SJS and TEN are “the rarest of the severe cutaneous adverse drug reactions” and have “the highest morbidity and mortality,” Dr. Young said. They appear to exist on a continuum where SJS may represent early TEN.
“This is a situation where you expect to see blistering of the skin [and] always mucosal involvement. You need to stop the drug immediately when you suspect this drug reaction,” Dr. Young said.
One reason to distinguish SJS or early TEN from later TEN is that high-dose steroids may play a role in the treatment of SJS or early TEN. “Once you get past about 10% total body surface area, there is good evidence that steroids actually increase morbidity and mortality,” she said.
If the eruption has occurred before, that factor suggests that a diagnosis of erythema multiforme or fixed drug reaction may be more likely than TEN.
An apparent lack of regulatory T cells in TEN could explain why patients with HIV infection are at much higher risk of developing SJS and TEN. Understanding the role that regulatory T cells play in severe drug eruptions may lead to new therapeutic options in the future, Dr. Young said.
Dr. Young had no disclosures.
EXPERT ANALYSIS FROM AES 2018
Study Design, Population, and Key Outcomes of DECLARE-TIMI 58 Compared With Other Cardiovascular Outcomes Trials for Sodium-Glucose Cotransporter-2 Inhibitors
Click here to read the supplement

- The cardiovascular (CV) safety and efficacy of the sodium-glucose cotransporter-2 inhibitor (SGLT-2i) dapagliflozin was evaluated in the DECLARE-TIMI 58 study.
- The study design and patient population of DECLARE-TIMI 58 differed from those of other CV outcomes trials of SGLT-2is (EMPA-REG OUTCOME and CANVAS)
- Key outcome results between the 3 CV outcomes trials of SGLT-2is may have been affected by variations in the study designs and patient populations, given that DECLARE-TIMI 58 evaluated a larger population of patients with type 2 diabetes (T2D) without prior CV events than the EMPA-REG OUTCOME or CANVAS studies, potentially allowing for a broader generalizability of the study results to patients with T2D in real-world clinical practice.
Click here to read the supplement
About the Author:
Bulent S. Atac, MD
Albert Einstein College of
Medicine and Montefiore Medical Center,
Bronx, New York
Click here to read the supplement
- The cardiovascular (CV) safety and efficacy of the sodium-glucose cotransporter-2 inhibitor (SGLT-2i) dapagliflozin was evaluated in the DECLARE-TIMI 58 study.
- The study design and patient population of DECLARE-TIMI 58 differed from those of other CV outcomes trials of SGLT-2is (EMPA-REG OUTCOME and CANVAS)
- Key outcome results between the 3 CV outcomes trials of SGLT-2is may have been affected by variations in the study designs and patient populations, given that DECLARE-TIMI 58 evaluated a larger population of patients with type 2 diabetes (T2D) without prior CV events than the EMPA-REG OUTCOME or CANVAS studies, potentially allowing for a broader generalizability of the study results to patients with T2D in real-world clinical practice.
Click here to read the supplement
About the Author:
Bulent S. Atac, MD
Albert Einstein College of
Medicine and Montefiore Medical Center,
Bronx, New York
Click here to read the supplement
- The cardiovascular (CV) safety and efficacy of the sodium-glucose cotransporter-2 inhibitor (SGLT-2i) dapagliflozin was evaluated in the DECLARE-TIMI 58 study.
- The study design and patient population of DECLARE-TIMI 58 differed from those of other CV outcomes trials of SGLT-2is (EMPA-REG OUTCOME and CANVAS)
- Key outcome results between the 3 CV outcomes trials of SGLT-2is may have been affected by variations in the study designs and patient populations, given that DECLARE-TIMI 58 evaluated a larger population of patients with type 2 diabetes (T2D) without prior CV events than the EMPA-REG OUTCOME or CANVAS studies, potentially allowing for a broader generalizability of the study results to patients with T2D in real-world clinical practice.
Click here to read the supplement
About the Author:
Bulent S. Atac, MD
Albert Einstein College of
Medicine and Montefiore Medical Center,
Bronx, New York

The amazing work we get to do
Serving people, connecting, and improving care
Stories are told of the first meeting, 20 years ago, where a hat was passed to collect donations to develop a fledgling organization of inpatient physicians. Today, 90% of hospitals with 200+ beds operate with a hospitalist model. Today, we are the Society of Hospital Medicine.

In the early 1900s, health care in many ways was simple. It was a doctor with a shingle hung. It was house calls. Remedies were limited. In the 1940s, companies developed insurance benefits to lure workers during World War II; this third party, the payer, added complexity. Meanwhile, treatment options began to diversify. Then, in the 1960s, Medicare was passed, and the government came into the mix, further increasing this complexity. Diagnostic and treatment options continued to diversify, seemingly exponentially. Some would say it took 30 years for our country to recognize that it had created the most advanced and expensive, as well as one of the least quality-controlled, health systems in the world. Thus, as hospital medicine was conceived in the 1990s, our national health system was awakening to the need – the creative niche – that hospitalists would fill.
When I began my career, I was unaware that I was a hospitalist. The title didn’t exist. Yes, I was working solely in the hospital. I was developing programs to improve care delivery. I was rounding, teaching, collaborating, connecting – everything that we now call hospital medicine. That first job has evolved into my career, one that I find both honorable and enjoyable.
As health care changes with the passing years, being a hospitalist continues to be about serving people, connecting, and improving care. Being a hospitalist is being innovative, willing, and even daring. Dare to try, dare to fail, dare to redesign and try again. Hospital medicine is thinking outside of the box while knowing how to color between the lines. In the coming decades, health care will continue to evolve, and hospital medicine will too. We now encompass surgical comanagement and perioperative care, palliative care, postacute care, and transitions of care services. In corners, hospital medicine is already experimenting with telecare, virtual health, and hospital at home. Our hospital medicine workforce is innovative, diverse, tech savvy and poised for leading.
We are ready and willing to face the pressures affecting health care in the United States today: the recognition of an overwhelming expense to society, the relative underperformance with regard to quality, the increasing complexity of illness and treatment options, the worsening health of the average American citizen, the aging population, the role of medical error in patient harm, the increasing engagement of people in their own care, and the desire to make care better. What our country is facing is actually a phenomenal opportunity, no matter what side of the political aisle you live on. Being in hospital medicine today is being at the center front of this evolutionary stage.
Since joining the SHM board of directors, I continue to find examples of the stellar work of our staff and our members across the country. Having the privilege as a board member to join several Chapter meetings, I have witnessed firsthand the camaraderie, the compassion, the team that makes our Society work. From Houston to San Francisco and from St. Louis to Seattle, I have been honored to work with SHM members that create and nurture local and regional networks with the support of SHM’s Chapters program – a program that now houses more than 50 chapters and has launched regional districts to further support networking and growth. SHM’s chapter venues allow our larger hospital medicine team – yes, the national one – to connect and collaborate.
Take the Pacific Northwest Chapter. In its early years hospitalists from various and competing health systems would convene at a restaurant and just talk. They spoke of how to staff, how to pay, and how to negotiate with hospital leadership. As I have joined chapter meetings in recent years, meetings continue to be the place to share ideas – how to develop new programs; what is the most recent approach to glycemic control, sepsis care, or antibiotic stewardship; how best to approach diagnosis without “anchoring”; and even how to care for each other in the time of loss of a colleague to suicide. It is here in our community that we share experiences, knowledge, new ideas – and this sharing makes us all stronger.
Our hospital medicine community also comes together through areas of shared interest. There are 18 Special Interest Groups (SIGs), focused on specific topic areas. I have been privileged as a board member to work with our Perioperative/Comanagement SIG as it launched in 2017 and has grown rapidly. Currently, the community hosts a “case of the month” hospital medicine discussion as well as a regular journal club webinar that allows participants to review recent literature and interact directly with the authors. As this SIG has grown, shared resources and ideas have allowed for diffusion of knowledge, providing our nation with infrastructure for improving perioperative care. It is networks like this that support our national hospital medicine team to build strength through sharing.
It is our society, our people, that have taken us from the passing of a hat to developing our national community and network. This March, we get to celebrate our field in a new way – Thursday, March 7, 2019, marks the inaugural National Hospitalist Day. Then, March 24-27, our annual conference, Hospital Medicine 2019, will bring thousands of our national team to National Harbor, Maryland. Join your colleagues. Find your niche and your community. Be a part of the change you want to see. While you are there, come introduce yourself to me and let me thank you for the amazing work you are doing.
We are all a part of this movement transforming patient care both on a local and national level. As we move to the future, our innovative, diverse, and connected network of hospital medicine will continue to create and guide health care advances in our country.
Dr. Thompson is professor and chief of the section of hospital medicine at University of Nebraska Medical Center, and medical director of clinical care transitions at Nebraska Medicine, Omaha.
Serving people, connecting, and improving care
Serving people, connecting, and improving care
Stories are told of the first meeting, 20 years ago, where a hat was passed to collect donations to develop a fledgling organization of inpatient physicians. Today, 90% of hospitals with 200+ beds operate with a hospitalist model. Today, we are the Society of Hospital Medicine.
In the early 1900s, health care in many ways was simple. It was a doctor with a shingle hung. It was house calls. Remedies were limited. In the 1940s, companies developed insurance benefits to lure workers during World War II; this third party, the payer, added complexity. Meanwhile, treatment options began to diversify. Then, in the 1960s, Medicare was passed, and the government came into the mix, further increasing this complexity. Diagnostic and treatment options continued to diversify, seemingly exponentially. Some would say it took 30 years for our country to recognize that it had created the most advanced and expensive, as well as one of the least quality-controlled, health systems in the world. Thus, as hospital medicine was conceived in the 1990s, our national health system was awakening to the need – the creative niche – that hospitalists would fill.
When I began my career, I was unaware that I was a hospitalist. The title didn’t exist. Yes, I was working solely in the hospital. I was developing programs to improve care delivery. I was rounding, teaching, collaborating, connecting – everything that we now call hospital medicine. That first job has evolved into my career, one that I find both honorable and enjoyable.
As health care changes with the passing years, being a hospitalist continues to be about serving people, connecting, and improving care. Being a hospitalist is being innovative, willing, and even daring. Dare to try, dare to fail, dare to redesign and try again. Hospital medicine is thinking outside of the box while knowing how to color between the lines. In the coming decades, health care will continue to evolve, and hospital medicine will too. We now encompass surgical comanagement and perioperative care, palliative care, postacute care, and transitions of care services. In corners, hospital medicine is already experimenting with telecare, virtual health, and hospital at home. Our hospital medicine workforce is innovative, diverse, tech savvy and poised for leading.
We are ready and willing to face the pressures affecting health care in the United States today: the recognition of an overwhelming expense to society, the relative underperformance with regard to quality, the increasing complexity of illness and treatment options, the worsening health of the average American citizen, the aging population, the role of medical error in patient harm, the increasing engagement of people in their own care, and the desire to make care better. What our country is facing is actually a phenomenal opportunity, no matter what side of the political aisle you live on. Being in hospital medicine today is being at the center front of this evolutionary stage.
Since joining the SHM board of directors, I continue to find examples of the stellar work of our staff and our members across the country. Having the privilege as a board member to join several Chapter meetings, I have witnessed firsthand the camaraderie, the compassion, the team that makes our Society work. From Houston to San Francisco and from St. Louis to Seattle, I have been honored to work with SHM members that create and nurture local and regional networks with the support of SHM’s Chapters program – a program that now houses more than 50 chapters and has launched regional districts to further support networking and growth. SHM’s chapter venues allow our larger hospital medicine team – yes, the national one – to connect and collaborate.
Take the Pacific Northwest Chapter. In its early years hospitalists from various and competing health systems would convene at a restaurant and just talk. They spoke of how to staff, how to pay, and how to negotiate with hospital leadership. As I have joined chapter meetings in recent years, meetings continue to be the place to share ideas – how to develop new programs; what is the most recent approach to glycemic control, sepsis care, or antibiotic stewardship; how best to approach diagnosis without “anchoring”; and even how to care for each other in the time of loss of a colleague to suicide. It is here in our community that we share experiences, knowledge, new ideas – and this sharing makes us all stronger.
Our hospital medicine community also comes together through areas of shared interest. There are 18 Special Interest Groups (SIGs), focused on specific topic areas. I have been privileged as a board member to work with our Perioperative/Comanagement SIG as it launched in 2017 and has grown rapidly. Currently, the community hosts a “case of the month” hospital medicine discussion as well as a regular journal club webinar that allows participants to review recent literature and interact directly with the authors. As this SIG has grown, shared resources and ideas have allowed for diffusion of knowledge, providing our nation with infrastructure for improving perioperative care. It is networks like this that support our national hospital medicine team to build strength through sharing.
It is our society, our people, that have taken us from the passing of a hat to developing our national community and network. This March, we get to celebrate our field in a new way – Thursday, March 7, 2019, marks the inaugural National Hospitalist Day. Then, March 24-27, our annual conference, Hospital Medicine 2019, will bring thousands of our national team to National Harbor, Maryland. Join your colleagues. Find your niche and your community. Be a part of the change you want to see. While you are there, come introduce yourself to me and let me thank you for the amazing work you are doing.
We are all a part of this movement transforming patient care both on a local and national level. As we move to the future, our innovative, diverse, and connected network of hospital medicine will continue to create and guide health care advances in our country.
Dr. Thompson is professor and chief of the section of hospital medicine at University of Nebraska Medical Center, and medical director of clinical care transitions at Nebraska Medicine, Omaha.
Stories are told of the first meeting, 20 years ago, where a hat was passed to collect donations to develop a fledgling organization of inpatient physicians. Today, 90% of hospitals with 200+ beds operate with a hospitalist model. Today, we are the Society of Hospital Medicine.
In the early 1900s, health care in many ways was simple. It was a doctor with a shingle hung. It was house calls. Remedies were limited. In the 1940s, companies developed insurance benefits to lure workers during World War II; this third party, the payer, added complexity. Meanwhile, treatment options began to diversify. Then, in the 1960s, Medicare was passed, and the government came into the mix, further increasing this complexity. Diagnostic and treatment options continued to diversify, seemingly exponentially. Some would say it took 30 years for our country to recognize that it had created the most advanced and expensive, as well as one of the least quality-controlled, health systems in the world. Thus, as hospital medicine was conceived in the 1990s, our national health system was awakening to the need – the creative niche – that hospitalists would fill.
When I began my career, I was unaware that I was a hospitalist. The title didn’t exist. Yes, I was working solely in the hospital. I was developing programs to improve care delivery. I was rounding, teaching, collaborating, connecting – everything that we now call hospital medicine. That first job has evolved into my career, one that I find both honorable and enjoyable.
As health care changes with the passing years, being a hospitalist continues to be about serving people, connecting, and improving care. Being a hospitalist is being innovative, willing, and even daring. Dare to try, dare to fail, dare to redesign and try again. Hospital medicine is thinking outside of the box while knowing how to color between the lines. In the coming decades, health care will continue to evolve, and hospital medicine will too. We now encompass surgical comanagement and perioperative care, palliative care, postacute care, and transitions of care services. In corners, hospital medicine is already experimenting with telecare, virtual health, and hospital at home. Our hospital medicine workforce is innovative, diverse, tech savvy and poised for leading.
We are ready and willing to face the pressures affecting health care in the United States today: the recognition of an overwhelming expense to society, the relative underperformance with regard to quality, the increasing complexity of illness and treatment options, the worsening health of the average American citizen, the aging population, the role of medical error in patient harm, the increasing engagement of people in their own care, and the desire to make care better. What our country is facing is actually a phenomenal opportunity, no matter what side of the political aisle you live on. Being in hospital medicine today is being at the center front of this evolutionary stage.
Since joining the SHM board of directors, I continue to find examples of the stellar work of our staff and our members across the country. Having the privilege as a board member to join several Chapter meetings, I have witnessed firsthand the camaraderie, the compassion, the team that makes our Society work. From Houston to San Francisco and from St. Louis to Seattle, I have been honored to work with SHM members that create and nurture local and regional networks with the support of SHM’s Chapters program – a program that now houses more than 50 chapters and has launched regional districts to further support networking and growth. SHM’s chapter venues allow our larger hospital medicine team – yes, the national one – to connect and collaborate.
Take the Pacific Northwest Chapter. In its early years hospitalists from various and competing health systems would convene at a restaurant and just talk. They spoke of how to staff, how to pay, and how to negotiate with hospital leadership. As I have joined chapter meetings in recent years, meetings continue to be the place to share ideas – how to develop new programs; what is the most recent approach to glycemic control, sepsis care, or antibiotic stewardship; how best to approach diagnosis without “anchoring”; and even how to care for each other in the time of loss of a colleague to suicide. It is here in our community that we share experiences, knowledge, new ideas – and this sharing makes us all stronger.
Our hospital medicine community also comes together through areas of shared interest. There are 18 Special Interest Groups (SIGs), focused on specific topic areas. I have been privileged as a board member to work with our Perioperative/Comanagement SIG as it launched in 2017 and has grown rapidly. Currently, the community hosts a “case of the month” hospital medicine discussion as well as a regular journal club webinar that allows participants to review recent literature and interact directly with the authors. As this SIG has grown, shared resources and ideas have allowed for diffusion of knowledge, providing our nation with infrastructure for improving perioperative care. It is networks like this that support our national hospital medicine team to build strength through sharing.
It is our society, our people, that have taken us from the passing of a hat to developing our national community and network. This March, we get to celebrate our field in a new way – Thursday, March 7, 2019, marks the inaugural National Hospitalist Day. Then, March 24-27, our annual conference, Hospital Medicine 2019, will bring thousands of our national team to National Harbor, Maryland. Join your colleagues. Find your niche and your community. Be a part of the change you want to see. While you are there, come introduce yourself to me and let me thank you for the amazing work you are doing.
We are all a part of this movement transforming patient care both on a local and national level. As we move to the future, our innovative, diverse, and connected network of hospital medicine will continue to create and guide health care advances in our country.
Dr. Thompson is professor and chief of the section of hospital medicine at University of Nebraska Medical Center, and medical director of clinical care transitions at Nebraska Medicine, Omaha.