User login
Long-term side effects of CAR T cells mostly mild
SAN DIEGO – Longer-term follow-up of patients treated with CD19-targeted chimeric antigen receptor (CAR) T cells for hematologic malignancies indicates that the altered cells are generally safe, with most late events being mild in nature and possibly related to therapies delivered before or after CAR T cells, investigators reported.

Among patients treated with CD19-targeted CAR T cells for relapsed or refractory chronic lymphocytic leukemia (CLL) or non-Hodgkin lymphoma (NHL), the most frequent late adverse event was hypogammaglobulinemia, which occurred in 29 of 48 patients evaluated, reported Ana Cordeiro, MD, from the Fred Hutchinson Cancer Research Center in Seattle.
“Our results suggest that CD19 CAR T cells are safe,” Dr. Cordeiro said at the annual meeting of the American Society of Hematology. “However, continuing with prospective systematic and long-term follow-up of these patients is required for better understanding of these late effects.”
Dr. Cordeiro and colleagues studied a total of 60 patients who were enrolled in a phase 1/2 trial at their center of a CD19-targeted CAR T-cell construct and survived for at least 1 year.
The goal of the study was to describe complications that occurred or persisted beyond 90 days after CAR T-cell infusion.
The cohort included 43 patients treated for NHL and 17 treated for CLL. Patients with CLL were followed for a median of 27.5 months, and patients with NHL were followed for a median of 23.8 months.
As of September 2018, 47 patients were still alive, including 15 patients with CLL (88%) and 32 patients with NHL (74%). Of the 17 patients who died, 10 died from progressive disease (2 from CLL and 8 from NHL), and 3 patients died from nonrelapse causes associated with complications from subsequent allogeneic stem cell transplantation (allo-HCT), including 1 patient from graft-versus-host disease (GVHD) and infection, 1 from infection, and 1 from cerberovascular accident/thrombotic microangiopathy.
Of 38 patients who received additional therapies, 17 had subsequent CAR T-cell infusions under the same protocol, and 16 went on to allo-HCT. Treatments for the remaining five patients were not specified.
Of the 22 patients who did not receive additional treatment for their primary malignancies, 21 were in ongoing complete remission following a single CAR T-cell infusion after a median follow-up of 28 months. However, two patients in this group did require treatment for therapy-related myelodysplastic syndrome (t-MDS). The remaining patient had a small CLL clone at last follow-up.
Late adverse events included the following:
- Late significant cytopenias in three of 19 patients evaluated.
- Late hypogammaglobulinemia in 29 of 48 evaluated patients.
- A total of 138 late infections in 31 of the 60 patients.
- Subsequent malignancies in 10 of the 60 patients, including t-MDS, nonmelanoma skin cancer, and noninvasive bladder cancer.
- Late immune-related events in seven patients.
- Late neurogenic/psychiatric events, including one case each of transient ischemic attack at 3.8 months, encephalopathy and myoclonic seizure in the setting of chemotherapy, and a fatal cerebrovascular accident in the setting of allo-HCT and thrombotic microangiopathy. These patients did not have acute neurotoxicity after CAR T-cell therapy, Dr. Cordeiro noted. In addition, three patients experienced exacerbation of depression or anxiety following infusion.
- GVHD in nine patients at a median time from allo-HCT to first CAR T-cell infusion of 46.3 months (range, 6.7 months to 11 years).
Focusing on those patients who achieve complete remissions after CAR T-cell therapy could help investigators isolate late events that are most likely related to CAR T cells, Dr. Cordeiro said.
Dr. Cordeiro reported having no relevant conflicts of interest.
SOURCE: Cordeiro A et al. ASH 2018, Abstract 223.
SAN DIEGO – Longer-term follow-up of patients treated with CD19-targeted chimeric antigen receptor (CAR) T cells for hematologic malignancies indicates that the altered cells are generally safe, with most late events being mild in nature and possibly related to therapies delivered before or after CAR T cells, investigators reported.
Among patients treated with CD19-targeted CAR T cells for relapsed or refractory chronic lymphocytic leukemia (CLL) or non-Hodgkin lymphoma (NHL), the most frequent late adverse event was hypogammaglobulinemia, which occurred in 29 of 48 patients evaluated, reported Ana Cordeiro, MD, from the Fred Hutchinson Cancer Research Center in Seattle.
“Our results suggest that CD19 CAR T cells are safe,” Dr. Cordeiro said at the annual meeting of the American Society of Hematology. “However, continuing with prospective systematic and long-term follow-up of these patients is required for better understanding of these late effects.”
Dr. Cordeiro and colleagues studied a total of 60 patients who were enrolled in a phase 1/2 trial at their center of a CD19-targeted CAR T-cell construct and survived for at least 1 year.
The goal of the study was to describe complications that occurred or persisted beyond 90 days after CAR T-cell infusion.
The cohort included 43 patients treated for NHL and 17 treated for CLL. Patients with CLL were followed for a median of 27.5 months, and patients with NHL were followed for a median of 23.8 months.
As of September 2018, 47 patients were still alive, including 15 patients with CLL (88%) and 32 patients with NHL (74%). Of the 17 patients who died, 10 died from progressive disease (2 from CLL and 8 from NHL), and 3 patients died from nonrelapse causes associated with complications from subsequent allogeneic stem cell transplantation (allo-HCT), including 1 patient from graft-versus-host disease (GVHD) and infection, 1 from infection, and 1 from cerberovascular accident/thrombotic microangiopathy.
Of 38 patients who received additional therapies, 17 had subsequent CAR T-cell infusions under the same protocol, and 16 went on to allo-HCT. Treatments for the remaining five patients were not specified.
Of the 22 patients who did not receive additional treatment for their primary malignancies, 21 were in ongoing complete remission following a single CAR T-cell infusion after a median follow-up of 28 months. However, two patients in this group did require treatment for therapy-related myelodysplastic syndrome (t-MDS). The remaining patient had a small CLL clone at last follow-up.
Late adverse events included the following:
- Late significant cytopenias in three of 19 patients evaluated.
- Late hypogammaglobulinemia in 29 of 48 evaluated patients.
- A total of 138 late infections in 31 of the 60 patients.
- Subsequent malignancies in 10 of the 60 patients, including t-MDS, nonmelanoma skin cancer, and noninvasive bladder cancer.
- Late immune-related events in seven patients.
- Late neurogenic/psychiatric events, including one case each of transient ischemic attack at 3.8 months, encephalopathy and myoclonic seizure in the setting of chemotherapy, and a fatal cerebrovascular accident in the setting of allo-HCT and thrombotic microangiopathy. These patients did not have acute neurotoxicity after CAR T-cell therapy, Dr. Cordeiro noted. In addition, three patients experienced exacerbation of depression or anxiety following infusion.
- GVHD in nine patients at a median time from allo-HCT to first CAR T-cell infusion of 46.3 months (range, 6.7 months to 11 years).
Focusing on those patients who achieve complete remissions after CAR T-cell therapy could help investigators isolate late events that are most likely related to CAR T cells, Dr. Cordeiro said.
Dr. Cordeiro reported having no relevant conflicts of interest.
SOURCE: Cordeiro A et al. ASH 2018, Abstract 223.
SAN DIEGO – Longer-term follow-up of patients treated with CD19-targeted chimeric antigen receptor (CAR) T cells for hematologic malignancies indicates that the altered cells are generally safe, with most late events being mild in nature and possibly related to therapies delivered before or after CAR T cells, investigators reported.
Among patients treated with CD19-targeted CAR T cells for relapsed or refractory chronic lymphocytic leukemia (CLL) or non-Hodgkin lymphoma (NHL), the most frequent late adverse event was hypogammaglobulinemia, which occurred in 29 of 48 patients evaluated, reported Ana Cordeiro, MD, from the Fred Hutchinson Cancer Research Center in Seattle.
“Our results suggest that CD19 CAR T cells are safe,” Dr. Cordeiro said at the annual meeting of the American Society of Hematology. “However, continuing with prospective systematic and long-term follow-up of these patients is required for better understanding of these late effects.”
Dr. Cordeiro and colleagues studied a total of 60 patients who were enrolled in a phase 1/2 trial at their center of a CD19-targeted CAR T-cell construct and survived for at least 1 year.
The goal of the study was to describe complications that occurred or persisted beyond 90 days after CAR T-cell infusion.
The cohort included 43 patients treated for NHL and 17 treated for CLL. Patients with CLL were followed for a median of 27.5 months, and patients with NHL were followed for a median of 23.8 months.
As of September 2018, 47 patients were still alive, including 15 patients with CLL (88%) and 32 patients with NHL (74%). Of the 17 patients who died, 10 died from progressive disease (2 from CLL and 8 from NHL), and 3 patients died from nonrelapse causes associated with complications from subsequent allogeneic stem cell transplantation (allo-HCT), including 1 patient from graft-versus-host disease (GVHD) and infection, 1 from infection, and 1 from cerberovascular accident/thrombotic microangiopathy.
Of 38 patients who received additional therapies, 17 had subsequent CAR T-cell infusions under the same protocol, and 16 went on to allo-HCT. Treatments for the remaining five patients were not specified.
Of the 22 patients who did not receive additional treatment for their primary malignancies, 21 were in ongoing complete remission following a single CAR T-cell infusion after a median follow-up of 28 months. However, two patients in this group did require treatment for therapy-related myelodysplastic syndrome (t-MDS). The remaining patient had a small CLL clone at last follow-up.
Late adverse events included the following:
- Late significant cytopenias in three of 19 patients evaluated.
- Late hypogammaglobulinemia in 29 of 48 evaluated patients.
- A total of 138 late infections in 31 of the 60 patients.
- Subsequent malignancies in 10 of the 60 patients, including t-MDS, nonmelanoma skin cancer, and noninvasive bladder cancer.
- Late immune-related events in seven patients.
- Late neurogenic/psychiatric events, including one case each of transient ischemic attack at 3.8 months, encephalopathy and myoclonic seizure in the setting of chemotherapy, and a fatal cerebrovascular accident in the setting of allo-HCT and thrombotic microangiopathy. These patients did not have acute neurotoxicity after CAR T-cell therapy, Dr. Cordeiro noted. In addition, three patients experienced exacerbation of depression or anxiety following infusion.
- GVHD in nine patients at a median time from allo-HCT to first CAR T-cell infusion of 46.3 months (range, 6.7 months to 11 years).
Focusing on those patients who achieve complete remissions after CAR T-cell therapy could help investigators isolate late events that are most likely related to CAR T cells, Dr. Cordeiro said.
Dr. Cordeiro reported having no relevant conflicts of interest.
SOURCE: Cordeiro A et al. ASH 2018, Abstract 223.
REPORTING FROM ASH 2018
Key clinical point:
Major finding: The most frequent adverse event was hypogammaglobulinemia in 60% of evaluable patients.
Study details: Prospective observational study of 60 patients with relapsed/refractory CLL or NHL.
Disclosures: Dr. Cordeiro reported having no relevant conflicts of interest.
Source: Cordeiro A et al. ASH 2018, Abstract 223.
Integrated analysis suggests cladribine’s safety in MS
according to an integrated analysis of several clinical trials published in Multiple Sclerosis and Related Disorders.

The drug causes transient lymphopenia, as is to be expected from its mechanism of action, but most patients who receive cladribine do not have grade 3 or 4 lymphopenia, the authors wrote. In general, cladribine is not associated with an increased risk of infections or malignancy.
Data indicate that cladribine’s mechanism of action contributes to its durable clinical effect, despite the brief treatment periods. Clinical trials have provided information about the treatment’s safety and tolerability. To examine the treatment’s long-term safety, Stuart Cook, MD, of New Jersey Medical School, Newark, and his colleagues pooled data for patients with multiple sclerosis (MS) treated with cladribine tablets (3.5 mg/kg) as monotherapy or placebo in three phase 3 clinical trials (CLARITY, CLARITY Extension, and ORACLE-MS) and followed up in the PREMIERE registry. The investigators called these patients the monotherapy oral cohort.
To investigate the potential associations between cladribine and rarer adverse events such as malignancies, Dr. Cook and his colleagues examined data from patients with MS who received cladribine, regardless of the formulation or route of administration, or placebo (the all-exposed cohort). This cohort included data from the ONWARD trial, in which patients received cladribine tablets or placebo in combination with interferon-beta, as well as data from five trials in which patients received parenteral cladribine or placebo.
The monotherapy oral cohort included 923 patients who received cladribine and 641 who received placebo. The median age at enrollment in this cohort was approximately 36 years. The majority of patients were women and disease characteristics were balanced between arms. The all-exposed cohort included 1,926 patients who received cladribine and 802 who received placebo. The demographic characteristics of this cohort were similar to those of the monotherapy oral cohort.
In the monotherapy oral cohort, the incidence rate of treatment-emergent adverse events, in adjusted adverse events per 100 patient-years, was 103.29 for the active group versus 94.26 for controls. Lymphopenia (7.94 vs. 1.06) and decreased lymphocyte count (0.78 vs. 0.10) occurred more frequently in the active group than in the placebo group.
Herpes zoster also occurred more frequently in the cladribine group (0.83 vs. 0.20). However, cladribine was not associated with systemic serious disseminated herpes zoster. Furthermore, the investigators found no overall increased risk of infections, including opportunistic infections, with cladribine tablets versus placebo, except for herpes zoster.
In addition, Dr. Cook and his colleagues found no increase in malignancy rates among patients who received cladribine, compared with those who received placebo. They also found no increase in the incidence of malignancies over time in the cladribine group.
The adverse event profile for cladribine tablets (3.5 mg/kg) as monotherapy has been well characterized, the investigators wrote. The results of this analysis are broadly similar to the short-term adverse event results reported in the individual trials.
EMD Serono and Merck Serono, two affiliates of Merck in Darmstadt, Germany, sponsored the study. Merck manufactures cladribine.
SOURCE: Cook S et al. Mult Scler Relat Disord. 2018 Nov 18. doi: 10.1016/j.msard.2018.11.021.
according to an integrated analysis of several clinical trials published in Multiple Sclerosis and Related Disorders.
The drug causes transient lymphopenia, as is to be expected from its mechanism of action, but most patients who receive cladribine do not have grade 3 or 4 lymphopenia, the authors wrote. In general, cladribine is not associated with an increased risk of infections or malignancy.
Data indicate that cladribine’s mechanism of action contributes to its durable clinical effect, despite the brief treatment periods. Clinical trials have provided information about the treatment’s safety and tolerability. To examine the treatment’s long-term safety, Stuart Cook, MD, of New Jersey Medical School, Newark, and his colleagues pooled data for patients with multiple sclerosis (MS) treated with cladribine tablets (3.5 mg/kg) as monotherapy or placebo in three phase 3 clinical trials (CLARITY, CLARITY Extension, and ORACLE-MS) and followed up in the PREMIERE registry. The investigators called these patients the monotherapy oral cohort.
To investigate the potential associations between cladribine and rarer adverse events such as malignancies, Dr. Cook and his colleagues examined data from patients with MS who received cladribine, regardless of the formulation or route of administration, or placebo (the all-exposed cohort). This cohort included data from the ONWARD trial, in which patients received cladribine tablets or placebo in combination with interferon-beta, as well as data from five trials in which patients received parenteral cladribine or placebo.
The monotherapy oral cohort included 923 patients who received cladribine and 641 who received placebo. The median age at enrollment in this cohort was approximately 36 years. The majority of patients were women and disease characteristics were balanced between arms. The all-exposed cohort included 1,926 patients who received cladribine and 802 who received placebo. The demographic characteristics of this cohort were similar to those of the monotherapy oral cohort.
In the monotherapy oral cohort, the incidence rate of treatment-emergent adverse events, in adjusted adverse events per 100 patient-years, was 103.29 for the active group versus 94.26 for controls. Lymphopenia (7.94 vs. 1.06) and decreased lymphocyte count (0.78 vs. 0.10) occurred more frequently in the active group than in the placebo group.
Herpes zoster also occurred more frequently in the cladribine group (0.83 vs. 0.20). However, cladribine was not associated with systemic serious disseminated herpes zoster. Furthermore, the investigators found no overall increased risk of infections, including opportunistic infections, with cladribine tablets versus placebo, except for herpes zoster.
In addition, Dr. Cook and his colleagues found no increase in malignancy rates among patients who received cladribine, compared with those who received placebo. They also found no increase in the incidence of malignancies over time in the cladribine group.
The adverse event profile for cladribine tablets (3.5 mg/kg) as monotherapy has been well characterized, the investigators wrote. The results of this analysis are broadly similar to the short-term adverse event results reported in the individual trials.
EMD Serono and Merck Serono, two affiliates of Merck in Darmstadt, Germany, sponsored the study. Merck manufactures cladribine.
SOURCE: Cook S et al. Mult Scler Relat Disord. 2018 Nov 18. doi: 10.1016/j.msard.2018.11.021.
according to an integrated analysis of several clinical trials published in Multiple Sclerosis and Related Disorders.
The drug causes transient lymphopenia, as is to be expected from its mechanism of action, but most patients who receive cladribine do not have grade 3 or 4 lymphopenia, the authors wrote. In general, cladribine is not associated with an increased risk of infections or malignancy.
Data indicate that cladribine’s mechanism of action contributes to its durable clinical effect, despite the brief treatment periods. Clinical trials have provided information about the treatment’s safety and tolerability. To examine the treatment’s long-term safety, Stuart Cook, MD, of New Jersey Medical School, Newark, and his colleagues pooled data for patients with multiple sclerosis (MS) treated with cladribine tablets (3.5 mg/kg) as monotherapy or placebo in three phase 3 clinical trials (CLARITY, CLARITY Extension, and ORACLE-MS) and followed up in the PREMIERE registry. The investigators called these patients the monotherapy oral cohort.
To investigate the potential associations between cladribine and rarer adverse events such as malignancies, Dr. Cook and his colleagues examined data from patients with MS who received cladribine, regardless of the formulation or route of administration, or placebo (the all-exposed cohort). This cohort included data from the ONWARD trial, in which patients received cladribine tablets or placebo in combination with interferon-beta, as well as data from five trials in which patients received parenteral cladribine or placebo.
The monotherapy oral cohort included 923 patients who received cladribine and 641 who received placebo. The median age at enrollment in this cohort was approximately 36 years. The majority of patients were women and disease characteristics were balanced between arms. The all-exposed cohort included 1,926 patients who received cladribine and 802 who received placebo. The demographic characteristics of this cohort were similar to those of the monotherapy oral cohort.
In the monotherapy oral cohort, the incidence rate of treatment-emergent adverse events, in adjusted adverse events per 100 patient-years, was 103.29 for the active group versus 94.26 for controls. Lymphopenia (7.94 vs. 1.06) and decreased lymphocyte count (0.78 vs. 0.10) occurred more frequently in the active group than in the placebo group.
Herpes zoster also occurred more frequently in the cladribine group (0.83 vs. 0.20). However, cladribine was not associated with systemic serious disseminated herpes zoster. Furthermore, the investigators found no overall increased risk of infections, including opportunistic infections, with cladribine tablets versus placebo, except for herpes zoster.
In addition, Dr. Cook and his colleagues found no increase in malignancy rates among patients who received cladribine, compared with those who received placebo. They also found no increase in the incidence of malignancies over time in the cladribine group.
The adverse event profile for cladribine tablets (3.5 mg/kg) as monotherapy has been well characterized, the investigators wrote. The results of this analysis are broadly similar to the short-term adverse event results reported in the individual trials.
EMD Serono and Merck Serono, two affiliates of Merck in Darmstadt, Germany, sponsored the study. Merck manufactures cladribine.
SOURCE: Cook S et al. Mult Scler Relat Disord. 2018 Nov 18. doi: 10.1016/j.msard.2018.11.021.
FROM MULTIPLE SCLEROSIS AND RELATED DISORDERS
Key clinical point: The safety results of an integrated analysis of cladribine therapy are broadly similar to those of previous trials.
Major finding: The incidence rate of treatment-emergent adverse events was similar between cladribine and placebo.
Study details: An integrated analysis including 4,292 patients with relapsing remitting multiple sclerosis.
Disclosures: EMD Serono and Merck Serono, two affiliates of Merck in Darmstadt, Germany, sponsored the study. Merck manufactures cladribine.
Source: Cook S et al. Mult Scler Relat Disord. 2018 Nov 18. doi: 10.1016/j.msard.2018.11.021.
White matter volume reduced in first-episode depression
Decrements ‘seem to vanish’ after 2-year follow-up
White matter volume was significantly reduced initially in patients with first-episode depression, but not after a 2-year follow-up, according to Mar Carceller-Sindreu, MD, of the department of psychiatry at Hospital de la Santa Creu i Sant Pau in Barcelona, and her associates.
A total of 33 patients with first-episode depression and 33 healthy controls were included in the study. Among them, 27 first-episode depression patients and 17 controls completed the 2-year follow-up. They underwent structural MRIs at baseline and at follow-up, the Hamilton Depressive Rating Scale was administered throughout the study period, and whole-brain, voxel-based morphometry was used to measure white matter and gray matter, Dr. Carceller-Sindreu and her associates wrote. The report is in the Journal of Affective Disorders.
At baseline, the white matter volume in the prefrontal cortex of patients with first-episode depression was significantly lower than in healthy controls; no difference was seen in gray matter volume. At the 2-year follow-up, no difference was seen in either white matter or gray matter volume. In other words, the baseline differences “seem to vanish, as if they were normalized,” Dr. Carceller-Sindreu said. The normalization of white matter might have been caused by treatment normalization or attributable to lack of study power, she and her associates noted.
In addition, patients who had recurring depression over the study period had higher white matter volume in the left posterior corona radiata and right posterior thalamic radiation at follow-up, compared with patients whose depression did not recur. This finding “could represent compensatory effects to cope with the disease,” the investigators wrote.
“, so as to unveil many of the open questions,” they concluded.
The study was supported by the Spanish FIS grant, the European Regional Development Fund, and the CERCA Programme. Two study authors reported conflicts of interest with numerous pharmaceutical companies.
SOURCE: Carceller-Sindreu M et al. J Affect Disord. 2018 Nov 13. doi: 10.1016/j.jad.2018.11.085.
Decrements ‘seem to vanish’ after 2-year follow-up
Decrements ‘seem to vanish’ after 2-year follow-up
White matter volume was significantly reduced initially in patients with first-episode depression, but not after a 2-year follow-up, according to Mar Carceller-Sindreu, MD, of the department of psychiatry at Hospital de la Santa Creu i Sant Pau in Barcelona, and her associates.
A total of 33 patients with first-episode depression and 33 healthy controls were included in the study. Among them, 27 first-episode depression patients and 17 controls completed the 2-year follow-up. They underwent structural MRIs at baseline and at follow-up, the Hamilton Depressive Rating Scale was administered throughout the study period, and whole-brain, voxel-based morphometry was used to measure white matter and gray matter, Dr. Carceller-Sindreu and her associates wrote. The report is in the Journal of Affective Disorders.
At baseline, the white matter volume in the prefrontal cortex of patients with first-episode depression was significantly lower than in healthy controls; no difference was seen in gray matter volume. At the 2-year follow-up, no difference was seen in either white matter or gray matter volume. In other words, the baseline differences “seem to vanish, as if they were normalized,” Dr. Carceller-Sindreu said. The normalization of white matter might have been caused by treatment normalization or attributable to lack of study power, she and her associates noted.
In addition, patients who had recurring depression over the study period had higher white matter volume in the left posterior corona radiata and right posterior thalamic radiation at follow-up, compared with patients whose depression did not recur. This finding “could represent compensatory effects to cope with the disease,” the investigators wrote.
“, so as to unveil many of the open questions,” they concluded.
The study was supported by the Spanish FIS grant, the European Regional Development Fund, and the CERCA Programme. Two study authors reported conflicts of interest with numerous pharmaceutical companies.
SOURCE: Carceller-Sindreu M et al. J Affect Disord. 2018 Nov 13. doi: 10.1016/j.jad.2018.11.085.
White matter volume was significantly reduced initially in patients with first-episode depression, but not after a 2-year follow-up, according to Mar Carceller-Sindreu, MD, of the department of psychiatry at Hospital de la Santa Creu i Sant Pau in Barcelona, and her associates.
A total of 33 patients with first-episode depression and 33 healthy controls were included in the study. Among them, 27 first-episode depression patients and 17 controls completed the 2-year follow-up. They underwent structural MRIs at baseline and at follow-up, the Hamilton Depressive Rating Scale was administered throughout the study period, and whole-brain, voxel-based morphometry was used to measure white matter and gray matter, Dr. Carceller-Sindreu and her associates wrote. The report is in the Journal of Affective Disorders.
At baseline, the white matter volume in the prefrontal cortex of patients with first-episode depression was significantly lower than in healthy controls; no difference was seen in gray matter volume. At the 2-year follow-up, no difference was seen in either white matter or gray matter volume. In other words, the baseline differences “seem to vanish, as if they were normalized,” Dr. Carceller-Sindreu said. The normalization of white matter might have been caused by treatment normalization or attributable to lack of study power, she and her associates noted.
In addition, patients who had recurring depression over the study period had higher white matter volume in the left posterior corona radiata and right posterior thalamic radiation at follow-up, compared with patients whose depression did not recur. This finding “could represent compensatory effects to cope with the disease,” the investigators wrote.
“, so as to unveil many of the open questions,” they concluded.
The study was supported by the Spanish FIS grant, the European Regional Development Fund, and the CERCA Programme. Two study authors reported conflicts of interest with numerous pharmaceutical companies.
SOURCE: Carceller-Sindreu M et al. J Affect Disord. 2018 Nov 13. doi: 10.1016/j.jad.2018.11.085.
FROM THE JOURNAL OF AFFECTIVE DISORDERS
Expert calls for better ways to preserve beta cell function in youth
LOS ANGELES –

At the same time, the SEARCH for Diabetes in Youth trial showed that the incidence of T2DM in U.S. youth continues to rise, especially among Native Americans and non-Hispanic blacks (P less than .001 for both associations; N Engl J Med. 2017;376:1419-29). In addition, the earlier Treatment Options for Type 2 Diabetes in Adolescents and Youth (TODAY) study showed that rapid treatment failure in youth-onset T2DM was associated with loss of beta cell function (N Engl J Med. 2012;366:2247-56).
“Early treatment of youth with impaired glucose tolerance or type 2 diabetes may require other medications alone or in combination or for longer periods of time to combat the severe insulin resistance of puberty and arrest progressive loss of beta cell function,” Sonia Caprio, MD, said at the World Congress on Insulin Resistance, Diabetes & Cardiovascular Disease.
She based her remarks on a review of the recently completed multicenter Restoring Insulin Secretion (RISE) Pediatric Medication Study, (Diabetes Care 2018;41[8]:1717-25). It set out to answer the following question: In adolescents with impaired glucose tolerance or recently diagnosed T2DM, can beta cell function be preserved or improved during 12 months of active treatment and maintained for 3 months following the withdrawal of therapy?
To find out, Dr. Caprio, a pediatric endocrinologist at Yale University, New Haven, Conn., and her colleagues enrolled 91 youth who were randomized to one of two treatment arms: metformin alone titrated over 4 weeks from 500 mg/day to a 1,000 mg twice daily dose (modified if necessary due to GI symptoms), or to glargine followed by metformin. This group received once-daily insulin glargine, titrated twice weekly over 1 month based on daily self-monitoring of blood glucose to a goal of 80-90 mg/dL. Glargine was discontinued after 3 months and metformin was titrated. Beta-cell function (insulin sensitivity paired with beta-cell responses) was assessed by the two-step hyperglycemic clamp at baseline, 12 months (on treatment), and 15 months (3 months off treatment). All clinical data were collected 3 months after discontinuation of active treatment.
Dr. Caprio described the two-step hyperglycemic clamp as “a robust approach to quantification of insulin sensitivity and beta-cell responses to both glucose and the nonglucose secretagogue arginine. It provides mechanistic insights into how the tested interventions affected two key metabolic defects of type 2 diabetes: insulin sensitivity and beta cell responses.”
The mean age of patients was 14 years, 71% were female, their mean body mass index was 37 kg/m2. The researchers observed no significant differences between treatment groups at baseline, 12 months, or 15 months in beta cell function, BMI percentile, hemoglobin A1c, fasting glucose, or oral glucose tolerance test 2-hour glucose results. In both treatment groups, clamp-measured beta cell function was significantly lower at 12 and 15 months, compared with baseline. HbA1c fell transiently at 6 months within both groups. BMI was higher in the glargine followed by metformin versus metformin alone group between 3 and 9 months. Only 5% of participants discontinued the interventions, and both treatments were well tolerated.
“These findings are discouraging,” Dr. Caprio said. “They contrast with previous studies in adults showing an improvement in beta cell function with metformin or insulin for type 2 diabetes prevention and treatment.” Results of the RISE Pediatric Medication Study “call for further studies to better understand the physiology underlying beta cell dysfunction in youth to identify effective treatment options. Better approaches to prevent and treat obesity in youth are critically needed.”
Dr. Caprio reported having no disclosures.
LOS ANGELES –
At the same time, the SEARCH for Diabetes in Youth trial showed that the incidence of T2DM in U.S. youth continues to rise, especially among Native Americans and non-Hispanic blacks (P less than .001 for both associations; N Engl J Med. 2017;376:1419-29). In addition, the earlier Treatment Options for Type 2 Diabetes in Adolescents and Youth (TODAY) study showed that rapid treatment failure in youth-onset T2DM was associated with loss of beta cell function (N Engl J Med. 2012;366:2247-56).
“Early treatment of youth with impaired glucose tolerance or type 2 diabetes may require other medications alone or in combination or for longer periods of time to combat the severe insulin resistance of puberty and arrest progressive loss of beta cell function,” Sonia Caprio, MD, said at the World Congress on Insulin Resistance, Diabetes & Cardiovascular Disease.
She based her remarks on a review of the recently completed multicenter Restoring Insulin Secretion (RISE) Pediatric Medication Study, (Diabetes Care 2018;41[8]:1717-25). It set out to answer the following question: In adolescents with impaired glucose tolerance or recently diagnosed T2DM, can beta cell function be preserved or improved during 12 months of active treatment and maintained for 3 months following the withdrawal of therapy?
To find out, Dr. Caprio, a pediatric endocrinologist at Yale University, New Haven, Conn., and her colleagues enrolled 91 youth who were randomized to one of two treatment arms: metformin alone titrated over 4 weeks from 500 mg/day to a 1,000 mg twice daily dose (modified if necessary due to GI symptoms), or to glargine followed by metformin. This group received once-daily insulin glargine, titrated twice weekly over 1 month based on daily self-monitoring of blood glucose to a goal of 80-90 mg/dL. Glargine was discontinued after 3 months and metformin was titrated. Beta-cell function (insulin sensitivity paired with beta-cell responses) was assessed by the two-step hyperglycemic clamp at baseline, 12 months (on treatment), and 15 months (3 months off treatment). All clinical data were collected 3 months after discontinuation of active treatment.
Dr. Caprio described the two-step hyperglycemic clamp as “a robust approach to quantification of insulin sensitivity and beta-cell responses to both glucose and the nonglucose secretagogue arginine. It provides mechanistic insights into how the tested interventions affected two key metabolic defects of type 2 diabetes: insulin sensitivity and beta cell responses.”
The mean age of patients was 14 years, 71% were female, their mean body mass index was 37 kg/m2. The researchers observed no significant differences between treatment groups at baseline, 12 months, or 15 months in beta cell function, BMI percentile, hemoglobin A1c, fasting glucose, or oral glucose tolerance test 2-hour glucose results. In both treatment groups, clamp-measured beta cell function was significantly lower at 12 and 15 months, compared with baseline. HbA1c fell transiently at 6 months within both groups. BMI was higher in the glargine followed by metformin versus metformin alone group between 3 and 9 months. Only 5% of participants discontinued the interventions, and both treatments were well tolerated.
“These findings are discouraging,” Dr. Caprio said. “They contrast with previous studies in adults showing an improvement in beta cell function with metformin or insulin for type 2 diabetes prevention and treatment.” Results of the RISE Pediatric Medication Study “call for further studies to better understand the physiology underlying beta cell dysfunction in youth to identify effective treatment options. Better approaches to prevent and treat obesity in youth are critically needed.”
Dr. Caprio reported having no disclosures.
LOS ANGELES –
At the same time, the SEARCH for Diabetes in Youth trial showed that the incidence of T2DM in U.S. youth continues to rise, especially among Native Americans and non-Hispanic blacks (P less than .001 for both associations; N Engl J Med. 2017;376:1419-29). In addition, the earlier Treatment Options for Type 2 Diabetes in Adolescents and Youth (TODAY) study showed that rapid treatment failure in youth-onset T2DM was associated with loss of beta cell function (N Engl J Med. 2012;366:2247-56).
“Early treatment of youth with impaired glucose tolerance or type 2 diabetes may require other medications alone or in combination or for longer periods of time to combat the severe insulin resistance of puberty and arrest progressive loss of beta cell function,” Sonia Caprio, MD, said at the World Congress on Insulin Resistance, Diabetes & Cardiovascular Disease.
She based her remarks on a review of the recently completed multicenter Restoring Insulin Secretion (RISE) Pediatric Medication Study, (Diabetes Care 2018;41[8]:1717-25). It set out to answer the following question: In adolescents with impaired glucose tolerance or recently diagnosed T2DM, can beta cell function be preserved or improved during 12 months of active treatment and maintained for 3 months following the withdrawal of therapy?
To find out, Dr. Caprio, a pediatric endocrinologist at Yale University, New Haven, Conn., and her colleagues enrolled 91 youth who were randomized to one of two treatment arms: metformin alone titrated over 4 weeks from 500 mg/day to a 1,000 mg twice daily dose (modified if necessary due to GI symptoms), or to glargine followed by metformin. This group received once-daily insulin glargine, titrated twice weekly over 1 month based on daily self-monitoring of blood glucose to a goal of 80-90 mg/dL. Glargine was discontinued after 3 months and metformin was titrated. Beta-cell function (insulin sensitivity paired with beta-cell responses) was assessed by the two-step hyperglycemic clamp at baseline, 12 months (on treatment), and 15 months (3 months off treatment). All clinical data were collected 3 months after discontinuation of active treatment.
Dr. Caprio described the two-step hyperglycemic clamp as “a robust approach to quantification of insulin sensitivity and beta-cell responses to both glucose and the nonglucose secretagogue arginine. It provides mechanistic insights into how the tested interventions affected two key metabolic defects of type 2 diabetes: insulin sensitivity and beta cell responses.”
The mean age of patients was 14 years, 71% were female, their mean body mass index was 37 kg/m2. The researchers observed no significant differences between treatment groups at baseline, 12 months, or 15 months in beta cell function, BMI percentile, hemoglobin A1c, fasting glucose, or oral glucose tolerance test 2-hour glucose results. In both treatment groups, clamp-measured beta cell function was significantly lower at 12 and 15 months, compared with baseline. HbA1c fell transiently at 6 months within both groups. BMI was higher in the glargine followed by metformin versus metformin alone group between 3 and 9 months. Only 5% of participants discontinued the interventions, and both treatments were well tolerated.
“These findings are discouraging,” Dr. Caprio said. “They contrast with previous studies in adults showing an improvement in beta cell function with metformin or insulin for type 2 diabetes prevention and treatment.” Results of the RISE Pediatric Medication Study “call for further studies to better understand the physiology underlying beta cell dysfunction in youth to identify effective treatment options. Better approaches to prevent and treat obesity in youth are critically needed.”
Dr. Caprio reported having no disclosures.
EXPERT ANALYSIS FROM WCIRDC 2018
Synthetic opioids drive spike in U.S. fatal drug overdoses
New federal statistics suggest that the opioid epidemic in the United States is evolving as physicians crack down on the use of prescription painkillers: Fatal drug overdose deaths rose by 12% from 2016 to 2017, boosted by a wave of fatalities linked to illicit synthetic opioids like fentanyl that are now linked to an estimated 60% of opioid-related deaths.

“Overall, the overdose epidemic continues to worsen, and it has grown increasingly complex by coinvolvement of prescription and illicit drugs,” Lawrence Scholl, PhD, MPH, and his associates at the Centers for Disease Control & Prevention wrote in the Morbidity and Mortality Weekly Report.
The new statistics provide more evidence that 2017 marked “a sharp increase in what has characterized as the third wave of the opioid epidemic,” said drug and health policy researcher Stephen Crystal, PhD, of Rutgers University, New Brunswick, N.J., in an interview. He was referring to a wave that experts believe started in 2013 amid a spike in U.S. overdose deaths from fentanyl and other synthetic opioids.
The new report analyzes fatal drug overdose data from 2013 to 2017. According to the findings, the total number of those overdoses rose to 70,237 in 2017, up from 63,632 in 2016. The highest drug overdose death rates in 2017 were in West Virginia, followed by Ohio, Pennsylvania, and the District of Columbia.
Some statistics did not change much from 2016 to 2017: About two-thirds of the drug overdose deaths were linked to opioids in both years, and the death rate of cases linked to prescription drugs and heroin remained steady. (Death rates in the report were age adjusted.)
However, the percentage of fatal overdose cases linked to synthetic opioids grew 45% from 2016 to 2017. Overall, 60% of opioid-related fatal overdoses in 2017 involved synthetic opioids.
The report identifies increases in several areas from 2016 to 2017. Opioid-related drug overdose deaths among black people rose by 25%, and an analysis of data from 34 states and the District of Columbia found the highest increases in death rates in North Carolina (29%), Ohio (19%), and Maine (19%).
In regard to deaths linked to synthetic opioids specifically, the highest death rates in 2017 were in West Virginia (37 per 100,000), Ohio (32 per 100,000), and New Hampshire (30 per 100,000).
“Part of what we’re seeing in these increased numbers are individuals who have pain, can’t get prescribed opioids, and turn to street drugs,” Dr. Crystal said, adding that “abruptly cutting patients off is not good, and leaving patients with a lot of untreated pain is not good. If people are going to be discontinued [from opioids] or have their doses reduced, the taper needs to be done very slowly and carefully.”
Synthetic opioids were not the only drugs that are driving up fatal overdoses, as the death rates of cases linked to cocaine and psychostimulants (such as methamphetamine) jumped by more than a third in 2017.
“The most important thing these numbers are telling me is that it’s becoming more and more attractive to drug dealers to put fentanyl in the heroin, cocaine, and other drugs they sell,” Dr. Crystal said. “When that happens, dependence on street drugs becomes much more deadly. It’s almost impossible to get the dose right. Every time you shoot up, you’re taking a chance that you’ll overdose.”
The report had limitations, including the fact that details about drug use were missing from 12% (2016) and 15% (2017) of death certificates in fatal overdose cases. By state, the percentages of those death certificates that included drug information ranged from as little as 55% to 99%.
There’s some possible positive news: The report points to preliminary data from 2018 suggesting that the number of annual drug overdose deaths may be leveling off – although it says more analysis is needed to confirm the trend.
Dr. Crystal, however, is not celebrating. “I don’t see this as a good news story, really,” he said, adding that there’s “a little too much of people patting themselves on the back” because they’re proud of cutbacks in opioid prescriptions.
“This doesn’t have to do with the huge number of people who got started with opioids years ago” and are now at risk of using street drugs, he said. “We haven’t engaged that population at the rate we need to. And flattening out at 70,000 drug overdoses a year is not a good news story.”
Dr. Crystal reported no relevant disclosures.
SOURCE: Scholl L et al. MMWR. 2019 Jan 4;67(5152):1419-27.
New federal statistics suggest that the opioid epidemic in the United States is evolving as physicians crack down on the use of prescription painkillers: Fatal drug overdose deaths rose by 12% from 2016 to 2017, boosted by a wave of fatalities linked to illicit synthetic opioids like fentanyl that are now linked to an estimated 60% of opioid-related deaths.
“Overall, the overdose epidemic continues to worsen, and it has grown increasingly complex by coinvolvement of prescription and illicit drugs,” Lawrence Scholl, PhD, MPH, and his associates at the Centers for Disease Control & Prevention wrote in the Morbidity and Mortality Weekly Report.
The new statistics provide more evidence that 2017 marked “a sharp increase in what has characterized as the third wave of the opioid epidemic,” said drug and health policy researcher Stephen Crystal, PhD, of Rutgers University, New Brunswick, N.J., in an interview. He was referring to a wave that experts believe started in 2013 amid a spike in U.S. overdose deaths from fentanyl and other synthetic opioids.
The new report analyzes fatal drug overdose data from 2013 to 2017. According to the findings, the total number of those overdoses rose to 70,237 in 2017, up from 63,632 in 2016. The highest drug overdose death rates in 2017 were in West Virginia, followed by Ohio, Pennsylvania, and the District of Columbia.
Some statistics did not change much from 2016 to 2017: About two-thirds of the drug overdose deaths were linked to opioids in both years, and the death rate of cases linked to prescription drugs and heroin remained steady. (Death rates in the report were age adjusted.)
However, the percentage of fatal overdose cases linked to synthetic opioids grew 45% from 2016 to 2017. Overall, 60% of opioid-related fatal overdoses in 2017 involved synthetic opioids.
The report identifies increases in several areas from 2016 to 2017. Opioid-related drug overdose deaths among black people rose by 25%, and an analysis of data from 34 states and the District of Columbia found the highest increases in death rates in North Carolina (29%), Ohio (19%), and Maine (19%).
In regard to deaths linked to synthetic opioids specifically, the highest death rates in 2017 were in West Virginia (37 per 100,000), Ohio (32 per 100,000), and New Hampshire (30 per 100,000).
“Part of what we’re seeing in these increased numbers are individuals who have pain, can’t get prescribed opioids, and turn to street drugs,” Dr. Crystal said, adding that “abruptly cutting patients off is not good, and leaving patients with a lot of untreated pain is not good. If people are going to be discontinued [from opioids] or have their doses reduced, the taper needs to be done very slowly and carefully.”
Synthetic opioids were not the only drugs that are driving up fatal overdoses, as the death rates of cases linked to cocaine and psychostimulants (such as methamphetamine) jumped by more than a third in 2017.
“The most important thing these numbers are telling me is that it’s becoming more and more attractive to drug dealers to put fentanyl in the heroin, cocaine, and other drugs they sell,” Dr. Crystal said. “When that happens, dependence on street drugs becomes much more deadly. It’s almost impossible to get the dose right. Every time you shoot up, you’re taking a chance that you’ll overdose.”
The report had limitations, including the fact that details about drug use were missing from 12% (2016) and 15% (2017) of death certificates in fatal overdose cases. By state, the percentages of those death certificates that included drug information ranged from as little as 55% to 99%.
There’s some possible positive news: The report points to preliminary data from 2018 suggesting that the number of annual drug overdose deaths may be leveling off – although it says more analysis is needed to confirm the trend.
Dr. Crystal, however, is not celebrating. “I don’t see this as a good news story, really,” he said, adding that there’s “a little too much of people patting themselves on the back” because they’re proud of cutbacks in opioid prescriptions.
“This doesn’t have to do with the huge number of people who got started with opioids years ago” and are now at risk of using street drugs, he said. “We haven’t engaged that population at the rate we need to. And flattening out at 70,000 drug overdoses a year is not a good news story.”
Dr. Crystal reported no relevant disclosures.
SOURCE: Scholl L et al. MMWR. 2019 Jan 4;67(5152):1419-27.
New federal statistics suggest that the opioid epidemic in the United States is evolving as physicians crack down on the use of prescription painkillers: Fatal drug overdose deaths rose by 12% from 2016 to 2017, boosted by a wave of fatalities linked to illicit synthetic opioids like fentanyl that are now linked to an estimated 60% of opioid-related deaths.
“Overall, the overdose epidemic continues to worsen, and it has grown increasingly complex by coinvolvement of prescription and illicit drugs,” Lawrence Scholl, PhD, MPH, and his associates at the Centers for Disease Control & Prevention wrote in the Morbidity and Mortality Weekly Report.
The new statistics provide more evidence that 2017 marked “a sharp increase in what has characterized as the third wave of the opioid epidemic,” said drug and health policy researcher Stephen Crystal, PhD, of Rutgers University, New Brunswick, N.J., in an interview. He was referring to a wave that experts believe started in 2013 amid a spike in U.S. overdose deaths from fentanyl and other synthetic opioids.
The new report analyzes fatal drug overdose data from 2013 to 2017. According to the findings, the total number of those overdoses rose to 70,237 in 2017, up from 63,632 in 2016. The highest drug overdose death rates in 2017 were in West Virginia, followed by Ohio, Pennsylvania, and the District of Columbia.
Some statistics did not change much from 2016 to 2017: About two-thirds of the drug overdose deaths were linked to opioids in both years, and the death rate of cases linked to prescription drugs and heroin remained steady. (Death rates in the report were age adjusted.)
However, the percentage of fatal overdose cases linked to synthetic opioids grew 45% from 2016 to 2017. Overall, 60% of opioid-related fatal overdoses in 2017 involved synthetic opioids.
The report identifies increases in several areas from 2016 to 2017. Opioid-related drug overdose deaths among black people rose by 25%, and an analysis of data from 34 states and the District of Columbia found the highest increases in death rates in North Carolina (29%), Ohio (19%), and Maine (19%).
In regard to deaths linked to synthetic opioids specifically, the highest death rates in 2017 were in West Virginia (37 per 100,000), Ohio (32 per 100,000), and New Hampshire (30 per 100,000).
“Part of what we’re seeing in these increased numbers are individuals who have pain, can’t get prescribed opioids, and turn to street drugs,” Dr. Crystal said, adding that “abruptly cutting patients off is not good, and leaving patients with a lot of untreated pain is not good. If people are going to be discontinued [from opioids] or have their doses reduced, the taper needs to be done very slowly and carefully.”
Synthetic opioids were not the only drugs that are driving up fatal overdoses, as the death rates of cases linked to cocaine and psychostimulants (such as methamphetamine) jumped by more than a third in 2017.
“The most important thing these numbers are telling me is that it’s becoming more and more attractive to drug dealers to put fentanyl in the heroin, cocaine, and other drugs they sell,” Dr. Crystal said. “When that happens, dependence on street drugs becomes much more deadly. It’s almost impossible to get the dose right. Every time you shoot up, you’re taking a chance that you’ll overdose.”
The report had limitations, including the fact that details about drug use were missing from 12% (2016) and 15% (2017) of death certificates in fatal overdose cases. By state, the percentages of those death certificates that included drug information ranged from as little as 55% to 99%.
There’s some possible positive news: The report points to preliminary data from 2018 suggesting that the number of annual drug overdose deaths may be leveling off – although it says more analysis is needed to confirm the trend.
Dr. Crystal, however, is not celebrating. “I don’t see this as a good news story, really,” he said, adding that there’s “a little too much of people patting themselves on the back” because they’re proud of cutbacks in opioid prescriptions.
“This doesn’t have to do with the huge number of people who got started with opioids years ago” and are now at risk of using street drugs, he said. “We haven’t engaged that population at the rate we need to. And flattening out at 70,000 drug overdoses a year is not a good news story.”
Dr. Crystal reported no relevant disclosures.
SOURCE: Scholl L et al. MMWR. 2019 Jan 4;67(5152):1419-27.
FROM MMWR
Ticagrelor holds no edge over aspirin in CABG patients
CHICAGO – Ticagrelor performed about as well as aspirin did as monotherapy for preventing coronary bypass graft failure during the year following surgery in a randomized, multicenter trial with almost 1,900 patients.

Ticagrelor monotherapy also produced about the same number of major bleeding events as did aspirin monotherapy, Heribert Schunkert, MD, said at the American Heart Association scientific sessions. There were two limitations of the trial: The incidence of cardiovascular disease events that served as the efficacy endpoint for the study was less than what Dr. Schunkert and his associates expected, and they enrolled about half the projected number of patients because the study lost industry support and then, a couple of years later, showed a relentlessly neutral result leading to early termination of recruitment, said Dr. Schunkert, professor of cardiology and medical director of the German Heart Center in Munich.
The TiCAB (Study Comparing Ticagrelor With Aspirin for Prevention of Vascular Events in Patients Undergoing CABG) trial randomized 1,893 patients during 2013-2017 who underwent CABG at any of 26 centers in Austria, Germany, or Switzerland. Eligible patients underwent surgery for three-vessel disease, left main disease, or had two-vessel disease plus a left ventricular ejection fraction of less than 50%. About 31% of patients had unstable angina or non-ST elevation MI, with the remaining 69% having stable angina. The study included 931 patients who received 90 mg oral ticagrelor (Brilinta) b.i.d. plus aspirin placebo, and 928 who received 100 mg aspirin once daily plus ticagrelor placebo. The study medications began prior to surgery.
The study’s primary efficacy endpoint was the combined rate of cardiovascular death, MI, stroke, or need for revascularization by 1 year after surgery. This occurred in 9.7% of the ticagrelor patients and in 8.2% of those who received aspirin, a difference that was not statistically significant. Several secondary efficacy endpoints examined also showed a neutral result. The primary safety measure was the incidence of major bleeds by the Bleeding Academic Research Consortium criteria, which occurred in 3.7% of the ticagrelor patients and 3.2% of those on aspirin, not a statistically significant difference. After the year of follow-up about 85% of patients in both treatment arms remained on their assigned regimen, Dr. Schunkert said.
TiCAB received funding from AstraZeneca, which markets ticagrelor (Brilinta). Dr. Schunkert has received honoraria and research support from, and has been a speaker on behalf of, AstraZeneca. He has also received honoraria from Amgen, Bayer Vital, Boehringer Ingelheim, Daiichi Sankyo, Merck Sharp & Dohme, Novartis, Pfizer, Sanofi, and Servier.
SOURCE: Schunkert H et al. AHA 2018, Abstract 19561.
Because the TiCAB study was about half the size of the planned study, its power was low and yielded a result with wide confidence intervals. Despite that, I do not believe that a further, larger study is warranted. The TiCAB results are sufficient to show that monotherapy with ticagrelor is not superior to monotherapy with aspirin in patients undergoing coronary artery bypass grafting and during the year following surgery. The TiCAB results add to a larger body of evidence indicating ticagrelor’s noninferiority to and lack of superiority to aspirin as monotherapy for patients with coronary artery disease or a history of ischemic stroke or transient ischemic attack.
How can these two drugs produce similar efficacy outcomes? Aspirin is an effective antiplatelet drug, and evidence also suggests that treatment with opiates such as morphine (Circ Cardiovasc Interv. 2016 Sept;9[9]:e004229) and fentanyl (Circulation. 2018 Jan 16;137[3]:307-9) during and after surgery can interfere with the intestinal absorption of ticagrelor and other oral P2Y12 receptor antagonists, such as clopidogrel and prasugrel.
Another interesting finding in TiCAB was that aspirin and ticagrelor monotherapy produced similar rates of major bleeds. Results from prior studies had raised concerns about ticagrelor’s safety in patients undergoing coronary artery bypass surgery, but the new results show that this may be a problem when patients receive dual antiplatelet therapy but not when they receive ticagrelor monotherapy. Current evidence favors dual antiplatelet therapy to achieve a greater decrease in cardiovascular disease events, but this occurs at the expense of increased bleeding. Larger trials of dual therapy after coronary artery bypass grafting are warranted; further study of monotherapy is not.
Robert F. Storey, MD , is a professor of cardiology at the University of Sheffield (England). He has been a consultant to, and received honoraria and research support from, AstraZeneca, and he has been a consultant to Actelion, Avacta, Bayer, Bristol-Myers Squibb/Pfizer, Haemonetics, Novartis, PlaqueTec, and Thromboserin. He made these comments as designated discussant for the TiCAB report.
Because the TiCAB study was about half the size of the planned study, its power was low and yielded a result with wide confidence intervals. Despite that, I do not believe that a further, larger study is warranted. The TiCAB results are sufficient to show that monotherapy with ticagrelor is not superior to monotherapy with aspirin in patients undergoing coronary artery bypass grafting and during the year following surgery. The TiCAB results add to a larger body of evidence indicating ticagrelor’s noninferiority to and lack of superiority to aspirin as monotherapy for patients with coronary artery disease or a history of ischemic stroke or transient ischemic attack.
How can these two drugs produce similar efficacy outcomes? Aspirin is an effective antiplatelet drug, and evidence also suggests that treatment with opiates such as morphine (Circ Cardiovasc Interv. 2016 Sept;9[9]:e004229) and fentanyl (Circulation. 2018 Jan 16;137[3]:307-9) during and after surgery can interfere with the intestinal absorption of ticagrelor and other oral P2Y12 receptor antagonists, such as clopidogrel and prasugrel.
Another interesting finding in TiCAB was that aspirin and ticagrelor monotherapy produced similar rates of major bleeds. Results from prior studies had raised concerns about ticagrelor’s safety in patients undergoing coronary artery bypass surgery, but the new results show that this may be a problem when patients receive dual antiplatelet therapy but not when they receive ticagrelor monotherapy. Current evidence favors dual antiplatelet therapy to achieve a greater decrease in cardiovascular disease events, but this occurs at the expense of increased bleeding. Larger trials of dual therapy after coronary artery bypass grafting are warranted; further study of monotherapy is not.
Robert F. Storey, MD , is a professor of cardiology at the University of Sheffield (England). He has been a consultant to, and received honoraria and research support from, AstraZeneca, and he has been a consultant to Actelion, Avacta, Bayer, Bristol-Myers Squibb/Pfizer, Haemonetics, Novartis, PlaqueTec, and Thromboserin. He made these comments as designated discussant for the TiCAB report.
Because the TiCAB study was about half the size of the planned study, its power was low and yielded a result with wide confidence intervals. Despite that, I do not believe that a further, larger study is warranted. The TiCAB results are sufficient to show that monotherapy with ticagrelor is not superior to monotherapy with aspirin in patients undergoing coronary artery bypass grafting and during the year following surgery. The TiCAB results add to a larger body of evidence indicating ticagrelor’s noninferiority to and lack of superiority to aspirin as monotherapy for patients with coronary artery disease or a history of ischemic stroke or transient ischemic attack.
How can these two drugs produce similar efficacy outcomes? Aspirin is an effective antiplatelet drug, and evidence also suggests that treatment with opiates such as morphine (Circ Cardiovasc Interv. 2016 Sept;9[9]:e004229) and fentanyl (Circulation. 2018 Jan 16;137[3]:307-9) during and after surgery can interfere with the intestinal absorption of ticagrelor and other oral P2Y12 receptor antagonists, such as clopidogrel and prasugrel.
Another interesting finding in TiCAB was that aspirin and ticagrelor monotherapy produced similar rates of major bleeds. Results from prior studies had raised concerns about ticagrelor’s safety in patients undergoing coronary artery bypass surgery, but the new results show that this may be a problem when patients receive dual antiplatelet therapy but not when they receive ticagrelor monotherapy. Current evidence favors dual antiplatelet therapy to achieve a greater decrease in cardiovascular disease events, but this occurs at the expense of increased bleeding. Larger trials of dual therapy after coronary artery bypass grafting are warranted; further study of monotherapy is not.
Robert F. Storey, MD , is a professor of cardiology at the University of Sheffield (England). He has been a consultant to, and received honoraria and research support from, AstraZeneca, and he has been a consultant to Actelion, Avacta, Bayer, Bristol-Myers Squibb/Pfizer, Haemonetics, Novartis, PlaqueTec, and Thromboserin. He made these comments as designated discussant for the TiCAB report.
CHICAGO – Ticagrelor performed about as well as aspirin did as monotherapy for preventing coronary bypass graft failure during the year following surgery in a randomized, multicenter trial with almost 1,900 patients.
Ticagrelor monotherapy also produced about the same number of major bleeding events as did aspirin monotherapy, Heribert Schunkert, MD, said at the American Heart Association scientific sessions. There were two limitations of the trial: The incidence of cardiovascular disease events that served as the efficacy endpoint for the study was less than what Dr. Schunkert and his associates expected, and they enrolled about half the projected number of patients because the study lost industry support and then, a couple of years later, showed a relentlessly neutral result leading to early termination of recruitment, said Dr. Schunkert, professor of cardiology and medical director of the German Heart Center in Munich.
The TiCAB (Study Comparing Ticagrelor With Aspirin for Prevention of Vascular Events in Patients Undergoing CABG) trial randomized 1,893 patients during 2013-2017 who underwent CABG at any of 26 centers in Austria, Germany, or Switzerland. Eligible patients underwent surgery for three-vessel disease, left main disease, or had two-vessel disease plus a left ventricular ejection fraction of less than 50%. About 31% of patients had unstable angina or non-ST elevation MI, with the remaining 69% having stable angina. The study included 931 patients who received 90 mg oral ticagrelor (Brilinta) b.i.d. plus aspirin placebo, and 928 who received 100 mg aspirin once daily plus ticagrelor placebo. The study medications began prior to surgery.
The study’s primary efficacy endpoint was the combined rate of cardiovascular death, MI, stroke, or need for revascularization by 1 year after surgery. This occurred in 9.7% of the ticagrelor patients and in 8.2% of those who received aspirin, a difference that was not statistically significant. Several secondary efficacy endpoints examined also showed a neutral result. The primary safety measure was the incidence of major bleeds by the Bleeding Academic Research Consortium criteria, which occurred in 3.7% of the ticagrelor patients and 3.2% of those on aspirin, not a statistically significant difference. After the year of follow-up about 85% of patients in both treatment arms remained on their assigned regimen, Dr. Schunkert said.
TiCAB received funding from AstraZeneca, which markets ticagrelor (Brilinta). Dr. Schunkert has received honoraria and research support from, and has been a speaker on behalf of, AstraZeneca. He has also received honoraria from Amgen, Bayer Vital, Boehringer Ingelheim, Daiichi Sankyo, Merck Sharp & Dohme, Novartis, Pfizer, Sanofi, and Servier.
SOURCE: Schunkert H et al. AHA 2018, Abstract 19561.
CHICAGO – Ticagrelor performed about as well as aspirin did as monotherapy for preventing coronary bypass graft failure during the year following surgery in a randomized, multicenter trial with almost 1,900 patients.
Ticagrelor monotherapy also produced about the same number of major bleeding events as did aspirin monotherapy, Heribert Schunkert, MD, said at the American Heart Association scientific sessions. There were two limitations of the trial: The incidence of cardiovascular disease events that served as the efficacy endpoint for the study was less than what Dr. Schunkert and his associates expected, and they enrolled about half the projected number of patients because the study lost industry support and then, a couple of years later, showed a relentlessly neutral result leading to early termination of recruitment, said Dr. Schunkert, professor of cardiology and medical director of the German Heart Center in Munich.
The TiCAB (Study Comparing Ticagrelor With Aspirin for Prevention of Vascular Events in Patients Undergoing CABG) trial randomized 1,893 patients during 2013-2017 who underwent CABG at any of 26 centers in Austria, Germany, or Switzerland. Eligible patients underwent surgery for three-vessel disease, left main disease, or had two-vessel disease plus a left ventricular ejection fraction of less than 50%. About 31% of patients had unstable angina or non-ST elevation MI, with the remaining 69% having stable angina. The study included 931 patients who received 90 mg oral ticagrelor (Brilinta) b.i.d. plus aspirin placebo, and 928 who received 100 mg aspirin once daily plus ticagrelor placebo. The study medications began prior to surgery.
The study’s primary efficacy endpoint was the combined rate of cardiovascular death, MI, stroke, or need for revascularization by 1 year after surgery. This occurred in 9.7% of the ticagrelor patients and in 8.2% of those who received aspirin, a difference that was not statistically significant. Several secondary efficacy endpoints examined also showed a neutral result. The primary safety measure was the incidence of major bleeds by the Bleeding Academic Research Consortium criteria, which occurred in 3.7% of the ticagrelor patients and 3.2% of those on aspirin, not a statistically significant difference. After the year of follow-up about 85% of patients in both treatment arms remained on their assigned regimen, Dr. Schunkert said.
TiCAB received funding from AstraZeneca, which markets ticagrelor (Brilinta). Dr. Schunkert has received honoraria and research support from, and has been a speaker on behalf of, AstraZeneca. He has also received honoraria from Amgen, Bayer Vital, Boehringer Ingelheim, Daiichi Sankyo, Merck Sharp & Dohme, Novartis, Pfizer, Sanofi, and Servier.
SOURCE: Schunkert H et al. AHA 2018, Abstract 19561.
REPORTING FROM THE AHA SCIENTIFIC SESSIONS
Key clinical point: Ticagrelor was similar to aspirin for preventing graft failure in CABG patients.
Major finding: After 1 year, the combined cardiovascular disease endpoint occurred in 9.7% of ticagrelor patients and in 8.2% on aspirin.
Study details: TiCAB, a multicenter, randomized trial with 1,893 patients.
Disclosures: TiCAB received funding from AstraZeneca, which markets ticagrelor (Brilinta). Dr. Schunkert has received honoraria and research support from, and has been a speaker on behalf of, AstraZeneca. He has received honoraria from Amgen, Bayer Vital, Boehringer Ingelheim, Daiichi Sankyo, Merck Sharp & Dohme, Novartis, Pfizer, Sanofi, and Servier.
Source: Schunkert H et al. AHA 2018, Abstract 19561.
Prenatal valproate exposure raises ADHD risk
Children exposed to valproate in utero were 48% more likely to be diagnosed with ADHD when compared with unexposed children in a population-based cohort study of more than 900,000 children in Denmark.

Antiepileptic drug exposure is associated with an increased risk of various congenital malformations, but its role in the development of ADHD in children has not been well documented, first author Jakob Christensen, MD, PhD, DrMedSci, of Aarhus (Denmark) University Hospital, and his colleagues wrote in their paper, published online Jan. 4 in JAMA Network Open.
The researchers identified 913,302 singleton births in Denmark from 1997 through 2011, with children followed through 2015.
Overall, children who were prenatally exposed to valproate had a 48% increased risk of ADHD. Antiepileptic drug exposure was defined as 30 days before the estimated day of conception to the day of birth, and included valproate, clobazam, and other antiepileptic drugs. The average age of the children at the study’s end was 10 years, and approximately half were male.
A total of 580 children were exposed to valproate in utero; of these, 8.4% were later diagnosed with ADHD, compared with 3.2% of 912,722 children who were not exposed to valproate. In addition, the absolute 15-year risk of ADHD was 11% in valproate-exposed children vs. 4.6% in unexposed children. No significant associations appeared between ADHD and other antiepileptic drugs.
The study findings were limited by several factors, including the contraindication of valproate for use in pregnancy, which may mean that the women taking valproate had more severe disease, the researchers noted.
“Due to the observational nature of this study, we cannot rule out that the observed risk increase for ADHD is at least in part explained by the mother’s health condition that triggered the prescription of valproate during pregnancy,” they said. Other limitations included a lack of data on the exact amounts of valproate taken during pregnancy and the potential impact of nonepilepsy medications, they noted.
However, the results were strengthened by the large size and population-based cohort, and support warnings by professional medical organizations against valproate use in pregnancy, the researchers said. “As randomized clinical trials of valproate use during pregnancy are neither feasible nor ethical, our study provides clinical information on the risk of ADHD associated with valproate use during pregnancy,” they concluded.
The study was supported by grants to various authors from the Danish Epilepsy Association Central Denmark Region, the Aarhus University Research Foundation, the Lundbeck Foundation, the National Institutes of Health, the Novo Nordisk Foundation, and the European Commission.
SOURCE: Christensen J et al. JAMA Network Open. 2019;2(1):e186606. doi: 10.1001/jamanetworkopen.2018.6606.
The data from the current study differ from a recent meta-analysis of five studies that did not find a statistically significant increase in ADHD risk in children associated with prenatal valproate exposure, Kimford J. Meador, MD, wrote in an accompanying editorial (JAMA Network Open. 2019;2[1]:e186603. doi: 10.1001/jamanetworkopen.2018.6603). 
“The discrepancy between the present study and the prior meta-analysis might be due to the meta-analysis using different analytical approaches and examining studies with smaller sample sizes, higher attrition rates, shorter follow-ups, and cohort differences,” Dr. Meador said. “Nevertheless, the findings by Christensen et al. are consistent with multiple studies demonstrating adverse neurodevelopmental effects associated with fetal valproate exposure.”
Given the potential risks associated with valproate exposure not only for behavior problems such as ADHD but also for congenital malformations and other cognitive and behavioral issues in children, women of childbearing age who are using valproate or considering a prescription should be counseled for informed consent, Dr. Meador said.
Dr. Meador advocated additional research on the impact of antiepileptic drugs during pregnancy and risk assessment strategies, including “a national reporting system for congenital malformations, routine preclinical testing of all new antiseizure medications for neurodevelopmental effects, monitoring of antiseizure medication prescription practices for women of childbearing age to determine whether emerging knowledge is being appropriately applied, and improved funding of basic and clinical research to fully delineate risks and underlying mechanisms of anatomical and behavioral teratogenesis from antiseizure medications.”
Dr. Meador is affiliated with the department of neurology and neurological sciences at Stanford (Calif.) University. He disclosed research support from the National Institutes of Health and Sunovion, and travel support from UCB. The Epilepsy Study Consortium pays Stanford University for his research consultant time related to Eisai, GW Pharmaceuticals, NeuroPace, Novartis, Supernus, Upsher-Smith Laboratories, UCB, and Vivus.
The data from the current study differ from a recent meta-analysis of five studies that did not find a statistically significant increase in ADHD risk in children associated with prenatal valproate exposure, Kimford J. Meador, MD, wrote in an accompanying editorial (JAMA Network Open. 2019;2[1]:e186603. doi: 10.1001/jamanetworkopen.2018.6603).
“The discrepancy between the present study and the prior meta-analysis might be due to the meta-analysis using different analytical approaches and examining studies with smaller sample sizes, higher attrition rates, shorter follow-ups, and cohort differences,” Dr. Meador said. “Nevertheless, the findings by Christensen et al. are consistent with multiple studies demonstrating adverse neurodevelopmental effects associated with fetal valproate exposure.”
Given the potential risks associated with valproate exposure not only for behavior problems such as ADHD but also for congenital malformations and other cognitive and behavioral issues in children, women of childbearing age who are using valproate or considering a prescription should be counseled for informed consent, Dr. Meador said.
Dr. Meador advocated additional research on the impact of antiepileptic drugs during pregnancy and risk assessment strategies, including “a national reporting system for congenital malformations, routine preclinical testing of all new antiseizure medications for neurodevelopmental effects, monitoring of antiseizure medication prescription practices for women of childbearing age to determine whether emerging knowledge is being appropriately applied, and improved funding of basic and clinical research to fully delineate risks and underlying mechanisms of anatomical and behavioral teratogenesis from antiseizure medications.”
Dr. Meador is affiliated with the department of neurology and neurological sciences at Stanford (Calif.) University. He disclosed research support from the National Institutes of Health and Sunovion, and travel support from UCB. The Epilepsy Study Consortium pays Stanford University for his research consultant time related to Eisai, GW Pharmaceuticals, NeuroPace, Novartis, Supernus, Upsher-Smith Laboratories, UCB, and Vivus.
The data from the current study differ from a recent meta-analysis of five studies that did not find a statistically significant increase in ADHD risk in children associated with prenatal valproate exposure, Kimford J. Meador, MD, wrote in an accompanying editorial (JAMA Network Open. 2019;2[1]:e186603. doi: 10.1001/jamanetworkopen.2018.6603).
“The discrepancy between the present study and the prior meta-analysis might be due to the meta-analysis using different analytical approaches and examining studies with smaller sample sizes, higher attrition rates, shorter follow-ups, and cohort differences,” Dr. Meador said. “Nevertheless, the findings by Christensen et al. are consistent with multiple studies demonstrating adverse neurodevelopmental effects associated with fetal valproate exposure.”
Given the potential risks associated with valproate exposure not only for behavior problems such as ADHD but also for congenital malformations and other cognitive and behavioral issues in children, women of childbearing age who are using valproate or considering a prescription should be counseled for informed consent, Dr. Meador said.
Dr. Meador advocated additional research on the impact of antiepileptic drugs during pregnancy and risk assessment strategies, including “a national reporting system for congenital malformations, routine preclinical testing of all new antiseizure medications for neurodevelopmental effects, monitoring of antiseizure medication prescription practices for women of childbearing age to determine whether emerging knowledge is being appropriately applied, and improved funding of basic and clinical research to fully delineate risks and underlying mechanisms of anatomical and behavioral teratogenesis from antiseizure medications.”
Dr. Meador is affiliated with the department of neurology and neurological sciences at Stanford (Calif.) University. He disclosed research support from the National Institutes of Health and Sunovion, and travel support from UCB. The Epilepsy Study Consortium pays Stanford University for his research consultant time related to Eisai, GW Pharmaceuticals, NeuroPace, Novartis, Supernus, Upsher-Smith Laboratories, UCB, and Vivus.
Children exposed to valproate in utero were 48% more likely to be diagnosed with ADHD when compared with unexposed children in a population-based cohort study of more than 900,000 children in Denmark.
Antiepileptic drug exposure is associated with an increased risk of various congenital malformations, but its role in the development of ADHD in children has not been well documented, first author Jakob Christensen, MD, PhD, DrMedSci, of Aarhus (Denmark) University Hospital, and his colleagues wrote in their paper, published online Jan. 4 in JAMA Network Open.
The researchers identified 913,302 singleton births in Denmark from 1997 through 2011, with children followed through 2015.
Overall, children who were prenatally exposed to valproate had a 48% increased risk of ADHD. Antiepileptic drug exposure was defined as 30 days before the estimated day of conception to the day of birth, and included valproate, clobazam, and other antiepileptic drugs. The average age of the children at the study’s end was 10 years, and approximately half were male.
A total of 580 children were exposed to valproate in utero; of these, 8.4% were later diagnosed with ADHD, compared with 3.2% of 912,722 children who were not exposed to valproate. In addition, the absolute 15-year risk of ADHD was 11% in valproate-exposed children vs. 4.6% in unexposed children. No significant associations appeared between ADHD and other antiepileptic drugs.
The study findings were limited by several factors, including the contraindication of valproate for use in pregnancy, which may mean that the women taking valproate had more severe disease, the researchers noted.
“Due to the observational nature of this study, we cannot rule out that the observed risk increase for ADHD is at least in part explained by the mother’s health condition that triggered the prescription of valproate during pregnancy,” they said. Other limitations included a lack of data on the exact amounts of valproate taken during pregnancy and the potential impact of nonepilepsy medications, they noted.
However, the results were strengthened by the large size and population-based cohort, and support warnings by professional medical organizations against valproate use in pregnancy, the researchers said. “As randomized clinical trials of valproate use during pregnancy are neither feasible nor ethical, our study provides clinical information on the risk of ADHD associated with valproate use during pregnancy,” they concluded.
The study was supported by grants to various authors from the Danish Epilepsy Association Central Denmark Region, the Aarhus University Research Foundation, the Lundbeck Foundation, the National Institutes of Health, the Novo Nordisk Foundation, and the European Commission.
SOURCE: Christensen J et al. JAMA Network Open. 2019;2(1):e186606. doi: 10.1001/jamanetworkopen.2018.6606.
Children exposed to valproate in utero were 48% more likely to be diagnosed with ADHD when compared with unexposed children in a population-based cohort study of more than 900,000 children in Denmark.
Antiepileptic drug exposure is associated with an increased risk of various congenital malformations, but its role in the development of ADHD in children has not been well documented, first author Jakob Christensen, MD, PhD, DrMedSci, of Aarhus (Denmark) University Hospital, and his colleagues wrote in their paper, published online Jan. 4 in JAMA Network Open.
The researchers identified 913,302 singleton births in Denmark from 1997 through 2011, with children followed through 2015.
Overall, children who were prenatally exposed to valproate had a 48% increased risk of ADHD. Antiepileptic drug exposure was defined as 30 days before the estimated day of conception to the day of birth, and included valproate, clobazam, and other antiepileptic drugs. The average age of the children at the study’s end was 10 years, and approximately half were male.
A total of 580 children were exposed to valproate in utero; of these, 8.4% were later diagnosed with ADHD, compared with 3.2% of 912,722 children who were not exposed to valproate. In addition, the absolute 15-year risk of ADHD was 11% in valproate-exposed children vs. 4.6% in unexposed children. No significant associations appeared between ADHD and other antiepileptic drugs.
The study findings were limited by several factors, including the contraindication of valproate for use in pregnancy, which may mean that the women taking valproate had more severe disease, the researchers noted.
“Due to the observational nature of this study, we cannot rule out that the observed risk increase for ADHD is at least in part explained by the mother’s health condition that triggered the prescription of valproate during pregnancy,” they said. Other limitations included a lack of data on the exact amounts of valproate taken during pregnancy and the potential impact of nonepilepsy medications, they noted.
However, the results were strengthened by the large size and population-based cohort, and support warnings by professional medical organizations against valproate use in pregnancy, the researchers said. “As randomized clinical trials of valproate use during pregnancy are neither feasible nor ethical, our study provides clinical information on the risk of ADHD associated with valproate use during pregnancy,” they concluded.
The study was supported by grants to various authors from the Danish Epilepsy Association Central Denmark Region, the Aarhus University Research Foundation, the Lundbeck Foundation, the National Institutes of Health, the Novo Nordisk Foundation, and the European Commission.
SOURCE: Christensen J et al. JAMA Network Open. 2019;2(1):e186606. doi: 10.1001/jamanetworkopen.2018.6606.
FROM JAMA NETWORK OPEN
Key clinical point:
Major finding: The children whose mothers used valproate between 90 days before conception and birth had a 48% increased risk of ADHD compared with children whose mothers did not use valproate.
Study details: The data come from a population-based cohort study of 913,302 children in Denmark.
Disclosures: The study was supported by grants to various authors from the Danish Epilepsy Association Central Denmark Region, the Aarhus University Research Foundation, the Lundbeck Foundation, the National Institutes of Health, the Novo Nordisk Foundation, and the European Commission.
Source: SOURCE: Christensen J et al. JAMA Network Open. 2019;2(1):e186606. doi: 10.1001/jamanetworkopen.2018.6606.
Sex differences provide insight into glioblastoma treatment
Sex-specific treatment strategies may prolong survival and improve outcomes in male and female patients with glioblastoma, investigators suggest after a retrospective analysis.
In an analysis of data from 63 men and women with glioblastoma, the researchers found that a significant reduction in tumor growth velocity during standard chemotherapeutic treatment was seen only for females patients with glioblastoma (P = .02569). In addition, they reported that for female patients, a reduction in tumor growth velocity was linked with significantly increased survival versus higher velocity growth (median survival, 3090 days vs. 681 days; P = .00817).
In contrast, the men in the study showed no statistically significant correlation between survival and velocity, the investigators reported.
The researchers analyzed data from 63 patients with glioblastoma using clinical information from a research database at the Mayo Clinic in Phoenix. They also incorporated transcriptome data, which was connected via an electronic algorithm, and were able to detect certain molecular variations of glioblastoma that are integral components of survival for individuals with the disease. From these findings, Wei Yang, PhD, of Washington University, St. Louis, along with his colleagues, were able to validate links between the effects of chemotherapy and gene expression.
“We measured sex differences in the in vitro cytotoxic effects of four common chemotherapeutics in a panel of nine (five male and four female) patient-derived glioblastoma cell isolates,” the investigators said in Science Translational Medicine.
The authors acknowledged a key limitation of the study was the retrospective nature of the imaging analysis, which has the potential to introduce interoperator differences in tumor growth velocity measurements. With these limitations, Dr. Yang and his colleagues highlighted the importance of ensuring imaging data is verified by trained professionals.
“Together, these results suggest that greater precision in glioblastoma molecular subtyping can be achieved through sex-specific analyses and that improved outcomes for all patients might be accomplished by tailoring treatment to sex differences in molecular mechanisms,” they concluded.
The study was supported by grant funding from the National Institutes of Health, Children’s Discovery Institute of Washington University, James S. McDonnell Foundation, Ivy Foundation, Ben & Catherine Ivy Foundation, and the Mayo Clinic. Albert H. Kim and Kristin R. Swanson reported financial affiliations with Monterris and the James S. McDonnell Foundation. Other authors reported no conflicts of interest related to the work.
SOURCE: Yang W et al. Sci Transl Med. 2019 Jan 02. doi: 10.1126/scitranslmed.aao5253.
Sex-specific treatment strategies may prolong survival and improve outcomes in male and female patients with glioblastoma, investigators suggest after a retrospective analysis.
In an analysis of data from 63 men and women with glioblastoma, the researchers found that a significant reduction in tumor growth velocity during standard chemotherapeutic treatment was seen only for females patients with glioblastoma (P = .02569). In addition, they reported that for female patients, a reduction in tumor growth velocity was linked with significantly increased survival versus higher velocity growth (median survival, 3090 days vs. 681 days; P = .00817).
In contrast, the men in the study showed no statistically significant correlation between survival and velocity, the investigators reported.
The researchers analyzed data from 63 patients with glioblastoma using clinical information from a research database at the Mayo Clinic in Phoenix. They also incorporated transcriptome data, which was connected via an electronic algorithm, and were able to detect certain molecular variations of glioblastoma that are integral components of survival for individuals with the disease. From these findings, Wei Yang, PhD, of Washington University, St. Louis, along with his colleagues, were able to validate links between the effects of chemotherapy and gene expression.
“We measured sex differences in the in vitro cytotoxic effects of four common chemotherapeutics in a panel of nine (five male and four female) patient-derived glioblastoma cell isolates,” the investigators said in Science Translational Medicine.
The authors acknowledged a key limitation of the study was the retrospective nature of the imaging analysis, which has the potential to introduce interoperator differences in tumor growth velocity measurements. With these limitations, Dr. Yang and his colleagues highlighted the importance of ensuring imaging data is verified by trained professionals.
“Together, these results suggest that greater precision in glioblastoma molecular subtyping can be achieved through sex-specific analyses and that improved outcomes for all patients might be accomplished by tailoring treatment to sex differences in molecular mechanisms,” they concluded.
The study was supported by grant funding from the National Institutes of Health, Children’s Discovery Institute of Washington University, James S. McDonnell Foundation, Ivy Foundation, Ben & Catherine Ivy Foundation, and the Mayo Clinic. Albert H. Kim and Kristin R. Swanson reported financial affiliations with Monterris and the James S. McDonnell Foundation. Other authors reported no conflicts of interest related to the work.
SOURCE: Yang W et al. Sci Transl Med. 2019 Jan 02. doi: 10.1126/scitranslmed.aao5253.
Sex-specific treatment strategies may prolong survival and improve outcomes in male and female patients with glioblastoma, investigators suggest after a retrospective analysis.
In an analysis of data from 63 men and women with glioblastoma, the researchers found that a significant reduction in tumor growth velocity during standard chemotherapeutic treatment was seen only for females patients with glioblastoma (P = .02569). In addition, they reported that for female patients, a reduction in tumor growth velocity was linked with significantly increased survival versus higher velocity growth (median survival, 3090 days vs. 681 days; P = .00817).
In contrast, the men in the study showed no statistically significant correlation between survival and velocity, the investigators reported.
The researchers analyzed data from 63 patients with glioblastoma using clinical information from a research database at the Mayo Clinic in Phoenix. They also incorporated transcriptome data, which was connected via an electronic algorithm, and were able to detect certain molecular variations of glioblastoma that are integral components of survival for individuals with the disease. From these findings, Wei Yang, PhD, of Washington University, St. Louis, along with his colleagues, were able to validate links between the effects of chemotherapy and gene expression.
“We measured sex differences in the in vitro cytotoxic effects of four common chemotherapeutics in a panel of nine (five male and four female) patient-derived glioblastoma cell isolates,” the investigators said in Science Translational Medicine.
The authors acknowledged a key limitation of the study was the retrospective nature of the imaging analysis, which has the potential to introduce interoperator differences in tumor growth velocity measurements. With these limitations, Dr. Yang and his colleagues highlighted the importance of ensuring imaging data is verified by trained professionals.
“Together, these results suggest that greater precision in glioblastoma molecular subtyping can be achieved through sex-specific analyses and that improved outcomes for all patients might be accomplished by tailoring treatment to sex differences in molecular mechanisms,” they concluded.
The study was supported by grant funding from the National Institutes of Health, Children’s Discovery Institute of Washington University, James S. McDonnell Foundation, Ivy Foundation, Ben & Catherine Ivy Foundation, and the Mayo Clinic. Albert H. Kim and Kristin R. Swanson reported financial affiliations with Monterris and the James S. McDonnell Foundation. Other authors reported no conflicts of interest related to the work.
SOURCE: Yang W et al. Sci Transl Med. 2019 Jan 02. doi: 10.1126/scitranslmed.aao5253.
FROM SCIENCE TRANSLATIONAL MEDICINE
Key clinical point: .
Major finding: In females, reduced tumor growth velocity was linked with significantly increased survival versus higher growth velocity (P = .00817).
Study details: Quantitative imaging and molecular analysis of 63 patients with glioblastoma.
Disclosures: The study was supported by grant funding from the National Institutes of Health, Children’s Discovery Institute of Washington University, James S. McDonnell Foundation, Ivy Foundation, Ben & Catherine Ivy Foundation, and the Mayo Clinic. Albert H. Kim and Kristin R. Swanson reported financial affiliations with Monterris and the James S. McDonnell Foundation. Other authors reported no conflicts of interest related to the work.
Source: Yang W et al. Sci Transl Med. 2019 Jan 02. doi: 10.1126/scitranslmed.aao5253.
Ascending Erythematous Nodules on the Arm
The Diagnosis: Primary Cutaneous Nocardiosis
Comprehensive metabolic panel and complete blood cell count were unremarkable; human immunodeficiency virus screening was nonreactive. Punch biopsies were obtained for histopathology, as well as bacterial, fungal, and mycobacterial cultures. Histopathologic examination of a 4-mm punch biopsy of the forearm nodule showed a dermal abscess with neutrophilic infiltration in the dermis (Figure 1). No organisms were seen on Gram, methenamine-silver, periodic acid–Schiff, or acid-fast bacteria stains. Given the clinical suspicion for lymphocutaneous sporotrichosis, the patient was started on itraconazole. She reported modest improvement but subsequently developed a morbilliform eruption necessitating medication discontinuation.
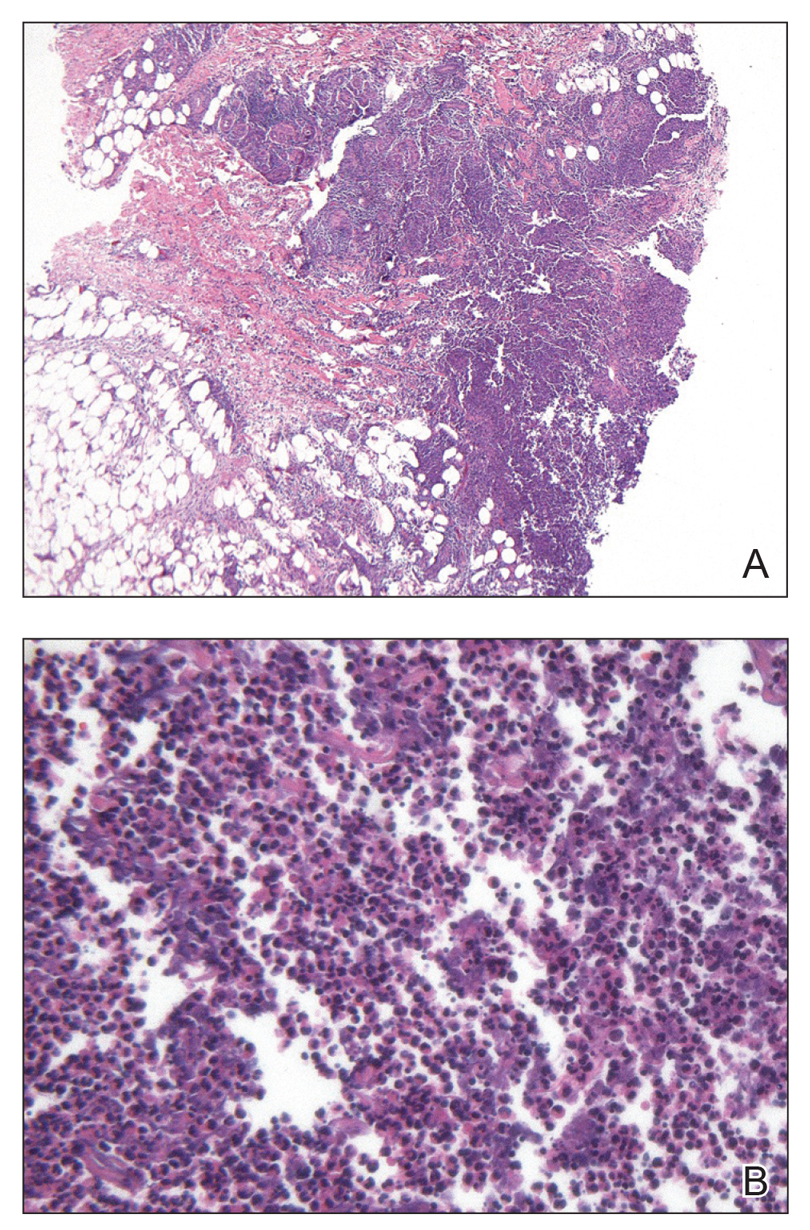
Eighteen days after obtaining the tissue culture, acid-fast organisms grew in culture. These organisms were subcultured on Middlebrook 7H11 agar (Sigma-Aldrich) with growth noted at 30°C and 37°C. Gram stain revealed filamentous gram-variable bacteria (Figure 2) that were identified as Nocardia brasiliensis by 16S ribosomal DNA analysis. Given the patient’s sulfonamide allergy, she started oral minocycline 100 mg twice daily. She responded to the therapy and subsequent testing confirmed susceptibility.
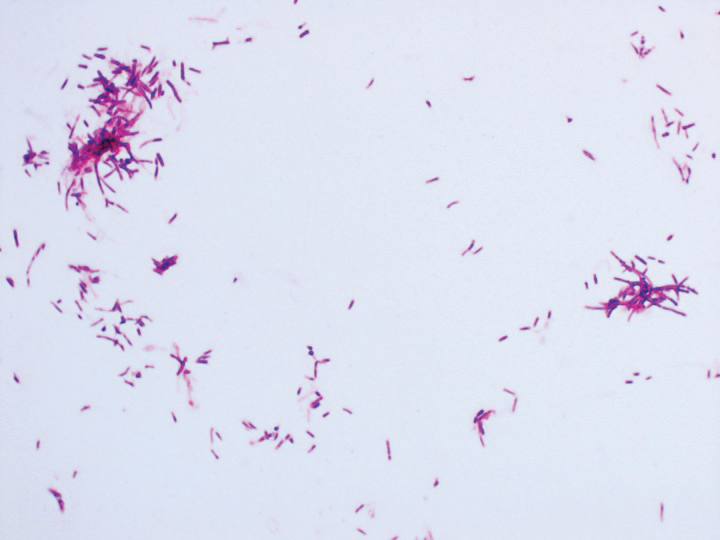
Nocardia brasiliensis, isolated from subculture on Gram stain (original
magnification ×1000).
The genus Nocardia consists of more than 50 species of gram-positive, weakly acid-fast, aerobic actinomycetes that can cause primary cutaneous infection via percutaneous inoculation. Nocardia brasiliensis is the leading cause (approximately 80% of cases) of primary cutaneous or subcutaneous nocardiosis and is found ubiquitously in soil and decaying vegetation.1 The clinical presentation varies, rendering definitive diagnosis a challenge without histopathologic and microbiologic testing.2 Patients presenting with nocardial cellulitis often are suspected to have Streptococcus pyogenes or Staphylococcus aureus infections. The differential diagnosis for patients presenting with nocardial nodular lymphangitis, also known as lymphocutaneous syndrome, includes atypical mycobacterial infections, leishmaniasis, and lymphocutaneous sporotrichosis.2
Histologic examination of nocardial nodules typically shows granulomatous or neutrophilic inflammation, and organisms may appear in small collections resembling sulfur granules.2 The organism itself is weakly positive on acid-fast stain, and useful stains include acid-fast bacteria, methenamine silver, and periodic acid–Schiff.2 Tissue culture often provides the definitive diagnosis, as the histology is nonspecific and organisms may not be visualized.
Oral trimethoprim-sulfamethoxazole 2.5 to 10 mg/kg and 12.5 to 50 mg/kg, respectively, twice daily is the treatment of choice for primary cutaneous nocardiosis. Minocycline 100 to 200 mg twice daily is an accepted alternative in case of sulfonamide allergy, as in our patient. Antibiotics should be tailored according to the susceptibility profile of the isolated organism.3
This case highlights the importance of forming a broad differential diagnosis for patients presenting with lymphocutaneous syndrome. The incidence and prevalence of N brasiliensis infection is difficult to determine due to its nonspecific clinical presentation and a lack of recent epidemiologic studies. Although primary cutaneous nocardiosis in the United States often is diagnosed in the South or Southwest, cases have been reported in other regions.4-6 Traumatic inoculation of contaminated soil, plants, and other organic matter, a well-known method of Sporothrix schenckii transmission, also is a method of N brasiliensis transmission. Because this organism may not be detected on histologic examination, empiric treatment should be considered if the diagnosis is suspected.
1. Brown-Eliot BA, Brown JM, Conville PS, et al. Clinical and laboratory features of the Nocardia spp. based on current molecular taxonomy. Clin Microbiol Rev. 2006;19:259-282.
2. Smego RA Jr, Castiglia M, Asperilla MO. Lymphocutaneous syndrome: a review of non-sporothrix causes. Medicine. 1999;78:38-63.
3. Lerner P. Nocardiosis. Clin Infect Dis. 1996;22:891-903.
4. Smego RA Jr, Gallis HA. The clinical spectrum of Nocardia brasiliensis infection in the United States. Rev Infect Dis. 1984;6:164-180.
5. Fukuda H, Saotome A, Usami N, et al. Lymphocutaneous type of nocardiosis caused by Nocardia brasiliensis: a case report and review of primary cutaneous nocardiosis caused by N. brasiliensis reported in Japan. J Dermatol. 2008;35:346-353.
6. Kil EH, Tsai CL, Kwark EH, et al. A case of nocardiosis with an uncharacteristically long incubation period. Cutis. 2005;76:33-36.
The Diagnosis: Primary Cutaneous Nocardiosis
Comprehensive metabolic panel and complete blood cell count were unremarkable; human immunodeficiency virus screening was nonreactive. Punch biopsies were obtained for histopathology, as well as bacterial, fungal, and mycobacterial cultures. Histopathologic examination of a 4-mm punch biopsy of the forearm nodule showed a dermal abscess with neutrophilic infiltration in the dermis (Figure 1). No organisms were seen on Gram, methenamine-silver, periodic acid–Schiff, or acid-fast bacteria stains. Given the clinical suspicion for lymphocutaneous sporotrichosis, the patient was started on itraconazole. She reported modest improvement but subsequently developed a morbilliform eruption necessitating medication discontinuation.
Eighteen days after obtaining the tissue culture, acid-fast organisms grew in culture. These organisms were subcultured on Middlebrook 7H11 agar (Sigma-Aldrich) with growth noted at 30°C and 37°C. Gram stain revealed filamentous gram-variable bacteria (Figure 2) that were identified as Nocardia brasiliensis by 16S ribosomal DNA analysis. Given the patient’s sulfonamide allergy, she started oral minocycline 100 mg twice daily. She responded to the therapy and subsequent testing confirmed susceptibility.
Nocardia brasiliensis, isolated from subculture on Gram stain (original
magnification ×1000).
The genus Nocardia consists of more than 50 species of gram-positive, weakly acid-fast, aerobic actinomycetes that can cause primary cutaneous infection via percutaneous inoculation. Nocardia brasiliensis is the leading cause (approximately 80% of cases) of primary cutaneous or subcutaneous nocardiosis and is found ubiquitously in soil and decaying vegetation.1 The clinical presentation varies, rendering definitive diagnosis a challenge without histopathologic and microbiologic testing.2 Patients presenting with nocardial cellulitis often are suspected to have Streptococcus pyogenes or Staphylococcus aureus infections. The differential diagnosis for patients presenting with nocardial nodular lymphangitis, also known as lymphocutaneous syndrome, includes atypical mycobacterial infections, leishmaniasis, and lymphocutaneous sporotrichosis.2
Histologic examination of nocardial nodules typically shows granulomatous or neutrophilic inflammation, and organisms may appear in small collections resembling sulfur granules.2 The organism itself is weakly positive on acid-fast stain, and useful stains include acid-fast bacteria, methenamine silver, and periodic acid–Schiff.2 Tissue culture often provides the definitive diagnosis, as the histology is nonspecific and organisms may not be visualized.
Oral trimethoprim-sulfamethoxazole 2.5 to 10 mg/kg and 12.5 to 50 mg/kg, respectively, twice daily is the treatment of choice for primary cutaneous nocardiosis. Minocycline 100 to 200 mg twice daily is an accepted alternative in case of sulfonamide allergy, as in our patient. Antibiotics should be tailored according to the susceptibility profile of the isolated organism.3
This case highlights the importance of forming a broad differential diagnosis for patients presenting with lymphocutaneous syndrome. The incidence and prevalence of N brasiliensis infection is difficult to determine due to its nonspecific clinical presentation and a lack of recent epidemiologic studies. Although primary cutaneous nocardiosis in the United States often is diagnosed in the South or Southwest, cases have been reported in other regions.4-6 Traumatic inoculation of contaminated soil, plants, and other organic matter, a well-known method of Sporothrix schenckii transmission, also is a method of N brasiliensis transmission. Because this organism may not be detected on histologic examination, empiric treatment should be considered if the diagnosis is suspected.
The Diagnosis: Primary Cutaneous Nocardiosis
Comprehensive metabolic panel and complete blood cell count were unremarkable; human immunodeficiency virus screening was nonreactive. Punch biopsies were obtained for histopathology, as well as bacterial, fungal, and mycobacterial cultures. Histopathologic examination of a 4-mm punch biopsy of the forearm nodule showed a dermal abscess with neutrophilic infiltration in the dermis (Figure 1). No organisms were seen on Gram, methenamine-silver, periodic acid–Schiff, or acid-fast bacteria stains. Given the clinical suspicion for lymphocutaneous sporotrichosis, the patient was started on itraconazole. She reported modest improvement but subsequently developed a morbilliform eruption necessitating medication discontinuation.
Eighteen days after obtaining the tissue culture, acid-fast organisms grew in culture. These organisms were subcultured on Middlebrook 7H11 agar (Sigma-Aldrich) with growth noted at 30°C and 37°C. Gram stain revealed filamentous gram-variable bacteria (Figure 2) that were identified as Nocardia brasiliensis by 16S ribosomal DNA analysis. Given the patient’s sulfonamide allergy, she started oral minocycline 100 mg twice daily. She responded to the therapy and subsequent testing confirmed susceptibility.
Nocardia brasiliensis, isolated from subculture on Gram stain (original
magnification ×1000).
The genus Nocardia consists of more than 50 species of gram-positive, weakly acid-fast, aerobic actinomycetes that can cause primary cutaneous infection via percutaneous inoculation. Nocardia brasiliensis is the leading cause (approximately 80% of cases) of primary cutaneous or subcutaneous nocardiosis and is found ubiquitously in soil and decaying vegetation.1 The clinical presentation varies, rendering definitive diagnosis a challenge without histopathologic and microbiologic testing.2 Patients presenting with nocardial cellulitis often are suspected to have Streptococcus pyogenes or Staphylococcus aureus infections. The differential diagnosis for patients presenting with nocardial nodular lymphangitis, also known as lymphocutaneous syndrome, includes atypical mycobacterial infections, leishmaniasis, and lymphocutaneous sporotrichosis.2
Histologic examination of nocardial nodules typically shows granulomatous or neutrophilic inflammation, and organisms may appear in small collections resembling sulfur granules.2 The organism itself is weakly positive on acid-fast stain, and useful stains include acid-fast bacteria, methenamine silver, and periodic acid–Schiff.2 Tissue culture often provides the definitive diagnosis, as the histology is nonspecific and organisms may not be visualized.
Oral trimethoprim-sulfamethoxazole 2.5 to 10 mg/kg and 12.5 to 50 mg/kg, respectively, twice daily is the treatment of choice for primary cutaneous nocardiosis. Minocycline 100 to 200 mg twice daily is an accepted alternative in case of sulfonamide allergy, as in our patient. Antibiotics should be tailored according to the susceptibility profile of the isolated organism.3
This case highlights the importance of forming a broad differential diagnosis for patients presenting with lymphocutaneous syndrome. The incidence and prevalence of N brasiliensis infection is difficult to determine due to its nonspecific clinical presentation and a lack of recent epidemiologic studies. Although primary cutaneous nocardiosis in the United States often is diagnosed in the South or Southwest, cases have been reported in other regions.4-6 Traumatic inoculation of contaminated soil, plants, and other organic matter, a well-known method of Sporothrix schenckii transmission, also is a method of N brasiliensis transmission. Because this organism may not be detected on histologic examination, empiric treatment should be considered if the diagnosis is suspected.
1. Brown-Eliot BA, Brown JM, Conville PS, et al. Clinical and laboratory features of the Nocardia spp. based on current molecular taxonomy. Clin Microbiol Rev. 2006;19:259-282.
2. Smego RA Jr, Castiglia M, Asperilla MO. Lymphocutaneous syndrome: a review of non-sporothrix causes. Medicine. 1999;78:38-63.
3. Lerner P. Nocardiosis. Clin Infect Dis. 1996;22:891-903.
4. Smego RA Jr, Gallis HA. The clinical spectrum of Nocardia brasiliensis infection in the United States. Rev Infect Dis. 1984;6:164-180.
5. Fukuda H, Saotome A, Usami N, et al. Lymphocutaneous type of nocardiosis caused by Nocardia brasiliensis: a case report and review of primary cutaneous nocardiosis caused by N. brasiliensis reported in Japan. J Dermatol. 2008;35:346-353.
6. Kil EH, Tsai CL, Kwark EH, et al. A case of nocardiosis with an uncharacteristically long incubation period. Cutis. 2005;76:33-36.
1. Brown-Eliot BA, Brown JM, Conville PS, et al. Clinical and laboratory features of the Nocardia spp. based on current molecular taxonomy. Clin Microbiol Rev. 2006;19:259-282.
2. Smego RA Jr, Castiglia M, Asperilla MO. Lymphocutaneous syndrome: a review of non-sporothrix causes. Medicine. 1999;78:38-63.
3. Lerner P. Nocardiosis. Clin Infect Dis. 1996;22:891-903.
4. Smego RA Jr, Gallis HA. The clinical spectrum of Nocardia brasiliensis infection in the United States. Rev Infect Dis. 1984;6:164-180.
5. Fukuda H, Saotome A, Usami N, et al. Lymphocutaneous type of nocardiosis caused by Nocardia brasiliensis: a case report and review of primary cutaneous nocardiosis caused by N. brasiliensis reported in Japan. J Dermatol. 2008;35:346-353.
6. Kil EH, Tsai CL, Kwark EH, et al. A case of nocardiosis with an uncharacteristically long incubation period. Cutis. 2005;76:33-36.

A 54-year-old woman called her primary care provider to report a painful pink nodule on the left wrist 1 week after sustaining thorn injuries while weeding in her garden. She started cephalexin and noted a pink streak with additional nodules extending up the arm over the next 2 days. She
was admitted to an outside hospital for incision and drainage of the wrist nodule and a 3-day course of intravenous vancomycin. Bacterial culture was negative, and she was discharged on oral clindamycin and doxycycline. Two days later, she presented to our emergency department with pain in the left axilla. Physical examination revealed 3 tender erythematous nodules in a linear distribution on the left arm with crusting at the incision and drainage site and painful left axillary lymphadenopathy. The patient was afebrile and otherwise asymptomatic.

Antidepressants tied to greater hip fracture incidence in older adults
Older patients in a Swedish registry who took antidepressants had a greater incidence of hip fracture the year before beginning antidepressant therapy and the year after starting therapy, compared with individuals in a matched control group.
The use of antidepressants is associated with adverse events such as a higher risk of falls, wrote Jon Brännström, MD, and his colleagues in JAMA Psychiatry. Some evidence also suggests that antidepressants “might affect bone metabolism, thereby increasing the risk of hip fracture.”
To examine the relationship between antidepressants and hip fracture, Dr. Brännström and his colleagues performed a nationwide cohort study of 204,072 individuals in the Prescribed Drug Register of Sweden’s National Board of Health and Welfare. All of the individuals were aged at least 65 years (mean age, 80.1 years; 63.1% women) and filled a prescription for an antidepressant between July 2006 and December 2011. Selective serotonin reuptake inhibitors made up 62.6% of the antidepressants used.
Patients who filled an antidepressant prescription during that time period were matched with a control group of individuals by birth year and gender and were studied the year before and after beginning antidepressant therapy.
In the year after initiating antidepressant therapy, there was a 3.5% incidence rate for hip fractures, compared with 1.3% in the control group.
After adjusting the results using a conditional logistic regression model, the highest rate of hip fracture among antidepressant users occurred between 16 days and 30 days prior to filling the prescription (odds ratio, 5.76; 95% confidence interval, 4.73-7.01); this association persisted in further subgroup analyses based on age, reported Dr. Brännström, who is affiliated with the department of community medicine and rehabilitation and geriatric medicine at Umeå University (Sweden), and his colleagues.
They noted that, although the study included all Swedish individuals who filled prescriptions for antidepressants during the study period, there is an absence of primary care comorbidity data and indications for antidepressant use. In addition, the definition of high- and low-medication doses does not always match what is considered high and low therapeutically and the information that can be gleaned from merging data from several different registries was limited.
“These findings raise questions about associations between antidepressant use and hip fracture seen in previous observational studies,” Dr. Brännström and his colleagues wrote. “Further analysis of this association in treatment studies and examination of the incidence of hip fracture before and after the discontinuation of treatment is required and may shed further light on the possible residual risk associated with treatment.”
This study was funded by the Swedish Research Council. The authors reported no relevant conflicts of interest.
SOURCE: Brännström J et al. JAMA Psychiatry. 2019 Jan 2. doi: 10.1001/jamapsychiatry.2018.3679.
In many cases where an adverse event is linked to a medication, such as in the case of gastrointestinal bleeds and blood thinners, the adverse event is not linked to the medication. However, this is not the case with antidepressants and hip fracture, Andrea Iaboni, MD, DPhil, and Donovan T. Maust, MD, wrote in a related editorial (JAMA Psychiatry. 2019 Jan 2. doi: 10.1001/jamapsychiatry.2018.3632).
“Patients are routinely prescribed antidepressants following a fracture,” the authors wrote, noting that depression can occur for patients who do not have a history of depression and can last as long as 1 year after hip fracture. The reasons for depression after hip fracture are possibly caused by the consequences of the event or a comorbid condition, such as cerebrovascular disease burden, cognitive impairment, frailty, and impaired functional status. In addition, new antidepressant prescriptions are 10 times the normal rate for older adults in the months after a hip fracture.
Many older users of antidepressants have a hip fracture event in their past, which could be caused by an untreated case of depression and an elevated risk of elevated fall or fracture, as suggested by Brännström et al., while other reasons could include off-label indications such as insomnia, poor motivation during rehabilitation therapy, pain, or hyperactive delirium.
“If individuals with untreated depression are at risk of falls and fractures, it follows that there would be an elevated rate of fractures before antidepressant use,” the authors wrote. “However, as discussed earlier, it is also important to recognize that, during the postfracture period, rightly or wrongly, antidepressants are prescribed at a high rate.”
Clinicians who treat these patients should not stop all antidepressant prescribing to this population. Instead, “a pragmatic preventive approach is warranted, starting with selecting the antidepressant, a cautious initial dose and dose-escalation schedule, a review of potentially interacting therapies ... and referral to fall prevention programs for patients with other risk factors for falls,” they wrote.
“For most older adults, the toll of untreated depression will likely outweigh the potential risks associated with antidepressant use.”
Dr. Iabroni is with the Toronto Rehabilitation Institute and the University of Toronto. He reported receiving fees from serving as a scientific adviser for Winterlight Labs. Dr. Maust is with the department of psychiatry at the University of Michigan, Ann Arbor. He reported no relevant conflicts of interest.
In many cases where an adverse event is linked to a medication, such as in the case of gastrointestinal bleeds and blood thinners, the adverse event is not linked to the medication. However, this is not the case with antidepressants and hip fracture, Andrea Iaboni, MD, DPhil, and Donovan T. Maust, MD, wrote in a related editorial (JAMA Psychiatry. 2019 Jan 2. doi: 10.1001/jamapsychiatry.2018.3632).
“Patients are routinely prescribed antidepressants following a fracture,” the authors wrote, noting that depression can occur for patients who do not have a history of depression and can last as long as 1 year after hip fracture. The reasons for depression after hip fracture are possibly caused by the consequences of the event or a comorbid condition, such as cerebrovascular disease burden, cognitive impairment, frailty, and impaired functional status. In addition, new antidepressant prescriptions are 10 times the normal rate for older adults in the months after a hip fracture.
Many older users of antidepressants have a hip fracture event in their past, which could be caused by an untreated case of depression and an elevated risk of elevated fall or fracture, as suggested by Brännström et al., while other reasons could include off-label indications such as insomnia, poor motivation during rehabilitation therapy, pain, or hyperactive delirium.
“If individuals with untreated depression are at risk of falls and fractures, it follows that there would be an elevated rate of fractures before antidepressant use,” the authors wrote. “However, as discussed earlier, it is also important to recognize that, during the postfracture period, rightly or wrongly, antidepressants are prescribed at a high rate.”
Clinicians who treat these patients should not stop all antidepressant prescribing to this population. Instead, “a pragmatic preventive approach is warranted, starting with selecting the antidepressant, a cautious initial dose and dose-escalation schedule, a review of potentially interacting therapies ... and referral to fall prevention programs for patients with other risk factors for falls,” they wrote.
“For most older adults, the toll of untreated depression will likely outweigh the potential risks associated with antidepressant use.”
Dr. Iabroni is with the Toronto Rehabilitation Institute and the University of Toronto. He reported receiving fees from serving as a scientific adviser for Winterlight Labs. Dr. Maust is with the department of psychiatry at the University of Michigan, Ann Arbor. He reported no relevant conflicts of interest.
In many cases where an adverse event is linked to a medication, such as in the case of gastrointestinal bleeds and blood thinners, the adverse event is not linked to the medication. However, this is not the case with antidepressants and hip fracture, Andrea Iaboni, MD, DPhil, and Donovan T. Maust, MD, wrote in a related editorial (JAMA Psychiatry. 2019 Jan 2. doi: 10.1001/jamapsychiatry.2018.3632).
“Patients are routinely prescribed antidepressants following a fracture,” the authors wrote, noting that depression can occur for patients who do not have a history of depression and can last as long as 1 year after hip fracture. The reasons for depression after hip fracture are possibly caused by the consequences of the event or a comorbid condition, such as cerebrovascular disease burden, cognitive impairment, frailty, and impaired functional status. In addition, new antidepressant prescriptions are 10 times the normal rate for older adults in the months after a hip fracture.
Many older users of antidepressants have a hip fracture event in their past, which could be caused by an untreated case of depression and an elevated risk of elevated fall or fracture, as suggested by Brännström et al., while other reasons could include off-label indications such as insomnia, poor motivation during rehabilitation therapy, pain, or hyperactive delirium.
“If individuals with untreated depression are at risk of falls and fractures, it follows that there would be an elevated rate of fractures before antidepressant use,” the authors wrote. “However, as discussed earlier, it is also important to recognize that, during the postfracture period, rightly or wrongly, antidepressants are prescribed at a high rate.”
Clinicians who treat these patients should not stop all antidepressant prescribing to this population. Instead, “a pragmatic preventive approach is warranted, starting with selecting the antidepressant, a cautious initial dose and dose-escalation schedule, a review of potentially interacting therapies ... and referral to fall prevention programs for patients with other risk factors for falls,” they wrote.
“For most older adults, the toll of untreated depression will likely outweigh the potential risks associated with antidepressant use.”
Dr. Iabroni is with the Toronto Rehabilitation Institute and the University of Toronto. He reported receiving fees from serving as a scientific adviser for Winterlight Labs. Dr. Maust is with the department of psychiatry at the University of Michigan, Ann Arbor. He reported no relevant conflicts of interest.
Older patients in a Swedish registry who took antidepressants had a greater incidence of hip fracture the year before beginning antidepressant therapy and the year after starting therapy, compared with individuals in a matched control group.
The use of antidepressants is associated with adverse events such as a higher risk of falls, wrote Jon Brännström, MD, and his colleagues in JAMA Psychiatry. Some evidence also suggests that antidepressants “might affect bone metabolism, thereby increasing the risk of hip fracture.”
To examine the relationship between antidepressants and hip fracture, Dr. Brännström and his colleagues performed a nationwide cohort study of 204,072 individuals in the Prescribed Drug Register of Sweden’s National Board of Health and Welfare. All of the individuals were aged at least 65 years (mean age, 80.1 years; 63.1% women) and filled a prescription for an antidepressant between July 2006 and December 2011. Selective serotonin reuptake inhibitors made up 62.6% of the antidepressants used.
Patients who filled an antidepressant prescription during that time period were matched with a control group of individuals by birth year and gender and were studied the year before and after beginning antidepressant therapy.
In the year after initiating antidepressant therapy, there was a 3.5% incidence rate for hip fractures, compared with 1.3% in the control group.
After adjusting the results using a conditional logistic regression model, the highest rate of hip fracture among antidepressant users occurred between 16 days and 30 days prior to filling the prescription (odds ratio, 5.76; 95% confidence interval, 4.73-7.01); this association persisted in further subgroup analyses based on age, reported Dr. Brännström, who is affiliated with the department of community medicine and rehabilitation and geriatric medicine at Umeå University (Sweden), and his colleagues.
They noted that, although the study included all Swedish individuals who filled prescriptions for antidepressants during the study period, there is an absence of primary care comorbidity data and indications for antidepressant use. In addition, the definition of high- and low-medication doses does not always match what is considered high and low therapeutically and the information that can be gleaned from merging data from several different registries was limited.
“These findings raise questions about associations between antidepressant use and hip fracture seen in previous observational studies,” Dr. Brännström and his colleagues wrote. “Further analysis of this association in treatment studies and examination of the incidence of hip fracture before and after the discontinuation of treatment is required and may shed further light on the possible residual risk associated with treatment.”
This study was funded by the Swedish Research Council. The authors reported no relevant conflicts of interest.
SOURCE: Brännström J et al. JAMA Psychiatry. 2019 Jan 2. doi: 10.1001/jamapsychiatry.2018.3679.
Older patients in a Swedish registry who took antidepressants had a greater incidence of hip fracture the year before beginning antidepressant therapy and the year after starting therapy, compared with individuals in a matched control group.
The use of antidepressants is associated with adverse events such as a higher risk of falls, wrote Jon Brännström, MD, and his colleagues in JAMA Psychiatry. Some evidence also suggests that antidepressants “might affect bone metabolism, thereby increasing the risk of hip fracture.”
To examine the relationship between antidepressants and hip fracture, Dr. Brännström and his colleagues performed a nationwide cohort study of 204,072 individuals in the Prescribed Drug Register of Sweden’s National Board of Health and Welfare. All of the individuals were aged at least 65 years (mean age, 80.1 years; 63.1% women) and filled a prescription for an antidepressant between July 2006 and December 2011. Selective serotonin reuptake inhibitors made up 62.6% of the antidepressants used.
Patients who filled an antidepressant prescription during that time period were matched with a control group of individuals by birth year and gender and were studied the year before and after beginning antidepressant therapy.
In the year after initiating antidepressant therapy, there was a 3.5% incidence rate for hip fractures, compared with 1.3% in the control group.
After adjusting the results using a conditional logistic regression model, the highest rate of hip fracture among antidepressant users occurred between 16 days and 30 days prior to filling the prescription (odds ratio, 5.76; 95% confidence interval, 4.73-7.01); this association persisted in further subgroup analyses based on age, reported Dr. Brännström, who is affiliated with the department of community medicine and rehabilitation and geriatric medicine at Umeå University (Sweden), and his colleagues.
They noted that, although the study included all Swedish individuals who filled prescriptions for antidepressants during the study period, there is an absence of primary care comorbidity data and indications for antidepressant use. In addition, the definition of high- and low-medication doses does not always match what is considered high and low therapeutically and the information that can be gleaned from merging data from several different registries was limited.
“These findings raise questions about associations between antidepressant use and hip fracture seen in previous observational studies,” Dr. Brännström and his colleagues wrote. “Further analysis of this association in treatment studies and examination of the incidence of hip fracture before and after the discontinuation of treatment is required and may shed further light on the possible residual risk associated with treatment.”
This study was funded by the Swedish Research Council. The authors reported no relevant conflicts of interest.
SOURCE: Brännström J et al. JAMA Psychiatry. 2019 Jan 2. doi: 10.1001/jamapsychiatry.2018.3679.
FROM JAMA PSYCHIATRY
Key clinical point: An association was found between greater hip fracture incidence for older individuals taking antidepressants in the year before beginning therapy and the year after starting therapy.
Major finding: Individuals who took antidepressants had a greater incidence of hip fractures in the year before (2.8% vs. 1.1%) and the year after (3.5% vs. 1.3%) beginning antidepressants, compared with individuals in a matched control group.
Study details: A nationwide cohort study of 408,144 individuals in the Prescribed Drugs Register of Sweden’s National Board of Health and Welfare who were aged 65 years or older.
Disclosures: This study was funded by the Swedish Research Council. The authors reported no relevant conflicts of interest.
Source: Brännström J et al. JAMA Psychiatry. 2019 Jan 2. doi: 10.1001/jamapsychiatry.2018.3679.