User login
Team Hospitalist at Work for you
A team of a dozen hospitalist experts has joined forces with The Hospitalist to provide our readers exclusive insights into the critical issues facing hospital medicine.
Team Hospitalist comprises a diverse array of hospital medicine talent by region, specialty, and experience. The team was selected late last year from a pool of more than two dozen candidates, and each member will serve a two-year term.
Meet Team Hospitalist

R. Neal Axon, MD, assistant professor, medicine and pediatrics, Medical University of South Carolina, Charleston

Brian Bossard, MD, director, Inpatient Physician Associates, Lincoln, Neb.

Maj. Heather Cereste, MD, MC, codirector, geriatric medicine service, assistant professor, Uniformed Services University of the Health Sciences, Bethesda, Md.; internist and chairperson, Bioethics Committee, Wilford Hall Medical Center, Lackland Air Force Base, San Antonio, Texas

Randy Ferrance, DC, MC, internal medicine and pediatrics medical director, Riverside Tappahannock Hospice, Riverside Tappahannock Hospital, Va.

William T. Ford, MD, program medical director, Cogent Healthcare; chief, section of hospital medicine, Temple University, Philadelphia

David Grace, MD, area medical officer, The Schumacher Group Hospital Medicine Division, Lafayette, La.

Kenneth Patrick, MD, intensive-care unit director, Chestnut Hill Hospital, Philadelphia

Richard Rohr, MD, vice president for medical affairs, Cortland Regional Medical Center, Cortland, N.Y.

Sandeep Sachdeva, MD, FAHA, director, hospitalist services, Banner Gateway Medical Center, Gilbert, Ariz.

Matthew Szvetecz, MD, director, Division of Internal Medicine, Kadlec Medical Associates, Richland, Wash.

Julia Wright, MD, clinical associate professor of medicine, University of Wisconsin Hospitals and Clinics; associate clinical professor of medicine and director of hospital medicine, University of Wisconsin School of Medicine and Public Health, Madison

David Yu, MD, FACP, medical director of hospitalist services, Decatur Memorial Hospital; clinical assistant professor, family and community medicine, Southern Illinois University, School of Medicine
Team members will share their professional expertise on a regular basis within the pages of The Hospitalist and on our Web site (www.the-hospitalist.org) via blogs and discussion rooms. The team’s contributions will range from being tapped as sources for stories to sharing short accounts of their experiences relating to topics they are intimately familiar with.
Advancing the mission of hospital medicine is at the core of why team members say they desire to participate on this unique panel.
“Physicians practicing hospital medicine over the next couple of years must remember that providing excellent care to our patients remains our highest priority,” says Ken Patrick, MD, director of the intensive-care unit at Chestnut Hill Hospital in Philadelphia. “Being compassionate, empathetic, and communicating effectively to our patients, their families, and their primary care physicians can be exceedingly difficult in the stressful hospital environment. Having been trained in both primary care and critical care medicine and practiced hospital medicine for more than 25 years remind me just how vitally important this is for our profession.”
Nuts-and-bolts issues like funding, technology, research, and quality standards are uppermost on these experts’ minds.
Specializing in electronic medical technology and progressive scheduling, David J. Yu, MD, hopes to share his approaches to innovating hospital medicine. “Hospitalist programs will encounter more difficult problems … which will require medical directors to forego traditional and exhausted methods of practice,” says Dr. Yu, medical director of hospitalist services, Decatur Memorial Hospital, and clinical assistant professor, family and community medicine, Southern Illinois University, School of Medicine. “I hope to share my experiences in creating innovative approaches to scheduling and our creative use of electronic medical technology to advance the art of hospital medicine into the 21st century.”
The evolution of hospital medicine presents opportunities—and risks—says Rajeev Alexander, MD, lead hospitalist, Oregon Medical Group, Eugene, Ore.
“I enjoy the intellectual challenge hospitalist medicine presents, the range of pathologies and sorts of problems we’re asked about—everything from intensive care work to end-of-life care,” he says. “I would like to see hospitalist medicine evolve an identity along the lines of emergency medicine and/or anesthesia.” However, he fears hospitalists could be seen as, or become, either “physicians with a rapid turnover and without ties to the community who treat the position as a mere stepping stone before a higher-paying specialty fellowship, or ... overgrown house officers who, because of their status as employed physicians, are seen as fungible by hospital administrators.”
But the buck should stop with hospitalists when it comes to improving care quality, says Randy Ferrance, DC, MC, internal medicine and pediatrics medical director, Riverside Tappahannock Hospice, Riverside Tappahannock Hospital, Va.
“So many outside forces are working to constrain medicine in so many ways, I am hoping that we … can come together to so thoroughly and definitively improve the quality of our care that those outside agencies will feel comfortable stepping back and interfering less in how we practice,” says Dr. Ferrance.
When it comes to research, hospitalists could be in the driver’s seat, says R. Neal Axon, MD, assistant professor, medicine and pediatrics, Medical University of South Carolina, Charleston.
“The [National Institutes of Health] and the academic institutions who count on NIH funding have focused a great deal of publicity in recent years on ‘translational’ research that is supposed to move scientific discovery from the bench more expeditiously to the bedside,” Dr. Axon says. “Increasingly, hospitalists are the doctors at the bedside, and I see a huge opportunity for our specialty to both perform research and to set a relevant research agenda over the next several years.”
The bottom line is that hospitalists must focus on achieving three things, says Julia Wright, MD, associate clinical professor of medicine and director of hospital medicine, University of Wisconsin School of Medicine and Public Health, Madison. Her priorities are establishing hospital medicine as a specialty, creating uniform standards for hospitalists, and excelling in patient care and care-delivery systems. TH
Geoff Giordano is editor of The Hospitalist.
A team of a dozen hospitalist experts has joined forces with The Hospitalist to provide our readers exclusive insights into the critical issues facing hospital medicine.
Team Hospitalist comprises a diverse array of hospital medicine talent by region, specialty, and experience. The team was selected late last year from a pool of more than two dozen candidates, and each member will serve a two-year term.
Meet Team Hospitalist
R. Neal Axon, MD, assistant professor, medicine and pediatrics, Medical University of South Carolina, Charleston
Brian Bossard, MD, director, Inpatient Physician Associates, Lincoln, Neb.
Maj. Heather Cereste, MD, MC, codirector, geriatric medicine service, assistant professor, Uniformed Services University of the Health Sciences, Bethesda, Md.; internist and chairperson, Bioethics Committee, Wilford Hall Medical Center, Lackland Air Force Base, San Antonio, Texas
Randy Ferrance, DC, MC, internal medicine and pediatrics medical director, Riverside Tappahannock Hospice, Riverside Tappahannock Hospital, Va.
William T. Ford, MD, program medical director, Cogent Healthcare; chief, section of hospital medicine, Temple University, Philadelphia
David Grace, MD, area medical officer, The Schumacher Group Hospital Medicine Division, Lafayette, La.
Kenneth Patrick, MD, intensive-care unit director, Chestnut Hill Hospital, Philadelphia
Richard Rohr, MD, vice president for medical affairs, Cortland Regional Medical Center, Cortland, N.Y.
Sandeep Sachdeva, MD, FAHA, director, hospitalist services, Banner Gateway Medical Center, Gilbert, Ariz.
Matthew Szvetecz, MD, director, Division of Internal Medicine, Kadlec Medical Associates, Richland, Wash.
Julia Wright, MD, clinical associate professor of medicine, University of Wisconsin Hospitals and Clinics; associate clinical professor of medicine and director of hospital medicine, University of Wisconsin School of Medicine and Public Health, Madison
David Yu, MD, FACP, medical director of hospitalist services, Decatur Memorial Hospital; clinical assistant professor, family and community medicine, Southern Illinois University, School of Medicine
Team members will share their professional expertise on a regular basis within the pages of The Hospitalist and on our Web site (www.the-hospitalist.org) via blogs and discussion rooms. The team’s contributions will range from being tapped as sources for stories to sharing short accounts of their experiences relating to topics they are intimately familiar with.
Advancing the mission of hospital medicine is at the core of why team members say they desire to participate on this unique panel.
“Physicians practicing hospital medicine over the next couple of years must remember that providing excellent care to our patients remains our highest priority,” says Ken Patrick, MD, director of the intensive-care unit at Chestnut Hill Hospital in Philadelphia. “Being compassionate, empathetic, and communicating effectively to our patients, their families, and their primary care physicians can be exceedingly difficult in the stressful hospital environment. Having been trained in both primary care and critical care medicine and practiced hospital medicine for more than 25 years remind me just how vitally important this is for our profession.”
Nuts-and-bolts issues like funding, technology, research, and quality standards are uppermost on these experts’ minds.
Specializing in electronic medical technology and progressive scheduling, David J. Yu, MD, hopes to share his approaches to innovating hospital medicine. “Hospitalist programs will encounter more difficult problems … which will require medical directors to forego traditional and exhausted methods of practice,” says Dr. Yu, medical director of hospitalist services, Decatur Memorial Hospital, and clinical assistant professor, family and community medicine, Southern Illinois University, School of Medicine. “I hope to share my experiences in creating innovative approaches to scheduling and our creative use of electronic medical technology to advance the art of hospital medicine into the 21st century.”
The evolution of hospital medicine presents opportunities—and risks—says Rajeev Alexander, MD, lead hospitalist, Oregon Medical Group, Eugene, Ore.
“I enjoy the intellectual challenge hospitalist medicine presents, the range of pathologies and sorts of problems we’re asked about—everything from intensive care work to end-of-life care,” he says. “I would like to see hospitalist medicine evolve an identity along the lines of emergency medicine and/or anesthesia.” However, he fears hospitalists could be seen as, or become, either “physicians with a rapid turnover and without ties to the community who treat the position as a mere stepping stone before a higher-paying specialty fellowship, or ... overgrown house officers who, because of their status as employed physicians, are seen as fungible by hospital administrators.”
But the buck should stop with hospitalists when it comes to improving care quality, says Randy Ferrance, DC, MC, internal medicine and pediatrics medical director, Riverside Tappahannock Hospice, Riverside Tappahannock Hospital, Va.
“So many outside forces are working to constrain medicine in so many ways, I am hoping that we … can come together to so thoroughly and definitively improve the quality of our care that those outside agencies will feel comfortable stepping back and interfering less in how we practice,” says Dr. Ferrance.
When it comes to research, hospitalists could be in the driver’s seat, says R. Neal Axon, MD, assistant professor, medicine and pediatrics, Medical University of South Carolina, Charleston.
“The [National Institutes of Health] and the academic institutions who count on NIH funding have focused a great deal of publicity in recent years on ‘translational’ research that is supposed to move scientific discovery from the bench more expeditiously to the bedside,” Dr. Axon says. “Increasingly, hospitalists are the doctors at the bedside, and I see a huge opportunity for our specialty to both perform research and to set a relevant research agenda over the next several years.”
The bottom line is that hospitalists must focus on achieving three things, says Julia Wright, MD, associate clinical professor of medicine and director of hospital medicine, University of Wisconsin School of Medicine and Public Health, Madison. Her priorities are establishing hospital medicine as a specialty, creating uniform standards for hospitalists, and excelling in patient care and care-delivery systems. TH
Geoff Giordano is editor of The Hospitalist.
A team of a dozen hospitalist experts has joined forces with The Hospitalist to provide our readers exclusive insights into the critical issues facing hospital medicine.
Team Hospitalist comprises a diverse array of hospital medicine talent by region, specialty, and experience. The team was selected late last year from a pool of more than two dozen candidates, and each member will serve a two-year term.
Meet Team Hospitalist
R. Neal Axon, MD, assistant professor, medicine and pediatrics, Medical University of South Carolina, Charleston
Brian Bossard, MD, director, Inpatient Physician Associates, Lincoln, Neb.
Maj. Heather Cereste, MD, MC, codirector, geriatric medicine service, assistant professor, Uniformed Services University of the Health Sciences, Bethesda, Md.; internist and chairperson, Bioethics Committee, Wilford Hall Medical Center, Lackland Air Force Base, San Antonio, Texas
Randy Ferrance, DC, MC, internal medicine and pediatrics medical director, Riverside Tappahannock Hospice, Riverside Tappahannock Hospital, Va.
William T. Ford, MD, program medical director, Cogent Healthcare; chief, section of hospital medicine, Temple University, Philadelphia
David Grace, MD, area medical officer, The Schumacher Group Hospital Medicine Division, Lafayette, La.
Kenneth Patrick, MD, intensive-care unit director, Chestnut Hill Hospital, Philadelphia
Richard Rohr, MD, vice president for medical affairs, Cortland Regional Medical Center, Cortland, N.Y.
Sandeep Sachdeva, MD, FAHA, director, hospitalist services, Banner Gateway Medical Center, Gilbert, Ariz.
Matthew Szvetecz, MD, director, Division of Internal Medicine, Kadlec Medical Associates, Richland, Wash.
Julia Wright, MD, clinical associate professor of medicine, University of Wisconsin Hospitals and Clinics; associate clinical professor of medicine and director of hospital medicine, University of Wisconsin School of Medicine and Public Health, Madison
David Yu, MD, FACP, medical director of hospitalist services, Decatur Memorial Hospital; clinical assistant professor, family and community medicine, Southern Illinois University, School of Medicine
Team members will share their professional expertise on a regular basis within the pages of The Hospitalist and on our Web site (www.the-hospitalist.org) via blogs and discussion rooms. The team’s contributions will range from being tapped as sources for stories to sharing short accounts of their experiences relating to topics they are intimately familiar with.
Advancing the mission of hospital medicine is at the core of why team members say they desire to participate on this unique panel.
“Physicians practicing hospital medicine over the next couple of years must remember that providing excellent care to our patients remains our highest priority,” says Ken Patrick, MD, director of the intensive-care unit at Chestnut Hill Hospital in Philadelphia. “Being compassionate, empathetic, and communicating effectively to our patients, their families, and their primary care physicians can be exceedingly difficult in the stressful hospital environment. Having been trained in both primary care and critical care medicine and practiced hospital medicine for more than 25 years remind me just how vitally important this is for our profession.”
Nuts-and-bolts issues like funding, technology, research, and quality standards are uppermost on these experts’ minds.
Specializing in electronic medical technology and progressive scheduling, David J. Yu, MD, hopes to share his approaches to innovating hospital medicine. “Hospitalist programs will encounter more difficult problems … which will require medical directors to forego traditional and exhausted methods of practice,” says Dr. Yu, medical director of hospitalist services, Decatur Memorial Hospital, and clinical assistant professor, family and community medicine, Southern Illinois University, School of Medicine. “I hope to share my experiences in creating innovative approaches to scheduling and our creative use of electronic medical technology to advance the art of hospital medicine into the 21st century.”
The evolution of hospital medicine presents opportunities—and risks—says Rajeev Alexander, MD, lead hospitalist, Oregon Medical Group, Eugene, Ore.
“I enjoy the intellectual challenge hospitalist medicine presents, the range of pathologies and sorts of problems we’re asked about—everything from intensive care work to end-of-life care,” he says. “I would like to see hospitalist medicine evolve an identity along the lines of emergency medicine and/or anesthesia.” However, he fears hospitalists could be seen as, or become, either “physicians with a rapid turnover and without ties to the community who treat the position as a mere stepping stone before a higher-paying specialty fellowship, or ... overgrown house officers who, because of their status as employed physicians, are seen as fungible by hospital administrators.”
But the buck should stop with hospitalists when it comes to improving care quality, says Randy Ferrance, DC, MC, internal medicine and pediatrics medical director, Riverside Tappahannock Hospice, Riverside Tappahannock Hospital, Va.
“So many outside forces are working to constrain medicine in so many ways, I am hoping that we … can come together to so thoroughly and definitively improve the quality of our care that those outside agencies will feel comfortable stepping back and interfering less in how we practice,” says Dr. Ferrance.
When it comes to research, hospitalists could be in the driver’s seat, says R. Neal Axon, MD, assistant professor, medicine and pediatrics, Medical University of South Carolina, Charleston.
“The [National Institutes of Health] and the academic institutions who count on NIH funding have focused a great deal of publicity in recent years on ‘translational’ research that is supposed to move scientific discovery from the bench more expeditiously to the bedside,” Dr. Axon says. “Increasingly, hospitalists are the doctors at the bedside, and I see a huge opportunity for our specialty to both perform research and to set a relevant research agenda over the next several years.”
The bottom line is that hospitalists must focus on achieving three things, says Julia Wright, MD, associate clinical professor of medicine and director of hospital medicine, University of Wisconsin School of Medicine and Public Health, Madison. Her priorities are establishing hospital medicine as a specialty, creating uniform standards for hospitalists, and excelling in patient care and care-delivery systems. TH
Geoff Giordano is editor of The Hospitalist.
The STAR*D study: Treating depression in the real world
Depression can be treated successfully by primary care physicians under “real-world” conditions.
Furthermore, the particular drug or drugs used are not as important as following a rational plan: giving antidepressant medications in adequate doses, monitoring the patient’s symptoms and side effects and adjusting the regimen accordingly, and switching drugs or adding new drugs to the regimen only after an adequate trial.
These are among the lessons learned from the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study, the largest prospective clinical trial of treatment of major depressive disorder ever conducted. It was funded by the National Institutes of Health and directed by A. John Rush, MD.
WHAT WERE THE AIMS OF STAR*D?
Depression, a common and debilitating condition, affects approximately one in eight people in the United States.1 It is expected2 to be the second-leading cause of disability in the world by the year 2020; today, it is the second-leading cause of disability-adjusted life years in those 15 to 44 years old.3
Nevertheless, the available evidence base for treatment is limited, since most participants in clinical trials are recruited by advertisement rather than from representative practices, and they are often selected to have few comorbid disorders, either medical or psychiatric. In addition, those with chronic depression or current suicidal ideation are excluded.1,4 These uncomplicated and “pristine” participants are unlike typical patients seen by primary care physicians or psychiatrists.
Similarly, the protocols used in these trials do not represent usual clinic practice.Patients in clinical trials undergo more assessment and more frequent follow-up than in real-world practice, they have no say in treatment decisions, the doses are fixed, and the patients and physicians are blinded to the intervention. Consequently, how to translate the results of these efficacy trials into practice is unclear.5
Further, even in relatively uncomplicated cases, only about one-half of outpatients with nonpsychotic major depressive disorder initially treated with a single medication or with psychotherapy will experience a clinically significant improvement in symptoms (ie, a response) during the 8 to 12 weeks of acute-phase treatment,6–10 and only 20% to 35% of patients will reach remission,9 the aim of treatment.8,11 The remission rates are even lower in treatment-resistant depression.12 How to manage most patients—those whose depression does not remit with the first, second, or third step of treatment—is unclear.
Accordingly, the overall objective of STAR*D was to develop and evaluate feasible treatment strategies to improve clinical outcomes for real-world patients with treatment-resistant depression, who were identified prospectively from a pool of patients in a current major depressive episode.13–15 Specifically, STAR*D aimed to determine prospectively which of several treatments is the most effective “next step” for patients who do not reach remission with an initial or subsequent treatment or who cannot tolerate the treatment.
WHY IS STAR*D RELEVANT FOR PRIMARY CARE?
Nearly 10% of all primary care office visits are depression-related.16 Primary care physicians provide nearly half the outpatient care for depressed patients.17 Indeed, primary care physicians log approximately as many outpatient visits for depression as psychiatrists do.18 Medical comorbidity is especially common in primary care settings.19 When to refer to a psychiatrist is not clear.
KEY FEATURES OF THE STUDY DESIGN
STAR*D involved a national consortium of 14 university-based regional centers, which oversaw a total of 23 participating psychiatric and 18 primary care clinics. Enrollment began in 2000, with follow-up completed in 2004.
Entry criteria were broad and inclusive
Patients had to:
- Be between 18 and 75 years of age
- Have a nonpsychotic major depressive disorder, identified by a clinician and confirmed with a symptom checklist based on the Diagnostic and Statistical Manual, fourth edition revised,20 and for which antidepressant treatment is recommended
- Score at least 14 on the 17-item Hamilton Rating Scale for Depression (HAMD17)21
- Not have a primary diagnosis of bipolar disorder, obsessive-compulsive disorder, or an eating disorder, which would require a different treatment strategy, or a seizure disorder (which would preclude bupropion as a second-step treatment).
Dosing recommendations were flexible but vigorous
Medications often were increased to maximally tolerated doses. For example, citalopram (Celexa) was started at 20 mg/day and increased by 20 mg every 2 to 4 weeks if the patient was tolerating it but had not achieved remission, to a maximum dose of 60 mg/day. Treatment could be given for up to 14 weeks, during which side effects22 and clinical ratings23 were assessed by both patients and study coordinators.
Measurement-based care
We used a systematic approach to treatment called “measurement-based care,”24 which involves routinely measuring symptoms23 and side effects22 and using this information to modify the medication doses at critical decision points. This algorithmic approach provided flexible treatment recommendations to ensure that the dosage and duration of antidepressant drug treatment were adequate.25
The severity of depression was assessed by the clinician-rated, 16-item Quick Inventory of Depressive Symptomatology (QIDS-C16). The QIDS-SR16 (the self-report version) can substitute for the QIDS-C1623 to make this approach more feasible. Both tools are available at www.ids-qids.org.
This approach was easily worked into busy primary care and specialty care office workflows (clinic physicians, most with limited research experience, provided the treatment), and could be translated into primary care practice in the community as well.
Four-step protocol
A unique feature of the study design was that the patients, in consultation with their physicians, had some choice in the treatments they received. In this “equipoise-stratified randomized design,”26 at levels 2 and 3 the patient could choose either to switch therapies (stop the current drug and be randomized to receive one of several different treatments) or to augment their current therapy (by adding one of several treatments in a randomized fashion). Patients could decline certain strategies as long as there were at least two possible options to which one might be randomized.
At level 2, one of the options for both switching and augmentation was cognitive therapy, although patients could decline that option. Conversely, if they definitely wanted cognitive therapy, they could choose to be randomized to either cognitive therapy alone or to cognitive therapy added to citalopram. Also, anyone who received cognitive therapy in level 2 and failed to enter remission was additionally randomized to either bupropion or venlafaxine (level 2a) to ensure that all patients had failed trials on two medications before entering level 3.
When switching to medications other than a monoamine oxidase inhibitor (MAOI), the clinician could choose either to stop the current medication and immediately begin the next one, or to decrease the current medication while starting the new one at a low dose and then tapering and titrating over 1 week. (Switching to an MAOI, used only in the final level of treatment, required a 7- to 10-day washout period.)
Outcomes measured
Remission (complete recovery from the depressive episode), the primary study outcome, was defined as a HAM-D17 score of 7 or less, as assessed by treatment-blinded raters.A secondary remission outcome was a QIDS-SR16 score of 5 or less. Of note, the HAM-D17 remission rates were slightly lower than the rates based on the QIDS-SR16, since patients who did not have a HAM-D17 score measured at exit were defined as not being in remission a priori. Thus, the QIDS-SR16 rates might have been a slightly better reflection of actual remission rates.
Response, a secondary outcome, was defined as a reduction of at least 50% in the QIDS-SR16 score from baseline at the last assessment.
FEW DIFFERENCES BETWEEN PSYCHIATRIC, PRIMARY CARE PATIENTS
The patients seen in primary care clinics were surprisingly similar to those seen in psychiatric clinics.27,28 The two groups did not differ in severity of depression, distribution of severity scores, the likelihood of presenting with any of the nine core criteria of a major depressive episode, or the likelihood of having a concomitant axis I psychiatric disorder in addition to depression (about half of participants in each setting had an anxiety disorder).
Recurrent major depressive disorders were common in both groups, though more so in psychiatric patients (78% vs 69%, P < .001), while chronic depression was more common in primary care than in psychiatric patients (30% vs 21%, P < .001). Having either a chronic index episode (ie, lasting > 2 years) or a recurrent major depressive disorder was common in both groups (86% vs 83%, P = .0067).
That said, primary care patients were older (44 years vs 39 years, P < .001), more of them were Hispanic (18% vs 9%, P < .001), and more of them had public insurance (23% vs 9%, P < .001). Fewer of the primary care patients had completed college (20% vs 28%, P < .001), and the primary care patients tended to have greater medical comorbidity. Psychiatric patients were more likely to have attempted suicide in the past and to have had their first depressive illness before age 18.
LEVEL 1: WHAT CAN WE EXPECT FROM INITIAL TREATMENT?
At level 1, all the patients received citalopram. The mean dose was 40.6 ± 16.6 mg/day in the primary care clinics and 42.5 ± 16.8 mg/day in the psychiatric clinics, which are adequate, middle-range doses and higher than the average US dose.29
Approximately 30% of patients achieved remission: 27% as measured on the HAM-D17 and 33% on the QIDS-SR16. The response rate (on the QIDS-SR16) was 47%. There were no differences between primary and psychiatric care settings in remission or response rates.
Patients were more likely to achieve remission if they were white, female, employed, more educated, or wealthier. Longer current episodes, more concurrent psychiatric disorders (especially anxiety disorders or drug abuse), more general medical disorders, and lower baseline function and quality of life were each associated with lower remission rates.
What is an adequate trial?
Longer times than expected were needed to reach response or remission. The average duration required to achieve remission was almost 7 weeks (44 days in primary care; 49 days in psychiatric care). Further, approximately one-third of those who ultimately responded and half of those who entered remission did so after 6 weeks.30 Forty percent of those who entered remission required 8 or more weeks to do so.
These results suggest that longer treatment durations and more vigorous medication dosing than generally used are needed to achieve optimal remission rates. It is imprudent to stop a treatment that the patient is tolerating in a robust dose if the patient reports only partial benefit by 6 weeks; indeed, raising the dose, if tolerated, may help a substantial number of patients respond by 12 or 14 weeks. Instruments to monitor depression severity (eg, self-report measures) can be useful. At least 8 weeks with at least moderately vigorous dosing is recommended.
LEVEL 2: IF THE FIRST TREATMENT FAILS
When switching to a new drug, does it matter which one?
No.
In level 2, if patients had not achieved remission on citalopram alone, they had the choice of switching: stopping citalopram and being randomized to receive either sertraline (Zoloft, another SSRI), venlafaxine extended-release (XR) (Effexor XR, a serotonin and norepinephrine reuptake inhibitor), or bupropion sustained-release (SR) (Wellbutrin SR, a norepinephrine and dopamine reuptake inhibitor). At the last visit the mean daily doses were bupropion SR 282.7 mg/day, sertraline 135.5 mg/day, and venlafaxine-XR 193.6 mg/day.
The remission rate was approximately one-fourth with all three drugs31:
- With bupropion SR—21.3% by HAM-D17, 25.5% by QIDS-SR16
- With sertraline—17.6% by HAM-D17, 26.6% by QIDS-SR16
- With venlafaxine-XR—24.8% by HAM-D17, 25.0% by QIDS-SR16. The remission rates were neither statistically nor clinically different by either measure.
Though the types of side effects related to specific medications may have varied, the overall side-effect burden and the rate of serious adverse events did not differ significantly.
When adding a new drug, does it matter which one?
Again, no.
Instead of switching, patients in level 2 could choose to stay on citalopram and be randomized to add either bupropion SR or buspirone (BuSpar) to the regimen (augmentation). The mean daily doses at the end of level 2 were bupropion SR 267.5 mg and buspirone 40.9 mg.
Rates of remission32:
- With bupropion SR—29.7% on the HAMD-D17, 39.0% on the QIDS-SR16
- With buspirone—30.1% on the HAM-D17, 32.9% on the QIDS-SR16.
However, the QIDS-SR16 scores declined significantly more with bupropion SR than with buspirone (25.3% vs 17.1%, P < .04). The mean total QIDS-SR16 score at the last visit was lower with bupropion SR (8.0) than with buspirone (9.1, P < .02), and augmentation with bupropion SR was better tolerated (the dropout rate due to intolerance was 12.5% with bupropion-SR vs 20.6% with buspirone 20.6%; P < .009).
Can we directly compare the benefits of switching vs augmenting?
No.
Patients could choose whether to switch from citalopram to another drug or to add another drug at the second treatment level.33 Consequently, we could not ensure that the patient groups were equivalent at the point of randomization at the beginning of level 2, and, indeed, they were not.
Those who benefitted more from citalopram treatment and who better tolerated it preferred augmentation, while those who benefitted little or who could not tolerate it preferred to switch. Consequently, those in the augmentation group at level 2 were somewhat less depressed than those who switched. Whether augmentation is better even if the initial treatment is minimally effective could not be evaluated in STAR*D.
What about cognitive therapy?
There was no difference between cognitive therapy (either as a switch or as augmentation) and medication (as a switch or as augmentation).34 Adding another drug was more rapidly effective than adding cognitive therapy. Switching to cognitive therapy was better tolerated than switching to a different antidepressant.
Of note, fewer patients accepted cognitive therapy as a randomization option than we expected, so the sample sizes were small. Possible reasons were that all patients had to receive a medication at study entry (which may have biased selection towards those preferring medication), and cognitive therapy entailed additional copayments and visiting still another provider at another site.
After two levels of treatment, how many patients reach remission?
About 30% of patients in level 1 achieved remission, and of those progressing to level 2, another 30% achieved remission. Together, this adds up to about 50% of patients achieving remission if they remained in treatment (30% in level 1 plus 30% of the roughly 70% remaining in level 2).
IF A SECOND TREATMENT FAILS
If switching again to another drug, does it matter which one?
No.
In level 3, patients could choose to stop the drug they had been taking and be randomized to receive either mirtazapine (Remeron) or nortriptyline (Pamelor).
Switching medications was not as effective as a third step as it was as a second step.35
Remission rates:
- With mirtazapine—12.3% on the HAM-D17, 8.0% on the QIDS-SR16
- With nortriptyline—19.8% on the HAM-D17, 12.4% on the QIDS-SR16.
Response rates were 13.4% with mirtazapine and 16.5% with nortriptyline. Statistically, neither the response nor the remission rates differed by treatment, nor did these two treatments differ in tolerability or side-effect burden.
Does choice of augmentation agent matter: Lithium vs T3?
Similarly, after two failed medication treatments, medication augmentation was less effective than it was at the second step.36 The two augmentation options tested, lithium and T3 thyroid hormone (Cytomel), are commonly considered by psychiatrists but less commonly used by primary care doctors.
Lithium is believed to increase serotonergic function, which may have a synergistic effect on the mechanism of action of antidepressants; a meta-analysis of placebo-controlled studies supports lithium’s effectiveness as adjunctive treatment.37 Its side effects, however, must be closely monitored.38 The primary monitoring concern is the small difference between the therapeutic blood level (0.6–1.2 mEq/L) and potentially toxic blood levels (> 1.5 mEq/L).
Lithium was started at 450 mg/day, and at week 2 it was increased to the recommended dose of 900 mg/day (a dose below the target dose for bipolar disorder). If patients could not tolerate 450 mg/day, the initial dose was 225 mg/day for 1 week before being increased to 450 mg/day, still with the target dose of 900 mg/day. The mean exit dose was 859.9 mg/day, and the median blood level was 0.6 mEq/L.
Thyroid hormone augmentation using T3 is believed to work through both direct and indirect effects on the hypothalamic-pituitary-thyroid axis, which has a strong relationship with depression. The efficacy of T3 augmentation is supported by a meta-analysis of eight studies,39 and T3 is effective whether or not thyroid abnormalities are present.
In STAR*D, T3 was started at 25 μg/day for 1 week, than increased to the recommended dose of 50 μg/day. The mean exit dose was 45.2 μg/day.
Remission rates:
- With lithium augmentation—15.9% by the HAM-D17, 13.2% by the QIDS-SR16
- With T3 augmentation—24.7% by both measures.
Response rates were 16.2% with lithium augmentation and 23.3% with T3 augmentation.
While neither response nor remission rates were statistically significantly different by treatment, lithium was more frequently associated with side effects (P = .045), and more participants in the lithium group left treatment because of side effects (23.2% vs 9.6%; P = .027). These results suggest that in cases in which a clinician is considering an augmentation trial, T3 has slight advantages over lithium in effectiveness and tolerability. T3 also offers the advantages of being easy to use and not necessitating blood level monitoring. These latter benefits are especially relevant to the primary care physician. However, T3’s potential for long-term side effects (eg, osteoporosis, cardiovascular effects) were not examined, and it is not clear when to discontinue it.
LEVEL 4: AFTER THREE FAILURES, HOW SHOULD A CLINICIAN PROCEED?
Switch to mirtazapine plus venlafaxine XR or tranylcypromine?
Patients who reached level 4 were considered to have a highly treatment-resistant depressive illness, so treatments at this level were, by design, more aggressive. Accordingly, at level 4 we investigated treatments that might be considered more demanding than those a primary care physician would use. Approximately 40% of patients in each treatment group were from primary care settings.
Remission rates40:
- With the combination of mirtazapine (mean dose 35.7 mg/day) and venlafaxine XR (mean dose 210.3 mg/day)—13.7% by the HAM-D17 and 15.7% by the QIDS-SR16
- With the MAOI tranylcypromine (Parnate, mean dose 36.9 mg/day)—6.9% by the HAM-D17 and 13.8% by the QIDS-SR16. Response rates were 23.5% with the combination and 12.1% with tranylcypromine. Neither remission nor response rates differed significantly.
However, the percentage reduction in QIDS-SR16 score between baseline and exit was greater with the combination than with tranylcypromine. Further, more patients dropped out of treatment with tranylcypromine because of side effects (P < .03). Tranylcypromine also has the disadvantage of necessitating dietary restrictions.
A significant limitation of this comparison is that patients were less likely to get an adequate trial of tranylcypromine, an MAOI, than of the combination. When the 2-week washout period (required before switching to an MAOI) is subtracted from the total time in treatment, approximately 30% of participants in the tranylcypromine group had less than 2 weeks of treatment, and nearly half had less than 6 weeks of treatment.
Therefore, even though the remission and response rates were similar between groups, the combination of venlafaxine-XR plus mirtazapine therapy might have some advantages over tranylcypromine. These results provided the first evidence of tolerability and at least modest efficacy of this combination for treatment-resistant cases.
Overall, what was the cumulative remission rate?
The theoretical cumulative remission rate after four acute treatment steps was 67%. Remission was more likely to occur during the first two levels of treatment than during the last two. The cumulative remission rates for the first four steps were:
- Level 1—33%
- Level 2—57%
- Level 3—63%
- Level 4—67%.
RESULTS FROM LONG-TERM FOLLOW-UP AFTER REMISSION OR RESPONSE
Patients with a clinically meaningful response or, preferably, remission at any level could enter into a 12-month observational follow-up phase. Those who had required more treatment levels had higher relapse rates during this phase.41 Further, if a patient achieved remission rather than just response to treatment, regardless of the treatment level, the prognosis at follow-up was better, confirming the importance of remission as the goal of treatment.
Results also provided a warning—the greater the number of treatment levels that a patient required, the more likely that patient and physician would settle for response. Whether the greater relapse rates reflect a harder-to-treat depression or the naturalistic design of the follow-up phase (with less control over dosing) is unclear.
WHAT DO THESE RESULTS MEAN FOR PRIMARY CARE PHYSICIANS?
- Measurement-based care is feasible in primary care. Primary care doctors can ensure vigorous but tolerable dosing using a self-report depression scale to monitor response, a side-effects tool to monitor tolerability, and medication adjustments at critical decision points guided by these two measures.
- Remission, ie, complete recovery from a depressive episode, rather than merely substantial improvement, is associated with a better prognosis and is the preferred goal of treatment.
- Pharmacologic differences between psychotropic medications did not translate into substantial clinical differences, although tolerability differed. These findings are consistent with a large-scale systematic evidence review recently completed by the Agency for Healthcare Research and Quality that compared the effectiveness of antidepressants.42 Given the difficulty in predicting what medication will be both efficacious for and tolerated by an individual patient, familiarity with a broad spectrum of antidepressants is prudent.
- Remission of depressive episodes will most likely require repeated trials of sufficiently sustained,vigorously dosed antidepressant medication. From treatment initiation, physicians should ensure maximal but tolerable doses for at least 8 weeks before deciding that an intervention has failed.
- If a first treatment doesn’t work, either switching or augmenting it is a reasonable choice. Augmentation may be preferred if the patient is tolerating and receiving partial benefit from the initial medication choice. While bupropion SR and buspirone were not different as augmenters by the primary remission outcome measure, secondary measures (eg, tolerability, depressive symptom change over the course of treatment, clinician-rated Quick Inventory of Depressive Symptomatology) recommended bupropion-SR over buspirone.
- If physicians switch, either a within-class switch (eg, citalopram to sertraline) or an out-of-class switch (eg, citalopram to bupropion SR) is effective, as is a switch to a dual-action agent (eg, venlafaxine XR).
- The likelihood of improvement after two aggressive medication trials is very low and likely requires more complicated medication regimens, and the existing evidence base is quite thin. These primary care patients should likely be referred to psychiatrists for more aggressive and intensive treatment.
- For patients who present with major depressive disorder, STAR*D suggests that with persistence and aggressive yet feasible care, there is hope: after one round, approximately 30% will have a remission; after two rounds, 50%; after three rounds, 60%; and after four rounds, 70%.
- While STAR*D excluded depressed patients with bipolar disorder, a depressive episode in a patient with bipolar disorder can be difficult to distinguish from a depressive episode in a patient with major depressive disorder. Primary care physicians need to consider bipolar disorder both in patients presenting with a depressive episode and in those who fail an adequate trial.43
FUTURE CONSIDERATIONS
Subsequent STAR*D analyses will compare in greater depth outcomes in primary care vs psychiatric settings at each level of treatment. Given the greater risk of depression persistence associated with more successive levels of treatment, subsequent research will focus on ways to more successfully treat depression in the earlier stages, possibly through medication combinations earlier in treatment (somewhat analogous to a “broad-spectrum antibiotic” approach for infections).
- Kessler RC, Berglund P, Demler O, et al. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA 2003; 289:3095–3105.
- Murray CJ, Lopez AD. Global mortality, disability, and the contribution of risk factors: Global Burden of Disease Study. Lancet 1997; 349:1436–1442.
- Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990–2020: Global Burden of Disease Study. Lancet 1997; 349:1498–1504.
- Zimmerman M, Chelminski I, Posternak MA. Generalizability of antidepressant efficacy trials: differences between depressed psychiatric outpatients who would or would not qualify for an efficacy trial. Am J Psychiatry 2005; 162:1370–1372.
- Rothwell PM. External validity of randomised controlled trials: to whom do the results of this trial apply? Lancet 2005; 365:82–93.
- Depression Guideline Panel. Depression in primary care: Volume 1, diagnosis and detection. AHCPR publication No. 93-0550. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research; 1993.
- Frank E, Karp J, Rush A. Efficacy of treatments for major depression. Psychopharmacol Bull 1993; 29:457–475.
- Depression Guideline Panel. Depression in primary care: Volume 2, Treatment of major depression. AHCPR publication No. 93-0550. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research; 1993.
- Fava M, Davidson KG. Definition and epidemiology of treatment-resistant depression. Psychiatr Clin North Am 1996; 19:179–200.
- Jarrett RB, Rush A. Short-term psychotherapy of depressive disorders: current status and future directions. Psychiatry: Interpers Biol Process 1994; 57:115–132.
- American Psychiatric Association. Practice guideline for the treatment of patients with major depression (revision). Am J Psychiatry 2000; 157(suppl 4):1–45.
- Dunner DL, Rush AJ, Russell JM, et al. Prospective, long-term, multicenter study of the naturalistic outcomes of patients with treatment-resistant depression. J Clin Psychiatry 2006; 67:688–695.
- Fava M, Rush A, Trivedi M, et al. Background and rationale for the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study. Psychiatr Clin North Am 2003; 26:457–494.
- Gaynes B, Davis L, Rush A, Trivedi M, Fava M, Wisniewski S. The aims and design of the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) Study. Prim Psychiatry 2005; 12:36–41.
- Rush A, Fava M, Wisniewski S, et al. Sequenced Treatment Alternatives to Relieve Depression (STAR*D): rationale and design. Control Clin Trials 2004; 25:119–142.
- Stafford RS, Ausiello JC, Misra B, Saglam D. National Patterns o fDepression Treatment in Primary Care. Prim Care Companion J Clin Psychiatry 2000; 2:211–216.
- Regier D, Narrow W, Rae D, Mandersheid R, Locke B, Goodwin F. The de facto US mental and addictive disorders service system: epidemiologic catchment area prospective 1-year prevalence rates of disorders and services. Arch Gen Psychiatry 1993; 50:85–94.
- Pincus H, Tanielian T, Marcus S, et al. Prescribing trends in psychotropic medications: primary care, psychiatry, and other medical specialities. JAMA 1998; 279:526–531.
- Vuorilehto M, Melartin T, Isometsa E. Depressive disorders in primary care: recurrent, chronic, and co-morbid. Psychol Med 2005; 35:673–682.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fourth edition, Text Revision. Washington, DC: American Psychiatric Association; 2000.
- Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry 1960; 23:56–61.
- Wisniewski SR, Rush AJ, Balasubramani GK, Trivedi MH, Nierenberg AA for the STAR*D Investigators. Self-rated global measure of the frequency, intensity, and burden of side effects. J Psychiatric Pract 2006; 12:71–79.
- Rush AJ, Bernstein IH, Trivedi MH, et al. An evaluation of the Quick Inventory of Depressive Symptomatology and the Hamilton Rating Scale for Depression: a Sequenced Treatment Alternatives to Relieve Depression (STAR*D) trial report. Biol Psychiatry 2006; 59:493–501.
- Trivedi MH, Rush AJ, Gaynes BN, et al. Maximizing the adequacy of medication treatment in controlled trials and clinical practice: STAR*D measurement-based care. Neuropsychopharmacology 2007/04/04/online 2007.
- Kawamoto K, Houlihan CA, Balas EA, Lobach DF. Improving clinical practice using clinical decision support systems: a systematic review of trials to identify features critical to success. BMJ 2005; 330:765 e-pub March 14 2005.
- Lavori P, Rush A, Wisniewski S, et al. Strengthening clinical effectiveness trials: equipoise-stratified randomization. Biol Psychiatry 2001; 50:792–801.
- Gaynes BN, Rush AJ, Trivedi MH, et al. Major depression symptoms in primary care and psychiatric care settings: a cross-sectional analysis. Ann Fam Med 2007; 5:126–134.
- Gaynes BN, Rush AJ, Trivedi M, et al. A direct comparison of presenting characteristics of depressed outpatients from primary vs. specialty care settings: preliminary findings from the STAR*D clinical trial. Gen Hosp Psychiatry 2005; 27:87–96.
- Sullivan PW, Valuck R, Saseen J, MacFall HM. A comparison of the direct costs and cost effectiveness of serotonin reuptake inhibitors and associated adverse drug reactions. CNS Drugs 2004; 18:911–932.
- Trivedi MH, Rush AJ, Wisniewski SR, et al. Evaluation of outcomes with citalopram for depression using measurement-based care in STAR*D: implications for clinical practice. Am J Psychiatry 2006; 163:28–40.
- Rush AJ, Trivedi MH, Wisniewski SR, et al. Bupropion-SR, sertraline, or venlafaxine-XR after failure of SSRIs for depression. N Engl J Med 2006; 354:1231–1242.
- Trivedi MH, Fava M, Wisniewski SR, et al. Medication augmentation after the failure of SSRIs for depression. N Engl J Med 2006; 354:1243–1252.
- Wisniewski SR, Fava M, Trivedi MH, et al. Acceptability of second-step treatments to depressed outpatients: a STAR*D report. Am J Psychiatry 2007; 164:753–760.
- Thase ME, Friedman ES, Biggs MM, et al. Cognitive therapy versus medication in augmentation and switch strategies as second-step treatments: a STAR*D report. Am J Psychiatry 2007; 164:739–752.
- Fava M, Rush AJ, Wisniewski SR, et al. A comparison of mirtazapine and nortriptyline following two consecutive failed medication treatments for depressed outpatients: a STAR*D report. Am J Psychiatry 2006; 163:1161–1172.
- Nierenberg AA, Fava M, Trivedi MH, et al. A comparison of lithium and T3 augmentation following two failed medication treatments for depression: a STAR*D report. Am J Psychiatry 2006; 163:1519–1530.
- Bschor T, Lewitzka U, Sasse J, Adli M, Koberle U, Bauer M. Lithium augmentation in treatment-resistant depression: clinical evidence, serotonergic and endocrine mechanisms. Pharmacopsychiatry 2003; 36(suppl 3):S230–S234.
- Freeman MP, Freeman SA. Lithium: clinical considerations in internal medicine. Am J Med 2006; 119:478–481.
- Aronson R, Offman HJ, Joffe RT, Naylor CD. Triiodothyronine augmentation in the treatment of refractory depression. A meta-analysis. Arch Gen Psychiatry 1996; 53:842–848.
- McGrath PJ, Stewart JW, Fava M, et al. Tranylcypromine versus venlafaxine plus mirtazapine following three failed antidepressant medication trials for depression: a STAR*D report. Am J Psychiatry 2006; 163:1531–1541.
- Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. Am J Psychiatry 2006; 163:1905–1917.
- Gartlehner G, Hansen R, Thieda P, et al. Comparative Effectiveness of Second-generation Antidepressants in the Pharmacologic Treatment of Depression. Agency for Healthcare Research and Quality. http://effectivehealthcare.ahrq.gov/reports/topic.cfm?topic=8&sid=39&rType=3. Accessed December 12, 2007.
- Das AK, Olfson M, Gameroff MJ, et al. Screening for bipolar disorder in a primary care practice. JAMA 2005; 293:956–963.
Depression can be treated successfully by primary care physicians under “real-world” conditions.
Furthermore, the particular drug or drugs used are not as important as following a rational plan: giving antidepressant medications in adequate doses, monitoring the patient’s symptoms and side effects and adjusting the regimen accordingly, and switching drugs or adding new drugs to the regimen only after an adequate trial.
These are among the lessons learned from the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study, the largest prospective clinical trial of treatment of major depressive disorder ever conducted. It was funded by the National Institutes of Health and directed by A. John Rush, MD.
WHAT WERE THE AIMS OF STAR*D?
Depression, a common and debilitating condition, affects approximately one in eight people in the United States.1 It is expected2 to be the second-leading cause of disability in the world by the year 2020; today, it is the second-leading cause of disability-adjusted life years in those 15 to 44 years old.3
Nevertheless, the available evidence base for treatment is limited, since most participants in clinical trials are recruited by advertisement rather than from representative practices, and they are often selected to have few comorbid disorders, either medical or psychiatric. In addition, those with chronic depression or current suicidal ideation are excluded.1,4 These uncomplicated and “pristine” participants are unlike typical patients seen by primary care physicians or psychiatrists.
Similarly, the protocols used in these trials do not represent usual clinic practice.Patients in clinical trials undergo more assessment and more frequent follow-up than in real-world practice, they have no say in treatment decisions, the doses are fixed, and the patients and physicians are blinded to the intervention. Consequently, how to translate the results of these efficacy trials into practice is unclear.5
Further, even in relatively uncomplicated cases, only about one-half of outpatients with nonpsychotic major depressive disorder initially treated with a single medication or with psychotherapy will experience a clinically significant improvement in symptoms (ie, a response) during the 8 to 12 weeks of acute-phase treatment,6–10 and only 20% to 35% of patients will reach remission,9 the aim of treatment.8,11 The remission rates are even lower in treatment-resistant depression.12 How to manage most patients—those whose depression does not remit with the first, second, or third step of treatment—is unclear.
Accordingly, the overall objective of STAR*D was to develop and evaluate feasible treatment strategies to improve clinical outcomes for real-world patients with treatment-resistant depression, who were identified prospectively from a pool of patients in a current major depressive episode.13–15 Specifically, STAR*D aimed to determine prospectively which of several treatments is the most effective “next step” for patients who do not reach remission with an initial or subsequent treatment or who cannot tolerate the treatment.
WHY IS STAR*D RELEVANT FOR PRIMARY CARE?
Nearly 10% of all primary care office visits are depression-related.16 Primary care physicians provide nearly half the outpatient care for depressed patients.17 Indeed, primary care physicians log approximately as many outpatient visits for depression as psychiatrists do.18 Medical comorbidity is especially common in primary care settings.19 When to refer to a psychiatrist is not clear.
KEY FEATURES OF THE STUDY DESIGN
STAR*D involved a national consortium of 14 university-based regional centers, which oversaw a total of 23 participating psychiatric and 18 primary care clinics. Enrollment began in 2000, with follow-up completed in 2004.
Entry criteria were broad and inclusive
Patients had to:
- Be between 18 and 75 years of age
- Have a nonpsychotic major depressive disorder, identified by a clinician and confirmed with a symptom checklist based on the Diagnostic and Statistical Manual, fourth edition revised,20 and for which antidepressant treatment is recommended
- Score at least 14 on the 17-item Hamilton Rating Scale for Depression (HAMD17)21
- Not have a primary diagnosis of bipolar disorder, obsessive-compulsive disorder, or an eating disorder, which would require a different treatment strategy, or a seizure disorder (which would preclude bupropion as a second-step treatment).
Dosing recommendations were flexible but vigorous
Medications often were increased to maximally tolerated doses. For example, citalopram (Celexa) was started at 20 mg/day and increased by 20 mg every 2 to 4 weeks if the patient was tolerating it but had not achieved remission, to a maximum dose of 60 mg/day. Treatment could be given for up to 14 weeks, during which side effects22 and clinical ratings23 were assessed by both patients and study coordinators.
Measurement-based care
We used a systematic approach to treatment called “measurement-based care,”24 which involves routinely measuring symptoms23 and side effects22 and using this information to modify the medication doses at critical decision points. This algorithmic approach provided flexible treatment recommendations to ensure that the dosage and duration of antidepressant drug treatment were adequate.25
The severity of depression was assessed by the clinician-rated, 16-item Quick Inventory of Depressive Symptomatology (QIDS-C16). The QIDS-SR16 (the self-report version) can substitute for the QIDS-C1623 to make this approach more feasible. Both tools are available at www.ids-qids.org.
This approach was easily worked into busy primary care and specialty care office workflows (clinic physicians, most with limited research experience, provided the treatment), and could be translated into primary care practice in the community as well.
Four-step protocol
A unique feature of the study design was that the patients, in consultation with their physicians, had some choice in the treatments they received. In this “equipoise-stratified randomized design,”26 at levels 2 and 3 the patient could choose either to switch therapies (stop the current drug and be randomized to receive one of several different treatments) or to augment their current therapy (by adding one of several treatments in a randomized fashion). Patients could decline certain strategies as long as there were at least two possible options to which one might be randomized.
At level 2, one of the options for both switching and augmentation was cognitive therapy, although patients could decline that option. Conversely, if they definitely wanted cognitive therapy, they could choose to be randomized to either cognitive therapy alone or to cognitive therapy added to citalopram. Also, anyone who received cognitive therapy in level 2 and failed to enter remission was additionally randomized to either bupropion or venlafaxine (level 2a) to ensure that all patients had failed trials on two medications before entering level 3.
When switching to medications other than a monoamine oxidase inhibitor (MAOI), the clinician could choose either to stop the current medication and immediately begin the next one, or to decrease the current medication while starting the new one at a low dose and then tapering and titrating over 1 week. (Switching to an MAOI, used only in the final level of treatment, required a 7- to 10-day washout period.)
Outcomes measured
Remission (complete recovery from the depressive episode), the primary study outcome, was defined as a HAM-D17 score of 7 or less, as assessed by treatment-blinded raters.A secondary remission outcome was a QIDS-SR16 score of 5 or less. Of note, the HAM-D17 remission rates were slightly lower than the rates based on the QIDS-SR16, since patients who did not have a HAM-D17 score measured at exit were defined as not being in remission a priori. Thus, the QIDS-SR16 rates might have been a slightly better reflection of actual remission rates.
Response, a secondary outcome, was defined as a reduction of at least 50% in the QIDS-SR16 score from baseline at the last assessment.
FEW DIFFERENCES BETWEEN PSYCHIATRIC, PRIMARY CARE PATIENTS
The patients seen in primary care clinics were surprisingly similar to those seen in psychiatric clinics.27,28 The two groups did not differ in severity of depression, distribution of severity scores, the likelihood of presenting with any of the nine core criteria of a major depressive episode, or the likelihood of having a concomitant axis I psychiatric disorder in addition to depression (about half of participants in each setting had an anxiety disorder).
Recurrent major depressive disorders were common in both groups, though more so in psychiatric patients (78% vs 69%, P < .001), while chronic depression was more common in primary care than in psychiatric patients (30% vs 21%, P < .001). Having either a chronic index episode (ie, lasting > 2 years) or a recurrent major depressive disorder was common in both groups (86% vs 83%, P = .0067).
That said, primary care patients were older (44 years vs 39 years, P < .001), more of them were Hispanic (18% vs 9%, P < .001), and more of them had public insurance (23% vs 9%, P < .001). Fewer of the primary care patients had completed college (20% vs 28%, P < .001), and the primary care patients tended to have greater medical comorbidity. Psychiatric patients were more likely to have attempted suicide in the past and to have had their first depressive illness before age 18.
LEVEL 1: WHAT CAN WE EXPECT FROM INITIAL TREATMENT?
At level 1, all the patients received citalopram. The mean dose was 40.6 ± 16.6 mg/day in the primary care clinics and 42.5 ± 16.8 mg/day in the psychiatric clinics, which are adequate, middle-range doses and higher than the average US dose.29
Approximately 30% of patients achieved remission: 27% as measured on the HAM-D17 and 33% on the QIDS-SR16. The response rate (on the QIDS-SR16) was 47%. There were no differences between primary and psychiatric care settings in remission or response rates.
Patients were more likely to achieve remission if they were white, female, employed, more educated, or wealthier. Longer current episodes, more concurrent psychiatric disorders (especially anxiety disorders or drug abuse), more general medical disorders, and lower baseline function and quality of life were each associated with lower remission rates.
What is an adequate trial?
Longer times than expected were needed to reach response or remission. The average duration required to achieve remission was almost 7 weeks (44 days in primary care; 49 days in psychiatric care). Further, approximately one-third of those who ultimately responded and half of those who entered remission did so after 6 weeks.30 Forty percent of those who entered remission required 8 or more weeks to do so.
These results suggest that longer treatment durations and more vigorous medication dosing than generally used are needed to achieve optimal remission rates. It is imprudent to stop a treatment that the patient is tolerating in a robust dose if the patient reports only partial benefit by 6 weeks; indeed, raising the dose, if tolerated, may help a substantial number of patients respond by 12 or 14 weeks. Instruments to monitor depression severity (eg, self-report measures) can be useful. At least 8 weeks with at least moderately vigorous dosing is recommended.
LEVEL 2: IF THE FIRST TREATMENT FAILS
When switching to a new drug, does it matter which one?
No.
In level 2, if patients had not achieved remission on citalopram alone, they had the choice of switching: stopping citalopram and being randomized to receive either sertraline (Zoloft, another SSRI), venlafaxine extended-release (XR) (Effexor XR, a serotonin and norepinephrine reuptake inhibitor), or bupropion sustained-release (SR) (Wellbutrin SR, a norepinephrine and dopamine reuptake inhibitor). At the last visit the mean daily doses were bupropion SR 282.7 mg/day, sertraline 135.5 mg/day, and venlafaxine-XR 193.6 mg/day.
The remission rate was approximately one-fourth with all three drugs31:
- With bupropion SR—21.3% by HAM-D17, 25.5% by QIDS-SR16
- With sertraline—17.6% by HAM-D17, 26.6% by QIDS-SR16
- With venlafaxine-XR—24.8% by HAM-D17, 25.0% by QIDS-SR16. The remission rates were neither statistically nor clinically different by either measure.
Though the types of side effects related to specific medications may have varied, the overall side-effect burden and the rate of serious adverse events did not differ significantly.
When adding a new drug, does it matter which one?
Again, no.
Instead of switching, patients in level 2 could choose to stay on citalopram and be randomized to add either bupropion SR or buspirone (BuSpar) to the regimen (augmentation). The mean daily doses at the end of level 2 were bupropion SR 267.5 mg and buspirone 40.9 mg.
Rates of remission32:
- With bupropion SR—29.7% on the HAMD-D17, 39.0% on the QIDS-SR16
- With buspirone—30.1% on the HAM-D17, 32.9% on the QIDS-SR16.
However, the QIDS-SR16 scores declined significantly more with bupropion SR than with buspirone (25.3% vs 17.1%, P < .04). The mean total QIDS-SR16 score at the last visit was lower with bupropion SR (8.0) than with buspirone (9.1, P < .02), and augmentation with bupropion SR was better tolerated (the dropout rate due to intolerance was 12.5% with bupropion-SR vs 20.6% with buspirone 20.6%; P < .009).
Can we directly compare the benefits of switching vs augmenting?
No.
Patients could choose whether to switch from citalopram to another drug or to add another drug at the second treatment level.33 Consequently, we could not ensure that the patient groups were equivalent at the point of randomization at the beginning of level 2, and, indeed, they were not.
Those who benefitted more from citalopram treatment and who better tolerated it preferred augmentation, while those who benefitted little or who could not tolerate it preferred to switch. Consequently, those in the augmentation group at level 2 were somewhat less depressed than those who switched. Whether augmentation is better even if the initial treatment is minimally effective could not be evaluated in STAR*D.
What about cognitive therapy?
There was no difference between cognitive therapy (either as a switch or as augmentation) and medication (as a switch or as augmentation).34 Adding another drug was more rapidly effective than adding cognitive therapy. Switching to cognitive therapy was better tolerated than switching to a different antidepressant.
Of note, fewer patients accepted cognitive therapy as a randomization option than we expected, so the sample sizes were small. Possible reasons were that all patients had to receive a medication at study entry (which may have biased selection towards those preferring medication), and cognitive therapy entailed additional copayments and visiting still another provider at another site.
After two levels of treatment, how many patients reach remission?
About 30% of patients in level 1 achieved remission, and of those progressing to level 2, another 30% achieved remission. Together, this adds up to about 50% of patients achieving remission if they remained in treatment (30% in level 1 plus 30% of the roughly 70% remaining in level 2).
IF A SECOND TREATMENT FAILS
If switching again to another drug, does it matter which one?
No.
In level 3, patients could choose to stop the drug they had been taking and be randomized to receive either mirtazapine (Remeron) or nortriptyline (Pamelor).
Switching medications was not as effective as a third step as it was as a second step.35
Remission rates:
- With mirtazapine—12.3% on the HAM-D17, 8.0% on the QIDS-SR16
- With nortriptyline—19.8% on the HAM-D17, 12.4% on the QIDS-SR16.
Response rates were 13.4% with mirtazapine and 16.5% with nortriptyline. Statistically, neither the response nor the remission rates differed by treatment, nor did these two treatments differ in tolerability or side-effect burden.
Does choice of augmentation agent matter: Lithium vs T3?
Similarly, after two failed medication treatments, medication augmentation was less effective than it was at the second step.36 The two augmentation options tested, lithium and T3 thyroid hormone (Cytomel), are commonly considered by psychiatrists but less commonly used by primary care doctors.
Lithium is believed to increase serotonergic function, which may have a synergistic effect on the mechanism of action of antidepressants; a meta-analysis of placebo-controlled studies supports lithium’s effectiveness as adjunctive treatment.37 Its side effects, however, must be closely monitored.38 The primary monitoring concern is the small difference between the therapeutic blood level (0.6–1.2 mEq/L) and potentially toxic blood levels (> 1.5 mEq/L).
Lithium was started at 450 mg/day, and at week 2 it was increased to the recommended dose of 900 mg/day (a dose below the target dose for bipolar disorder). If patients could not tolerate 450 mg/day, the initial dose was 225 mg/day for 1 week before being increased to 450 mg/day, still with the target dose of 900 mg/day. The mean exit dose was 859.9 mg/day, and the median blood level was 0.6 mEq/L.
Thyroid hormone augmentation using T3 is believed to work through both direct and indirect effects on the hypothalamic-pituitary-thyroid axis, which has a strong relationship with depression. The efficacy of T3 augmentation is supported by a meta-analysis of eight studies,39 and T3 is effective whether or not thyroid abnormalities are present.
In STAR*D, T3 was started at 25 μg/day for 1 week, than increased to the recommended dose of 50 μg/day. The mean exit dose was 45.2 μg/day.
Remission rates:
- With lithium augmentation—15.9% by the HAM-D17, 13.2% by the QIDS-SR16
- With T3 augmentation—24.7% by both measures.
Response rates were 16.2% with lithium augmentation and 23.3% with T3 augmentation.
While neither response nor remission rates were statistically significantly different by treatment, lithium was more frequently associated with side effects (P = .045), and more participants in the lithium group left treatment because of side effects (23.2% vs 9.6%; P = .027). These results suggest that in cases in which a clinician is considering an augmentation trial, T3 has slight advantages over lithium in effectiveness and tolerability. T3 also offers the advantages of being easy to use and not necessitating blood level monitoring. These latter benefits are especially relevant to the primary care physician. However, T3’s potential for long-term side effects (eg, osteoporosis, cardiovascular effects) were not examined, and it is not clear when to discontinue it.
LEVEL 4: AFTER THREE FAILURES, HOW SHOULD A CLINICIAN PROCEED?
Switch to mirtazapine plus venlafaxine XR or tranylcypromine?
Patients who reached level 4 were considered to have a highly treatment-resistant depressive illness, so treatments at this level were, by design, more aggressive. Accordingly, at level 4 we investigated treatments that might be considered more demanding than those a primary care physician would use. Approximately 40% of patients in each treatment group were from primary care settings.
Remission rates40:
- With the combination of mirtazapine (mean dose 35.7 mg/day) and venlafaxine XR (mean dose 210.3 mg/day)—13.7% by the HAM-D17 and 15.7% by the QIDS-SR16
- With the MAOI tranylcypromine (Parnate, mean dose 36.9 mg/day)—6.9% by the HAM-D17 and 13.8% by the QIDS-SR16. Response rates were 23.5% with the combination and 12.1% with tranylcypromine. Neither remission nor response rates differed significantly.
However, the percentage reduction in QIDS-SR16 score between baseline and exit was greater with the combination than with tranylcypromine. Further, more patients dropped out of treatment with tranylcypromine because of side effects (P < .03). Tranylcypromine also has the disadvantage of necessitating dietary restrictions.
A significant limitation of this comparison is that patients were less likely to get an adequate trial of tranylcypromine, an MAOI, than of the combination. When the 2-week washout period (required before switching to an MAOI) is subtracted from the total time in treatment, approximately 30% of participants in the tranylcypromine group had less than 2 weeks of treatment, and nearly half had less than 6 weeks of treatment.
Therefore, even though the remission and response rates were similar between groups, the combination of venlafaxine-XR plus mirtazapine therapy might have some advantages over tranylcypromine. These results provided the first evidence of tolerability and at least modest efficacy of this combination for treatment-resistant cases.
Overall, what was the cumulative remission rate?
The theoretical cumulative remission rate after four acute treatment steps was 67%. Remission was more likely to occur during the first two levels of treatment than during the last two. The cumulative remission rates for the first four steps were:
- Level 1—33%
- Level 2—57%
- Level 3—63%
- Level 4—67%.
RESULTS FROM LONG-TERM FOLLOW-UP AFTER REMISSION OR RESPONSE
Patients with a clinically meaningful response or, preferably, remission at any level could enter into a 12-month observational follow-up phase. Those who had required more treatment levels had higher relapse rates during this phase.41 Further, if a patient achieved remission rather than just response to treatment, regardless of the treatment level, the prognosis at follow-up was better, confirming the importance of remission as the goal of treatment.
Results also provided a warning—the greater the number of treatment levels that a patient required, the more likely that patient and physician would settle for response. Whether the greater relapse rates reflect a harder-to-treat depression or the naturalistic design of the follow-up phase (with less control over dosing) is unclear.
WHAT DO THESE RESULTS MEAN FOR PRIMARY CARE PHYSICIANS?
- Measurement-based care is feasible in primary care. Primary care doctors can ensure vigorous but tolerable dosing using a self-report depression scale to monitor response, a side-effects tool to monitor tolerability, and medication adjustments at critical decision points guided by these two measures.
- Remission, ie, complete recovery from a depressive episode, rather than merely substantial improvement, is associated with a better prognosis and is the preferred goal of treatment.
- Pharmacologic differences between psychotropic medications did not translate into substantial clinical differences, although tolerability differed. These findings are consistent with a large-scale systematic evidence review recently completed by the Agency for Healthcare Research and Quality that compared the effectiveness of antidepressants.42 Given the difficulty in predicting what medication will be both efficacious for and tolerated by an individual patient, familiarity with a broad spectrum of antidepressants is prudent.
- Remission of depressive episodes will most likely require repeated trials of sufficiently sustained,vigorously dosed antidepressant medication. From treatment initiation, physicians should ensure maximal but tolerable doses for at least 8 weeks before deciding that an intervention has failed.
- If a first treatment doesn’t work, either switching or augmenting it is a reasonable choice. Augmentation may be preferred if the patient is tolerating and receiving partial benefit from the initial medication choice. While bupropion SR and buspirone were not different as augmenters by the primary remission outcome measure, secondary measures (eg, tolerability, depressive symptom change over the course of treatment, clinician-rated Quick Inventory of Depressive Symptomatology) recommended bupropion-SR over buspirone.
- If physicians switch, either a within-class switch (eg, citalopram to sertraline) or an out-of-class switch (eg, citalopram to bupropion SR) is effective, as is a switch to a dual-action agent (eg, venlafaxine XR).
- The likelihood of improvement after two aggressive medication trials is very low and likely requires more complicated medication regimens, and the existing evidence base is quite thin. These primary care patients should likely be referred to psychiatrists for more aggressive and intensive treatment.
- For patients who present with major depressive disorder, STAR*D suggests that with persistence and aggressive yet feasible care, there is hope: after one round, approximately 30% will have a remission; after two rounds, 50%; after three rounds, 60%; and after four rounds, 70%.
- While STAR*D excluded depressed patients with bipolar disorder, a depressive episode in a patient with bipolar disorder can be difficult to distinguish from a depressive episode in a patient with major depressive disorder. Primary care physicians need to consider bipolar disorder both in patients presenting with a depressive episode and in those who fail an adequate trial.43
FUTURE CONSIDERATIONS
Subsequent STAR*D analyses will compare in greater depth outcomes in primary care vs psychiatric settings at each level of treatment. Given the greater risk of depression persistence associated with more successive levels of treatment, subsequent research will focus on ways to more successfully treat depression in the earlier stages, possibly through medication combinations earlier in treatment (somewhat analogous to a “broad-spectrum antibiotic” approach for infections).
Depression can be treated successfully by primary care physicians under “real-world” conditions.
Furthermore, the particular drug or drugs used are not as important as following a rational plan: giving antidepressant medications in adequate doses, monitoring the patient’s symptoms and side effects and adjusting the regimen accordingly, and switching drugs or adding new drugs to the regimen only after an adequate trial.
These are among the lessons learned from the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study, the largest prospective clinical trial of treatment of major depressive disorder ever conducted. It was funded by the National Institutes of Health and directed by A. John Rush, MD.
WHAT WERE THE AIMS OF STAR*D?
Depression, a common and debilitating condition, affects approximately one in eight people in the United States.1 It is expected2 to be the second-leading cause of disability in the world by the year 2020; today, it is the second-leading cause of disability-adjusted life years in those 15 to 44 years old.3
Nevertheless, the available evidence base for treatment is limited, since most participants in clinical trials are recruited by advertisement rather than from representative practices, and they are often selected to have few comorbid disorders, either medical or psychiatric. In addition, those with chronic depression or current suicidal ideation are excluded.1,4 These uncomplicated and “pristine” participants are unlike typical patients seen by primary care physicians or psychiatrists.
Similarly, the protocols used in these trials do not represent usual clinic practice.Patients in clinical trials undergo more assessment and more frequent follow-up than in real-world practice, they have no say in treatment decisions, the doses are fixed, and the patients and physicians are blinded to the intervention. Consequently, how to translate the results of these efficacy trials into practice is unclear.5
Further, even in relatively uncomplicated cases, only about one-half of outpatients with nonpsychotic major depressive disorder initially treated with a single medication or with psychotherapy will experience a clinically significant improvement in symptoms (ie, a response) during the 8 to 12 weeks of acute-phase treatment,6–10 and only 20% to 35% of patients will reach remission,9 the aim of treatment.8,11 The remission rates are even lower in treatment-resistant depression.12 How to manage most patients—those whose depression does not remit with the first, second, or third step of treatment—is unclear.
Accordingly, the overall objective of STAR*D was to develop and evaluate feasible treatment strategies to improve clinical outcomes for real-world patients with treatment-resistant depression, who were identified prospectively from a pool of patients in a current major depressive episode.13–15 Specifically, STAR*D aimed to determine prospectively which of several treatments is the most effective “next step” for patients who do not reach remission with an initial or subsequent treatment or who cannot tolerate the treatment.
WHY IS STAR*D RELEVANT FOR PRIMARY CARE?
Nearly 10% of all primary care office visits are depression-related.16 Primary care physicians provide nearly half the outpatient care for depressed patients.17 Indeed, primary care physicians log approximately as many outpatient visits for depression as psychiatrists do.18 Medical comorbidity is especially common in primary care settings.19 When to refer to a psychiatrist is not clear.
KEY FEATURES OF THE STUDY DESIGN
STAR*D involved a national consortium of 14 university-based regional centers, which oversaw a total of 23 participating psychiatric and 18 primary care clinics. Enrollment began in 2000, with follow-up completed in 2004.
Entry criteria were broad and inclusive
Patients had to:
- Be between 18 and 75 years of age
- Have a nonpsychotic major depressive disorder, identified by a clinician and confirmed with a symptom checklist based on the Diagnostic and Statistical Manual, fourth edition revised,20 and for which antidepressant treatment is recommended
- Score at least 14 on the 17-item Hamilton Rating Scale for Depression (HAMD17)21
- Not have a primary diagnosis of bipolar disorder, obsessive-compulsive disorder, or an eating disorder, which would require a different treatment strategy, or a seizure disorder (which would preclude bupropion as a second-step treatment).
Dosing recommendations were flexible but vigorous
Medications often were increased to maximally tolerated doses. For example, citalopram (Celexa) was started at 20 mg/day and increased by 20 mg every 2 to 4 weeks if the patient was tolerating it but had not achieved remission, to a maximum dose of 60 mg/day. Treatment could be given for up to 14 weeks, during which side effects22 and clinical ratings23 were assessed by both patients and study coordinators.
Measurement-based care
We used a systematic approach to treatment called “measurement-based care,”24 which involves routinely measuring symptoms23 and side effects22 and using this information to modify the medication doses at critical decision points. This algorithmic approach provided flexible treatment recommendations to ensure that the dosage and duration of antidepressant drug treatment were adequate.25
The severity of depression was assessed by the clinician-rated, 16-item Quick Inventory of Depressive Symptomatology (QIDS-C16). The QIDS-SR16 (the self-report version) can substitute for the QIDS-C1623 to make this approach more feasible. Both tools are available at www.ids-qids.org.
This approach was easily worked into busy primary care and specialty care office workflows (clinic physicians, most with limited research experience, provided the treatment), and could be translated into primary care practice in the community as well.
Four-step protocol
A unique feature of the study design was that the patients, in consultation with their physicians, had some choice in the treatments they received. In this “equipoise-stratified randomized design,”26 at levels 2 and 3 the patient could choose either to switch therapies (stop the current drug and be randomized to receive one of several different treatments) or to augment their current therapy (by adding one of several treatments in a randomized fashion). Patients could decline certain strategies as long as there were at least two possible options to which one might be randomized.
At level 2, one of the options for both switching and augmentation was cognitive therapy, although patients could decline that option. Conversely, if they definitely wanted cognitive therapy, they could choose to be randomized to either cognitive therapy alone or to cognitive therapy added to citalopram. Also, anyone who received cognitive therapy in level 2 and failed to enter remission was additionally randomized to either bupropion or venlafaxine (level 2a) to ensure that all patients had failed trials on two medications before entering level 3.
When switching to medications other than a monoamine oxidase inhibitor (MAOI), the clinician could choose either to stop the current medication and immediately begin the next one, or to decrease the current medication while starting the new one at a low dose and then tapering and titrating over 1 week. (Switching to an MAOI, used only in the final level of treatment, required a 7- to 10-day washout period.)
Outcomes measured
Remission (complete recovery from the depressive episode), the primary study outcome, was defined as a HAM-D17 score of 7 or less, as assessed by treatment-blinded raters.A secondary remission outcome was a QIDS-SR16 score of 5 or less. Of note, the HAM-D17 remission rates were slightly lower than the rates based on the QIDS-SR16, since patients who did not have a HAM-D17 score measured at exit were defined as not being in remission a priori. Thus, the QIDS-SR16 rates might have been a slightly better reflection of actual remission rates.
Response, a secondary outcome, was defined as a reduction of at least 50% in the QIDS-SR16 score from baseline at the last assessment.
FEW DIFFERENCES BETWEEN PSYCHIATRIC, PRIMARY CARE PATIENTS
The patients seen in primary care clinics were surprisingly similar to those seen in psychiatric clinics.27,28 The two groups did not differ in severity of depression, distribution of severity scores, the likelihood of presenting with any of the nine core criteria of a major depressive episode, or the likelihood of having a concomitant axis I psychiatric disorder in addition to depression (about half of participants in each setting had an anxiety disorder).
Recurrent major depressive disorders were common in both groups, though more so in psychiatric patients (78% vs 69%, P < .001), while chronic depression was more common in primary care than in psychiatric patients (30% vs 21%, P < .001). Having either a chronic index episode (ie, lasting > 2 years) or a recurrent major depressive disorder was common in both groups (86% vs 83%, P = .0067).
That said, primary care patients were older (44 years vs 39 years, P < .001), more of them were Hispanic (18% vs 9%, P < .001), and more of them had public insurance (23% vs 9%, P < .001). Fewer of the primary care patients had completed college (20% vs 28%, P < .001), and the primary care patients tended to have greater medical comorbidity. Psychiatric patients were more likely to have attempted suicide in the past and to have had their first depressive illness before age 18.
LEVEL 1: WHAT CAN WE EXPECT FROM INITIAL TREATMENT?
At level 1, all the patients received citalopram. The mean dose was 40.6 ± 16.6 mg/day in the primary care clinics and 42.5 ± 16.8 mg/day in the psychiatric clinics, which are adequate, middle-range doses and higher than the average US dose.29
Approximately 30% of patients achieved remission: 27% as measured on the HAM-D17 and 33% on the QIDS-SR16. The response rate (on the QIDS-SR16) was 47%. There were no differences between primary and psychiatric care settings in remission or response rates.
Patients were more likely to achieve remission if they were white, female, employed, more educated, or wealthier. Longer current episodes, more concurrent psychiatric disorders (especially anxiety disorders or drug abuse), more general medical disorders, and lower baseline function and quality of life were each associated with lower remission rates.
What is an adequate trial?
Longer times than expected were needed to reach response or remission. The average duration required to achieve remission was almost 7 weeks (44 days in primary care; 49 days in psychiatric care). Further, approximately one-third of those who ultimately responded and half of those who entered remission did so after 6 weeks.30 Forty percent of those who entered remission required 8 or more weeks to do so.
These results suggest that longer treatment durations and more vigorous medication dosing than generally used are needed to achieve optimal remission rates. It is imprudent to stop a treatment that the patient is tolerating in a robust dose if the patient reports only partial benefit by 6 weeks; indeed, raising the dose, if tolerated, may help a substantial number of patients respond by 12 or 14 weeks. Instruments to monitor depression severity (eg, self-report measures) can be useful. At least 8 weeks with at least moderately vigorous dosing is recommended.
LEVEL 2: IF THE FIRST TREATMENT FAILS
When switching to a new drug, does it matter which one?
No.
In level 2, if patients had not achieved remission on citalopram alone, they had the choice of switching: stopping citalopram and being randomized to receive either sertraline (Zoloft, another SSRI), venlafaxine extended-release (XR) (Effexor XR, a serotonin and norepinephrine reuptake inhibitor), or bupropion sustained-release (SR) (Wellbutrin SR, a norepinephrine and dopamine reuptake inhibitor). At the last visit the mean daily doses were bupropion SR 282.7 mg/day, sertraline 135.5 mg/day, and venlafaxine-XR 193.6 mg/day.
The remission rate was approximately one-fourth with all three drugs31:
- With bupropion SR—21.3% by HAM-D17, 25.5% by QIDS-SR16
- With sertraline—17.6% by HAM-D17, 26.6% by QIDS-SR16
- With venlafaxine-XR—24.8% by HAM-D17, 25.0% by QIDS-SR16. The remission rates were neither statistically nor clinically different by either measure.
Though the types of side effects related to specific medications may have varied, the overall side-effect burden and the rate of serious adverse events did not differ significantly.
When adding a new drug, does it matter which one?
Again, no.
Instead of switching, patients in level 2 could choose to stay on citalopram and be randomized to add either bupropion SR or buspirone (BuSpar) to the regimen (augmentation). The mean daily doses at the end of level 2 were bupropion SR 267.5 mg and buspirone 40.9 mg.
Rates of remission32:
- With bupropion SR—29.7% on the HAMD-D17, 39.0% on the QIDS-SR16
- With buspirone—30.1% on the HAM-D17, 32.9% on the QIDS-SR16.
However, the QIDS-SR16 scores declined significantly more with bupropion SR than with buspirone (25.3% vs 17.1%, P < .04). The mean total QIDS-SR16 score at the last visit was lower with bupropion SR (8.0) than with buspirone (9.1, P < .02), and augmentation with bupropion SR was better tolerated (the dropout rate due to intolerance was 12.5% with bupropion-SR vs 20.6% with buspirone 20.6%; P < .009).
Can we directly compare the benefits of switching vs augmenting?
No.
Patients could choose whether to switch from citalopram to another drug or to add another drug at the second treatment level.33 Consequently, we could not ensure that the patient groups were equivalent at the point of randomization at the beginning of level 2, and, indeed, they were not.
Those who benefitted more from citalopram treatment and who better tolerated it preferred augmentation, while those who benefitted little or who could not tolerate it preferred to switch. Consequently, those in the augmentation group at level 2 were somewhat less depressed than those who switched. Whether augmentation is better even if the initial treatment is minimally effective could not be evaluated in STAR*D.
What about cognitive therapy?
There was no difference between cognitive therapy (either as a switch or as augmentation) and medication (as a switch or as augmentation).34 Adding another drug was more rapidly effective than adding cognitive therapy. Switching to cognitive therapy was better tolerated than switching to a different antidepressant.
Of note, fewer patients accepted cognitive therapy as a randomization option than we expected, so the sample sizes were small. Possible reasons were that all patients had to receive a medication at study entry (which may have biased selection towards those preferring medication), and cognitive therapy entailed additional copayments and visiting still another provider at another site.
After two levels of treatment, how many patients reach remission?
About 30% of patients in level 1 achieved remission, and of those progressing to level 2, another 30% achieved remission. Together, this adds up to about 50% of patients achieving remission if they remained in treatment (30% in level 1 plus 30% of the roughly 70% remaining in level 2).
IF A SECOND TREATMENT FAILS
If switching again to another drug, does it matter which one?
No.
In level 3, patients could choose to stop the drug they had been taking and be randomized to receive either mirtazapine (Remeron) or nortriptyline (Pamelor).
Switching medications was not as effective as a third step as it was as a second step.35
Remission rates:
- With mirtazapine—12.3% on the HAM-D17, 8.0% on the QIDS-SR16
- With nortriptyline—19.8% on the HAM-D17, 12.4% on the QIDS-SR16.
Response rates were 13.4% with mirtazapine and 16.5% with nortriptyline. Statistically, neither the response nor the remission rates differed by treatment, nor did these two treatments differ in tolerability or side-effect burden.
Does choice of augmentation agent matter: Lithium vs T3?
Similarly, after two failed medication treatments, medication augmentation was less effective than it was at the second step.36 The two augmentation options tested, lithium and T3 thyroid hormone (Cytomel), are commonly considered by psychiatrists but less commonly used by primary care doctors.
Lithium is believed to increase serotonergic function, which may have a synergistic effect on the mechanism of action of antidepressants; a meta-analysis of placebo-controlled studies supports lithium’s effectiveness as adjunctive treatment.37 Its side effects, however, must be closely monitored.38 The primary monitoring concern is the small difference between the therapeutic blood level (0.6–1.2 mEq/L) and potentially toxic blood levels (> 1.5 mEq/L).
Lithium was started at 450 mg/day, and at week 2 it was increased to the recommended dose of 900 mg/day (a dose below the target dose for bipolar disorder). If patients could not tolerate 450 mg/day, the initial dose was 225 mg/day for 1 week before being increased to 450 mg/day, still with the target dose of 900 mg/day. The mean exit dose was 859.9 mg/day, and the median blood level was 0.6 mEq/L.
Thyroid hormone augmentation using T3 is believed to work through both direct and indirect effects on the hypothalamic-pituitary-thyroid axis, which has a strong relationship with depression. The efficacy of T3 augmentation is supported by a meta-analysis of eight studies,39 and T3 is effective whether or not thyroid abnormalities are present.
In STAR*D, T3 was started at 25 μg/day for 1 week, than increased to the recommended dose of 50 μg/day. The mean exit dose was 45.2 μg/day.
Remission rates:
- With lithium augmentation—15.9% by the HAM-D17, 13.2% by the QIDS-SR16
- With T3 augmentation—24.7% by both measures.
Response rates were 16.2% with lithium augmentation and 23.3% with T3 augmentation.
While neither response nor remission rates were statistically significantly different by treatment, lithium was more frequently associated with side effects (P = .045), and more participants in the lithium group left treatment because of side effects (23.2% vs 9.6%; P = .027). These results suggest that in cases in which a clinician is considering an augmentation trial, T3 has slight advantages over lithium in effectiveness and tolerability. T3 also offers the advantages of being easy to use and not necessitating blood level monitoring. These latter benefits are especially relevant to the primary care physician. However, T3’s potential for long-term side effects (eg, osteoporosis, cardiovascular effects) were not examined, and it is not clear when to discontinue it.
LEVEL 4: AFTER THREE FAILURES, HOW SHOULD A CLINICIAN PROCEED?
Switch to mirtazapine plus venlafaxine XR or tranylcypromine?
Patients who reached level 4 were considered to have a highly treatment-resistant depressive illness, so treatments at this level were, by design, more aggressive. Accordingly, at level 4 we investigated treatments that might be considered more demanding than those a primary care physician would use. Approximately 40% of patients in each treatment group were from primary care settings.
Remission rates40:
- With the combination of mirtazapine (mean dose 35.7 mg/day) and venlafaxine XR (mean dose 210.3 mg/day)—13.7% by the HAM-D17 and 15.7% by the QIDS-SR16
- With the MAOI tranylcypromine (Parnate, mean dose 36.9 mg/day)—6.9% by the HAM-D17 and 13.8% by the QIDS-SR16. Response rates were 23.5% with the combination and 12.1% with tranylcypromine. Neither remission nor response rates differed significantly.
However, the percentage reduction in QIDS-SR16 score between baseline and exit was greater with the combination than with tranylcypromine. Further, more patients dropped out of treatment with tranylcypromine because of side effects (P < .03). Tranylcypromine also has the disadvantage of necessitating dietary restrictions.
A significant limitation of this comparison is that patients were less likely to get an adequate trial of tranylcypromine, an MAOI, than of the combination. When the 2-week washout period (required before switching to an MAOI) is subtracted from the total time in treatment, approximately 30% of participants in the tranylcypromine group had less than 2 weeks of treatment, and nearly half had less than 6 weeks of treatment.
Therefore, even though the remission and response rates were similar between groups, the combination of venlafaxine-XR plus mirtazapine therapy might have some advantages over tranylcypromine. These results provided the first evidence of tolerability and at least modest efficacy of this combination for treatment-resistant cases.
Overall, what was the cumulative remission rate?
The theoretical cumulative remission rate after four acute treatment steps was 67%. Remission was more likely to occur during the first two levels of treatment than during the last two. The cumulative remission rates for the first four steps were:
- Level 1—33%
- Level 2—57%
- Level 3—63%
- Level 4—67%.
RESULTS FROM LONG-TERM FOLLOW-UP AFTER REMISSION OR RESPONSE
Patients with a clinically meaningful response or, preferably, remission at any level could enter into a 12-month observational follow-up phase. Those who had required more treatment levels had higher relapse rates during this phase.41 Further, if a patient achieved remission rather than just response to treatment, regardless of the treatment level, the prognosis at follow-up was better, confirming the importance of remission as the goal of treatment.
Results also provided a warning—the greater the number of treatment levels that a patient required, the more likely that patient and physician would settle for response. Whether the greater relapse rates reflect a harder-to-treat depression or the naturalistic design of the follow-up phase (with less control over dosing) is unclear.
WHAT DO THESE RESULTS MEAN FOR PRIMARY CARE PHYSICIANS?
- Measurement-based care is feasible in primary care. Primary care doctors can ensure vigorous but tolerable dosing using a self-report depression scale to monitor response, a side-effects tool to monitor tolerability, and medication adjustments at critical decision points guided by these two measures.
- Remission, ie, complete recovery from a depressive episode, rather than merely substantial improvement, is associated with a better prognosis and is the preferred goal of treatment.
- Pharmacologic differences between psychotropic medications did not translate into substantial clinical differences, although tolerability differed. These findings are consistent with a large-scale systematic evidence review recently completed by the Agency for Healthcare Research and Quality that compared the effectiveness of antidepressants.42 Given the difficulty in predicting what medication will be both efficacious for and tolerated by an individual patient, familiarity with a broad spectrum of antidepressants is prudent.
- Remission of depressive episodes will most likely require repeated trials of sufficiently sustained,vigorously dosed antidepressant medication. From treatment initiation, physicians should ensure maximal but tolerable doses for at least 8 weeks before deciding that an intervention has failed.
- If a first treatment doesn’t work, either switching or augmenting it is a reasonable choice. Augmentation may be preferred if the patient is tolerating and receiving partial benefit from the initial medication choice. While bupropion SR and buspirone were not different as augmenters by the primary remission outcome measure, secondary measures (eg, tolerability, depressive symptom change over the course of treatment, clinician-rated Quick Inventory of Depressive Symptomatology) recommended bupropion-SR over buspirone.
- If physicians switch, either a within-class switch (eg, citalopram to sertraline) or an out-of-class switch (eg, citalopram to bupropion SR) is effective, as is a switch to a dual-action agent (eg, venlafaxine XR).
- The likelihood of improvement after two aggressive medication trials is very low and likely requires more complicated medication regimens, and the existing evidence base is quite thin. These primary care patients should likely be referred to psychiatrists for more aggressive and intensive treatment.
- For patients who present with major depressive disorder, STAR*D suggests that with persistence and aggressive yet feasible care, there is hope: after one round, approximately 30% will have a remission; after two rounds, 50%; after three rounds, 60%; and after four rounds, 70%.
- While STAR*D excluded depressed patients with bipolar disorder, a depressive episode in a patient with bipolar disorder can be difficult to distinguish from a depressive episode in a patient with major depressive disorder. Primary care physicians need to consider bipolar disorder both in patients presenting with a depressive episode and in those who fail an adequate trial.43
FUTURE CONSIDERATIONS
Subsequent STAR*D analyses will compare in greater depth outcomes in primary care vs psychiatric settings at each level of treatment. Given the greater risk of depression persistence associated with more successive levels of treatment, subsequent research will focus on ways to more successfully treat depression in the earlier stages, possibly through medication combinations earlier in treatment (somewhat analogous to a “broad-spectrum antibiotic” approach for infections).
- Kessler RC, Berglund P, Demler O, et al. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA 2003; 289:3095–3105.
- Murray CJ, Lopez AD. Global mortality, disability, and the contribution of risk factors: Global Burden of Disease Study. Lancet 1997; 349:1436–1442.
- Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990–2020: Global Burden of Disease Study. Lancet 1997; 349:1498–1504.
- Zimmerman M, Chelminski I, Posternak MA. Generalizability of antidepressant efficacy trials: differences between depressed psychiatric outpatients who would or would not qualify for an efficacy trial. Am J Psychiatry 2005; 162:1370–1372.
- Rothwell PM. External validity of randomised controlled trials: to whom do the results of this trial apply? Lancet 2005; 365:82–93.
- Depression Guideline Panel. Depression in primary care: Volume 1, diagnosis and detection. AHCPR publication No. 93-0550. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research; 1993.
- Frank E, Karp J, Rush A. Efficacy of treatments for major depression. Psychopharmacol Bull 1993; 29:457–475.
- Depression Guideline Panel. Depression in primary care: Volume 2, Treatment of major depression. AHCPR publication No. 93-0550. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research; 1993.
- Fava M, Davidson KG. Definition and epidemiology of treatment-resistant depression. Psychiatr Clin North Am 1996; 19:179–200.
- Jarrett RB, Rush A. Short-term psychotherapy of depressive disorders: current status and future directions. Psychiatry: Interpers Biol Process 1994; 57:115–132.
- American Psychiatric Association. Practice guideline for the treatment of patients with major depression (revision). Am J Psychiatry 2000; 157(suppl 4):1–45.
- Dunner DL, Rush AJ, Russell JM, et al. Prospective, long-term, multicenter study of the naturalistic outcomes of patients with treatment-resistant depression. J Clin Psychiatry 2006; 67:688–695.
- Fava M, Rush A, Trivedi M, et al. Background and rationale for the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study. Psychiatr Clin North Am 2003; 26:457–494.
- Gaynes B, Davis L, Rush A, Trivedi M, Fava M, Wisniewski S. The aims and design of the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) Study. Prim Psychiatry 2005; 12:36–41.
- Rush A, Fava M, Wisniewski S, et al. Sequenced Treatment Alternatives to Relieve Depression (STAR*D): rationale and design. Control Clin Trials 2004; 25:119–142.
- Stafford RS, Ausiello JC, Misra B, Saglam D. National Patterns o fDepression Treatment in Primary Care. Prim Care Companion J Clin Psychiatry 2000; 2:211–216.
- Regier D, Narrow W, Rae D, Mandersheid R, Locke B, Goodwin F. The de facto US mental and addictive disorders service system: epidemiologic catchment area prospective 1-year prevalence rates of disorders and services. Arch Gen Psychiatry 1993; 50:85–94.
- Pincus H, Tanielian T, Marcus S, et al. Prescribing trends in psychotropic medications: primary care, psychiatry, and other medical specialities. JAMA 1998; 279:526–531.
- Vuorilehto M, Melartin T, Isometsa E. Depressive disorders in primary care: recurrent, chronic, and co-morbid. Psychol Med 2005; 35:673–682.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fourth edition, Text Revision. Washington, DC: American Psychiatric Association; 2000.
- Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry 1960; 23:56–61.
- Wisniewski SR, Rush AJ, Balasubramani GK, Trivedi MH, Nierenberg AA for the STAR*D Investigators. Self-rated global measure of the frequency, intensity, and burden of side effects. J Psychiatric Pract 2006; 12:71–79.
- Rush AJ, Bernstein IH, Trivedi MH, et al. An evaluation of the Quick Inventory of Depressive Symptomatology and the Hamilton Rating Scale for Depression: a Sequenced Treatment Alternatives to Relieve Depression (STAR*D) trial report. Biol Psychiatry 2006; 59:493–501.
- Trivedi MH, Rush AJ, Gaynes BN, et al. Maximizing the adequacy of medication treatment in controlled trials and clinical practice: STAR*D measurement-based care. Neuropsychopharmacology 2007/04/04/online 2007.
- Kawamoto K, Houlihan CA, Balas EA, Lobach DF. Improving clinical practice using clinical decision support systems: a systematic review of trials to identify features critical to success. BMJ 2005; 330:765 e-pub March 14 2005.
- Lavori P, Rush A, Wisniewski S, et al. Strengthening clinical effectiveness trials: equipoise-stratified randomization. Biol Psychiatry 2001; 50:792–801.
- Gaynes BN, Rush AJ, Trivedi MH, et al. Major depression symptoms in primary care and psychiatric care settings: a cross-sectional analysis. Ann Fam Med 2007; 5:126–134.
- Gaynes BN, Rush AJ, Trivedi M, et al. A direct comparison of presenting characteristics of depressed outpatients from primary vs. specialty care settings: preliminary findings from the STAR*D clinical trial. Gen Hosp Psychiatry 2005; 27:87–96.
- Sullivan PW, Valuck R, Saseen J, MacFall HM. A comparison of the direct costs and cost effectiveness of serotonin reuptake inhibitors and associated adverse drug reactions. CNS Drugs 2004; 18:911–932.
- Trivedi MH, Rush AJ, Wisniewski SR, et al. Evaluation of outcomes with citalopram for depression using measurement-based care in STAR*D: implications for clinical practice. Am J Psychiatry 2006; 163:28–40.
- Rush AJ, Trivedi MH, Wisniewski SR, et al. Bupropion-SR, sertraline, or venlafaxine-XR after failure of SSRIs for depression. N Engl J Med 2006; 354:1231–1242.
- Trivedi MH, Fava M, Wisniewski SR, et al. Medication augmentation after the failure of SSRIs for depression. N Engl J Med 2006; 354:1243–1252.
- Wisniewski SR, Fava M, Trivedi MH, et al. Acceptability of second-step treatments to depressed outpatients: a STAR*D report. Am J Psychiatry 2007; 164:753–760.
- Thase ME, Friedman ES, Biggs MM, et al. Cognitive therapy versus medication in augmentation and switch strategies as second-step treatments: a STAR*D report. Am J Psychiatry 2007; 164:739–752.
- Fava M, Rush AJ, Wisniewski SR, et al. A comparison of mirtazapine and nortriptyline following two consecutive failed medication treatments for depressed outpatients: a STAR*D report. Am J Psychiatry 2006; 163:1161–1172.
- Nierenberg AA, Fava M, Trivedi MH, et al. A comparison of lithium and T3 augmentation following two failed medication treatments for depression: a STAR*D report. Am J Psychiatry 2006; 163:1519–1530.
- Bschor T, Lewitzka U, Sasse J, Adli M, Koberle U, Bauer M. Lithium augmentation in treatment-resistant depression: clinical evidence, serotonergic and endocrine mechanisms. Pharmacopsychiatry 2003; 36(suppl 3):S230–S234.
- Freeman MP, Freeman SA. Lithium: clinical considerations in internal medicine. Am J Med 2006; 119:478–481.
- Aronson R, Offman HJ, Joffe RT, Naylor CD. Triiodothyronine augmentation in the treatment of refractory depression. A meta-analysis. Arch Gen Psychiatry 1996; 53:842–848.
- McGrath PJ, Stewart JW, Fava M, et al. Tranylcypromine versus venlafaxine plus mirtazapine following three failed antidepressant medication trials for depression: a STAR*D report. Am J Psychiatry 2006; 163:1531–1541.
- Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. Am J Psychiatry 2006; 163:1905–1917.
- Gartlehner G, Hansen R, Thieda P, et al. Comparative Effectiveness of Second-generation Antidepressants in the Pharmacologic Treatment of Depression. Agency for Healthcare Research and Quality. http://effectivehealthcare.ahrq.gov/reports/topic.cfm?topic=8&sid=39&rType=3. Accessed December 12, 2007.
- Das AK, Olfson M, Gameroff MJ, et al. Screening for bipolar disorder in a primary care practice. JAMA 2005; 293:956–963.
- Kessler RC, Berglund P, Demler O, et al. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA 2003; 289:3095–3105.
- Murray CJ, Lopez AD. Global mortality, disability, and the contribution of risk factors: Global Burden of Disease Study. Lancet 1997; 349:1436–1442.
- Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990–2020: Global Burden of Disease Study. Lancet 1997; 349:1498–1504.
- Zimmerman M, Chelminski I, Posternak MA. Generalizability of antidepressant efficacy trials: differences between depressed psychiatric outpatients who would or would not qualify for an efficacy trial. Am J Psychiatry 2005; 162:1370–1372.
- Rothwell PM. External validity of randomised controlled trials: to whom do the results of this trial apply? Lancet 2005; 365:82–93.
- Depression Guideline Panel. Depression in primary care: Volume 1, diagnosis and detection. AHCPR publication No. 93-0550. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research; 1993.
- Frank E, Karp J, Rush A. Efficacy of treatments for major depression. Psychopharmacol Bull 1993; 29:457–475.
- Depression Guideline Panel. Depression in primary care: Volume 2, Treatment of major depression. AHCPR publication No. 93-0550. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research; 1993.
- Fava M, Davidson KG. Definition and epidemiology of treatment-resistant depression. Psychiatr Clin North Am 1996; 19:179–200.
- Jarrett RB, Rush A. Short-term psychotherapy of depressive disorders: current status and future directions. Psychiatry: Interpers Biol Process 1994; 57:115–132.
- American Psychiatric Association. Practice guideline for the treatment of patients with major depression (revision). Am J Psychiatry 2000; 157(suppl 4):1–45.
- Dunner DL, Rush AJ, Russell JM, et al. Prospective, long-term, multicenter study of the naturalistic outcomes of patients with treatment-resistant depression. J Clin Psychiatry 2006; 67:688–695.
- Fava M, Rush A, Trivedi M, et al. Background and rationale for the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study. Psychiatr Clin North Am 2003; 26:457–494.
- Gaynes B, Davis L, Rush A, Trivedi M, Fava M, Wisniewski S. The aims and design of the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) Study. Prim Psychiatry 2005; 12:36–41.
- Rush A, Fava M, Wisniewski S, et al. Sequenced Treatment Alternatives to Relieve Depression (STAR*D): rationale and design. Control Clin Trials 2004; 25:119–142.
- Stafford RS, Ausiello JC, Misra B, Saglam D. National Patterns o fDepression Treatment in Primary Care. Prim Care Companion J Clin Psychiatry 2000; 2:211–216.
- Regier D, Narrow W, Rae D, Mandersheid R, Locke B, Goodwin F. The de facto US mental and addictive disorders service system: epidemiologic catchment area prospective 1-year prevalence rates of disorders and services. Arch Gen Psychiatry 1993; 50:85–94.
- Pincus H, Tanielian T, Marcus S, et al. Prescribing trends in psychotropic medications: primary care, psychiatry, and other medical specialities. JAMA 1998; 279:526–531.
- Vuorilehto M, Melartin T, Isometsa E. Depressive disorders in primary care: recurrent, chronic, and co-morbid. Psychol Med 2005; 35:673–682.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fourth edition, Text Revision. Washington, DC: American Psychiatric Association; 2000.
- Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry 1960; 23:56–61.
- Wisniewski SR, Rush AJ, Balasubramani GK, Trivedi MH, Nierenberg AA for the STAR*D Investigators. Self-rated global measure of the frequency, intensity, and burden of side effects. J Psychiatric Pract 2006; 12:71–79.
- Rush AJ, Bernstein IH, Trivedi MH, et al. An evaluation of the Quick Inventory of Depressive Symptomatology and the Hamilton Rating Scale for Depression: a Sequenced Treatment Alternatives to Relieve Depression (STAR*D) trial report. Biol Psychiatry 2006; 59:493–501.
- Trivedi MH, Rush AJ, Gaynes BN, et al. Maximizing the adequacy of medication treatment in controlled trials and clinical practice: STAR*D measurement-based care. Neuropsychopharmacology 2007/04/04/online 2007.
- Kawamoto K, Houlihan CA, Balas EA, Lobach DF. Improving clinical practice using clinical decision support systems: a systematic review of trials to identify features critical to success. BMJ 2005; 330:765 e-pub March 14 2005.
- Lavori P, Rush A, Wisniewski S, et al. Strengthening clinical effectiveness trials: equipoise-stratified randomization. Biol Psychiatry 2001; 50:792–801.
- Gaynes BN, Rush AJ, Trivedi MH, et al. Major depression symptoms in primary care and psychiatric care settings: a cross-sectional analysis. Ann Fam Med 2007; 5:126–134.
- Gaynes BN, Rush AJ, Trivedi M, et al. A direct comparison of presenting characteristics of depressed outpatients from primary vs. specialty care settings: preliminary findings from the STAR*D clinical trial. Gen Hosp Psychiatry 2005; 27:87–96.
- Sullivan PW, Valuck R, Saseen J, MacFall HM. A comparison of the direct costs and cost effectiveness of serotonin reuptake inhibitors and associated adverse drug reactions. CNS Drugs 2004; 18:911–932.
- Trivedi MH, Rush AJ, Wisniewski SR, et al. Evaluation of outcomes with citalopram for depression using measurement-based care in STAR*D: implications for clinical practice. Am J Psychiatry 2006; 163:28–40.
- Rush AJ, Trivedi MH, Wisniewski SR, et al. Bupropion-SR, sertraline, or venlafaxine-XR after failure of SSRIs for depression. N Engl J Med 2006; 354:1231–1242.
- Trivedi MH, Fava M, Wisniewski SR, et al. Medication augmentation after the failure of SSRIs for depression. N Engl J Med 2006; 354:1243–1252.
- Wisniewski SR, Fava M, Trivedi MH, et al. Acceptability of second-step treatments to depressed outpatients: a STAR*D report. Am J Psychiatry 2007; 164:753–760.
- Thase ME, Friedman ES, Biggs MM, et al. Cognitive therapy versus medication in augmentation and switch strategies as second-step treatments: a STAR*D report. Am J Psychiatry 2007; 164:739–752.
- Fava M, Rush AJ, Wisniewski SR, et al. A comparison of mirtazapine and nortriptyline following two consecutive failed medication treatments for depressed outpatients: a STAR*D report. Am J Psychiatry 2006; 163:1161–1172.
- Nierenberg AA, Fava M, Trivedi MH, et al. A comparison of lithium and T3 augmentation following two failed medication treatments for depression: a STAR*D report. Am J Psychiatry 2006; 163:1519–1530.
- Bschor T, Lewitzka U, Sasse J, Adli M, Koberle U, Bauer M. Lithium augmentation in treatment-resistant depression: clinical evidence, serotonergic and endocrine mechanisms. Pharmacopsychiatry 2003; 36(suppl 3):S230–S234.
- Freeman MP, Freeman SA. Lithium: clinical considerations in internal medicine. Am J Med 2006; 119:478–481.
- Aronson R, Offman HJ, Joffe RT, Naylor CD. Triiodothyronine augmentation in the treatment of refractory depression. A meta-analysis. Arch Gen Psychiatry 1996; 53:842–848.
- McGrath PJ, Stewart JW, Fava M, et al. Tranylcypromine versus venlafaxine plus mirtazapine following three failed antidepressant medication trials for depression: a STAR*D report. Am J Psychiatry 2006; 163:1531–1541.
- Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. Am J Psychiatry 2006; 163:1905–1917.
- Gartlehner G, Hansen R, Thieda P, et al. Comparative Effectiveness of Second-generation Antidepressants in the Pharmacologic Treatment of Depression. Agency for Healthcare Research and Quality. http://effectivehealthcare.ahrq.gov/reports/topic.cfm?topic=8&sid=39&rType=3. Accessed December 12, 2007.
- Das AK, Olfson M, Gameroff MJ, et al. Screening for bipolar disorder in a primary care practice. JAMA 2005; 293:956–963.
KEY POINTS
- Remission (ie, complete relief from a depressive episode) rather than response (merely substantial improvement) should be the goal of treatment, as it is associated with a better prognosis and better function.
- Should the first treatment fail, either switching treat mentor augmenting the current treatment is reasonable.
- For most patients, remission will require repeated trials of sufficiently sustained, vigorously dosed antidepressant medication. Physicians should give maximal but tolerable doses for at least 8 weeks before deciding that an intervention has failed.
- After two well-delivered medication trials, the likelihood of remission substantially decreases. Such patients likely require more complicated regimens. Given the thin existing database, these patients are best referred to a psychiatrist for more complex treatments.
- With persistent and vigorous treatment, most patients will enter remission: about 33% after one step, 50% after two steps, 60% after three steps, and 70% after four steps (assuming patients stay in treatment).
Masquerade: Nonspinal musculoskeletal disorders that mimic spinal conditions
Not all pain in the neck or back actually originates from the spine. Sometimes pain in the neck or back is caused by a problem in the shoulder or hip or from peripheral nerve compression in the arms or legs.
This article focuses on the diagnostic features of common—and uncommon—nonspinal musculoskeletal problems that can masquerade as disorders of the spine. A myriad of nonmusculoskeletal disorders can also cause neck or back pain, but they are beyond the scope of this article. Medical disorders that can present as possible spinal problems have been reviewed in the December 2007 issue of the Cleveland Clinic Journal of Medicine.
CAUSE OF NECK OR BACK PAIN IS NOT ALWAYS OBVIOUS
Pain in the neck or back is one of the most common reasons for visits to primary care physicians.
Usually the diagnosis is straightforward, but atypical pain patterns frequently make the cause of the problem difficult to decipher.1 Axial neck or back pain is in many cases caused by problems in the joints, muscles, tendons, or ligaments of the arms or legs because the nerves in these structures arise from the spinal cord.2 Because these structures can move relative to one another, pain often varies with position, further confusing the picture.2 Despite these challenges, a correct diagnosis can usually be made on the basis of the history, physical examination, and ancillary testing.
NONSPINAL MUSCULOSKELETAL CAUSES OF NECK PAIN
Many shoulder problems present as neck pain
Shoulder problems frequently cause neck pain4 because the shoulder and neck are near the brachial plexus, which connects them. The shoulder joint is a complex of several structures; problems in any of them can present with specific features that can be distinguished from neck problems.5
In general, shoulder problems in older people are due to degenerative conditions, whereas younger people generally have problems arising from trauma, inflammation, or instability.1
Rotator cuff disease is one of the most common shoulder problems that can present with neck pain. The rotator cuff consists of four muscles—the supraspinatus, infraspinatus, subscapularis, and teres minor—which form a common tendon that attaches to the proximal humeral tuberosities and allows rotation of the arm at the glenohumeral joint.1 The rotator cuff probably undergoes both mechanical and biologic degeneration over time, making it prone to painful tears.
Rotator cuff tears can cause pain in the anterolateral or medial aspect of the shoulder or in the trapezius and neck area.1,6 Many older patients present with pain in the trapezius and paraspinal muscles.2,5,7 Many patients report pain when they raise the arms over their head or when they reach and hold the arm away from the body (eg, holding the steering wheel while driving), and at night while lying on the affected side.1
On physical examination, weakness of the rotator cuff muscles can be detected by externally rotating the shoulder or applying a downward force to the arm with the shoulder abducted 90 degrees, forward flexed 30 degrees, and internally rotated with the thumbs pointing to the ground.1
Magnetic resonance imaging (MRI) can very accurately diagnose a rotator cuff tear: diagnostic findings include a discontinuity and retraction in the rotator cuff tendon and edema.
Not all rotator cuff tears are symptomatic.6 If a rotator cuff tear is evident on MRI but the patient does not have pain at night or during overhead activity, then neck pain is more likely due to spinal disease.
Glenohumeral arthritis is another common shoulder problem that can cause axial neck pain.1 Most cases are idiopathic, although many patients have a history of rheumatoid arthritis, prior shoulder trauma, or glenohumeral instability for which they may have had surgery. Patients with shoulder arthritis usually also have arthritis in the cervical spine.
Patients report pain in the trapezius muscle and possibly a sensation of swelling around the shoulder joint, as well as difficulty with overhead activities such as combing hair or applying makeup.1
The most significant clinical finding is eliciting the shoulder pain with motion. Patients may also have limited range of motion accompanied by pain and crepitation.1

Humeral head osteonecrosis is a less common intra-articular problem that can cause neck pain. It occurs most frequently with human immunodeficiency virus infection, alcoholism, or corticosteroid use.8 Radiography shows sclerosis or collapse of the subchondral bone of the humeral head. MRI is best for detecting early changes of osteonecrosis.
Peripheral nerve compression may mimic cervical radiculopathy
Peripheral nerve compression is common and may present with paresthesias mimicking a cervical radiculopathy.9
Carpal tunnel syndrome usually presents with hand numbness and tingling or decreased sensation in the median nerve distribution (the radial three digits). Thenar atrophy is present in advanced cases.1,9 Carpal tunnel syndrome may also present with nonspecific hand pain or other symptoms. Chowet al9 found that 84% of patients with carpal tunnel syndrome had nocturnal hand paresthesias, 82% had paresthesias that were aggravated by hand activity, and 64% had hand pain. However, some patients with cervical spondylosis also had these symptoms: 10% had hand pain, 7% had nocturnal hand paresthesias, and 10% had paresthesias that were aggravated by hand activity.
Cubital tunnel syndrome can also present with radiating arm symptoms and is usually associated with pain at the elbow and a positive Tinel sign (ie, tapping over the cubital tunnel—at the elbow between the olecranon process and the medial epicondyle—elicits pain and tingling in the small and ring fingers).1 Electromyography and a nerve conduction study can help determine the diagnosis.
Suprascapular nerve impingement is another peripheral nerve problem that can mimic a cervical spine problem.1,10 The supraspinatus and infraspinatus muscles and can become entrapped by a ganglion cyst at the suprascapular notch of the scapula. The condition is more commonly seen in young, active patients who participate in overhead activities (eg, volleyball or tennis).
Chronic suprascapular nerve impingement can cause weakness and atrophy of the supraspinatus or infraspinatus muscles or both and can be detected on physical examination and confirmed by electromyography.1,10 Electromyography is best for diagnosing peripheral nerve compression: a decreased amplitude and increased latency indicates severe nerve compression. MRI can reveal a ganglion cyst if it is the source of nerve compression at the notch.
Brachial neuritis: Acute, severe neck or shoulder pain, followed by weakness
Brachial neuritis (Parsonage-Turner syndrome) presents with abrupt onset of intense pain in the neck or shoulder, mimicking a cervical spine radiculopathy. The pain typically improves over several days to weeks,11 but may be followed by weakness of the arm muscles. The cause of this condition is unclear.
Brachial neuritis characteristically involves multiple nerve roots and the rapid onset of severe pain.11 Cervical radiculopathy, on the other hand, usually starts insidiously and has a single dermatomal distribution. Another distinguishing feature is that neck movement typically exacerbates the symptoms of cervical radiculopathy but not of brachial neuritis.12 Brachial neuritis should be suspected in patients who have these features and who do not respond to conventional therapy.11
A mass can be detected with imaging studies
A mass in or around the shoulder can present as neck or arm pain by compressing or stretching nervous structures or connective tissues in the shoulder.13
Bony masses. Although most bony lesions in the shoulder are benign (osteochondromaor bone cysts), malignant osseous lesions such as metastatic disease and primary bone sarcomas also occur. Metastatic disease should be suspected in older patients with a history of malignancy, even if the presentation is atypical.13 Most bony lesions can be diagnosed by radiography or CT.
Soft tissue masses (eg, lipomas, elastofibromas, and sarcomas) can also cause a confusing pain pattern when they arise in the shoulder. They can be diagnosed with MRI.13
NONSPINAL MUSCULOSKELETAL CAUSES OF BACK PAIN
Hip and spine arthritis are commonly found together

Several studies found that if a patient has problems in both the spine and the hip, treating only one of the conditions may not relieve the pain.11,16,17 Birrell et al15 evaluated patients with concomitant hip and spinal disease and found that most patients who underwent total hip arthroplasty followed by spinal decompression had excellent results.
Other studies suggested that it is better to treat spinal stenosis first, because neurologic sequelae could result if it is left untreated.16 On the other hand, several other studies found that patients with symptoms and spinal stenosis seen by radiography can function for years without neurologic compromise.14,15,18 Conflicting data such as these make it difficult to determine whether hip disease or spinal disease should be treated first in patients with both conditions. Generally, the more symptomatic condition is treated first, unless a neurologic problem is progressing.
Recent studies examined clinical features that help distinguish symptomatic hip disease from spine disease in patients with concomitant radiographic hip and spine arthritis.15,18 Limping, groin pain, and limited and painful internal rotation of the hip strongly implicate the hip as the source of pain. Brown et al18 found that patients with a limp were seven times more likely to have pain from the hip alone or from the spine and hip combined than from the spine alone. Patients with groin pain or painful and limited internal rotation of the hip were 14 times more likely to have either the hip or the hip and spine as the source of pain. A positive straight-leg-raising sign or a contralateral straight-leg-raising sign strongly suggests the spine as the source of pain.12 (Straight-leg tests are performed with the patient lying on a table and the examiner lifting the leg while the knee is straight. The test is positive if pain is elicited between 30 and 70 degrees.)
Femoral necrosis or fractures are detectable by imaging
Femoral head osteonecrosis is another intra-articular hip process that can cause backpain.13 As is also true of osteonecrosis of the shoulder, patients who abuse alcohol or take corticosteroids are at increased risk. Recently, human immunodeficiency virus has also been associated with this condition.
Femoral head osteonecrosis typically presents with insidiously worsening reduction of hip rotation and pain in the buttock, thigh, and groin. The pain is not in a dermatomal pattern and is usually unilateral but can be bilateral.18
Radiographs can be diagnostic for femoral head collapse in late disease. MRI is best for diagnosing early disease before collapse occurs.
Occult or impending femoral neck fracture (ie, in metastatic or metabolic bone disease) usually presents with groin pain, similar to hip osteoarthritis and osteonecrosis,13 but it can also present with vague back pain with or without groin pain. The pain is produced by weight-bearing on the affected leg. Young patients with femoral neck stress fractures or primary benign bone lesions of the hip can also present with buttock pain that can be misinterpreted as coming from the back.
MRI of the pelvis and proximal femur is best for diagnosing a stress fracture and some bone lesions, because they are often not visible on radiographs.
Because the rate of osteonecrosis is very high in displaced femoral neck fractures, it is important that an impending fracture be detected and treated before a complete fracture occurs.
Hip dysplasia requires early treatment
Hip dysplasia, in which the hip joint does not develop normally, can present as back, buttock, and groin pain in young patients. Back pain may be caused by asymmetric spinal loading and abnormal muscular tension in the lumbar spine.13 Early diagnosis is important so that it can be surgically treated (with osteotomies of the proximal femur or pelvis, or both) to preserve hip function.
Piriformis syndrome occurs in athletic patients
Piriformis syndrome, which mimics sciatica from a spinal cause, is controversial because the diagnosis must be based on history and clinical findings without any objective imaging or electrodiagnostic testing. The condition is thought to be caused by sciatic nerve entrapment and compression under the piriformis muscle, which externally rotates the hip and may become swollen and inflamed inactive, athletic people.13,16
The diagnosis is confirmed on physical examination if the pain is replicated when the piriformis muscle is stretched by externally rotating the hip (ie, with the patient supine, flexing the affected hip and knee and pulling the ipsilateral knee toward the contralateral shoulder).13,16
Imaging studies of the spine or hip are notd iagnostic but should be done to look for other possible causes of the pain.
Some patients with this condition are helped by exercises to stretch the hip muscles, particularly the external rotators.
Bursitis causes localized tenderness
Trochanteric bursitis is a fairly common soft-tissue problem that can cause pain along the lateral aspect of the hip and proximal thigh. Unlike radiculopathy, the condition causes localized tenderness over the greater trochanter.
Ischial bursitis can cause back pain and can be differentiated from spinal pathology by localized tenderness over the ischial tuberosity.
Peripheral nerve compression can cause radicular pain
Peripheral nerve compression in and around the leg can cause radicular pain that mimics lumbar spine pathology.
The lateral femoral cutaneous nerve, if compressed and irritated as it exits the pelvis, can cause meralgia paresthetica, which is characterized by pain, numbness, and tinglingin the anterolateral proximal thigh, mimicking an L1 or L2 radiculopathy. Many patients report that the pain worsens when they wear a belt or tight pants and improves when they remove or loosen them.
The saphenous and peroneal nerves can be compressed around the knee, causing paresthesias in the medial and lateral aspect of the knee and leg, respectively, mimicking a radiculopathy of the nerve roots at L3-L4 (saphenous nerve) and L5 (peroneal nerve).
The tibial nerve can be compressed in the tarsal tunnel on the medial aspect of the ankle, causing distal paresthesias in the medial aspect of the foot, mimicking radiculopathy at L4-L5.
Stimulating the area of nerve compression by external compression or tapping with the examiner’s fingers generally causes paresthesias and aggravates the symptoms. Electromyography can also help with diagnosis.
- McFarland EG. Examination of the Shoulder: The Complete Guide. New York: Thieme; 2006.
- Macnab I, McCulloch J. Neck Ache and Shoulder Pain. Baltimore: Williams & Wilkins; 1994.
- Tong HC, Haig AJ, Yamakawa K. The Spurling test and cervical radiculopathy. Spine 2002; 27:156–159.
- Gorski JM, Schwartz LH. Shoulder impingement presenting as neck pain. J Bone Joint Surg Am 2003; 85-A:635–638.
- Borenstein DG, Wiesel SW, Boden SD. Neck Pain: Medical Diagnosis and Comprehensive Management. Philadelphia: WB Saunders; 1996.
- Spindler KP, Dovan TT, McCarty EC. Assessment and management of the painful shoulder. Clin Cornerstone 2001; 3:26–37.
- Margoles MS. The pain chart: spatial properties of pain. In: Melzack R,editor. Pain Measurement and Assessment. New York: Raven Press; 1983:215–225.
- Pateder DB, Park HB, Chronopoulos E, Fayad LM, McFarland EG.Humeral head osteonecrosis after anterior shoulder stabilization in an adolescent. A case report. J Bone Joint Surg Am 2004; 86-A:2290–2293.
- Chow CS, Hung LK, Chiu CP, et al. Is symptomatology useful in distinguishing between carpal tunnel syndrome and cervical spondylosis? Hand Surg 2005; 10:1–5.
- Johnson TR. Shoulder. In: Snider RK, editor. Essentials of Musculoskeletal Care. 1st ed. Rosemont, Ill.: American Academy of Orthopaedic Surgeons; 1997.
- Mamula CJ, Erhard RE, Piva SR. Cervical radiculopathy or Parsonage-Turner syndrome: differential diagnosis of a patient with neck and upper extremity symptoms. J Orthop Sports Phys Ther 2005; 35:659–664.
- Hoppenfeld S. Physical Examination of the Spine and Extremities. New York: Appleton-Century-Crofts; 1976.
- McCarthy EF, Frassica FJ. Pathology of Bone and Joint Disorders: With Clinical and Radiographic Correlation. Philadelphia: WB Saunders; 1998.
- Borenstein D. Does osteoarthritis of the lumbar spine cause chronic low back pain? Curr Pain Headache Rep 2004; 8:512–517.
- Birrell F, Lunt M, Macfarlane G, Silman A. Association between pain in the hip region and radiographic changes of osteoarthritis: results from a population-based study. Rheumatology (Oxford) 2005; 44:337–341. Erratum in: Rheumatology (Oxford) 2005; 44:569.
- Papadopoulos EC, Khan SN. Piriformis syndrome and low back pain: a new classification and review of the literature. Orthop Clin North Am 2004; 35:65–71.
- Offierski CM, MacNab I. Hip-spine syndrome. Spine 1983; 8:316–321.
- Brown MD, Gomez-Marin O, Brookfield KF, Li PS. Differential diagnosis of hip disease versus spine disease. Clin Orthop Relat Res 2004; 419:280–284.
Not all pain in the neck or back actually originates from the spine. Sometimes pain in the neck or back is caused by a problem in the shoulder or hip or from peripheral nerve compression in the arms or legs.
This article focuses on the diagnostic features of common—and uncommon—nonspinal musculoskeletal problems that can masquerade as disorders of the spine. A myriad of nonmusculoskeletal disorders can also cause neck or back pain, but they are beyond the scope of this article. Medical disorders that can present as possible spinal problems have been reviewed in the December 2007 issue of the Cleveland Clinic Journal of Medicine.
CAUSE OF NECK OR BACK PAIN IS NOT ALWAYS OBVIOUS
Pain in the neck or back is one of the most common reasons for visits to primary care physicians.
Usually the diagnosis is straightforward, but atypical pain patterns frequently make the cause of the problem difficult to decipher.1 Axial neck or back pain is in many cases caused by problems in the joints, muscles, tendons, or ligaments of the arms or legs because the nerves in these structures arise from the spinal cord.2 Because these structures can move relative to one another, pain often varies with position, further confusing the picture.2 Despite these challenges, a correct diagnosis can usually be made on the basis of the history, physical examination, and ancillary testing.
NONSPINAL MUSCULOSKELETAL CAUSES OF NECK PAIN
Many shoulder problems present as neck pain
Shoulder problems frequently cause neck pain4 because the shoulder and neck are near the brachial plexus, which connects them. The shoulder joint is a complex of several structures; problems in any of them can present with specific features that can be distinguished from neck problems.5
In general, shoulder problems in older people are due to degenerative conditions, whereas younger people generally have problems arising from trauma, inflammation, or instability.1
Rotator cuff disease is one of the most common shoulder problems that can present with neck pain. The rotator cuff consists of four muscles—the supraspinatus, infraspinatus, subscapularis, and teres minor—which form a common tendon that attaches to the proximal humeral tuberosities and allows rotation of the arm at the glenohumeral joint.1 The rotator cuff probably undergoes both mechanical and biologic degeneration over time, making it prone to painful tears.
Rotator cuff tears can cause pain in the anterolateral or medial aspect of the shoulder or in the trapezius and neck area.1,6 Many older patients present with pain in the trapezius and paraspinal muscles.2,5,7 Many patients report pain when they raise the arms over their head or when they reach and hold the arm away from the body (eg, holding the steering wheel while driving), and at night while lying on the affected side.1
On physical examination, weakness of the rotator cuff muscles can be detected by externally rotating the shoulder or applying a downward force to the arm with the shoulder abducted 90 degrees, forward flexed 30 degrees, and internally rotated with the thumbs pointing to the ground.1
Magnetic resonance imaging (MRI) can very accurately diagnose a rotator cuff tear: diagnostic findings include a discontinuity and retraction in the rotator cuff tendon and edema.
Not all rotator cuff tears are symptomatic.6 If a rotator cuff tear is evident on MRI but the patient does not have pain at night or during overhead activity, then neck pain is more likely due to spinal disease.
Glenohumeral arthritis is another common shoulder problem that can cause axial neck pain.1 Most cases are idiopathic, although many patients have a history of rheumatoid arthritis, prior shoulder trauma, or glenohumeral instability for which they may have had surgery. Patients with shoulder arthritis usually also have arthritis in the cervical spine.
Patients report pain in the trapezius muscle and possibly a sensation of swelling around the shoulder joint, as well as difficulty with overhead activities such as combing hair or applying makeup.1
The most significant clinical finding is eliciting the shoulder pain with motion. Patients may also have limited range of motion accompanied by pain and crepitation.1
Humeral head osteonecrosis is a less common intra-articular problem that can cause neck pain. It occurs most frequently with human immunodeficiency virus infection, alcoholism, or corticosteroid use.8 Radiography shows sclerosis or collapse of the subchondral bone of the humeral head. MRI is best for detecting early changes of osteonecrosis.
Peripheral nerve compression may mimic cervical radiculopathy
Peripheral nerve compression is common and may present with paresthesias mimicking a cervical radiculopathy.9
Carpal tunnel syndrome usually presents with hand numbness and tingling or decreased sensation in the median nerve distribution (the radial three digits). Thenar atrophy is present in advanced cases.1,9 Carpal tunnel syndrome may also present with nonspecific hand pain or other symptoms. Chowet al9 found that 84% of patients with carpal tunnel syndrome had nocturnal hand paresthesias, 82% had paresthesias that were aggravated by hand activity, and 64% had hand pain. However, some patients with cervical spondylosis also had these symptoms: 10% had hand pain, 7% had nocturnal hand paresthesias, and 10% had paresthesias that were aggravated by hand activity.
Cubital tunnel syndrome can also present with radiating arm symptoms and is usually associated with pain at the elbow and a positive Tinel sign (ie, tapping over the cubital tunnel—at the elbow between the olecranon process and the medial epicondyle—elicits pain and tingling in the small and ring fingers).1 Electromyography and a nerve conduction study can help determine the diagnosis.
Suprascapular nerve impingement is another peripheral nerve problem that can mimic a cervical spine problem.1,10 The supraspinatus and infraspinatus muscles and can become entrapped by a ganglion cyst at the suprascapular notch of the scapula. The condition is more commonly seen in young, active patients who participate in overhead activities (eg, volleyball or tennis).
Chronic suprascapular nerve impingement can cause weakness and atrophy of the supraspinatus or infraspinatus muscles or both and can be detected on physical examination and confirmed by electromyography.1,10 Electromyography is best for diagnosing peripheral nerve compression: a decreased amplitude and increased latency indicates severe nerve compression. MRI can reveal a ganglion cyst if it is the source of nerve compression at the notch.
Brachial neuritis: Acute, severe neck or shoulder pain, followed by weakness
Brachial neuritis (Parsonage-Turner syndrome) presents with abrupt onset of intense pain in the neck or shoulder, mimicking a cervical spine radiculopathy. The pain typically improves over several days to weeks,11 but may be followed by weakness of the arm muscles. The cause of this condition is unclear.
Brachial neuritis characteristically involves multiple nerve roots and the rapid onset of severe pain.11 Cervical radiculopathy, on the other hand, usually starts insidiously and has a single dermatomal distribution. Another distinguishing feature is that neck movement typically exacerbates the symptoms of cervical radiculopathy but not of brachial neuritis.12 Brachial neuritis should be suspected in patients who have these features and who do not respond to conventional therapy.11
A mass can be detected with imaging studies
A mass in or around the shoulder can present as neck or arm pain by compressing or stretching nervous structures or connective tissues in the shoulder.13
Bony masses. Although most bony lesions in the shoulder are benign (osteochondromaor bone cysts), malignant osseous lesions such as metastatic disease and primary bone sarcomas also occur. Metastatic disease should be suspected in older patients with a history of malignancy, even if the presentation is atypical.13 Most bony lesions can be diagnosed by radiography or CT.
Soft tissue masses (eg, lipomas, elastofibromas, and sarcomas) can also cause a confusing pain pattern when they arise in the shoulder. They can be diagnosed with MRI.13
NONSPINAL MUSCULOSKELETAL CAUSES OF BACK PAIN
Hip and spine arthritis are commonly found together
Several studies found that if a patient has problems in both the spine and the hip, treating only one of the conditions may not relieve the pain.11,16,17 Birrell et al15 evaluated patients with concomitant hip and spinal disease and found that most patients who underwent total hip arthroplasty followed by spinal decompression had excellent results.
Other studies suggested that it is better to treat spinal stenosis first, because neurologic sequelae could result if it is left untreated.16 On the other hand, several other studies found that patients with symptoms and spinal stenosis seen by radiography can function for years without neurologic compromise.14,15,18 Conflicting data such as these make it difficult to determine whether hip disease or spinal disease should be treated first in patients with both conditions. Generally, the more symptomatic condition is treated first, unless a neurologic problem is progressing.
Recent studies examined clinical features that help distinguish symptomatic hip disease from spine disease in patients with concomitant radiographic hip and spine arthritis.15,18 Limping, groin pain, and limited and painful internal rotation of the hip strongly implicate the hip as the source of pain. Brown et al18 found that patients with a limp were seven times more likely to have pain from the hip alone or from the spine and hip combined than from the spine alone. Patients with groin pain or painful and limited internal rotation of the hip were 14 times more likely to have either the hip or the hip and spine as the source of pain. A positive straight-leg-raising sign or a contralateral straight-leg-raising sign strongly suggests the spine as the source of pain.12 (Straight-leg tests are performed with the patient lying on a table and the examiner lifting the leg while the knee is straight. The test is positive if pain is elicited between 30 and 70 degrees.)
Femoral necrosis or fractures are detectable by imaging
Femoral head osteonecrosis is another intra-articular hip process that can cause backpain.13 As is also true of osteonecrosis of the shoulder, patients who abuse alcohol or take corticosteroids are at increased risk. Recently, human immunodeficiency virus has also been associated with this condition.
Femoral head osteonecrosis typically presents with insidiously worsening reduction of hip rotation and pain in the buttock, thigh, and groin. The pain is not in a dermatomal pattern and is usually unilateral but can be bilateral.18
Radiographs can be diagnostic for femoral head collapse in late disease. MRI is best for diagnosing early disease before collapse occurs.
Occult or impending femoral neck fracture (ie, in metastatic or metabolic bone disease) usually presents with groin pain, similar to hip osteoarthritis and osteonecrosis,13 but it can also present with vague back pain with or without groin pain. The pain is produced by weight-bearing on the affected leg. Young patients with femoral neck stress fractures or primary benign bone lesions of the hip can also present with buttock pain that can be misinterpreted as coming from the back.
MRI of the pelvis and proximal femur is best for diagnosing a stress fracture and some bone lesions, because they are often not visible on radiographs.
Because the rate of osteonecrosis is very high in displaced femoral neck fractures, it is important that an impending fracture be detected and treated before a complete fracture occurs.
Hip dysplasia requires early treatment
Hip dysplasia, in which the hip joint does not develop normally, can present as back, buttock, and groin pain in young patients. Back pain may be caused by asymmetric spinal loading and abnormal muscular tension in the lumbar spine.13 Early diagnosis is important so that it can be surgically treated (with osteotomies of the proximal femur or pelvis, or both) to preserve hip function.
Piriformis syndrome occurs in athletic patients
Piriformis syndrome, which mimics sciatica from a spinal cause, is controversial because the diagnosis must be based on history and clinical findings without any objective imaging or electrodiagnostic testing. The condition is thought to be caused by sciatic nerve entrapment and compression under the piriformis muscle, which externally rotates the hip and may become swollen and inflamed inactive, athletic people.13,16
The diagnosis is confirmed on physical examination if the pain is replicated when the piriformis muscle is stretched by externally rotating the hip (ie, with the patient supine, flexing the affected hip and knee and pulling the ipsilateral knee toward the contralateral shoulder).13,16
Imaging studies of the spine or hip are notd iagnostic but should be done to look for other possible causes of the pain.
Some patients with this condition are helped by exercises to stretch the hip muscles, particularly the external rotators.
Bursitis causes localized tenderness
Trochanteric bursitis is a fairly common soft-tissue problem that can cause pain along the lateral aspect of the hip and proximal thigh. Unlike radiculopathy, the condition causes localized tenderness over the greater trochanter.
Ischial bursitis can cause back pain and can be differentiated from spinal pathology by localized tenderness over the ischial tuberosity.
Peripheral nerve compression can cause radicular pain
Peripheral nerve compression in and around the leg can cause radicular pain that mimics lumbar spine pathology.
The lateral femoral cutaneous nerve, if compressed and irritated as it exits the pelvis, can cause meralgia paresthetica, which is characterized by pain, numbness, and tinglingin the anterolateral proximal thigh, mimicking an L1 or L2 radiculopathy. Many patients report that the pain worsens when they wear a belt or tight pants and improves when they remove or loosen them.
The saphenous and peroneal nerves can be compressed around the knee, causing paresthesias in the medial and lateral aspect of the knee and leg, respectively, mimicking a radiculopathy of the nerve roots at L3-L4 (saphenous nerve) and L5 (peroneal nerve).
The tibial nerve can be compressed in the tarsal tunnel on the medial aspect of the ankle, causing distal paresthesias in the medial aspect of the foot, mimicking radiculopathy at L4-L5.
Stimulating the area of nerve compression by external compression or tapping with the examiner’s fingers generally causes paresthesias and aggravates the symptoms. Electromyography can also help with diagnosis.
Not all pain in the neck or back actually originates from the spine. Sometimes pain in the neck or back is caused by a problem in the shoulder or hip or from peripheral nerve compression in the arms or legs.
This article focuses on the diagnostic features of common—and uncommon—nonspinal musculoskeletal problems that can masquerade as disorders of the spine. A myriad of nonmusculoskeletal disorders can also cause neck or back pain, but they are beyond the scope of this article. Medical disorders that can present as possible spinal problems have been reviewed in the December 2007 issue of the Cleveland Clinic Journal of Medicine.
CAUSE OF NECK OR BACK PAIN IS NOT ALWAYS OBVIOUS
Pain in the neck or back is one of the most common reasons for visits to primary care physicians.
Usually the diagnosis is straightforward, but atypical pain patterns frequently make the cause of the problem difficult to decipher.1 Axial neck or back pain is in many cases caused by problems in the joints, muscles, tendons, or ligaments of the arms or legs because the nerves in these structures arise from the spinal cord.2 Because these structures can move relative to one another, pain often varies with position, further confusing the picture.2 Despite these challenges, a correct diagnosis can usually be made on the basis of the history, physical examination, and ancillary testing.
NONSPINAL MUSCULOSKELETAL CAUSES OF NECK PAIN
Many shoulder problems present as neck pain
Shoulder problems frequently cause neck pain4 because the shoulder and neck are near the brachial plexus, which connects them. The shoulder joint is a complex of several structures; problems in any of them can present with specific features that can be distinguished from neck problems.5
In general, shoulder problems in older people are due to degenerative conditions, whereas younger people generally have problems arising from trauma, inflammation, or instability.1
Rotator cuff disease is one of the most common shoulder problems that can present with neck pain. The rotator cuff consists of four muscles—the supraspinatus, infraspinatus, subscapularis, and teres minor—which form a common tendon that attaches to the proximal humeral tuberosities and allows rotation of the arm at the glenohumeral joint.1 The rotator cuff probably undergoes both mechanical and biologic degeneration over time, making it prone to painful tears.
Rotator cuff tears can cause pain in the anterolateral or medial aspect of the shoulder or in the trapezius and neck area.1,6 Many older patients present with pain in the trapezius and paraspinal muscles.2,5,7 Many patients report pain when they raise the arms over their head or when they reach and hold the arm away from the body (eg, holding the steering wheel while driving), and at night while lying on the affected side.1
On physical examination, weakness of the rotator cuff muscles can be detected by externally rotating the shoulder or applying a downward force to the arm with the shoulder abducted 90 degrees, forward flexed 30 degrees, and internally rotated with the thumbs pointing to the ground.1
Magnetic resonance imaging (MRI) can very accurately diagnose a rotator cuff tear: diagnostic findings include a discontinuity and retraction in the rotator cuff tendon and edema.
Not all rotator cuff tears are symptomatic.6 If a rotator cuff tear is evident on MRI but the patient does not have pain at night or during overhead activity, then neck pain is more likely due to spinal disease.
Glenohumeral arthritis is another common shoulder problem that can cause axial neck pain.1 Most cases are idiopathic, although many patients have a history of rheumatoid arthritis, prior shoulder trauma, or glenohumeral instability for which they may have had surgery. Patients with shoulder arthritis usually also have arthritis in the cervical spine.
Patients report pain in the trapezius muscle and possibly a sensation of swelling around the shoulder joint, as well as difficulty with overhead activities such as combing hair or applying makeup.1
The most significant clinical finding is eliciting the shoulder pain with motion. Patients may also have limited range of motion accompanied by pain and crepitation.1
Humeral head osteonecrosis is a less common intra-articular problem that can cause neck pain. It occurs most frequently with human immunodeficiency virus infection, alcoholism, or corticosteroid use.8 Radiography shows sclerosis or collapse of the subchondral bone of the humeral head. MRI is best for detecting early changes of osteonecrosis.
Peripheral nerve compression may mimic cervical radiculopathy
Peripheral nerve compression is common and may present with paresthesias mimicking a cervical radiculopathy.9
Carpal tunnel syndrome usually presents with hand numbness and tingling or decreased sensation in the median nerve distribution (the radial three digits). Thenar atrophy is present in advanced cases.1,9 Carpal tunnel syndrome may also present with nonspecific hand pain or other symptoms. Chowet al9 found that 84% of patients with carpal tunnel syndrome had nocturnal hand paresthesias, 82% had paresthesias that were aggravated by hand activity, and 64% had hand pain. However, some patients with cervical spondylosis also had these symptoms: 10% had hand pain, 7% had nocturnal hand paresthesias, and 10% had paresthesias that were aggravated by hand activity.
Cubital tunnel syndrome can also present with radiating arm symptoms and is usually associated with pain at the elbow and a positive Tinel sign (ie, tapping over the cubital tunnel—at the elbow between the olecranon process and the medial epicondyle—elicits pain and tingling in the small and ring fingers).1 Electromyography and a nerve conduction study can help determine the diagnosis.
Suprascapular nerve impingement is another peripheral nerve problem that can mimic a cervical spine problem.1,10 The supraspinatus and infraspinatus muscles and can become entrapped by a ganglion cyst at the suprascapular notch of the scapula. The condition is more commonly seen in young, active patients who participate in overhead activities (eg, volleyball or tennis).
Chronic suprascapular nerve impingement can cause weakness and atrophy of the supraspinatus or infraspinatus muscles or both and can be detected on physical examination and confirmed by electromyography.1,10 Electromyography is best for diagnosing peripheral nerve compression: a decreased amplitude and increased latency indicates severe nerve compression. MRI can reveal a ganglion cyst if it is the source of nerve compression at the notch.
Brachial neuritis: Acute, severe neck or shoulder pain, followed by weakness
Brachial neuritis (Parsonage-Turner syndrome) presents with abrupt onset of intense pain in the neck or shoulder, mimicking a cervical spine radiculopathy. The pain typically improves over several days to weeks,11 but may be followed by weakness of the arm muscles. The cause of this condition is unclear.
Brachial neuritis characteristically involves multiple nerve roots and the rapid onset of severe pain.11 Cervical radiculopathy, on the other hand, usually starts insidiously and has a single dermatomal distribution. Another distinguishing feature is that neck movement typically exacerbates the symptoms of cervical radiculopathy but not of brachial neuritis.12 Brachial neuritis should be suspected in patients who have these features and who do not respond to conventional therapy.11
A mass can be detected with imaging studies
A mass in or around the shoulder can present as neck or arm pain by compressing or stretching nervous structures or connective tissues in the shoulder.13
Bony masses. Although most bony lesions in the shoulder are benign (osteochondromaor bone cysts), malignant osseous lesions such as metastatic disease and primary bone sarcomas also occur. Metastatic disease should be suspected in older patients with a history of malignancy, even if the presentation is atypical.13 Most bony lesions can be diagnosed by radiography or CT.
Soft tissue masses (eg, lipomas, elastofibromas, and sarcomas) can also cause a confusing pain pattern when they arise in the shoulder. They can be diagnosed with MRI.13
NONSPINAL MUSCULOSKELETAL CAUSES OF BACK PAIN
Hip and spine arthritis are commonly found together
Several studies found that if a patient has problems in both the spine and the hip, treating only one of the conditions may not relieve the pain.11,16,17 Birrell et al15 evaluated patients with concomitant hip and spinal disease and found that most patients who underwent total hip arthroplasty followed by spinal decompression had excellent results.
Other studies suggested that it is better to treat spinal stenosis first, because neurologic sequelae could result if it is left untreated.16 On the other hand, several other studies found that patients with symptoms and spinal stenosis seen by radiography can function for years without neurologic compromise.14,15,18 Conflicting data such as these make it difficult to determine whether hip disease or spinal disease should be treated first in patients with both conditions. Generally, the more symptomatic condition is treated first, unless a neurologic problem is progressing.
Recent studies examined clinical features that help distinguish symptomatic hip disease from spine disease in patients with concomitant radiographic hip and spine arthritis.15,18 Limping, groin pain, and limited and painful internal rotation of the hip strongly implicate the hip as the source of pain. Brown et al18 found that patients with a limp were seven times more likely to have pain from the hip alone or from the spine and hip combined than from the spine alone. Patients with groin pain or painful and limited internal rotation of the hip were 14 times more likely to have either the hip or the hip and spine as the source of pain. A positive straight-leg-raising sign or a contralateral straight-leg-raising sign strongly suggests the spine as the source of pain.12 (Straight-leg tests are performed with the patient lying on a table and the examiner lifting the leg while the knee is straight. The test is positive if pain is elicited between 30 and 70 degrees.)
Femoral necrosis or fractures are detectable by imaging
Femoral head osteonecrosis is another intra-articular hip process that can cause backpain.13 As is also true of osteonecrosis of the shoulder, patients who abuse alcohol or take corticosteroids are at increased risk. Recently, human immunodeficiency virus has also been associated with this condition.
Femoral head osteonecrosis typically presents with insidiously worsening reduction of hip rotation and pain in the buttock, thigh, and groin. The pain is not in a dermatomal pattern and is usually unilateral but can be bilateral.18
Radiographs can be diagnostic for femoral head collapse in late disease. MRI is best for diagnosing early disease before collapse occurs.
Occult or impending femoral neck fracture (ie, in metastatic or metabolic bone disease) usually presents with groin pain, similar to hip osteoarthritis and osteonecrosis,13 but it can also present with vague back pain with or without groin pain. The pain is produced by weight-bearing on the affected leg. Young patients with femoral neck stress fractures or primary benign bone lesions of the hip can also present with buttock pain that can be misinterpreted as coming from the back.
MRI of the pelvis and proximal femur is best for diagnosing a stress fracture and some bone lesions, because they are often not visible on radiographs.
Because the rate of osteonecrosis is very high in displaced femoral neck fractures, it is important that an impending fracture be detected and treated before a complete fracture occurs.
Hip dysplasia requires early treatment
Hip dysplasia, in which the hip joint does not develop normally, can present as back, buttock, and groin pain in young patients. Back pain may be caused by asymmetric spinal loading and abnormal muscular tension in the lumbar spine.13 Early diagnosis is important so that it can be surgically treated (with osteotomies of the proximal femur or pelvis, or both) to preserve hip function.
Piriformis syndrome occurs in athletic patients
Piriformis syndrome, which mimics sciatica from a spinal cause, is controversial because the diagnosis must be based on history and clinical findings without any objective imaging or electrodiagnostic testing. The condition is thought to be caused by sciatic nerve entrapment and compression under the piriformis muscle, which externally rotates the hip and may become swollen and inflamed inactive, athletic people.13,16
The diagnosis is confirmed on physical examination if the pain is replicated when the piriformis muscle is stretched by externally rotating the hip (ie, with the patient supine, flexing the affected hip and knee and pulling the ipsilateral knee toward the contralateral shoulder).13,16
Imaging studies of the spine or hip are notd iagnostic but should be done to look for other possible causes of the pain.
Some patients with this condition are helped by exercises to stretch the hip muscles, particularly the external rotators.
Bursitis causes localized tenderness
Trochanteric bursitis is a fairly common soft-tissue problem that can cause pain along the lateral aspect of the hip and proximal thigh. Unlike radiculopathy, the condition causes localized tenderness over the greater trochanter.
Ischial bursitis can cause back pain and can be differentiated from spinal pathology by localized tenderness over the ischial tuberosity.
Peripheral nerve compression can cause radicular pain
Peripheral nerve compression in and around the leg can cause radicular pain that mimics lumbar spine pathology.
The lateral femoral cutaneous nerve, if compressed and irritated as it exits the pelvis, can cause meralgia paresthetica, which is characterized by pain, numbness, and tinglingin the anterolateral proximal thigh, mimicking an L1 or L2 radiculopathy. Many patients report that the pain worsens when they wear a belt or tight pants and improves when they remove or loosen them.
The saphenous and peroneal nerves can be compressed around the knee, causing paresthesias in the medial and lateral aspect of the knee and leg, respectively, mimicking a radiculopathy of the nerve roots at L3-L4 (saphenous nerve) and L5 (peroneal nerve).
The tibial nerve can be compressed in the tarsal tunnel on the medial aspect of the ankle, causing distal paresthesias in the medial aspect of the foot, mimicking radiculopathy at L4-L5.
Stimulating the area of nerve compression by external compression or tapping with the examiner’s fingers generally causes paresthesias and aggravates the symptoms. Electromyography can also help with diagnosis.
- McFarland EG. Examination of the Shoulder: The Complete Guide. New York: Thieme; 2006.
- Macnab I, McCulloch J. Neck Ache and Shoulder Pain. Baltimore: Williams & Wilkins; 1994.
- Tong HC, Haig AJ, Yamakawa K. The Spurling test and cervical radiculopathy. Spine 2002; 27:156–159.
- Gorski JM, Schwartz LH. Shoulder impingement presenting as neck pain. J Bone Joint Surg Am 2003; 85-A:635–638.
- Borenstein DG, Wiesel SW, Boden SD. Neck Pain: Medical Diagnosis and Comprehensive Management. Philadelphia: WB Saunders; 1996.
- Spindler KP, Dovan TT, McCarty EC. Assessment and management of the painful shoulder. Clin Cornerstone 2001; 3:26–37.
- Margoles MS. The pain chart: spatial properties of pain. In: Melzack R,editor. Pain Measurement and Assessment. New York: Raven Press; 1983:215–225.
- Pateder DB, Park HB, Chronopoulos E, Fayad LM, McFarland EG.Humeral head osteonecrosis after anterior shoulder stabilization in an adolescent. A case report. J Bone Joint Surg Am 2004; 86-A:2290–2293.
- Chow CS, Hung LK, Chiu CP, et al. Is symptomatology useful in distinguishing between carpal tunnel syndrome and cervical spondylosis? Hand Surg 2005; 10:1–5.
- Johnson TR. Shoulder. In: Snider RK, editor. Essentials of Musculoskeletal Care. 1st ed. Rosemont, Ill.: American Academy of Orthopaedic Surgeons; 1997.
- Mamula CJ, Erhard RE, Piva SR. Cervical radiculopathy or Parsonage-Turner syndrome: differential diagnosis of a patient with neck and upper extremity symptoms. J Orthop Sports Phys Ther 2005; 35:659–664.
- Hoppenfeld S. Physical Examination of the Spine and Extremities. New York: Appleton-Century-Crofts; 1976.
- McCarthy EF, Frassica FJ. Pathology of Bone and Joint Disorders: With Clinical and Radiographic Correlation. Philadelphia: WB Saunders; 1998.
- Borenstein D. Does osteoarthritis of the lumbar spine cause chronic low back pain? Curr Pain Headache Rep 2004; 8:512–517.
- Birrell F, Lunt M, Macfarlane G, Silman A. Association between pain in the hip region and radiographic changes of osteoarthritis: results from a population-based study. Rheumatology (Oxford) 2005; 44:337–341. Erratum in: Rheumatology (Oxford) 2005; 44:569.
- Papadopoulos EC, Khan SN. Piriformis syndrome and low back pain: a new classification and review of the literature. Orthop Clin North Am 2004; 35:65–71.
- Offierski CM, MacNab I. Hip-spine syndrome. Spine 1983; 8:316–321.
- Brown MD, Gomez-Marin O, Brookfield KF, Li PS. Differential diagnosis of hip disease versus spine disease. Clin Orthop Relat Res 2004; 419:280–284.
- McFarland EG. Examination of the Shoulder: The Complete Guide. New York: Thieme; 2006.
- Macnab I, McCulloch J. Neck Ache and Shoulder Pain. Baltimore: Williams & Wilkins; 1994.
- Tong HC, Haig AJ, Yamakawa K. The Spurling test and cervical radiculopathy. Spine 2002; 27:156–159.
- Gorski JM, Schwartz LH. Shoulder impingement presenting as neck pain. J Bone Joint Surg Am 2003; 85-A:635–638.
- Borenstein DG, Wiesel SW, Boden SD. Neck Pain: Medical Diagnosis and Comprehensive Management. Philadelphia: WB Saunders; 1996.
- Spindler KP, Dovan TT, McCarty EC. Assessment and management of the painful shoulder. Clin Cornerstone 2001; 3:26–37.
- Margoles MS. The pain chart: spatial properties of pain. In: Melzack R,editor. Pain Measurement and Assessment. New York: Raven Press; 1983:215–225.
- Pateder DB, Park HB, Chronopoulos E, Fayad LM, McFarland EG.Humeral head osteonecrosis after anterior shoulder stabilization in an adolescent. A case report. J Bone Joint Surg Am 2004; 86-A:2290–2293.
- Chow CS, Hung LK, Chiu CP, et al. Is symptomatology useful in distinguishing between carpal tunnel syndrome and cervical spondylosis? Hand Surg 2005; 10:1–5.
- Johnson TR. Shoulder. In: Snider RK, editor. Essentials of Musculoskeletal Care. 1st ed. Rosemont, Ill.: American Academy of Orthopaedic Surgeons; 1997.
- Mamula CJ, Erhard RE, Piva SR. Cervical radiculopathy or Parsonage-Turner syndrome: differential diagnosis of a patient with neck and upper extremity symptoms. J Orthop Sports Phys Ther 2005; 35:659–664.
- Hoppenfeld S. Physical Examination of the Spine and Extremities. New York: Appleton-Century-Crofts; 1976.
- McCarthy EF, Frassica FJ. Pathology of Bone and Joint Disorders: With Clinical and Radiographic Correlation. Philadelphia: WB Saunders; 1998.
- Borenstein D. Does osteoarthritis of the lumbar spine cause chronic low back pain? Curr Pain Headache Rep 2004; 8:512–517.
- Birrell F, Lunt M, Macfarlane G, Silman A. Association between pain in the hip region and radiographic changes of osteoarthritis: results from a population-based study. Rheumatology (Oxford) 2005; 44:337–341. Erratum in: Rheumatology (Oxford) 2005; 44:569.
- Papadopoulos EC, Khan SN. Piriformis syndrome and low back pain: a new classification and review of the literature. Orthop Clin North Am 2004; 35:65–71.
- Offierski CM, MacNab I. Hip-spine syndrome. Spine 1983; 8:316–321.
- Brown MD, Gomez-Marin O, Brookfield KF, Li PS. Differential diagnosis of hip disease versus spine disease. Clin Orthop Relat Res 2004; 419:280–284.
KEY POINTS
- Neck pain is commonly caused by shoulder problems such as rotator cuff disease, glenohumeral arthritis, and humeral head osteonecrosis.
- Brachial neuritis involves acute, severe neck or shoulder pain, followed by weakness as pain resolves.
- Low back pain can be caused by hip or spine arthritis, femoral head osteonecrosis, an occult or impending femoral neck fracture, hip dysplasia, piriformis syndrome, and bursitis.
- Bony and soft tissue masses can be detected with imaging studies.
- Peripheral nerve compression can mimic cervical or lumbar spine radiculopathy. Electromyography and eliciting symptoms by tapping over the compressed nerve aid in making a diagnosis.
- Patients with human immunodeficiency virus infection, alcoholism, or corticosteroid use are at increased risk of developing osteonecrosis of the humeral or femoral head.
Fluid restriction is superior in acute lung injury and ARDS
Although most clinicians tend to manage acute lung injury (ALI) and acute respiratory distress syndrome (ARDS) by giving more rather than less fluid,1,2 patients may actually fare better under a strategy of limited fluid intake and increased fluid excretion.
According to the results of the Fluids and Catheters Treatment Trial (FACTT),3 patients managed with fluid restriction (the “dry” or conservative strategy) spent significantly less time in the intensive care unit (ICU) and on mechanical ventilation than did patients who received a high fluid intake (the “wet” or liberal strategy). These benefits of the conservative strategy were attained without any increase in the mortality rate at 60 days or in nonpulmonary organ failure at 28 days.
In this article, I discuss the basis for the FACTT researchers’ conclusion that a conservative fluid strategy is preferable to a liberal fluid strategy in ALI/ARDS.
STUDY RATIONALE
One of the more enduring questions in critical care medicine is which fluid-management strategy is best for patients with ALI/ARDS.
The conservative strategy results in a lower vascular filling pressure, which in turn reduces pulmonary edema and improves gas exchange. The drawback to this strategy is that it may have a negative effect on cardiac output and nonpulmonary organ function.
The liberal strategy results in a higher vascular filling pressure, which may be beneficial in terms of cardiac output and nonpulmonary organ perfusion. However, this strategy does not reduce lung edema.
The evidence accumulated before FACTT did not favor one strategy over the other. However, most deaths among patients with ALI/ARDS are attributable to the failure of organs other than the lungs.4,5 As a result, aggressive fluid restriction has not been a common approach in hospitals throughout the United States.1,2
In an effort to resolve the controversy surrounding the management of ALI/ARDS and to broaden the scope of what we know about fluid balance, we undertook this multicenter, randomized, prospective clinical comparison of the two strategies. This study was conducted under the auspices of the National Heart, Lung, and Blood Institute’s Acute Respiratory Distress Syndrome Clinical Trials Network (ARDSnet).
STUDY DESIGN
Between June 8, 2000, and October 3, 2005, we screened more than 11,000 patients with ALI/ARDS at 20 centers in North America.
Eligibility
Eligible patients had experienced ALI/ARDS within the previous 48 hours, had been intubated for positive-pressure ventilation, had a ratio of partial pressure of arterial oxygen (PaO2) to the fraction of inspired oxygen (FIO2) of less than 300, and exhibited bilateral infiltrates on chest radiography that were consistent with the presence of pulmonary edema without evidence of left atrial hypertension.6
Major exclusion criteria included the placement of a pulmonary artery catheter prior to randomization and the presence of certain illnesses that might have compromised the study results.
Patient population
The target enrollment of 1,000 patients was reached. These patients were randomized into one of four roughly equal groups based on the type of fluid-management strategy—conservative or liberal—and the type of catheter that was placed—pulmonary artery or central venous. (The ARDSnet researchers published the results of the catheter comparison in a separate article.7 Those results are not discussed here except to note that there were no statistically significant differences in outcomes between the two catheter groups.)
There were no statistically significant differences between the two groups with respect to baseline demographic characteristics. The conservative-strategy group consisted of 503 patients, of whom 52% were male and 65% were white; the mean age was 50.1 years. The liberal-strategy group consisted of 497 patients, of whom 55% were male and 63% were white; mean age was 49.5 years.
Management
Ventilation according to a low tidal volume strategy (6 mg/kg) was initiated within 1 hour after randomization. The pulmonary artery catheter or central venous catheter was inserted within 4 hours of randomization, and fluid management was started within 2 hours after catheter insertion. Fluid management was continued for 7 days or until 12 hours after extubation in patients who became able to breathe without assistance, whichever occurred first.
Target filling pressures. In the conservative-strategy group, the target filling pressures were low—a pulmonary artery occlusion pressure less than 8 mm Hg for those randomized to receive a pulmonary artery catheter, and a central venous pressure less than 4 mm Hg for those randomized to receive a central venous catheter. Barring adverse effects, patients were to undergo diuresis with furosemide (Lasix) until their goal was achieved, and then they would be maintained on that dosage through day 7. If we experienced difficulty in safely reaching these goals—say, if a patient developed hypoxemia, oliguria, or hypotension—we backed off the diuresis until the patient stabilized, and then we tried again. An inability to reach these filling pressure targets was not considered to be a treatment failure; our actual aim was to get as close to the target as possible as long as the patient tolerated the treatment.
In the liberal-strategy group, the target pressures were in the high-to-normal range—14 to 18 mm Hg for those with a pulmonary artery catheter and 10 to 14 mm Hg for those with a central venous catheter.
Patients with a pulmonary artery catheter who were hemodynamically stable after 3 days could be switched to a central venous catheter at the discretion of the clinician.
Monitoring. Patients were monitored once every 4 hours—more often if the clinician felt it necessary—for four variables:
- Pulmonary artery occlusion pressure or central venous pressure, depending on the type of catheter
- Shock, indicated by a mean arterial pressure of less than 60 mm Hg or the need for a vasopressor
- Oliguria, indicated by a urine output of less than 0.5 mL/kg/hour
- Ineffective circulation, represented by a cardiac index of less than 2.5 L/minute/cm2 in the pulmonary artery catheter group and by the presence of cold, mottled skin and a capillary-refilling time of more than 2 seconds in the central venous catheter group.
Depending on what the clinician found during monitoring, patients could receive a fluid bolus (if the filling pressure was too low), furosemide (if the filling pressure was too high), dobutamine (in certain rare circumstances), or nothing.
We monitored compliance with the protocol instructions twice each day—at a set time each morning and later in the day at a randomly selected time. An important aspect of this study is that we had no protocol instructions for managing shock. Individual clinicians were free to treat shock however they deemed best. In essence, then, our study was a comparison of liberal and conservative strategies during the nonshock phase of ALI/ARDS.
End points
The primary end point was the mortality rate at 60 days. Patients who were discharged earlier were assumed to be alive at 60 days.
The secondary end points were the number of ICU-free and ventilator-free days and the number of organ-failure-free days at day 28. Other end points included various indicators of lung physiology.
Statistical analysis
This intention-to-treat analysis was powered so that we had a 90% chance of detecting a 10% difference in mortality rate at day 60 (statistical significance: P < .05).
Protocol safeguards
Prior to treatment, we knew that some patients in the liberal-strategy group would not reach their filling-pressure targets despite the infusion of large amounts of fluid. To avoid “overdosing” these patients, we limited all patients to a maximum of three fluid boluses per 24 hours. Also, we withheld fluid boluses if a patient’s FIO2 level reached or exceeded 0.7 or if the cardiac index rose to 4.5 L/minute/cm2 or higher.
Diuretics were withheld when a patient had received a vasopressor or had emerged from shock within the preceding 12 hours. Also, diuretics were not given to any patient who had received a fluid bolus within the preceding 12 hours or when renal failure was present (these patients were given renal support therapy).
Finally, physicians and coordinators were instructed to assess each protocol instruction for safety and clinical validity before implementing the particular instruction. If, in their medical judgment, a particular protocol instruction should not be implemented, they were authorized to override the instruction and record the reason for doing so in the case report form.
RESULTS
Protocol compliance
Clinicians adhered to the protocol instructions during approximately 90% of the time.
Diuretic administration. In response to high filling pressures, patients in the conservative-strategy and liberal-strategy groups received furosemide during 41% and 10% of assessment periods, respectively (P < .0001). By day 7, the average patient in the conservative-strategy group had received a cumulative dose of approximately 1,000 mg of furosemide, while the average patient in the liberal-strategy group had received 500 mg.
Fluid administration. Low filling pressure prompted the administration of a fluid bolus to the liberal-strategy group during 15% of the assessment periods, compared with 6% in the conservative-strategy group (P < .0001).
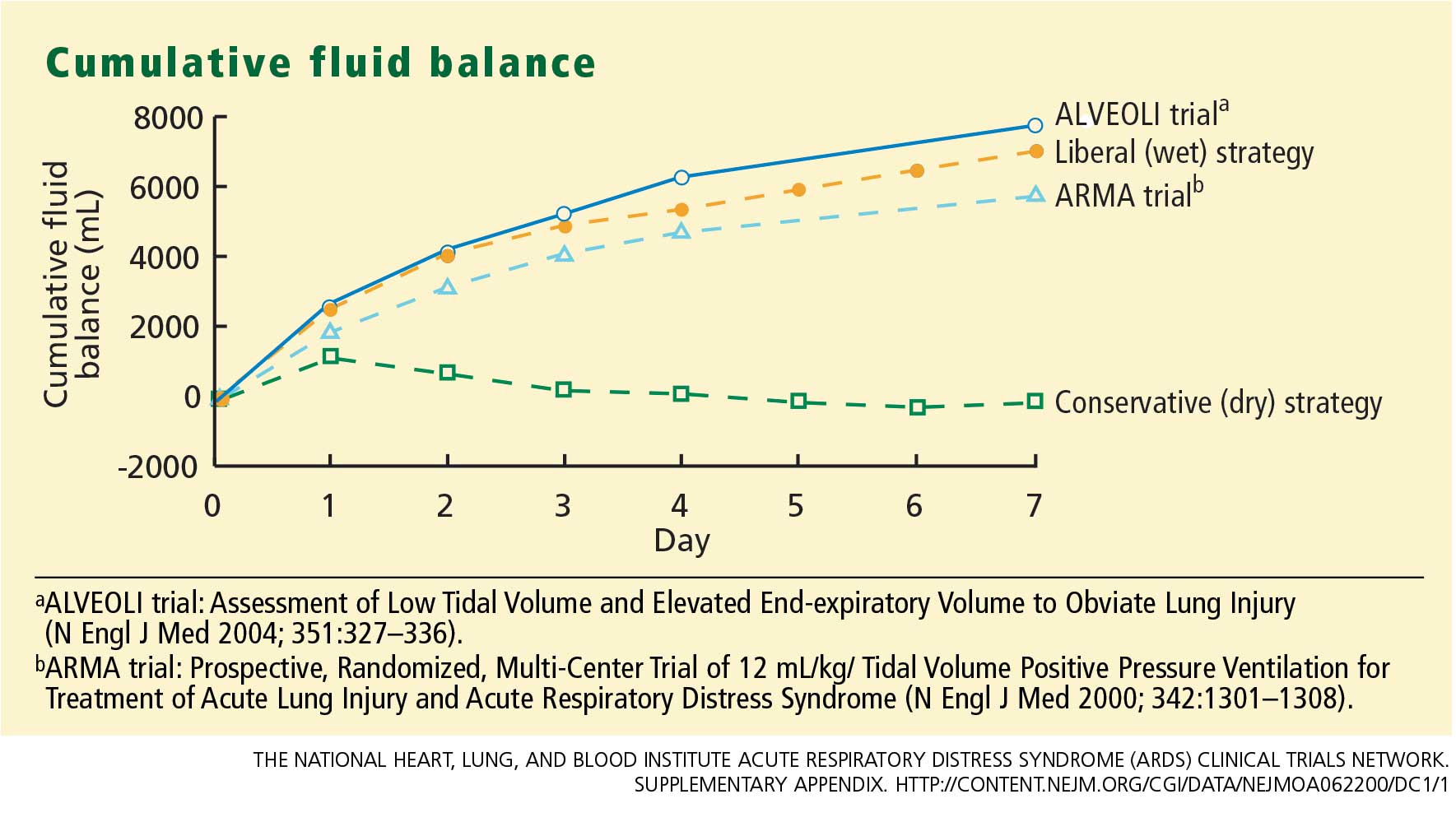
The conservative-strategy patients who were in shock at study entry had a net gain of approximately 3 L of fluid by day 7, while the liberal-strategy group had a gain of approximately 10 L. Among the patients who were shock-free at baseline, the conservative-strategy group had a net loss of almost 2 L at day 7 while the liberal-strategy group had a net gain of about 5 L.
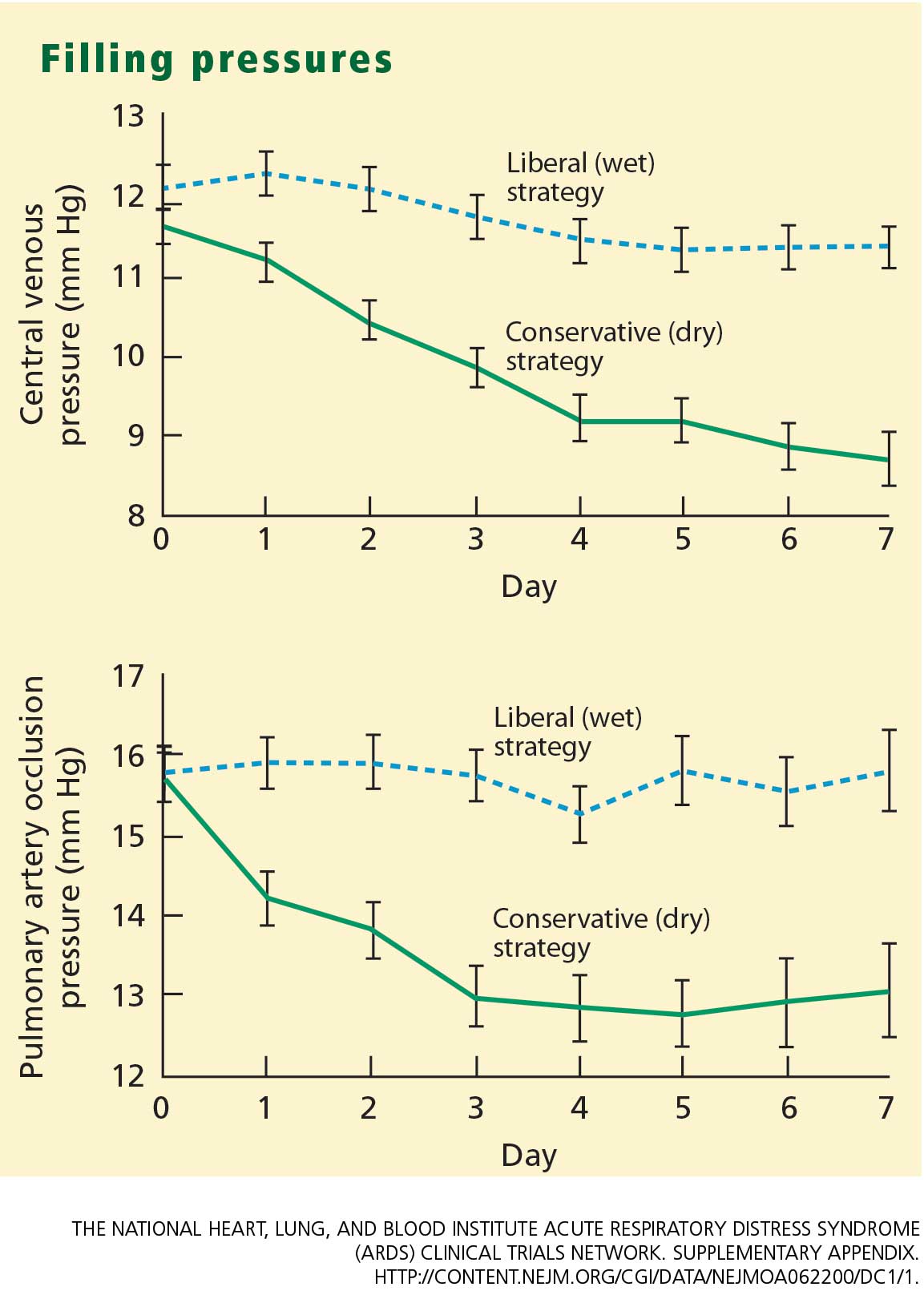
The pulmonary artery occlusion pressure fell from 15.6 mm Hg to just below 13 mm Hg in the conservative-strategy group by day 7, although there was a wide variation among individual patients. The pressure in the liberal-strategy group (15.7 mm Hg at baseline) was unchanged at day 7 (Figure 2).
Primary end point
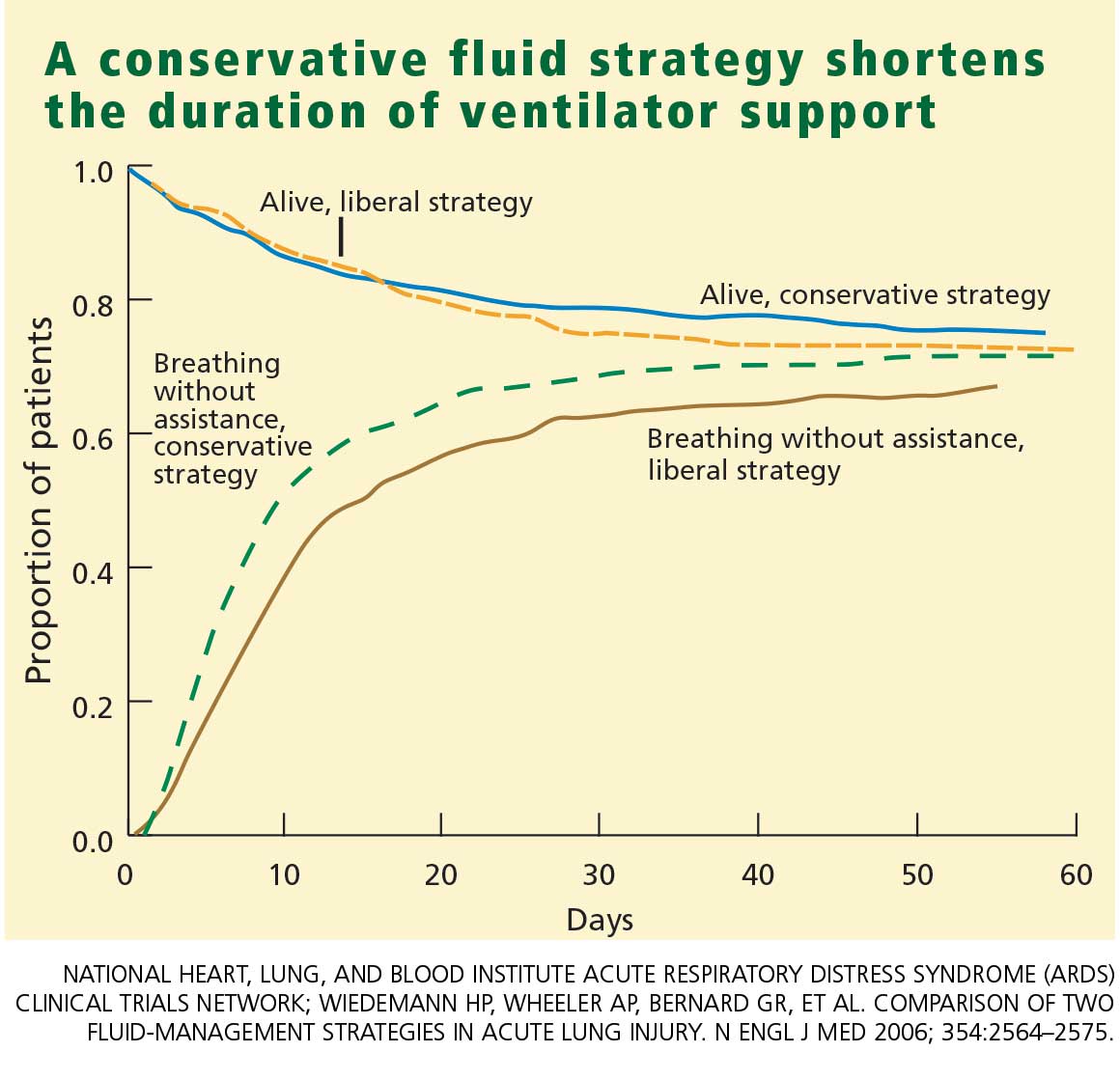
Secondary end points
Through day 7, the average patient in the conservative-strategy group experienced significantly more ICU-free days (0.9 vs 0.6; P <.001) and more days free of central nervous system (CNS) failure (3.4 vs 2.9; P = .02). No significant differences were observed in the number of days free from coagulation abnormalities and renal or hepatic failure at day 28.
Through day 28, the average patient in the conservative-strategy group experienced significantly more ventilator-free days (14.6 vs 12.1; P < .001). The other 7-day results held up after 28 days, as the average conservative-strategy patient continued to experience more ICU-free days (13.4 vs 11.2; P < .001) and more days free of CNS failure (18.8 vs 17.2; P = .03). Again, no significant differences were observed in the number of days free of coagulation abnormalities and cardiovascular, renal, or hepatic failure.
It is not clear if the conservative strategy’s advantage in terms of more CNS-failure-free days was actually the result of the strategy itself or due to the fact that these patients were weaned off ventilation earlier and therefore received less sedation.
Other outcomes
Shock. One concern we had with the conservative strategy was that it might induce shock more frequently, but this did not occur. The percentage of patients who developed shock at least once during the 7-day treatment protocol was quite similar in the two groups. Also, it is interesting that patients who presented with no baseline shock had only about a 30% chance of developing shock during therapy. There was no significant difference in vasopressor use between the two groups.
Lung function. The conservative-strategy group had a significantly better Murray lung injury score at day 7: 2.03 vs 2.27 (P < .001).
Tidal-volume scores (7.4 mL/kg in both groups at baseline) dropped at an equal rate and were virtually identical at day 7 (6.36 mL/kg in the conservative-strategy group and 6.34 in the liberal-strategy group), as expected.The plateau pressure, positive end-expiraory pressure, PaO2–FIO2 ratio, and oxygenation index were slightly but not significantly better in the conservative-strategy group at day 7.
Overall, lung function was considerably better in the conservative-strategy group.
Cardiovascular function. The mean arterial pressure was significantly lower in the conservative-strategy group at day 7 (81.00 vs 84.36 mm Hg; P = .03). It is interesting that both levels were higher than the baseline levels (77.1 and 77.2, respectively; not significant).
The stroke volume index and the cardiac index were slightly lower in the conservative-strategy group at day 7, but not significantly so. No differences were seen in heart rate and venous oxygen saturation levels.
Renal and metabolic function. At day 7, the conservative-strategy group had a significantly higher blood urea nitrogen level (33.62 vs 28.44 mg/dL; P = .009). No significant differences were seen between the groups in creatinine levels at day 7 and day 28.
At day 60, dialysis was needed by 10% of the conservative-strategy group and 14% of the liberal-strategy group (P = .06). The important finding here is that there was no trend toward a more frequent need for dialysis in the conservative-strategy group. Also, the average number of days on dialysis in the two groups was essentially the same (11.0 and 10.9, respectively).
Again, there was no difference in the number of renal-failure-free days at either day 7 or day 28.
Hematologic factors. At day 7, the conservative-strategy group had significantly higher hemoglobin (10.22 vs 9.65 g/dL) and albumin (2.30 vs 2.11 g/dL) levels and capillary osmotic pressure (19.18 vs 17.39 mm Hg), even though significantly more patients in the liberal-strategy group received transfusions through day 7 (39% vs 29%; P = .0007).
Safety. Although the number of adverse events—particularly, metabolic alkalosis and electrolyte imbalance—was significantly higher in the conservative-strategy group (42 vs 19; P = .001), the overall incidence was low. No adverse event was associated with arrhythmia.
CONCLUSION
The two fluid-management protocols used in this study were designed to be prudent yet distinctly different. While designing our protocol, we were concerned on the one hand that despite our best efforts fluid balance would turn out to be very similar in the two groups; this did not happen. On the other hand, we were also worried that the fluid level in one of the two groups might turn out to be so bizarre that it would invalidate our study; this too did not occur. Therefore, we are pleased with the way the study was designed and conducted, and we are satisfied that the two protocols were legitimate.
As we went into our study, the literature contained only one other prospective trial that was in some way similar to ours. Mitchell et al9 conducted a randomized, prospective study of 101 critically ill patients, including 89 with pulmonary edema. A group of 52 patients were managed with a conservative strategy intended to reduce the amount of extravascular lung water; the other 49 patients were managed with a strategy similar to the liberal strategy used in our study. At the study’s end, the patients in the conservative-strategy group had a significantly lower amount of extravascular lung water and spent significantly fewer days on ventilation and in the ICU. No clinically significant adverse effects were associated with the conservative strategy. This small study was not highly powered, but it did show that aggressive fluid restriction conferred some benefit.
In our study, the conservative strategy improved lung function and shortened the duration of mechanical ventilation and ICU stay without increasing nonpulmonary organ failures or increasing the risk of death within 60 days. Therefore, we recommend the conservative strategy for patients with ALI/ARDS.
- The Acute Respiratory Distress Syndrome Network.Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 2000; 342:1301–1308.
- Brower RG, Lanken PN, MacIntyre N, et al; National Heart, Lung, and Blood Institute ARDS Clinical Trials Network. Higher versus lower positive end-expiratory pressures in patients with the acute respiratory distress syndrome. N Engl J Med 2004; 351:327–336.
- National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network; Wiedemann HP, Wheeler AP, Bernard GR, et al. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med 2006; 354:2564–2575.
- Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med 2000; 342:1334–1349.
- Montgomery AB, Stager MA, Carrico CJ, Hudson LD. Causes of mortality in patients with the adult respiratory distress syndrome. Am Rev Respir Dis 1985; 132:485–489.
- Bernard GR, Artigas A, Brigham KL, et al. The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med 1994; 149:818–824.
- National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network; Wheeler AP, Bernard GR, Thompson BT, et al. Pulmonary-artery versus central venous catheter to guide treatment of acute lung injury. N Engl J Med 2006; 354:2213–2224.
- The National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical TrialsNetwork. Supplementary appendix.http://content.nejm.org/cgi/data/NEJMoa062200/DC1/1.Accessed August 3, 2007.
- Mitchell JP, Schuller D, Calandrino FS, Schuster DP.Improved outcome based on fluid management in criticallyill patients requiring pulmonary artery catheterization.Am Rev Respir Dis 1992; 145:990–998.
Although most clinicians tend to manage acute lung injury (ALI) and acute respiratory distress syndrome (ARDS) by giving more rather than less fluid,1,2 patients may actually fare better under a strategy of limited fluid intake and increased fluid excretion.
According to the results of the Fluids and Catheters Treatment Trial (FACTT),3 patients managed with fluid restriction (the “dry” or conservative strategy) spent significantly less time in the intensive care unit (ICU) and on mechanical ventilation than did patients who received a high fluid intake (the “wet” or liberal strategy). These benefits of the conservative strategy were attained without any increase in the mortality rate at 60 days or in nonpulmonary organ failure at 28 days.
In this article, I discuss the basis for the FACTT researchers’ conclusion that a conservative fluid strategy is preferable to a liberal fluid strategy in ALI/ARDS.
STUDY RATIONALE
One of the more enduring questions in critical care medicine is which fluid-management strategy is best for patients with ALI/ARDS.
The conservative strategy results in a lower vascular filling pressure, which in turn reduces pulmonary edema and improves gas exchange. The drawback to this strategy is that it may have a negative effect on cardiac output and nonpulmonary organ function.
The liberal strategy results in a higher vascular filling pressure, which may be beneficial in terms of cardiac output and nonpulmonary organ perfusion. However, this strategy does not reduce lung edema.
The evidence accumulated before FACTT did not favor one strategy over the other. However, most deaths among patients with ALI/ARDS are attributable to the failure of organs other than the lungs.4,5 As a result, aggressive fluid restriction has not been a common approach in hospitals throughout the United States.1,2
In an effort to resolve the controversy surrounding the management of ALI/ARDS and to broaden the scope of what we know about fluid balance, we undertook this multicenter, randomized, prospective clinical comparison of the two strategies. This study was conducted under the auspices of the National Heart, Lung, and Blood Institute’s Acute Respiratory Distress Syndrome Clinical Trials Network (ARDSnet).
STUDY DESIGN
Between June 8, 2000, and October 3, 2005, we screened more than 11,000 patients with ALI/ARDS at 20 centers in North America.
Eligibility
Eligible patients had experienced ALI/ARDS within the previous 48 hours, had been intubated for positive-pressure ventilation, had a ratio of partial pressure of arterial oxygen (PaO2) to the fraction of inspired oxygen (FIO2) of less than 300, and exhibited bilateral infiltrates on chest radiography that were consistent with the presence of pulmonary edema without evidence of left atrial hypertension.6
Major exclusion criteria included the placement of a pulmonary artery catheter prior to randomization and the presence of certain illnesses that might have compromised the study results.
Patient population
The target enrollment of 1,000 patients was reached. These patients were randomized into one of four roughly equal groups based on the type of fluid-management strategy—conservative or liberal—and the type of catheter that was placed—pulmonary artery or central venous. (The ARDSnet researchers published the results of the catheter comparison in a separate article.7 Those results are not discussed here except to note that there were no statistically significant differences in outcomes between the two catheter groups.)
There were no statistically significant differences between the two groups with respect to baseline demographic characteristics. The conservative-strategy group consisted of 503 patients, of whom 52% were male and 65% were white; the mean age was 50.1 years. The liberal-strategy group consisted of 497 patients, of whom 55% were male and 63% were white; mean age was 49.5 years.
Management
Ventilation according to a low tidal volume strategy (6 mg/kg) was initiated within 1 hour after randomization. The pulmonary artery catheter or central venous catheter was inserted within 4 hours of randomization, and fluid management was started within 2 hours after catheter insertion. Fluid management was continued for 7 days or until 12 hours after extubation in patients who became able to breathe without assistance, whichever occurred first.
Target filling pressures. In the conservative-strategy group, the target filling pressures were low—a pulmonary artery occlusion pressure less than 8 mm Hg for those randomized to receive a pulmonary artery catheter, and a central venous pressure less than 4 mm Hg for those randomized to receive a central venous catheter. Barring adverse effects, patients were to undergo diuresis with furosemide (Lasix) until their goal was achieved, and then they would be maintained on that dosage through day 7. If we experienced difficulty in safely reaching these goals—say, if a patient developed hypoxemia, oliguria, or hypotension—we backed off the diuresis until the patient stabilized, and then we tried again. An inability to reach these filling pressure targets was not considered to be a treatment failure; our actual aim was to get as close to the target as possible as long as the patient tolerated the treatment.
In the liberal-strategy group, the target pressures were in the high-to-normal range—14 to 18 mm Hg for those with a pulmonary artery catheter and 10 to 14 mm Hg for those with a central venous catheter.
Patients with a pulmonary artery catheter who were hemodynamically stable after 3 days could be switched to a central venous catheter at the discretion of the clinician.
Monitoring. Patients were monitored once every 4 hours—more often if the clinician felt it necessary—for four variables:
- Pulmonary artery occlusion pressure or central venous pressure, depending on the type of catheter
- Shock, indicated by a mean arterial pressure of less than 60 mm Hg or the need for a vasopressor
- Oliguria, indicated by a urine output of less than 0.5 mL/kg/hour
- Ineffective circulation, represented by a cardiac index of less than 2.5 L/minute/cm2 in the pulmonary artery catheter group and by the presence of cold, mottled skin and a capillary-refilling time of more than 2 seconds in the central venous catheter group.
Depending on what the clinician found during monitoring, patients could receive a fluid bolus (if the filling pressure was too low), furosemide (if the filling pressure was too high), dobutamine (in certain rare circumstances), or nothing.
We monitored compliance with the protocol instructions twice each day—at a set time each morning and later in the day at a randomly selected time. An important aspect of this study is that we had no protocol instructions for managing shock. Individual clinicians were free to treat shock however they deemed best. In essence, then, our study was a comparison of liberal and conservative strategies during the nonshock phase of ALI/ARDS.
End points
The primary end point was the mortality rate at 60 days. Patients who were discharged earlier were assumed to be alive at 60 days.
The secondary end points were the number of ICU-free and ventilator-free days and the number of organ-failure-free days at day 28. Other end points included various indicators of lung physiology.
Statistical analysis
This intention-to-treat analysis was powered so that we had a 90% chance of detecting a 10% difference in mortality rate at day 60 (statistical significance: P < .05).
Protocol safeguards
Prior to treatment, we knew that some patients in the liberal-strategy group would not reach their filling-pressure targets despite the infusion of large amounts of fluid. To avoid “overdosing” these patients, we limited all patients to a maximum of three fluid boluses per 24 hours. Also, we withheld fluid boluses if a patient’s FIO2 level reached or exceeded 0.7 or if the cardiac index rose to 4.5 L/minute/cm2 or higher.
Diuretics were withheld when a patient had received a vasopressor or had emerged from shock within the preceding 12 hours. Also, diuretics were not given to any patient who had received a fluid bolus within the preceding 12 hours or when renal failure was present (these patients were given renal support therapy).
Finally, physicians and coordinators were instructed to assess each protocol instruction for safety and clinical validity before implementing the particular instruction. If, in their medical judgment, a particular protocol instruction should not be implemented, they were authorized to override the instruction and record the reason for doing so in the case report form.
RESULTS
Protocol compliance
Clinicians adhered to the protocol instructions during approximately 90% of the time.
Diuretic administration. In response to high filling pressures, patients in the conservative-strategy and liberal-strategy groups received furosemide during 41% and 10% of assessment periods, respectively (P < .0001). By day 7, the average patient in the conservative-strategy group had received a cumulative dose of approximately 1,000 mg of furosemide, while the average patient in the liberal-strategy group had received 500 mg.
Fluid administration. Low filling pressure prompted the administration of a fluid bolus to the liberal-strategy group during 15% of the assessment periods, compared with 6% in the conservative-strategy group (P < .0001).
The conservative-strategy patients who were in shock at study entry had a net gain of approximately 3 L of fluid by day 7, while the liberal-strategy group had a gain of approximately 10 L. Among the patients who were shock-free at baseline, the conservative-strategy group had a net loss of almost 2 L at day 7 while the liberal-strategy group had a net gain of about 5 L.
The pulmonary artery occlusion pressure fell from 15.6 mm Hg to just below 13 mm Hg in the conservative-strategy group by day 7, although there was a wide variation among individual patients. The pressure in the liberal-strategy group (15.7 mm Hg at baseline) was unchanged at day 7 (Figure 2).
Primary end point
Secondary end points
Through day 7, the average patient in the conservative-strategy group experienced significantly more ICU-free days (0.9 vs 0.6; P <.001) and more days free of central nervous system (CNS) failure (3.4 vs 2.9; P = .02). No significant differences were observed in the number of days free from coagulation abnormalities and renal or hepatic failure at day 28.
Through day 28, the average patient in the conservative-strategy group experienced significantly more ventilator-free days (14.6 vs 12.1; P < .001). The other 7-day results held up after 28 days, as the average conservative-strategy patient continued to experience more ICU-free days (13.4 vs 11.2; P < .001) and more days free of CNS failure (18.8 vs 17.2; P = .03). Again, no significant differences were observed in the number of days free of coagulation abnormalities and cardiovascular, renal, or hepatic failure.
It is not clear if the conservative strategy’s advantage in terms of more CNS-failure-free days was actually the result of the strategy itself or due to the fact that these patients were weaned off ventilation earlier and therefore received less sedation.
Other outcomes
Shock. One concern we had with the conservative strategy was that it might induce shock more frequently, but this did not occur. The percentage of patients who developed shock at least once during the 7-day treatment protocol was quite similar in the two groups. Also, it is interesting that patients who presented with no baseline shock had only about a 30% chance of developing shock during therapy. There was no significant difference in vasopressor use between the two groups.
Lung function. The conservative-strategy group had a significantly better Murray lung injury score at day 7: 2.03 vs 2.27 (P < .001).
Tidal-volume scores (7.4 mL/kg in both groups at baseline) dropped at an equal rate and were virtually identical at day 7 (6.36 mL/kg in the conservative-strategy group and 6.34 in the liberal-strategy group), as expected.The plateau pressure, positive end-expiraory pressure, PaO2–FIO2 ratio, and oxygenation index were slightly but not significantly better in the conservative-strategy group at day 7.
Overall, lung function was considerably better in the conservative-strategy group.
Cardiovascular function. The mean arterial pressure was significantly lower in the conservative-strategy group at day 7 (81.00 vs 84.36 mm Hg; P = .03). It is interesting that both levels were higher than the baseline levels (77.1 and 77.2, respectively; not significant).
The stroke volume index and the cardiac index were slightly lower in the conservative-strategy group at day 7, but not significantly so. No differences were seen in heart rate and venous oxygen saturation levels.
Renal and metabolic function. At day 7, the conservative-strategy group had a significantly higher blood urea nitrogen level (33.62 vs 28.44 mg/dL; P = .009). No significant differences were seen between the groups in creatinine levels at day 7 and day 28.
At day 60, dialysis was needed by 10% of the conservative-strategy group and 14% of the liberal-strategy group (P = .06). The important finding here is that there was no trend toward a more frequent need for dialysis in the conservative-strategy group. Also, the average number of days on dialysis in the two groups was essentially the same (11.0 and 10.9, respectively).
Again, there was no difference in the number of renal-failure-free days at either day 7 or day 28.
Hematologic factors. At day 7, the conservative-strategy group had significantly higher hemoglobin (10.22 vs 9.65 g/dL) and albumin (2.30 vs 2.11 g/dL) levels and capillary osmotic pressure (19.18 vs 17.39 mm Hg), even though significantly more patients in the liberal-strategy group received transfusions through day 7 (39% vs 29%; P = .0007).
Safety. Although the number of adverse events—particularly, metabolic alkalosis and electrolyte imbalance—was significantly higher in the conservative-strategy group (42 vs 19; P = .001), the overall incidence was low. No adverse event was associated with arrhythmia.
CONCLUSION
The two fluid-management protocols used in this study were designed to be prudent yet distinctly different. While designing our protocol, we were concerned on the one hand that despite our best efforts fluid balance would turn out to be very similar in the two groups; this did not happen. On the other hand, we were also worried that the fluid level in one of the two groups might turn out to be so bizarre that it would invalidate our study; this too did not occur. Therefore, we are pleased with the way the study was designed and conducted, and we are satisfied that the two protocols were legitimate.
As we went into our study, the literature contained only one other prospective trial that was in some way similar to ours. Mitchell et al9 conducted a randomized, prospective study of 101 critically ill patients, including 89 with pulmonary edema. A group of 52 patients were managed with a conservative strategy intended to reduce the amount of extravascular lung water; the other 49 patients were managed with a strategy similar to the liberal strategy used in our study. At the study’s end, the patients in the conservative-strategy group had a significantly lower amount of extravascular lung water and spent significantly fewer days on ventilation and in the ICU. No clinically significant adverse effects were associated with the conservative strategy. This small study was not highly powered, but it did show that aggressive fluid restriction conferred some benefit.
In our study, the conservative strategy improved lung function and shortened the duration of mechanical ventilation and ICU stay without increasing nonpulmonary organ failures or increasing the risk of death within 60 days. Therefore, we recommend the conservative strategy for patients with ALI/ARDS.
Although most clinicians tend to manage acute lung injury (ALI) and acute respiratory distress syndrome (ARDS) by giving more rather than less fluid,1,2 patients may actually fare better under a strategy of limited fluid intake and increased fluid excretion.
According to the results of the Fluids and Catheters Treatment Trial (FACTT),3 patients managed with fluid restriction (the “dry” or conservative strategy) spent significantly less time in the intensive care unit (ICU) and on mechanical ventilation than did patients who received a high fluid intake (the “wet” or liberal strategy). These benefits of the conservative strategy were attained without any increase in the mortality rate at 60 days or in nonpulmonary organ failure at 28 days.
In this article, I discuss the basis for the FACTT researchers’ conclusion that a conservative fluid strategy is preferable to a liberal fluid strategy in ALI/ARDS.
STUDY RATIONALE
One of the more enduring questions in critical care medicine is which fluid-management strategy is best for patients with ALI/ARDS.
The conservative strategy results in a lower vascular filling pressure, which in turn reduces pulmonary edema and improves gas exchange. The drawback to this strategy is that it may have a negative effect on cardiac output and nonpulmonary organ function.
The liberal strategy results in a higher vascular filling pressure, which may be beneficial in terms of cardiac output and nonpulmonary organ perfusion. However, this strategy does not reduce lung edema.
The evidence accumulated before FACTT did not favor one strategy over the other. However, most deaths among patients with ALI/ARDS are attributable to the failure of organs other than the lungs.4,5 As a result, aggressive fluid restriction has not been a common approach in hospitals throughout the United States.1,2
In an effort to resolve the controversy surrounding the management of ALI/ARDS and to broaden the scope of what we know about fluid balance, we undertook this multicenter, randomized, prospective clinical comparison of the two strategies. This study was conducted under the auspices of the National Heart, Lung, and Blood Institute’s Acute Respiratory Distress Syndrome Clinical Trials Network (ARDSnet).
STUDY DESIGN
Between June 8, 2000, and October 3, 2005, we screened more than 11,000 patients with ALI/ARDS at 20 centers in North America.
Eligibility
Eligible patients had experienced ALI/ARDS within the previous 48 hours, had been intubated for positive-pressure ventilation, had a ratio of partial pressure of arterial oxygen (PaO2) to the fraction of inspired oxygen (FIO2) of less than 300, and exhibited bilateral infiltrates on chest radiography that were consistent with the presence of pulmonary edema without evidence of left atrial hypertension.6
Major exclusion criteria included the placement of a pulmonary artery catheter prior to randomization and the presence of certain illnesses that might have compromised the study results.
Patient population
The target enrollment of 1,000 patients was reached. These patients were randomized into one of four roughly equal groups based on the type of fluid-management strategy—conservative or liberal—and the type of catheter that was placed—pulmonary artery or central venous. (The ARDSnet researchers published the results of the catheter comparison in a separate article.7 Those results are not discussed here except to note that there were no statistically significant differences in outcomes between the two catheter groups.)
There were no statistically significant differences between the two groups with respect to baseline demographic characteristics. The conservative-strategy group consisted of 503 patients, of whom 52% were male and 65% were white; the mean age was 50.1 years. The liberal-strategy group consisted of 497 patients, of whom 55% were male and 63% were white; mean age was 49.5 years.
Management
Ventilation according to a low tidal volume strategy (6 mg/kg) was initiated within 1 hour after randomization. The pulmonary artery catheter or central venous catheter was inserted within 4 hours of randomization, and fluid management was started within 2 hours after catheter insertion. Fluid management was continued for 7 days or until 12 hours after extubation in patients who became able to breathe without assistance, whichever occurred first.
Target filling pressures. In the conservative-strategy group, the target filling pressures were low—a pulmonary artery occlusion pressure less than 8 mm Hg for those randomized to receive a pulmonary artery catheter, and a central venous pressure less than 4 mm Hg for those randomized to receive a central venous catheter. Barring adverse effects, patients were to undergo diuresis with furosemide (Lasix) until their goal was achieved, and then they would be maintained on that dosage through day 7. If we experienced difficulty in safely reaching these goals—say, if a patient developed hypoxemia, oliguria, or hypotension—we backed off the diuresis until the patient stabilized, and then we tried again. An inability to reach these filling pressure targets was not considered to be a treatment failure; our actual aim was to get as close to the target as possible as long as the patient tolerated the treatment.
In the liberal-strategy group, the target pressures were in the high-to-normal range—14 to 18 mm Hg for those with a pulmonary artery catheter and 10 to 14 mm Hg for those with a central venous catheter.
Patients with a pulmonary artery catheter who were hemodynamically stable after 3 days could be switched to a central venous catheter at the discretion of the clinician.
Monitoring. Patients were monitored once every 4 hours—more often if the clinician felt it necessary—for four variables:
- Pulmonary artery occlusion pressure or central venous pressure, depending on the type of catheter
- Shock, indicated by a mean arterial pressure of less than 60 mm Hg or the need for a vasopressor
- Oliguria, indicated by a urine output of less than 0.5 mL/kg/hour
- Ineffective circulation, represented by a cardiac index of less than 2.5 L/minute/cm2 in the pulmonary artery catheter group and by the presence of cold, mottled skin and a capillary-refilling time of more than 2 seconds in the central venous catheter group.
Depending on what the clinician found during monitoring, patients could receive a fluid bolus (if the filling pressure was too low), furosemide (if the filling pressure was too high), dobutamine (in certain rare circumstances), or nothing.
We monitored compliance with the protocol instructions twice each day—at a set time each morning and later in the day at a randomly selected time. An important aspect of this study is that we had no protocol instructions for managing shock. Individual clinicians were free to treat shock however they deemed best. In essence, then, our study was a comparison of liberal and conservative strategies during the nonshock phase of ALI/ARDS.
End points
The primary end point was the mortality rate at 60 days. Patients who were discharged earlier were assumed to be alive at 60 days.
The secondary end points were the number of ICU-free and ventilator-free days and the number of organ-failure-free days at day 28. Other end points included various indicators of lung physiology.
Statistical analysis
This intention-to-treat analysis was powered so that we had a 90% chance of detecting a 10% difference in mortality rate at day 60 (statistical significance: P < .05).
Protocol safeguards
Prior to treatment, we knew that some patients in the liberal-strategy group would not reach their filling-pressure targets despite the infusion of large amounts of fluid. To avoid “overdosing” these patients, we limited all patients to a maximum of three fluid boluses per 24 hours. Also, we withheld fluid boluses if a patient’s FIO2 level reached or exceeded 0.7 or if the cardiac index rose to 4.5 L/minute/cm2 or higher.
Diuretics were withheld when a patient had received a vasopressor or had emerged from shock within the preceding 12 hours. Also, diuretics were not given to any patient who had received a fluid bolus within the preceding 12 hours or when renal failure was present (these patients were given renal support therapy).
Finally, physicians and coordinators were instructed to assess each protocol instruction for safety and clinical validity before implementing the particular instruction. If, in their medical judgment, a particular protocol instruction should not be implemented, they were authorized to override the instruction and record the reason for doing so in the case report form.
RESULTS
Protocol compliance
Clinicians adhered to the protocol instructions during approximately 90% of the time.
Diuretic administration. In response to high filling pressures, patients in the conservative-strategy and liberal-strategy groups received furosemide during 41% and 10% of assessment periods, respectively (P < .0001). By day 7, the average patient in the conservative-strategy group had received a cumulative dose of approximately 1,000 mg of furosemide, while the average patient in the liberal-strategy group had received 500 mg.
Fluid administration. Low filling pressure prompted the administration of a fluid bolus to the liberal-strategy group during 15% of the assessment periods, compared with 6% in the conservative-strategy group (P < .0001).
The conservative-strategy patients who were in shock at study entry had a net gain of approximately 3 L of fluid by day 7, while the liberal-strategy group had a gain of approximately 10 L. Among the patients who were shock-free at baseline, the conservative-strategy group had a net loss of almost 2 L at day 7 while the liberal-strategy group had a net gain of about 5 L.
The pulmonary artery occlusion pressure fell from 15.6 mm Hg to just below 13 mm Hg in the conservative-strategy group by day 7, although there was a wide variation among individual patients. The pressure in the liberal-strategy group (15.7 mm Hg at baseline) was unchanged at day 7 (Figure 2).
Primary end point
Secondary end points
Through day 7, the average patient in the conservative-strategy group experienced significantly more ICU-free days (0.9 vs 0.6; P <.001) and more days free of central nervous system (CNS) failure (3.4 vs 2.9; P = .02). No significant differences were observed in the number of days free from coagulation abnormalities and renal or hepatic failure at day 28.
Through day 28, the average patient in the conservative-strategy group experienced significantly more ventilator-free days (14.6 vs 12.1; P < .001). The other 7-day results held up after 28 days, as the average conservative-strategy patient continued to experience more ICU-free days (13.4 vs 11.2; P < .001) and more days free of CNS failure (18.8 vs 17.2; P = .03). Again, no significant differences were observed in the number of days free of coagulation abnormalities and cardiovascular, renal, or hepatic failure.
It is not clear if the conservative strategy’s advantage in terms of more CNS-failure-free days was actually the result of the strategy itself or due to the fact that these patients were weaned off ventilation earlier and therefore received less sedation.
Other outcomes
Shock. One concern we had with the conservative strategy was that it might induce shock more frequently, but this did not occur. The percentage of patients who developed shock at least once during the 7-day treatment protocol was quite similar in the two groups. Also, it is interesting that patients who presented with no baseline shock had only about a 30% chance of developing shock during therapy. There was no significant difference in vasopressor use between the two groups.
Lung function. The conservative-strategy group had a significantly better Murray lung injury score at day 7: 2.03 vs 2.27 (P < .001).
Tidal-volume scores (7.4 mL/kg in both groups at baseline) dropped at an equal rate and were virtually identical at day 7 (6.36 mL/kg in the conservative-strategy group and 6.34 in the liberal-strategy group), as expected.The plateau pressure, positive end-expiraory pressure, PaO2–FIO2 ratio, and oxygenation index were slightly but not significantly better in the conservative-strategy group at day 7.
Overall, lung function was considerably better in the conservative-strategy group.
Cardiovascular function. The mean arterial pressure was significantly lower in the conservative-strategy group at day 7 (81.00 vs 84.36 mm Hg; P = .03). It is interesting that both levels were higher than the baseline levels (77.1 and 77.2, respectively; not significant).
The stroke volume index and the cardiac index were slightly lower in the conservative-strategy group at day 7, but not significantly so. No differences were seen in heart rate and venous oxygen saturation levels.
Renal and metabolic function. At day 7, the conservative-strategy group had a significantly higher blood urea nitrogen level (33.62 vs 28.44 mg/dL; P = .009). No significant differences were seen between the groups in creatinine levels at day 7 and day 28.
At day 60, dialysis was needed by 10% of the conservative-strategy group and 14% of the liberal-strategy group (P = .06). The important finding here is that there was no trend toward a more frequent need for dialysis in the conservative-strategy group. Also, the average number of days on dialysis in the two groups was essentially the same (11.0 and 10.9, respectively).
Again, there was no difference in the number of renal-failure-free days at either day 7 or day 28.
Hematologic factors. At day 7, the conservative-strategy group had significantly higher hemoglobin (10.22 vs 9.65 g/dL) and albumin (2.30 vs 2.11 g/dL) levels and capillary osmotic pressure (19.18 vs 17.39 mm Hg), even though significantly more patients in the liberal-strategy group received transfusions through day 7 (39% vs 29%; P = .0007).
Safety. Although the number of adverse events—particularly, metabolic alkalosis and electrolyte imbalance—was significantly higher in the conservative-strategy group (42 vs 19; P = .001), the overall incidence was low. No adverse event was associated with arrhythmia.
CONCLUSION
The two fluid-management protocols used in this study were designed to be prudent yet distinctly different. While designing our protocol, we were concerned on the one hand that despite our best efforts fluid balance would turn out to be very similar in the two groups; this did not happen. On the other hand, we were also worried that the fluid level in one of the two groups might turn out to be so bizarre that it would invalidate our study; this too did not occur. Therefore, we are pleased with the way the study was designed and conducted, and we are satisfied that the two protocols were legitimate.
As we went into our study, the literature contained only one other prospective trial that was in some way similar to ours. Mitchell et al9 conducted a randomized, prospective study of 101 critically ill patients, including 89 with pulmonary edema. A group of 52 patients were managed with a conservative strategy intended to reduce the amount of extravascular lung water; the other 49 patients were managed with a strategy similar to the liberal strategy used in our study. At the study’s end, the patients in the conservative-strategy group had a significantly lower amount of extravascular lung water and spent significantly fewer days on ventilation and in the ICU. No clinically significant adverse effects were associated with the conservative strategy. This small study was not highly powered, but it did show that aggressive fluid restriction conferred some benefit.
In our study, the conservative strategy improved lung function and shortened the duration of mechanical ventilation and ICU stay without increasing nonpulmonary organ failures or increasing the risk of death within 60 days. Therefore, we recommend the conservative strategy for patients with ALI/ARDS.
- The Acute Respiratory Distress Syndrome Network.Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 2000; 342:1301–1308.
- Brower RG, Lanken PN, MacIntyre N, et al; National Heart, Lung, and Blood Institute ARDS Clinical Trials Network. Higher versus lower positive end-expiratory pressures in patients with the acute respiratory distress syndrome. N Engl J Med 2004; 351:327–336.
- National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network; Wiedemann HP, Wheeler AP, Bernard GR, et al. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med 2006; 354:2564–2575.
- Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med 2000; 342:1334–1349.
- Montgomery AB, Stager MA, Carrico CJ, Hudson LD. Causes of mortality in patients with the adult respiratory distress syndrome. Am Rev Respir Dis 1985; 132:485–489.
- Bernard GR, Artigas A, Brigham KL, et al. The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med 1994; 149:818–824.
- National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network; Wheeler AP, Bernard GR, Thompson BT, et al. Pulmonary-artery versus central venous catheter to guide treatment of acute lung injury. N Engl J Med 2006; 354:2213–2224.
- The National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical TrialsNetwork. Supplementary appendix.http://content.nejm.org/cgi/data/NEJMoa062200/DC1/1.Accessed August 3, 2007.
- Mitchell JP, Schuller D, Calandrino FS, Schuster DP.Improved outcome based on fluid management in criticallyill patients requiring pulmonary artery catheterization.Am Rev Respir Dis 1992; 145:990–998.
- The Acute Respiratory Distress Syndrome Network.Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 2000; 342:1301–1308.
- Brower RG, Lanken PN, MacIntyre N, et al; National Heart, Lung, and Blood Institute ARDS Clinical Trials Network. Higher versus lower positive end-expiratory pressures in patients with the acute respiratory distress syndrome. N Engl J Med 2004; 351:327–336.
- National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network; Wiedemann HP, Wheeler AP, Bernard GR, et al. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med 2006; 354:2564–2575.
- Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med 2000; 342:1334–1349.
- Montgomery AB, Stager MA, Carrico CJ, Hudson LD. Causes of mortality in patients with the adult respiratory distress syndrome. Am Rev Respir Dis 1985; 132:485–489.
- Bernard GR, Artigas A, Brigham KL, et al. The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med 1994; 149:818–824.
- National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network; Wheeler AP, Bernard GR, Thompson BT, et al. Pulmonary-artery versus central venous catheter to guide treatment of acute lung injury. N Engl J Med 2006; 354:2213–2224.
- The National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical TrialsNetwork. Supplementary appendix.http://content.nejm.org/cgi/data/NEJMoa062200/DC1/1.Accessed August 3, 2007.
- Mitchell JP, Schuller D, Calandrino FS, Schuster DP.Improved outcome based on fluid management in criticallyill patients requiring pulmonary artery catheterization.Am Rev Respir Dis 1992; 145:990–998.
KEY POINTS
- In the conservative-strategy group, the target filling pressures were a pulmonary artery occlusion pressure less than 8 mm Hg for those with a pulmonary artery catheter and a central venous pressure less than 4 mm Hg for those with only a central venous catheter. Pressures were brought into these ranges by diuresis.
- The conservative-strategy group did not experience more frequent need for dialysis or more shock.
- Although the number of adverse events—particularly ,metabolic alkalosis and electrolyte imbalance—was significantly higher in the conservative-strategy group, the overall incidence was low.
Acute aortic syndromes: Time to talk of many things
“The time has come,” the Walrus said,
“To talk of many things:
Of shoes—and ships—and sealing-wax—
Of cabbages—and kings—
And why the sea is boiling hot
And whether pigs have wings.”
—Lewis Carroll, The Walrus and the Carpenter (from Through the Looking-Glass and What Alice Found There, 1872).
Lewis Carroll's poem of 1872 is a useful starting point for identifying issues resulting from confusion over the variously described acute aortic syndromes—and, for oysters, the dangers of listening to walruses.
TALK OF MANY THINGS
In cases of aortic dissection (splitting or separation of the layers of the aortic wall), it is important to establish the type (ie, the location and extent) and class (ie, the structure) of the dissection, because these distinctions determine the treatment.1 Similarly, in cases of painful or leaking degenerative aneurysms, we need to know the location of the aneurysm and whether the presenting pain is from compression of surrounding tissue, particularly of the vertebral bodies, or from leakage.
The location and extent of an aortic dissection can be classified in three ways (see Figure 3 in Smith and Schoenhagen’s excellent review of the use of computed tomography [CT] in acute aortic syndromes in this issue of the Cleveland Clinic Journal of Medicine2):
- The DeBakey system (type I, II, or III)
- The Stanford system (type A or B)
- Distal or proximal to the left subclavian artery.
Of note, the DeBakey system does not include tears in the arch that extend distally without ascending involvement. The original Stanford system included arch tears with distal extension in type B; hence, type B excluded all patients without ascending involvement.
The importance of the extent of dissection is that most patients with Stanford type A or DeBakey type I or II dissections should undergo immediate surgery, as most of them would die without it. Surgery is also indicated for arch tears (non-DeBakey, original Stanford type B).
Because these classifications are somewhat confusing, the simplest approach is to note whether the dissection extends proximal or distal to the left subclavian artery, because proximal dissections need surgery and distal ones are first managed medically.
The classes of dissection also have bearing on treatment.1 These are:
- Class I—classic aortic dissection in the media with two lumens separated by a “flap” or septum
- Class II—intramural hematoma in the aortic wall from dissection in which the intimal tear cannot be imaged (these are nearly always found duringsurgery or autopsy)
- Class III—localized confined intimal tears without extensive undermining of the intima or flap formation. These are often seen with Marfan syndrome and can rupture or cause tamponade, as can any type of proximal dissection. The typical appearance is of a bulging bubble in the aortic wall.
- Class IV—penetrating atherosclerotic ulcers with localized dissections or wall hematomas, often with calcium at the base of a mushroom-shaped area of extraluminal contrast. Of note, the plane of dissection is often between the media and adventitia.
- Class V—iatrogenic or posttraumatic dissection.
All class I to class IV tears of the proximal aorta require surgery, whereas distal class IV and V tears may require either open or endovascular surgical intervention. Surgery is also indicated for patients with distal dissections who have severe narrowing of the true lumen, distal ischemia, uncontrolled pain, severe hypertension, or evidence of leaking, particularly with class IV tears.
In distal dissections that are subacute (2–6 week sold), the Investigation of Stent grafts in Patients With Type B Aortic Dissection (INSTEAD) trial found that inserting a stent prophylactically provided no benefit. Further-more, there is no proof that stenting is beneficial if the aortic dissection is chronic, ie, more than 6 weeks old.1,3–5
WHICH SHOE FITS?
There is no ideal procedure to detect dissection, although the trend is towards CT angiography, as Smith and Schoenhagen report.2 Although some investigators have optimistically estimated CT’s sensitivity and specificity as 100%, cardiovascular surgeons are well aware of both false-positive and false-negative CT studies. Thus, for emergency repairs of proximal dissections, transesophageal echocardiography should be done after intubation and before opening a patient’s chest if time allows. Magnetic resonance imaging, CT, and transesophageal echocardiography may all miss class III tears, but these are frequently evidenced by eccentric “bubbles”or “ballooning.”1
SHIPS
Patients with either acute aortic dissection or severe pain associated with degenerative aneurysms need to be “shipped” promptly to a tertiary medical center after diagnosis, since larger volumes of procedures appear to be associated with better outcomes.
SEALING WAX
Using current surgical methods, the aortic valve can be preserved during aortic dissection repair unless the valve is bicuspid or the patient has Marfan syndrome.1,3,4,6–8
Sealing wax in the form of biological glues, rather than for letters, is a new innovation. A caveat remains, however: we have seen patients who have required reoperation for false aneurysms or infection. Hence, glues should be used with caution.
CABBAGES
A dilemma is whether patients should undergo coronary catheterization (or CT angiography—a separate question) and subsequent coronary artery bypass grafting (CABG), if needed, at the time of aortic dissection repair. The problem is that approximately one-third of patients have coronary artery disease that may require CABG, but the delay for catheterization increases the risk of rupture or tamponade before surgery.
Indeed, 40% of patients with proximal dissections die immediately, and 1% to 3% die in the hour before surgery. The short-term (in-hospital and 30-day) mortality rates range from 3.4% (Cleveland Clinic 2006 data) to 25%, and of the survivors only about 50% area live 5 years after surgery.
Though dismal, the prognosis is improving. In 162 patients with aortic dissection and Marfan syndrome or connective tissue disorders who underwent surgery at Cleveland Clinic in the years 1978–2003, the 5-year survival rate in those with aortic dissection was 75% and the 10-year rate was 55%.7 In those without dissection, the 10-year survival rate was approximately 90% (P < .001).
KINGS
Noted personalities who have had aortic dissection include King George II of England (who died in 1760), Lucille Ball, Conway Twitty, Jan Larson, and most recently John Ritter. None of these famous people survived their aortic dissections. Indeed, dissection and diseases of the aorta or its branches cause between 43,000 and 47,000 deaths annually,9 more than from breast cancer, murders, or motor vehicle accidents. The main reason for these dismal statistics is that the disease is often misdiagnosed at the time of presentation.
BOILING SEA
Careful studies from Olmsted County, Minnesota,10 have shown a tripling of the incidence of aortic disease, particularly in women, even though the rate of deaths from coronary artery disease has been decreasing. Furthermore, Olsson et al11 report that the incidence of aortic dissection in men in Sweden increased to approximately16 per 100,000 per year from 1987 to 2002, a 52% increase. The aging of the population must play a large role, but other factors may exist that are not well understood or defined and require further research.
PIGS HAVE WINGS
Will it be possible to overcome this rising problem? The answer is a definite yes. The results of aortic surgery have never been better. Many new innovations are available, such as aortic root preservation and endovascular stenting procedures. It may be possible to slow the growth of or prevent some aneurysms and aortic dissections, particularly with beta-blockers and, potentially, with losartan (Cozaar) for Marfan syndrome patients.
One of the keys to preventing aortic catastrophes and aortic dissection is to repair aortic aneurysms. The threshold for surgery, however, depends on a surgeon’s experience and results, the underlying pathology, and the aortic size.
We observed that 12.5% of dissections in patients with bicuspid valves and 15% of those in patients with Marfan syndrome were in aortas smaller than 5.0 cm in diameter, that aortic dissection occurred at smaller diameters in shorter patients, and that the risk of dissection increased exponentially with the size of the aorta. Subsequently, we found that a better measure of risk is the maximal aortic cross-sectional area in cm2 divided by the patient’s height in meters; if this ratio exceeds 10, then surgery is recommended.12
Results of surgery are good in experienced hands. In patients who undergo surgical repair of bicuspid aortic valves with or without concurrent repair of the ascending aorta (mostly in patients with an aortic cross-section-to-height ratio > 10), the perioperative mortality rate is about 1.0% for both groups, and at 10 years about 98% of patients are free from re-operation on the aorta and more than 90% are free from re-operation on the aortic valve.8 This is important because these are typically young patients who would do better without biological replacement valves (which are not very durable) or mechanical valves (which necessitate lifelong anticoagulation). Results are also good in surgery of the aortic arch and even better in patients with tricuspid aortic valves.4,6,8
Increasingly, in patients at high risk, we are inserting thoracic, abdominal, and thoracoabdominal stent grafts, with excellent early results. An even newer innovation is to replace the aortic valve in high-risk patients via a transcatheter balloon-expandable valve stent inserted through the groin or left ventricular apex.
These treatment innovations have been big strides, but aortic disease continues to increase. Indeed, our volume of thoracic aortic surgery at Cleveland Clinic increased from 190 procedures in 1999 to 717 in 2006. Early detection—before acute emergency surgery is required, with its concomitant high risk of death—is the key to successful surgical outcome and long-term survival.
- Svensson LG, Labib SB, Eisenhauer AC, Butterly JR. Intimal tear without hematoma: an important variant of aortic dissection that can elude current imaging techniques. Circulation 1999; 99:1331–1336.
- Smith AD, Schoenhagen P. CT imaging for acute aortic syndrome. Cleve Clin J Med 2008; 75:7–24.
- Svensson LG, Nadolny EM, Kimmel WA. Multimodal protocol influence on stroke and neurocognitive deficit prevention after ascending/arch aortic operations. Ann Thorac Surg 2002; 74:2040–2046.
- Svensson LG, Kim KH, Blackstone EH, et al. Elephant trunk procedure: newer indications and uses. Ann Thorac Surg 2004; 78:109–116.
- Greenberg RK, Haddad F, Svensson L, et al. Hybrid approaches to thoracic aortic aneurysms: the role of endovascular elephant trunk completion. Circulation 2005; 112:2619–2626.
- Svensson LG. Sizing for modified David’s reimplantation procedure. Ann Thorac Surg 2003; 76:1751–1753.
- Svensson LG, Blackstone EH, Feng J, et al. Are Marfan syndrome and marfanoid patients distinguishable on long-term follow-up? Ann Thorac Surg 2007; 83:1067–1074.
- Svensson LG, Blackstone EH, Cosgrove DM 3rd. Surgical options in young adults with aortic valve disease. Curr Probl Cardiol 2003; 28:417–480.
- Svensson LG, Rodriguez ER. Aortic organ disease epidemic, and why do balloons pop? Circulation 2005; 112:1082–1084.
- Clouse WD, Hallett JW Jr, Schaff HV, Gayari MM, Ilstrup DM, Melton LJ 3rd. Improved prognosis of thoracic aortic aneurysms: a population-based study. JAMA 1998; 280:1926–1929.
- Olsson C, Thelin S, Ståhle E, Ekbom A, Granath F. Thoracic aortic aneurysm and dissection: increasing prevalence and improved outcomes reported in a nationwide population-based study of more than 14,000 cases from 1987 to 2002. Circulation 2006; 114:2611–2618.
- Svensson LG, Kim KH, Lytle BW, Cosgrove DM. Relationship of aortic cross-sectional area to height ratio and the risk of aortic dissection inpatients with bicuspid aortic valves. J Thorac Cardiovasc Surg 2003;126:892–893.
“The time has come,” the Walrus said,
“To talk of many things:
Of shoes—and ships—and sealing-wax—
Of cabbages—and kings—
And why the sea is boiling hot
And whether pigs have wings.”
—Lewis Carroll, The Walrus and the Carpenter (from Through the Looking-Glass and What Alice Found There, 1872).
Lewis Carroll's poem of 1872 is a useful starting point for identifying issues resulting from confusion over the variously described acute aortic syndromes—and, for oysters, the dangers of listening to walruses.
TALK OF MANY THINGS
In cases of aortic dissection (splitting or separation of the layers of the aortic wall), it is important to establish the type (ie, the location and extent) and class (ie, the structure) of the dissection, because these distinctions determine the treatment.1 Similarly, in cases of painful or leaking degenerative aneurysms, we need to know the location of the aneurysm and whether the presenting pain is from compression of surrounding tissue, particularly of the vertebral bodies, or from leakage.
The location and extent of an aortic dissection can be classified in three ways (see Figure 3 in Smith and Schoenhagen’s excellent review of the use of computed tomography [CT] in acute aortic syndromes in this issue of the Cleveland Clinic Journal of Medicine2):
- The DeBakey system (type I, II, or III)
- The Stanford system (type A or B)
- Distal or proximal to the left subclavian artery.
Of note, the DeBakey system does not include tears in the arch that extend distally without ascending involvement. The original Stanford system included arch tears with distal extension in type B; hence, type B excluded all patients without ascending involvement.
The importance of the extent of dissection is that most patients with Stanford type A or DeBakey type I or II dissections should undergo immediate surgery, as most of them would die without it. Surgery is also indicated for arch tears (non-DeBakey, original Stanford type B).
Because these classifications are somewhat confusing, the simplest approach is to note whether the dissection extends proximal or distal to the left subclavian artery, because proximal dissections need surgery and distal ones are first managed medically.
The classes of dissection also have bearing on treatment.1 These are:
- Class I—classic aortic dissection in the media with two lumens separated by a “flap” or septum
- Class II—intramural hematoma in the aortic wall from dissection in which the intimal tear cannot be imaged (these are nearly always found duringsurgery or autopsy)
- Class III—localized confined intimal tears without extensive undermining of the intima or flap formation. These are often seen with Marfan syndrome and can rupture or cause tamponade, as can any type of proximal dissection. The typical appearance is of a bulging bubble in the aortic wall.
- Class IV—penetrating atherosclerotic ulcers with localized dissections or wall hematomas, often with calcium at the base of a mushroom-shaped area of extraluminal contrast. Of note, the plane of dissection is often between the media and adventitia.
- Class V—iatrogenic or posttraumatic dissection.
All class I to class IV tears of the proximal aorta require surgery, whereas distal class IV and V tears may require either open or endovascular surgical intervention. Surgery is also indicated for patients with distal dissections who have severe narrowing of the true lumen, distal ischemia, uncontrolled pain, severe hypertension, or evidence of leaking, particularly with class IV tears.
In distal dissections that are subacute (2–6 week sold), the Investigation of Stent grafts in Patients With Type B Aortic Dissection (INSTEAD) trial found that inserting a stent prophylactically provided no benefit. Further-more, there is no proof that stenting is beneficial if the aortic dissection is chronic, ie, more than 6 weeks old.1,3–5
WHICH SHOE FITS?
There is no ideal procedure to detect dissection, although the trend is towards CT angiography, as Smith and Schoenhagen report.2 Although some investigators have optimistically estimated CT’s sensitivity and specificity as 100%, cardiovascular surgeons are well aware of both false-positive and false-negative CT studies. Thus, for emergency repairs of proximal dissections, transesophageal echocardiography should be done after intubation and before opening a patient’s chest if time allows. Magnetic resonance imaging, CT, and transesophageal echocardiography may all miss class III tears, but these are frequently evidenced by eccentric “bubbles”or “ballooning.”1
SHIPS
Patients with either acute aortic dissection or severe pain associated with degenerative aneurysms need to be “shipped” promptly to a tertiary medical center after diagnosis, since larger volumes of procedures appear to be associated with better outcomes.
SEALING WAX
Using current surgical methods, the aortic valve can be preserved during aortic dissection repair unless the valve is bicuspid or the patient has Marfan syndrome.1,3,4,6–8
Sealing wax in the form of biological glues, rather than for letters, is a new innovation. A caveat remains, however: we have seen patients who have required reoperation for false aneurysms or infection. Hence, glues should be used with caution.
CABBAGES
A dilemma is whether patients should undergo coronary catheterization (or CT angiography—a separate question) and subsequent coronary artery bypass grafting (CABG), if needed, at the time of aortic dissection repair. The problem is that approximately one-third of patients have coronary artery disease that may require CABG, but the delay for catheterization increases the risk of rupture or tamponade before surgery.
Indeed, 40% of patients with proximal dissections die immediately, and 1% to 3% die in the hour before surgery. The short-term (in-hospital and 30-day) mortality rates range from 3.4% (Cleveland Clinic 2006 data) to 25%, and of the survivors only about 50% area live 5 years after surgery.
Though dismal, the prognosis is improving. In 162 patients with aortic dissection and Marfan syndrome or connective tissue disorders who underwent surgery at Cleveland Clinic in the years 1978–2003, the 5-year survival rate in those with aortic dissection was 75% and the 10-year rate was 55%.7 In those without dissection, the 10-year survival rate was approximately 90% (P < .001).
KINGS
Noted personalities who have had aortic dissection include King George II of England (who died in 1760), Lucille Ball, Conway Twitty, Jan Larson, and most recently John Ritter. None of these famous people survived their aortic dissections. Indeed, dissection and diseases of the aorta or its branches cause between 43,000 and 47,000 deaths annually,9 more than from breast cancer, murders, or motor vehicle accidents. The main reason for these dismal statistics is that the disease is often misdiagnosed at the time of presentation.
BOILING SEA
Careful studies from Olmsted County, Minnesota,10 have shown a tripling of the incidence of aortic disease, particularly in women, even though the rate of deaths from coronary artery disease has been decreasing. Furthermore, Olsson et al11 report that the incidence of aortic dissection in men in Sweden increased to approximately16 per 100,000 per year from 1987 to 2002, a 52% increase. The aging of the population must play a large role, but other factors may exist that are not well understood or defined and require further research.
PIGS HAVE WINGS
Will it be possible to overcome this rising problem? The answer is a definite yes. The results of aortic surgery have never been better. Many new innovations are available, such as aortic root preservation and endovascular stenting procedures. It may be possible to slow the growth of or prevent some aneurysms and aortic dissections, particularly with beta-blockers and, potentially, with losartan (Cozaar) for Marfan syndrome patients.
One of the keys to preventing aortic catastrophes and aortic dissection is to repair aortic aneurysms. The threshold for surgery, however, depends on a surgeon’s experience and results, the underlying pathology, and the aortic size.
We observed that 12.5% of dissections in patients with bicuspid valves and 15% of those in patients with Marfan syndrome were in aortas smaller than 5.0 cm in diameter, that aortic dissection occurred at smaller diameters in shorter patients, and that the risk of dissection increased exponentially with the size of the aorta. Subsequently, we found that a better measure of risk is the maximal aortic cross-sectional area in cm2 divided by the patient’s height in meters; if this ratio exceeds 10, then surgery is recommended.12
Results of surgery are good in experienced hands. In patients who undergo surgical repair of bicuspid aortic valves with or without concurrent repair of the ascending aorta (mostly in patients with an aortic cross-section-to-height ratio > 10), the perioperative mortality rate is about 1.0% for both groups, and at 10 years about 98% of patients are free from re-operation on the aorta and more than 90% are free from re-operation on the aortic valve.8 This is important because these are typically young patients who would do better without biological replacement valves (which are not very durable) or mechanical valves (which necessitate lifelong anticoagulation). Results are also good in surgery of the aortic arch and even better in patients with tricuspid aortic valves.4,6,8
Increasingly, in patients at high risk, we are inserting thoracic, abdominal, and thoracoabdominal stent grafts, with excellent early results. An even newer innovation is to replace the aortic valve in high-risk patients via a transcatheter balloon-expandable valve stent inserted through the groin or left ventricular apex.
These treatment innovations have been big strides, but aortic disease continues to increase. Indeed, our volume of thoracic aortic surgery at Cleveland Clinic increased from 190 procedures in 1999 to 717 in 2006. Early detection—before acute emergency surgery is required, with its concomitant high risk of death—is the key to successful surgical outcome and long-term survival.
“The time has come,” the Walrus said,
“To talk of many things:
Of shoes—and ships—and sealing-wax—
Of cabbages—and kings—
And why the sea is boiling hot
And whether pigs have wings.”
—Lewis Carroll, The Walrus and the Carpenter (from Through the Looking-Glass and What Alice Found There, 1872).
Lewis Carroll's poem of 1872 is a useful starting point for identifying issues resulting from confusion over the variously described acute aortic syndromes—and, for oysters, the dangers of listening to walruses.
TALK OF MANY THINGS
In cases of aortic dissection (splitting or separation of the layers of the aortic wall), it is important to establish the type (ie, the location and extent) and class (ie, the structure) of the dissection, because these distinctions determine the treatment.1 Similarly, in cases of painful or leaking degenerative aneurysms, we need to know the location of the aneurysm and whether the presenting pain is from compression of surrounding tissue, particularly of the vertebral bodies, or from leakage.
The location and extent of an aortic dissection can be classified in three ways (see Figure 3 in Smith and Schoenhagen’s excellent review of the use of computed tomography [CT] in acute aortic syndromes in this issue of the Cleveland Clinic Journal of Medicine2):
- The DeBakey system (type I, II, or III)
- The Stanford system (type A or B)
- Distal or proximal to the left subclavian artery.
Of note, the DeBakey system does not include tears in the arch that extend distally without ascending involvement. The original Stanford system included arch tears with distal extension in type B; hence, type B excluded all patients without ascending involvement.
The importance of the extent of dissection is that most patients with Stanford type A or DeBakey type I or II dissections should undergo immediate surgery, as most of them would die without it. Surgery is also indicated for arch tears (non-DeBakey, original Stanford type B).
Because these classifications are somewhat confusing, the simplest approach is to note whether the dissection extends proximal or distal to the left subclavian artery, because proximal dissections need surgery and distal ones are first managed medically.
The classes of dissection also have bearing on treatment.1 These are:
- Class I—classic aortic dissection in the media with two lumens separated by a “flap” or septum
- Class II—intramural hematoma in the aortic wall from dissection in which the intimal tear cannot be imaged (these are nearly always found duringsurgery or autopsy)
- Class III—localized confined intimal tears without extensive undermining of the intima or flap formation. These are often seen with Marfan syndrome and can rupture or cause tamponade, as can any type of proximal dissection. The typical appearance is of a bulging bubble in the aortic wall.
- Class IV—penetrating atherosclerotic ulcers with localized dissections or wall hematomas, often with calcium at the base of a mushroom-shaped area of extraluminal contrast. Of note, the plane of dissection is often between the media and adventitia.
- Class V—iatrogenic or posttraumatic dissection.
All class I to class IV tears of the proximal aorta require surgery, whereas distal class IV and V tears may require either open or endovascular surgical intervention. Surgery is also indicated for patients with distal dissections who have severe narrowing of the true lumen, distal ischemia, uncontrolled pain, severe hypertension, or evidence of leaking, particularly with class IV tears.
In distal dissections that are subacute (2–6 week sold), the Investigation of Stent grafts in Patients With Type B Aortic Dissection (INSTEAD) trial found that inserting a stent prophylactically provided no benefit. Further-more, there is no proof that stenting is beneficial if the aortic dissection is chronic, ie, more than 6 weeks old.1,3–5
WHICH SHOE FITS?
There is no ideal procedure to detect dissection, although the trend is towards CT angiography, as Smith and Schoenhagen report.2 Although some investigators have optimistically estimated CT’s sensitivity and specificity as 100%, cardiovascular surgeons are well aware of both false-positive and false-negative CT studies. Thus, for emergency repairs of proximal dissections, transesophageal echocardiography should be done after intubation and before opening a patient’s chest if time allows. Magnetic resonance imaging, CT, and transesophageal echocardiography may all miss class III tears, but these are frequently evidenced by eccentric “bubbles”or “ballooning.”1
SHIPS
Patients with either acute aortic dissection or severe pain associated with degenerative aneurysms need to be “shipped” promptly to a tertiary medical center after diagnosis, since larger volumes of procedures appear to be associated with better outcomes.
SEALING WAX
Using current surgical methods, the aortic valve can be preserved during aortic dissection repair unless the valve is bicuspid or the patient has Marfan syndrome.1,3,4,6–8
Sealing wax in the form of biological glues, rather than for letters, is a new innovation. A caveat remains, however: we have seen patients who have required reoperation for false aneurysms or infection. Hence, glues should be used with caution.
CABBAGES
A dilemma is whether patients should undergo coronary catheterization (or CT angiography—a separate question) and subsequent coronary artery bypass grafting (CABG), if needed, at the time of aortic dissection repair. The problem is that approximately one-third of patients have coronary artery disease that may require CABG, but the delay for catheterization increases the risk of rupture or tamponade before surgery.
Indeed, 40% of patients with proximal dissections die immediately, and 1% to 3% die in the hour before surgery. The short-term (in-hospital and 30-day) mortality rates range from 3.4% (Cleveland Clinic 2006 data) to 25%, and of the survivors only about 50% area live 5 years after surgery.
Though dismal, the prognosis is improving. In 162 patients with aortic dissection and Marfan syndrome or connective tissue disorders who underwent surgery at Cleveland Clinic in the years 1978–2003, the 5-year survival rate in those with aortic dissection was 75% and the 10-year rate was 55%.7 In those without dissection, the 10-year survival rate was approximately 90% (P < .001).
KINGS
Noted personalities who have had aortic dissection include King George II of England (who died in 1760), Lucille Ball, Conway Twitty, Jan Larson, and most recently John Ritter. None of these famous people survived their aortic dissections. Indeed, dissection and diseases of the aorta or its branches cause between 43,000 and 47,000 deaths annually,9 more than from breast cancer, murders, or motor vehicle accidents. The main reason for these dismal statistics is that the disease is often misdiagnosed at the time of presentation.
BOILING SEA
Careful studies from Olmsted County, Minnesota,10 have shown a tripling of the incidence of aortic disease, particularly in women, even though the rate of deaths from coronary artery disease has been decreasing. Furthermore, Olsson et al11 report that the incidence of aortic dissection in men in Sweden increased to approximately16 per 100,000 per year from 1987 to 2002, a 52% increase. The aging of the population must play a large role, but other factors may exist that are not well understood or defined and require further research.
PIGS HAVE WINGS
Will it be possible to overcome this rising problem? The answer is a definite yes. The results of aortic surgery have never been better. Many new innovations are available, such as aortic root preservation and endovascular stenting procedures. It may be possible to slow the growth of or prevent some aneurysms and aortic dissections, particularly with beta-blockers and, potentially, with losartan (Cozaar) for Marfan syndrome patients.
One of the keys to preventing aortic catastrophes and aortic dissection is to repair aortic aneurysms. The threshold for surgery, however, depends on a surgeon’s experience and results, the underlying pathology, and the aortic size.
We observed that 12.5% of dissections in patients with bicuspid valves and 15% of those in patients with Marfan syndrome were in aortas smaller than 5.0 cm in diameter, that aortic dissection occurred at smaller diameters in shorter patients, and that the risk of dissection increased exponentially with the size of the aorta. Subsequently, we found that a better measure of risk is the maximal aortic cross-sectional area in cm2 divided by the patient’s height in meters; if this ratio exceeds 10, then surgery is recommended.12
Results of surgery are good in experienced hands. In patients who undergo surgical repair of bicuspid aortic valves with or without concurrent repair of the ascending aorta (mostly in patients with an aortic cross-section-to-height ratio > 10), the perioperative mortality rate is about 1.0% for both groups, and at 10 years about 98% of patients are free from re-operation on the aorta and more than 90% are free from re-operation on the aortic valve.8 This is important because these are typically young patients who would do better without biological replacement valves (which are not very durable) or mechanical valves (which necessitate lifelong anticoagulation). Results are also good in surgery of the aortic arch and even better in patients with tricuspid aortic valves.4,6,8
Increasingly, in patients at high risk, we are inserting thoracic, abdominal, and thoracoabdominal stent grafts, with excellent early results. An even newer innovation is to replace the aortic valve in high-risk patients via a transcatheter balloon-expandable valve stent inserted through the groin or left ventricular apex.
These treatment innovations have been big strides, but aortic disease continues to increase. Indeed, our volume of thoracic aortic surgery at Cleveland Clinic increased from 190 procedures in 1999 to 717 in 2006. Early detection—before acute emergency surgery is required, with its concomitant high risk of death—is the key to successful surgical outcome and long-term survival.
- Svensson LG, Labib SB, Eisenhauer AC, Butterly JR. Intimal tear without hematoma: an important variant of aortic dissection that can elude current imaging techniques. Circulation 1999; 99:1331–1336.
- Smith AD, Schoenhagen P. CT imaging for acute aortic syndrome. Cleve Clin J Med 2008; 75:7–24.
- Svensson LG, Nadolny EM, Kimmel WA. Multimodal protocol influence on stroke and neurocognitive deficit prevention after ascending/arch aortic operations. Ann Thorac Surg 2002; 74:2040–2046.
- Svensson LG, Kim KH, Blackstone EH, et al. Elephant trunk procedure: newer indications and uses. Ann Thorac Surg 2004; 78:109–116.
- Greenberg RK, Haddad F, Svensson L, et al. Hybrid approaches to thoracic aortic aneurysms: the role of endovascular elephant trunk completion. Circulation 2005; 112:2619–2626.
- Svensson LG. Sizing for modified David’s reimplantation procedure. Ann Thorac Surg 2003; 76:1751–1753.
- Svensson LG, Blackstone EH, Feng J, et al. Are Marfan syndrome and marfanoid patients distinguishable on long-term follow-up? Ann Thorac Surg 2007; 83:1067–1074.
- Svensson LG, Blackstone EH, Cosgrove DM 3rd. Surgical options in young adults with aortic valve disease. Curr Probl Cardiol 2003; 28:417–480.
- Svensson LG, Rodriguez ER. Aortic organ disease epidemic, and why do balloons pop? Circulation 2005; 112:1082–1084.
- Clouse WD, Hallett JW Jr, Schaff HV, Gayari MM, Ilstrup DM, Melton LJ 3rd. Improved prognosis of thoracic aortic aneurysms: a population-based study. JAMA 1998; 280:1926–1929.
- Olsson C, Thelin S, Ståhle E, Ekbom A, Granath F. Thoracic aortic aneurysm and dissection: increasing prevalence and improved outcomes reported in a nationwide population-based study of more than 14,000 cases from 1987 to 2002. Circulation 2006; 114:2611–2618.
- Svensson LG, Kim KH, Lytle BW, Cosgrove DM. Relationship of aortic cross-sectional area to height ratio and the risk of aortic dissection inpatients with bicuspid aortic valves. J Thorac Cardiovasc Surg 2003;126:892–893.
- Svensson LG, Labib SB, Eisenhauer AC, Butterly JR. Intimal tear without hematoma: an important variant of aortic dissection that can elude current imaging techniques. Circulation 1999; 99:1331–1336.
- Smith AD, Schoenhagen P. CT imaging for acute aortic syndrome. Cleve Clin J Med 2008; 75:7–24.
- Svensson LG, Nadolny EM, Kimmel WA. Multimodal protocol influence on stroke and neurocognitive deficit prevention after ascending/arch aortic operations. Ann Thorac Surg 2002; 74:2040–2046.
- Svensson LG, Kim KH, Blackstone EH, et al. Elephant trunk procedure: newer indications and uses. Ann Thorac Surg 2004; 78:109–116.
- Greenberg RK, Haddad F, Svensson L, et al. Hybrid approaches to thoracic aortic aneurysms: the role of endovascular elephant trunk completion. Circulation 2005; 112:2619–2626.
- Svensson LG. Sizing for modified David’s reimplantation procedure. Ann Thorac Surg 2003; 76:1751–1753.
- Svensson LG, Blackstone EH, Feng J, et al. Are Marfan syndrome and marfanoid patients distinguishable on long-term follow-up? Ann Thorac Surg 2007; 83:1067–1074.
- Svensson LG, Blackstone EH, Cosgrove DM 3rd. Surgical options in young adults with aortic valve disease. Curr Probl Cardiol 2003; 28:417–480.
- Svensson LG, Rodriguez ER. Aortic organ disease epidemic, and why do balloons pop? Circulation 2005; 112:1082–1084.
- Clouse WD, Hallett JW Jr, Schaff HV, Gayari MM, Ilstrup DM, Melton LJ 3rd. Improved prognosis of thoracic aortic aneurysms: a population-based study. JAMA 1998; 280:1926–1929.
- Olsson C, Thelin S, Ståhle E, Ekbom A, Granath F. Thoracic aortic aneurysm and dissection: increasing prevalence and improved outcomes reported in a nationwide population-based study of more than 14,000 cases from 1987 to 2002. Circulation 2006; 114:2611–2618.
- Svensson LG, Kim KH, Lytle BW, Cosgrove DM. Relationship of aortic cross-sectional area to height ratio and the risk of aortic dissection inpatients with bicuspid aortic valves. J Thorac Cardiovasc Surg 2003;126:892–893.
What is the most important public health problem facing the world today and how should it be addressed?
Urticarial Vasculitis in an Infant
Sigh syndrome: Is it a sign of trouble?
- Sigh syndrome is a genuine medical diagnosis with distinct criteria, conferring significant stress for those affected. Despite outward signs of an abnormal breathing pattern, this symptomatology is unrelated to any respiratory or organic pathology.
- Ancillary testing and medication seem unnecessary; supporting reassurance appears sufficient, since the syndrome has a favorable outcome.
Objective The goal of this study was to identify the characteristics and clinical course of patients presenting with considerable stress regarding irrepressible persistent sighing, and to determine whether any association exists between this syndrome and respiratory or other organic disease during the acute or follow-up period.
Study design We conducted a case series review of patients diagnosed with a defined symptom complex and gathered relevant data.
Population Forty patients who presented to 3 clinics in Israel met our 10 criteria for sigh syndrome: recurrent sighing (at least once a minute, for varying lengths of time throughout the day); otherwise shallow respiration; patient conviction that deep breaths are obstructed; intensity of episodes provokes stress leading to consultation; no obvious trigger; episodes last a few days to several weeks; no interference with speech; sighing is absent during sleep; no correlation with physical activity or rest; and self-limited.
Outcomes measured We assessed demographic and health status information, as well as recent circumstances that could have served as triggers for the symptoms. We also performed systematic diagnoses of acute and chronic organic disease.
Results Physicians diagnosed “sigh syndrome” in 40 subjects (19 men [47.5%]), mean age 31.8 years, during the 3-year study period. All patients conformed to 10 sigh syndrome criteria. In 13 patients (32.5%), a significant traumatic event preceded onset of symptoms. Ten (25%) had previous anxiety or somatoform-related disorders. For 23 patients (57.5%), the sigh syndrome episode repeated itself after an initial episode. We found no association in any of the cases with any form of organic disease. Likewise, during the follow-up period (on average, 18 months), we did not observe the development of a specific organic disorder in any case.
Conclusions The “sigh syndrome” runs a benign course; it mainly demands the support and understanding of the treating physician to allay any patient concerns.
In our clinical practices, we have repeatedly cared for patients who came into our clinics because of a worrisome irregular breathing pattern characterized by a deep inspiration, and followed by a noisy expiration. We have referred to the set of clinical signs that these patients present with as “sigh syndrome.”
We have long suspected that sigh syndrome is an underdiagnosed and self-limited condition that is often mistaken for a serious respiratory disorder. In our experience, this syndrome runs a benign course. However, we believed that this syndrome had characteristic and consistent features, and should not be considered a diagnosis of exclusion.
Thus, we undertook a study to observe a group of subjects with these features to judge whether this subjectively alarming symptom complex is in fact harmless, and whether it is appropriate to respond to it as we had, by taking a stress-alleviating approach alone.
What is sigh syndrome?
Patients with sigh syndrome exhibit a compulsion to perform single but repeated deep inspirations, accompanied by a sensation of difficulty in inhaling a sufficient quantity of air. Each inspiration is followed by a prolonged, sometimes noisy expiration—namely, a sigh. Observing such abnormal breaths and confirming that the patient feels a concomitant inability to fill his lungs to capacity is sufficient to make the diagnosis.
This breathing compulsion is irregular in nature: It may occur once a minute or several times a minute, and this breathing pattern may continue—on and off throughout the day—for a few days to several weeks. In our experience, it provokes significant anxiety in patients, prompting them to seek medical advice. It does not occur when the patient is asleep, and it is not triggered by physical activity.
Both patient and doctor may, at first, be convinced that the problem reflects a serious illness. The 10 features of sigh syndrome (TABLE 1) constitute a proposed definition. All of our study subjects exhibited these 10 features.
TABLE 1
10 features of sigh syndrome
|
Sighing as an illness marker
Sighing has been described as one member of a group of signs exhibited by depressed or anxiety-ridden patients.1 While Perin et al2 were the first to point out the importance of distinguishing between sighing and respiratory disease, sighing per se has never been identified as a discrete illness marker.
A number of psychiatric disorders are already well known to incorporate breathing and chest symptoms along with widespread somatization. These include globus hystericus, neurocirculatory asthenia, and Tietze syndrome.3-6 As such, the acute pain of precordial catch syndrome stands out as an example of a distinguishable, clear-cut clinical state devoid of any apparent organic basis.7,8
Methods
How we recruited the patients
Data was collected from 3 family practice clinics in Israel from February 2002 to February 2005. We requested that these practices contribute data of consecutive clinical cases presenting with the 10 set symptoms of sigh syndrome (TABLE 1).
Data collected included basic demographics, the circumstances of the onset of symptoms, concurrent medical conditions, and any associated symptoms. We assessed the patients’ education level by asking questions pertaining to their years of schooling and college degrees. Patients rated their own economic status as being below, average, or above-average income.
The main outcome we examined was the clinical course of the sighing episodes during the ensuing months after their visit, in order to determine whether any patients developed a form of significant organic disease or a disorder that led to hospitalization.
Results
40 cases that cut across the socioeconomic spectrum
Forty patients were recruited for this study. Nineteen (47.5%) were male; their ages ranged from 7 to 53 (mean, 31.8; standard deviation, 13.7). Two patients (5%) were Ashkenazi Jews; 34 (85%) were of North African ethnicity (Sephardic Jews); the other 4 were of varied Asian and European ethnicity. The number of patients with North African ethnicity overrepresents that of the population in their communities. Additionally, 3 members of this group were from the same family.
There was no predilection toward any specific education level or socioeconomic status. The occupations of the subjects were diverse.
Their clinical characteristics
The clinical characteristics of the 40 patients are presented in TABLE 2. The subjects’ sighing began at various times of the day, without relationship to eating or any other activity, and disappeared during sleep. All patients reported the same feeling: that of an extra effort demanded to perform full inspiration. In many cases, adult patients were certain their complaints were a sign of cardiac or respiratory disease, and they were very concerned that there was some grave, underlying disorder.
History and examination failed to reveal evidence of any somatic findings related to breathing difficulty. Breathing rate was within normal limits in all cases.
The physicians’ initial encounters with these patients led to further examination in many cases: electrocardiography, blood oxygen saturation, and complete blood counts. However, no abnormalities were found on any of these tests. Medications, if prescribed at all during these consultations, were usually given to alleviate insomnia or anxiety. Further ancillary investigations or referrals were not ordered.
The sole notable finding on physical examination was a typical murmur (which had already been diagnosed) in a young girl with a congenital atrial septal defect. This 7-year-old developed repeated episodes of sigh syndrome just before her annual visit to the pediatric cardiologist; her mother believed that the child was frightened by the thought of possible future surgery.
TABLE 2
Clinical characteristics of the 40 patients studied—One third experienced a traumatic event
| CHARACTERISTIC | YES | NO |
|---|---|---|
| Smoker | 2 (5%) | 38 (95%) |
| History of anxiety or somatoform disorder | 10 (25%) | 30 (75%) |
| Taking prescription medication at time of diagnosis | 4 (10%) | 36 (90%) |
| Recurrence of sighing episodes during follow-up period | 24 (60%) | 16 (40%) |
| Trigger event (eg, exposure to traumatic event 1 month before presentation with syndrome) | 13 (32.5%) | 27 (67.5%) |
Traumatic events, anxiety disorders suggest stress as a cause
Thirteen patient histories disclosed a definite, recent, significant traumatic event that may have triggered the onset of sigh syndrome. Examples of 2 triggering events are the terrorist murder of several members of a neighbor’s family, and a near-miss with a mortar shell. One subject—a teenager—had recently been left alone in the dark with 2 younger siblings during a power blackout; another young woman said that the sighing episodes began when she decided to get married.
Ten patients had previously diagnosed neurotic disorders, mainly generalized anxiety; these included 2 cases of somatization disorder and 1 case of posttraumatic stress disorder. This information from the patients’ histories was documented in their medical files.
Episodes appear to be self-limited
In all patients, the episodes were self-limited. During the follow-up period, lasting an average of 18 months, none of the patients showed additional medical conditions—respiratory or otherwise—that could be linked to episodes of sigh syndrome. Recurrences of sighing episodes were reported by 24 subjects (60%) after the marker episode. One patient was diagnosed with carcinoma of the pancreas 2 years into follow-up, and later died.
Discussion
A benign, transient disorder
Aside from the solitary and unrelated death noted above, examination and follow-up in all 40 cases did not lead to an alternative diagnosis. Sigh syndrome thus seems to be an entirely benign and transient condition with no sequelae aside from possible recurrences.
Although the pathophysiology is unclear, our finding that 32.5% of patients had a recent traumatic incident strongly suggests a stress-related condition. Furthermore, 25% of the patients were already known to suffer from intermittent anxiety or somatoform disorders, although none were taking medications for these conditions. This adds support to the assumption that a mind-body interaction is underpinning the disorder. Large-scale migration, recent war or terrorist acts, or natural disaster are likely to increase the chances that the average physician will see a patient with sigh syndrome.
A tendency towards North African/Sephardic ethnicity, rather than European ethnicity—in addition to the cluster of 3 cases belonging to the same family—suggests the presentation may be a subconscious cultural, learned, or adopted expression of uneasiness.
Making your evaluation: History and physical are enough
The diagnostic evaluation of sigh syndrome—consisting of careful history-taking and a thorough physical examination—should be sufficient to differentiate it from an array of organic diseases. A physical examination is imperative to exclude other causes for this breathing abnormality.
Ancillary testing is rarely, if ever, indicated. It can perhaps be justified only if the condition is accompanied by an additional (if serendipitous) finding such as the cardiac murmur in the 7-year-old girl noted earlier. Physicians sometimes perform unnecessary investigations, being reluctant to base their diagnoses solely on their clinical expertise.9 A patient may interpret this testing as uncertainty or begin to doubt the diagnosis, thus augmenting—rather than reducing—any anxiety.10 The additional burden of the costs and possible side effects compound the futility of testing indiscriminately.11
Identifying these symptoms with the name “sigh syndrome,” and basing this diagnosis on the history and physical examination, stresses certainty and familiarity with the diagnosis.9 Not only does this reassure the patient, but it eases communication between professionals and forms a basis for research.
Management: Reassure your patient
Management of sigh syndrome consists largely of providing reassurances to your patient. You should emphasize that the condition is real, albeit benign, and that you understand the concern it causes.
Further treatment is unnecessary, aside perhaps from addressing any associated anxiety. A self-limiting (if sometimes recurrent) course can be confidently predicted, and follow-up visits can safely be left to the patient’s own discretion. Since the major correlation with sigh syndrome seems to be stress and the experience of a recent traumatic event, you should always investigate these 2 possibilities when taking the history of a patient with suspected sigh syndrome.
Acknowledgments
This work was inspired and developed by arthur Furst, MD, who died following the submission of this manuscript. Dr Furst was a distinguished and dedicated family physician, a thorough researcher, and a renowned tutor. We dedicate this article to the fond memory of a true leader in the field of rural medicine, and an exceptionally funny and amicable colleague.
Correspondence
Abby Naimer Sody, MD, Gush Katif Health Center, Neve Dekalim, Goosh Katif, Israel 79779; sodyna@clalit.org.il
1. Rakel RE. Textbook of Family Practice. 6th ed. St louis, Mo: WB Saunders; 2002.
2. Perin PV, Perin RJ, Rooklin AR. When a sigh is just a sigh…and not asthma. Ann Allergy 1993;71:478-480.
3. Wilhelm FH, Gevirtz R, Roth WT. Respiratory dys-regulation in anxiety, functional cardiac, and pain disorders. Assessment, phenomenology, and treatment. Behav Modif 2001;25:513-45.
4. Malcomson KG. Globus hystericus vel pharyngis (a reconnaissance of proximal vagal modalities). J Laryngol Otol 1968;82:219-230.
5. Ravich WJ, Wilson RS, Jones B, Donner MW. Psychogenic dysphagia and globus: reevaluation of 23 patients. Dysphagia 1989;4:35-38.
6. Eifert GHB. Cardiophobia: a paradigmatic behavioural model of heart-focused anxiety and non-anginal chest pain. Behav Res Ther 1992;30:329-345.
7. Miller AJ, Texidor TA. “Precordial catch,” a syndrome of anterior chest pain. Ann Intern Med 1959;51:461-467.
8. Sparrow MJ, Bird EL. “Precordial catch”: a benign syndrome of chest pain in young persons. NZ Med J 1978;88:325-326.
9. Balint M. The Doctor, his Patient and the Illness. 2nd ed. London: Sir Isaac Pitman & Sons, 1964.
10. Salmon P. The potentially somatizing effect of clinical consultation. CNS Spectr 2006;11:190-200.
11. Hajioff D, Lowe D. The diagnostic value of barium swallow in globus syndrome. Int J Clin Pract 2004;58:86-89.
- Sigh syndrome is a genuine medical diagnosis with distinct criteria, conferring significant stress for those affected. Despite outward signs of an abnormal breathing pattern, this symptomatology is unrelated to any respiratory or organic pathology.
- Ancillary testing and medication seem unnecessary; supporting reassurance appears sufficient, since the syndrome has a favorable outcome.
Objective The goal of this study was to identify the characteristics and clinical course of patients presenting with considerable stress regarding irrepressible persistent sighing, and to determine whether any association exists between this syndrome and respiratory or other organic disease during the acute or follow-up period.
Study design We conducted a case series review of patients diagnosed with a defined symptom complex and gathered relevant data.
Population Forty patients who presented to 3 clinics in Israel met our 10 criteria for sigh syndrome: recurrent sighing (at least once a minute, for varying lengths of time throughout the day); otherwise shallow respiration; patient conviction that deep breaths are obstructed; intensity of episodes provokes stress leading to consultation; no obvious trigger; episodes last a few days to several weeks; no interference with speech; sighing is absent during sleep; no correlation with physical activity or rest; and self-limited.
Outcomes measured We assessed demographic and health status information, as well as recent circumstances that could have served as triggers for the symptoms. We also performed systematic diagnoses of acute and chronic organic disease.
Results Physicians diagnosed “sigh syndrome” in 40 subjects (19 men [47.5%]), mean age 31.8 years, during the 3-year study period. All patients conformed to 10 sigh syndrome criteria. In 13 patients (32.5%), a significant traumatic event preceded onset of symptoms. Ten (25%) had previous anxiety or somatoform-related disorders. For 23 patients (57.5%), the sigh syndrome episode repeated itself after an initial episode. We found no association in any of the cases with any form of organic disease. Likewise, during the follow-up period (on average, 18 months), we did not observe the development of a specific organic disorder in any case.
Conclusions The “sigh syndrome” runs a benign course; it mainly demands the support and understanding of the treating physician to allay any patient concerns.
In our clinical practices, we have repeatedly cared for patients who came into our clinics because of a worrisome irregular breathing pattern characterized by a deep inspiration, and followed by a noisy expiration. We have referred to the set of clinical signs that these patients present with as “sigh syndrome.”
We have long suspected that sigh syndrome is an underdiagnosed and self-limited condition that is often mistaken for a serious respiratory disorder. In our experience, this syndrome runs a benign course. However, we believed that this syndrome had characteristic and consistent features, and should not be considered a diagnosis of exclusion.
Thus, we undertook a study to observe a group of subjects with these features to judge whether this subjectively alarming symptom complex is in fact harmless, and whether it is appropriate to respond to it as we had, by taking a stress-alleviating approach alone.
What is sigh syndrome?
Patients with sigh syndrome exhibit a compulsion to perform single but repeated deep inspirations, accompanied by a sensation of difficulty in inhaling a sufficient quantity of air. Each inspiration is followed by a prolonged, sometimes noisy expiration—namely, a sigh. Observing such abnormal breaths and confirming that the patient feels a concomitant inability to fill his lungs to capacity is sufficient to make the diagnosis.
This breathing compulsion is irregular in nature: It may occur once a minute or several times a minute, and this breathing pattern may continue—on and off throughout the day—for a few days to several weeks. In our experience, it provokes significant anxiety in patients, prompting them to seek medical advice. It does not occur when the patient is asleep, and it is not triggered by physical activity.
Both patient and doctor may, at first, be convinced that the problem reflects a serious illness. The 10 features of sigh syndrome (TABLE 1) constitute a proposed definition. All of our study subjects exhibited these 10 features.
TABLE 1
10 features of sigh syndrome
|
Sighing as an illness marker
Sighing has been described as one member of a group of signs exhibited by depressed or anxiety-ridden patients.1 While Perin et al2 were the first to point out the importance of distinguishing between sighing and respiratory disease, sighing per se has never been identified as a discrete illness marker.
A number of psychiatric disorders are already well known to incorporate breathing and chest symptoms along with widespread somatization. These include globus hystericus, neurocirculatory asthenia, and Tietze syndrome.3-6 As such, the acute pain of precordial catch syndrome stands out as an example of a distinguishable, clear-cut clinical state devoid of any apparent organic basis.7,8
Methods
How we recruited the patients
Data was collected from 3 family practice clinics in Israel from February 2002 to February 2005. We requested that these practices contribute data of consecutive clinical cases presenting with the 10 set symptoms of sigh syndrome (TABLE 1).
Data collected included basic demographics, the circumstances of the onset of symptoms, concurrent medical conditions, and any associated symptoms. We assessed the patients’ education level by asking questions pertaining to their years of schooling and college degrees. Patients rated their own economic status as being below, average, or above-average income.
The main outcome we examined was the clinical course of the sighing episodes during the ensuing months after their visit, in order to determine whether any patients developed a form of significant organic disease or a disorder that led to hospitalization.
Results
40 cases that cut across the socioeconomic spectrum
Forty patients were recruited for this study. Nineteen (47.5%) were male; their ages ranged from 7 to 53 (mean, 31.8; standard deviation, 13.7). Two patients (5%) were Ashkenazi Jews; 34 (85%) were of North African ethnicity (Sephardic Jews); the other 4 were of varied Asian and European ethnicity. The number of patients with North African ethnicity overrepresents that of the population in their communities. Additionally, 3 members of this group were from the same family.
There was no predilection toward any specific education level or socioeconomic status. The occupations of the subjects were diverse.
Their clinical characteristics
The clinical characteristics of the 40 patients are presented in TABLE 2. The subjects’ sighing began at various times of the day, without relationship to eating or any other activity, and disappeared during sleep. All patients reported the same feeling: that of an extra effort demanded to perform full inspiration. In many cases, adult patients were certain their complaints were a sign of cardiac or respiratory disease, and they were very concerned that there was some grave, underlying disorder.
History and examination failed to reveal evidence of any somatic findings related to breathing difficulty. Breathing rate was within normal limits in all cases.
The physicians’ initial encounters with these patients led to further examination in many cases: electrocardiography, blood oxygen saturation, and complete blood counts. However, no abnormalities were found on any of these tests. Medications, if prescribed at all during these consultations, were usually given to alleviate insomnia or anxiety. Further ancillary investigations or referrals were not ordered.
The sole notable finding on physical examination was a typical murmur (which had already been diagnosed) in a young girl with a congenital atrial septal defect. This 7-year-old developed repeated episodes of sigh syndrome just before her annual visit to the pediatric cardiologist; her mother believed that the child was frightened by the thought of possible future surgery.
TABLE 2
Clinical characteristics of the 40 patients studied—One third experienced a traumatic event
| CHARACTERISTIC | YES | NO |
|---|---|---|
| Smoker | 2 (5%) | 38 (95%) |
| History of anxiety or somatoform disorder | 10 (25%) | 30 (75%) |
| Taking prescription medication at time of diagnosis | 4 (10%) | 36 (90%) |
| Recurrence of sighing episodes during follow-up period | 24 (60%) | 16 (40%) |
| Trigger event (eg, exposure to traumatic event 1 month before presentation with syndrome) | 13 (32.5%) | 27 (67.5%) |
Traumatic events, anxiety disorders suggest stress as a cause
Thirteen patient histories disclosed a definite, recent, significant traumatic event that may have triggered the onset of sigh syndrome. Examples of 2 triggering events are the terrorist murder of several members of a neighbor’s family, and a near-miss with a mortar shell. One subject—a teenager—had recently been left alone in the dark with 2 younger siblings during a power blackout; another young woman said that the sighing episodes began when she decided to get married.
Ten patients had previously diagnosed neurotic disorders, mainly generalized anxiety; these included 2 cases of somatization disorder and 1 case of posttraumatic stress disorder. This information from the patients’ histories was documented in their medical files.
Episodes appear to be self-limited
In all patients, the episodes were self-limited. During the follow-up period, lasting an average of 18 months, none of the patients showed additional medical conditions—respiratory or otherwise—that could be linked to episodes of sigh syndrome. Recurrences of sighing episodes were reported by 24 subjects (60%) after the marker episode. One patient was diagnosed with carcinoma of the pancreas 2 years into follow-up, and later died.
Discussion
A benign, transient disorder
Aside from the solitary and unrelated death noted above, examination and follow-up in all 40 cases did not lead to an alternative diagnosis. Sigh syndrome thus seems to be an entirely benign and transient condition with no sequelae aside from possible recurrences.
Although the pathophysiology is unclear, our finding that 32.5% of patients had a recent traumatic incident strongly suggests a stress-related condition. Furthermore, 25% of the patients were already known to suffer from intermittent anxiety or somatoform disorders, although none were taking medications for these conditions. This adds support to the assumption that a mind-body interaction is underpinning the disorder. Large-scale migration, recent war or terrorist acts, or natural disaster are likely to increase the chances that the average physician will see a patient with sigh syndrome.
A tendency towards North African/Sephardic ethnicity, rather than European ethnicity—in addition to the cluster of 3 cases belonging to the same family—suggests the presentation may be a subconscious cultural, learned, or adopted expression of uneasiness.
Making your evaluation: History and physical are enough
The diagnostic evaluation of sigh syndrome—consisting of careful history-taking and a thorough physical examination—should be sufficient to differentiate it from an array of organic diseases. A physical examination is imperative to exclude other causes for this breathing abnormality.
Ancillary testing is rarely, if ever, indicated. It can perhaps be justified only if the condition is accompanied by an additional (if serendipitous) finding such as the cardiac murmur in the 7-year-old girl noted earlier. Physicians sometimes perform unnecessary investigations, being reluctant to base their diagnoses solely on their clinical expertise.9 A patient may interpret this testing as uncertainty or begin to doubt the diagnosis, thus augmenting—rather than reducing—any anxiety.10 The additional burden of the costs and possible side effects compound the futility of testing indiscriminately.11
Identifying these symptoms with the name “sigh syndrome,” and basing this diagnosis on the history and physical examination, stresses certainty and familiarity with the diagnosis.9 Not only does this reassure the patient, but it eases communication between professionals and forms a basis for research.
Management: Reassure your patient
Management of sigh syndrome consists largely of providing reassurances to your patient. You should emphasize that the condition is real, albeit benign, and that you understand the concern it causes.
Further treatment is unnecessary, aside perhaps from addressing any associated anxiety. A self-limiting (if sometimes recurrent) course can be confidently predicted, and follow-up visits can safely be left to the patient’s own discretion. Since the major correlation with sigh syndrome seems to be stress and the experience of a recent traumatic event, you should always investigate these 2 possibilities when taking the history of a patient with suspected sigh syndrome.
Acknowledgments
This work was inspired and developed by arthur Furst, MD, who died following the submission of this manuscript. Dr Furst was a distinguished and dedicated family physician, a thorough researcher, and a renowned tutor. We dedicate this article to the fond memory of a true leader in the field of rural medicine, and an exceptionally funny and amicable colleague.
Correspondence
Abby Naimer Sody, MD, Gush Katif Health Center, Neve Dekalim, Goosh Katif, Israel 79779; sodyna@clalit.org.il
- Sigh syndrome is a genuine medical diagnosis with distinct criteria, conferring significant stress for those affected. Despite outward signs of an abnormal breathing pattern, this symptomatology is unrelated to any respiratory or organic pathology.
- Ancillary testing and medication seem unnecessary; supporting reassurance appears sufficient, since the syndrome has a favorable outcome.
Objective The goal of this study was to identify the characteristics and clinical course of patients presenting with considerable stress regarding irrepressible persistent sighing, and to determine whether any association exists between this syndrome and respiratory or other organic disease during the acute or follow-up period.
Study design We conducted a case series review of patients diagnosed with a defined symptom complex and gathered relevant data.
Population Forty patients who presented to 3 clinics in Israel met our 10 criteria for sigh syndrome: recurrent sighing (at least once a minute, for varying lengths of time throughout the day); otherwise shallow respiration; patient conviction that deep breaths are obstructed; intensity of episodes provokes stress leading to consultation; no obvious trigger; episodes last a few days to several weeks; no interference with speech; sighing is absent during sleep; no correlation with physical activity or rest; and self-limited.
Outcomes measured We assessed demographic and health status information, as well as recent circumstances that could have served as triggers for the symptoms. We also performed systematic diagnoses of acute and chronic organic disease.
Results Physicians diagnosed “sigh syndrome” in 40 subjects (19 men [47.5%]), mean age 31.8 years, during the 3-year study period. All patients conformed to 10 sigh syndrome criteria. In 13 patients (32.5%), a significant traumatic event preceded onset of symptoms. Ten (25%) had previous anxiety or somatoform-related disorders. For 23 patients (57.5%), the sigh syndrome episode repeated itself after an initial episode. We found no association in any of the cases with any form of organic disease. Likewise, during the follow-up period (on average, 18 months), we did not observe the development of a specific organic disorder in any case.
Conclusions The “sigh syndrome” runs a benign course; it mainly demands the support and understanding of the treating physician to allay any patient concerns.
In our clinical practices, we have repeatedly cared for patients who came into our clinics because of a worrisome irregular breathing pattern characterized by a deep inspiration, and followed by a noisy expiration. We have referred to the set of clinical signs that these patients present with as “sigh syndrome.”
We have long suspected that sigh syndrome is an underdiagnosed and self-limited condition that is often mistaken for a serious respiratory disorder. In our experience, this syndrome runs a benign course. However, we believed that this syndrome had characteristic and consistent features, and should not be considered a diagnosis of exclusion.
Thus, we undertook a study to observe a group of subjects with these features to judge whether this subjectively alarming symptom complex is in fact harmless, and whether it is appropriate to respond to it as we had, by taking a stress-alleviating approach alone.
What is sigh syndrome?
Patients with sigh syndrome exhibit a compulsion to perform single but repeated deep inspirations, accompanied by a sensation of difficulty in inhaling a sufficient quantity of air. Each inspiration is followed by a prolonged, sometimes noisy expiration—namely, a sigh. Observing such abnormal breaths and confirming that the patient feels a concomitant inability to fill his lungs to capacity is sufficient to make the diagnosis.
This breathing compulsion is irregular in nature: It may occur once a minute or several times a minute, and this breathing pattern may continue—on and off throughout the day—for a few days to several weeks. In our experience, it provokes significant anxiety in patients, prompting them to seek medical advice. It does not occur when the patient is asleep, and it is not triggered by physical activity.
Both patient and doctor may, at first, be convinced that the problem reflects a serious illness. The 10 features of sigh syndrome (TABLE 1) constitute a proposed definition. All of our study subjects exhibited these 10 features.
TABLE 1
10 features of sigh syndrome
|
Sighing as an illness marker
Sighing has been described as one member of a group of signs exhibited by depressed or anxiety-ridden patients.1 While Perin et al2 were the first to point out the importance of distinguishing between sighing and respiratory disease, sighing per se has never been identified as a discrete illness marker.
A number of psychiatric disorders are already well known to incorporate breathing and chest symptoms along with widespread somatization. These include globus hystericus, neurocirculatory asthenia, and Tietze syndrome.3-6 As such, the acute pain of precordial catch syndrome stands out as an example of a distinguishable, clear-cut clinical state devoid of any apparent organic basis.7,8
Methods
How we recruited the patients
Data was collected from 3 family practice clinics in Israel from February 2002 to February 2005. We requested that these practices contribute data of consecutive clinical cases presenting with the 10 set symptoms of sigh syndrome (TABLE 1).
Data collected included basic demographics, the circumstances of the onset of symptoms, concurrent medical conditions, and any associated symptoms. We assessed the patients’ education level by asking questions pertaining to their years of schooling and college degrees. Patients rated their own economic status as being below, average, or above-average income.
The main outcome we examined was the clinical course of the sighing episodes during the ensuing months after their visit, in order to determine whether any patients developed a form of significant organic disease or a disorder that led to hospitalization.
Results
40 cases that cut across the socioeconomic spectrum
Forty patients were recruited for this study. Nineteen (47.5%) were male; their ages ranged from 7 to 53 (mean, 31.8; standard deviation, 13.7). Two patients (5%) were Ashkenazi Jews; 34 (85%) were of North African ethnicity (Sephardic Jews); the other 4 were of varied Asian and European ethnicity. The number of patients with North African ethnicity overrepresents that of the population in their communities. Additionally, 3 members of this group were from the same family.
There was no predilection toward any specific education level or socioeconomic status. The occupations of the subjects were diverse.
Their clinical characteristics
The clinical characteristics of the 40 patients are presented in TABLE 2. The subjects’ sighing began at various times of the day, without relationship to eating or any other activity, and disappeared during sleep. All patients reported the same feeling: that of an extra effort demanded to perform full inspiration. In many cases, adult patients were certain their complaints were a sign of cardiac or respiratory disease, and they were very concerned that there was some grave, underlying disorder.
History and examination failed to reveal evidence of any somatic findings related to breathing difficulty. Breathing rate was within normal limits in all cases.
The physicians’ initial encounters with these patients led to further examination in many cases: electrocardiography, blood oxygen saturation, and complete blood counts. However, no abnormalities were found on any of these tests. Medications, if prescribed at all during these consultations, were usually given to alleviate insomnia or anxiety. Further ancillary investigations or referrals were not ordered.
The sole notable finding on physical examination was a typical murmur (which had already been diagnosed) in a young girl with a congenital atrial septal defect. This 7-year-old developed repeated episodes of sigh syndrome just before her annual visit to the pediatric cardiologist; her mother believed that the child was frightened by the thought of possible future surgery.
TABLE 2
Clinical characteristics of the 40 patients studied—One third experienced a traumatic event
| CHARACTERISTIC | YES | NO |
|---|---|---|
| Smoker | 2 (5%) | 38 (95%) |
| History of anxiety or somatoform disorder | 10 (25%) | 30 (75%) |
| Taking prescription medication at time of diagnosis | 4 (10%) | 36 (90%) |
| Recurrence of sighing episodes during follow-up period | 24 (60%) | 16 (40%) |
| Trigger event (eg, exposure to traumatic event 1 month before presentation with syndrome) | 13 (32.5%) | 27 (67.5%) |
Traumatic events, anxiety disorders suggest stress as a cause
Thirteen patient histories disclosed a definite, recent, significant traumatic event that may have triggered the onset of sigh syndrome. Examples of 2 triggering events are the terrorist murder of several members of a neighbor’s family, and a near-miss with a mortar shell. One subject—a teenager—had recently been left alone in the dark with 2 younger siblings during a power blackout; another young woman said that the sighing episodes began when she decided to get married.
Ten patients had previously diagnosed neurotic disorders, mainly generalized anxiety; these included 2 cases of somatization disorder and 1 case of posttraumatic stress disorder. This information from the patients’ histories was documented in their medical files.
Episodes appear to be self-limited
In all patients, the episodes were self-limited. During the follow-up period, lasting an average of 18 months, none of the patients showed additional medical conditions—respiratory or otherwise—that could be linked to episodes of sigh syndrome. Recurrences of sighing episodes were reported by 24 subjects (60%) after the marker episode. One patient was diagnosed with carcinoma of the pancreas 2 years into follow-up, and later died.
Discussion
A benign, transient disorder
Aside from the solitary and unrelated death noted above, examination and follow-up in all 40 cases did not lead to an alternative diagnosis. Sigh syndrome thus seems to be an entirely benign and transient condition with no sequelae aside from possible recurrences.
Although the pathophysiology is unclear, our finding that 32.5% of patients had a recent traumatic incident strongly suggests a stress-related condition. Furthermore, 25% of the patients were already known to suffer from intermittent anxiety or somatoform disorders, although none were taking medications for these conditions. This adds support to the assumption that a mind-body interaction is underpinning the disorder. Large-scale migration, recent war or terrorist acts, or natural disaster are likely to increase the chances that the average physician will see a patient with sigh syndrome.
A tendency towards North African/Sephardic ethnicity, rather than European ethnicity—in addition to the cluster of 3 cases belonging to the same family—suggests the presentation may be a subconscious cultural, learned, or adopted expression of uneasiness.
Making your evaluation: History and physical are enough
The diagnostic evaluation of sigh syndrome—consisting of careful history-taking and a thorough physical examination—should be sufficient to differentiate it from an array of organic diseases. A physical examination is imperative to exclude other causes for this breathing abnormality.
Ancillary testing is rarely, if ever, indicated. It can perhaps be justified only if the condition is accompanied by an additional (if serendipitous) finding such as the cardiac murmur in the 7-year-old girl noted earlier. Physicians sometimes perform unnecessary investigations, being reluctant to base their diagnoses solely on their clinical expertise.9 A patient may interpret this testing as uncertainty or begin to doubt the diagnosis, thus augmenting—rather than reducing—any anxiety.10 The additional burden of the costs and possible side effects compound the futility of testing indiscriminately.11
Identifying these symptoms with the name “sigh syndrome,” and basing this diagnosis on the history and physical examination, stresses certainty and familiarity with the diagnosis.9 Not only does this reassure the patient, but it eases communication between professionals and forms a basis for research.
Management: Reassure your patient
Management of sigh syndrome consists largely of providing reassurances to your patient. You should emphasize that the condition is real, albeit benign, and that you understand the concern it causes.
Further treatment is unnecessary, aside perhaps from addressing any associated anxiety. A self-limiting (if sometimes recurrent) course can be confidently predicted, and follow-up visits can safely be left to the patient’s own discretion. Since the major correlation with sigh syndrome seems to be stress and the experience of a recent traumatic event, you should always investigate these 2 possibilities when taking the history of a patient with suspected sigh syndrome.
Acknowledgments
This work was inspired and developed by arthur Furst, MD, who died following the submission of this manuscript. Dr Furst was a distinguished and dedicated family physician, a thorough researcher, and a renowned tutor. We dedicate this article to the fond memory of a true leader in the field of rural medicine, and an exceptionally funny and amicable colleague.
Correspondence
Abby Naimer Sody, MD, Gush Katif Health Center, Neve Dekalim, Goosh Katif, Israel 79779; sodyna@clalit.org.il
1. Rakel RE. Textbook of Family Practice. 6th ed. St louis, Mo: WB Saunders; 2002.
2. Perin PV, Perin RJ, Rooklin AR. When a sigh is just a sigh…and not asthma. Ann Allergy 1993;71:478-480.
3. Wilhelm FH, Gevirtz R, Roth WT. Respiratory dys-regulation in anxiety, functional cardiac, and pain disorders. Assessment, phenomenology, and treatment. Behav Modif 2001;25:513-45.
4. Malcomson KG. Globus hystericus vel pharyngis (a reconnaissance of proximal vagal modalities). J Laryngol Otol 1968;82:219-230.
5. Ravich WJ, Wilson RS, Jones B, Donner MW. Psychogenic dysphagia and globus: reevaluation of 23 patients. Dysphagia 1989;4:35-38.
6. Eifert GHB. Cardiophobia: a paradigmatic behavioural model of heart-focused anxiety and non-anginal chest pain. Behav Res Ther 1992;30:329-345.
7. Miller AJ, Texidor TA. “Precordial catch,” a syndrome of anterior chest pain. Ann Intern Med 1959;51:461-467.
8. Sparrow MJ, Bird EL. “Precordial catch”: a benign syndrome of chest pain in young persons. NZ Med J 1978;88:325-326.
9. Balint M. The Doctor, his Patient and the Illness. 2nd ed. London: Sir Isaac Pitman & Sons, 1964.
10. Salmon P. The potentially somatizing effect of clinical consultation. CNS Spectr 2006;11:190-200.
11. Hajioff D, Lowe D. The diagnostic value of barium swallow in globus syndrome. Int J Clin Pract 2004;58:86-89.
1. Rakel RE. Textbook of Family Practice. 6th ed. St louis, Mo: WB Saunders; 2002.
2. Perin PV, Perin RJ, Rooklin AR. When a sigh is just a sigh…and not asthma. Ann Allergy 1993;71:478-480.
3. Wilhelm FH, Gevirtz R, Roth WT. Respiratory dys-regulation in anxiety, functional cardiac, and pain disorders. Assessment, phenomenology, and treatment. Behav Modif 2001;25:513-45.
4. Malcomson KG. Globus hystericus vel pharyngis (a reconnaissance of proximal vagal modalities). J Laryngol Otol 1968;82:219-230.
5. Ravich WJ, Wilson RS, Jones B, Donner MW. Psychogenic dysphagia and globus: reevaluation of 23 patients. Dysphagia 1989;4:35-38.
6. Eifert GHB. Cardiophobia: a paradigmatic behavioural model of heart-focused anxiety and non-anginal chest pain. Behav Res Ther 1992;30:329-345.
7. Miller AJ, Texidor TA. “Precordial catch,” a syndrome of anterior chest pain. Ann Intern Med 1959;51:461-467.
8. Sparrow MJ, Bird EL. “Precordial catch”: a benign syndrome of chest pain in young persons. NZ Med J 1978;88:325-326.
9. Balint M. The Doctor, his Patient and the Illness. 2nd ed. London: Sir Isaac Pitman & Sons, 1964.
10. Salmon P. The potentially somatizing effect of clinical consultation. CNS Spectr 2006;11:190-200.
11. Hajioff D, Lowe D. The diagnostic value of barium swallow in globus syndrome. Int J Clin Pract 2004;58:86-89.
Codes for phone and online counseling, team meetings
Old codes 99371–99373 that were used to report a call you made to a patient, or to consult or coordinate medical management with other health-care professionals, are deleted in 2008. In their place? A series of new codes that cover not only physician–patient contact but nonphysician–patient contact on the telephone.
Additional codes have also been added for non–face-to-face physician– provider contact regarding the care of a patient. Although these new codes may not be reimbursed by many payers, they do allow you to bill the patient for such services in many instances. They’ll also help the practice better track the care given by its providers.
Patient-initiated telephone contact
99441 Telephone evaluation and management service provided by a physician to an established patient, parent, or guardian not originating from a related E/M service provided within the previous 7 days nor leading to an E/M service or procedure within the next 24 hours or soonest available appointment; 5–10 minutes of medical discussion
99442 …11–20 minutes of medical discussion
99443 …21–30 minutes of medical discussion
98966 Telephone assessment and management service provided by a qualified nonphysician health care professional to an established patient, parent, or guardian not originating from a related assessment and management service provided within the previous seven days nor leading to an assessment and management service or procedure within the next 24 hours or soonest available appointment; 5–10 minutes of medical discussion
98967 …11–20 minutes of medical discussion
98968 …21–30 minutes of medical discussion
To use these codes, keep in mind a few rules:
- Contact must be initiated by the patient or the established patient’s guardian
- Don’t report the new codes if the patient is then seen for the problem within 24 hours after the call or at the next available urgent appointment. When that happens, the call is considered part of the pre-service work and may be counted as part of the billable E/M service
- Don’t report the new codes if the call relates to an E/M service that was reported by the provider within the prior 7 days—whether the provider did or did not request that the call be made
- Don’t report the new codes for any follow-up regarding a procedure that was performed while the patient is still in the postop period.
Conferring with the medical team
99367 Medical team conference with interdisciplinary team of health care professionals, patient and/or family not present, 30 minutes or more; participation by physician
99368 …participation by nonphysician qualified health care professional
The interactions of an interdisciplinary team are more comprehensive and complex than the conversations that might take place during a regular E/M service. So, the rules for these codes are somewhat different:
- The patient must be an established patient who has a chronic health condition or multiple health conditions that require a team approach to manage
- The participants in the conference are familiar with the patient and have seen the patient within 60 days prior to the conference call
- Only one provider from the same specialty may report these codes for each conference
- The conference must be at least 30 minutes long; the clock starts at the beginning of the review of the patient’s case and ends at the conclusion of that review. Time spent writing reports on the conference can’t be counted.
Providing your services online
99444 Online evaluation and management service provided by a physician to an established patient, guardian, or health care provider not originating from a related E/M service provided within the previous 7 days, using the Internet or similar electronic communications network
98969 Online assessment and management service provided by a qualified nonphysician health care professional to an established patient, guardian, or health care provider not originating from a related assessment and management service provided within the previous 7 days, using the Internet or similar electronic communications network
Just as telephone calls are becoming a more common method of communicating with providers, online medical services are tracing a similar pattern of use. The Internet has allowed many patients to contact their physician (or nonphysician provider) directly; with assurances of privacy offered by current Internet communications systems, information can be readily shared between patient and physician.
Criteria for using these new codes are:
- The established patient or her guardian must have initiated the online evaluation request
- The provider’s response must be timely and must include permanent electronic or hard-copy documentation of the encounter
- The online service can only be reported once during a 7-day period for the same problem, but more than one provider can report his (her) separate online communication with the patient
- As with the rules for telephone contact with a patient, do not report the new codes if the provider has billed an E/M service related to the online query within the prior 7 days or within the postop period of a procedure.
Old codes 99371–99373 that were used to report a call you made to a patient, or to consult or coordinate medical management with other health-care professionals, are deleted in 2008. In their place? A series of new codes that cover not only physician–patient contact but nonphysician–patient contact on the telephone.
Additional codes have also been added for non–face-to-face physician– provider contact regarding the care of a patient. Although these new codes may not be reimbursed by many payers, they do allow you to bill the patient for such services in many instances. They’ll also help the practice better track the care given by its providers.
Patient-initiated telephone contact
99441 Telephone evaluation and management service provided by a physician to an established patient, parent, or guardian not originating from a related E/M service provided within the previous 7 days nor leading to an E/M service or procedure within the next 24 hours or soonest available appointment; 5–10 minutes of medical discussion
99442 …11–20 minutes of medical discussion
99443 …21–30 minutes of medical discussion
98966 Telephone assessment and management service provided by a qualified nonphysician health care professional to an established patient, parent, or guardian not originating from a related assessment and management service provided within the previous seven days nor leading to an assessment and management service or procedure within the next 24 hours or soonest available appointment; 5–10 minutes of medical discussion
98967 …11–20 minutes of medical discussion
98968 …21–30 minutes of medical discussion
To use these codes, keep in mind a few rules:
- Contact must be initiated by the patient or the established patient’s guardian
- Don’t report the new codes if the patient is then seen for the problem within 24 hours after the call or at the next available urgent appointment. When that happens, the call is considered part of the pre-service work and may be counted as part of the billable E/M service
- Don’t report the new codes if the call relates to an E/M service that was reported by the provider within the prior 7 days—whether the provider did or did not request that the call be made
- Don’t report the new codes for any follow-up regarding a procedure that was performed while the patient is still in the postop period.
Conferring with the medical team
99367 Medical team conference with interdisciplinary team of health care professionals, patient and/or family not present, 30 minutes or more; participation by physician
99368 …participation by nonphysician qualified health care professional
The interactions of an interdisciplinary team are more comprehensive and complex than the conversations that might take place during a regular E/M service. So, the rules for these codes are somewhat different:
- The patient must be an established patient who has a chronic health condition or multiple health conditions that require a team approach to manage
- The participants in the conference are familiar with the patient and have seen the patient within 60 days prior to the conference call
- Only one provider from the same specialty may report these codes for each conference
- The conference must be at least 30 minutes long; the clock starts at the beginning of the review of the patient’s case and ends at the conclusion of that review. Time spent writing reports on the conference can’t be counted.
Providing your services online
99444 Online evaluation and management service provided by a physician to an established patient, guardian, or health care provider not originating from a related E/M service provided within the previous 7 days, using the Internet or similar electronic communications network
98969 Online assessment and management service provided by a qualified nonphysician health care professional to an established patient, guardian, or health care provider not originating from a related assessment and management service provided within the previous 7 days, using the Internet or similar electronic communications network
Just as telephone calls are becoming a more common method of communicating with providers, online medical services are tracing a similar pattern of use. The Internet has allowed many patients to contact their physician (or nonphysician provider) directly; with assurances of privacy offered by current Internet communications systems, information can be readily shared between patient and physician.
Criteria for using these new codes are:
- The established patient or her guardian must have initiated the online evaluation request
- The provider’s response must be timely and must include permanent electronic or hard-copy documentation of the encounter
- The online service can only be reported once during a 7-day period for the same problem, but more than one provider can report his (her) separate online communication with the patient
- As with the rules for telephone contact with a patient, do not report the new codes if the provider has billed an E/M service related to the online query within the prior 7 days or within the postop period of a procedure.
Old codes 99371–99373 that were used to report a call you made to a patient, or to consult or coordinate medical management with other health-care professionals, are deleted in 2008. In their place? A series of new codes that cover not only physician–patient contact but nonphysician–patient contact on the telephone.
Additional codes have also been added for non–face-to-face physician– provider contact regarding the care of a patient. Although these new codes may not be reimbursed by many payers, they do allow you to bill the patient for such services in many instances. They’ll also help the practice better track the care given by its providers.
Patient-initiated telephone contact
99441 Telephone evaluation and management service provided by a physician to an established patient, parent, or guardian not originating from a related E/M service provided within the previous 7 days nor leading to an E/M service or procedure within the next 24 hours or soonest available appointment; 5–10 minutes of medical discussion
99442 …11–20 minutes of medical discussion
99443 …21–30 minutes of medical discussion
98966 Telephone assessment and management service provided by a qualified nonphysician health care professional to an established patient, parent, or guardian not originating from a related assessment and management service provided within the previous seven days nor leading to an assessment and management service or procedure within the next 24 hours or soonest available appointment; 5–10 minutes of medical discussion
98967 …11–20 minutes of medical discussion
98968 …21–30 minutes of medical discussion
To use these codes, keep in mind a few rules:
- Contact must be initiated by the patient or the established patient’s guardian
- Don’t report the new codes if the patient is then seen for the problem within 24 hours after the call or at the next available urgent appointment. When that happens, the call is considered part of the pre-service work and may be counted as part of the billable E/M service
- Don’t report the new codes if the call relates to an E/M service that was reported by the provider within the prior 7 days—whether the provider did or did not request that the call be made
- Don’t report the new codes for any follow-up regarding a procedure that was performed while the patient is still in the postop period.
Conferring with the medical team
99367 Medical team conference with interdisciplinary team of health care professionals, patient and/or family not present, 30 minutes or more; participation by physician
99368 …participation by nonphysician qualified health care professional
The interactions of an interdisciplinary team are more comprehensive and complex than the conversations that might take place during a regular E/M service. So, the rules for these codes are somewhat different:
- The patient must be an established patient who has a chronic health condition or multiple health conditions that require a team approach to manage
- The participants in the conference are familiar with the patient and have seen the patient within 60 days prior to the conference call
- Only one provider from the same specialty may report these codes for each conference
- The conference must be at least 30 minutes long; the clock starts at the beginning of the review of the patient’s case and ends at the conclusion of that review. Time spent writing reports on the conference can’t be counted.
Providing your services online
99444 Online evaluation and management service provided by a physician to an established patient, guardian, or health care provider not originating from a related E/M service provided within the previous 7 days, using the Internet or similar electronic communications network
98969 Online assessment and management service provided by a qualified nonphysician health care professional to an established patient, guardian, or health care provider not originating from a related assessment and management service provided within the previous 7 days, using the Internet or similar electronic communications network
Just as telephone calls are becoming a more common method of communicating with providers, online medical services are tracing a similar pattern of use. The Internet has allowed many patients to contact their physician (or nonphysician provider) directly; with assurances of privacy offered by current Internet communications systems, information can be readily shared between patient and physician.
Criteria for using these new codes are:
- The established patient or her guardian must have initiated the online evaluation request
- The provider’s response must be timely and must include permanent electronic or hard-copy documentation of the encounter
- The online service can only be reported once during a 7-day period for the same problem, but more than one provider can report his (her) separate online communication with the patient
- As with the rules for telephone contact with a patient, do not report the new codes if the provider has billed an E/M service related to the online query within the prior 7 days or within the postop period of a procedure.
When not to use beta-blockers in seniors with hypertension
Beta-blockers should not be used to treat hypertension in patients older than age 60 unless they have another compelling indication to use these agents, such as heart failure or ischemic heart disease.1,2
Strength of recommendation
A: Based on a well-done meta-analyses
Khan N, Mcalister FA. Re-examining the efficacy of beta-blockers for the treatment of hypertension: a meta-analysis. CMAJ 2006; 174:1737– 1742.1
Wiysonge CS, Bradley H, Mayosi BM, et al. Beta-blockers for hypertension. Cochrane Database Syst Rev 2007; (1):CD002003.2
Illustrative case
A 70-year-old man with newly diagnosed hypertension comes to your office. You don’t want to prescribe a diuretic due to his history of gout. He has no history of coronary artery disease or heart failure.
What is the best antihypertensive agent for him?
Background: Guidelines do not reflect new evidence
Guidelines for the use of beta-blockers in the elderly do not reflect current evidence.
JNC recommendations
The 2003 JNC 7 Report recommended the same antihypertensive medications for adults of all ages.3 (JNC 7 is the most recent report from the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure.)
JNC 7 recommends thiazide diuretics for first-line treatment of hypertension, and recommends other drugs—including beta-blockers, calcium-channel blockers, angiotensin-converting enzyme (ACE) inhibitors, and angiotensin receptor blockers (ARBs)—for first-line therapy if a thiazide is contraindicated, or in combination with thiazides for higher initial blood pressure.
Compelling indications. Beta-blockers are recommended in the JNC 7 Report as first-line therapy in patients with “compelling indications” such as ischemic heart disease and heart failure.
Clinical context: Seniors taking beta-blockers to their detriment?
Many elderly patients are on beta-blockers, perhaps to their detriment. Treatment choices for hypertension can have an enormous impact on outcomes among older patients:
Two thirds of US adults 60 years of age and older have hypertension, mostly isolated systolic hypertension.4,5
Multiple studies, including the Systolic Hypertension in the Elderly Program and the Systolic Hypertension in Europe, have shown that lowering blood pressure with pharmacologic interventions in older patients can reduce the risk of cardiovascular events and possibly dementia.6
Beta-blockers have been a mainstay of hypertension treatment for many decades and we suspect continue to be widely used as first-line therapy in patients for whom the evidence now indicates they are inferior.
Heart failure and angina are indications for beta-blockers
New evidence does not alter the 2003 JNC 7 recommendations to use beta-blockers as first-line therapy in patients with “compelling indications” such as ischemic heart disease and heart failure.
Study summaries
Two well-done reviews of beta-blocker trials show that they are inferior for first-line hypertension treatment in the elderly who do not have heart failure or angina.
2007 Cochrane review
The 2007 Cochrane review2 analyzed randomized trials that compared beta-blockers for hypertension in adults 18 years of age and older to each of the other major classes of antihypertensives.
Conclusion. This meta-analysis showed a “relatively weak effect of beta-blockers to reduce stroke, and the absence of effect on coronary heart disease when compared with placebo or no treatment” and a “trend toward worse outcomes in comparison with calcium channel blockers, renin-angiotensin system inhibitors, and thiazide diuretics.”
This meta-analysis included all adults and did not make any conclusions based on age.
2006 CMAJ meta-analysis
The Kahn and McAlister meta-analysis1 pooled data from 21 randomized hyper-tension trials (including 6 placebo-controlled trials) that evaluated the efficacy of beta-blockers as first-line therapy for hypertension in preventing major cardiovascular outcomes (death, nonfatal MI, or nonfatal stroke).
The results were analyzed by age group: trials enrolling patients with a mean age of 60 years or older at baseline vs trials enrolling patients with a mean age of under 60 years.
Conclusion. They concluded that in trials comparing other antihypertensive medications with beta-blockers, all agents showed similar efficacy in younger patients, while in older patients, beta-blockers were associated with a higher risk of both composite events and strokes ( TABLE ).
TABLE
Adverse outcomes more likely in seniors taking a beta-blocker vs other antihypertensives1
| ADVERSE OUTCOME | PATIENTS UNDER AGE 60 | PATIENTS AGE 60 AND OVER |
|---|---|---|
| ADVERSE OUTCOMES LESS LIKELY WITH A BETA-BLOCKER | ADVERSE OUTCOMES MORE LIKELY WITH A BETA-BLOCKER | |
| Composite outcomes (death, stroke, or MI) | RR=0.97 (95% CI, 0.88–1.07) | RR=1.06 (95% CI, 1.01–1.1) |
| Stroke | RR=0.99 (95% CI, 0.67–1.44) | RR=1.18 (95% CI, 1.07–1.3) |
| RR, relative risk of adverse outcomes, in randomized clinical trials of hypertensive patients treated with beta-blockers, compared with other antihypertensive drugs. | ||
What’s new?: The age distinction
These 2 meta-analyses1,2 help overturn a long-held belief about the value of beta-blockers for the treatment of hypertension. Beta-blockers may not be a good first-line choice for any hypertensive patient—and the evidence clearly shows they are not a good first-line choice for patients over 60 years old.
Two earlier systematic reviews did raise the concern about using beta-blockers as first-line treatment for hypertension (even when thiazides are not contraindicated).
The first systematic review to raise this concern was a 1998 study of 10 hypertension trials in more than 16,000 patients, ages 60 and older. This review showed that diuretics were superior to beta-blockers in reducing cardiovascular and all-cause mortality—which supports the JNC 7 recommendation to choose a thiazide diuretic as the first-line drug of choice.7
The second study, a meta-analysis published in 2005, also concluded that beta-blockers should no longer be considered first-line therapy for hypertension, due to a 16% increase in the relative risk of stroke compared with other agents. This meta-analysis, however, did not report outcomes by patient age.8
Beta-blockers are not 1st-line, even if thiazides are contraindicated
What is new about the Kahn and McAlister evidence is that beta-blockers should not be the first-line drug of choice even when thiazide diuretics are contraindicated. Their study included a larger number of trials (21 trials vs 13 in the 2005 meta-analysis), which allowed the investigators to examine outcomes in patients younger than 60 and in those 60 years and older.
Caveats: Continue beta-blockers for the right reasons
Patients over 60 with ischemic heart disease or heart failure should still be prescribed beta-blockers for heart failure and angina. Also, in older patients with hypertension who need multiple agents to control their blood pressure, a beta-blocker could be added as a third or fourth agent in addition to a diuretic, ACE inhibitor, ARB, or calcium-channel blocker. Metoprolol is a good choice, as it is inexpensive and proven to reduce mortality in patients with a history of MI or heart failure.
Atenolol may underperform
In a meta-analysis of 31 trials, Freemantle9 found that after MI, acebutolol, metoprolol, propranolol, and timolol significantly reduced mortality, while there was no mortality reduction with atenolol. Similarly, in heart failure, only bisoprolol, metoprolol, and carvedilol have evidence to support a reduction in mortality.10
Although atenolol is one of the most commonly prescribed beta-blockers due to its low cost and once-daily dosing, it may be the least effective. In a systematic review of 9 hypertension studies, Carlberg11 showed that atenolol was no more effective than placebo at reducing MI, cardiovascular mortality, or all-cause mortality, and that patients on atenolol had significantly higher mortality than those taking other antihypertensives. Khan and McAlister do not differentiate between atenolol and other beta-blockers in their meta-analysis.1
Challenges to implementation: Letting go
The evidence supporting this change in practice has been accumulating over time. The change itself represents a significant reversal of long-standing belief in the value of beta-blockers as an antihypertensive agent. For each individual patient, the risk is not dramatic even though the cumulative “harm” from using a beta-blocker compared to other options is potentially staggering because so many people over 60 have hypertension.
We suspect that the main challenge will be changing the beliefs of both physicians and patients. Once doctors are convinced that beta-blockers are not indicated for uncomplicated hypertension in patients over 60, changing medications in the millions of older patients who have been taking a beta-blocker for some time and have become comfortable with it will take tact and excellent communication skills.
Providing patient information may help. Sources for patients are available free or at low cost at www.nhlbi.nih.gov/health/public/heart/index.htm#hbp. These materials explain that diuretics are inexpensive and are the preferred drugs for initial treatment of hypertension.
In patients over 60 who can’t tolerate a thiazide, the least expensive option is an ACE inhibitor. For example, in the Target and Walmart discount generic programs, benazepril, captopril, enalapril, and lisinopril are all available for $4 per month.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
1. Khan N, McAlister FA. Re-examining the efficacy of beta-blockers for the treatment of hypertension: a meta-analysis. CMAJ 2006;174:1737-1742.
2. Wiysonge CS, Bradley H, Mayosi BM, et al. Beta-blockers for hypertension. Cochrane Database Syst Rev 2007;(1):CD002003.-
3. The Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. US Department of Health and Human Services/National Heart, Lung and Blood Institute; 2003. Available at: www.nhlbi.nih.gov/guidelines/hypertension. Accessed on Dec 11, 2007.
4. Ostchega Y, Dillon CF, Hughes JP, Carroll M, Yoon S. Trends in hypertension prevalence, awareness, treatment, and control in older US adults: data from the National Health and Nutrition Examination Survey 1988 to 2004. J Am Geriatr Soc 2007;55:1056-1065.
5. Chobanian A. Isolated systolic hypertension in the elderly. N Engl J Med 2007;357:789-796.
6. Waeber B. Trials in isolated systolic hypertension: an update. Curr Hypertens Rep 2003;5:329-336.
7. Messerli FH, Grossman E, Goldbourt U. Are beta-blockers efficacious as first-line therapy for hypertension in the elderly? a systematic review. JAMA 1998;279:1903-1907.
8. Lindholm LH, Carlberg B, Samuelsson O. Should beta blockers remain first choice in the treatment of primary hypertension? A meta-analysis. Lancet 2005;366:1545-1553.
9. Freemantle N, Cleland J, Young P, Mason J, Harrison J. Beta blockade after myocardial infarction: systematic review and meta regression analysis. BMJ 1999;318:1730-1737.
10. Ong HT. Beta blockers in hypertension and cardiovascular disease. BMJ 2007;334:946-949.
11. Carlberg B, Samuelsson O, Lindholm LH. Atenolol in hypertension: is it a wise choice? Lancet 2004;364:1684-1689.
Beta-blockers should not be used to treat hypertension in patients older than age 60 unless they have another compelling indication to use these agents, such as heart failure or ischemic heart disease.1,2
Strength of recommendation
A: Based on a well-done meta-analyses
Khan N, Mcalister FA. Re-examining the efficacy of beta-blockers for the treatment of hypertension: a meta-analysis. CMAJ 2006; 174:1737– 1742.1
Wiysonge CS, Bradley H, Mayosi BM, et al. Beta-blockers for hypertension. Cochrane Database Syst Rev 2007; (1):CD002003.2
Illustrative case
A 70-year-old man with newly diagnosed hypertension comes to your office. You don’t want to prescribe a diuretic due to his history of gout. He has no history of coronary artery disease or heart failure.
What is the best antihypertensive agent for him?
Background: Guidelines do not reflect new evidence
Guidelines for the use of beta-blockers in the elderly do not reflect current evidence.
JNC recommendations
The 2003 JNC 7 Report recommended the same antihypertensive medications for adults of all ages.3 (JNC 7 is the most recent report from the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure.)
JNC 7 recommends thiazide diuretics for first-line treatment of hypertension, and recommends other drugs—including beta-blockers, calcium-channel blockers, angiotensin-converting enzyme (ACE) inhibitors, and angiotensin receptor blockers (ARBs)—for first-line therapy if a thiazide is contraindicated, or in combination with thiazides for higher initial blood pressure.
Compelling indications. Beta-blockers are recommended in the JNC 7 Report as first-line therapy in patients with “compelling indications” such as ischemic heart disease and heart failure.
Clinical context: Seniors taking beta-blockers to their detriment?
Many elderly patients are on beta-blockers, perhaps to their detriment. Treatment choices for hypertension can have an enormous impact on outcomes among older patients:
Two thirds of US adults 60 years of age and older have hypertension, mostly isolated systolic hypertension.4,5
Multiple studies, including the Systolic Hypertension in the Elderly Program and the Systolic Hypertension in Europe, have shown that lowering blood pressure with pharmacologic interventions in older patients can reduce the risk of cardiovascular events and possibly dementia.6
Beta-blockers have been a mainstay of hypertension treatment for many decades and we suspect continue to be widely used as first-line therapy in patients for whom the evidence now indicates they are inferior.
Heart failure and angina are indications for beta-blockers
New evidence does not alter the 2003 JNC 7 recommendations to use beta-blockers as first-line therapy in patients with “compelling indications” such as ischemic heart disease and heart failure.
Study summaries
Two well-done reviews of beta-blocker trials show that they are inferior for first-line hypertension treatment in the elderly who do not have heart failure or angina.
2007 Cochrane review
The 2007 Cochrane review2 analyzed randomized trials that compared beta-blockers for hypertension in adults 18 years of age and older to each of the other major classes of antihypertensives.
Conclusion. This meta-analysis showed a “relatively weak effect of beta-blockers to reduce stroke, and the absence of effect on coronary heart disease when compared with placebo or no treatment” and a “trend toward worse outcomes in comparison with calcium channel blockers, renin-angiotensin system inhibitors, and thiazide diuretics.”
This meta-analysis included all adults and did not make any conclusions based on age.
2006 CMAJ meta-analysis
The Kahn and McAlister meta-analysis1 pooled data from 21 randomized hyper-tension trials (including 6 placebo-controlled trials) that evaluated the efficacy of beta-blockers as first-line therapy for hypertension in preventing major cardiovascular outcomes (death, nonfatal MI, or nonfatal stroke).
The results were analyzed by age group: trials enrolling patients with a mean age of 60 years or older at baseline vs trials enrolling patients with a mean age of under 60 years.
Conclusion. They concluded that in trials comparing other antihypertensive medications with beta-blockers, all agents showed similar efficacy in younger patients, while in older patients, beta-blockers were associated with a higher risk of both composite events and strokes ( TABLE ).
TABLE
Adverse outcomes more likely in seniors taking a beta-blocker vs other antihypertensives1
| ADVERSE OUTCOME | PATIENTS UNDER AGE 60 | PATIENTS AGE 60 AND OVER |
|---|---|---|
| ADVERSE OUTCOMES LESS LIKELY WITH A BETA-BLOCKER | ADVERSE OUTCOMES MORE LIKELY WITH A BETA-BLOCKER | |
| Composite outcomes (death, stroke, or MI) | RR=0.97 (95% CI, 0.88–1.07) | RR=1.06 (95% CI, 1.01–1.1) |
| Stroke | RR=0.99 (95% CI, 0.67–1.44) | RR=1.18 (95% CI, 1.07–1.3) |
| RR, relative risk of adverse outcomes, in randomized clinical trials of hypertensive patients treated with beta-blockers, compared with other antihypertensive drugs. | ||
What’s new?: The age distinction
These 2 meta-analyses1,2 help overturn a long-held belief about the value of beta-blockers for the treatment of hypertension. Beta-blockers may not be a good first-line choice for any hypertensive patient—and the evidence clearly shows they are not a good first-line choice for patients over 60 years old.
Two earlier systematic reviews did raise the concern about using beta-blockers as first-line treatment for hypertension (even when thiazides are not contraindicated).
The first systematic review to raise this concern was a 1998 study of 10 hypertension trials in more than 16,000 patients, ages 60 and older. This review showed that diuretics were superior to beta-blockers in reducing cardiovascular and all-cause mortality—which supports the JNC 7 recommendation to choose a thiazide diuretic as the first-line drug of choice.7
The second study, a meta-analysis published in 2005, also concluded that beta-blockers should no longer be considered first-line therapy for hypertension, due to a 16% increase in the relative risk of stroke compared with other agents. This meta-analysis, however, did not report outcomes by patient age.8
Beta-blockers are not 1st-line, even if thiazides are contraindicated
What is new about the Kahn and McAlister evidence is that beta-blockers should not be the first-line drug of choice even when thiazide diuretics are contraindicated. Their study included a larger number of trials (21 trials vs 13 in the 2005 meta-analysis), which allowed the investigators to examine outcomes in patients younger than 60 and in those 60 years and older.
Caveats: Continue beta-blockers for the right reasons
Patients over 60 with ischemic heart disease or heart failure should still be prescribed beta-blockers for heart failure and angina. Also, in older patients with hypertension who need multiple agents to control their blood pressure, a beta-blocker could be added as a third or fourth agent in addition to a diuretic, ACE inhibitor, ARB, or calcium-channel blocker. Metoprolol is a good choice, as it is inexpensive and proven to reduce mortality in patients with a history of MI or heart failure.
Atenolol may underperform
In a meta-analysis of 31 trials, Freemantle9 found that after MI, acebutolol, metoprolol, propranolol, and timolol significantly reduced mortality, while there was no mortality reduction with atenolol. Similarly, in heart failure, only bisoprolol, metoprolol, and carvedilol have evidence to support a reduction in mortality.10
Although atenolol is one of the most commonly prescribed beta-blockers due to its low cost and once-daily dosing, it may be the least effective. In a systematic review of 9 hypertension studies, Carlberg11 showed that atenolol was no more effective than placebo at reducing MI, cardiovascular mortality, or all-cause mortality, and that patients on atenolol had significantly higher mortality than those taking other antihypertensives. Khan and McAlister do not differentiate between atenolol and other beta-blockers in their meta-analysis.1
Challenges to implementation: Letting go
The evidence supporting this change in practice has been accumulating over time. The change itself represents a significant reversal of long-standing belief in the value of beta-blockers as an antihypertensive agent. For each individual patient, the risk is not dramatic even though the cumulative “harm” from using a beta-blocker compared to other options is potentially staggering because so many people over 60 have hypertension.
We suspect that the main challenge will be changing the beliefs of both physicians and patients. Once doctors are convinced that beta-blockers are not indicated for uncomplicated hypertension in patients over 60, changing medications in the millions of older patients who have been taking a beta-blocker for some time and have become comfortable with it will take tact and excellent communication skills.
Providing patient information may help. Sources for patients are available free or at low cost at www.nhlbi.nih.gov/health/public/heart/index.htm#hbp. These materials explain that diuretics are inexpensive and are the preferred drugs for initial treatment of hypertension.
In patients over 60 who can’t tolerate a thiazide, the least expensive option is an ACE inhibitor. For example, in the Target and Walmart discount generic programs, benazepril, captopril, enalapril, and lisinopril are all available for $4 per month.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
Beta-blockers should not be used to treat hypertension in patients older than age 60 unless they have another compelling indication to use these agents, such as heart failure or ischemic heart disease.1,2
Strength of recommendation
A: Based on a well-done meta-analyses
Khan N, Mcalister FA. Re-examining the efficacy of beta-blockers for the treatment of hypertension: a meta-analysis. CMAJ 2006; 174:1737– 1742.1
Wiysonge CS, Bradley H, Mayosi BM, et al. Beta-blockers for hypertension. Cochrane Database Syst Rev 2007; (1):CD002003.2
Illustrative case
A 70-year-old man with newly diagnosed hypertension comes to your office. You don’t want to prescribe a diuretic due to his history of gout. He has no history of coronary artery disease or heart failure.
What is the best antihypertensive agent for him?
Background: Guidelines do not reflect new evidence
Guidelines for the use of beta-blockers in the elderly do not reflect current evidence.
JNC recommendations
The 2003 JNC 7 Report recommended the same antihypertensive medications for adults of all ages.3 (JNC 7 is the most recent report from the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure.)
JNC 7 recommends thiazide diuretics for first-line treatment of hypertension, and recommends other drugs—including beta-blockers, calcium-channel blockers, angiotensin-converting enzyme (ACE) inhibitors, and angiotensin receptor blockers (ARBs)—for first-line therapy if a thiazide is contraindicated, or in combination with thiazides for higher initial blood pressure.
Compelling indications. Beta-blockers are recommended in the JNC 7 Report as first-line therapy in patients with “compelling indications” such as ischemic heart disease and heart failure.
Clinical context: Seniors taking beta-blockers to their detriment?
Many elderly patients are on beta-blockers, perhaps to their detriment. Treatment choices for hypertension can have an enormous impact on outcomes among older patients:
Two thirds of US adults 60 years of age and older have hypertension, mostly isolated systolic hypertension.4,5
Multiple studies, including the Systolic Hypertension in the Elderly Program and the Systolic Hypertension in Europe, have shown that lowering blood pressure with pharmacologic interventions in older patients can reduce the risk of cardiovascular events and possibly dementia.6
Beta-blockers have been a mainstay of hypertension treatment for many decades and we suspect continue to be widely used as first-line therapy in patients for whom the evidence now indicates they are inferior.
Heart failure and angina are indications for beta-blockers
New evidence does not alter the 2003 JNC 7 recommendations to use beta-blockers as first-line therapy in patients with “compelling indications” such as ischemic heart disease and heart failure.
Study summaries
Two well-done reviews of beta-blocker trials show that they are inferior for first-line hypertension treatment in the elderly who do not have heart failure or angina.
2007 Cochrane review
The 2007 Cochrane review2 analyzed randomized trials that compared beta-blockers for hypertension in adults 18 years of age and older to each of the other major classes of antihypertensives.
Conclusion. This meta-analysis showed a “relatively weak effect of beta-blockers to reduce stroke, and the absence of effect on coronary heart disease when compared with placebo or no treatment” and a “trend toward worse outcomes in comparison with calcium channel blockers, renin-angiotensin system inhibitors, and thiazide diuretics.”
This meta-analysis included all adults and did not make any conclusions based on age.
2006 CMAJ meta-analysis
The Kahn and McAlister meta-analysis1 pooled data from 21 randomized hyper-tension trials (including 6 placebo-controlled trials) that evaluated the efficacy of beta-blockers as first-line therapy for hypertension in preventing major cardiovascular outcomes (death, nonfatal MI, or nonfatal stroke).
The results were analyzed by age group: trials enrolling patients with a mean age of 60 years or older at baseline vs trials enrolling patients with a mean age of under 60 years.
Conclusion. They concluded that in trials comparing other antihypertensive medications with beta-blockers, all agents showed similar efficacy in younger patients, while in older patients, beta-blockers were associated with a higher risk of both composite events and strokes ( TABLE ).
TABLE
Adverse outcomes more likely in seniors taking a beta-blocker vs other antihypertensives1
| ADVERSE OUTCOME | PATIENTS UNDER AGE 60 | PATIENTS AGE 60 AND OVER |
|---|---|---|
| ADVERSE OUTCOMES LESS LIKELY WITH A BETA-BLOCKER | ADVERSE OUTCOMES MORE LIKELY WITH A BETA-BLOCKER | |
| Composite outcomes (death, stroke, or MI) | RR=0.97 (95% CI, 0.88–1.07) | RR=1.06 (95% CI, 1.01–1.1) |
| Stroke | RR=0.99 (95% CI, 0.67–1.44) | RR=1.18 (95% CI, 1.07–1.3) |
| RR, relative risk of adverse outcomes, in randomized clinical trials of hypertensive patients treated with beta-blockers, compared with other antihypertensive drugs. | ||
What’s new?: The age distinction
These 2 meta-analyses1,2 help overturn a long-held belief about the value of beta-blockers for the treatment of hypertension. Beta-blockers may not be a good first-line choice for any hypertensive patient—and the evidence clearly shows they are not a good first-line choice for patients over 60 years old.
Two earlier systematic reviews did raise the concern about using beta-blockers as first-line treatment for hypertension (even when thiazides are not contraindicated).
The first systematic review to raise this concern was a 1998 study of 10 hypertension trials in more than 16,000 patients, ages 60 and older. This review showed that diuretics were superior to beta-blockers in reducing cardiovascular and all-cause mortality—which supports the JNC 7 recommendation to choose a thiazide diuretic as the first-line drug of choice.7
The second study, a meta-analysis published in 2005, also concluded that beta-blockers should no longer be considered first-line therapy for hypertension, due to a 16% increase in the relative risk of stroke compared with other agents. This meta-analysis, however, did not report outcomes by patient age.8
Beta-blockers are not 1st-line, even if thiazides are contraindicated
What is new about the Kahn and McAlister evidence is that beta-blockers should not be the first-line drug of choice even when thiazide diuretics are contraindicated. Their study included a larger number of trials (21 trials vs 13 in the 2005 meta-analysis), which allowed the investigators to examine outcomes in patients younger than 60 and in those 60 years and older.
Caveats: Continue beta-blockers for the right reasons
Patients over 60 with ischemic heart disease or heart failure should still be prescribed beta-blockers for heart failure and angina. Also, in older patients with hypertension who need multiple agents to control their blood pressure, a beta-blocker could be added as a third or fourth agent in addition to a diuretic, ACE inhibitor, ARB, or calcium-channel blocker. Metoprolol is a good choice, as it is inexpensive and proven to reduce mortality in patients with a history of MI or heart failure.
Atenolol may underperform
In a meta-analysis of 31 trials, Freemantle9 found that after MI, acebutolol, metoprolol, propranolol, and timolol significantly reduced mortality, while there was no mortality reduction with atenolol. Similarly, in heart failure, only bisoprolol, metoprolol, and carvedilol have evidence to support a reduction in mortality.10
Although atenolol is one of the most commonly prescribed beta-blockers due to its low cost and once-daily dosing, it may be the least effective. In a systematic review of 9 hypertension studies, Carlberg11 showed that atenolol was no more effective than placebo at reducing MI, cardiovascular mortality, or all-cause mortality, and that patients on atenolol had significantly higher mortality than those taking other antihypertensives. Khan and McAlister do not differentiate between atenolol and other beta-blockers in their meta-analysis.1
Challenges to implementation: Letting go
The evidence supporting this change in practice has been accumulating over time. The change itself represents a significant reversal of long-standing belief in the value of beta-blockers as an antihypertensive agent. For each individual patient, the risk is not dramatic even though the cumulative “harm” from using a beta-blocker compared to other options is potentially staggering because so many people over 60 have hypertension.
We suspect that the main challenge will be changing the beliefs of both physicians and patients. Once doctors are convinced that beta-blockers are not indicated for uncomplicated hypertension in patients over 60, changing medications in the millions of older patients who have been taking a beta-blocker for some time and have become comfortable with it will take tact and excellent communication skills.
Providing patient information may help. Sources for patients are available free or at low cost at www.nhlbi.nih.gov/health/public/heart/index.htm#hbp. These materials explain that diuretics are inexpensive and are the preferred drugs for initial treatment of hypertension.
In patients over 60 who can’t tolerate a thiazide, the least expensive option is an ACE inhibitor. For example, in the Target and Walmart discount generic programs, benazepril, captopril, enalapril, and lisinopril are all available for $4 per month.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
1. Khan N, McAlister FA. Re-examining the efficacy of beta-blockers for the treatment of hypertension: a meta-analysis. CMAJ 2006;174:1737-1742.
2. Wiysonge CS, Bradley H, Mayosi BM, et al. Beta-blockers for hypertension. Cochrane Database Syst Rev 2007;(1):CD002003.-
3. The Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. US Department of Health and Human Services/National Heart, Lung and Blood Institute; 2003. Available at: www.nhlbi.nih.gov/guidelines/hypertension. Accessed on Dec 11, 2007.
4. Ostchega Y, Dillon CF, Hughes JP, Carroll M, Yoon S. Trends in hypertension prevalence, awareness, treatment, and control in older US adults: data from the National Health and Nutrition Examination Survey 1988 to 2004. J Am Geriatr Soc 2007;55:1056-1065.
5. Chobanian A. Isolated systolic hypertension in the elderly. N Engl J Med 2007;357:789-796.
6. Waeber B. Trials in isolated systolic hypertension: an update. Curr Hypertens Rep 2003;5:329-336.
7. Messerli FH, Grossman E, Goldbourt U. Are beta-blockers efficacious as first-line therapy for hypertension in the elderly? a systematic review. JAMA 1998;279:1903-1907.
8. Lindholm LH, Carlberg B, Samuelsson O. Should beta blockers remain first choice in the treatment of primary hypertension? A meta-analysis. Lancet 2005;366:1545-1553.
9. Freemantle N, Cleland J, Young P, Mason J, Harrison J. Beta blockade after myocardial infarction: systematic review and meta regression analysis. BMJ 1999;318:1730-1737.
10. Ong HT. Beta blockers in hypertension and cardiovascular disease. BMJ 2007;334:946-949.
11. Carlberg B, Samuelsson O, Lindholm LH. Atenolol in hypertension: is it a wise choice? Lancet 2004;364:1684-1689.
1. Khan N, McAlister FA. Re-examining the efficacy of beta-blockers for the treatment of hypertension: a meta-analysis. CMAJ 2006;174:1737-1742.
2. Wiysonge CS, Bradley H, Mayosi BM, et al. Beta-blockers for hypertension. Cochrane Database Syst Rev 2007;(1):CD002003.-
3. The Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. US Department of Health and Human Services/National Heart, Lung and Blood Institute; 2003. Available at: www.nhlbi.nih.gov/guidelines/hypertension. Accessed on Dec 11, 2007.
4. Ostchega Y, Dillon CF, Hughes JP, Carroll M, Yoon S. Trends in hypertension prevalence, awareness, treatment, and control in older US adults: data from the National Health and Nutrition Examination Survey 1988 to 2004. J Am Geriatr Soc 2007;55:1056-1065.
5. Chobanian A. Isolated systolic hypertension in the elderly. N Engl J Med 2007;357:789-796.
6. Waeber B. Trials in isolated systolic hypertension: an update. Curr Hypertens Rep 2003;5:329-336.
7. Messerli FH, Grossman E, Goldbourt U. Are beta-blockers efficacious as first-line therapy for hypertension in the elderly? a systematic review. JAMA 1998;279:1903-1907.
8. Lindholm LH, Carlberg B, Samuelsson O. Should beta blockers remain first choice in the treatment of primary hypertension? A meta-analysis. Lancet 2005;366:1545-1553.
9. Freemantle N, Cleland J, Young P, Mason J, Harrison J. Beta blockade after myocardial infarction: systematic review and meta regression analysis. BMJ 1999;318:1730-1737.
10. Ong HT. Beta blockers in hypertension and cardiovascular disease. BMJ 2007;334:946-949.
11. Carlberg B, Samuelsson O, Lindholm LH. Atenolol in hypertension: is it a wise choice? Lancet 2004;364:1684-1689.
Copyright © 2008 The Family Physicians Inquiries Network.
All rights reserved.