User login
Succeed in Business
You may have an idea for a business you’d like to start, perhaps attracted by the prospect of controlling your time and work, chasing extra income, or fulfilling the dream of having an alternate career. Should you try turning your dream into reality—and if so, how?
Philippa Kennealy, MD, MPH, has guided hospitalists and other physicians along this path. She heads The Entrepreneurial MD, a Los Angeles-based coaching service for physicians who want to become more entrepreneurial with their practices or start a side business. She has a unique perspective on how physicians can add a satisfying second career to their practice of medicine. “I myself am a physician-entrepreneur,” says Dr. Kennealy.
Why Increase Workloads?
What makes busy hospitalists seek a side business? Why overload your schedule with the extra hours and responsibilities of running a business?
“It’s an opportunity to do something that feels creative, that gives you control,” explains Dr. Kennealy. “I feel that physicians don’t get to use creativity, and they don’t have much control. Their daily actions and decisions are quite regulated. Owning their own time is attractive to physicians. Hospitalists in particular are at it all day in the hospital.”
Is it really possible to continue to work as a hospitalist while shaping a second business? Yes—and others have done it.
“A lot of physicians dream of [entrepreneurship] but feel trapped by their existing time commitments,” says Dr. Kennealy. “But there are some who take the necessary steps, who carve out the time to do it. Many of them hook up with someone to form a partnership—often this is with a non-physician.”
Types of Endeavors
Some physicians are interested in a start-up business that goes hand in hand with their patient care; others may go in a completely different direction.
“There’s an enormous array of [physician-owned businesses] out there,” says Dr. Kennealy. “Many of my clients go into consulting, mostly within healthcare. Some have developed a software application that supports some aspect of healthcare.” Other physicians open health and wellness centers. One of Dr. Kennealy’s clients has developed a sculpting business and is ready to open her own gallery.
Lucia Ferreras-Cox, MD, works as an independent contractor in urgent care and hospital medicine while she runs her company, Ejerce Medecina USA, in Gilbert, Ariz. Ejerce offers Web-based training for Spanish-speaking physicians in other countries to help them pass the U.S. medical board review, then serves as a recruiting firm for those physicians once they get their U.S. licenses.
“I went back to business school for three months to refresh my skills,” says Dr. Ferreras-Cox, who previously had a pediatric practice. “I had to relearn—to learn that I was not a not-for-profit anymore.”
Marica Pook, MD, is a full-time hospitalist in Superior, Colo., and president of ExtraMD PC, a company that provides short-term physician staffing. Her start-up was quite simple. “I’ve been a hospitalist for seven years now, and of course part of my job is to call primary care physicians about patients,” Dr. Pook says. “I started thinking about what it’s like for those physicians and how they can get some help when they’re at their busiest.”
She decided to provide that help. In 2004 she used her contacts to start a kind of mini locum tenens job, working for different physician groups and hospitals. “Nine months into it, I started bringing in other physicians,” she says. Today, the business is thriving, with a growing number of local physicians involved, as well as some much-needed staff.
“I have an excellent bookkeeper, who does all the financials, invoicing, and budgeting—almost like a controller,” says Dr. Pook. “And I just hired a virtual assistant last week. I’ve found that it works best when I farm out the calling and scheduling and I just focus on the marketing. And I include talking to the physicians in that.”
Get Started
So how do you begin your transformation from hospitalist to hospitalist-entrepreneur?
“The basic steps begin with identifying whether this is an escapist fantasy or a deep, abiding interest,” stresses Dr. Kennealy. “It will take a deep interest to get you through the difficult times—it’s a real commitment.”
Once you determine you’re willing to invest time and expense in your own business, Dr. Kennealy advises you to assess your skills and acquire any new ones you’ll need. One way is to meet businesspeople, learn how they think, and understand the language of business. You can also study business and marketing books and journals or take business courses.
“I think physicians don’t know how to run a business,” says Dr. Pook. “We’re not trained to do this. What really helped me was a business coach. I’d advise others to either get a coach or get hooked up with someone who knows a lot about business.”
Before you make too deep a commitment, consider an important component. “You need some sense of the marketplace,” says Dr. Kennealy. Who will buy your product or service? Is there enough interest to support your efforts? What is the competition like in your area?
The next step, she says, is to develop a business plan. “There are free resources available at SCORE.org [the Web site of SCORE, Counselors to America’s Small Business],” she says. “As you start on your plan, you may see that you require further analysis. You need to close those knowledge gaps before you start the business.”
And finally, you have to have marketing savvy to make it work. “Wrap it all up in a sound marketing plan,” concludes Dr. Kennealy. “How will you reach your target audience, and how will you do it efficiently? You must learn the art of marketing, and most physicians don’t have a clue. You have to shift your thinking from a physician whose patients basically come flocking to someone who has to attract and keep customers.” TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
You may have an idea for a business you’d like to start, perhaps attracted by the prospect of controlling your time and work, chasing extra income, or fulfilling the dream of having an alternate career. Should you try turning your dream into reality—and if so, how?
Philippa Kennealy, MD, MPH, has guided hospitalists and other physicians along this path. She heads The Entrepreneurial MD, a Los Angeles-based coaching service for physicians who want to become more entrepreneurial with their practices or start a side business. She has a unique perspective on how physicians can add a satisfying second career to their practice of medicine. “I myself am a physician-entrepreneur,” says Dr. Kennealy.
Why Increase Workloads?
What makes busy hospitalists seek a side business? Why overload your schedule with the extra hours and responsibilities of running a business?
“It’s an opportunity to do something that feels creative, that gives you control,” explains Dr. Kennealy. “I feel that physicians don’t get to use creativity, and they don’t have much control. Their daily actions and decisions are quite regulated. Owning their own time is attractive to physicians. Hospitalists in particular are at it all day in the hospital.”
Is it really possible to continue to work as a hospitalist while shaping a second business? Yes—and others have done it.
“A lot of physicians dream of [entrepreneurship] but feel trapped by their existing time commitments,” says Dr. Kennealy. “But there are some who take the necessary steps, who carve out the time to do it. Many of them hook up with someone to form a partnership—often this is with a non-physician.”
Types of Endeavors
Some physicians are interested in a start-up business that goes hand in hand with their patient care; others may go in a completely different direction.
“There’s an enormous array of [physician-owned businesses] out there,” says Dr. Kennealy. “Many of my clients go into consulting, mostly within healthcare. Some have developed a software application that supports some aspect of healthcare.” Other physicians open health and wellness centers. One of Dr. Kennealy’s clients has developed a sculpting business and is ready to open her own gallery.
Lucia Ferreras-Cox, MD, works as an independent contractor in urgent care and hospital medicine while she runs her company, Ejerce Medecina USA, in Gilbert, Ariz. Ejerce offers Web-based training for Spanish-speaking physicians in other countries to help them pass the U.S. medical board review, then serves as a recruiting firm for those physicians once they get their U.S. licenses.
“I went back to business school for three months to refresh my skills,” says Dr. Ferreras-Cox, who previously had a pediatric practice. “I had to relearn—to learn that I was not a not-for-profit anymore.”
Marica Pook, MD, is a full-time hospitalist in Superior, Colo., and president of ExtraMD PC, a company that provides short-term physician staffing. Her start-up was quite simple. “I’ve been a hospitalist for seven years now, and of course part of my job is to call primary care physicians about patients,” Dr. Pook says. “I started thinking about what it’s like for those physicians and how they can get some help when they’re at their busiest.”
She decided to provide that help. In 2004 she used her contacts to start a kind of mini locum tenens job, working for different physician groups and hospitals. “Nine months into it, I started bringing in other physicians,” she says. Today, the business is thriving, with a growing number of local physicians involved, as well as some much-needed staff.
“I have an excellent bookkeeper, who does all the financials, invoicing, and budgeting—almost like a controller,” says Dr. Pook. “And I just hired a virtual assistant last week. I’ve found that it works best when I farm out the calling and scheduling and I just focus on the marketing. And I include talking to the physicians in that.”
Get Started
So how do you begin your transformation from hospitalist to hospitalist-entrepreneur?
“The basic steps begin with identifying whether this is an escapist fantasy or a deep, abiding interest,” stresses Dr. Kennealy. “It will take a deep interest to get you through the difficult times—it’s a real commitment.”
Once you determine you’re willing to invest time and expense in your own business, Dr. Kennealy advises you to assess your skills and acquire any new ones you’ll need. One way is to meet businesspeople, learn how they think, and understand the language of business. You can also study business and marketing books and journals or take business courses.
“I think physicians don’t know how to run a business,” says Dr. Pook. “We’re not trained to do this. What really helped me was a business coach. I’d advise others to either get a coach or get hooked up with someone who knows a lot about business.”
Before you make too deep a commitment, consider an important component. “You need some sense of the marketplace,” says Dr. Kennealy. Who will buy your product or service? Is there enough interest to support your efforts? What is the competition like in your area?
The next step, she says, is to develop a business plan. “There are free resources available at SCORE.org [the Web site of SCORE, Counselors to America’s Small Business],” she says. “As you start on your plan, you may see that you require further analysis. You need to close those knowledge gaps before you start the business.”
And finally, you have to have marketing savvy to make it work. “Wrap it all up in a sound marketing plan,” concludes Dr. Kennealy. “How will you reach your target audience, and how will you do it efficiently? You must learn the art of marketing, and most physicians don’t have a clue. You have to shift your thinking from a physician whose patients basically come flocking to someone who has to attract and keep customers.” TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
You may have an idea for a business you’d like to start, perhaps attracted by the prospect of controlling your time and work, chasing extra income, or fulfilling the dream of having an alternate career. Should you try turning your dream into reality—and if so, how?
Philippa Kennealy, MD, MPH, has guided hospitalists and other physicians along this path. She heads The Entrepreneurial MD, a Los Angeles-based coaching service for physicians who want to become more entrepreneurial with their practices or start a side business. She has a unique perspective on how physicians can add a satisfying second career to their practice of medicine. “I myself am a physician-entrepreneur,” says Dr. Kennealy.
Why Increase Workloads?
What makes busy hospitalists seek a side business? Why overload your schedule with the extra hours and responsibilities of running a business?
“It’s an opportunity to do something that feels creative, that gives you control,” explains Dr. Kennealy. “I feel that physicians don’t get to use creativity, and they don’t have much control. Their daily actions and decisions are quite regulated. Owning their own time is attractive to physicians. Hospitalists in particular are at it all day in the hospital.”
Is it really possible to continue to work as a hospitalist while shaping a second business? Yes—and others have done it.
“A lot of physicians dream of [entrepreneurship] but feel trapped by their existing time commitments,” says Dr. Kennealy. “But there are some who take the necessary steps, who carve out the time to do it. Many of them hook up with someone to form a partnership—often this is with a non-physician.”
Types of Endeavors
Some physicians are interested in a start-up business that goes hand in hand with their patient care; others may go in a completely different direction.
“There’s an enormous array of [physician-owned businesses] out there,” says Dr. Kennealy. “Many of my clients go into consulting, mostly within healthcare. Some have developed a software application that supports some aspect of healthcare.” Other physicians open health and wellness centers. One of Dr. Kennealy’s clients has developed a sculpting business and is ready to open her own gallery.
Lucia Ferreras-Cox, MD, works as an independent contractor in urgent care and hospital medicine while she runs her company, Ejerce Medecina USA, in Gilbert, Ariz. Ejerce offers Web-based training for Spanish-speaking physicians in other countries to help them pass the U.S. medical board review, then serves as a recruiting firm for those physicians once they get their U.S. licenses.
“I went back to business school for three months to refresh my skills,” says Dr. Ferreras-Cox, who previously had a pediatric practice. “I had to relearn—to learn that I was not a not-for-profit anymore.”
Marica Pook, MD, is a full-time hospitalist in Superior, Colo., and president of ExtraMD PC, a company that provides short-term physician staffing. Her start-up was quite simple. “I’ve been a hospitalist for seven years now, and of course part of my job is to call primary care physicians about patients,” Dr. Pook says. “I started thinking about what it’s like for those physicians and how they can get some help when they’re at their busiest.”
She decided to provide that help. In 2004 she used her contacts to start a kind of mini locum tenens job, working for different physician groups and hospitals. “Nine months into it, I started bringing in other physicians,” she says. Today, the business is thriving, with a growing number of local physicians involved, as well as some much-needed staff.
“I have an excellent bookkeeper, who does all the financials, invoicing, and budgeting—almost like a controller,” says Dr. Pook. “And I just hired a virtual assistant last week. I’ve found that it works best when I farm out the calling and scheduling and I just focus on the marketing. And I include talking to the physicians in that.”
Get Started
So how do you begin your transformation from hospitalist to hospitalist-entrepreneur?
“The basic steps begin with identifying whether this is an escapist fantasy or a deep, abiding interest,” stresses Dr. Kennealy. “It will take a deep interest to get you through the difficult times—it’s a real commitment.”
Once you determine you’re willing to invest time and expense in your own business, Dr. Kennealy advises you to assess your skills and acquire any new ones you’ll need. One way is to meet businesspeople, learn how they think, and understand the language of business. You can also study business and marketing books and journals or take business courses.
“I think physicians don’t know how to run a business,” says Dr. Pook. “We’re not trained to do this. What really helped me was a business coach. I’d advise others to either get a coach or get hooked up with someone who knows a lot about business.”
Before you make too deep a commitment, consider an important component. “You need some sense of the marketplace,” says Dr. Kennealy. Who will buy your product or service? Is there enough interest to support your efforts? What is the competition like in your area?
The next step, she says, is to develop a business plan. “There are free resources available at SCORE.org [the Web site of SCORE, Counselors to America’s Small Business],” she says. “As you start on your plan, you may see that you require further analysis. You need to close those knowledge gaps before you start the business.”
And finally, you have to have marketing savvy to make it work. “Wrap it all up in a sound marketing plan,” concludes Dr. Kennealy. “How will you reach your target audience, and how will you do it efficiently? You must learn the art of marketing, and most physicians don’t have a clue. You have to shift your thinking from a physician whose patients basically come flocking to someone who has to attract and keep customers.” TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
The DNR Dilemma

When it comes to communicating do-not-resuscitate (DNR) orders, hospitals rely on a bewildering array of paper documentation, electronic records, and colored wristbands that can easily be misinterpreted.
These are the findings reported in the November-December issue of the Journal of Hospital Medicine by Niraj Sehgal, MD, and Robert Wachter, MD. Dr. Wachter is associate chair of the department of medicine at the University of California, San Francisco. Dr. Sehgal is an assistant clinical professor of medicine at the school.
In a survey of 69 nursing executives representing hospitals in a consortium of academic medical centers, “More than 70% of respondents recalled situations when confusion around a DNR order led to problems in patient care,” the authors say.
Everyone has a “near-miss” story, says Dr. Sehgal.
In one budget-minded hospital where materials were recycled, someone forgot to remove a DNR sticker from a previous patient’s folder before the folder was assigned to someone else. Several nurses told of instances in which patients were resuscitated inappropriately because hospital staff members did not see DNR stickers in the patient’s chart, the patient was off the unit for a procedure without a complete chart, or the DNR order was buried under other materials.
Much of the problem stems from the lack of a standardized method for making a patient’s DNR wishes known, Dr. Sehgal explains.
For example, in 2004 Dr. Sehgal saw a newspaper report that BayCare Health hospitals, in and around Tampa, Fla., were covering yellow “Livestrong” bracelets issued by the Lance Armstrong Foundation and worn by some patients to support those living with cancer. BayCare uses yellow bracelets for DNR patients. Nearly 20% of Americans wear “Livestrong” bracelets, posing a challenge for any hospital that also uses yellow bracelets to indicate DNR.
The newspaper story was the impetus for this study, Dr. Sehgal recalls. “I saw that article and thought, ‘What a great metaphor for the need for standardization.’”
He and Dr. Wachter designed a brief survey and distributed it via an e-mail listserve to senior nursing staff members of the University HealthSystem Consortium, an alliance of 97 academic medical centers and their affiliated hospitals. Those institutions represent 90% of the nation’s nonprofit academic medical centers.
Of the 127 nursing executives who received survey announcements, 69 (54%) returned completed questionnaires. Of those, 39 (56%) reported that their hospitals documented patients’ DNR preferences only in the charts, while 11 (16%) used only electronic health records (EHRs). Seventeen (25%) augmented the paper charts or EHRs with color-coded wristbands in eight colors.
“We expected variability, but even so we were struck by how much variability existed in our findings,” Dr. Sehgal says.
Hospitals use wristbands in a rainbow of colors to convey many messages. Of the hospitals represented in this survey, 55% used them to warn of allergies, fall risks, and even same last names. The authors found “12 different indications were depicted by various colors, with variations in both the color choice for a given indication (e.g., red and yellow used for allergy wristbands at different hospitals) and across indications (e.g., red for allergy at one hospital and red for bleeding risk at another).”

A national, standardized system for conveying patients’ DNR wishes would seem logical, but no system is in place, Dr. Sehgal says. Hospitals cannot even agree on which method to use. While some use wristbands, others use notices or stickers incorporated into the chart. Still others use EHRs.
A few states, including Arizona, Pennsylvania, and Colorado have established statewide standards for using wristbands—but each state chose a different color. “I suspect that many physicians don’t know the meaning of many of the wristbands used in their hospitals, especially if those doctors rotate among different hospitals or hospital systems,” Dr. Sehgal says.
Developing a system for making a patient’s wishes known to hospital staff is one of two challenges reflected in this study, he adds. The second is to use what might be perfunctory questions about advance directives as an opening for a deeper discussion about the patient’s thoughts on end-of-life care. Right now, those questions are just another process measure hospitals must document. “It becomes just another box to check instead of a tool for opening a conversation about what the patient’s wishes are,” he says.
Hospitalists should embrace the opportunity to involve the patient, the patient’s family members, and the primary care provider in an ongoing discussion about the patient’s desires over the course of the hospital stay. “This can give patients a mechanism for thinking about what they’d want under certain circumstances,” Dr. Sehgal explains.
From this study’s findings emerge two take-home messages for hospitalists, he maintains. The first is to remember that “we in inpatient settings spend a lot of time taking care of patients, and we must be aware of what those patients’ wishes are with respect to DNR.” The second is to step back and take an even broader view by remaining alert to processes other than DNR that might benefit from a standardized approach. “Maybe we should think about that, particularly when there is the potential to significantly harm patients,” he says. TH
Norra MacReady is a medical writer based in California.
When it comes to communicating do-not-resuscitate (DNR) orders, hospitals rely on a bewildering array of paper documentation, electronic records, and colored wristbands that can easily be misinterpreted.
These are the findings reported in the November-December issue of the Journal of Hospital Medicine by Niraj Sehgal, MD, and Robert Wachter, MD. Dr. Wachter is associate chair of the department of medicine at the University of California, San Francisco. Dr. Sehgal is an assistant clinical professor of medicine at the school.
In a survey of 69 nursing executives representing hospitals in a consortium of academic medical centers, “More than 70% of respondents recalled situations when confusion around a DNR order led to problems in patient care,” the authors say.
Everyone has a “near-miss” story, says Dr. Sehgal.
In one budget-minded hospital where materials were recycled, someone forgot to remove a DNR sticker from a previous patient’s folder before the folder was assigned to someone else. Several nurses told of instances in which patients were resuscitated inappropriately because hospital staff members did not see DNR stickers in the patient’s chart, the patient was off the unit for a procedure without a complete chart, or the DNR order was buried under other materials.
Much of the problem stems from the lack of a standardized method for making a patient’s DNR wishes known, Dr. Sehgal explains.
For example, in 2004 Dr. Sehgal saw a newspaper report that BayCare Health hospitals, in and around Tampa, Fla., were covering yellow “Livestrong” bracelets issued by the Lance Armstrong Foundation and worn by some patients to support those living with cancer. BayCare uses yellow bracelets for DNR patients. Nearly 20% of Americans wear “Livestrong” bracelets, posing a challenge for any hospital that also uses yellow bracelets to indicate DNR.
The newspaper story was the impetus for this study, Dr. Sehgal recalls. “I saw that article and thought, ‘What a great metaphor for the need for standardization.’”
He and Dr. Wachter designed a brief survey and distributed it via an e-mail listserve to senior nursing staff members of the University HealthSystem Consortium, an alliance of 97 academic medical centers and their affiliated hospitals. Those institutions represent 90% of the nation’s nonprofit academic medical centers.
Of the 127 nursing executives who received survey announcements, 69 (54%) returned completed questionnaires. Of those, 39 (56%) reported that their hospitals documented patients’ DNR preferences only in the charts, while 11 (16%) used only electronic health records (EHRs). Seventeen (25%) augmented the paper charts or EHRs with color-coded wristbands in eight colors.
“We expected variability, but even so we were struck by how much variability existed in our findings,” Dr. Sehgal says.
Hospitals use wristbands in a rainbow of colors to convey many messages. Of the hospitals represented in this survey, 55% used them to warn of allergies, fall risks, and even same last names. The authors found “12 different indications were depicted by various colors, with variations in both the color choice for a given indication (e.g., red and yellow used for allergy wristbands at different hospitals) and across indications (e.g., red for allergy at one hospital and red for bleeding risk at another).”
A national, standardized system for conveying patients’ DNR wishes would seem logical, but no system is in place, Dr. Sehgal says. Hospitals cannot even agree on which method to use. While some use wristbands, others use notices or stickers incorporated into the chart. Still others use EHRs.
A few states, including Arizona, Pennsylvania, and Colorado have established statewide standards for using wristbands—but each state chose a different color. “I suspect that many physicians don’t know the meaning of many of the wristbands used in their hospitals, especially if those doctors rotate among different hospitals or hospital systems,” Dr. Sehgal says.
Developing a system for making a patient’s wishes known to hospital staff is one of two challenges reflected in this study, he adds. The second is to use what might be perfunctory questions about advance directives as an opening for a deeper discussion about the patient’s thoughts on end-of-life care. Right now, those questions are just another process measure hospitals must document. “It becomes just another box to check instead of a tool for opening a conversation about what the patient’s wishes are,” he says.
Hospitalists should embrace the opportunity to involve the patient, the patient’s family members, and the primary care provider in an ongoing discussion about the patient’s desires over the course of the hospital stay. “This can give patients a mechanism for thinking about what they’d want under certain circumstances,” Dr. Sehgal explains.
From this study’s findings emerge two take-home messages for hospitalists, he maintains. The first is to remember that “we in inpatient settings spend a lot of time taking care of patients, and we must be aware of what those patients’ wishes are with respect to DNR.” The second is to step back and take an even broader view by remaining alert to processes other than DNR that might benefit from a standardized approach. “Maybe we should think about that, particularly when there is the potential to significantly harm patients,” he says. TH
Norra MacReady is a medical writer based in California.
When it comes to communicating do-not-resuscitate (DNR) orders, hospitals rely on a bewildering array of paper documentation, electronic records, and colored wristbands that can easily be misinterpreted.
These are the findings reported in the November-December issue of the Journal of Hospital Medicine by Niraj Sehgal, MD, and Robert Wachter, MD. Dr. Wachter is associate chair of the department of medicine at the University of California, San Francisco. Dr. Sehgal is an assistant clinical professor of medicine at the school.
In a survey of 69 nursing executives representing hospitals in a consortium of academic medical centers, “More than 70% of respondents recalled situations when confusion around a DNR order led to problems in patient care,” the authors say.
Everyone has a “near-miss” story, says Dr. Sehgal.
In one budget-minded hospital where materials were recycled, someone forgot to remove a DNR sticker from a previous patient’s folder before the folder was assigned to someone else. Several nurses told of instances in which patients were resuscitated inappropriately because hospital staff members did not see DNR stickers in the patient’s chart, the patient was off the unit for a procedure without a complete chart, or the DNR order was buried under other materials.
Much of the problem stems from the lack of a standardized method for making a patient’s DNR wishes known, Dr. Sehgal explains.
For example, in 2004 Dr. Sehgal saw a newspaper report that BayCare Health hospitals, in and around Tampa, Fla., were covering yellow “Livestrong” bracelets issued by the Lance Armstrong Foundation and worn by some patients to support those living with cancer. BayCare uses yellow bracelets for DNR patients. Nearly 20% of Americans wear “Livestrong” bracelets, posing a challenge for any hospital that also uses yellow bracelets to indicate DNR.
The newspaper story was the impetus for this study, Dr. Sehgal recalls. “I saw that article and thought, ‘What a great metaphor for the need for standardization.’”
He and Dr. Wachter designed a brief survey and distributed it via an e-mail listserve to senior nursing staff members of the University HealthSystem Consortium, an alliance of 97 academic medical centers and their affiliated hospitals. Those institutions represent 90% of the nation’s nonprofit academic medical centers.
Of the 127 nursing executives who received survey announcements, 69 (54%) returned completed questionnaires. Of those, 39 (56%) reported that their hospitals documented patients’ DNR preferences only in the charts, while 11 (16%) used only electronic health records (EHRs). Seventeen (25%) augmented the paper charts or EHRs with color-coded wristbands in eight colors.
“We expected variability, but even so we were struck by how much variability existed in our findings,” Dr. Sehgal says.
Hospitals use wristbands in a rainbow of colors to convey many messages. Of the hospitals represented in this survey, 55% used them to warn of allergies, fall risks, and even same last names. The authors found “12 different indications were depicted by various colors, with variations in both the color choice for a given indication (e.g., red and yellow used for allergy wristbands at different hospitals) and across indications (e.g., red for allergy at one hospital and red for bleeding risk at another).”
A national, standardized system for conveying patients’ DNR wishes would seem logical, but no system is in place, Dr. Sehgal says. Hospitals cannot even agree on which method to use. While some use wristbands, others use notices or stickers incorporated into the chart. Still others use EHRs.
A few states, including Arizona, Pennsylvania, and Colorado have established statewide standards for using wristbands—but each state chose a different color. “I suspect that many physicians don’t know the meaning of many of the wristbands used in their hospitals, especially if those doctors rotate among different hospitals or hospital systems,” Dr. Sehgal says.
Developing a system for making a patient’s wishes known to hospital staff is one of two challenges reflected in this study, he adds. The second is to use what might be perfunctory questions about advance directives as an opening for a deeper discussion about the patient’s thoughts on end-of-life care. Right now, those questions are just another process measure hospitals must document. “It becomes just another box to check instead of a tool for opening a conversation about what the patient’s wishes are,” he says.
Hospitalists should embrace the opportunity to involve the patient, the patient’s family members, and the primary care provider in an ongoing discussion about the patient’s desires over the course of the hospital stay. “This can give patients a mechanism for thinking about what they’d want under certain circumstances,” Dr. Sehgal explains.
From this study’s findings emerge two take-home messages for hospitalists, he maintains. The first is to remember that “we in inpatient settings spend a lot of time taking care of patients, and we must be aware of what those patients’ wishes are with respect to DNR.” The second is to step back and take an even broader view by remaining alert to processes other than DNR that might benefit from a standardized approach. “Maybe we should think about that, particularly when there is the potential to significantly harm patients,” he says. TH
Norra MacReady is a medical writer based in California.
Avoid Pancreatitis Risk
Drugs are an often-overlooked cause of pancreatitis in hospitalized patients.1,2 Knowing which drugs are associated with acute pancreatic inflammation can help the hospitalist consider specific drugs as the cause within their differential diagnosis.
The two most common causes of acute pancreatitis are biliary disease (30%-60%) and chronic alcohol use (15%-30%). Drug-induced pancreatitis (DIP) has occurred with more than 100 prescribed medications.3,4
Most cases of acute pancreatitis are reversible and resolve on their own within three to seven days after treatment begins. A small number of patients develop severe complications, and their mortality rate nears 30%. Symptoms may last a few days and can include mild to severe epigastric pain that can radiate to the back, chest, flank, or lower abdomen.
Other symptoms can include nausea, vomiting, fever, abdominal tenderness, jaundice, or hypotension. Serum amylase and lipase levels usually rise to three times the upper limit of normal. Use of computerized tomography (CT) or ultrasound can help the diagnosis.
The mechanism of DIP is not known, but is thought to be predominantly due to an idiosyncratic reaction, and for a few agents/classes, to intrinsic drug toxicity.5 The incidence of DIP is approximately 1.4%-5%. Not knowing the exact number of prescriptions for each medication and the cases of pancreatitis from each impedes the determination of incidence.
Most data on DIP are from case reports or reviews of compiled cases. The validity and severity of DIP is unknown mostly because cases are underreported to MedWatch. Reasons for underreporting include:
- Low index of suspicion for DIP compared with drug- induced hepatotoxicity;
- Milder cases due to missed lower enzyme levels (not routinely ascertained in a metabolic panel);
- Missed latency of exposure; and
- Erroneous classification as alcoholic or biliary disease by default.
Drug-induced pancreatitis is more common in patients who have inflammatory bowel disease, AIDS, cancer, or gastrointestinal disease. It is also common in those who are geriatric, HIV positive, or who are on immunomodulating agents.6
An early compilation of DIP reports was published by Lankisch, et al. This was a retrospective evaluation that excluded all other pancreatitis etiologies (e.g., post-endoscopic retrograde cholangiopancreatography (ERCP), post-traumatic, post-operative, viral), except drugs. Out of 1,613 patients with acute pancreatitis, there were 22 cases of DIP due to the following agents: azathioprine (n=6), mesalamine/sulfasalazine (n=5) didanosine (ddI, n=4), estrogens (n=3), furosemide (n=2), hydrochlorothiazide (HCTZ, n=1), and rifampicin (n=1). Rechallenge was not attempted for ethical reasons. The mean hospital stay was 25.5 days (range two to 78 days), with an incidence of 1.2%. Two patients died (from AIDS and tuberculosis). The authors noted that other studies show a high fatality rate from azathioprine, ddI, furosemide, and HCTZ.
New Drugs
![]()
Raltegravir (Isentress), an oral integrase inhibitor, is in a new class of antiretrovirals. This agent was FDA approved for use in combination with other antiretroviral therapy for treating HIV infection in patients with ongoing viral replication despite treatment.
New Indications
Levofloxacin 750 mg IV injection and oral tablets (Levaquin) have been FDA approved as a five-day, once-daily course for the treatment of complicated urinary tract infections and acute pyelonephritis.
Raloxifene 60 mg tablets (Evista) have been FDA approved to reduce the risk of invasive breast cancer in two populations of postmenopausal women: those with osteoporosis and those at high risk for invasive breast cancer.
Additionally, Triveldi, et al., evaluated cases reported in the literature or unpublished cases from 1966 through 2004. They then classified the drugs into one of three categories based on strength of evidence of DIP association.
Class I included medications causing more than 20 reported cases with at least one case following rechallenge. Class II were medications causing more than 10 but fewer than 20 reported cases with/without a positive rechallenge, and Class III were all medications in 10 or fewer cases or unpublished reports (FDA or pharmaceutical company records). Following are some of the most common reports from drugs available in the U.S.:
- Class I: ddI (n=883), asparaginase (n=177), azathioprine (n=86), valproic acid (n=80), pentavalent antimonials (parenterals to treat leishmaniasis, n=80), pentamidine (n=79), mercaptopurine (n=69), mesalamine (n=59), estrogens (n=42), opiates (n=42), tetracycline (n=34), cytarabine (n=26), steroids (n=25), sulfamethoxazole/trimethoprim (SMZ-TMP, n=24), sulfasalazine (n=23), furosemide (n=21), sulindac (n=21);
- Class II: rifampin, lamivudine, octreotide, carbamazepine, acetaminophen, interferon alfa-2b, enalapril, HCTZ, cisplatin, erythromycin; and
- Class III (numerous agents, including the following classes): quinolones, macrolides, angiotensin-converting enzyme inhibitors (ACEIs), statins, and others.
Most recently Badalov, et al., evaluated cases from Medline (through July 1, 2006) and classified them based on levels of evidence. These levels were:
- Definite (imaging study or autopsy confirmed diagnosis);
- Probable (typical symptoms present and threefold increase in amylase and/or lipase); or
- Possible (all others, not included in the final analysis).
Cases were further subclassified into four classes:
- Class Ia (1 or more cases with positive rechallenge, excluding all other causes): codeine, conjugated estrogens, enalapril, isoniazid, metronidazole, mesalamine, pravastatin (other statins), procainamide, simvastatin, sulindac, sulfa drugs, tetracycline, and valproic acid;
- Class Ib (1 or more cases with positive rechallenge, not excluding all other causes): amiodarone, azathioprine, clomiphene, cytosine arabinoside, dapsone, dexamethasone (other steroids), estrogens, furosemide, ifosfamide, lamivudine, losartan, 6-MP, methimazole, methyldopa, nelfinavir, omeprazole, pentamidine, SMZ-TMP, and trans-retinoic acid (not topical);
- Class II (four or more cases, consistent latency in 75% of cases): acetaminophen, clozapine, ddI, erythromycin, l-asparaginase/peg-asparaginase, pentamidine, propofol, and tamoxifen;
- Class III (two or more cases, no consistent latency, no rechallenge): alendronate, captopril, carbamazepine, ceftriaxone, HCTZ, interferon, lisinopril, metformin, mirtazapine, naproxen, and others; and
- Class IV (one case, no other class, without rechallenge): too numerous.
Additionally, the Australian Adverse Drug Reactions Advisory Committee reported on the top 12 DIP-associated medications (n=414 reports implicating 695 drugs). The most commonly reported drugs included azathioprine, ddI, valproate, stavudine, simvastatin, clozapine, lamivudine, ezetimibe, prednisolone, olanzapine, celecoxib and 6-MP, which are listed in each medication’s Australian product information.
The following drugs/classes have been implicated in causing DIP:
- AIDS therapies: ddI, pentamidine;
- Antimicrobials: metronidazole, sulfonamides, tetracyclines;
- Diuretics: furosemide, HCTZ;
- Anti-inflammatories: mesalamine, salicylates, sulindac, sulfasalazine;
- Immunosuppressives: asparaginase, azathioprine, mercaptopurine; and
- Neuropsychiatric agents: valproic acid.
The American Gastroenterologic Association Institute has developed a guide for managing acute pancreatitis. Additionally, they note that when assessing DIP, consider prescription, over-the-counter, and herbal products, too.7 Pancreatitis can occur with certain drugs or medication classes, some more often than others.
Consider DIP in the differential diagnosis of patients who present with or develop epigastric pain. Question all patients with acute pancreatitis about their medication use as a possible cause for the disease. Assessment of amylase/lipase will aid in the diagnosis. To prevent further compromise in cases where DIP is suspected, hold the offending agent (and substitute if possible) to decrease further episodes. TH
Michele B Kaufman is a freelance medical writer based in New York City.
References
- Lankisch PG, Dröge M, Gottesleben F. Drug-induced acute pancreatitis: incidence and severity. Gut. 1995 Oct;37(4):565-567.
- Eltookhy A, Pearson NL. Drug-induced pancreatitis. Can Pharm J. 2006;139(6):58-60.
- Trivedi CD, Pitchumoni CS. Drug-induced pancreatitis: an update. J Clin Gastroenterol. 2005 Sept;39(8):709-716.
- Badalov N, Baradarian R, Iswara K, et al. Drug-induced pancreatitis: an evidence-based review. Clin Gastroenterol Hepatol. 2007 Jun;5(6):648-661.
- Vege SS, Chari ST. Etiology of acute pancreatitis. In: UpToDate, Rose, BD (Ed), UpToDate, Waltham, Mass., 2007.
- Skirvin A. Drug-induced pancreatitis. Aust Adv Drug Reactions Bull. 2006 Dec;25(6):22.
- American Gastroenterological Association Institute Medical Position Statement on Acute Pancreatitis. Gastroenterology. 1998 Sep;115(3):763-764.
Drugs are an often-overlooked cause of pancreatitis in hospitalized patients.1,2 Knowing which drugs are associated with acute pancreatic inflammation can help the hospitalist consider specific drugs as the cause within their differential diagnosis.
The two most common causes of acute pancreatitis are biliary disease (30%-60%) and chronic alcohol use (15%-30%). Drug-induced pancreatitis (DIP) has occurred with more than 100 prescribed medications.3,4
Most cases of acute pancreatitis are reversible and resolve on their own within three to seven days after treatment begins. A small number of patients develop severe complications, and their mortality rate nears 30%. Symptoms may last a few days and can include mild to severe epigastric pain that can radiate to the back, chest, flank, or lower abdomen.
Other symptoms can include nausea, vomiting, fever, abdominal tenderness, jaundice, or hypotension. Serum amylase and lipase levels usually rise to three times the upper limit of normal. Use of computerized tomography (CT) or ultrasound can help the diagnosis.
The mechanism of DIP is not known, but is thought to be predominantly due to an idiosyncratic reaction, and for a few agents/classes, to intrinsic drug toxicity.5 The incidence of DIP is approximately 1.4%-5%. Not knowing the exact number of prescriptions for each medication and the cases of pancreatitis from each impedes the determination of incidence.
Most data on DIP are from case reports or reviews of compiled cases. The validity and severity of DIP is unknown mostly because cases are underreported to MedWatch. Reasons for underreporting include:
- Low index of suspicion for DIP compared with drug- induced hepatotoxicity;
- Milder cases due to missed lower enzyme levels (not routinely ascertained in a metabolic panel);
- Missed latency of exposure; and
- Erroneous classification as alcoholic or biliary disease by default.
Drug-induced pancreatitis is more common in patients who have inflammatory bowel disease, AIDS, cancer, or gastrointestinal disease. It is also common in those who are geriatric, HIV positive, or who are on immunomodulating agents.6
An early compilation of DIP reports was published by Lankisch, et al. This was a retrospective evaluation that excluded all other pancreatitis etiologies (e.g., post-endoscopic retrograde cholangiopancreatography (ERCP), post-traumatic, post-operative, viral), except drugs. Out of 1,613 patients with acute pancreatitis, there were 22 cases of DIP due to the following agents: azathioprine (n=6), mesalamine/sulfasalazine (n=5) didanosine (ddI, n=4), estrogens (n=3), furosemide (n=2), hydrochlorothiazide (HCTZ, n=1), and rifampicin (n=1). Rechallenge was not attempted for ethical reasons. The mean hospital stay was 25.5 days (range two to 78 days), with an incidence of 1.2%. Two patients died (from AIDS and tuberculosis). The authors noted that other studies show a high fatality rate from azathioprine, ddI, furosemide, and HCTZ.
New Drugs
![]()
Raltegravir (Isentress), an oral integrase inhibitor, is in a new class of antiretrovirals. This agent was FDA approved for use in combination with other antiretroviral therapy for treating HIV infection in patients with ongoing viral replication despite treatment.
New Indications
Levofloxacin 750 mg IV injection and oral tablets (Levaquin) have been FDA approved as a five-day, once-daily course for the treatment of complicated urinary tract infections and acute pyelonephritis.
Raloxifene 60 mg tablets (Evista) have been FDA approved to reduce the risk of invasive breast cancer in two populations of postmenopausal women: those with osteoporosis and those at high risk for invasive breast cancer.
Additionally, Triveldi, et al., evaluated cases reported in the literature or unpublished cases from 1966 through 2004. They then classified the drugs into one of three categories based on strength of evidence of DIP association.
Class I included medications causing more than 20 reported cases with at least one case following rechallenge. Class II were medications causing more than 10 but fewer than 20 reported cases with/without a positive rechallenge, and Class III were all medications in 10 or fewer cases or unpublished reports (FDA or pharmaceutical company records). Following are some of the most common reports from drugs available in the U.S.:
- Class I: ddI (n=883), asparaginase (n=177), azathioprine (n=86), valproic acid (n=80), pentavalent antimonials (parenterals to treat leishmaniasis, n=80), pentamidine (n=79), mercaptopurine (n=69), mesalamine (n=59), estrogens (n=42), opiates (n=42), tetracycline (n=34), cytarabine (n=26), steroids (n=25), sulfamethoxazole/trimethoprim (SMZ-TMP, n=24), sulfasalazine (n=23), furosemide (n=21), sulindac (n=21);
- Class II: rifampin, lamivudine, octreotide, carbamazepine, acetaminophen, interferon alfa-2b, enalapril, HCTZ, cisplatin, erythromycin; and
- Class III (numerous agents, including the following classes): quinolones, macrolides, angiotensin-converting enzyme inhibitors (ACEIs), statins, and others.
Most recently Badalov, et al., evaluated cases from Medline (through July 1, 2006) and classified them based on levels of evidence. These levels were:
- Definite (imaging study or autopsy confirmed diagnosis);
- Probable (typical symptoms present and threefold increase in amylase and/or lipase); or
- Possible (all others, not included in the final analysis).
Cases were further subclassified into four classes:
- Class Ia (1 or more cases with positive rechallenge, excluding all other causes): codeine, conjugated estrogens, enalapril, isoniazid, metronidazole, mesalamine, pravastatin (other statins), procainamide, simvastatin, sulindac, sulfa drugs, tetracycline, and valproic acid;
- Class Ib (1 or more cases with positive rechallenge, not excluding all other causes): amiodarone, azathioprine, clomiphene, cytosine arabinoside, dapsone, dexamethasone (other steroids), estrogens, furosemide, ifosfamide, lamivudine, losartan, 6-MP, methimazole, methyldopa, nelfinavir, omeprazole, pentamidine, SMZ-TMP, and trans-retinoic acid (not topical);
- Class II (four or more cases, consistent latency in 75% of cases): acetaminophen, clozapine, ddI, erythromycin, l-asparaginase/peg-asparaginase, pentamidine, propofol, and tamoxifen;
- Class III (two or more cases, no consistent latency, no rechallenge): alendronate, captopril, carbamazepine, ceftriaxone, HCTZ, interferon, lisinopril, metformin, mirtazapine, naproxen, and others; and
- Class IV (one case, no other class, without rechallenge): too numerous.
Additionally, the Australian Adverse Drug Reactions Advisory Committee reported on the top 12 DIP-associated medications (n=414 reports implicating 695 drugs). The most commonly reported drugs included azathioprine, ddI, valproate, stavudine, simvastatin, clozapine, lamivudine, ezetimibe, prednisolone, olanzapine, celecoxib and 6-MP, which are listed in each medication’s Australian product information.
The following drugs/classes have been implicated in causing DIP:
- AIDS therapies: ddI, pentamidine;
- Antimicrobials: metronidazole, sulfonamides, tetracyclines;
- Diuretics: furosemide, HCTZ;
- Anti-inflammatories: mesalamine, salicylates, sulindac, sulfasalazine;
- Immunosuppressives: asparaginase, azathioprine, mercaptopurine; and
- Neuropsychiatric agents: valproic acid.
The American Gastroenterologic Association Institute has developed a guide for managing acute pancreatitis. Additionally, they note that when assessing DIP, consider prescription, over-the-counter, and herbal products, too.7 Pancreatitis can occur with certain drugs or medication classes, some more often than others.
Consider DIP in the differential diagnosis of patients who present with or develop epigastric pain. Question all patients with acute pancreatitis about their medication use as a possible cause for the disease. Assessment of amylase/lipase will aid in the diagnosis. To prevent further compromise in cases where DIP is suspected, hold the offending agent (and substitute if possible) to decrease further episodes. TH
Michele B Kaufman is a freelance medical writer based in New York City.
References
- Lankisch PG, Dröge M, Gottesleben F. Drug-induced acute pancreatitis: incidence and severity. Gut. 1995 Oct;37(4):565-567.
- Eltookhy A, Pearson NL. Drug-induced pancreatitis. Can Pharm J. 2006;139(6):58-60.
- Trivedi CD, Pitchumoni CS. Drug-induced pancreatitis: an update. J Clin Gastroenterol. 2005 Sept;39(8):709-716.
- Badalov N, Baradarian R, Iswara K, et al. Drug-induced pancreatitis: an evidence-based review. Clin Gastroenterol Hepatol. 2007 Jun;5(6):648-661.
- Vege SS, Chari ST. Etiology of acute pancreatitis. In: UpToDate, Rose, BD (Ed), UpToDate, Waltham, Mass., 2007.
- Skirvin A. Drug-induced pancreatitis. Aust Adv Drug Reactions Bull. 2006 Dec;25(6):22.
- American Gastroenterological Association Institute Medical Position Statement on Acute Pancreatitis. Gastroenterology. 1998 Sep;115(3):763-764.
Drugs are an often-overlooked cause of pancreatitis in hospitalized patients.1,2 Knowing which drugs are associated with acute pancreatic inflammation can help the hospitalist consider specific drugs as the cause within their differential diagnosis.
The two most common causes of acute pancreatitis are biliary disease (30%-60%) and chronic alcohol use (15%-30%). Drug-induced pancreatitis (DIP) has occurred with more than 100 prescribed medications.3,4
Most cases of acute pancreatitis are reversible and resolve on their own within three to seven days after treatment begins. A small number of patients develop severe complications, and their mortality rate nears 30%. Symptoms may last a few days and can include mild to severe epigastric pain that can radiate to the back, chest, flank, or lower abdomen.
Other symptoms can include nausea, vomiting, fever, abdominal tenderness, jaundice, or hypotension. Serum amylase and lipase levels usually rise to three times the upper limit of normal. Use of computerized tomography (CT) or ultrasound can help the diagnosis.
The mechanism of DIP is not known, but is thought to be predominantly due to an idiosyncratic reaction, and for a few agents/classes, to intrinsic drug toxicity.5 The incidence of DIP is approximately 1.4%-5%. Not knowing the exact number of prescriptions for each medication and the cases of pancreatitis from each impedes the determination of incidence.
Most data on DIP are from case reports or reviews of compiled cases. The validity and severity of DIP is unknown mostly because cases are underreported to MedWatch. Reasons for underreporting include:
- Low index of suspicion for DIP compared with drug- induced hepatotoxicity;
- Milder cases due to missed lower enzyme levels (not routinely ascertained in a metabolic panel);
- Missed latency of exposure; and
- Erroneous classification as alcoholic or biliary disease by default.
Drug-induced pancreatitis is more common in patients who have inflammatory bowel disease, AIDS, cancer, or gastrointestinal disease. It is also common in those who are geriatric, HIV positive, or who are on immunomodulating agents.6
An early compilation of DIP reports was published by Lankisch, et al. This was a retrospective evaluation that excluded all other pancreatitis etiologies (e.g., post-endoscopic retrograde cholangiopancreatography (ERCP), post-traumatic, post-operative, viral), except drugs. Out of 1,613 patients with acute pancreatitis, there were 22 cases of DIP due to the following agents: azathioprine (n=6), mesalamine/sulfasalazine (n=5) didanosine (ddI, n=4), estrogens (n=3), furosemide (n=2), hydrochlorothiazide (HCTZ, n=1), and rifampicin (n=1). Rechallenge was not attempted for ethical reasons. The mean hospital stay was 25.5 days (range two to 78 days), with an incidence of 1.2%. Two patients died (from AIDS and tuberculosis). The authors noted that other studies show a high fatality rate from azathioprine, ddI, furosemide, and HCTZ.
New Drugs
![]()
Raltegravir (Isentress), an oral integrase inhibitor, is in a new class of antiretrovirals. This agent was FDA approved for use in combination with other antiretroviral therapy for treating HIV infection in patients with ongoing viral replication despite treatment.
New Indications
Levofloxacin 750 mg IV injection and oral tablets (Levaquin) have been FDA approved as a five-day, once-daily course for the treatment of complicated urinary tract infections and acute pyelonephritis.
Raloxifene 60 mg tablets (Evista) have been FDA approved to reduce the risk of invasive breast cancer in two populations of postmenopausal women: those with osteoporosis and those at high risk for invasive breast cancer.
Additionally, Triveldi, et al., evaluated cases reported in the literature or unpublished cases from 1966 through 2004. They then classified the drugs into one of three categories based on strength of evidence of DIP association.
Class I included medications causing more than 20 reported cases with at least one case following rechallenge. Class II were medications causing more than 10 but fewer than 20 reported cases with/without a positive rechallenge, and Class III were all medications in 10 or fewer cases or unpublished reports (FDA or pharmaceutical company records). Following are some of the most common reports from drugs available in the U.S.:
- Class I: ddI (n=883), asparaginase (n=177), azathioprine (n=86), valproic acid (n=80), pentavalent antimonials (parenterals to treat leishmaniasis, n=80), pentamidine (n=79), mercaptopurine (n=69), mesalamine (n=59), estrogens (n=42), opiates (n=42), tetracycline (n=34), cytarabine (n=26), steroids (n=25), sulfamethoxazole/trimethoprim (SMZ-TMP, n=24), sulfasalazine (n=23), furosemide (n=21), sulindac (n=21);
- Class II: rifampin, lamivudine, octreotide, carbamazepine, acetaminophen, interferon alfa-2b, enalapril, HCTZ, cisplatin, erythromycin; and
- Class III (numerous agents, including the following classes): quinolones, macrolides, angiotensin-converting enzyme inhibitors (ACEIs), statins, and others.
Most recently Badalov, et al., evaluated cases from Medline (through July 1, 2006) and classified them based on levels of evidence. These levels were:
- Definite (imaging study or autopsy confirmed diagnosis);
- Probable (typical symptoms present and threefold increase in amylase and/or lipase); or
- Possible (all others, not included in the final analysis).
Cases were further subclassified into four classes:
- Class Ia (1 or more cases with positive rechallenge, excluding all other causes): codeine, conjugated estrogens, enalapril, isoniazid, metronidazole, mesalamine, pravastatin (other statins), procainamide, simvastatin, sulindac, sulfa drugs, tetracycline, and valproic acid;
- Class Ib (1 or more cases with positive rechallenge, not excluding all other causes): amiodarone, azathioprine, clomiphene, cytosine arabinoside, dapsone, dexamethasone (other steroids), estrogens, furosemide, ifosfamide, lamivudine, losartan, 6-MP, methimazole, methyldopa, nelfinavir, omeprazole, pentamidine, SMZ-TMP, and trans-retinoic acid (not topical);
- Class II (four or more cases, consistent latency in 75% of cases): acetaminophen, clozapine, ddI, erythromycin, l-asparaginase/peg-asparaginase, pentamidine, propofol, and tamoxifen;
- Class III (two or more cases, no consistent latency, no rechallenge): alendronate, captopril, carbamazepine, ceftriaxone, HCTZ, interferon, lisinopril, metformin, mirtazapine, naproxen, and others; and
- Class IV (one case, no other class, without rechallenge): too numerous.
Additionally, the Australian Adverse Drug Reactions Advisory Committee reported on the top 12 DIP-associated medications (n=414 reports implicating 695 drugs). The most commonly reported drugs included azathioprine, ddI, valproate, stavudine, simvastatin, clozapine, lamivudine, ezetimibe, prednisolone, olanzapine, celecoxib and 6-MP, which are listed in each medication’s Australian product information.
The following drugs/classes have been implicated in causing DIP:
- AIDS therapies: ddI, pentamidine;
- Antimicrobials: metronidazole, sulfonamides, tetracyclines;
- Diuretics: furosemide, HCTZ;
- Anti-inflammatories: mesalamine, salicylates, sulindac, sulfasalazine;
- Immunosuppressives: asparaginase, azathioprine, mercaptopurine; and
- Neuropsychiatric agents: valproic acid.
The American Gastroenterologic Association Institute has developed a guide for managing acute pancreatitis. Additionally, they note that when assessing DIP, consider prescription, over-the-counter, and herbal products, too.7 Pancreatitis can occur with certain drugs or medication classes, some more often than others.
Consider DIP in the differential diagnosis of patients who present with or develop epigastric pain. Question all patients with acute pancreatitis about their medication use as a possible cause for the disease. Assessment of amylase/lipase will aid in the diagnosis. To prevent further compromise in cases where DIP is suspected, hold the offending agent (and substitute if possible) to decrease further episodes. TH
Michele B Kaufman is a freelance medical writer based in New York City.
References
- Lankisch PG, Dröge M, Gottesleben F. Drug-induced acute pancreatitis: incidence and severity. Gut. 1995 Oct;37(4):565-567.
- Eltookhy A, Pearson NL. Drug-induced pancreatitis. Can Pharm J. 2006;139(6):58-60.
- Trivedi CD, Pitchumoni CS. Drug-induced pancreatitis: an update. J Clin Gastroenterol. 2005 Sept;39(8):709-716.
- Badalov N, Baradarian R, Iswara K, et al. Drug-induced pancreatitis: an evidence-based review. Clin Gastroenterol Hepatol. 2007 Jun;5(6):648-661.
- Vege SS, Chari ST. Etiology of acute pancreatitis. In: UpToDate, Rose, BD (Ed), UpToDate, Waltham, Mass., 2007.
- Skirvin A. Drug-induced pancreatitis. Aust Adv Drug Reactions Bull. 2006 Dec;25(6):22.
- American Gastroenterological Association Institute Medical Position Statement on Acute Pancreatitis. Gastroenterology. 1998 Sep;115(3):763-764.
In the Literature
In This Edition
- C-reactive protein levels predict death from cardiac causes after MI.
- SSRIs reduce risk for recurrent cardiac events in acute coronary syndrome.
- Vancomycin is as effective as metronidazole in routine treatment of C. difficile and superior in severe infection.
- Prevalence and severity of C. difficile are increasing in hospitalized patients in the U.S.
- Deviations in recommended enoxaparin dosing in NSTEMI result in worse outcomes.
- Most outpatient VTE events occur in recently hospitalized patients.
- Poor health literacy predicts mortality in older adults.
- A validated model predicts the risk for delirium at hospital discharge.
Do C-reactive Protein Levels Predict Death from Heart Failure?
Background: Ultra-sensitive quantitative assessment of C-reactive protein (CRP), a surrogate marker of systemic inflammation, has previously been shown to predict plaque instability in acute coronary syndromes. Data are lacking as to whether this blood test can also predict subsequent risk of heart failure or death on presentation in patients admitted for acute myocardial infarction (MI).
Study design: Prospec-tive observational study.
Setting: Olmstead County, Minn.
Synopsis: Ultra-sensitive quantitative serum CRP levels were obtained a median of 6.1 hours following onset of symptoms in 329 patients admitted with acute MI. The patients were stratified into tertiles based levels of CRP less than 3 mg/L, 3-15 mg/L, and more than 15 mg/L.
Tertiles were similar in respect to age, male-predominance, most cardiac risk factors, body mass index, and electrocardiographic (EKG) changes. However, there were statistically significant differences between groups, particularly the frequency of diabetes (10.7%, 31.2%, and 38.0%), previous MI history (2.7%, 4.6%, and 9.3%), Killip class greater than one (15.2%, 31.2%, and 39.8%), peak cardiac enzyme levels (both were higher in the bottom tertile, and lowest in the top tertile), and likelihood of significant comorbidities (lower likelihood in the bottom tertile, higher likelihood in the top tertile).
One-year survival was highly correlated with CRP tertile (93%, 84%, and 62% respectively). Once corrected for age, gender, peak cardiac enzymes, Killip class, coronary history, and recurring ischemic events, there remained a robust hazard ratio for heart failure and death at one year based on CRP tertile (1.00, 1.73, and 3.96, respectively).
Bottom line: Ultra-sensitive quantitative CRP levels obtained on admission for acute MI predict one-year risk for heart failure or death. The ability to generalize these results into clinical practice may be limited due to heterogeneity of the studied groups with a higher frequency of diabetes, prior coronary disease, and higher comorbidities in the group that had the highest CRP levels and thus more mortality and heart failure.
Citation: Bursi F, Weston SA, Killian JM, et al. C-reactive protein and heart failure after myocardial infarction in the community. Am J Med. 2007;120(7):616-622.
Do Selective Serotonin Reuptake Inhibitors Confer Cardiac Benefit?
Background: Selective serotonin reuptake inhibitors (SSRIs) theoretically lead to qualitative platelet dysfunction due to inhibition of serotonin-induced platelet activation (and thus resultant inhibition of platelet aggregation and vasoconstriction).
Study design: Retrospective observational study.
Setting: Large teaching hospital in Baltimore.
Synopsis: Of 1,254 patients admitted during the three-year study, 158 patients were on an SSRI at the time of admission. Of the remaining 1,096 patients, a cohort of 158 propensity-matched patients was identified who were statistically similar to the study group in all comorbidities (except for depression, which was higher in the SSRI group).
There were no statistically significant differences between the SSRI group and the propensity-matched group in regards to treatment for acute coronary syndrome (ACS). Almost all received aspirin (98.7% versus 99.4%), clopidogrel (95.6% versus 93.7%), unfractionated heparin (96.8% versus 99.4%), and a glycoprotein IIb/IIIa inhibitor (100% in both).
Patients in the SSRI group had a statistically lower incidence of minor adverse cardiac events (7.0% versus 13.9%), but had increased bleeding events (37.3% versus 26.6%). Minor cardiac events were defined as recurrent EKG findings of ischemia without resultant cardiac enzyme increase, new heart failure, or asymptomatic cardiac enzyme elevation without EKG changes.
Bottom line: Patients taking SSRIs when admitted with an ACS (for an unknown duration) appear to be at lower risk for minor cardiac complications compared with patients not taking an SSRI on admission. These patients also appear to be at elevated risk for bleeding in the setting of maximum antiplatelet and heparin therapy typical in management of ACS.
Citation: Ziegelstein RC, Meuchel J, Kim TJ, et al. Selective serotonin reuptake inhibitor use by patients with acute coronary syndromes. Am J Med. 2007;120(6):525-530.
When Is Vancomycin Superior in Treating C. difficile-Associated Diarrhea?
Background: Epidemic strains of C. difficile raise issues about which antibiotic treatment for C. difficile-associated diarrhea (CDAD) may be superior, particularly due to the availability of more potent antibiotics that can wipe out the protective flora of the intestinal tract.
Study design: Prospec-tive, randomized, double-blind, placebo-controlled trial over 7.5 years.
Setting: A teaching hospital in Chicago.
Synopsis: One hundred seventy-two patients with diarrhea were stratified into mild (fewer than two risks) or severe (two or more risks) disease groups within 48 hours of randomization. These patients were older than 60, with temperature greater than 38.3°C, albumin level lower than 2.5 mg/dL, or peripheral white blood count greater than 15,000 cells/mm. Patients requiring intensive care unit treatment or those with colonscopic evidence of pseudomembranous colitis received an additional risk score of two.
One hundred fifty patients completed the study, 71 in the vancomycin group (125 mg orally, four times a day) and 79 in the metronidazole group (250 mg orally, four times a day). Both groups were similar in composition and numbers of patients with mild and severe CDAD. Patients received placebo plus either vancomycin or metronidazole.
Cure was defined as resolution of diarrhea by day six of therapy and negative C. difficile toxin A assays on days six and 10 of therapy. Results were statistically similar in both treatment groups with mild disease (98% vancomycin versus 90% metronidazole), but favored vancomycin in severe disease (97% versus 76%).
Relapse were not statistically different in either group (7% versus 14%). An albumin level less than 2.5 mg/dL or the presence of colonoscopy-confirmed pseudomembranous colitis showed statistically significant correlation with metronidazole treatment failure (relative risks of 12.70 and 6.67, respectively).
Bottom line: Oral vancomycin, with its commensurate potential for inducing vancomycin-resistant Enterococcus, proved to be equally effective as metronidazole in treating mild CDAD. It was statistically superior to metronidazole in severe disease with hypoalbuminemia and pseudomembranous colitis predicting failure of metronidazole therapy.
Citation: Zar FA, Bakkanagari SR, Moorthi KM, et al. A comparison of vancomycin and metronidazole for the treatment of C. difficile-associated diarrhea, stratified by disease severity. Clin Infect Dis. 2007;45(3):302-307.
What Risk Factors Affect VTE Development in Outpatients?
Background: Decreasing lengths of stay have raised concern that treatments that previously would have continued during the longer hospital stays in the past, such as deep vein thrombosis prophylaxis, may result in unintended adverse consequences after discharge.
Study design: Retrospective observational study
Setting: Worcester, Mass., in 1999, 2001, and 2003, comprising residents who had diagnosis of venous thromboembolism (VTE) at any one of the 12 hospitals in the region
Synopsis: VTE was diagnosed in 1,897 residents (71.1%, 15.0% had pulmonary embolism [PE], and 13.9% had both). Further, 73.7% of the patients presented as an outpatient or were diagnosed within one day of hospital admission.
Compared with inpatients with VTE, outpatients were younger (63.3 years versus 67.4), were less likely to have had a recent infection (18.6% versus 46.8%), central venous catheter (10.4% versus 41.0%), recent fracture (7.3% versus 18.7%), heart failure (4.2% versus 16.5%), cardiac procedures (2.9% versus 7.8%), or recent intensive care unit care stay (8.7% versus 38.2%), but were more likely to have had a prior episode of VTE (19.9% versus 10.2%) or to be taking hormonal therapy (8.0% versus 3.0%).
The prevalence of malignancy was similar in both groups (29.0% versus 32.3%). Most outpatients diagnosed with VTE (59.9%) had been hospitalized in the preceding three months with a majority of VTEs diagnosed within 30 days of discharge. Only 59.7% of those previously hospitalized had any DVT prophylaxis (42.8% received anticoagulants, 16.9% had mechanical prophylaxis).
Bottom line: In an era of decreasing lengths of stay, the possible high level of outpatient VTE attributable to recent hospitalization may be at least partially due to inadequate inpatient pharmacologic VTE prophylaxis in more than 50% of the patients.
Citation: Spencer FA, Lessard D, Emery C, et al. Venous thromboembolism in the outpatient setting. Arch Intern Med. 2007;167(14):1471-1475.
How Has C. difficile Colitis Changed in Severity and Prevalence?
Background: Recent epidemic strains of Clostridium difficile have been reported with several studies suggesting that C. difficile infection has become more serious with risks for sepsis, colectomy, and death.
Study design: Cohort analysis of nationwide inpatient sample (NIS) discharge data for 11 years.
Synopsis: Of the more than 78 million discharge abstracts available for analysis, 299,453 patients were discharged with either a principle or secondary diagnosis of Clostridium difficile colitis (CDC). Demographics trends comparing the early period (1993-1996) versus the middle period (1997-2000) versus the late period (2001-2003) showed CDC incidence:
- Increased in older groups (65.6 years, 66.9 years, 67.6 years);
- Decreased in females (59.8%, 59.1%, 58.9%); and
- Decreased in Caucasians (70.90%, 67.20%, 59.10%).
From 1993 to 2003, the prevalence of CDC discharge diagnoses increased from 261 to 546 cases per 100,000; the colectomy rate due to CDC increased from 1.2 up to 3.4 per 1000, and the case fatality rate statistically significantly increased from 7.84% to 9.26%.
Bottom line: Despite the limitations of using discharge coding abstracts, this study confirms the significantly increasing prevalence (particularly in older, non-Caucasian men) and severity of CDC over the previous decade. This has resulted in a higher incidence of colectomy and death.
Citation: Ricciardi R, Rothenberger DA, Madoff RD. Increasing prevalence and severity of Clostridium difficile colitis in hospitalized patients in the United States. Arch Surg. 2007;142(7):624-631.
How Often Do Clinicians Deviate from Recommended Enoxaparin Doses?
Background: Low molecular heparins have been increasingly utilized in the setting of non-ST-segment elevation myocardial infarctions (NSTEMI) in place of unfractionated heparin. They require careful dose adjustment to ensure appropriate therapeutic effect and prevent bleeding and thrombotic complications.
Study design: Retrospective observational cohort study.
Setting: Medical centers throughout the U.S. that participated in the Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the ACC/AHA Guidelines (CRUSADE) initiative.
Synopsis: A total of 10,687 patients from 332 hospitals received enoxaparin for NSTEMI as part of CRUSADE. Patients were stratified by whether they received:
- The recommended dose of enoxaparin (1 mg/kg twice daily for glomerular filtration rate (GFR) more than 30 mL/min versus 0.5 mg/kg twice daily for estimated GFR of 30 mL/min or less; 52.1%);
- An excess dose (more than 10 mg/day over recommended dose; 18.7%); or
- A lower-than-recommended dose (more than 10 mg/day less than the recommended dose; 29.2%).
Those receiving an excess dose were more likely to be older, have lower body-mass indexes (BMI), weigh less, be female, have estimated GFRs less than 60 mL/min, and smoke. Those receiving less-than-recommended dosing were more likely to have a higher BMI, weigh more, and be male. Major bleeding episodes (14.2%) and deaths (5.6%) were more common statistically in the excess dose group compared with the recommended dose group (7.3% and 2.4%, respectively). Deaths, but not bleeding, also were higher in the lower-than-recommended dose group (3.3% versus 2.4%).
Bottom line: A little more than half of patients received the correct dose of enoxaparin in NSTEMIs. Those who received too high a dose had marked increases in risk of bleeding and death, and those receiving subtherapeutic doses suffered increased mortality.
Citation: LaPointe NMA, Chen AY, Alexander KP, et al. Enoxaparin dosing and associated risk of in-hospital bleeding and death in patients with non-ST-segment elevation acute coronary syndromes. Arch Intern Med. 2007;167(14):1539-1344.
Does Poor Health Literacy Predict Mortality?
Background: Prior studies have shown increased hospitalization rates in patients with poor health literacy (e.g., inability to comprehend prescriptions or educational materials). At least one study has shown an increase in mortality in 70-to-79-year-olds with impaired health literacy.
Study design: Prospective cohort study.
Setting: Four U.S. metropolitan areas.
Synopsis: Poor health literacy predicts patients’ inability to understand basic health information, such as prescription information, drug dosing intervals, or follow-up schedules. In 1997, 3,260 patients age 65 or older were included in the study, which used a face-to-face standardized test to quantify health literacy.
Patients were tracked via the National Death Index through 2003. Patients were stratified as having adequate, marginal, or inadequate health literacy (64.2%, 11.2%, and 24.5% of patients, respectively). Marginal and inadequate health literacy were strongly associated with increasing age, African American race, lower incomes, lower levels of education, worse physical and mental health, limitations in activities of daily living (ADLs), and lower BMIs. These patients were also less likely to perform vigorous exercise, and less likely to have smoked or used alcohol.
Health literacy (adequate, marginal, or inadequate) predicted unadjusted mortality rates (18.9%, 28.7%, and 39.4%, respectively). Adjusting for socioeconomic status, demographics, and baseline health, all-cause mortality hazard ratios of marginal and inadequate literacy (compared with adequate health literacy) were 1.13 (0.90-1.41 not statistically significant) and 1.52 (1.26-1.83, statistically significant).
Bottom line: Limited data exists regarding how to improve health literacy, and there is no easy bedside test to identify patients with varying levels of literacy. But there appears to be a strong, independent correlation to health literacy and mortality. Physicians need to remain vigilant in their patients’ understanding of their disease, treatment, and follow-up.
Citation: Baker DW, Wolf MS, Feinglass J, et al. Health literacy and mortality among elderly persons. Arch Intern Med. 2007;167(14):1503-1509.
Which Factors Predict Delirium at Discharge?
Background: Delirium at hospital discharge, which can persist for months following hospitalization, may be a contributing factor to dementia, results in increased medical errors during the traditionally high-risk period between discharge and follow-up. Further, it results in serious complications, and, if unrecognized, a high mortality rate.
Study design: Prospective validation model.
Synopsis: A model to predict delirium at hospital discharge was studied in a development cohort of 491 patients age 70 or older who had no evidence of delirium on admission. Of twenty-two different candidate factors, five factors correlated with high odds ratios of delirium at discharge in the 106 (21.6%) of those in the study group who developed delirium: dementia, vision impairment, inability to perform more than one ADL, multiple comorbidities (based on a Charlson score of four or more), and restraint use during delirium.
Patients were stratified into low-risk (zero-one factors), intermediate risk (two-three factors), or high risk (four or more factors) for delirium at hospital discharge. Relative risks (RR) for each group were 1, 4.4, and 15.3, respectively; RR for nursing home placement or death (NHPOD) at one year was 1, 2.4, and 3.4, respectively. A validation cohort of 461 statistically similar patients showed RR for development in the low-, intermediate-, and high-risk groups of 1, 5.4, 10.2, respectively; and RR at one year for NHPOD was 1, 2.7, and 4.4, respectively.
Bottom line: Dementia, vision impairment, inability to perform at least one ADL, multiple comorbidities, and use of restraints are risk factors that can stratify patients into low, intermediate, and high risk for delirium at hospital discharge. Commensurate risks exist for nursing home placement or death at one year.
Citation: Inouye SK, Zhang Y, Jones RN. Risk factors for delirium at discharge. Arch Intern Med. 2007;167(13):1406-1413.
In This Edition
- C-reactive protein levels predict death from cardiac causes after MI.
- SSRIs reduce risk for recurrent cardiac events in acute coronary syndrome.
- Vancomycin is as effective as metronidazole in routine treatment of C. difficile and superior in severe infection.
- Prevalence and severity of C. difficile are increasing in hospitalized patients in the U.S.
- Deviations in recommended enoxaparin dosing in NSTEMI result in worse outcomes.
- Most outpatient VTE events occur in recently hospitalized patients.
- Poor health literacy predicts mortality in older adults.
- A validated model predicts the risk for delirium at hospital discharge.
Do C-reactive Protein Levels Predict Death from Heart Failure?
Background: Ultra-sensitive quantitative assessment of C-reactive protein (CRP), a surrogate marker of systemic inflammation, has previously been shown to predict plaque instability in acute coronary syndromes. Data are lacking as to whether this blood test can also predict subsequent risk of heart failure or death on presentation in patients admitted for acute myocardial infarction (MI).
Study design: Prospec-tive observational study.
Setting: Olmstead County, Minn.
Synopsis: Ultra-sensitive quantitative serum CRP levels were obtained a median of 6.1 hours following onset of symptoms in 329 patients admitted with acute MI. The patients were stratified into tertiles based levels of CRP less than 3 mg/L, 3-15 mg/L, and more than 15 mg/L.
Tertiles were similar in respect to age, male-predominance, most cardiac risk factors, body mass index, and electrocardiographic (EKG) changes. However, there were statistically significant differences between groups, particularly the frequency of diabetes (10.7%, 31.2%, and 38.0%), previous MI history (2.7%, 4.6%, and 9.3%), Killip class greater than one (15.2%, 31.2%, and 39.8%), peak cardiac enzyme levels (both were higher in the bottom tertile, and lowest in the top tertile), and likelihood of significant comorbidities (lower likelihood in the bottom tertile, higher likelihood in the top tertile).
One-year survival was highly correlated with CRP tertile (93%, 84%, and 62% respectively). Once corrected for age, gender, peak cardiac enzymes, Killip class, coronary history, and recurring ischemic events, there remained a robust hazard ratio for heart failure and death at one year based on CRP tertile (1.00, 1.73, and 3.96, respectively).
Bottom line: Ultra-sensitive quantitative CRP levels obtained on admission for acute MI predict one-year risk for heart failure or death. The ability to generalize these results into clinical practice may be limited due to heterogeneity of the studied groups with a higher frequency of diabetes, prior coronary disease, and higher comorbidities in the group that had the highest CRP levels and thus more mortality and heart failure.
Citation: Bursi F, Weston SA, Killian JM, et al. C-reactive protein and heart failure after myocardial infarction in the community. Am J Med. 2007;120(7):616-622.
Do Selective Serotonin Reuptake Inhibitors Confer Cardiac Benefit?
Background: Selective serotonin reuptake inhibitors (SSRIs) theoretically lead to qualitative platelet dysfunction due to inhibition of serotonin-induced platelet activation (and thus resultant inhibition of platelet aggregation and vasoconstriction).
Study design: Retrospective observational study.
Setting: Large teaching hospital in Baltimore.
Synopsis: Of 1,254 patients admitted during the three-year study, 158 patients were on an SSRI at the time of admission. Of the remaining 1,096 patients, a cohort of 158 propensity-matched patients was identified who were statistically similar to the study group in all comorbidities (except for depression, which was higher in the SSRI group).
There were no statistically significant differences between the SSRI group and the propensity-matched group in regards to treatment for acute coronary syndrome (ACS). Almost all received aspirin (98.7% versus 99.4%), clopidogrel (95.6% versus 93.7%), unfractionated heparin (96.8% versus 99.4%), and a glycoprotein IIb/IIIa inhibitor (100% in both).
Patients in the SSRI group had a statistically lower incidence of minor adverse cardiac events (7.0% versus 13.9%), but had increased bleeding events (37.3% versus 26.6%). Minor cardiac events were defined as recurrent EKG findings of ischemia without resultant cardiac enzyme increase, new heart failure, or asymptomatic cardiac enzyme elevation without EKG changes.
Bottom line: Patients taking SSRIs when admitted with an ACS (for an unknown duration) appear to be at lower risk for minor cardiac complications compared with patients not taking an SSRI on admission. These patients also appear to be at elevated risk for bleeding in the setting of maximum antiplatelet and heparin therapy typical in management of ACS.
Citation: Ziegelstein RC, Meuchel J, Kim TJ, et al. Selective serotonin reuptake inhibitor use by patients with acute coronary syndromes. Am J Med. 2007;120(6):525-530.
When Is Vancomycin Superior in Treating C. difficile-Associated Diarrhea?
Background: Epidemic strains of C. difficile raise issues about which antibiotic treatment for C. difficile-associated diarrhea (CDAD) may be superior, particularly due to the availability of more potent antibiotics that can wipe out the protective flora of the intestinal tract.
Study design: Prospec-tive, randomized, double-blind, placebo-controlled trial over 7.5 years.
Setting: A teaching hospital in Chicago.
Synopsis: One hundred seventy-two patients with diarrhea were stratified into mild (fewer than two risks) or severe (two or more risks) disease groups within 48 hours of randomization. These patients were older than 60, with temperature greater than 38.3°C, albumin level lower than 2.5 mg/dL, or peripheral white blood count greater than 15,000 cells/mm. Patients requiring intensive care unit treatment or those with colonscopic evidence of pseudomembranous colitis received an additional risk score of two.
One hundred fifty patients completed the study, 71 in the vancomycin group (125 mg orally, four times a day) and 79 in the metronidazole group (250 mg orally, four times a day). Both groups were similar in composition and numbers of patients with mild and severe CDAD. Patients received placebo plus either vancomycin or metronidazole.
Cure was defined as resolution of diarrhea by day six of therapy and negative C. difficile toxin A assays on days six and 10 of therapy. Results were statistically similar in both treatment groups with mild disease (98% vancomycin versus 90% metronidazole), but favored vancomycin in severe disease (97% versus 76%).
Relapse were not statistically different in either group (7% versus 14%). An albumin level less than 2.5 mg/dL or the presence of colonoscopy-confirmed pseudomembranous colitis showed statistically significant correlation with metronidazole treatment failure (relative risks of 12.70 and 6.67, respectively).
Bottom line: Oral vancomycin, with its commensurate potential for inducing vancomycin-resistant Enterococcus, proved to be equally effective as metronidazole in treating mild CDAD. It was statistically superior to metronidazole in severe disease with hypoalbuminemia and pseudomembranous colitis predicting failure of metronidazole therapy.
Citation: Zar FA, Bakkanagari SR, Moorthi KM, et al. A comparison of vancomycin and metronidazole for the treatment of C. difficile-associated diarrhea, stratified by disease severity. Clin Infect Dis. 2007;45(3):302-307.
What Risk Factors Affect VTE Development in Outpatients?
Background: Decreasing lengths of stay have raised concern that treatments that previously would have continued during the longer hospital stays in the past, such as deep vein thrombosis prophylaxis, may result in unintended adverse consequences after discharge.
Study design: Retrospective observational study
Setting: Worcester, Mass., in 1999, 2001, and 2003, comprising residents who had diagnosis of venous thromboembolism (VTE) at any one of the 12 hospitals in the region
Synopsis: VTE was diagnosed in 1,897 residents (71.1%, 15.0% had pulmonary embolism [PE], and 13.9% had both). Further, 73.7% of the patients presented as an outpatient or were diagnosed within one day of hospital admission.
Compared with inpatients with VTE, outpatients were younger (63.3 years versus 67.4), were less likely to have had a recent infection (18.6% versus 46.8%), central venous catheter (10.4% versus 41.0%), recent fracture (7.3% versus 18.7%), heart failure (4.2% versus 16.5%), cardiac procedures (2.9% versus 7.8%), or recent intensive care unit care stay (8.7% versus 38.2%), but were more likely to have had a prior episode of VTE (19.9% versus 10.2%) or to be taking hormonal therapy (8.0% versus 3.0%).
The prevalence of malignancy was similar in both groups (29.0% versus 32.3%). Most outpatients diagnosed with VTE (59.9%) had been hospitalized in the preceding three months with a majority of VTEs diagnosed within 30 days of discharge. Only 59.7% of those previously hospitalized had any DVT prophylaxis (42.8% received anticoagulants, 16.9% had mechanical prophylaxis).
Bottom line: In an era of decreasing lengths of stay, the possible high level of outpatient VTE attributable to recent hospitalization may be at least partially due to inadequate inpatient pharmacologic VTE prophylaxis in more than 50% of the patients.
Citation: Spencer FA, Lessard D, Emery C, et al. Venous thromboembolism in the outpatient setting. Arch Intern Med. 2007;167(14):1471-1475.
How Has C. difficile Colitis Changed in Severity and Prevalence?
Background: Recent epidemic strains of Clostridium difficile have been reported with several studies suggesting that C. difficile infection has become more serious with risks for sepsis, colectomy, and death.
Study design: Cohort analysis of nationwide inpatient sample (NIS) discharge data for 11 years.
Synopsis: Of the more than 78 million discharge abstracts available for analysis, 299,453 patients were discharged with either a principle or secondary diagnosis of Clostridium difficile colitis (CDC). Demographics trends comparing the early period (1993-1996) versus the middle period (1997-2000) versus the late period (2001-2003) showed CDC incidence:
- Increased in older groups (65.6 years, 66.9 years, 67.6 years);
- Decreased in females (59.8%, 59.1%, 58.9%); and
- Decreased in Caucasians (70.90%, 67.20%, 59.10%).
From 1993 to 2003, the prevalence of CDC discharge diagnoses increased from 261 to 546 cases per 100,000; the colectomy rate due to CDC increased from 1.2 up to 3.4 per 1000, and the case fatality rate statistically significantly increased from 7.84% to 9.26%.
Bottom line: Despite the limitations of using discharge coding abstracts, this study confirms the significantly increasing prevalence (particularly in older, non-Caucasian men) and severity of CDC over the previous decade. This has resulted in a higher incidence of colectomy and death.
Citation: Ricciardi R, Rothenberger DA, Madoff RD. Increasing prevalence and severity of Clostridium difficile colitis in hospitalized patients in the United States. Arch Surg. 2007;142(7):624-631.
How Often Do Clinicians Deviate from Recommended Enoxaparin Doses?
Background: Low molecular heparins have been increasingly utilized in the setting of non-ST-segment elevation myocardial infarctions (NSTEMI) in place of unfractionated heparin. They require careful dose adjustment to ensure appropriate therapeutic effect and prevent bleeding and thrombotic complications.
Study design: Retrospective observational cohort study.
Setting: Medical centers throughout the U.S. that participated in the Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the ACC/AHA Guidelines (CRUSADE) initiative.
Synopsis: A total of 10,687 patients from 332 hospitals received enoxaparin for NSTEMI as part of CRUSADE. Patients were stratified by whether they received:
- The recommended dose of enoxaparin (1 mg/kg twice daily for glomerular filtration rate (GFR) more than 30 mL/min versus 0.5 mg/kg twice daily for estimated GFR of 30 mL/min or less; 52.1%);
- An excess dose (more than 10 mg/day over recommended dose; 18.7%); or
- A lower-than-recommended dose (more than 10 mg/day less than the recommended dose; 29.2%).
Those receiving an excess dose were more likely to be older, have lower body-mass indexes (BMI), weigh less, be female, have estimated GFRs less than 60 mL/min, and smoke. Those receiving less-than-recommended dosing were more likely to have a higher BMI, weigh more, and be male. Major bleeding episodes (14.2%) and deaths (5.6%) were more common statistically in the excess dose group compared with the recommended dose group (7.3% and 2.4%, respectively). Deaths, but not bleeding, also were higher in the lower-than-recommended dose group (3.3% versus 2.4%).
Bottom line: A little more than half of patients received the correct dose of enoxaparin in NSTEMIs. Those who received too high a dose had marked increases in risk of bleeding and death, and those receiving subtherapeutic doses suffered increased mortality.
Citation: LaPointe NMA, Chen AY, Alexander KP, et al. Enoxaparin dosing and associated risk of in-hospital bleeding and death in patients with non-ST-segment elevation acute coronary syndromes. Arch Intern Med. 2007;167(14):1539-1344.
Does Poor Health Literacy Predict Mortality?
Background: Prior studies have shown increased hospitalization rates in patients with poor health literacy (e.g., inability to comprehend prescriptions or educational materials). At least one study has shown an increase in mortality in 70-to-79-year-olds with impaired health literacy.
Study design: Prospective cohort study.
Setting: Four U.S. metropolitan areas.
Synopsis: Poor health literacy predicts patients’ inability to understand basic health information, such as prescription information, drug dosing intervals, or follow-up schedules. In 1997, 3,260 patients age 65 or older were included in the study, which used a face-to-face standardized test to quantify health literacy.
Patients were tracked via the National Death Index through 2003. Patients were stratified as having adequate, marginal, or inadequate health literacy (64.2%, 11.2%, and 24.5% of patients, respectively). Marginal and inadequate health literacy were strongly associated with increasing age, African American race, lower incomes, lower levels of education, worse physical and mental health, limitations in activities of daily living (ADLs), and lower BMIs. These patients were also less likely to perform vigorous exercise, and less likely to have smoked or used alcohol.
Health literacy (adequate, marginal, or inadequate) predicted unadjusted mortality rates (18.9%, 28.7%, and 39.4%, respectively). Adjusting for socioeconomic status, demographics, and baseline health, all-cause mortality hazard ratios of marginal and inadequate literacy (compared with adequate health literacy) were 1.13 (0.90-1.41 not statistically significant) and 1.52 (1.26-1.83, statistically significant).
Bottom line: Limited data exists regarding how to improve health literacy, and there is no easy bedside test to identify patients with varying levels of literacy. But there appears to be a strong, independent correlation to health literacy and mortality. Physicians need to remain vigilant in their patients’ understanding of their disease, treatment, and follow-up.
Citation: Baker DW, Wolf MS, Feinglass J, et al. Health literacy and mortality among elderly persons. Arch Intern Med. 2007;167(14):1503-1509.
Which Factors Predict Delirium at Discharge?
Background: Delirium at hospital discharge, which can persist for months following hospitalization, may be a contributing factor to dementia, results in increased medical errors during the traditionally high-risk period between discharge and follow-up. Further, it results in serious complications, and, if unrecognized, a high mortality rate.
Study design: Prospective validation model.
Synopsis: A model to predict delirium at hospital discharge was studied in a development cohort of 491 patients age 70 or older who had no evidence of delirium on admission. Of twenty-two different candidate factors, five factors correlated with high odds ratios of delirium at discharge in the 106 (21.6%) of those in the study group who developed delirium: dementia, vision impairment, inability to perform more than one ADL, multiple comorbidities (based on a Charlson score of four or more), and restraint use during delirium.
Patients were stratified into low-risk (zero-one factors), intermediate risk (two-three factors), or high risk (four or more factors) for delirium at hospital discharge. Relative risks (RR) for each group were 1, 4.4, and 15.3, respectively; RR for nursing home placement or death (NHPOD) at one year was 1, 2.4, and 3.4, respectively. A validation cohort of 461 statistically similar patients showed RR for development in the low-, intermediate-, and high-risk groups of 1, 5.4, 10.2, respectively; and RR at one year for NHPOD was 1, 2.7, and 4.4, respectively.
Bottom line: Dementia, vision impairment, inability to perform at least one ADL, multiple comorbidities, and use of restraints are risk factors that can stratify patients into low, intermediate, and high risk for delirium at hospital discharge. Commensurate risks exist for nursing home placement or death at one year.
Citation: Inouye SK, Zhang Y, Jones RN. Risk factors for delirium at discharge. Arch Intern Med. 2007;167(13):1406-1413.
In This Edition
- C-reactive protein levels predict death from cardiac causes after MI.
- SSRIs reduce risk for recurrent cardiac events in acute coronary syndrome.
- Vancomycin is as effective as metronidazole in routine treatment of C. difficile and superior in severe infection.
- Prevalence and severity of C. difficile are increasing in hospitalized patients in the U.S.
- Deviations in recommended enoxaparin dosing in NSTEMI result in worse outcomes.
- Most outpatient VTE events occur in recently hospitalized patients.
- Poor health literacy predicts mortality in older adults.
- A validated model predicts the risk for delirium at hospital discharge.
Do C-reactive Protein Levels Predict Death from Heart Failure?
Background: Ultra-sensitive quantitative assessment of C-reactive protein (CRP), a surrogate marker of systemic inflammation, has previously been shown to predict plaque instability in acute coronary syndromes. Data are lacking as to whether this blood test can also predict subsequent risk of heart failure or death on presentation in patients admitted for acute myocardial infarction (MI).
Study design: Prospec-tive observational study.
Setting: Olmstead County, Minn.
Synopsis: Ultra-sensitive quantitative serum CRP levels were obtained a median of 6.1 hours following onset of symptoms in 329 patients admitted with acute MI. The patients were stratified into tertiles based levels of CRP less than 3 mg/L, 3-15 mg/L, and more than 15 mg/L.
Tertiles were similar in respect to age, male-predominance, most cardiac risk factors, body mass index, and electrocardiographic (EKG) changes. However, there were statistically significant differences between groups, particularly the frequency of diabetes (10.7%, 31.2%, and 38.0%), previous MI history (2.7%, 4.6%, and 9.3%), Killip class greater than one (15.2%, 31.2%, and 39.8%), peak cardiac enzyme levels (both were higher in the bottom tertile, and lowest in the top tertile), and likelihood of significant comorbidities (lower likelihood in the bottom tertile, higher likelihood in the top tertile).
One-year survival was highly correlated with CRP tertile (93%, 84%, and 62% respectively). Once corrected for age, gender, peak cardiac enzymes, Killip class, coronary history, and recurring ischemic events, there remained a robust hazard ratio for heart failure and death at one year based on CRP tertile (1.00, 1.73, and 3.96, respectively).
Bottom line: Ultra-sensitive quantitative CRP levels obtained on admission for acute MI predict one-year risk for heart failure or death. The ability to generalize these results into clinical practice may be limited due to heterogeneity of the studied groups with a higher frequency of diabetes, prior coronary disease, and higher comorbidities in the group that had the highest CRP levels and thus more mortality and heart failure.
Citation: Bursi F, Weston SA, Killian JM, et al. C-reactive protein and heart failure after myocardial infarction in the community. Am J Med. 2007;120(7):616-622.
Do Selective Serotonin Reuptake Inhibitors Confer Cardiac Benefit?
Background: Selective serotonin reuptake inhibitors (SSRIs) theoretically lead to qualitative platelet dysfunction due to inhibition of serotonin-induced platelet activation (and thus resultant inhibition of platelet aggregation and vasoconstriction).
Study design: Retrospective observational study.
Setting: Large teaching hospital in Baltimore.
Synopsis: Of 1,254 patients admitted during the three-year study, 158 patients were on an SSRI at the time of admission. Of the remaining 1,096 patients, a cohort of 158 propensity-matched patients was identified who were statistically similar to the study group in all comorbidities (except for depression, which was higher in the SSRI group).
There were no statistically significant differences between the SSRI group and the propensity-matched group in regards to treatment for acute coronary syndrome (ACS). Almost all received aspirin (98.7% versus 99.4%), clopidogrel (95.6% versus 93.7%), unfractionated heparin (96.8% versus 99.4%), and a glycoprotein IIb/IIIa inhibitor (100% in both).
Patients in the SSRI group had a statistically lower incidence of minor adverse cardiac events (7.0% versus 13.9%), but had increased bleeding events (37.3% versus 26.6%). Minor cardiac events were defined as recurrent EKG findings of ischemia without resultant cardiac enzyme increase, new heart failure, or asymptomatic cardiac enzyme elevation without EKG changes.
Bottom line: Patients taking SSRIs when admitted with an ACS (for an unknown duration) appear to be at lower risk for minor cardiac complications compared with patients not taking an SSRI on admission. These patients also appear to be at elevated risk for bleeding in the setting of maximum antiplatelet and heparin therapy typical in management of ACS.
Citation: Ziegelstein RC, Meuchel J, Kim TJ, et al. Selective serotonin reuptake inhibitor use by patients with acute coronary syndromes. Am J Med. 2007;120(6):525-530.
When Is Vancomycin Superior in Treating C. difficile-Associated Diarrhea?
Background: Epidemic strains of C. difficile raise issues about which antibiotic treatment for C. difficile-associated diarrhea (CDAD) may be superior, particularly due to the availability of more potent antibiotics that can wipe out the protective flora of the intestinal tract.
Study design: Prospec-tive, randomized, double-blind, placebo-controlled trial over 7.5 years.
Setting: A teaching hospital in Chicago.
Synopsis: One hundred seventy-two patients with diarrhea were stratified into mild (fewer than two risks) or severe (two or more risks) disease groups within 48 hours of randomization. These patients were older than 60, with temperature greater than 38.3°C, albumin level lower than 2.5 mg/dL, or peripheral white blood count greater than 15,000 cells/mm. Patients requiring intensive care unit treatment or those with colonscopic evidence of pseudomembranous colitis received an additional risk score of two.
One hundred fifty patients completed the study, 71 in the vancomycin group (125 mg orally, four times a day) and 79 in the metronidazole group (250 mg orally, four times a day). Both groups were similar in composition and numbers of patients with mild and severe CDAD. Patients received placebo plus either vancomycin or metronidazole.
Cure was defined as resolution of diarrhea by day six of therapy and negative C. difficile toxin A assays on days six and 10 of therapy. Results were statistically similar in both treatment groups with mild disease (98% vancomycin versus 90% metronidazole), but favored vancomycin in severe disease (97% versus 76%).
Relapse were not statistically different in either group (7% versus 14%). An albumin level less than 2.5 mg/dL or the presence of colonoscopy-confirmed pseudomembranous colitis showed statistically significant correlation with metronidazole treatment failure (relative risks of 12.70 and 6.67, respectively).
Bottom line: Oral vancomycin, with its commensurate potential for inducing vancomycin-resistant Enterococcus, proved to be equally effective as metronidazole in treating mild CDAD. It was statistically superior to metronidazole in severe disease with hypoalbuminemia and pseudomembranous colitis predicting failure of metronidazole therapy.
Citation: Zar FA, Bakkanagari SR, Moorthi KM, et al. A comparison of vancomycin and metronidazole for the treatment of C. difficile-associated diarrhea, stratified by disease severity. Clin Infect Dis. 2007;45(3):302-307.
What Risk Factors Affect VTE Development in Outpatients?
Background: Decreasing lengths of stay have raised concern that treatments that previously would have continued during the longer hospital stays in the past, such as deep vein thrombosis prophylaxis, may result in unintended adverse consequences after discharge.
Study design: Retrospective observational study
Setting: Worcester, Mass., in 1999, 2001, and 2003, comprising residents who had diagnosis of venous thromboembolism (VTE) at any one of the 12 hospitals in the region
Synopsis: VTE was diagnosed in 1,897 residents (71.1%, 15.0% had pulmonary embolism [PE], and 13.9% had both). Further, 73.7% of the patients presented as an outpatient or were diagnosed within one day of hospital admission.
Compared with inpatients with VTE, outpatients were younger (63.3 years versus 67.4), were less likely to have had a recent infection (18.6% versus 46.8%), central venous catheter (10.4% versus 41.0%), recent fracture (7.3% versus 18.7%), heart failure (4.2% versus 16.5%), cardiac procedures (2.9% versus 7.8%), or recent intensive care unit care stay (8.7% versus 38.2%), but were more likely to have had a prior episode of VTE (19.9% versus 10.2%) or to be taking hormonal therapy (8.0% versus 3.0%).
The prevalence of malignancy was similar in both groups (29.0% versus 32.3%). Most outpatients diagnosed with VTE (59.9%) had been hospitalized in the preceding three months with a majority of VTEs diagnosed within 30 days of discharge. Only 59.7% of those previously hospitalized had any DVT prophylaxis (42.8% received anticoagulants, 16.9% had mechanical prophylaxis).
Bottom line: In an era of decreasing lengths of stay, the possible high level of outpatient VTE attributable to recent hospitalization may be at least partially due to inadequate inpatient pharmacologic VTE prophylaxis in more than 50% of the patients.
Citation: Spencer FA, Lessard D, Emery C, et al. Venous thromboembolism in the outpatient setting. Arch Intern Med. 2007;167(14):1471-1475.
How Has C. difficile Colitis Changed in Severity and Prevalence?
Background: Recent epidemic strains of Clostridium difficile have been reported with several studies suggesting that C. difficile infection has become more serious with risks for sepsis, colectomy, and death.
Study design: Cohort analysis of nationwide inpatient sample (NIS) discharge data for 11 years.
Synopsis: Of the more than 78 million discharge abstracts available for analysis, 299,453 patients were discharged with either a principle or secondary diagnosis of Clostridium difficile colitis (CDC). Demographics trends comparing the early period (1993-1996) versus the middle period (1997-2000) versus the late period (2001-2003) showed CDC incidence:
- Increased in older groups (65.6 years, 66.9 years, 67.6 years);
- Decreased in females (59.8%, 59.1%, 58.9%); and
- Decreased in Caucasians (70.90%, 67.20%, 59.10%).
From 1993 to 2003, the prevalence of CDC discharge diagnoses increased from 261 to 546 cases per 100,000; the colectomy rate due to CDC increased from 1.2 up to 3.4 per 1000, and the case fatality rate statistically significantly increased from 7.84% to 9.26%.
Bottom line: Despite the limitations of using discharge coding abstracts, this study confirms the significantly increasing prevalence (particularly in older, non-Caucasian men) and severity of CDC over the previous decade. This has resulted in a higher incidence of colectomy and death.
Citation: Ricciardi R, Rothenberger DA, Madoff RD. Increasing prevalence and severity of Clostridium difficile colitis in hospitalized patients in the United States. Arch Surg. 2007;142(7):624-631.
How Often Do Clinicians Deviate from Recommended Enoxaparin Doses?
Background: Low molecular heparins have been increasingly utilized in the setting of non-ST-segment elevation myocardial infarctions (NSTEMI) in place of unfractionated heparin. They require careful dose adjustment to ensure appropriate therapeutic effect and prevent bleeding and thrombotic complications.
Study design: Retrospective observational cohort study.
Setting: Medical centers throughout the U.S. that participated in the Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the ACC/AHA Guidelines (CRUSADE) initiative.
Synopsis: A total of 10,687 patients from 332 hospitals received enoxaparin for NSTEMI as part of CRUSADE. Patients were stratified by whether they received:
- The recommended dose of enoxaparin (1 mg/kg twice daily for glomerular filtration rate (GFR) more than 30 mL/min versus 0.5 mg/kg twice daily for estimated GFR of 30 mL/min or less; 52.1%);
- An excess dose (more than 10 mg/day over recommended dose; 18.7%); or
- A lower-than-recommended dose (more than 10 mg/day less than the recommended dose; 29.2%).
Those receiving an excess dose were more likely to be older, have lower body-mass indexes (BMI), weigh less, be female, have estimated GFRs less than 60 mL/min, and smoke. Those receiving less-than-recommended dosing were more likely to have a higher BMI, weigh more, and be male. Major bleeding episodes (14.2%) and deaths (5.6%) were more common statistically in the excess dose group compared with the recommended dose group (7.3% and 2.4%, respectively). Deaths, but not bleeding, also were higher in the lower-than-recommended dose group (3.3% versus 2.4%).
Bottom line: A little more than half of patients received the correct dose of enoxaparin in NSTEMIs. Those who received too high a dose had marked increases in risk of bleeding and death, and those receiving subtherapeutic doses suffered increased mortality.
Citation: LaPointe NMA, Chen AY, Alexander KP, et al. Enoxaparin dosing and associated risk of in-hospital bleeding and death in patients with non-ST-segment elevation acute coronary syndromes. Arch Intern Med. 2007;167(14):1539-1344.
Does Poor Health Literacy Predict Mortality?
Background: Prior studies have shown increased hospitalization rates in patients with poor health literacy (e.g., inability to comprehend prescriptions or educational materials). At least one study has shown an increase in mortality in 70-to-79-year-olds with impaired health literacy.
Study design: Prospective cohort study.
Setting: Four U.S. metropolitan areas.
Synopsis: Poor health literacy predicts patients’ inability to understand basic health information, such as prescription information, drug dosing intervals, or follow-up schedules. In 1997, 3,260 patients age 65 or older were included in the study, which used a face-to-face standardized test to quantify health literacy.
Patients were tracked via the National Death Index through 2003. Patients were stratified as having adequate, marginal, or inadequate health literacy (64.2%, 11.2%, and 24.5% of patients, respectively). Marginal and inadequate health literacy were strongly associated with increasing age, African American race, lower incomes, lower levels of education, worse physical and mental health, limitations in activities of daily living (ADLs), and lower BMIs. These patients were also less likely to perform vigorous exercise, and less likely to have smoked or used alcohol.
Health literacy (adequate, marginal, or inadequate) predicted unadjusted mortality rates (18.9%, 28.7%, and 39.4%, respectively). Adjusting for socioeconomic status, demographics, and baseline health, all-cause mortality hazard ratios of marginal and inadequate literacy (compared with adequate health literacy) were 1.13 (0.90-1.41 not statistically significant) and 1.52 (1.26-1.83, statistically significant).
Bottom line: Limited data exists regarding how to improve health literacy, and there is no easy bedside test to identify patients with varying levels of literacy. But there appears to be a strong, independent correlation to health literacy and mortality. Physicians need to remain vigilant in their patients’ understanding of their disease, treatment, and follow-up.
Citation: Baker DW, Wolf MS, Feinglass J, et al. Health literacy and mortality among elderly persons. Arch Intern Med. 2007;167(14):1503-1509.
Which Factors Predict Delirium at Discharge?
Background: Delirium at hospital discharge, which can persist for months following hospitalization, may be a contributing factor to dementia, results in increased medical errors during the traditionally high-risk period between discharge and follow-up. Further, it results in serious complications, and, if unrecognized, a high mortality rate.
Study design: Prospective validation model.
Synopsis: A model to predict delirium at hospital discharge was studied in a development cohort of 491 patients age 70 or older who had no evidence of delirium on admission. Of twenty-two different candidate factors, five factors correlated with high odds ratios of delirium at discharge in the 106 (21.6%) of those in the study group who developed delirium: dementia, vision impairment, inability to perform more than one ADL, multiple comorbidities (based on a Charlson score of four or more), and restraint use during delirium.
Patients were stratified into low-risk (zero-one factors), intermediate risk (two-three factors), or high risk (four or more factors) for delirium at hospital discharge. Relative risks (RR) for each group were 1, 4.4, and 15.3, respectively; RR for nursing home placement or death (NHPOD) at one year was 1, 2.4, and 3.4, respectively. A validation cohort of 461 statistically similar patients showed RR for development in the low-, intermediate-, and high-risk groups of 1, 5.4, 10.2, respectively; and RR at one year for NHPOD was 1, 2.7, and 4.4, respectively.
Bottom line: Dementia, vision impairment, inability to perform at least one ADL, multiple comorbidities, and use of restraints are risk factors that can stratify patients into low, intermediate, and high risk for delirium at hospital discharge. Commensurate risks exist for nursing home placement or death at one year.
Citation: Inouye SK, Zhang Y, Jones RN. Risk factors for delirium at discharge. Arch Intern Med. 2007;167(13):1406-1413.
Mission in D.C.
SHM’s Public Policy Committee (PPC) has been monitoring federal legislation and regulations affecting hospital medicine and recommending appropriate action by the Society. Over the past several months, the PPC has been engaged in a variety of initiatives.
Physician Payment (Part B)
One of lawmakers’ top priorities in 2007 was addressing pending cuts in Medicare payments to physicians. Under the flawed sustainable growth rate (SGR) formula, Part B Medicare payments were to be reduced by 10% in 2008 and by an additional 5% in January 2009. SHM is working to influence the debate.
Chapter Summaries
Montana

Nashville
The Nashville chapter met Sept. 13 for a roundtable discussion on challenges in the management of hospitalist programs. Eleven hospitalist physicians attended, including five medical directors who represented five area hospitalist programs:
- Kimberly Bell, MD, HCA/Centennial Medical Center, Nashville;
- Rizwan Faisal, MD, Horizon Medical Center, Dickson;
- Randal Rampp, MD, River Park Hospital, McMinnville;
- James Snyder, MD, St. Thomas Hospital, Nashville; and
- James Tedesco, MD, Summit Medical Associates, Hermitage.
These medical directors de-scribed their programs and how they manage variation in daily patient volume, plan for staffing needs, and recruiting. They also discussed jeopardy plans, physician extenders, how to attract new applicants, and incentive plans.
As Congress began to consider legislation on physician payment reform, SHM quickly launched a comprehensive grassroots campaign to stop the cuts. In an e-mail to 7,745 hospitalists, PPC Chair Eric Siegal, MD, director of the hospital medicine program, Cogent Healthcare, Nashville, Tenn., urged members to contact their lawmakers using SHM’s online advocacy tool, Capwiz. Several issues of the e-newsletter also reminded members to write their representatives in support of two years of positive updates. As the congressional session came to a close, SHM members had sent a record 800 messages to their lawmakers urging them to block the pending reductions.
Then, in a letter to the chairs of the Ways and Means and Energy and Commerce committees, SHM commented on key provisions of draft Medicare legislation, expressing appreciation for the inclusion of language averting the scheduled cuts. SHM voiced concern about provisions of the bill that would reconfigure the Medicare payment formula into six service-specific categories with their own expenditure targets and conversion rates, in an effort to control volume of services. The letter also urged Congress to continue to provide funding for voluntary participation in the Physician Quality Reporting Initiative (PQRI) in 2008.
SHM also joined 130 state and national medical societies to urge Senate Majority Leader Harry Reid, D-Nev., to include two years of positive Medicare physician payment updates in pending legislation that would reauthorize the State Children’s Health Insurance Program. The letter underscored the importance of Congress acting sooner rather than later to reverse the cuts. “Temporary Congressional interventions to prevent past cuts, while necessary, have not kept up with increases in medical practice costs and have pushed the cost of fixing the problem to future years, making a meaningful long-term resolution more and more expensive,” the letter read. “Physician payment rates are about the same today as they were in 2001, while practice costs have increased nearly 20% and will increase another 20% over next nine years, according to the government’s conservative Medicare Economic Index (MEI).”
Last fall, two PPC members, Eric Howell, MD, from Maryland, and Greg Seymann, MD, from California, visited members of their congressional delegation on Capitol Hill. Dr. Howell is director of Collaborative Inpatient Medicine Service, Department of Medicine, Johns Hopkins Bayview Medical Center, Baltimore. Dr. Seymann is associate clinical professor, University of California, San Diego School of Medicine, Division of Hospital Medicine. During their meetings, Drs. Howell and Seymann voiced support for legislation to avert the Medicare cuts and discussed other elements of SHM’s quality-centered legislative agenda, emphasizing the role of hospitalists in improving the quality of care provided in America’s hospitals.
Hospital Payment (Part A)
SHM joined the American Hospital Association in opposition to a provision in the fiscal year 2008 Medicare inpatient prospective payment system, a proposed rule that would have cut Medicare payment for hospital services in fiscal year 2008.
The Centers for Medicare and Medicaid Services (CMS) sought to reduce hospital payments by 2.4% in 2008 and 2009 based on the assumption that hospitals will adjust coding practices to receive higher payments as a result of proposed changes in the payment system designed to account more fully for patients’ severity of illness.
This proposed “behavioral offset” would have cut $24 billion over five years from payments to hospitals. Congress enacted legislation in September that significantly reduces the cuts hospitals face in the next two years.
Quality Reporting
Together with the Performance and Standards Task Force (PSTF), PPC and staff have posted educational material on our Web site and made other resources available to SHM members to help them determine whether or not they should participate in the PQRI, which began July 1.
For example, SHM sponsored a nationwide call with CMS on the “Nuts and Bolts of Applying the PQRI to Your Hospital Medicine Practice.” Staff have since surveyed the SHM members who participated in this members-only call to learn more about what led them to participate or not to participate in the program. Those participating were asked for information on their experiences to help inform our policy on the initiative.
PPC and the PSTF also collaborated on comments to CMS on the 2008 proposed physician payment rule that dealt with the PQRI and submitted comments to CMS staff on the draft feedback report that PQRI participating physicians and other health professionals will receive upon completion of the 2007 program.
In other action, at the PPC’s recommendation, SHM endorsed legislation that would authorize federal funding for the development and testing of inpatient pediatric quality measures. When it comes to measuring and reporting on healthcare quality, children’s measures lag far behind those for adult care. The Children’s Health Care Quality Act (S. 1226/H.R. 2723) would address this disparity.
FY 2008 Appropriations
SHM continues to call on Congress to increase funding for the Agency for Health Care Research and Quality (AHRQ) in view of the important role the agency plays in supporting quality improvement and patient safety initiatives.
Our efforts are paying off. Legislation approved by the House of Representatives and by the Senate Appropriations Committee would boost AHRQ funding in FY 2008 by $10 million to $329 million, the first increase for the agency in several years. SHM members sent 100 messages to Capitol Hill in support of increased spending for AHRQ. Research Committee Chair Andrew Auerbach, MD, visited with legislative staff Sept. 17 to advocate for greater funding for AHRQ and the creation of a new Center for Comparative Effectiveness Research within the agency. Dr. Auerbach is assistant professor of medicine in residence at the University of California, San Francisco.
At press time, Congress had not taken final action on FY 2008 appropriations for AHRQ.
The PPC keeps you informed about our legislative and regulatory activities through monthly updates posted via the SHM Web site, The Hospitalist, and our e-newsletter. SHM letters to Congress and CMS are on the SHM Web site as well. Depending on the issue, you might also get an e-mail urging you to visit our legislative action center at www.hospitalmedicine.org/beheard and contact your members of Congress. We depend on your involvement in the legislative process to be effective in Washington. We appreciate your feedback. You can reach me at lallendorf@hospitalmedicine.org.
SHM’s Public Policy Committee (PPC) has been monitoring federal legislation and regulations affecting hospital medicine and recommending appropriate action by the Society. Over the past several months, the PPC has been engaged in a variety of initiatives.
Physician Payment (Part B)
One of lawmakers’ top priorities in 2007 was addressing pending cuts in Medicare payments to physicians. Under the flawed sustainable growth rate (SGR) formula, Part B Medicare payments were to be reduced by 10% in 2008 and by an additional 5% in January 2009. SHM is working to influence the debate.
Chapter Summaries
Montana
Nashville
The Nashville chapter met Sept. 13 for a roundtable discussion on challenges in the management of hospitalist programs. Eleven hospitalist physicians attended, including five medical directors who represented five area hospitalist programs:
- Kimberly Bell, MD, HCA/Centennial Medical Center, Nashville;
- Rizwan Faisal, MD, Horizon Medical Center, Dickson;
- Randal Rampp, MD, River Park Hospital, McMinnville;
- James Snyder, MD, St. Thomas Hospital, Nashville; and
- James Tedesco, MD, Summit Medical Associates, Hermitage.
These medical directors de-scribed their programs and how they manage variation in daily patient volume, plan for staffing needs, and recruiting. They also discussed jeopardy plans, physician extenders, how to attract new applicants, and incentive plans.
As Congress began to consider legislation on physician payment reform, SHM quickly launched a comprehensive grassroots campaign to stop the cuts. In an e-mail to 7,745 hospitalists, PPC Chair Eric Siegal, MD, director of the hospital medicine program, Cogent Healthcare, Nashville, Tenn., urged members to contact their lawmakers using SHM’s online advocacy tool, Capwiz. Several issues of the e-newsletter also reminded members to write their representatives in support of two years of positive updates. As the congressional session came to a close, SHM members had sent a record 800 messages to their lawmakers urging them to block the pending reductions.
Then, in a letter to the chairs of the Ways and Means and Energy and Commerce committees, SHM commented on key provisions of draft Medicare legislation, expressing appreciation for the inclusion of language averting the scheduled cuts. SHM voiced concern about provisions of the bill that would reconfigure the Medicare payment formula into six service-specific categories with their own expenditure targets and conversion rates, in an effort to control volume of services. The letter also urged Congress to continue to provide funding for voluntary participation in the Physician Quality Reporting Initiative (PQRI) in 2008.
SHM also joined 130 state and national medical societies to urge Senate Majority Leader Harry Reid, D-Nev., to include two years of positive Medicare physician payment updates in pending legislation that would reauthorize the State Children’s Health Insurance Program. The letter underscored the importance of Congress acting sooner rather than later to reverse the cuts. “Temporary Congressional interventions to prevent past cuts, while necessary, have not kept up with increases in medical practice costs and have pushed the cost of fixing the problem to future years, making a meaningful long-term resolution more and more expensive,” the letter read. “Physician payment rates are about the same today as they were in 2001, while practice costs have increased nearly 20% and will increase another 20% over next nine years, according to the government’s conservative Medicare Economic Index (MEI).”
Last fall, two PPC members, Eric Howell, MD, from Maryland, and Greg Seymann, MD, from California, visited members of their congressional delegation on Capitol Hill. Dr. Howell is director of Collaborative Inpatient Medicine Service, Department of Medicine, Johns Hopkins Bayview Medical Center, Baltimore. Dr. Seymann is associate clinical professor, University of California, San Diego School of Medicine, Division of Hospital Medicine. During their meetings, Drs. Howell and Seymann voiced support for legislation to avert the Medicare cuts and discussed other elements of SHM’s quality-centered legislative agenda, emphasizing the role of hospitalists in improving the quality of care provided in America’s hospitals.
Hospital Payment (Part A)
SHM joined the American Hospital Association in opposition to a provision in the fiscal year 2008 Medicare inpatient prospective payment system, a proposed rule that would have cut Medicare payment for hospital services in fiscal year 2008.
The Centers for Medicare and Medicaid Services (CMS) sought to reduce hospital payments by 2.4% in 2008 and 2009 based on the assumption that hospitals will adjust coding practices to receive higher payments as a result of proposed changes in the payment system designed to account more fully for patients’ severity of illness.
This proposed “behavioral offset” would have cut $24 billion over five years from payments to hospitals. Congress enacted legislation in September that significantly reduces the cuts hospitals face in the next two years.
Quality Reporting
Together with the Performance and Standards Task Force (PSTF), PPC and staff have posted educational material on our Web site and made other resources available to SHM members to help them determine whether or not they should participate in the PQRI, which began July 1.
For example, SHM sponsored a nationwide call with CMS on the “Nuts and Bolts of Applying the PQRI to Your Hospital Medicine Practice.” Staff have since surveyed the SHM members who participated in this members-only call to learn more about what led them to participate or not to participate in the program. Those participating were asked for information on their experiences to help inform our policy on the initiative.
PPC and the PSTF also collaborated on comments to CMS on the 2008 proposed physician payment rule that dealt with the PQRI and submitted comments to CMS staff on the draft feedback report that PQRI participating physicians and other health professionals will receive upon completion of the 2007 program.
In other action, at the PPC’s recommendation, SHM endorsed legislation that would authorize federal funding for the development and testing of inpatient pediatric quality measures. When it comes to measuring and reporting on healthcare quality, children’s measures lag far behind those for adult care. The Children’s Health Care Quality Act (S. 1226/H.R. 2723) would address this disparity.
FY 2008 Appropriations
SHM continues to call on Congress to increase funding for the Agency for Health Care Research and Quality (AHRQ) in view of the important role the agency plays in supporting quality improvement and patient safety initiatives.
Our efforts are paying off. Legislation approved by the House of Representatives and by the Senate Appropriations Committee would boost AHRQ funding in FY 2008 by $10 million to $329 million, the first increase for the agency in several years. SHM members sent 100 messages to Capitol Hill in support of increased spending for AHRQ. Research Committee Chair Andrew Auerbach, MD, visited with legislative staff Sept. 17 to advocate for greater funding for AHRQ and the creation of a new Center for Comparative Effectiveness Research within the agency. Dr. Auerbach is assistant professor of medicine in residence at the University of California, San Francisco.
At press time, Congress had not taken final action on FY 2008 appropriations for AHRQ.
The PPC keeps you informed about our legislative and regulatory activities through monthly updates posted via the SHM Web site, The Hospitalist, and our e-newsletter. SHM letters to Congress and CMS are on the SHM Web site as well. Depending on the issue, you might also get an e-mail urging you to visit our legislative action center at www.hospitalmedicine.org/beheard and contact your members of Congress. We depend on your involvement in the legislative process to be effective in Washington. We appreciate your feedback. You can reach me at lallendorf@hospitalmedicine.org.
SHM’s Public Policy Committee (PPC) has been monitoring federal legislation and regulations affecting hospital medicine and recommending appropriate action by the Society. Over the past several months, the PPC has been engaged in a variety of initiatives.
Physician Payment (Part B)
One of lawmakers’ top priorities in 2007 was addressing pending cuts in Medicare payments to physicians. Under the flawed sustainable growth rate (SGR) formula, Part B Medicare payments were to be reduced by 10% in 2008 and by an additional 5% in January 2009. SHM is working to influence the debate.
Chapter Summaries
Montana
Nashville
The Nashville chapter met Sept. 13 for a roundtable discussion on challenges in the management of hospitalist programs. Eleven hospitalist physicians attended, including five medical directors who represented five area hospitalist programs:
- Kimberly Bell, MD, HCA/Centennial Medical Center, Nashville;
- Rizwan Faisal, MD, Horizon Medical Center, Dickson;
- Randal Rampp, MD, River Park Hospital, McMinnville;
- James Snyder, MD, St. Thomas Hospital, Nashville; and
- James Tedesco, MD, Summit Medical Associates, Hermitage.
These medical directors de-scribed their programs and how they manage variation in daily patient volume, plan for staffing needs, and recruiting. They also discussed jeopardy plans, physician extenders, how to attract new applicants, and incentive plans.
As Congress began to consider legislation on physician payment reform, SHM quickly launched a comprehensive grassroots campaign to stop the cuts. In an e-mail to 7,745 hospitalists, PPC Chair Eric Siegal, MD, director of the hospital medicine program, Cogent Healthcare, Nashville, Tenn., urged members to contact their lawmakers using SHM’s online advocacy tool, Capwiz. Several issues of the e-newsletter also reminded members to write their representatives in support of two years of positive updates. As the congressional session came to a close, SHM members had sent a record 800 messages to their lawmakers urging them to block the pending reductions.
Then, in a letter to the chairs of the Ways and Means and Energy and Commerce committees, SHM commented on key provisions of draft Medicare legislation, expressing appreciation for the inclusion of language averting the scheduled cuts. SHM voiced concern about provisions of the bill that would reconfigure the Medicare payment formula into six service-specific categories with their own expenditure targets and conversion rates, in an effort to control volume of services. The letter also urged Congress to continue to provide funding for voluntary participation in the Physician Quality Reporting Initiative (PQRI) in 2008.
SHM also joined 130 state and national medical societies to urge Senate Majority Leader Harry Reid, D-Nev., to include two years of positive Medicare physician payment updates in pending legislation that would reauthorize the State Children’s Health Insurance Program. The letter underscored the importance of Congress acting sooner rather than later to reverse the cuts. “Temporary Congressional interventions to prevent past cuts, while necessary, have not kept up with increases in medical practice costs and have pushed the cost of fixing the problem to future years, making a meaningful long-term resolution more and more expensive,” the letter read. “Physician payment rates are about the same today as they were in 2001, while practice costs have increased nearly 20% and will increase another 20% over next nine years, according to the government’s conservative Medicare Economic Index (MEI).”
Last fall, two PPC members, Eric Howell, MD, from Maryland, and Greg Seymann, MD, from California, visited members of their congressional delegation on Capitol Hill. Dr. Howell is director of Collaborative Inpatient Medicine Service, Department of Medicine, Johns Hopkins Bayview Medical Center, Baltimore. Dr. Seymann is associate clinical professor, University of California, San Diego School of Medicine, Division of Hospital Medicine. During their meetings, Drs. Howell and Seymann voiced support for legislation to avert the Medicare cuts and discussed other elements of SHM’s quality-centered legislative agenda, emphasizing the role of hospitalists in improving the quality of care provided in America’s hospitals.
Hospital Payment (Part A)
SHM joined the American Hospital Association in opposition to a provision in the fiscal year 2008 Medicare inpatient prospective payment system, a proposed rule that would have cut Medicare payment for hospital services in fiscal year 2008.
The Centers for Medicare and Medicaid Services (CMS) sought to reduce hospital payments by 2.4% in 2008 and 2009 based on the assumption that hospitals will adjust coding practices to receive higher payments as a result of proposed changes in the payment system designed to account more fully for patients’ severity of illness.
This proposed “behavioral offset” would have cut $24 billion over five years from payments to hospitals. Congress enacted legislation in September that significantly reduces the cuts hospitals face in the next two years.
Quality Reporting
Together with the Performance and Standards Task Force (PSTF), PPC and staff have posted educational material on our Web site and made other resources available to SHM members to help them determine whether or not they should participate in the PQRI, which began July 1.
For example, SHM sponsored a nationwide call with CMS on the “Nuts and Bolts of Applying the PQRI to Your Hospital Medicine Practice.” Staff have since surveyed the SHM members who participated in this members-only call to learn more about what led them to participate or not to participate in the program. Those participating were asked for information on their experiences to help inform our policy on the initiative.
PPC and the PSTF also collaborated on comments to CMS on the 2008 proposed physician payment rule that dealt with the PQRI and submitted comments to CMS staff on the draft feedback report that PQRI participating physicians and other health professionals will receive upon completion of the 2007 program.
In other action, at the PPC’s recommendation, SHM endorsed legislation that would authorize federal funding for the development and testing of inpatient pediatric quality measures. When it comes to measuring and reporting on healthcare quality, children’s measures lag far behind those for adult care. The Children’s Health Care Quality Act (S. 1226/H.R. 2723) would address this disparity.
FY 2008 Appropriations
SHM continues to call on Congress to increase funding for the Agency for Health Care Research and Quality (AHRQ) in view of the important role the agency plays in supporting quality improvement and patient safety initiatives.
Our efforts are paying off. Legislation approved by the House of Representatives and by the Senate Appropriations Committee would boost AHRQ funding in FY 2008 by $10 million to $329 million, the first increase for the agency in several years. SHM members sent 100 messages to Capitol Hill in support of increased spending for AHRQ. Research Committee Chair Andrew Auerbach, MD, visited with legislative staff Sept. 17 to advocate for greater funding for AHRQ and the creation of a new Center for Comparative Effectiveness Research within the agency. Dr. Auerbach is assistant professor of medicine in residence at the University of California, San Francisco.
At press time, Congress had not taken final action on FY 2008 appropriations for AHRQ.
The PPC keeps you informed about our legislative and regulatory activities through monthly updates posted via the SHM Web site, The Hospitalist, and our e-newsletter. SHM letters to Congress and CMS are on the SHM Web site as well. Depending on the issue, you might also get an e-mail urging you to visit our legislative action center at www.hospitalmedicine.org/beheard and contact your members of Congress. We depend on your involvement in the legislative process to be effective in Washington. We appreciate your feedback. You can reach me at lallendorf@hospitalmedicine.org.
Use Incentives, Moonlighters to Staff the Holidays

Holidays can pose a challenge for hospitalists who have to balance proper patient care with appropriate staffing. Good communication and chart documentation can make all the difference.
Bradley A. Sharpe, MD, assistant chief of medical service at the University of California, San Francisco, department of medicine, says patients admitted on holidays should be able to know treatment they receive is as good as on any other day of the year.
“All groups should probably act under the premise that a patient admitted on Thanksgiving day should get exactly the same care as one who gets admitted the following Tuesday,” he says. “Because there are fewer admissions, fewer tests, [and] fewer procedures, groups can probably dial down their staffing a bit. But it should not be a skeleton crew that could put patients at risk.”
Certainly, maintaining a high level of patient care depends on the attitudes of the caretakers.
Ken Simone, DO, president and founder of Hospitalist and Practice Solutions in Veazie, Maine, suggests making holiday work worthwhile for your staff.
“Hospitalist programs can make holidays more attractive to the hospitalist staff by offering a pay differential or by rewarding holiday work with additional days off,” he says.
Dr. Sharpe also recommends getting staff involved in the scheduling process early so they feel empowered.
—Ken Simone, DO, president and founder, Hospitalist and Practice Solutions, Veazie, Maine
“There is plenty of evidence that a lack of control contributes to unhappiness and burnout,” Dr. Sharpe says. “If the staff feels like they have been part of deciding how to do this, they will be less likely to complain.”
He also discourages using rank or seniority in dealing with holiday schedules.
“For our group, regardless of rank or seniority, everyone is expected to do the same number of major holidays over a three-year period, and then the cycle starts over,” he says.
Brigham and Women’s Hospital in Boston uses blocks of time—usually two weeks—rather than typical shifts; residents are available to cover off-hours, says Sylvia C. W. McKean, MD, FACP, medical director of the hospital and Faulkner Hospitalist Service.
“If there are difficulties with the availability of the existing staff, consider hiring moonlighters such as established physicians in the community, internal medicine or family practice residents, or utilizing locum tenens,” Dr. Simone says. “Non-physician clinicians can also be a resource.”
He notes that staffing needs should be estimated by the hospitalist inpatient census and average number of admissions and discharges per day.
Once that is determined, he recommends “a defined checkout process” between providers who will be off and the providers who work on holidays, similar to checkout protocol on weekends.
“Provider-to-provider checkout is a key component to ensuring patient continuity and safety,” he says. “Appropriate (e.g., clear and detailed) documentation in the patient’s medical record is also important.”
Dr. Sharpe agrees, adding that moonlighters especially should be made fully aware of the process.
“Groups should be sure they have a robust signout and sign-in system to make sure nothing is lost in the shuffle,” he cautions.
The bottom line is that working holiday shifts should not compromise patient care, Dr. Simone says. “Excellent communication, excellent chart documentation, and appropriate staffing are keys to maintaining continuity of care, quality patient care, and patient safety,” he says. TH
Molly Okeon is journalist based in California.
Holidays can pose a challenge for hospitalists who have to balance proper patient care with appropriate staffing. Good communication and chart documentation can make all the difference.
Bradley A. Sharpe, MD, assistant chief of medical service at the University of California, San Francisco, department of medicine, says patients admitted on holidays should be able to know treatment they receive is as good as on any other day of the year.
“All groups should probably act under the premise that a patient admitted on Thanksgiving day should get exactly the same care as one who gets admitted the following Tuesday,” he says. “Because there are fewer admissions, fewer tests, [and] fewer procedures, groups can probably dial down their staffing a bit. But it should not be a skeleton crew that could put patients at risk.”
Certainly, maintaining a high level of patient care depends on the attitudes of the caretakers.
Ken Simone, DO, president and founder of Hospitalist and Practice Solutions in Veazie, Maine, suggests making holiday work worthwhile for your staff.
“Hospitalist programs can make holidays more attractive to the hospitalist staff by offering a pay differential or by rewarding holiday work with additional days off,” he says.
Dr. Sharpe also recommends getting staff involved in the scheduling process early so they feel empowered.
—Ken Simone, DO, president and founder, Hospitalist and Practice Solutions, Veazie, Maine
“There is plenty of evidence that a lack of control contributes to unhappiness and burnout,” Dr. Sharpe says. “If the staff feels like they have been part of deciding how to do this, they will be less likely to complain.”
He also discourages using rank or seniority in dealing with holiday schedules.
“For our group, regardless of rank or seniority, everyone is expected to do the same number of major holidays over a three-year period, and then the cycle starts over,” he says.
Brigham and Women’s Hospital in Boston uses blocks of time—usually two weeks—rather than typical shifts; residents are available to cover off-hours, says Sylvia C. W. McKean, MD, FACP, medical director of the hospital and Faulkner Hospitalist Service.
“If there are difficulties with the availability of the existing staff, consider hiring moonlighters such as established physicians in the community, internal medicine or family practice residents, or utilizing locum tenens,” Dr. Simone says. “Non-physician clinicians can also be a resource.”
He notes that staffing needs should be estimated by the hospitalist inpatient census and average number of admissions and discharges per day.
Once that is determined, he recommends “a defined checkout process” between providers who will be off and the providers who work on holidays, similar to checkout protocol on weekends.
“Provider-to-provider checkout is a key component to ensuring patient continuity and safety,” he says. “Appropriate (e.g., clear and detailed) documentation in the patient’s medical record is also important.”
Dr. Sharpe agrees, adding that moonlighters especially should be made fully aware of the process.
“Groups should be sure they have a robust signout and sign-in system to make sure nothing is lost in the shuffle,” he cautions.
The bottom line is that working holiday shifts should not compromise patient care, Dr. Simone says. “Excellent communication, excellent chart documentation, and appropriate staffing are keys to maintaining continuity of care, quality patient care, and patient safety,” he says. TH
Molly Okeon is journalist based in California.
Holidays can pose a challenge for hospitalists who have to balance proper patient care with appropriate staffing. Good communication and chart documentation can make all the difference.
Bradley A. Sharpe, MD, assistant chief of medical service at the University of California, San Francisco, department of medicine, says patients admitted on holidays should be able to know treatment they receive is as good as on any other day of the year.
“All groups should probably act under the premise that a patient admitted on Thanksgiving day should get exactly the same care as one who gets admitted the following Tuesday,” he says. “Because there are fewer admissions, fewer tests, [and] fewer procedures, groups can probably dial down their staffing a bit. But it should not be a skeleton crew that could put patients at risk.”
Certainly, maintaining a high level of patient care depends on the attitudes of the caretakers.
Ken Simone, DO, president and founder of Hospitalist and Practice Solutions in Veazie, Maine, suggests making holiday work worthwhile for your staff.
“Hospitalist programs can make holidays more attractive to the hospitalist staff by offering a pay differential or by rewarding holiday work with additional days off,” he says.
Dr. Sharpe also recommends getting staff involved in the scheduling process early so they feel empowered.
—Ken Simone, DO, president and founder, Hospitalist and Practice Solutions, Veazie, Maine
“There is plenty of evidence that a lack of control contributes to unhappiness and burnout,” Dr. Sharpe says. “If the staff feels like they have been part of deciding how to do this, they will be less likely to complain.”
He also discourages using rank or seniority in dealing with holiday schedules.
“For our group, regardless of rank or seniority, everyone is expected to do the same number of major holidays over a three-year period, and then the cycle starts over,” he says.
Brigham and Women’s Hospital in Boston uses blocks of time—usually two weeks—rather than typical shifts; residents are available to cover off-hours, says Sylvia C. W. McKean, MD, FACP, medical director of the hospital and Faulkner Hospitalist Service.
“If there are difficulties with the availability of the existing staff, consider hiring moonlighters such as established physicians in the community, internal medicine or family practice residents, or utilizing locum tenens,” Dr. Simone says. “Non-physician clinicians can also be a resource.”
He notes that staffing needs should be estimated by the hospitalist inpatient census and average number of admissions and discharges per day.
Once that is determined, he recommends “a defined checkout process” between providers who will be off and the providers who work on holidays, similar to checkout protocol on weekends.
“Provider-to-provider checkout is a key component to ensuring patient continuity and safety,” he says. “Appropriate (e.g., clear and detailed) documentation in the patient’s medical record is also important.”
Dr. Sharpe agrees, adding that moonlighters especially should be made fully aware of the process.
“Groups should be sure they have a robust signout and sign-in system to make sure nothing is lost in the shuffle,” he cautions.
The bottom line is that working holiday shifts should not compromise patient care, Dr. Simone says. “Excellent communication, excellent chart documentation, and appropriate staffing are keys to maintaining continuity of care, quality patient care, and patient safety,” he says. TH
Molly Okeon is journalist based in California.
How Am I Doing?
How hospitalists assess their performance and hone their skills is critical to patient care. Continuing medical education (CME), relicensure, specialty recertification, and lifelong learning are all linked to hospitalists’ abilities to assess and meet their learning needs.
But the preponderance of evidence suggests physicians have limited ability to accurately assess their performance, according to a physician self-assessment literature review published in September 2006 in JAMA.1
“Self-assessment should be guided by tools designed by experts, based on standards, and aimed at filling gaps in knowledge, skills, and competencies—not simply the internally based self-rating of individual practitioners,” says C. Michael Fordis, MD, senior associate dean for con-
tinuing medical education at the Baylor College of Medicine in Houston, and one of the authors of the study.
“Hospitalists and other physicians are not doing themselves a service to rely on their own internal self-rated judgments of knowledge and performance,” Dr. Fordis says. “There’s too much to know, too much that’s changing, and too much that affects the implementation into practice of the knowledge that you have for any one person to be able to take care of patients and at the same time have some sense of whether there are gaps along that implementation pathway.”
“Guided” self-assessment represents the thinking of many experts who ask questions, consider guidelines, and suggest tools that can help physicians pursue the best ways of identifying those gaps that reflect differences in what they think they are doing and their actual performance.
Regular, consistent self-assessment is imperative for a self-regulating profession such as medicine. How well are hospitalists doing—and what mechanisms or tools do they use?
Group Assessment
Hospital medicine groups are increasingly able to measure their clinical competence against other hospitals’ and hospitalist groups. SHM’s Benchmarks Committee has been working on performance assessment at a program level.
“When the JCAHO [Joint Commission on Accreditation of Healthcare Organizations] Core Measures were coming out a few years back, as a whole most docs when reflecting on their practice would say they do a fine job within these measures,” says Burke T. Kealey, MD, chairman of the Benchmarks Committee from 2006-07. “For instance, [they might say] ‘I always send people out on ACE inhibitors and beta-blockers,’ or, ‘We always start people on aspirin when they come into the ER,’ but when you looked at the data, you found that their self-assessment was not as accurate as we hoped it would be.”
A lot of hard work went into discovering why their self-assessment was inaccurate. “We found there were documentation problems that they didn’t really incorporate a lot of the contraindications when giving their answer about self-assessment,” says Dr. Kealey, who leads the hospital medicine program at Regions Hospital and HealthPartners Medical Group in St. Paul, Minn.
If patients had kidney dysfunction or kidney failure, they were not discharged on ACE inhibitors.
“But we as doctors didn’t do a great job of explaining why we weren’t doing that,” Dr. Kealey says. “We were not transparent in our reasoning, but the core measures caused us to become more transparent, to explain what we were thinking and what we were doing in a way that the public could see.”
At SHM’s annual meeting in May, the Benchmarks Committee released the white paper “Measuring Hospitalist Performance: Metrics, Reports, and Dashboards” with the intent of assisting hospitals and hospital medicine programs develop or improve their performance monitoring and reporting.
“Hospitalists in general could do a better job of assessing themselves,” says Arpana Vidyarthi, MD, an assistant professor in the division of hospital medicine at the University of California, San Francisco (UCSF). “Self-assessment for those of us in cognitive specialties, like internists, is more complicated than in procedural specialties like surgery, partly because these procedural specialties have very specific outcomes that are linked to the procedure and that level of skill. With the new drivers of quality improvement and patient safety, and the dramatic increase of quality indicators for hospitals overall, this is now trickling down to thinking about how we truly assess the doctors themselves.”
The quality indicators that hospitalist groups are benchmarking may not be linked to the individual, she says. Dr. Vidyarthi, also director of quality for the Inpatient General Medicine Service at UCSF Medical Center, provides an example. “Pneumovax as a quality indicator is part of the Joint Commission core measures,” says Dr. Vidyarthi. “You can go online where it is publicly reported and choose this or other indicators to compare one hospital to another. That is the sort of benchmarking that some hospitalists groups are doing.”
But using that kind of evaluation for individual assessment misses the mark.
“Does the fact that the patient does not get Pneumovax reflect upon me and my abilities as a hospitalist? Not at all,” she says, “because my institution and those institutions who have done well with this specific indicator have taken it out of the hands of the doctors. It’s an automated sort of thing. At our hospital, the pharmacists do it.”
Although the American Board of Internal Medicine asks that the individual physician assess his or her own care as part of recredentialing, it’s more difficult for a hospitalist than for an outpatient internist. Hospitalists don’t have a panel of diabetic patients, for instance, for which the outcomes data can be easily analyzed.
Hospitalists as a group also haven’t had a tradition of self-assessment or peer assessment. Further, hospitalist groups differ as to how they handle assessments of individual physicians.
“In general if you ask our [UCSF] hospitalists, the way that we assess competency is generally through hospital privileging,” Dr. Vidyarthi says. Because the hospital as a whole reviews the competency of all the doctors that work there, the process known as “privileging” has consisted of asking a couple of colleagues to write letters of recommendation. “The division is changing this, but that is just on the cusp.
“We’ve built a new system for our quality committee in which one layer is peer assessment, looking at just the individual cases that bubble up from an incident report or a root-cause analysis or other sources. We’re looking at and identifying both systems issues and individual issues and trying to build a way to feed back those assessments.”
But that’s just half the equation, she says, the flip side being continual self-assessment for what a hospitalist is doing well.
To Dr. Kealey, self-assessment plays a significant role in helping physicians with their career goals and ensuring that their careers are on track and on target.
At HealthPartners, physicians fill out a self-evaluation form on which they list all activities they’ve been involved in over the previous year. Then they are asked what they got out of these activities, what their career goals are, and whether they are meeting them. They’re also asked how the group can help them reach those goals.
“We ask them to pause and reflect on where they’re headed with their career and their life, and put it down in writing so that in that moment they take the time to ask, ‘What is it that I’m ultimately after?’ ” says Dr. Kealey.
Day to day, they are immersed in patient care and focused on doing a good job. “But in the trajectory of where they are headed—the committees, projects, and educational activities they are involved in—are they all aligned and pointing in the same direction and the right direction?” Dr Kealey asks.
The process, which HealthPartners hospitalists have been using for about 10 years, was modified from the American College of Physician Executives course “Managing Physician Performance.”
“It is a tool to help hospitalists pause and reflect on their career and how to move it forward,” Dr. Kealey says.
Marc B. Westle, DO, FACP, president and managing partner of the Asheville Hospitalist Group, PA, in Asheville, N.C., relies on ongoing conversations. This group also uses Crimson’s Physician Management Software to track various group quality and cost indicators, looking at data from as many angles as possible.
“It’s an excellent tool to look at a group, it is a poor tool to look at an individual,” Dr. Westle says. “Although the insurance companies like to say you can apply it to the individual, in reality there is no good way to attribute that data down to the physician level.”
Within the group data, it may be possible to recognize underperformers, but still it is anecdotal, based on experience and interaction.
“Under, ‘How am I doing?’ there is an objective category in the software where there are hard end-points and measures you can look at,” says Dr. Westle
On the subjective side, Dr. Westle collects data on relative value units (RVUs), non-monetary, numeric values Medicare uses to represent the relative amount of physician time, resources, and expertise needed to provide various services to patients. They review total RVUs as well as individual-components that make up total RVUs.
“I’ll track how many simple, moderate, or complex follow-up visits were made, how many simple or moderate histories and physicals or consultations, how many procedures are they doing.” Dr. Westle says. “I’ll track every statistic that way for every individual and give them that feedback so they can see how they’re doing from a performance and a work standard, compared to their peers within the group, and nationally as published by Medicare.”
Dr. Westle uses charts and graphs to drive his points home.
“It just gives them an idea about where they are,’’ he says. “It doesn’t mean they’re doing a bad job. Our patients may be sicker than some other patients. And that is why we do it as a group, too, because their patients should be similar to the group’s patients and the group’s patients may be different than the average Medicare patient.”
They also look at hospitalists’ quality of life, their schedules, and the quantity of work the average physician is doing compared with those around the country. They discuss scheduling, income, disposable income, and the kind of work they’re doing in the hospital. “All this comes into a discussion of where they are in their lives and are they happy with what they’re doing,” Dr. Westle says. TH
Andrea Sattinger is a medical writer based in North Carolina.
Reference
- Davis DA, Mazmanian PE, Fordis M, et al. Accuracy of physician self-assessment compared with observed measures of competence: a systematic review. JAMA. 2006;296(9):1094-1102.
How hospitalists assess their performance and hone their skills is critical to patient care. Continuing medical education (CME), relicensure, specialty recertification, and lifelong learning are all linked to hospitalists’ abilities to assess and meet their learning needs.
But the preponderance of evidence suggests physicians have limited ability to accurately assess their performance, according to a physician self-assessment literature review published in September 2006 in JAMA.1
“Self-assessment should be guided by tools designed by experts, based on standards, and aimed at filling gaps in knowledge, skills, and competencies—not simply the internally based self-rating of individual practitioners,” says C. Michael Fordis, MD, senior associate dean for con-
tinuing medical education at the Baylor College of Medicine in Houston, and one of the authors of the study.
“Hospitalists and other physicians are not doing themselves a service to rely on their own internal self-rated judgments of knowledge and performance,” Dr. Fordis says. “There’s too much to know, too much that’s changing, and too much that affects the implementation into practice of the knowledge that you have for any one person to be able to take care of patients and at the same time have some sense of whether there are gaps along that implementation pathway.”
“Guided” self-assessment represents the thinking of many experts who ask questions, consider guidelines, and suggest tools that can help physicians pursue the best ways of identifying those gaps that reflect differences in what they think they are doing and their actual performance.
Regular, consistent self-assessment is imperative for a self-regulating profession such as medicine. How well are hospitalists doing—and what mechanisms or tools do they use?
Group Assessment
Hospital medicine groups are increasingly able to measure their clinical competence against other hospitals’ and hospitalist groups. SHM’s Benchmarks Committee has been working on performance assessment at a program level.
“When the JCAHO [Joint Commission on Accreditation of Healthcare Organizations] Core Measures were coming out a few years back, as a whole most docs when reflecting on their practice would say they do a fine job within these measures,” says Burke T. Kealey, MD, chairman of the Benchmarks Committee from 2006-07. “For instance, [they might say] ‘I always send people out on ACE inhibitors and beta-blockers,’ or, ‘We always start people on aspirin when they come into the ER,’ but when you looked at the data, you found that their self-assessment was not as accurate as we hoped it would be.”
A lot of hard work went into discovering why their self-assessment was inaccurate. “We found there were documentation problems that they didn’t really incorporate a lot of the contraindications when giving their answer about self-assessment,” says Dr. Kealey, who leads the hospital medicine program at Regions Hospital and HealthPartners Medical Group in St. Paul, Minn.
If patients had kidney dysfunction or kidney failure, they were not discharged on ACE inhibitors.
“But we as doctors didn’t do a great job of explaining why we weren’t doing that,” Dr. Kealey says. “We were not transparent in our reasoning, but the core measures caused us to become more transparent, to explain what we were thinking and what we were doing in a way that the public could see.”
At SHM’s annual meeting in May, the Benchmarks Committee released the white paper “Measuring Hospitalist Performance: Metrics, Reports, and Dashboards” with the intent of assisting hospitals and hospital medicine programs develop or improve their performance monitoring and reporting.
“Hospitalists in general could do a better job of assessing themselves,” says Arpana Vidyarthi, MD, an assistant professor in the division of hospital medicine at the University of California, San Francisco (UCSF). “Self-assessment for those of us in cognitive specialties, like internists, is more complicated than in procedural specialties like surgery, partly because these procedural specialties have very specific outcomes that are linked to the procedure and that level of skill. With the new drivers of quality improvement and patient safety, and the dramatic increase of quality indicators for hospitals overall, this is now trickling down to thinking about how we truly assess the doctors themselves.”
The quality indicators that hospitalist groups are benchmarking may not be linked to the individual, she says. Dr. Vidyarthi, also director of quality for the Inpatient General Medicine Service at UCSF Medical Center, provides an example. “Pneumovax as a quality indicator is part of the Joint Commission core measures,” says Dr. Vidyarthi. “You can go online where it is publicly reported and choose this or other indicators to compare one hospital to another. That is the sort of benchmarking that some hospitalists groups are doing.”
But using that kind of evaluation for individual assessment misses the mark.
“Does the fact that the patient does not get Pneumovax reflect upon me and my abilities as a hospitalist? Not at all,” she says, “because my institution and those institutions who have done well with this specific indicator have taken it out of the hands of the doctors. It’s an automated sort of thing. At our hospital, the pharmacists do it.”
Although the American Board of Internal Medicine asks that the individual physician assess his or her own care as part of recredentialing, it’s more difficult for a hospitalist than for an outpatient internist. Hospitalists don’t have a panel of diabetic patients, for instance, for which the outcomes data can be easily analyzed.
Hospitalists as a group also haven’t had a tradition of self-assessment or peer assessment. Further, hospitalist groups differ as to how they handle assessments of individual physicians.
“In general if you ask our [UCSF] hospitalists, the way that we assess competency is generally through hospital privileging,” Dr. Vidyarthi says. Because the hospital as a whole reviews the competency of all the doctors that work there, the process known as “privileging” has consisted of asking a couple of colleagues to write letters of recommendation. “The division is changing this, but that is just on the cusp.
“We’ve built a new system for our quality committee in which one layer is peer assessment, looking at just the individual cases that bubble up from an incident report or a root-cause analysis or other sources. We’re looking at and identifying both systems issues and individual issues and trying to build a way to feed back those assessments.”
But that’s just half the equation, she says, the flip side being continual self-assessment for what a hospitalist is doing well.
To Dr. Kealey, self-assessment plays a significant role in helping physicians with their career goals and ensuring that their careers are on track and on target.
At HealthPartners, physicians fill out a self-evaluation form on which they list all activities they’ve been involved in over the previous year. Then they are asked what they got out of these activities, what their career goals are, and whether they are meeting them. They’re also asked how the group can help them reach those goals.
“We ask them to pause and reflect on where they’re headed with their career and their life, and put it down in writing so that in that moment they take the time to ask, ‘What is it that I’m ultimately after?’ ” says Dr. Kealey.
Day to day, they are immersed in patient care and focused on doing a good job. “But in the trajectory of where they are headed—the committees, projects, and educational activities they are involved in—are they all aligned and pointing in the same direction and the right direction?” Dr Kealey asks.
The process, which HealthPartners hospitalists have been using for about 10 years, was modified from the American College of Physician Executives course “Managing Physician Performance.”
“It is a tool to help hospitalists pause and reflect on their career and how to move it forward,” Dr. Kealey says.
Marc B. Westle, DO, FACP, president and managing partner of the Asheville Hospitalist Group, PA, in Asheville, N.C., relies on ongoing conversations. This group also uses Crimson’s Physician Management Software to track various group quality and cost indicators, looking at data from as many angles as possible.
“It’s an excellent tool to look at a group, it is a poor tool to look at an individual,” Dr. Westle says. “Although the insurance companies like to say you can apply it to the individual, in reality there is no good way to attribute that data down to the physician level.”
Within the group data, it may be possible to recognize underperformers, but still it is anecdotal, based on experience and interaction.
“Under, ‘How am I doing?’ there is an objective category in the software where there are hard end-points and measures you can look at,” says Dr. Westle
On the subjective side, Dr. Westle collects data on relative value units (RVUs), non-monetary, numeric values Medicare uses to represent the relative amount of physician time, resources, and expertise needed to provide various services to patients. They review total RVUs as well as individual-components that make up total RVUs.
“I’ll track how many simple, moderate, or complex follow-up visits were made, how many simple or moderate histories and physicals or consultations, how many procedures are they doing.” Dr. Westle says. “I’ll track every statistic that way for every individual and give them that feedback so they can see how they’re doing from a performance and a work standard, compared to their peers within the group, and nationally as published by Medicare.”
Dr. Westle uses charts and graphs to drive his points home.
“It just gives them an idea about where they are,’’ he says. “It doesn’t mean they’re doing a bad job. Our patients may be sicker than some other patients. And that is why we do it as a group, too, because their patients should be similar to the group’s patients and the group’s patients may be different than the average Medicare patient.”
They also look at hospitalists’ quality of life, their schedules, and the quantity of work the average physician is doing compared with those around the country. They discuss scheduling, income, disposable income, and the kind of work they’re doing in the hospital. “All this comes into a discussion of where they are in their lives and are they happy with what they’re doing,” Dr. Westle says. TH
Andrea Sattinger is a medical writer based in North Carolina.
Reference
- Davis DA, Mazmanian PE, Fordis M, et al. Accuracy of physician self-assessment compared with observed measures of competence: a systematic review. JAMA. 2006;296(9):1094-1102.
How hospitalists assess their performance and hone their skills is critical to patient care. Continuing medical education (CME), relicensure, specialty recertification, and lifelong learning are all linked to hospitalists’ abilities to assess and meet their learning needs.
But the preponderance of evidence suggests physicians have limited ability to accurately assess their performance, according to a physician self-assessment literature review published in September 2006 in JAMA.1
“Self-assessment should be guided by tools designed by experts, based on standards, and aimed at filling gaps in knowledge, skills, and competencies—not simply the internally based self-rating of individual practitioners,” says C. Michael Fordis, MD, senior associate dean for con-
tinuing medical education at the Baylor College of Medicine in Houston, and one of the authors of the study.
“Hospitalists and other physicians are not doing themselves a service to rely on their own internal self-rated judgments of knowledge and performance,” Dr. Fordis says. “There’s too much to know, too much that’s changing, and too much that affects the implementation into practice of the knowledge that you have for any one person to be able to take care of patients and at the same time have some sense of whether there are gaps along that implementation pathway.”
“Guided” self-assessment represents the thinking of many experts who ask questions, consider guidelines, and suggest tools that can help physicians pursue the best ways of identifying those gaps that reflect differences in what they think they are doing and their actual performance.
Regular, consistent self-assessment is imperative for a self-regulating profession such as medicine. How well are hospitalists doing—and what mechanisms or tools do they use?
Group Assessment
Hospital medicine groups are increasingly able to measure their clinical competence against other hospitals’ and hospitalist groups. SHM’s Benchmarks Committee has been working on performance assessment at a program level.
“When the JCAHO [Joint Commission on Accreditation of Healthcare Organizations] Core Measures were coming out a few years back, as a whole most docs when reflecting on their practice would say they do a fine job within these measures,” says Burke T. Kealey, MD, chairman of the Benchmarks Committee from 2006-07. “For instance, [they might say] ‘I always send people out on ACE inhibitors and beta-blockers,’ or, ‘We always start people on aspirin when they come into the ER,’ but when you looked at the data, you found that their self-assessment was not as accurate as we hoped it would be.”
A lot of hard work went into discovering why their self-assessment was inaccurate. “We found there were documentation problems that they didn’t really incorporate a lot of the contraindications when giving their answer about self-assessment,” says Dr. Kealey, who leads the hospital medicine program at Regions Hospital and HealthPartners Medical Group in St. Paul, Minn.
If patients had kidney dysfunction or kidney failure, they were not discharged on ACE inhibitors.
“But we as doctors didn’t do a great job of explaining why we weren’t doing that,” Dr. Kealey says. “We were not transparent in our reasoning, but the core measures caused us to become more transparent, to explain what we were thinking and what we were doing in a way that the public could see.”
At SHM’s annual meeting in May, the Benchmarks Committee released the white paper “Measuring Hospitalist Performance: Metrics, Reports, and Dashboards” with the intent of assisting hospitals and hospital medicine programs develop or improve their performance monitoring and reporting.
“Hospitalists in general could do a better job of assessing themselves,” says Arpana Vidyarthi, MD, an assistant professor in the division of hospital medicine at the University of California, San Francisco (UCSF). “Self-assessment for those of us in cognitive specialties, like internists, is more complicated than in procedural specialties like surgery, partly because these procedural specialties have very specific outcomes that are linked to the procedure and that level of skill. With the new drivers of quality improvement and patient safety, and the dramatic increase of quality indicators for hospitals overall, this is now trickling down to thinking about how we truly assess the doctors themselves.”
The quality indicators that hospitalist groups are benchmarking may not be linked to the individual, she says. Dr. Vidyarthi, also director of quality for the Inpatient General Medicine Service at UCSF Medical Center, provides an example. “Pneumovax as a quality indicator is part of the Joint Commission core measures,” says Dr. Vidyarthi. “You can go online where it is publicly reported and choose this or other indicators to compare one hospital to another. That is the sort of benchmarking that some hospitalists groups are doing.”
But using that kind of evaluation for individual assessment misses the mark.
“Does the fact that the patient does not get Pneumovax reflect upon me and my abilities as a hospitalist? Not at all,” she says, “because my institution and those institutions who have done well with this specific indicator have taken it out of the hands of the doctors. It’s an automated sort of thing. At our hospital, the pharmacists do it.”
Although the American Board of Internal Medicine asks that the individual physician assess his or her own care as part of recredentialing, it’s more difficult for a hospitalist than for an outpatient internist. Hospitalists don’t have a panel of diabetic patients, for instance, for which the outcomes data can be easily analyzed.
Hospitalists as a group also haven’t had a tradition of self-assessment or peer assessment. Further, hospitalist groups differ as to how they handle assessments of individual physicians.
“In general if you ask our [UCSF] hospitalists, the way that we assess competency is generally through hospital privileging,” Dr. Vidyarthi says. Because the hospital as a whole reviews the competency of all the doctors that work there, the process known as “privileging” has consisted of asking a couple of colleagues to write letters of recommendation. “The division is changing this, but that is just on the cusp.
“We’ve built a new system for our quality committee in which one layer is peer assessment, looking at just the individual cases that bubble up from an incident report or a root-cause analysis or other sources. We’re looking at and identifying both systems issues and individual issues and trying to build a way to feed back those assessments.”
But that’s just half the equation, she says, the flip side being continual self-assessment for what a hospitalist is doing well.
To Dr. Kealey, self-assessment plays a significant role in helping physicians with their career goals and ensuring that their careers are on track and on target.
At HealthPartners, physicians fill out a self-evaluation form on which they list all activities they’ve been involved in over the previous year. Then they are asked what they got out of these activities, what their career goals are, and whether they are meeting them. They’re also asked how the group can help them reach those goals.
“We ask them to pause and reflect on where they’re headed with their career and their life, and put it down in writing so that in that moment they take the time to ask, ‘What is it that I’m ultimately after?’ ” says Dr. Kealey.
Day to day, they are immersed in patient care and focused on doing a good job. “But in the trajectory of where they are headed—the committees, projects, and educational activities they are involved in—are they all aligned and pointing in the same direction and the right direction?” Dr Kealey asks.
The process, which HealthPartners hospitalists have been using for about 10 years, was modified from the American College of Physician Executives course “Managing Physician Performance.”
“It is a tool to help hospitalists pause and reflect on their career and how to move it forward,” Dr. Kealey says.
Marc B. Westle, DO, FACP, president and managing partner of the Asheville Hospitalist Group, PA, in Asheville, N.C., relies on ongoing conversations. This group also uses Crimson’s Physician Management Software to track various group quality and cost indicators, looking at data from as many angles as possible.
“It’s an excellent tool to look at a group, it is a poor tool to look at an individual,” Dr. Westle says. “Although the insurance companies like to say you can apply it to the individual, in reality there is no good way to attribute that data down to the physician level.”
Within the group data, it may be possible to recognize underperformers, but still it is anecdotal, based on experience and interaction.
“Under, ‘How am I doing?’ there is an objective category in the software where there are hard end-points and measures you can look at,” says Dr. Westle
On the subjective side, Dr. Westle collects data on relative value units (RVUs), non-monetary, numeric values Medicare uses to represent the relative amount of physician time, resources, and expertise needed to provide various services to patients. They review total RVUs as well as individual-components that make up total RVUs.
“I’ll track how many simple, moderate, or complex follow-up visits were made, how many simple or moderate histories and physicals or consultations, how many procedures are they doing.” Dr. Westle says. “I’ll track every statistic that way for every individual and give them that feedback so they can see how they’re doing from a performance and a work standard, compared to their peers within the group, and nationally as published by Medicare.”
Dr. Westle uses charts and graphs to drive his points home.
“It just gives them an idea about where they are,’’ he says. “It doesn’t mean they’re doing a bad job. Our patients may be sicker than some other patients. And that is why we do it as a group, too, because their patients should be similar to the group’s patients and the group’s patients may be different than the average Medicare patient.”
They also look at hospitalists’ quality of life, their schedules, and the quantity of work the average physician is doing compared with those around the country. They discuss scheduling, income, disposable income, and the kind of work they’re doing in the hospital. “All this comes into a discussion of where they are in their lives and are they happy with what they’re doing,” Dr. Westle says. TH
Andrea Sattinger is a medical writer based in North Carolina.
Reference
- Davis DA, Mazmanian PE, Fordis M, et al. Accuracy of physician self-assessment compared with observed measures of competence: a systematic review. JAMA. 2006;296(9):1094-1102.
The Surgical Surge
New limits on resident work hours and the graying of the U.S. population are putting hospitalists in the forefront of helping surgeons manage their patients.
Because the Accreditation Council for Graduate Medical Education restricted resident duty hours, surgeons can no longer rely automatically on residents to medically manage their patients on the floors, says Amir K. Jaffer, MD, a hospitalist and an associate professor of medicine at the Cleveland Clinic Lerner College of Medicine of Case Western Reserve University in Ohio.
Meanwhile, the population over age 65 will double, increasing to 70 million over the next 10 to 15 years.1
“More patients living longer means an increase in surgeries along the way,” says Dr. Jaffer, who is also the medical director of the Internal Medicine Preoperative Assessment Consultation and Treatment program in the section of hospital medicine at the Cleveland Clinic. For him, the first place hospitalists need to co-manage is in the postoperative setting.
“Studies have suggested that as patients age there is an increase in cardiological complications, noncardiological complications, pulmonary complications, and overall mortality,” he continues. “In my opinion there is going to be a crisis in regard to managing medical issues and complications surrounding surgery.” (See Table 1, p. 24)
Medications issues are another major reason hospitalists are called for surgical consults, says Benny Gavi, MD, hospitalist at Stanford Hospitals and Clinics in Calif. “I got consulted for a patient with tachycardia in the inpatient setting,” says Dr. Gavi. “By the time we saw the patient, the orthopedic surgeon had already ordered an echocardiogram and added a beta-blocker. When I looked at the patient I realized he had a gout flare; the colchicine that he took daily for his gout was never started in the inpatient setting, which ultimately delayed his physical therapy and added three additional days to his hospital stay.”
Co-management makes sense for still other reasons, he says.
“The knowledge base of both surgery and medicine is growing rapidly; no one person can remain on top of what is needed for both fields,” says Dr. Gavi. “In the last 20 years there has been a dramatic rise in the number of medications and some are very complicated. Also, physicians and surgeons both are being approached to participate more in quality initiatives and increasing throughput. As a result, physicians have to work faster and do more.”
Opportunities
In the United States, approximately 100,000 surgeries are performed each day and 36 million surgeries are performed each year at a cost of $450 billion annually. More than 1 million serious surgical adverse events each year cost $45 billion. Within two decades, the surgeries will increase by 25%, the associated cost will increase 50%, and the cost of in-hospital and long-term complications will increase 100%.
Along with postoperative care, there are increasing opportunities in the preoperative setting.
“At our institution, which is a tertiary care center with a huge surgical hospital, we determined that there was a need for hospitalists to provide medical management of surgical patients 10 years ago,” Dr. Jaffer says. “Patients were often not adequately prepared when they went to surgery, and sometimes in the morning of surgery the anesthesiologists would cancel their cases.”
The traditional model of physicians calling in consultants when problems arise might need to change.
“We are increasingly looking for ways to identify patients who have a high likelihood of developing medical problems and proactively getting involved,” says Dr. Gavi.
To co-manage, hospitalists must take ownership of some medical issues under specific conditions (diabetes, anticoagulation, blood pressure), says Dr. Jaffer.
The Benefits
To Latha Sivaprasad, MD, hospitalist at Beth Israel Medical Center in New York City, there are three main advantages of hospitalists’ involvement in perioperative co-management:
- Hospitalists typically perform comprehensive, multisystemic patient evaluations;
- Hospitalists are extremely accessible; and
- Hospitalists are up to date on inpatient medicine.
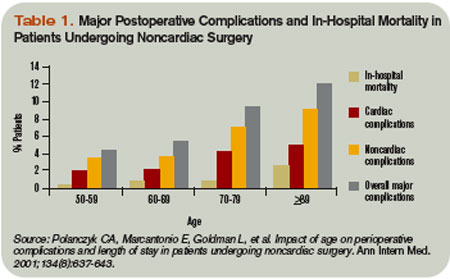
How up to date?
“Periop isn’t routinely taught in residency,” says Ali Usmani, MD, a hospitalist at the Cleveland Clinic. “In fact, I had little information about perioperative care.”
When he joined the hospitalist group after a three-year residency at Cleveland Clinic, Dr. Usmani did preparatory reading. Later, the hospitalist group gave him a helpful collection of essays.
“I was very nervous because, of course, I had never done this before,” he says. “Surprisingly, I also had not done a general medicine consult service where we see postoperative patients. It was scary to some extent, but I found out that it is easier than I thought because there are guidelines you can follow from the AHA/ACC that are fairly straightforward. It also meant a nice schedule change from being on the floors.”
Although conducting preoperative evaluations with patients was technically outpatient work, it was not like he was seeing patients with such simple illnesses as a cold or a sore throat. Also, he says, there were no new surprises postoperatively because either he or a hospitalist colleague had seen the patient preoperatively.
Dr. Usmani, also a clinical assistant professor of medicine at Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, believes patients are happier when seen by hospitalists because they get a standardized, holistic preoperative assessment. And, helping to reduce the number of unnecessary tests ordered by primary care physicians or surgeons makes him feel as though he’s making a valuable contribution.
New Niche
Dr. Sivaprasad, who is also doing a one-year fellowship in quality improvement and patient safety at Beth Israel, has practiced hospital medicine in four hospitals ranging from 500 to 1,000 beds. “The primary reason we are consulted by surgeons is for perioperative cardiac risk assessment,” says Dr. Sivaprasad. “Other reasons include co-managing a patient with comorbidities such as a history of diabetes, hypertension, or renal failure.”
From 2003-2006, Dr. Sivaprasad was one of 14 hospitalists consulted often by surgeons at St. John’s Mercy Hospital in St Louis, a 1,000-bed Level I trauma center. “We were consulted for postoperative co-management, preoperative evaluation, or more urgent cases such as a patient experiencing hypotension, atrial fibrillation, shortness of breath, decreased urine output, or renal failure,” she says.
Dr. Sivaprasad recently attended the Johns Hopkins conference on Perioperative Management. The session made it easier for her to do a systems-based consult.
“All hospitalists differ to the degree of perioperative medicine they feel comfortable with,” she says. “Hospitalists understand perioperative medicine on different levels. They all can do an acceptable consult; but there is a spectrum of how detailed one can be and what service one can provide for the surgeon and the patient.”
Dr. Jaffer finds his work in perioperative care fulfilling and considers it another way hospitalists can increase their influence.
“Often when you manage medical patients in the hospital, it’s you, the medical patient, and the patient’s primary care physician,” Dr. Jaffer says. “But when you start to manage surgical patients, you are really being looked at by your surgical colleagues as an expert in managing medical problems, just as you view them as experts in managing surgical problems. What I realize from this is that I can be a perioperative medicine expert as well.”
Are there any downfalls to co-managing surgical patients?
“Sometimes the surgeons order unnecessary lab tests such as PTTs [partial thromboplastin time] because they are concerned about bleeding and complications,” Dr. Usmani says. “The next day if there is a deranged PTT, we need to figure out whether to suggest postponing the surgery or go ahead with the surgery based on the patients’ past medical/family history. We try to get our surgeons and our colleagues to work together with us in that regard because they don’t want to postpone surgery either.”
Drs. Usmani, Gavi, Jaffer, and Sivaprasad all say that when surgeons can observe firsthand their hospitalist partners exhibiting expertise in acute care it appears to improve surgeons’ attitudes about the role and value of hospitalists.
In fact, says Dr. Usmani, surgeons call him or one of his colleagues to thank them. “They say, ‘We really appreciate what you’ve done for this patient,’ ’’ he says. “Even if we suggest canceling surgery, they respect that we have seen a potential problem instead of letting it go ahead. They are happy to receive this advice.”
Another new relationship is between anesthesiologists and hospitalists. “I spend a lot of time calling anesthesiologists in regard to patient cases, and a good many of them are surprised to get a call from a hospitalist,” Dr. Gavi says. “We especially work closely together when we get complicated patients ready for surgery.”
A recent encounter proved to Dr. Gavi the complementary nature of the hospitalist-anesthesiologist relationship.2
“A patient came to the hospital two weeks ago to have an elective total knee replacement,” says Dr. Gavi. “She was an older woman with severe pulmonary disease. When the anesthesiologists saw her in the preoperative waiting area and realized how sick she is, they wanted to cancel the surgery. But the surgeon told the anesthesiologist that this patient had been seen in our own preoperative clinic and cleared by a hospitalist.”
Dr. Gavi had done what is customary for an internist. He took a more in-depth look at her pulmonology and cardiac records, called her cardiologist for further history, and reassured the anesthesiologist and surgeon. The patient had her surgery.
The Future
“Perioperative co-management is becoming more of a visible need,” says Dr. Sivaprasad. “It bridges the gap between surgeons and internists.”
To those of his hospitalist colleagues who have little information and are a bit afraid to begin perioperative care practice, Dr. Usmani recommends attending a perioperative summit conference.
The session should teach how to set up a perioperative center and what to do when managing patients with certain conditions.
“Although you meet with patients preoperatively in an office setting, you don’t feel like a primary care physician,” Dr. Usmani says. “You feel as if you are a specialist. You are respected, and you are contributing to postoperative outcomes to the benefit of the patient.”
Perioperative patient management is also financially rewarding because reimbursement is higher than customary hospital medicine duties.
Dr. Jaffer, soon to be chief of the division of hospital medicine at the University of Miami Medical Center in Florida, is proud of the work he and his colleagues have done to grow the Cleveland Clinic perioperative summit. This third summit, in September, was organized in collaboration with the Society of Perioperative Assessment and Quality Improvement.
“I think this is something that every hospitalist should try,” Dr. Usmani says. “It is definitely a niche.” TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Mangano DT. Perioperative medicine: NHLBI working group deliberations and recommendations. J Cardiothorac Vasc Anesth. 2004;18(1):1-6.
- Adebola O, Adesanya AO, Joshi GP. Hospitalists and anesthesiologists as perioperative physicians: Are their roles complementary? Proc. (Bayl Univ Med Cent) 2007 April;20(2):140-142.
New limits on resident work hours and the graying of the U.S. population are putting hospitalists in the forefront of helping surgeons manage their patients.
Because the Accreditation Council for Graduate Medical Education restricted resident duty hours, surgeons can no longer rely automatically on residents to medically manage their patients on the floors, says Amir K. Jaffer, MD, a hospitalist and an associate professor of medicine at the Cleveland Clinic Lerner College of Medicine of Case Western Reserve University in Ohio.
Meanwhile, the population over age 65 will double, increasing to 70 million over the next 10 to 15 years.1
“More patients living longer means an increase in surgeries along the way,” says Dr. Jaffer, who is also the medical director of the Internal Medicine Preoperative Assessment Consultation and Treatment program in the section of hospital medicine at the Cleveland Clinic. For him, the first place hospitalists need to co-manage is in the postoperative setting.
“Studies have suggested that as patients age there is an increase in cardiological complications, noncardiological complications, pulmonary complications, and overall mortality,” he continues. “In my opinion there is going to be a crisis in regard to managing medical issues and complications surrounding surgery.” (See Table 1, p. 24)
Medications issues are another major reason hospitalists are called for surgical consults, says Benny Gavi, MD, hospitalist at Stanford Hospitals and Clinics in Calif. “I got consulted for a patient with tachycardia in the inpatient setting,” says Dr. Gavi. “By the time we saw the patient, the orthopedic surgeon had already ordered an echocardiogram and added a beta-blocker. When I looked at the patient I realized he had a gout flare; the colchicine that he took daily for his gout was never started in the inpatient setting, which ultimately delayed his physical therapy and added three additional days to his hospital stay.”
Co-management makes sense for still other reasons, he says.
“The knowledge base of both surgery and medicine is growing rapidly; no one person can remain on top of what is needed for both fields,” says Dr. Gavi. “In the last 20 years there has been a dramatic rise in the number of medications and some are very complicated. Also, physicians and surgeons both are being approached to participate more in quality initiatives and increasing throughput. As a result, physicians have to work faster and do more.”
Opportunities
In the United States, approximately 100,000 surgeries are performed each day and 36 million surgeries are performed each year at a cost of $450 billion annually. More than 1 million serious surgical adverse events each year cost $45 billion. Within two decades, the surgeries will increase by 25%, the associated cost will increase 50%, and the cost of in-hospital and long-term complications will increase 100%.
Along with postoperative care, there are increasing opportunities in the preoperative setting.
“At our institution, which is a tertiary care center with a huge surgical hospital, we determined that there was a need for hospitalists to provide medical management of surgical patients 10 years ago,” Dr. Jaffer says. “Patients were often not adequately prepared when they went to surgery, and sometimes in the morning of surgery the anesthesiologists would cancel their cases.”
The traditional model of physicians calling in consultants when problems arise might need to change.
“We are increasingly looking for ways to identify patients who have a high likelihood of developing medical problems and proactively getting involved,” says Dr. Gavi.
To co-manage, hospitalists must take ownership of some medical issues under specific conditions (diabetes, anticoagulation, blood pressure), says Dr. Jaffer.
The Benefits
To Latha Sivaprasad, MD, hospitalist at Beth Israel Medical Center in New York City, there are three main advantages of hospitalists’ involvement in perioperative co-management:
- Hospitalists typically perform comprehensive, multisystemic patient evaluations;
- Hospitalists are extremely accessible; and
- Hospitalists are up to date on inpatient medicine.
How up to date?
“Periop isn’t routinely taught in residency,” says Ali Usmani, MD, a hospitalist at the Cleveland Clinic. “In fact, I had little information about perioperative care.”
When he joined the hospitalist group after a three-year residency at Cleveland Clinic, Dr. Usmani did preparatory reading. Later, the hospitalist group gave him a helpful collection of essays.
“I was very nervous because, of course, I had never done this before,” he says. “Surprisingly, I also had not done a general medicine consult service where we see postoperative patients. It was scary to some extent, but I found out that it is easier than I thought because there are guidelines you can follow from the AHA/ACC that are fairly straightforward. It also meant a nice schedule change from being on the floors.”
Although conducting preoperative evaluations with patients was technically outpatient work, it was not like he was seeing patients with such simple illnesses as a cold or a sore throat. Also, he says, there were no new surprises postoperatively because either he or a hospitalist colleague had seen the patient preoperatively.
Dr. Usmani, also a clinical assistant professor of medicine at Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, believes patients are happier when seen by hospitalists because they get a standardized, holistic preoperative assessment. And, helping to reduce the number of unnecessary tests ordered by primary care physicians or surgeons makes him feel as though he’s making a valuable contribution.
New Niche
Dr. Sivaprasad, who is also doing a one-year fellowship in quality improvement and patient safety at Beth Israel, has practiced hospital medicine in four hospitals ranging from 500 to 1,000 beds. “The primary reason we are consulted by surgeons is for perioperative cardiac risk assessment,” says Dr. Sivaprasad. “Other reasons include co-managing a patient with comorbidities such as a history of diabetes, hypertension, or renal failure.”
From 2003-2006, Dr. Sivaprasad was one of 14 hospitalists consulted often by surgeons at St. John’s Mercy Hospital in St Louis, a 1,000-bed Level I trauma center. “We were consulted for postoperative co-management, preoperative evaluation, or more urgent cases such as a patient experiencing hypotension, atrial fibrillation, shortness of breath, decreased urine output, or renal failure,” she says.
Dr. Sivaprasad recently attended the Johns Hopkins conference on Perioperative Management. The session made it easier for her to do a systems-based consult.
“All hospitalists differ to the degree of perioperative medicine they feel comfortable with,” she says. “Hospitalists understand perioperative medicine on different levels. They all can do an acceptable consult; but there is a spectrum of how detailed one can be and what service one can provide for the surgeon and the patient.”
Dr. Jaffer finds his work in perioperative care fulfilling and considers it another way hospitalists can increase their influence.
“Often when you manage medical patients in the hospital, it’s you, the medical patient, and the patient’s primary care physician,” Dr. Jaffer says. “But when you start to manage surgical patients, you are really being looked at by your surgical colleagues as an expert in managing medical problems, just as you view them as experts in managing surgical problems. What I realize from this is that I can be a perioperative medicine expert as well.”
Are there any downfalls to co-managing surgical patients?
“Sometimes the surgeons order unnecessary lab tests such as PTTs [partial thromboplastin time] because they are concerned about bleeding and complications,” Dr. Usmani says. “The next day if there is a deranged PTT, we need to figure out whether to suggest postponing the surgery or go ahead with the surgery based on the patients’ past medical/family history. We try to get our surgeons and our colleagues to work together with us in that regard because they don’t want to postpone surgery either.”
Drs. Usmani, Gavi, Jaffer, and Sivaprasad all say that when surgeons can observe firsthand their hospitalist partners exhibiting expertise in acute care it appears to improve surgeons’ attitudes about the role and value of hospitalists.
In fact, says Dr. Usmani, surgeons call him or one of his colleagues to thank them. “They say, ‘We really appreciate what you’ve done for this patient,’ ’’ he says. “Even if we suggest canceling surgery, they respect that we have seen a potential problem instead of letting it go ahead. They are happy to receive this advice.”
Another new relationship is between anesthesiologists and hospitalists. “I spend a lot of time calling anesthesiologists in regard to patient cases, and a good many of them are surprised to get a call from a hospitalist,” Dr. Gavi says. “We especially work closely together when we get complicated patients ready for surgery.”
A recent encounter proved to Dr. Gavi the complementary nature of the hospitalist-anesthesiologist relationship.2
“A patient came to the hospital two weeks ago to have an elective total knee replacement,” says Dr. Gavi. “She was an older woman with severe pulmonary disease. When the anesthesiologists saw her in the preoperative waiting area and realized how sick she is, they wanted to cancel the surgery. But the surgeon told the anesthesiologist that this patient had been seen in our own preoperative clinic and cleared by a hospitalist.”
Dr. Gavi had done what is customary for an internist. He took a more in-depth look at her pulmonology and cardiac records, called her cardiologist for further history, and reassured the anesthesiologist and surgeon. The patient had her surgery.
The Future
“Perioperative co-management is becoming more of a visible need,” says Dr. Sivaprasad. “It bridges the gap between surgeons and internists.”
To those of his hospitalist colleagues who have little information and are a bit afraid to begin perioperative care practice, Dr. Usmani recommends attending a perioperative summit conference.
The session should teach how to set up a perioperative center and what to do when managing patients with certain conditions.
“Although you meet with patients preoperatively in an office setting, you don’t feel like a primary care physician,” Dr. Usmani says. “You feel as if you are a specialist. You are respected, and you are contributing to postoperative outcomes to the benefit of the patient.”
Perioperative patient management is also financially rewarding because reimbursement is higher than customary hospital medicine duties.
Dr. Jaffer, soon to be chief of the division of hospital medicine at the University of Miami Medical Center in Florida, is proud of the work he and his colleagues have done to grow the Cleveland Clinic perioperative summit. This third summit, in September, was organized in collaboration with the Society of Perioperative Assessment and Quality Improvement.
“I think this is something that every hospitalist should try,” Dr. Usmani says. “It is definitely a niche.” TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Mangano DT. Perioperative medicine: NHLBI working group deliberations and recommendations. J Cardiothorac Vasc Anesth. 2004;18(1):1-6.
- Adebola O, Adesanya AO, Joshi GP. Hospitalists and anesthesiologists as perioperative physicians: Are their roles complementary? Proc. (Bayl Univ Med Cent) 2007 April;20(2):140-142.
New limits on resident work hours and the graying of the U.S. population are putting hospitalists in the forefront of helping surgeons manage their patients.
Because the Accreditation Council for Graduate Medical Education restricted resident duty hours, surgeons can no longer rely automatically on residents to medically manage their patients on the floors, says Amir K. Jaffer, MD, a hospitalist and an associate professor of medicine at the Cleveland Clinic Lerner College of Medicine of Case Western Reserve University in Ohio.
Meanwhile, the population over age 65 will double, increasing to 70 million over the next 10 to 15 years.1
“More patients living longer means an increase in surgeries along the way,” says Dr. Jaffer, who is also the medical director of the Internal Medicine Preoperative Assessment Consultation and Treatment program in the section of hospital medicine at the Cleveland Clinic. For him, the first place hospitalists need to co-manage is in the postoperative setting.
“Studies have suggested that as patients age there is an increase in cardiological complications, noncardiological complications, pulmonary complications, and overall mortality,” he continues. “In my opinion there is going to be a crisis in regard to managing medical issues and complications surrounding surgery.” (See Table 1, p. 24)
Medications issues are another major reason hospitalists are called for surgical consults, says Benny Gavi, MD, hospitalist at Stanford Hospitals and Clinics in Calif. “I got consulted for a patient with tachycardia in the inpatient setting,” says Dr. Gavi. “By the time we saw the patient, the orthopedic surgeon had already ordered an echocardiogram and added a beta-blocker. When I looked at the patient I realized he had a gout flare; the colchicine that he took daily for his gout was never started in the inpatient setting, which ultimately delayed his physical therapy and added three additional days to his hospital stay.”
Co-management makes sense for still other reasons, he says.
“The knowledge base of both surgery and medicine is growing rapidly; no one person can remain on top of what is needed for both fields,” says Dr. Gavi. “In the last 20 years there has been a dramatic rise in the number of medications and some are very complicated. Also, physicians and surgeons both are being approached to participate more in quality initiatives and increasing throughput. As a result, physicians have to work faster and do more.”
Opportunities
In the United States, approximately 100,000 surgeries are performed each day and 36 million surgeries are performed each year at a cost of $450 billion annually. More than 1 million serious surgical adverse events each year cost $45 billion. Within two decades, the surgeries will increase by 25%, the associated cost will increase 50%, and the cost of in-hospital and long-term complications will increase 100%.
Along with postoperative care, there are increasing opportunities in the preoperative setting.
“At our institution, which is a tertiary care center with a huge surgical hospital, we determined that there was a need for hospitalists to provide medical management of surgical patients 10 years ago,” Dr. Jaffer says. “Patients were often not adequately prepared when they went to surgery, and sometimes in the morning of surgery the anesthesiologists would cancel their cases.”
The traditional model of physicians calling in consultants when problems arise might need to change.
“We are increasingly looking for ways to identify patients who have a high likelihood of developing medical problems and proactively getting involved,” says Dr. Gavi.
To co-manage, hospitalists must take ownership of some medical issues under specific conditions (diabetes, anticoagulation, blood pressure), says Dr. Jaffer.
The Benefits
To Latha Sivaprasad, MD, hospitalist at Beth Israel Medical Center in New York City, there are three main advantages of hospitalists’ involvement in perioperative co-management:
- Hospitalists typically perform comprehensive, multisystemic patient evaluations;
- Hospitalists are extremely accessible; and
- Hospitalists are up to date on inpatient medicine.
How up to date?
“Periop isn’t routinely taught in residency,” says Ali Usmani, MD, a hospitalist at the Cleveland Clinic. “In fact, I had little information about perioperative care.”
When he joined the hospitalist group after a three-year residency at Cleveland Clinic, Dr. Usmani did preparatory reading. Later, the hospitalist group gave him a helpful collection of essays.
“I was very nervous because, of course, I had never done this before,” he says. “Surprisingly, I also had not done a general medicine consult service where we see postoperative patients. It was scary to some extent, but I found out that it is easier than I thought because there are guidelines you can follow from the AHA/ACC that are fairly straightforward. It also meant a nice schedule change from being on the floors.”
Although conducting preoperative evaluations with patients was technically outpatient work, it was not like he was seeing patients with such simple illnesses as a cold or a sore throat. Also, he says, there were no new surprises postoperatively because either he or a hospitalist colleague had seen the patient preoperatively.
Dr. Usmani, also a clinical assistant professor of medicine at Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, believes patients are happier when seen by hospitalists because they get a standardized, holistic preoperative assessment. And, helping to reduce the number of unnecessary tests ordered by primary care physicians or surgeons makes him feel as though he’s making a valuable contribution.
New Niche
Dr. Sivaprasad, who is also doing a one-year fellowship in quality improvement and patient safety at Beth Israel, has practiced hospital medicine in four hospitals ranging from 500 to 1,000 beds. “The primary reason we are consulted by surgeons is for perioperative cardiac risk assessment,” says Dr. Sivaprasad. “Other reasons include co-managing a patient with comorbidities such as a history of diabetes, hypertension, or renal failure.”
From 2003-2006, Dr. Sivaprasad was one of 14 hospitalists consulted often by surgeons at St. John’s Mercy Hospital in St Louis, a 1,000-bed Level I trauma center. “We were consulted for postoperative co-management, preoperative evaluation, or more urgent cases such as a patient experiencing hypotension, atrial fibrillation, shortness of breath, decreased urine output, or renal failure,” she says.
Dr. Sivaprasad recently attended the Johns Hopkins conference on Perioperative Management. The session made it easier for her to do a systems-based consult.
“All hospitalists differ to the degree of perioperative medicine they feel comfortable with,” she says. “Hospitalists understand perioperative medicine on different levels. They all can do an acceptable consult; but there is a spectrum of how detailed one can be and what service one can provide for the surgeon and the patient.”
Dr. Jaffer finds his work in perioperative care fulfilling and considers it another way hospitalists can increase their influence.
“Often when you manage medical patients in the hospital, it’s you, the medical patient, and the patient’s primary care physician,” Dr. Jaffer says. “But when you start to manage surgical patients, you are really being looked at by your surgical colleagues as an expert in managing medical problems, just as you view them as experts in managing surgical problems. What I realize from this is that I can be a perioperative medicine expert as well.”
Are there any downfalls to co-managing surgical patients?
“Sometimes the surgeons order unnecessary lab tests such as PTTs [partial thromboplastin time] because they are concerned about bleeding and complications,” Dr. Usmani says. “The next day if there is a deranged PTT, we need to figure out whether to suggest postponing the surgery or go ahead with the surgery based on the patients’ past medical/family history. We try to get our surgeons and our colleagues to work together with us in that regard because they don’t want to postpone surgery either.”
Drs. Usmani, Gavi, Jaffer, and Sivaprasad all say that when surgeons can observe firsthand their hospitalist partners exhibiting expertise in acute care it appears to improve surgeons’ attitudes about the role and value of hospitalists.
In fact, says Dr. Usmani, surgeons call him or one of his colleagues to thank them. “They say, ‘We really appreciate what you’ve done for this patient,’ ’’ he says. “Even if we suggest canceling surgery, they respect that we have seen a potential problem instead of letting it go ahead. They are happy to receive this advice.”
Another new relationship is between anesthesiologists and hospitalists. “I spend a lot of time calling anesthesiologists in regard to patient cases, and a good many of them are surprised to get a call from a hospitalist,” Dr. Gavi says. “We especially work closely together when we get complicated patients ready for surgery.”
A recent encounter proved to Dr. Gavi the complementary nature of the hospitalist-anesthesiologist relationship.2
“A patient came to the hospital two weeks ago to have an elective total knee replacement,” says Dr. Gavi. “She was an older woman with severe pulmonary disease. When the anesthesiologists saw her in the preoperative waiting area and realized how sick she is, they wanted to cancel the surgery. But the surgeon told the anesthesiologist that this patient had been seen in our own preoperative clinic and cleared by a hospitalist.”
Dr. Gavi had done what is customary for an internist. He took a more in-depth look at her pulmonology and cardiac records, called her cardiologist for further history, and reassured the anesthesiologist and surgeon. The patient had her surgery.
The Future
“Perioperative co-management is becoming more of a visible need,” says Dr. Sivaprasad. “It bridges the gap between surgeons and internists.”
To those of his hospitalist colleagues who have little information and are a bit afraid to begin perioperative care practice, Dr. Usmani recommends attending a perioperative summit conference.
The session should teach how to set up a perioperative center and what to do when managing patients with certain conditions.
“Although you meet with patients preoperatively in an office setting, you don’t feel like a primary care physician,” Dr. Usmani says. “You feel as if you are a specialist. You are respected, and you are contributing to postoperative outcomes to the benefit of the patient.”
Perioperative patient management is also financially rewarding because reimbursement is higher than customary hospital medicine duties.
Dr. Jaffer, soon to be chief of the division of hospital medicine at the University of Miami Medical Center in Florida, is proud of the work he and his colleagues have done to grow the Cleveland Clinic perioperative summit. This third summit, in September, was organized in collaboration with the Society of Perioperative Assessment and Quality Improvement.
“I think this is something that every hospitalist should try,” Dr. Usmani says. “It is definitely a niche.” TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Mangano DT. Perioperative medicine: NHLBI working group deliberations and recommendations. J Cardiothorac Vasc Anesth. 2004;18(1):1-6.
- Adebola O, Adesanya AO, Joshi GP. Hospitalists and anesthesiologists as perioperative physicians: Are their roles complementary? Proc. (Bayl Univ Med Cent) 2007 April;20(2):140-142.