User login
Voters Weigh in Early
A poll by the Kaiser Family Foundation in August found that healthcare is the top domestic issue that the public wants presidential candidates to address.
Republicans and independent voters ranked healthcare second only to Iraq in the poll, while for the first time, Democrats ranked the two issues as equally important for the candidates to discuss as they campaign.
With more voters interested in changes to American healthcare—which is really shorthand for affordable access to health insurance coverage—the presidential candidates are also showing interest. Sort of.
Some, including John Edwards, Barack Obama, Hillary Clinton, and Mitt Romney, have a broad plan or opinion in place. Others, such as Mike Huckabee and John McCain, have not yet shared a plan.
As the election progresses—or even after a new president is sworn into office—will we see any real changes to healthcare access? “There has to be [some change],” states Bradley Flansbaum, DO, MPH, chief of hospitalist section at Lenox Hill Hospital in New York, N.Y. “We’ve reached a tipping point. You can’t continue to play kick the can.” The impetus for change, Dr. Flansbaum believes, will not be public opinion so much as money.
“I think that we’re reaching a critical mass, and that premiums will drive the change,” he predicts. “Employers can’t afford insurance benefits any more, and now that employers are changing plans and employees are paying more and faced with higher premiums, I think the house of cards will collapse.”
Laura Allendorf, SHM’s senior adviser for advocacy and government affairs, agrees change is in the air.
“I do think there are better opportunities for action than there have been in the past,” she says. “Various polls show that healthcare [access] is an important issue. That’s why so many candidates are developing proposals on this, or already have a proposal.” She adds, “A U.S. Census Bureau report just came out showing an increase in the number of unemployed—this will lend pressure for policymakers.”
Where Will the Trail Lead?
Campaigning for the 2008 election is in full swing, and no one is surprised the candidates lack firm or detailed opinions on healthcare access. But what can we expect to see in the next year of campaigning?
“As much as Hillary [Clinton] is a lightening rod in some ways, she’s going to be driving the debate on this,” predicts Dr. Flansbaum. “As we get closer to the election and the second- and third-tier candidates start to come apart, she’ll be the one leading the healthcare debate.”
In general, Democrats and Republicans have settled into two camps on the issue.
“It’s easy to say, ‘Don’t listen to the Democrats—they want socialized medicine,’ while the Democrats are saying ‘The Republicans want corporate America to take over,’” says Dr. Flansbaum. “They’re playing games right now. I can’t say if a purely government or a purely corporate system would work, but we probably need and are going to get a mixture of both.” After the election, he says, “There’s got to be some compromise in the middle.”
What about other healthcare issues besides the rising costs and lack of access? “In addition to access, quality improvement is certainly key,” says Allendorf.
For Dr. Flansbaum, everything is connected to access, including healthcare IT, informatics, quality reporting, cost control, and waste reduction.
Hail to the New Chief
Once a new president and his or her administration is in place, will the concerns—and possibly the campaign promises—over healthcare access be dropped?
“Definitely something would—or rather, should—be done,” says Allendorf. “The two parties obviously have different philosophic approaches, but if [the next president] listens to the voters, they’ll act. The voters have spoken.” And if no action is taken on the issues, Allendorf adds, “It’s up to associations like SHM to push for reform.”
But Dr. Flansbaum warns that whatever the change is, it won’t happen overnight.
“There are too many lobbyists and people with their hand in the till to turn this around overnight,” states Dr. Flansbaum. “It will be an incremental change, and it will probably start out like the Massachusetts plan.”
Beginning July 1, Massachusetts enacted a law designed to cover the state’s uninsured population. The law mandates that individuals purchase health insurance with government subsidies to ensure affordability.

—Laura Allendorf, SHM’s senior adviser for advocacy and government affairs
Physician, Educate Thyself
The next year promises more campaigning, including debates and town hall forums, updated Web sites, media interviews, and so on. Allendorf says that as the candidates change and their positions on healthcare issues are fleshed out and become more apparent.
“SHM will provide information through our usual channels and publications about the candidates’ positions as they gel,” she says. “We’ll probably also want to hear from any SHM members who are involved in working with candidates on their positions, crafting proposals or working on healthcare advisory groups.”
For information on the candidates’ healthcare access positions, you can download an August report from the Council for Affordable Health Insurance, “The 2008 Presidential Candidates on Health Care Reform,” from www.cahi.org.
You can also find nonpartisan, up-to-date information about candidates’ healthcare policy, as well as analysis of health policy issues, regular public opinion surveys, and news coverage, on a site hosted by the Kaiser Family Foundation: www.health08.org. TH
Jane Jerrard has been writing for The Hospitalist since 2005.
A poll by the Kaiser Family Foundation in August found that healthcare is the top domestic issue that the public wants presidential candidates to address.
Republicans and independent voters ranked healthcare second only to Iraq in the poll, while for the first time, Democrats ranked the two issues as equally important for the candidates to discuss as they campaign.
With more voters interested in changes to American healthcare—which is really shorthand for affordable access to health insurance coverage—the presidential candidates are also showing interest. Sort of.
Some, including John Edwards, Barack Obama, Hillary Clinton, and Mitt Romney, have a broad plan or opinion in place. Others, such as Mike Huckabee and John McCain, have not yet shared a plan.
As the election progresses—or even after a new president is sworn into office—will we see any real changes to healthcare access? “There has to be [some change],” states Bradley Flansbaum, DO, MPH, chief of hospitalist section at Lenox Hill Hospital in New York, N.Y. “We’ve reached a tipping point. You can’t continue to play kick the can.” The impetus for change, Dr. Flansbaum believes, will not be public opinion so much as money.
“I think that we’re reaching a critical mass, and that premiums will drive the change,” he predicts. “Employers can’t afford insurance benefits any more, and now that employers are changing plans and employees are paying more and faced with higher premiums, I think the house of cards will collapse.”
Laura Allendorf, SHM’s senior adviser for advocacy and government affairs, agrees change is in the air.
“I do think there are better opportunities for action than there have been in the past,” she says. “Various polls show that healthcare [access] is an important issue. That’s why so many candidates are developing proposals on this, or already have a proposal.” She adds, “A U.S. Census Bureau report just came out showing an increase in the number of unemployed—this will lend pressure for policymakers.”
Where Will the Trail Lead?
Campaigning for the 2008 election is in full swing, and no one is surprised the candidates lack firm or detailed opinions on healthcare access. But what can we expect to see in the next year of campaigning?
“As much as Hillary [Clinton] is a lightening rod in some ways, she’s going to be driving the debate on this,” predicts Dr. Flansbaum. “As we get closer to the election and the second- and third-tier candidates start to come apart, she’ll be the one leading the healthcare debate.”
In general, Democrats and Republicans have settled into two camps on the issue.
“It’s easy to say, ‘Don’t listen to the Democrats—they want socialized medicine,’ while the Democrats are saying ‘The Republicans want corporate America to take over,’” says Dr. Flansbaum. “They’re playing games right now. I can’t say if a purely government or a purely corporate system would work, but we probably need and are going to get a mixture of both.” After the election, he says, “There’s got to be some compromise in the middle.”
What about other healthcare issues besides the rising costs and lack of access? “In addition to access, quality improvement is certainly key,” says Allendorf.
For Dr. Flansbaum, everything is connected to access, including healthcare IT, informatics, quality reporting, cost control, and waste reduction.
Hail to the New Chief
Once a new president and his or her administration is in place, will the concerns—and possibly the campaign promises—over healthcare access be dropped?
“Definitely something would—or rather, should—be done,” says Allendorf. “The two parties obviously have different philosophic approaches, but if [the next president] listens to the voters, they’ll act. The voters have spoken.” And if no action is taken on the issues, Allendorf adds, “It’s up to associations like SHM to push for reform.”
But Dr. Flansbaum warns that whatever the change is, it won’t happen overnight.
“There are too many lobbyists and people with their hand in the till to turn this around overnight,” states Dr. Flansbaum. “It will be an incremental change, and it will probably start out like the Massachusetts plan.”
Beginning July 1, Massachusetts enacted a law designed to cover the state’s uninsured population. The law mandates that individuals purchase health insurance with government subsidies to ensure affordability.
—Laura Allendorf, SHM’s senior adviser for advocacy and government affairs
Physician, Educate Thyself
The next year promises more campaigning, including debates and town hall forums, updated Web sites, media interviews, and so on. Allendorf says that as the candidates change and their positions on healthcare issues are fleshed out and become more apparent.
“SHM will provide information through our usual channels and publications about the candidates’ positions as they gel,” she says. “We’ll probably also want to hear from any SHM members who are involved in working with candidates on their positions, crafting proposals or working on healthcare advisory groups.”
For information on the candidates’ healthcare access positions, you can download an August report from the Council for Affordable Health Insurance, “The 2008 Presidential Candidates on Health Care Reform,” from www.cahi.org.
You can also find nonpartisan, up-to-date information about candidates’ healthcare policy, as well as analysis of health policy issues, regular public opinion surveys, and news coverage, on a site hosted by the Kaiser Family Foundation: www.health08.org. TH
Jane Jerrard has been writing for The Hospitalist since 2005.
A poll by the Kaiser Family Foundation in August found that healthcare is the top domestic issue that the public wants presidential candidates to address.
Republicans and independent voters ranked healthcare second only to Iraq in the poll, while for the first time, Democrats ranked the two issues as equally important for the candidates to discuss as they campaign.
With more voters interested in changes to American healthcare—which is really shorthand for affordable access to health insurance coverage—the presidential candidates are also showing interest. Sort of.
Some, including John Edwards, Barack Obama, Hillary Clinton, and Mitt Romney, have a broad plan or opinion in place. Others, such as Mike Huckabee and John McCain, have not yet shared a plan.
As the election progresses—or even after a new president is sworn into office—will we see any real changes to healthcare access? “There has to be [some change],” states Bradley Flansbaum, DO, MPH, chief of hospitalist section at Lenox Hill Hospital in New York, N.Y. “We’ve reached a tipping point. You can’t continue to play kick the can.” The impetus for change, Dr. Flansbaum believes, will not be public opinion so much as money.
“I think that we’re reaching a critical mass, and that premiums will drive the change,” he predicts. “Employers can’t afford insurance benefits any more, and now that employers are changing plans and employees are paying more and faced with higher premiums, I think the house of cards will collapse.”
Laura Allendorf, SHM’s senior adviser for advocacy and government affairs, agrees change is in the air.
“I do think there are better opportunities for action than there have been in the past,” she says. “Various polls show that healthcare [access] is an important issue. That’s why so many candidates are developing proposals on this, or already have a proposal.” She adds, “A U.S. Census Bureau report just came out showing an increase in the number of unemployed—this will lend pressure for policymakers.”
Where Will the Trail Lead?
Campaigning for the 2008 election is in full swing, and no one is surprised the candidates lack firm or detailed opinions on healthcare access. But what can we expect to see in the next year of campaigning?
“As much as Hillary [Clinton] is a lightening rod in some ways, she’s going to be driving the debate on this,” predicts Dr. Flansbaum. “As we get closer to the election and the second- and third-tier candidates start to come apart, she’ll be the one leading the healthcare debate.”
In general, Democrats and Republicans have settled into two camps on the issue.
“It’s easy to say, ‘Don’t listen to the Democrats—they want socialized medicine,’ while the Democrats are saying ‘The Republicans want corporate America to take over,’” says Dr. Flansbaum. “They’re playing games right now. I can’t say if a purely government or a purely corporate system would work, but we probably need and are going to get a mixture of both.” After the election, he says, “There’s got to be some compromise in the middle.”
What about other healthcare issues besides the rising costs and lack of access? “In addition to access, quality improvement is certainly key,” says Allendorf.
For Dr. Flansbaum, everything is connected to access, including healthcare IT, informatics, quality reporting, cost control, and waste reduction.
Hail to the New Chief
Once a new president and his or her administration is in place, will the concerns—and possibly the campaign promises—over healthcare access be dropped?
“Definitely something would—or rather, should—be done,” says Allendorf. “The two parties obviously have different philosophic approaches, but if [the next president] listens to the voters, they’ll act. The voters have spoken.” And if no action is taken on the issues, Allendorf adds, “It’s up to associations like SHM to push for reform.”
But Dr. Flansbaum warns that whatever the change is, it won’t happen overnight.
“There are too many lobbyists and people with their hand in the till to turn this around overnight,” states Dr. Flansbaum. “It will be an incremental change, and it will probably start out like the Massachusetts plan.”
Beginning July 1, Massachusetts enacted a law designed to cover the state’s uninsured population. The law mandates that individuals purchase health insurance with government subsidies to ensure affordability.
—Laura Allendorf, SHM’s senior adviser for advocacy and government affairs
Physician, Educate Thyself
The next year promises more campaigning, including debates and town hall forums, updated Web sites, media interviews, and so on. Allendorf says that as the candidates change and their positions on healthcare issues are fleshed out and become more apparent.
“SHM will provide information through our usual channels and publications about the candidates’ positions as they gel,” she says. “We’ll probably also want to hear from any SHM members who are involved in working with candidates on their positions, crafting proposals or working on healthcare advisory groups.”
For information on the candidates’ healthcare access positions, you can download an August report from the Council for Affordable Health Insurance, “The 2008 Presidential Candidates on Health Care Reform,” from www.cahi.org.
You can also find nonpartisan, up-to-date information about candidates’ healthcare policy, as well as analysis of health policy issues, regular public opinion surveys, and news coverage, on a site hosted by the Kaiser Family Foundation: www.health08.org. TH
Jane Jerrard has been writing for The Hospitalist since 2005.
Administrative Ambition
Interested in a promotion? If you have your eye on an administrative career, go ahead and think big—because the opportunities for today’s hospitalists are there for the taking, with some planning and the careful acquisition of skills, experience, and training.
“Any hospitalist who has any desire to be a leader, whether in a medical practice or in a hospital, has numerous opportunities,” says Patrick Cawley, MD, chief medical officer of Medical University of South Carolina (MUSC) Medical Center in Charleston. “If you’re willing to step up, you can attain that leadership position.”
Plan Your Path
Ambitious hospitalists must consider the administrative positions available to them in the long run.
“Within a hospital medicine practice, you have just one director,” says Joan C. Faro, MD, FACP, MBA, chief medical officer, John T. Mather Memorial Hospital, Port Jefferson, N.Y. “So people working in the ranks need to be creative and come up with ideas on gaining experience, such as creating a QA position.” She advises hospitalists to look at the job description and the performance measures of the director’s position to see what expectations come with the job.
The promotion to director may involve switching practices. “If you want to move quickly, you have to be able to move [to a different group],” explains Dr. Cawley. “In a local community, there will be others ahead of you. If you’re willing to move to a less-than-ideal location, you can find better opportunities.” For community-based hospitalists especially, the director’s position is a necessary one before moving higher up the administrative ladder.
“You need to be managing some people before you become a CMO [chief medical officer] or administrator,” explains Dr. Faro. “You really have to show that you can do some significant work. In academia, you can do this as a division chief or something like that.” As the director of a hospital medicine program, she says, “you can broaden your scope and move higher up into hospital administration.”
First Steps
How do you move from working hospitalist to director or department head? Start small.
“You can start with easy committee assignments,” says Dr. Cawley. “Even while you’re getting leadership training, you can be building those skills on the job. Start with small projects, such as small committee roles or quality management projects. You can then move up, but consider that you’ll need new skills as you do. Before you chair your first committee, you’ll have to brush up on how to run a meeting. You can progressively take on larger, broader roles.”
Enlist the help of your own leaders to help you get started.
“You could go to your CMO or your medical director—if they’re in a position to help—and ask what you need to do to get to the next step,” advises Dr. Faro. “You don’t need formal training at this point; test the waters, find what you’re interested in and make sure that leading change is something you enjoy before you [invest in] formal training.”
Dr. Faro was working as an internist in an academic medical setting when she discovered an affinity for leadership. “I went to my dean and asked to be put on committees,” she recalls. “I also worked in a volunteer capacity and did committee work for the local chapter of the American Heart Association. I ended up chairing a number of committees over the years. It just seemed to happen naturally because I enjoyed it. After these experiences, I knew I had a talent for working with disparate groups and getting things done.”
As you concentrate on committee work and project work, focus on building clinical and administrative skills.
“The most important things are having the right skills and experience,” stresses Dr. Cawley. “In my opinion, experience will count for more than skills, because people tend to assume that your skills improve as you gain experience. Experience is more important than an advanced degree, with the caveat that degrees are one way that leaders can prove themselves. Having that MBA or MPH doesn’t hurt, and it shows that you’re serious; it requires some dedication to earn that.”
Leadership Training A Must
If your committee and project experience assures you that you want to pursue a leadership path, says Dr. Cawley, “you really need leadership training. Now, is that an MBA or simply selective reading and coursework? That depends on what you want and how you want to go about it.”
However you decide to educate yourself, that leadership training should emphasize certain skills.
“You definitely need formal negotiation skills training,” says Dr. Cawley. “You should also train in how to deal with a physician who’s disruptive. You’ll need a little bit of financial training, and then leadership training itself—what is a leader and what are the expectations of a leader? These are the basics.”
Dr. Faro adds that communication skills and presentation skills are important for leaders. “These are things that physicians think they know— after all we all feel we communicate well and we need to talk to our patients—but there’s a difference between teaching your patients about medications and engaging an audience,” she warns. “It’s also important to understand your management or your leadership style.”
Leadership training is easy to find. “Every single organization has now recognized that being a leader is something that requires training,” Dr. Faro points out. Physician leadership training is offered by the American College of Healthcare Executives, the American College of Physician Executives, the American College of Physicians, and SHM.
Opportunities Abound
In the growing field of hospital medicine, opportunities for advancement are growing as well. “Within just a few years, you’d be surprised what level you can reach,” says Dr. Cawley.
“There is a lot of potential for leadership within hospital medicine groups, and for moving from leading a group to a leadership role at a hospital,” says Dr. Cawley. “But the leadership chasm [in healthcare today] extends to every area where physicians are providing care.
“To me, it’s all about opportunities, skills and experience. With these, you’ll find that the sky’s the limit.”
Dr. Faro believes hospitalists are in a perfect position to rise to administrative positions. “You are, by definition, working in an institution,’’ he says. “Hospital medicine is replete with opportunities for leadership—opportunities to start a team for quality endeavors, an IHI [Institute of Healthcare Improvement] campaign, look at medication reconciliation, DVT prophylaxis, or glucose control. There are so many right things for physicians to be doing in a hospital setting. In any hospital today, there are going to be opportunities.” TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
Interested in a promotion? If you have your eye on an administrative career, go ahead and think big—because the opportunities for today’s hospitalists are there for the taking, with some planning and the careful acquisition of skills, experience, and training.
“Any hospitalist who has any desire to be a leader, whether in a medical practice or in a hospital, has numerous opportunities,” says Patrick Cawley, MD, chief medical officer of Medical University of South Carolina (MUSC) Medical Center in Charleston. “If you’re willing to step up, you can attain that leadership position.”
Plan Your Path
Ambitious hospitalists must consider the administrative positions available to them in the long run.
“Within a hospital medicine practice, you have just one director,” says Joan C. Faro, MD, FACP, MBA, chief medical officer, John T. Mather Memorial Hospital, Port Jefferson, N.Y. “So people working in the ranks need to be creative and come up with ideas on gaining experience, such as creating a QA position.” She advises hospitalists to look at the job description and the performance measures of the director’s position to see what expectations come with the job.
The promotion to director may involve switching practices. “If you want to move quickly, you have to be able to move [to a different group],” explains Dr. Cawley. “In a local community, there will be others ahead of you. If you’re willing to move to a less-than-ideal location, you can find better opportunities.” For community-based hospitalists especially, the director’s position is a necessary one before moving higher up the administrative ladder.
“You need to be managing some people before you become a CMO [chief medical officer] or administrator,” explains Dr. Faro. “You really have to show that you can do some significant work. In academia, you can do this as a division chief or something like that.” As the director of a hospital medicine program, she says, “you can broaden your scope and move higher up into hospital administration.”
First Steps
How do you move from working hospitalist to director or department head? Start small.
“You can start with easy committee assignments,” says Dr. Cawley. “Even while you’re getting leadership training, you can be building those skills on the job. Start with small projects, such as small committee roles or quality management projects. You can then move up, but consider that you’ll need new skills as you do. Before you chair your first committee, you’ll have to brush up on how to run a meeting. You can progressively take on larger, broader roles.”
Enlist the help of your own leaders to help you get started.
“You could go to your CMO or your medical director—if they’re in a position to help—and ask what you need to do to get to the next step,” advises Dr. Faro. “You don’t need formal training at this point; test the waters, find what you’re interested in and make sure that leading change is something you enjoy before you [invest in] formal training.”
Dr. Faro was working as an internist in an academic medical setting when she discovered an affinity for leadership. “I went to my dean and asked to be put on committees,” she recalls. “I also worked in a volunteer capacity and did committee work for the local chapter of the American Heart Association. I ended up chairing a number of committees over the years. It just seemed to happen naturally because I enjoyed it. After these experiences, I knew I had a talent for working with disparate groups and getting things done.”
As you concentrate on committee work and project work, focus on building clinical and administrative skills.
“The most important things are having the right skills and experience,” stresses Dr. Cawley. “In my opinion, experience will count for more than skills, because people tend to assume that your skills improve as you gain experience. Experience is more important than an advanced degree, with the caveat that degrees are one way that leaders can prove themselves. Having that MBA or MPH doesn’t hurt, and it shows that you’re serious; it requires some dedication to earn that.”
Leadership Training A Must
If your committee and project experience assures you that you want to pursue a leadership path, says Dr. Cawley, “you really need leadership training. Now, is that an MBA or simply selective reading and coursework? That depends on what you want and how you want to go about it.”
However you decide to educate yourself, that leadership training should emphasize certain skills.
“You definitely need formal negotiation skills training,” says Dr. Cawley. “You should also train in how to deal with a physician who’s disruptive. You’ll need a little bit of financial training, and then leadership training itself—what is a leader and what are the expectations of a leader? These are the basics.”
Dr. Faro adds that communication skills and presentation skills are important for leaders. “These are things that physicians think they know— after all we all feel we communicate well and we need to talk to our patients—but there’s a difference between teaching your patients about medications and engaging an audience,” she warns. “It’s also important to understand your management or your leadership style.”
Leadership training is easy to find. “Every single organization has now recognized that being a leader is something that requires training,” Dr. Faro points out. Physician leadership training is offered by the American College of Healthcare Executives, the American College of Physician Executives, the American College of Physicians, and SHM.
Opportunities Abound
In the growing field of hospital medicine, opportunities for advancement are growing as well. “Within just a few years, you’d be surprised what level you can reach,” says Dr. Cawley.
“There is a lot of potential for leadership within hospital medicine groups, and for moving from leading a group to a leadership role at a hospital,” says Dr. Cawley. “But the leadership chasm [in healthcare today] extends to every area where physicians are providing care.
“To me, it’s all about opportunities, skills and experience. With these, you’ll find that the sky’s the limit.”
Dr. Faro believes hospitalists are in a perfect position to rise to administrative positions. “You are, by definition, working in an institution,’’ he says. “Hospital medicine is replete with opportunities for leadership—opportunities to start a team for quality endeavors, an IHI [Institute of Healthcare Improvement] campaign, look at medication reconciliation, DVT prophylaxis, or glucose control. There are so many right things for physicians to be doing in a hospital setting. In any hospital today, there are going to be opportunities.” TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
Interested in a promotion? If you have your eye on an administrative career, go ahead and think big—because the opportunities for today’s hospitalists are there for the taking, with some planning and the careful acquisition of skills, experience, and training.
“Any hospitalist who has any desire to be a leader, whether in a medical practice or in a hospital, has numerous opportunities,” says Patrick Cawley, MD, chief medical officer of Medical University of South Carolina (MUSC) Medical Center in Charleston. “If you’re willing to step up, you can attain that leadership position.”
Plan Your Path
Ambitious hospitalists must consider the administrative positions available to them in the long run.
“Within a hospital medicine practice, you have just one director,” says Joan C. Faro, MD, FACP, MBA, chief medical officer, John T. Mather Memorial Hospital, Port Jefferson, N.Y. “So people working in the ranks need to be creative and come up with ideas on gaining experience, such as creating a QA position.” She advises hospitalists to look at the job description and the performance measures of the director’s position to see what expectations come with the job.
The promotion to director may involve switching practices. “If you want to move quickly, you have to be able to move [to a different group],” explains Dr. Cawley. “In a local community, there will be others ahead of you. If you’re willing to move to a less-than-ideal location, you can find better opportunities.” For community-based hospitalists especially, the director’s position is a necessary one before moving higher up the administrative ladder.
“You need to be managing some people before you become a CMO [chief medical officer] or administrator,” explains Dr. Faro. “You really have to show that you can do some significant work. In academia, you can do this as a division chief or something like that.” As the director of a hospital medicine program, she says, “you can broaden your scope and move higher up into hospital administration.”
First Steps
How do you move from working hospitalist to director or department head? Start small.
“You can start with easy committee assignments,” says Dr. Cawley. “Even while you’re getting leadership training, you can be building those skills on the job. Start with small projects, such as small committee roles or quality management projects. You can then move up, but consider that you’ll need new skills as you do. Before you chair your first committee, you’ll have to brush up on how to run a meeting. You can progressively take on larger, broader roles.”
Enlist the help of your own leaders to help you get started.
“You could go to your CMO or your medical director—if they’re in a position to help—and ask what you need to do to get to the next step,” advises Dr. Faro. “You don’t need formal training at this point; test the waters, find what you’re interested in and make sure that leading change is something you enjoy before you [invest in] formal training.”
Dr. Faro was working as an internist in an academic medical setting when she discovered an affinity for leadership. “I went to my dean and asked to be put on committees,” she recalls. “I also worked in a volunteer capacity and did committee work for the local chapter of the American Heart Association. I ended up chairing a number of committees over the years. It just seemed to happen naturally because I enjoyed it. After these experiences, I knew I had a talent for working with disparate groups and getting things done.”
As you concentrate on committee work and project work, focus on building clinical and administrative skills.
“The most important things are having the right skills and experience,” stresses Dr. Cawley. “In my opinion, experience will count for more than skills, because people tend to assume that your skills improve as you gain experience. Experience is more important than an advanced degree, with the caveat that degrees are one way that leaders can prove themselves. Having that MBA or MPH doesn’t hurt, and it shows that you’re serious; it requires some dedication to earn that.”
Leadership Training A Must
If your committee and project experience assures you that you want to pursue a leadership path, says Dr. Cawley, “you really need leadership training. Now, is that an MBA or simply selective reading and coursework? That depends on what you want and how you want to go about it.”
However you decide to educate yourself, that leadership training should emphasize certain skills.
“You definitely need formal negotiation skills training,” says Dr. Cawley. “You should also train in how to deal with a physician who’s disruptive. You’ll need a little bit of financial training, and then leadership training itself—what is a leader and what are the expectations of a leader? These are the basics.”
Dr. Faro adds that communication skills and presentation skills are important for leaders. “These are things that physicians think they know— after all we all feel we communicate well and we need to talk to our patients—but there’s a difference between teaching your patients about medications and engaging an audience,” she warns. “It’s also important to understand your management or your leadership style.”
Leadership training is easy to find. “Every single organization has now recognized that being a leader is something that requires training,” Dr. Faro points out. Physician leadership training is offered by the American College of Healthcare Executives, the American College of Physician Executives, the American College of Physicians, and SHM.
Opportunities Abound
In the growing field of hospital medicine, opportunities for advancement are growing as well. “Within just a few years, you’d be surprised what level you can reach,” says Dr. Cawley.
“There is a lot of potential for leadership within hospital medicine groups, and for moving from leading a group to a leadership role at a hospital,” says Dr. Cawley. “But the leadership chasm [in healthcare today] extends to every area where physicians are providing care.
“To me, it’s all about opportunities, skills and experience. With these, you’ll find that the sky’s the limit.”
Dr. Faro believes hospitalists are in a perfect position to rise to administrative positions. “You are, by definition, working in an institution,’’ he says. “Hospital medicine is replete with opportunities for leadership—opportunities to start a team for quality endeavors, an IHI [Institute of Healthcare Improvement] campaign, look at medication reconciliation, DVT prophylaxis, or glucose control. There are so many right things for physicians to be doing in a hospital setting. In any hospital today, there are going to be opportunities.” TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
Drug Stents and Surgery

Drug-eluting stents (DES) are a medical success story: In the four years since they were approved, in-stent restenosis rates have gone from the 25%-30% associated with bare-metal stents to the single digits.
Thanks to this track record, the world market for stents has doubled to $5 billion—despite the fact patients with DES must take aspirin or clopidogrel to prevent thromboses.
It’s easy to forget not all questions concerning DES have been answered, despite their wide acceptance and good overall outcomes.
One concern is discontinuation of antiplatelet therapy for DES patients who require noncardiac surgery.
In the November-December 2007 Journal of Hospital Medicine, senior author Amir Jaffer, MD, and colleagues at the Cleveland Clinic in Ohio studied the relationship between a patient’s time on antiplatelet medication and the consequences of discontinuing those agents in preparation for surgery.
“This is a common clinical conundrum,” says Dr. Jaffer, director of the Cleveland Clinic’s Internal Medicine Preoperative Assessment Consultation and Treatment (IMPACT) Center. “We face this question almost every day in our practice relative to perioperative care.”
Patients slated for noncardiac surgery are seen first at the IMPACT center, where hospitalists conduct the preoperative evaluation.
Data show that patients with bare-metal stents run a high risk of stent thrombosis if they undergo noncardiac surgery within two to six weeks of stent placement.
But information on DES is hard to come by, “so we decided to try to get a handle on the safety of stopping these drugs,” says Dr. Jaffer.
The authors, led by Daniel J. Brotman, MD, studied all patients who had undergone DES placement and were evaluated for noncardiac surgery at the IMPACT Center from July 2003 to July 2005. They examined 30-day rates of postoperative myocardial infarction (MI), DES thrombosis, major bleeding, and all-cause mortality—all relative to how long the patient had been on and off antiplatelet therapy.
The type of surgery each patient underwent was classified by invasiveness and anticipated blood loss, according to the system developed by L. Reuven Pasternak, MD, vice dean, Bayview Campus, Johns Hopkins University in Baltimore, and his colleagues.1
The categories range from one, which includes cystoscopy, breast biopsy, and other minor procedures that involve little if any blood loss, to five, which encompasses highly invasive procedures with anticipated blood losses in excess of 1,500 cc, such as major vascular repair.
A total of 114 patients met the study criteria. Seventy-five (66%) of the patients were men, and the median age was 71.
The most common comorbidities were diabetes (in 41% of patients), a history of coronary bypass (34%), and chronic renal insufficiency (20%). Most patients (73%) received sirolimus (Rapamune) stents; 28% received paclitaxel (Onxol) stents; and 33% had more than one DES.
Of the patients studied, 69 (61%) underwent surgery more than 180 days after receiving their DES; 30 (26%) had their procedures within 91-180 days of receiving the stent; and 15 (13%) had their operations within 90 days of stenting.
The most common procedures were major orthopedic surgeries such as hip replacement (34.2% of patients), and ophthalmologic procedures like cataract removal (26.3%).
No procedures fell into category five, and only 6.1% fell into category four; the rest were in categories one to three.
In most cases (77%), antiplatelet therapy had been discontinued a median of 10 days before surgery, with patients remaining off the drugs a median of 14 days after surgery.
There were no deaths. The most serious complications were non-ST-elevation myocardial infarction (NSTEMI) in two patients, and retroperitoneal hemorrhage following kidney transplantation in a patient who had been taking aspirin and clopidogrel until a week before surgery.
These findings suggest that “transient termination of antiplatelet agents in the perioperative setting is not associated with high morbidity and mortality in patients with DES, even when patients have had their stents implanted in the previous three to six months,” the authors write.
The study has limitations, Dr. Jaffer warns. “This was a small study, and more than 50% of our patients had surgery more than six months after DES placement,’’ he says. “It is difficult to predict a true relationship between timing of stent placement and subsequent surgery.”
Also, about a third of the patients underwent minor procedures, and roughly one-fifth never discontinued antiplatelet medication.
There were “several issues that may have led to fairly reasonable outcomes, and which could also be related to why we saw a fairly low rate of thrombosis,” he says.
In part because of these remaining questions, he recommends hospitalists take the timing of stent placement into account when evaluating patients with DES for surgery.
If it has been six months or less since the stent was implanted, the risk of thrombosis is still high, and “we can’t accurately say if it’s safe to stop antiplatelet medication,’’ he says. “I would treat those patients cautiously, as the literature suggests they may have a high risk of adverse events.”
But if the patient needs urgent surgery and more than six months have elapsed, “it may be safer to discontinue clopidogrel and continue baby aspirin, or to continue both antiplatelet medications during surgery if an urgent procedure is needed within six months of receiving the DES” he says. TH
Norra MacReady is a medical writer based in California.
Reference
- Pasternak LR. Preoperative assessment: guidelines and challenges. Acta Anaesthesiol Scand Suppl. 1997;111:318-320.
Drug-eluting stents (DES) are a medical success story: In the four years since they were approved, in-stent restenosis rates have gone from the 25%-30% associated with bare-metal stents to the single digits.
Thanks to this track record, the world market for stents has doubled to $5 billion—despite the fact patients with DES must take aspirin or clopidogrel to prevent thromboses.
It’s easy to forget not all questions concerning DES have been answered, despite their wide acceptance and good overall outcomes.
One concern is discontinuation of antiplatelet therapy for DES patients who require noncardiac surgery.
In the November-December 2007 Journal of Hospital Medicine, senior author Amir Jaffer, MD, and colleagues at the Cleveland Clinic in Ohio studied the relationship between a patient’s time on antiplatelet medication and the consequences of discontinuing those agents in preparation for surgery.
“This is a common clinical conundrum,” says Dr. Jaffer, director of the Cleveland Clinic’s Internal Medicine Preoperative Assessment Consultation and Treatment (IMPACT) Center. “We face this question almost every day in our practice relative to perioperative care.”
Patients slated for noncardiac surgery are seen first at the IMPACT center, where hospitalists conduct the preoperative evaluation.
Data show that patients with bare-metal stents run a high risk of stent thrombosis if they undergo noncardiac surgery within two to six weeks of stent placement.
But information on DES is hard to come by, “so we decided to try to get a handle on the safety of stopping these drugs,” says Dr. Jaffer.
The authors, led by Daniel J. Brotman, MD, studied all patients who had undergone DES placement and were evaluated for noncardiac surgery at the IMPACT Center from July 2003 to July 2005. They examined 30-day rates of postoperative myocardial infarction (MI), DES thrombosis, major bleeding, and all-cause mortality—all relative to how long the patient had been on and off antiplatelet therapy.
The type of surgery each patient underwent was classified by invasiveness and anticipated blood loss, according to the system developed by L. Reuven Pasternak, MD, vice dean, Bayview Campus, Johns Hopkins University in Baltimore, and his colleagues.1
The categories range from one, which includes cystoscopy, breast biopsy, and other minor procedures that involve little if any blood loss, to five, which encompasses highly invasive procedures with anticipated blood losses in excess of 1,500 cc, such as major vascular repair.
A total of 114 patients met the study criteria. Seventy-five (66%) of the patients were men, and the median age was 71.
The most common comorbidities were diabetes (in 41% of patients), a history of coronary bypass (34%), and chronic renal insufficiency (20%). Most patients (73%) received sirolimus (Rapamune) stents; 28% received paclitaxel (Onxol) stents; and 33% had more than one DES.
Of the patients studied, 69 (61%) underwent surgery more than 180 days after receiving their DES; 30 (26%) had their procedures within 91-180 days of receiving the stent; and 15 (13%) had their operations within 90 days of stenting.
The most common procedures were major orthopedic surgeries such as hip replacement (34.2% of patients), and ophthalmologic procedures like cataract removal (26.3%).
No procedures fell into category five, and only 6.1% fell into category four; the rest were in categories one to three.
In most cases (77%), antiplatelet therapy had been discontinued a median of 10 days before surgery, with patients remaining off the drugs a median of 14 days after surgery.
There were no deaths. The most serious complications were non-ST-elevation myocardial infarction (NSTEMI) in two patients, and retroperitoneal hemorrhage following kidney transplantation in a patient who had been taking aspirin and clopidogrel until a week before surgery.
These findings suggest that “transient termination of antiplatelet agents in the perioperative setting is not associated with high morbidity and mortality in patients with DES, even when patients have had their stents implanted in the previous three to six months,” the authors write.
The study has limitations, Dr. Jaffer warns. “This was a small study, and more than 50% of our patients had surgery more than six months after DES placement,’’ he says. “It is difficult to predict a true relationship between timing of stent placement and subsequent surgery.”
Also, about a third of the patients underwent minor procedures, and roughly one-fifth never discontinued antiplatelet medication.
There were “several issues that may have led to fairly reasonable outcomes, and which could also be related to why we saw a fairly low rate of thrombosis,” he says.
In part because of these remaining questions, he recommends hospitalists take the timing of stent placement into account when evaluating patients with DES for surgery.
If it has been six months or less since the stent was implanted, the risk of thrombosis is still high, and “we can’t accurately say if it’s safe to stop antiplatelet medication,’’ he says. “I would treat those patients cautiously, as the literature suggests they may have a high risk of adverse events.”
But if the patient needs urgent surgery and more than six months have elapsed, “it may be safer to discontinue clopidogrel and continue baby aspirin, or to continue both antiplatelet medications during surgery if an urgent procedure is needed within six months of receiving the DES” he says. TH
Norra MacReady is a medical writer based in California.
Reference
- Pasternak LR. Preoperative assessment: guidelines and challenges. Acta Anaesthesiol Scand Suppl. 1997;111:318-320.
Drug-eluting stents (DES) are a medical success story: In the four years since they were approved, in-stent restenosis rates have gone from the 25%-30% associated with bare-metal stents to the single digits.
Thanks to this track record, the world market for stents has doubled to $5 billion—despite the fact patients with DES must take aspirin or clopidogrel to prevent thromboses.
It’s easy to forget not all questions concerning DES have been answered, despite their wide acceptance and good overall outcomes.
One concern is discontinuation of antiplatelet therapy for DES patients who require noncardiac surgery.
In the November-December 2007 Journal of Hospital Medicine, senior author Amir Jaffer, MD, and colleagues at the Cleveland Clinic in Ohio studied the relationship between a patient’s time on antiplatelet medication and the consequences of discontinuing those agents in preparation for surgery.
“This is a common clinical conundrum,” says Dr. Jaffer, director of the Cleveland Clinic’s Internal Medicine Preoperative Assessment Consultation and Treatment (IMPACT) Center. “We face this question almost every day in our practice relative to perioperative care.”
Patients slated for noncardiac surgery are seen first at the IMPACT center, where hospitalists conduct the preoperative evaluation.
Data show that patients with bare-metal stents run a high risk of stent thrombosis if they undergo noncardiac surgery within two to six weeks of stent placement.
But information on DES is hard to come by, “so we decided to try to get a handle on the safety of stopping these drugs,” says Dr. Jaffer.
The authors, led by Daniel J. Brotman, MD, studied all patients who had undergone DES placement and were evaluated for noncardiac surgery at the IMPACT Center from July 2003 to July 2005. They examined 30-day rates of postoperative myocardial infarction (MI), DES thrombosis, major bleeding, and all-cause mortality—all relative to how long the patient had been on and off antiplatelet therapy.
The type of surgery each patient underwent was classified by invasiveness and anticipated blood loss, according to the system developed by L. Reuven Pasternak, MD, vice dean, Bayview Campus, Johns Hopkins University in Baltimore, and his colleagues.1
The categories range from one, which includes cystoscopy, breast biopsy, and other minor procedures that involve little if any blood loss, to five, which encompasses highly invasive procedures with anticipated blood losses in excess of 1,500 cc, such as major vascular repair.
A total of 114 patients met the study criteria. Seventy-five (66%) of the patients were men, and the median age was 71.
The most common comorbidities were diabetes (in 41% of patients), a history of coronary bypass (34%), and chronic renal insufficiency (20%). Most patients (73%) received sirolimus (Rapamune) stents; 28% received paclitaxel (Onxol) stents; and 33% had more than one DES.
Of the patients studied, 69 (61%) underwent surgery more than 180 days after receiving their DES; 30 (26%) had their procedures within 91-180 days of receiving the stent; and 15 (13%) had their operations within 90 days of stenting.
The most common procedures were major orthopedic surgeries such as hip replacement (34.2% of patients), and ophthalmologic procedures like cataract removal (26.3%).
No procedures fell into category five, and only 6.1% fell into category four; the rest were in categories one to three.
In most cases (77%), antiplatelet therapy had been discontinued a median of 10 days before surgery, with patients remaining off the drugs a median of 14 days after surgery.
There were no deaths. The most serious complications were non-ST-elevation myocardial infarction (NSTEMI) in two patients, and retroperitoneal hemorrhage following kidney transplantation in a patient who had been taking aspirin and clopidogrel until a week before surgery.
These findings suggest that “transient termination of antiplatelet agents in the perioperative setting is not associated with high morbidity and mortality in patients with DES, even when patients have had their stents implanted in the previous three to six months,” the authors write.
The study has limitations, Dr. Jaffer warns. “This was a small study, and more than 50% of our patients had surgery more than six months after DES placement,’’ he says. “It is difficult to predict a true relationship between timing of stent placement and subsequent surgery.”
Also, about a third of the patients underwent minor procedures, and roughly one-fifth never discontinued antiplatelet medication.
There were “several issues that may have led to fairly reasonable outcomes, and which could also be related to why we saw a fairly low rate of thrombosis,” he says.
In part because of these remaining questions, he recommends hospitalists take the timing of stent placement into account when evaluating patients with DES for surgery.
If it has been six months or less since the stent was implanted, the risk of thrombosis is still high, and “we can’t accurately say if it’s safe to stop antiplatelet medication,’’ he says. “I would treat those patients cautiously, as the literature suggests they may have a high risk of adverse events.”
But if the patient needs urgent surgery and more than six months have elapsed, “it may be safer to discontinue clopidogrel and continue baby aspirin, or to continue both antiplatelet medications during surgery if an urgent procedure is needed within six months of receiving the DES” he says. TH
Norra MacReady is a medical writer based in California.
Reference
- Pasternak LR. Preoperative assessment: guidelines and challenges. Acta Anaesthesiol Scand Suppl. 1997;111:318-320.
Manage Cancer Drugs
Human epidural growth factor receptor (HER1/EGFR) signaling pathways are crucial in regulating cell proliferation, survival, and differentiation.
HER1/EGFR is a protein tyrosine kinase with therapeutic applications in cancer treatment.1 Two approved drugs categories target HER1/EGFR: anti-HER1/EGFR monoclonal antibodies (mAb) and HER1/EGFR tyrosine kinase inhibitors (TKIs). The drugs have different complex actions, some leading to disruption of cellular processes at the level of cell division, apoptosis, and angiogenesis.
Approximately 30% to 100% of solid tumors express HER1/EGFR on the tumor surface, while some overexpress it. This is thought to lead to tumor growth.2,3 Increased HER1/EGFR activity has been associated with poor survival in some cancers.
The Agents
A number of HER1/EGFR TKIs are FDA approved and administered orally, including erlotinib (Tarceva), gefitinib (Iressa), imatinib (Gleevec), lapatinib (Tykerb), sorafenib (Nexavar), and sunitinib (Sutent).4-6
Cetuximab (Erbitux) and panitumumab (Vectibix) are approved mAbs given intravenously. Both categories treat different cancers including advanced/metastatic non-small cell lung cancer, colorectal cancer, pancreatic cancer, renal cell carcinoma, myelodysplastic syndrome, and others. The HER1/EGFR targeted agents have a more favorable side effect profile compared with more traditional chemotherapeutic agents with primarily dermatologic toxicities and limited hematopoietic effects. Because many patients are being treated with these oral anti-cancer agents, it is important to remain aware of the agents, their toxicities, and their management.
Adverse Effects
The most common adverse effect associated with HER1/EGFR inhibitors is a dose-dependent, folliculitis-like rash.
The rash affects up to two-thirds of treated patients within the first two weeks of therapy. It is usually on the face, neck, and upper torso and is characterized by inter- and intrafollicular papulopustules of mild-to-moderate severity. The rash develops in three phases: sensory disturbance with erythema and edema (weeks zero to one), papulopustular flare (weeks one to three), crusting (weeks three to five), and erythematotelangiectasias (weeks five to eight).
Dry skin and erythema may remain in the areas after resolution. The skin rash appears to be dose-dependent. The mechanism of the rash is not precisely known. However, HER1/EGFR is expressed by normal keratinocytes and skin fibroblasts, along the outer sheath of the hair follicle, and in many epidermal processes, which probably contributes.
Hair effects occur within two to three months of starting treatment. Scalp hair becomes more brittle, fine, and curly. Frontal alopecia gradually develops, and patients experience progressive trichomegaly of the eyelashes and hypertrichosis of the face. Paronychial inflammation can occur on the fingernails or toenails and be so painful it prevents patients from wearing shoes. Its origin is unknown, and it disappears after discontinuation of the drug. Xerosis is also common, which can be treated with topically applied 5% to 10% urea emollient.
New Drugs

Cefotetan Disodium for injection (generic Cefotan) has been FDA approved. It can be used to treat infections due to abdominal or vaginal hysterectomy and/or Caesarean section, as well as colorectal surgery, and others.
IN THE PIPELINE
Gabapentin GR, an extended-release, once-daily formulation, is undergoing Phase III clinical trials for treating postherpetic neuralgia. Depomed recently reported results from a randomized, double-blind, placebo-controlled, multicenter trial using 1,800 mg daily that did not meet the primary endpoint (efficacy to reduce average daily pain). Secondary endpoints of sleep interference were all statistically significant in favor of Gabapentin GR. The most common adverse effects were dizziness and peripheral edema.
Natalizumab (Tysabri) received a favorable recommendation for treating moderate-to-severe Crohn’s disease in patients who have failed tumor necrosis factor inhibitor therapies and are not on immunosuppressive therapy—a narrower indication than that proposed by the manufacturers. The recommendation was made at a joint meeting of the Advisory Committees of Gastrointestinal Drugs and Drug Safety and Risk Management. Natalizumab is FDA-approved for the treatment of relapsing forms of multiple sclerosis (MS). Natalizumab is a recombinant, humanized immunoglobulin G4 mAb against alpha4 integrins that is administered via intravenous infusion. Natalizumab increases the risk of progressive multifocal leukoencephalopathy (PML), an opportunistic viral brain infection that usually leads to severe disability or death. A risk-management program is being developed in case the agent is approved for Crohn’s disease.
Raloxifene (Evista), a selective estrogen receptor modulator, originally approved in December 1997 for the treatment and prevention of postmenopausal osteoporosis has been recommended by an FDA advisory panel to add new indications to its label. The new indications include: (1) reducing the risk of invasive breast cancer in postmenopausal women with osteoporosis, and (2) reducing the risk of invasive breast cancer in postmenopausal women at high risk for developing breast cancer.—MK
Rash as a Marker
There appears to be some evidence of a relationship between HER1/EGFR efficacy and associated rash severity. There have been at least 19 trials and additional compassionate use centers that have found the relationship of a positive correlation between rash and response/survival.
For example, in a Phase II study in 57 patients with non-small cell lung cancer, those with grade zero rashes had a median survival of 1.5 months, those with rash grade one had a median survival of 8.5 months, and those with rash grades two or three had a 19.6 month survival. In another study with erlotinib monotherapy, patients with a skin rash had significantly greater survival rates (approximately 80%) than those without skin rashes. In trials of cetuximab in patients with different cancer types, those who developed a rash lived substantially longer than those who did not.
There are also data supporting gefitinib and cetuximab. Many of the studies note a poorer clinical outcome in those patients without rash. These findings suggest that lack of a rash after a specific period of therapy may be an early indicator of treatment failure and the need for another treatment.
Rash Treatment
While receiving treatment with these agents, patients should be advised to moisturize dry body areas twice daily with a thick alcohol-free emollient. Patients should minimize sun exposure and wear a broad-spectrum sunscreen (SPF 15). Zinc oxide or titanium dioxide is preferred over chemical sunscreens. The following treatment interventions are suggested:
- Mild toxicity: topical hydrocortisone 1% to 2.5% cream or clindamycin 1% gel. The HER1/EGFR dose should not be adjusted;
- Moderate toxicity: topical hydrocortisone 2.5% cream, clindamycin 1% gel, or pimecrolimus 1% cream (Elidel) with doxycycline 100mg orally twice a day or minocycline 100mg orally twice a day. The HER1/EGFR dose should not be adjusted; or
- Severe toxicity: topical hydrocortisone 2.5% cream, clindamycin 1% gel, or pimecrolimus 1% cream (Elidel) with doxycycline 100mg orally twice a day or minocycline 100mg orally twice a day. Also add methylprednisolone dose pack.
Reduce the HER1/EGFR dose, if after two to four weeks the toxicities have not sufficiently abated, then the HER1/EGFR therapy should be interrupted. Once the skin reactions have resolved or diminished in severity, the HER1/EGFR dose may typically be restarted or re-escalated.
Results of a recent double-blind, placebo-controlled study suggest tetracycline may be effective in decreasing EGFR-associated rash severity and improving some quality-of-life parameters (e.g., irritation, burning, stinging).7 Remaining alert to these reactions in patients receiving HER1/EGFRs is important for monitoring treatment and managing patients. TH
Michele B. Kaufman is a freelance medical writer based in New York City.
References
- Castillo L, Etienne-Grimaldi MC, Fischel JL, et al. Pharmacologic background of EGFR targeting. Ann Oncol. 2004;15(7):1007-1012.
- Robert C, Soria JC, Spatz A et al. Cutaneous side effects of kinase inhibitors and blocking antibodies. Lancet Oncol. 2005;6(7):491-500.
- Peréz-Soler R, Saltz L. Cutaneous adverse effects with HER1/EGFR-targeted agents: Is there a silver lining? J Clin Oncol. 2005;23(22):5235-5246.
- Seiverling EV, Fernandez EM, Adams D. Epidermal growth factor receptor inhibitor associated skin eruption. J Drugs Dermatol. 2006;5(4)368-369. Available at http://findarticles.com/p/articles/ mi_m0PDG/ is_4_5/ai_n16361317Accessed August 7, 2007
- Tyrosine Kinase Inhibitors. www.oncolink.com/treatment/article.cfm?c=12&s=90&id=268. Accessed August 7, 2007
- Lynch TJ, Kim ES, Eaby B, et al. Epidermal growth factor receptor inhibitor-associated toxicities: An evolving paradigm in clinical management. Oncologist 2007;12(5):610-621.
- Jatoi A, Rowland K, Sloan JA, et al. J Clin Oncol 2007; ASCO Annual Meeting Proceedings Part I. Vol. 25(18S);June 20:LBA9006.
Human epidural growth factor receptor (HER1/EGFR) signaling pathways are crucial in regulating cell proliferation, survival, and differentiation.
HER1/EGFR is a protein tyrosine kinase with therapeutic applications in cancer treatment.1 Two approved drugs categories target HER1/EGFR: anti-HER1/EGFR monoclonal antibodies (mAb) and HER1/EGFR tyrosine kinase inhibitors (TKIs). The drugs have different complex actions, some leading to disruption of cellular processes at the level of cell division, apoptosis, and angiogenesis.
Approximately 30% to 100% of solid tumors express HER1/EGFR on the tumor surface, while some overexpress it. This is thought to lead to tumor growth.2,3 Increased HER1/EGFR activity has been associated with poor survival in some cancers.
The Agents
A number of HER1/EGFR TKIs are FDA approved and administered orally, including erlotinib (Tarceva), gefitinib (Iressa), imatinib (Gleevec), lapatinib (Tykerb), sorafenib (Nexavar), and sunitinib (Sutent).4-6
Cetuximab (Erbitux) and panitumumab (Vectibix) are approved mAbs given intravenously. Both categories treat different cancers including advanced/metastatic non-small cell lung cancer, colorectal cancer, pancreatic cancer, renal cell carcinoma, myelodysplastic syndrome, and others. The HER1/EGFR targeted agents have a more favorable side effect profile compared with more traditional chemotherapeutic agents with primarily dermatologic toxicities and limited hematopoietic effects. Because many patients are being treated with these oral anti-cancer agents, it is important to remain aware of the agents, their toxicities, and their management.
Adverse Effects
The most common adverse effect associated with HER1/EGFR inhibitors is a dose-dependent, folliculitis-like rash.
The rash affects up to two-thirds of treated patients within the first two weeks of therapy. It is usually on the face, neck, and upper torso and is characterized by inter- and intrafollicular papulopustules of mild-to-moderate severity. The rash develops in three phases: sensory disturbance with erythema and edema (weeks zero to one), papulopustular flare (weeks one to three), crusting (weeks three to five), and erythematotelangiectasias (weeks five to eight).
Dry skin and erythema may remain in the areas after resolution. The skin rash appears to be dose-dependent. The mechanism of the rash is not precisely known. However, HER1/EGFR is expressed by normal keratinocytes and skin fibroblasts, along the outer sheath of the hair follicle, and in many epidermal processes, which probably contributes.
Hair effects occur within two to three months of starting treatment. Scalp hair becomes more brittle, fine, and curly. Frontal alopecia gradually develops, and patients experience progressive trichomegaly of the eyelashes and hypertrichosis of the face. Paronychial inflammation can occur on the fingernails or toenails and be so painful it prevents patients from wearing shoes. Its origin is unknown, and it disappears after discontinuation of the drug. Xerosis is also common, which can be treated with topically applied 5% to 10% urea emollient.
New Drugs
Cefotetan Disodium for injection (generic Cefotan) has been FDA approved. It can be used to treat infections due to abdominal or vaginal hysterectomy and/or Caesarean section, as well as colorectal surgery, and others.
IN THE PIPELINE
Gabapentin GR, an extended-release, once-daily formulation, is undergoing Phase III clinical trials for treating postherpetic neuralgia. Depomed recently reported results from a randomized, double-blind, placebo-controlled, multicenter trial using 1,800 mg daily that did not meet the primary endpoint (efficacy to reduce average daily pain). Secondary endpoints of sleep interference were all statistically significant in favor of Gabapentin GR. The most common adverse effects were dizziness and peripheral edema.
Natalizumab (Tysabri) received a favorable recommendation for treating moderate-to-severe Crohn’s disease in patients who have failed tumor necrosis factor inhibitor therapies and are not on immunosuppressive therapy—a narrower indication than that proposed by the manufacturers. The recommendation was made at a joint meeting of the Advisory Committees of Gastrointestinal Drugs and Drug Safety and Risk Management. Natalizumab is FDA-approved for the treatment of relapsing forms of multiple sclerosis (MS). Natalizumab is a recombinant, humanized immunoglobulin G4 mAb against alpha4 integrins that is administered via intravenous infusion. Natalizumab increases the risk of progressive multifocal leukoencephalopathy (PML), an opportunistic viral brain infection that usually leads to severe disability or death. A risk-management program is being developed in case the agent is approved for Crohn’s disease.
Raloxifene (Evista), a selective estrogen receptor modulator, originally approved in December 1997 for the treatment and prevention of postmenopausal osteoporosis has been recommended by an FDA advisory panel to add new indications to its label. The new indications include: (1) reducing the risk of invasive breast cancer in postmenopausal women with osteoporosis, and (2) reducing the risk of invasive breast cancer in postmenopausal women at high risk for developing breast cancer.—MK
Rash as a Marker
There appears to be some evidence of a relationship between HER1/EGFR efficacy and associated rash severity. There have been at least 19 trials and additional compassionate use centers that have found the relationship of a positive correlation between rash and response/survival.
For example, in a Phase II study in 57 patients with non-small cell lung cancer, those with grade zero rashes had a median survival of 1.5 months, those with rash grade one had a median survival of 8.5 months, and those with rash grades two or three had a 19.6 month survival. In another study with erlotinib monotherapy, patients with a skin rash had significantly greater survival rates (approximately 80%) than those without skin rashes. In trials of cetuximab in patients with different cancer types, those who developed a rash lived substantially longer than those who did not.
There are also data supporting gefitinib and cetuximab. Many of the studies note a poorer clinical outcome in those patients without rash. These findings suggest that lack of a rash after a specific period of therapy may be an early indicator of treatment failure and the need for another treatment.
Rash Treatment
While receiving treatment with these agents, patients should be advised to moisturize dry body areas twice daily with a thick alcohol-free emollient. Patients should minimize sun exposure and wear a broad-spectrum sunscreen (SPF 15). Zinc oxide or titanium dioxide is preferred over chemical sunscreens. The following treatment interventions are suggested:
- Mild toxicity: topical hydrocortisone 1% to 2.5% cream or clindamycin 1% gel. The HER1/EGFR dose should not be adjusted;
- Moderate toxicity: topical hydrocortisone 2.5% cream, clindamycin 1% gel, or pimecrolimus 1% cream (Elidel) with doxycycline 100mg orally twice a day or minocycline 100mg orally twice a day. The HER1/EGFR dose should not be adjusted; or
- Severe toxicity: topical hydrocortisone 2.5% cream, clindamycin 1% gel, or pimecrolimus 1% cream (Elidel) with doxycycline 100mg orally twice a day or minocycline 100mg orally twice a day. Also add methylprednisolone dose pack.
Reduce the HER1/EGFR dose, if after two to four weeks the toxicities have not sufficiently abated, then the HER1/EGFR therapy should be interrupted. Once the skin reactions have resolved or diminished in severity, the HER1/EGFR dose may typically be restarted or re-escalated.
Results of a recent double-blind, placebo-controlled study suggest tetracycline may be effective in decreasing EGFR-associated rash severity and improving some quality-of-life parameters (e.g., irritation, burning, stinging).7 Remaining alert to these reactions in patients receiving HER1/EGFRs is important for monitoring treatment and managing patients. TH
Michele B. Kaufman is a freelance medical writer based in New York City.
References
- Castillo L, Etienne-Grimaldi MC, Fischel JL, et al. Pharmacologic background of EGFR targeting. Ann Oncol. 2004;15(7):1007-1012.
- Robert C, Soria JC, Spatz A et al. Cutaneous side effects of kinase inhibitors and blocking antibodies. Lancet Oncol. 2005;6(7):491-500.
- Peréz-Soler R, Saltz L. Cutaneous adverse effects with HER1/EGFR-targeted agents: Is there a silver lining? J Clin Oncol. 2005;23(22):5235-5246.
- Seiverling EV, Fernandez EM, Adams D. Epidermal growth factor receptor inhibitor associated skin eruption. J Drugs Dermatol. 2006;5(4)368-369. Available at http://findarticles.com/p/articles/ mi_m0PDG/ is_4_5/ai_n16361317Accessed August 7, 2007
- Tyrosine Kinase Inhibitors. www.oncolink.com/treatment/article.cfm?c=12&s=90&id=268. Accessed August 7, 2007
- Lynch TJ, Kim ES, Eaby B, et al. Epidermal growth factor receptor inhibitor-associated toxicities: An evolving paradigm in clinical management. Oncologist 2007;12(5):610-621.
- Jatoi A, Rowland K, Sloan JA, et al. J Clin Oncol 2007; ASCO Annual Meeting Proceedings Part I. Vol. 25(18S);June 20:LBA9006.
Human epidural growth factor receptor (HER1/EGFR) signaling pathways are crucial in regulating cell proliferation, survival, and differentiation.
HER1/EGFR is a protein tyrosine kinase with therapeutic applications in cancer treatment.1 Two approved drugs categories target HER1/EGFR: anti-HER1/EGFR monoclonal antibodies (mAb) and HER1/EGFR tyrosine kinase inhibitors (TKIs). The drugs have different complex actions, some leading to disruption of cellular processes at the level of cell division, apoptosis, and angiogenesis.
Approximately 30% to 100% of solid tumors express HER1/EGFR on the tumor surface, while some overexpress it. This is thought to lead to tumor growth.2,3 Increased HER1/EGFR activity has been associated with poor survival in some cancers.
The Agents
A number of HER1/EGFR TKIs are FDA approved and administered orally, including erlotinib (Tarceva), gefitinib (Iressa), imatinib (Gleevec), lapatinib (Tykerb), sorafenib (Nexavar), and sunitinib (Sutent).4-6
Cetuximab (Erbitux) and panitumumab (Vectibix) are approved mAbs given intravenously. Both categories treat different cancers including advanced/metastatic non-small cell lung cancer, colorectal cancer, pancreatic cancer, renal cell carcinoma, myelodysplastic syndrome, and others. The HER1/EGFR targeted agents have a more favorable side effect profile compared with more traditional chemotherapeutic agents with primarily dermatologic toxicities and limited hematopoietic effects. Because many patients are being treated with these oral anti-cancer agents, it is important to remain aware of the agents, their toxicities, and their management.
Adverse Effects
The most common adverse effect associated with HER1/EGFR inhibitors is a dose-dependent, folliculitis-like rash.
The rash affects up to two-thirds of treated patients within the first two weeks of therapy. It is usually on the face, neck, and upper torso and is characterized by inter- and intrafollicular papulopustules of mild-to-moderate severity. The rash develops in three phases: sensory disturbance with erythema and edema (weeks zero to one), papulopustular flare (weeks one to three), crusting (weeks three to five), and erythematotelangiectasias (weeks five to eight).
Dry skin and erythema may remain in the areas after resolution. The skin rash appears to be dose-dependent. The mechanism of the rash is not precisely known. However, HER1/EGFR is expressed by normal keratinocytes and skin fibroblasts, along the outer sheath of the hair follicle, and in many epidermal processes, which probably contributes.
Hair effects occur within two to three months of starting treatment. Scalp hair becomes more brittle, fine, and curly. Frontal alopecia gradually develops, and patients experience progressive trichomegaly of the eyelashes and hypertrichosis of the face. Paronychial inflammation can occur on the fingernails or toenails and be so painful it prevents patients from wearing shoes. Its origin is unknown, and it disappears after discontinuation of the drug. Xerosis is also common, which can be treated with topically applied 5% to 10% urea emollient.
New Drugs
Cefotetan Disodium for injection (generic Cefotan) has been FDA approved. It can be used to treat infections due to abdominal or vaginal hysterectomy and/or Caesarean section, as well as colorectal surgery, and others.
IN THE PIPELINE
Gabapentin GR, an extended-release, once-daily formulation, is undergoing Phase III clinical trials for treating postherpetic neuralgia. Depomed recently reported results from a randomized, double-blind, placebo-controlled, multicenter trial using 1,800 mg daily that did not meet the primary endpoint (efficacy to reduce average daily pain). Secondary endpoints of sleep interference were all statistically significant in favor of Gabapentin GR. The most common adverse effects were dizziness and peripheral edema.
Natalizumab (Tysabri) received a favorable recommendation for treating moderate-to-severe Crohn’s disease in patients who have failed tumor necrosis factor inhibitor therapies and are not on immunosuppressive therapy—a narrower indication than that proposed by the manufacturers. The recommendation was made at a joint meeting of the Advisory Committees of Gastrointestinal Drugs and Drug Safety and Risk Management. Natalizumab is FDA-approved for the treatment of relapsing forms of multiple sclerosis (MS). Natalizumab is a recombinant, humanized immunoglobulin G4 mAb against alpha4 integrins that is administered via intravenous infusion. Natalizumab increases the risk of progressive multifocal leukoencephalopathy (PML), an opportunistic viral brain infection that usually leads to severe disability or death. A risk-management program is being developed in case the agent is approved for Crohn’s disease.
Raloxifene (Evista), a selective estrogen receptor modulator, originally approved in December 1997 for the treatment and prevention of postmenopausal osteoporosis has been recommended by an FDA advisory panel to add new indications to its label. The new indications include: (1) reducing the risk of invasive breast cancer in postmenopausal women with osteoporosis, and (2) reducing the risk of invasive breast cancer in postmenopausal women at high risk for developing breast cancer.—MK
Rash as a Marker
There appears to be some evidence of a relationship between HER1/EGFR efficacy and associated rash severity. There have been at least 19 trials and additional compassionate use centers that have found the relationship of a positive correlation between rash and response/survival.
For example, in a Phase II study in 57 patients with non-small cell lung cancer, those with grade zero rashes had a median survival of 1.5 months, those with rash grade one had a median survival of 8.5 months, and those with rash grades two or three had a 19.6 month survival. In another study with erlotinib monotherapy, patients with a skin rash had significantly greater survival rates (approximately 80%) than those without skin rashes. In trials of cetuximab in patients with different cancer types, those who developed a rash lived substantially longer than those who did not.
There are also data supporting gefitinib and cetuximab. Many of the studies note a poorer clinical outcome in those patients without rash. These findings suggest that lack of a rash after a specific period of therapy may be an early indicator of treatment failure and the need for another treatment.
Rash Treatment
While receiving treatment with these agents, patients should be advised to moisturize dry body areas twice daily with a thick alcohol-free emollient. Patients should minimize sun exposure and wear a broad-spectrum sunscreen (SPF 15). Zinc oxide or titanium dioxide is preferred over chemical sunscreens. The following treatment interventions are suggested:
- Mild toxicity: topical hydrocortisone 1% to 2.5% cream or clindamycin 1% gel. The HER1/EGFR dose should not be adjusted;
- Moderate toxicity: topical hydrocortisone 2.5% cream, clindamycin 1% gel, or pimecrolimus 1% cream (Elidel) with doxycycline 100mg orally twice a day or minocycline 100mg orally twice a day. The HER1/EGFR dose should not be adjusted; or
- Severe toxicity: topical hydrocortisone 2.5% cream, clindamycin 1% gel, or pimecrolimus 1% cream (Elidel) with doxycycline 100mg orally twice a day or minocycline 100mg orally twice a day. Also add methylprednisolone dose pack.
Reduce the HER1/EGFR dose, if after two to four weeks the toxicities have not sufficiently abated, then the HER1/EGFR therapy should be interrupted. Once the skin reactions have resolved or diminished in severity, the HER1/EGFR dose may typically be restarted or re-escalated.
Results of a recent double-blind, placebo-controlled study suggest tetracycline may be effective in decreasing EGFR-associated rash severity and improving some quality-of-life parameters (e.g., irritation, burning, stinging).7 Remaining alert to these reactions in patients receiving HER1/EGFRs is important for monitoring treatment and managing patients. TH
Michele B. Kaufman is a freelance medical writer based in New York City.
References
- Castillo L, Etienne-Grimaldi MC, Fischel JL, et al. Pharmacologic background of EGFR targeting. Ann Oncol. 2004;15(7):1007-1012.
- Robert C, Soria JC, Spatz A et al. Cutaneous side effects of kinase inhibitors and blocking antibodies. Lancet Oncol. 2005;6(7):491-500.
- Peréz-Soler R, Saltz L. Cutaneous adverse effects with HER1/EGFR-targeted agents: Is there a silver lining? J Clin Oncol. 2005;23(22):5235-5246.
- Seiverling EV, Fernandez EM, Adams D. Epidermal growth factor receptor inhibitor associated skin eruption. J Drugs Dermatol. 2006;5(4)368-369. Available at http://findarticles.com/p/articles/ mi_m0PDG/ is_4_5/ai_n16361317Accessed August 7, 2007
- Tyrosine Kinase Inhibitors. www.oncolink.com/treatment/article.cfm?c=12&s=90&id=268. Accessed August 7, 2007
- Lynch TJ, Kim ES, Eaby B, et al. Epidermal growth factor receptor inhibitor-associated toxicities: An evolving paradigm in clinical management. Oncologist 2007;12(5):610-621.
- Jatoi A, Rowland K, Sloan JA, et al. J Clin Oncol 2007; ASCO Annual Meeting Proceedings Part I. Vol. 25(18S);June 20:LBA9006.
In the Literature
In This Edition
- Cost sharing for prescription medications increases consumption of more costly healthcare services
- Community-acquired pneumonia core measures can lead to unintended consequences
- Prophylactic revascularization has no clear benefit for high-risk patients undergoing vascular surgery
- Aspirin resistance correlates with adverse clinical events
- Low-molecular-weight heparin appears to have greater efficacy as a prophylactic agent against deep-vein thrombosis and pulmonary embolism
- Antipsychotic medications appear to be associated with increased risk of death in demented patients
- Anticoagulation plus antiplatelet therapy fails to show benefit for peripheral arterial disease
- Transient atrial fibrillation following myocardial infarction increases the risk of recurrence and stroke
Do Incentives to Encourage Use of Certain Medications Affect Care?
Background: Insurers are increasingly using financial mechanisms to affect pharmaceutical usage. These practices may affect medication use and health outcomes in ways that are poorly defined and difficult to detect.
Study design: Literature review
Synopsis: There are numerous structures for drug-cost sharing, and this study evaluated co-payments, tiers/co-insurance, benefit caps, formulary limitations, and reference pricing strategies for their effect on prescription drug usage and healthcare outcomes.
Included articles varied widely in study design, making generalizable results difficult to isolate, and insurers may have instituted more than one cost-sharing mechanism simultaneously. Overall, for every 10% increase in cost sharing (via copayments or co-insurance) there was an associated 2%-6% decrease in prescription drug spending. Increasing consumer costs for medications clearly decreases usage.
Some studies demonstrated that the decrease in medication utilization was more pronounced for “nonessential” medications over “essential” medications. However, in specific chronic illnesses this is clearly associated with greater usage of inpatient and emergency medical services.
Cost sharing was also more likely to have adverse health consequences in vulnerable populations, particularly the elderly and poor. One in four Medicaid patients couldn’t fill at least one prescription in the past year, as opposed to one in 10 privately insured patients who couldn’t purchase one or more medications.
Further impact on healthcare consumption and outcomes may be masked because it is difficult to determine individual disease severity, and the effect on the more severely ill would be expected to be greater. These authors attempted to sort out a complex interaction between cost, consumption, and health, and they found important trends.
The goal of cost sharing is to align consumption more clearly with appropriate and economic products, thereby using cost sharing as a public health tool. The consequence of creating the incentives for ill patients to forego necessary treatments is a counterbalancing concern that is supported in some, but not all, of the literature.
Bottom line: Cost sharing for prescription medications decreases medication spending and utilization but disproportionately affects the disadvantaged and increases consumption of more costly healthcare services in patients with some chronic illnesses.
Citation: Goldman DP, Joyce GF, Zheng Y. Prescription drug cost sharing: associations with medication and medical utilization and spending and health. JAMA. 2007;298(1):61-69.
Does Antibiotic Requirement for Suspected CAP Increase Misdiagnosis?
Background: Early administration of antibiotics in community-acquired pneumonia (CAP) improves patient outcomes. The Infectious Disease Society of America instituted guidelines that recommend initiation of antibiotics to all patients with suspected CAP within four hours of triage, and some payors are using this as a quality measure affecting reimbursement. However, this incentive may cause premature diagnosis of CAP and overuse of antibiotics.
Study design: Retrospective chart review
Setting: A large, high-volume teaching hospital with more than 500 beds and more than 112,000 annual emergency department (ED) visits
Synopsis: Charts of all patients with an admitting diagnosis of CAP were reviewed over two six-month periods. The initial review was prior to initiation of a four-hour antibiotics rule; the second was after a financial incentive to initiate antibiotics within four hours of triage was initiated.
After initiation of the four-hour rule, of the patients with an admitting diagnosis of CAP, significantly more patients received antibiotics within four hours of triage (66% versus 54%). However, the number of patients with abnormal chest X-ray findings associated with the diagnosis of CAP decreased from 28.5% to 20.6%, and the proportion of patients with a discharge diagnosis of CAP decreased from 75.9% to 58.9%.
The authors also used two diagnostic paradigms to make an independent diagnosis of CAP based on chart data. With the less rigorous independent analysis 44.7% of patients actually had CAP prior to the four-hour rule, and this fell to 36% after the four-hour rule. Using a more rigorous definition, only 32.7% of patients actually had CAP prior to initiation of the four-hour rule, and this fell to 27%.
There was no difference in length of stay or ICU transfers between the two analysis periods. The authors concluded that a four-hour rule increases premature diagnosis of CAP, presumably because providers felt compelled to initiate antibiotics before they had complete clinical data.
This tendency was associated with misuse and overuse of antibiotics, and increased laboratory testing, such as blood cultures, which had to be obtained before antibiotics were initiated. The authors emphasized the importance of reimbursement-associated quality measures creating incentives to treat the right patients for the correct diagnosis, and the potential harmful consequences of applying a quality-driven protocol to the wrong patient.
They suggest a six-hour rule would decrease the misdiagnosis of CAP. They also feel eliminating a mandatory time frame and requiring only that the first dose of antibiotics be administered in the ED will further ameliorate these effects.
Bottom line: Mandatory administration of antibiotics to patients with suspected CAP within four hours of triage increases the percentage of patients who receive antibiotics within four hours, but also increases the rate of misdiagnosis of CAP, inappropriate administration of antibiotics, and increased use of some laboratory services.
Citation: Kanwar M, Brar N, Khatib R, et al. Misdiagnosis of community-acquired pneumonia and inappropriate utilization of antibiotics: side effects of the 4-hour antibiotic administration rule. Chest. 2007 Jun;131(6):1865-1869.
Does prophylactic cardiac revascularization benefit patients undergoing vascular surgery?
Background: American College of Cardiology/American Heart Association Guidelines recommend referral for patients with multiple cardiac risk factors for non-invasive cardiac stress testing prior to surgery and prophylactic revascularization in high-risk patients. The authors performed a pilot analysis to determine how many patients would be needed to prospectively validate this recommendation in those with more significant ischemic cardiac disease.
Study design: Randomized controlled pilot study of 1,880 consecutive patients undergoing elective vascular surgery
Setting: Brazil, Belgium, the Netherlands, Italy, Serbia, and Montenegro
Synopsis: This was a pilot study to determine the necessary power to prove or disprove the benefit of the recommendation for cardiac revascularization in high-risk patients before major vascular surgery.
Prior research had shown that prophylactic revascularization is not of demonstrable benefit in this cohort. However, the majority of the patients in this previous trial had two-vessel disease and preserved left ventricular function. This study examined a sicker cohort of patients with more significant coronary artery disease and depressed left ventricular function.
This pilot screened all patients undergoing high-risk vascular surgery. All patients with three or more risk factors underwent non-invasive evaluation for cardiac ischemia. Patients with extensive ischemia were randomized to invasive evaluation and revascularization as appropriate or non-invasive management. Both arms received optimal medical management.
Prophylactic revascularization did not improve 30-day outcome after vascular surgery, demonstrated no difference in perioperative cardiac events, and found no difference in all-cause mortality or nonfatal myocardial infarction. Similarly, there was no evidence of long-term (at one year) difference between groups. The sample size needed to definitively establish that coronary revascularization is superior to medical therapy would be 300 patients per arm. That would require screening 9,000 patients.
Bottom line: Prophylactic revascularization has no clear benefit for high-risk patients undergoing vascular surgery, but a much larger sample size would be required to definitively prove or disprove benefit.
Citation: Poldermans D, Schouten O, Vidakovic R, et al. Clinical randomized trial to evaluate the safety of a noninvasive approach in high-risk patients undergoing major vascular surgery: the DECREASE-V pilot study. J. Am Coll Cardiol. 2007;49(17):1763-1769.
How Does Aspirin Resistance Affect Patients with Coronary Artery Disease?
Background: Although aspirin is used to decrease the risk of ischemic events, up to 45% of patients do not derive adequate anti-platelet activity. Few prospective studies have used laboratory-measured aspirin resistance to assess clinical outcomes.
Study design: Blinded cohort
Setting: Patients affiliated with Queen Mary Hospital, the University of Hong Kong.
Synopsis: Aspirin-induced platelet inhibition was measured quantitatively on 468 patients with stable coronary artery disease who take 80-325 mg of aspirin per day. The study found 128 patients were aspirin resistant. Aspirin resistance was more prevalent with increased age, female gender, renal insufficiency, anemia, and with use of low-dose aspirin. At follow up, aspirin-resistant patients were more likely to develop a primary outcome event: cardiovascular deaths, myocardial infarction, stroke, transient ischemic attack, and unstable angina. Aspirin resistance was an independent risk factor for developing the aforementioned outcomes, as are diabetes, prior myocardial infarction, and low hemoglobin.
Bottom line: Aspirin resistance, as defined by an aggregation-based assay, is associated with adverse outcomes in patients with stable coronary artery disease.
Citation: Chen W, Cheng X, Lee PY, et al. Aspirin resistance and adverse clinical events in patients with coronary artery disease. Am J Med. 2007 Jul;120(7):631-635.
Which Agents Best Prevent Venous Thromboembolism?
Background: Pulmonary emboli have been linked to 10% of in-hospital deaths. There continues to be a strong emphasis on prevention. Unfractionated heparin (UFH), low-molecular-weight heparin (LMWH), and selective factor Xa inhibitors are used for prophylaxis.
Study design: A meta-analysis of randomized controlled trials
Synopsis: The meta-analysis included 36 studies of hospitalized medical patients that compared UFH with control, LMWH with control, LMWH with UFH, and a selective factor Xa inhibitor with a placebo.
When each was compared with a control, UFH and LMWH were associated with a decreased risk of deep venous thrombosis (DVT) (risk ratio=0.33; 0.56) and pulmonary embolism (PE) (risk ratio=0.64; 0.37). Compared with control, LMWH three times daily was more effective than twice-daily dosing (risk ratio=0.27, 0.52). Through direct comparison of UFH and LMWH, LMWH was shown to have decreased DVT risk (risk ratio=0.68) and fewer injection site hematomas (risk ratio=0.47).
Neither UFH nor LMWH reduced mortality. LMWH and UFH were associated with significantly more bleeding events than control, but this increased risk was significant only for minor bleeding.
Bottom line: LMWH appears to have greater efficacy than UFH as a prophylactic agent against DVT/PE. If UFH is used, three times daily dosing is preferred.
Citation: Wein L, Wein S, Haas SJ, et al. Pharmacological venous thromboembolism prophylaxis in hospitalized medical patients. Arch Intern Med. 2007;167(14):1476-1486.
What Is the Association Between Antipsychotic Drugs and Mortality?
Background: Atypical antipsychotics prescribed off-label for problematic behaviors in dementia have been associated with risks including diabetes, stroke, and increased mortality. This resulted in the FDA placing a “black box” warning on atypical antipsychotics used for dementia. Subsequent studies have suggested that conventional antipsychotics are perhaps even more problematic.
Study Design: Retrospective cohort study
Synopsis: This trial found a small but significant increase in the risk of death in patients taking an antipsychotic medication.
The adjusted hazard ratio for death with the use of atypical antipsychotics in community dwelling patients with dementia was 1.3 (confidence interval 1.02-1.70). Similar to prior research, the authors found that conventional antipsychotics carried a higher risk than atypical agents.
Patients in long-term care settings also suffered increased risk compared with community dwelling patients. Interestingly, the increased risk of death was apparent after as little as a month of treatment.
As with all retrospective observational cohort trials, there remains the risk that an unanticipated confounding factor could skew the data and create a false association. However, the findings of this research support prior concerns that antipsychotics carry risk of increased mortality. This research bolsters the argument that these agents should not be used lightly or without full discussion of risks and benefits with the patient and/or proxy.
Bottom line: Antipsychotic agents used in patients with dementia may create increased risk of death. Potential benefit needs to be carefully weighted against this serious harm.
Citation: Gill S, Bronskill SE, Normand SL, et al. Antipsychotic drug use and mortality in older adults with dementia. Ann Intern Med. 2007 June 5;146(11):775-786.
Does Combination Therapy Help Prevent Serious Vascular Ischemic Events?
Background: Peripheral arterial disease (PAD) manifests as claudication and limb ischemia affecting 8.5 million Americans. Atherosclerotic disease in the periphery also reflects increased risk for ischemic events in the coronary and cranial circulations. Both antiplatelet agents and anticoagulation will decrease the probability of thrombus formation, although this must be weighed against bleeding risk.
Study design: Randomized, open-label, multicenter trial
Setting: Eighty centers in Europe, Asia, Australia, and North America
Synopsis: This trial randomized more than 2,000 patients with PAD to treatment with antiplatelet therapy (aspirin, ticlopidine, or clopidogrel) with or without additional anticoagulation.
During the next 3.5 years serious vascular events occurred at approximately the same rate in both combination and monotherapy groups (15.9% versus 17.4%, p=0.37). There was no significant difference between the occurrence of the composite ischemic endpoints or any of the individual endpoints. There was, however, a significantly higher rate of both moderate and life-threatening bleeding in the combination therapy group.
The 4% risk of life-threatening hemorrhage in the combination group exceeded the 1.2% rate of the monotherapy group creating a relative risk for bleeding of 3.4.
This trial demonstrates that for patients with PAD on antiplatelet therapy, the increased rate of bleeding without significant added benefit makes addition of warfarin inadvisable.1 Evidence of utility of combination therapy from studies in other arterial systems provides mixed results.2-4 Based on the results of this study, combination therapy cannot be advocated if the primary symptoms are from PAD.
Bottom line: This study provides further evidence that more is not always better when it comes to preventing thrombosis and ischemia in the peripheral arterial system. Antiplatelet agents are preferable for PAD to combination antiplatelet plus anticoagulation.
Citations:
- The Warfarin Antiplatelet Vascular Evaluation Trial Investigators. Oral anticoagulant and antiplatelet therapy and peripheral arterial disease. N Engl J Med. 2007 Jul 19;357(3):217-227.
- Hurlen M, Abdelnoor M, Smith P, et al. Warfarin, aspirin, or both after myocardial infarction. N Engl J Med. 2002 Sep 26;347(13):969-974.
- Mohr JP, Thompson JL, Lazar RM, et al. A comparison of warfarin and aspirin for the prevention of recurrent ischemic stroke. N Engl J Med. 2001 Nov 15;345(20):1444-1451.
- The ESPRIT Study Group. Medium intensity oral anticoagulants versus aspirin after cerebral ischaemia of arterial origin (ESPRIT): a randomised controlled trial. Lancet Neurol. 2007 Feb;6:115-124.
Does Transient Atrial Fibrillation Increase Stroke Risk After ST-Elevation Myocardial Infarction?
Background: Prior research has demonstrated that 2.1% of patients will suffer a stroke in the year following a heart attack. Persistent and paroxysmal atrial fibrillation (AF) are well recognized as risk factors for stroke, but the significance of transient ischemia-induced AF is less clear.
Study design: Retrospective cohort study
Setting: Queen Mary Hospital, Hong Kong
Synopsis: The study involved patients admitted for acute inferior ST-segment-elevation myocardial infarction (MI) with preserved left ventricular ejection fraction.
Transient AF that had converted back to normal sinus rhythm by discharge was observed in 14% of patients after the MI. Over the next three years the transient AF patients were 15 times more likely than those who remained in sinus rhythm during the index hospitalization to have recurrent AF (34% versus 2%). Despite antiplatelet therapy in both groups, ischemic stroke developed in 22% of patients who had transient AF following their MI, compared with only 4% in patients who did not (HR 5.1, confidence interval 2.4-11.2). Cerebrovascular accidents generally occurred simultaneously with recurrence of paroxysmal AF.1-2
The finding that patients with transient-ischemia-induced AF represents a group with markedly higher risk of ischemic stroke is compelling. It suggests that these patients may be candidates for combined antiplatelet and anticoagulant therapy. Trials of combined therapy following MI demonstrate that this strategy reduces the rate of recurrent cardiac ischemia, stroke, or death but does carry significantly increased risk of bleeding.3-4
Bottom line: The presence of transient AF following MI represents a significant risk factor for the development of subsequent paroxysmal AF. These patients have a five-fold increased risk of ischemic stroke over the next three years and should be considered for combined antiplatelet and anticoagulant therapy.
Citations:
- Chung-Wah S, Man-Hong J, Hee-Hwa H, et al. Transient atrial fibrillation complicating acute inferior myocardial infarction: implications for future risk of ischemic stroke. Chest. 2007 Mar 30;132(1):44-49.
- Witt BJ, Ballman KV, Brown RD Jr., Meverden RA, Jacobsen SJ, Roger VL. The incidence of stroke after myocardial infarction: a meta-analysis. Am J. Med. 2006;119(4):354 e1-9.
- Van Es RF, Jonker J, Verheugt F, et al. Aspirin and Coumadin after acute coronary syndromes (the ASPECT-2 study): a randomised controlled trial. Lancet. 2002 Jul 13;360(9327):109-113.
- Hurlen M, Abdelnoor M, Smith P, et al. Warfarin, aspirin, or both after myocardial infarction. N Engl J Med. 2002 Sep 26;347(13):969-974. TH
In This Edition
- Cost sharing for prescription medications increases consumption of more costly healthcare services
- Community-acquired pneumonia core measures can lead to unintended consequences
- Prophylactic revascularization has no clear benefit for high-risk patients undergoing vascular surgery
- Aspirin resistance correlates with adverse clinical events
- Low-molecular-weight heparin appears to have greater efficacy as a prophylactic agent against deep-vein thrombosis and pulmonary embolism
- Antipsychotic medications appear to be associated with increased risk of death in demented patients
- Anticoagulation plus antiplatelet therapy fails to show benefit for peripheral arterial disease
- Transient atrial fibrillation following myocardial infarction increases the risk of recurrence and stroke
Do Incentives to Encourage Use of Certain Medications Affect Care?
Background: Insurers are increasingly using financial mechanisms to affect pharmaceutical usage. These practices may affect medication use and health outcomes in ways that are poorly defined and difficult to detect.
Study design: Literature review
Synopsis: There are numerous structures for drug-cost sharing, and this study evaluated co-payments, tiers/co-insurance, benefit caps, formulary limitations, and reference pricing strategies for their effect on prescription drug usage and healthcare outcomes.
Included articles varied widely in study design, making generalizable results difficult to isolate, and insurers may have instituted more than one cost-sharing mechanism simultaneously. Overall, for every 10% increase in cost sharing (via copayments or co-insurance) there was an associated 2%-6% decrease in prescription drug spending. Increasing consumer costs for medications clearly decreases usage.
Some studies demonstrated that the decrease in medication utilization was more pronounced for “nonessential” medications over “essential” medications. However, in specific chronic illnesses this is clearly associated with greater usage of inpatient and emergency medical services.
Cost sharing was also more likely to have adverse health consequences in vulnerable populations, particularly the elderly and poor. One in four Medicaid patients couldn’t fill at least one prescription in the past year, as opposed to one in 10 privately insured patients who couldn’t purchase one or more medications.
Further impact on healthcare consumption and outcomes may be masked because it is difficult to determine individual disease severity, and the effect on the more severely ill would be expected to be greater. These authors attempted to sort out a complex interaction between cost, consumption, and health, and they found important trends.
The goal of cost sharing is to align consumption more clearly with appropriate and economic products, thereby using cost sharing as a public health tool. The consequence of creating the incentives for ill patients to forego necessary treatments is a counterbalancing concern that is supported in some, but not all, of the literature.
Bottom line: Cost sharing for prescription medications decreases medication spending and utilization but disproportionately affects the disadvantaged and increases consumption of more costly healthcare services in patients with some chronic illnesses.
Citation: Goldman DP, Joyce GF, Zheng Y. Prescription drug cost sharing: associations with medication and medical utilization and spending and health. JAMA. 2007;298(1):61-69.
Does Antibiotic Requirement for Suspected CAP Increase Misdiagnosis?
Background: Early administration of antibiotics in community-acquired pneumonia (CAP) improves patient outcomes. The Infectious Disease Society of America instituted guidelines that recommend initiation of antibiotics to all patients with suspected CAP within four hours of triage, and some payors are using this as a quality measure affecting reimbursement. However, this incentive may cause premature diagnosis of CAP and overuse of antibiotics.
Study design: Retrospective chart review
Setting: A large, high-volume teaching hospital with more than 500 beds and more than 112,000 annual emergency department (ED) visits
Synopsis: Charts of all patients with an admitting diagnosis of CAP were reviewed over two six-month periods. The initial review was prior to initiation of a four-hour antibiotics rule; the second was after a financial incentive to initiate antibiotics within four hours of triage was initiated.
After initiation of the four-hour rule, of the patients with an admitting diagnosis of CAP, significantly more patients received antibiotics within four hours of triage (66% versus 54%). However, the number of patients with abnormal chest X-ray findings associated with the diagnosis of CAP decreased from 28.5% to 20.6%, and the proportion of patients with a discharge diagnosis of CAP decreased from 75.9% to 58.9%.
The authors also used two diagnostic paradigms to make an independent diagnosis of CAP based on chart data. With the less rigorous independent analysis 44.7% of patients actually had CAP prior to the four-hour rule, and this fell to 36% after the four-hour rule. Using a more rigorous definition, only 32.7% of patients actually had CAP prior to initiation of the four-hour rule, and this fell to 27%.
There was no difference in length of stay or ICU transfers between the two analysis periods. The authors concluded that a four-hour rule increases premature diagnosis of CAP, presumably because providers felt compelled to initiate antibiotics before they had complete clinical data.
This tendency was associated with misuse and overuse of antibiotics, and increased laboratory testing, such as blood cultures, which had to be obtained before antibiotics were initiated. The authors emphasized the importance of reimbursement-associated quality measures creating incentives to treat the right patients for the correct diagnosis, and the potential harmful consequences of applying a quality-driven protocol to the wrong patient.
They suggest a six-hour rule would decrease the misdiagnosis of CAP. They also feel eliminating a mandatory time frame and requiring only that the first dose of antibiotics be administered in the ED will further ameliorate these effects.
Bottom line: Mandatory administration of antibiotics to patients with suspected CAP within four hours of triage increases the percentage of patients who receive antibiotics within four hours, but also increases the rate of misdiagnosis of CAP, inappropriate administration of antibiotics, and increased use of some laboratory services.
Citation: Kanwar M, Brar N, Khatib R, et al. Misdiagnosis of community-acquired pneumonia and inappropriate utilization of antibiotics: side effects of the 4-hour antibiotic administration rule. Chest. 2007 Jun;131(6):1865-1869.
Does prophylactic cardiac revascularization benefit patients undergoing vascular surgery?
Background: American College of Cardiology/American Heart Association Guidelines recommend referral for patients with multiple cardiac risk factors for non-invasive cardiac stress testing prior to surgery and prophylactic revascularization in high-risk patients. The authors performed a pilot analysis to determine how many patients would be needed to prospectively validate this recommendation in those with more significant ischemic cardiac disease.
Study design: Randomized controlled pilot study of 1,880 consecutive patients undergoing elective vascular surgery
Setting: Brazil, Belgium, the Netherlands, Italy, Serbia, and Montenegro
Synopsis: This was a pilot study to determine the necessary power to prove or disprove the benefit of the recommendation for cardiac revascularization in high-risk patients before major vascular surgery.
Prior research had shown that prophylactic revascularization is not of demonstrable benefit in this cohort. However, the majority of the patients in this previous trial had two-vessel disease and preserved left ventricular function. This study examined a sicker cohort of patients with more significant coronary artery disease and depressed left ventricular function.
This pilot screened all patients undergoing high-risk vascular surgery. All patients with three or more risk factors underwent non-invasive evaluation for cardiac ischemia. Patients with extensive ischemia were randomized to invasive evaluation and revascularization as appropriate or non-invasive management. Both arms received optimal medical management.
Prophylactic revascularization did not improve 30-day outcome after vascular surgery, demonstrated no difference in perioperative cardiac events, and found no difference in all-cause mortality or nonfatal myocardial infarction. Similarly, there was no evidence of long-term (at one year) difference between groups. The sample size needed to definitively establish that coronary revascularization is superior to medical therapy would be 300 patients per arm. That would require screening 9,000 patients.
Bottom line: Prophylactic revascularization has no clear benefit for high-risk patients undergoing vascular surgery, but a much larger sample size would be required to definitively prove or disprove benefit.
Citation: Poldermans D, Schouten O, Vidakovic R, et al. Clinical randomized trial to evaluate the safety of a noninvasive approach in high-risk patients undergoing major vascular surgery: the DECREASE-V pilot study. J. Am Coll Cardiol. 2007;49(17):1763-1769.
How Does Aspirin Resistance Affect Patients with Coronary Artery Disease?
Background: Although aspirin is used to decrease the risk of ischemic events, up to 45% of patients do not derive adequate anti-platelet activity. Few prospective studies have used laboratory-measured aspirin resistance to assess clinical outcomes.
Study design: Blinded cohort
Setting: Patients affiliated with Queen Mary Hospital, the University of Hong Kong.
Synopsis: Aspirin-induced platelet inhibition was measured quantitatively on 468 patients with stable coronary artery disease who take 80-325 mg of aspirin per day. The study found 128 patients were aspirin resistant. Aspirin resistance was more prevalent with increased age, female gender, renal insufficiency, anemia, and with use of low-dose aspirin. At follow up, aspirin-resistant patients were more likely to develop a primary outcome event: cardiovascular deaths, myocardial infarction, stroke, transient ischemic attack, and unstable angina. Aspirin resistance was an independent risk factor for developing the aforementioned outcomes, as are diabetes, prior myocardial infarction, and low hemoglobin.
Bottom line: Aspirin resistance, as defined by an aggregation-based assay, is associated with adverse outcomes in patients with stable coronary artery disease.
Citation: Chen W, Cheng X, Lee PY, et al. Aspirin resistance and adverse clinical events in patients with coronary artery disease. Am J Med. 2007 Jul;120(7):631-635.
Which Agents Best Prevent Venous Thromboembolism?
Background: Pulmonary emboli have been linked to 10% of in-hospital deaths. There continues to be a strong emphasis on prevention. Unfractionated heparin (UFH), low-molecular-weight heparin (LMWH), and selective factor Xa inhibitors are used for prophylaxis.
Study design: A meta-analysis of randomized controlled trials
Synopsis: The meta-analysis included 36 studies of hospitalized medical patients that compared UFH with control, LMWH with control, LMWH with UFH, and a selective factor Xa inhibitor with a placebo.
When each was compared with a control, UFH and LMWH were associated with a decreased risk of deep venous thrombosis (DVT) (risk ratio=0.33; 0.56) and pulmonary embolism (PE) (risk ratio=0.64; 0.37). Compared with control, LMWH three times daily was more effective than twice-daily dosing (risk ratio=0.27, 0.52). Through direct comparison of UFH and LMWH, LMWH was shown to have decreased DVT risk (risk ratio=0.68) and fewer injection site hematomas (risk ratio=0.47).
Neither UFH nor LMWH reduced mortality. LMWH and UFH were associated with significantly more bleeding events than control, but this increased risk was significant only for minor bleeding.
Bottom line: LMWH appears to have greater efficacy than UFH as a prophylactic agent against DVT/PE. If UFH is used, three times daily dosing is preferred.
Citation: Wein L, Wein S, Haas SJ, et al. Pharmacological venous thromboembolism prophylaxis in hospitalized medical patients. Arch Intern Med. 2007;167(14):1476-1486.
What Is the Association Between Antipsychotic Drugs and Mortality?
Background: Atypical antipsychotics prescribed off-label for problematic behaviors in dementia have been associated with risks including diabetes, stroke, and increased mortality. This resulted in the FDA placing a “black box” warning on atypical antipsychotics used for dementia. Subsequent studies have suggested that conventional antipsychotics are perhaps even more problematic.
Study Design: Retrospective cohort study
Synopsis: This trial found a small but significant increase in the risk of death in patients taking an antipsychotic medication.
The adjusted hazard ratio for death with the use of atypical antipsychotics in community dwelling patients with dementia was 1.3 (confidence interval 1.02-1.70). Similar to prior research, the authors found that conventional antipsychotics carried a higher risk than atypical agents.
Patients in long-term care settings also suffered increased risk compared with community dwelling patients. Interestingly, the increased risk of death was apparent after as little as a month of treatment.
As with all retrospective observational cohort trials, there remains the risk that an unanticipated confounding factor could skew the data and create a false association. However, the findings of this research support prior concerns that antipsychotics carry risk of increased mortality. This research bolsters the argument that these agents should not be used lightly or without full discussion of risks and benefits with the patient and/or proxy.
Bottom line: Antipsychotic agents used in patients with dementia may create increased risk of death. Potential benefit needs to be carefully weighted against this serious harm.
Citation: Gill S, Bronskill SE, Normand SL, et al. Antipsychotic drug use and mortality in older adults with dementia. Ann Intern Med. 2007 June 5;146(11):775-786.
Does Combination Therapy Help Prevent Serious Vascular Ischemic Events?
Background: Peripheral arterial disease (PAD) manifests as claudication and limb ischemia affecting 8.5 million Americans. Atherosclerotic disease in the periphery also reflects increased risk for ischemic events in the coronary and cranial circulations. Both antiplatelet agents and anticoagulation will decrease the probability of thrombus formation, although this must be weighed against bleeding risk.
Study design: Randomized, open-label, multicenter trial
Setting: Eighty centers in Europe, Asia, Australia, and North America
Synopsis: This trial randomized more than 2,000 patients with PAD to treatment with antiplatelet therapy (aspirin, ticlopidine, or clopidogrel) with or without additional anticoagulation.
During the next 3.5 years serious vascular events occurred at approximately the same rate in both combination and monotherapy groups (15.9% versus 17.4%, p=0.37). There was no significant difference between the occurrence of the composite ischemic endpoints or any of the individual endpoints. There was, however, a significantly higher rate of both moderate and life-threatening bleeding in the combination therapy group.
The 4% risk of life-threatening hemorrhage in the combination group exceeded the 1.2% rate of the monotherapy group creating a relative risk for bleeding of 3.4.
This trial demonstrates that for patients with PAD on antiplatelet therapy, the increased rate of bleeding without significant added benefit makes addition of warfarin inadvisable.1 Evidence of utility of combination therapy from studies in other arterial systems provides mixed results.2-4 Based on the results of this study, combination therapy cannot be advocated if the primary symptoms are from PAD.
Bottom line: This study provides further evidence that more is not always better when it comes to preventing thrombosis and ischemia in the peripheral arterial system. Antiplatelet agents are preferable for PAD to combination antiplatelet plus anticoagulation.
Citations:
- The Warfarin Antiplatelet Vascular Evaluation Trial Investigators. Oral anticoagulant and antiplatelet therapy and peripheral arterial disease. N Engl J Med. 2007 Jul 19;357(3):217-227.
- Hurlen M, Abdelnoor M, Smith P, et al. Warfarin, aspirin, or both after myocardial infarction. N Engl J Med. 2002 Sep 26;347(13):969-974.
- Mohr JP, Thompson JL, Lazar RM, et al. A comparison of warfarin and aspirin for the prevention of recurrent ischemic stroke. N Engl J Med. 2001 Nov 15;345(20):1444-1451.
- The ESPRIT Study Group. Medium intensity oral anticoagulants versus aspirin after cerebral ischaemia of arterial origin (ESPRIT): a randomised controlled trial. Lancet Neurol. 2007 Feb;6:115-124.
Does Transient Atrial Fibrillation Increase Stroke Risk After ST-Elevation Myocardial Infarction?
Background: Prior research has demonstrated that 2.1% of patients will suffer a stroke in the year following a heart attack. Persistent and paroxysmal atrial fibrillation (AF) are well recognized as risk factors for stroke, but the significance of transient ischemia-induced AF is less clear.
Study design: Retrospective cohort study
Setting: Queen Mary Hospital, Hong Kong
Synopsis: The study involved patients admitted for acute inferior ST-segment-elevation myocardial infarction (MI) with preserved left ventricular ejection fraction.
Transient AF that had converted back to normal sinus rhythm by discharge was observed in 14% of patients after the MI. Over the next three years the transient AF patients were 15 times more likely than those who remained in sinus rhythm during the index hospitalization to have recurrent AF (34% versus 2%). Despite antiplatelet therapy in both groups, ischemic stroke developed in 22% of patients who had transient AF following their MI, compared with only 4% in patients who did not (HR 5.1, confidence interval 2.4-11.2). Cerebrovascular accidents generally occurred simultaneously with recurrence of paroxysmal AF.1-2
The finding that patients with transient-ischemia-induced AF represents a group with markedly higher risk of ischemic stroke is compelling. It suggests that these patients may be candidates for combined antiplatelet and anticoagulant therapy. Trials of combined therapy following MI demonstrate that this strategy reduces the rate of recurrent cardiac ischemia, stroke, or death but does carry significantly increased risk of bleeding.3-4
Bottom line: The presence of transient AF following MI represents a significant risk factor for the development of subsequent paroxysmal AF. These patients have a five-fold increased risk of ischemic stroke over the next three years and should be considered for combined antiplatelet and anticoagulant therapy.
Citations:
- Chung-Wah S, Man-Hong J, Hee-Hwa H, et al. Transient atrial fibrillation complicating acute inferior myocardial infarction: implications for future risk of ischemic stroke. Chest. 2007 Mar 30;132(1):44-49.
- Witt BJ, Ballman KV, Brown RD Jr., Meverden RA, Jacobsen SJ, Roger VL. The incidence of stroke after myocardial infarction: a meta-analysis. Am J. Med. 2006;119(4):354 e1-9.
- Van Es RF, Jonker J, Verheugt F, et al. Aspirin and Coumadin after acute coronary syndromes (the ASPECT-2 study): a randomised controlled trial. Lancet. 2002 Jul 13;360(9327):109-113.
- Hurlen M, Abdelnoor M, Smith P, et al. Warfarin, aspirin, or both after myocardial infarction. N Engl J Med. 2002 Sep 26;347(13):969-974. TH
In This Edition
- Cost sharing for prescription medications increases consumption of more costly healthcare services
- Community-acquired pneumonia core measures can lead to unintended consequences
- Prophylactic revascularization has no clear benefit for high-risk patients undergoing vascular surgery
- Aspirin resistance correlates with adverse clinical events
- Low-molecular-weight heparin appears to have greater efficacy as a prophylactic agent against deep-vein thrombosis and pulmonary embolism
- Antipsychotic medications appear to be associated with increased risk of death in demented patients
- Anticoagulation plus antiplatelet therapy fails to show benefit for peripheral arterial disease
- Transient atrial fibrillation following myocardial infarction increases the risk of recurrence and stroke
Do Incentives to Encourage Use of Certain Medications Affect Care?
Background: Insurers are increasingly using financial mechanisms to affect pharmaceutical usage. These practices may affect medication use and health outcomes in ways that are poorly defined and difficult to detect.
Study design: Literature review
Synopsis: There are numerous structures for drug-cost sharing, and this study evaluated co-payments, tiers/co-insurance, benefit caps, formulary limitations, and reference pricing strategies for their effect on prescription drug usage and healthcare outcomes.
Included articles varied widely in study design, making generalizable results difficult to isolate, and insurers may have instituted more than one cost-sharing mechanism simultaneously. Overall, for every 10% increase in cost sharing (via copayments or co-insurance) there was an associated 2%-6% decrease in prescription drug spending. Increasing consumer costs for medications clearly decreases usage.
Some studies demonstrated that the decrease in medication utilization was more pronounced for “nonessential” medications over “essential” medications. However, in specific chronic illnesses this is clearly associated with greater usage of inpatient and emergency medical services.
Cost sharing was also more likely to have adverse health consequences in vulnerable populations, particularly the elderly and poor. One in four Medicaid patients couldn’t fill at least one prescription in the past year, as opposed to one in 10 privately insured patients who couldn’t purchase one or more medications.
Further impact on healthcare consumption and outcomes may be masked because it is difficult to determine individual disease severity, and the effect on the more severely ill would be expected to be greater. These authors attempted to sort out a complex interaction between cost, consumption, and health, and they found important trends.
The goal of cost sharing is to align consumption more clearly with appropriate and economic products, thereby using cost sharing as a public health tool. The consequence of creating the incentives for ill patients to forego necessary treatments is a counterbalancing concern that is supported in some, but not all, of the literature.
Bottom line: Cost sharing for prescription medications decreases medication spending and utilization but disproportionately affects the disadvantaged and increases consumption of more costly healthcare services in patients with some chronic illnesses.
Citation: Goldman DP, Joyce GF, Zheng Y. Prescription drug cost sharing: associations with medication and medical utilization and spending and health. JAMA. 2007;298(1):61-69.
Does Antibiotic Requirement for Suspected CAP Increase Misdiagnosis?
Background: Early administration of antibiotics in community-acquired pneumonia (CAP) improves patient outcomes. The Infectious Disease Society of America instituted guidelines that recommend initiation of antibiotics to all patients with suspected CAP within four hours of triage, and some payors are using this as a quality measure affecting reimbursement. However, this incentive may cause premature diagnosis of CAP and overuse of antibiotics.
Study design: Retrospective chart review
Setting: A large, high-volume teaching hospital with more than 500 beds and more than 112,000 annual emergency department (ED) visits
Synopsis: Charts of all patients with an admitting diagnosis of CAP were reviewed over two six-month periods. The initial review was prior to initiation of a four-hour antibiotics rule; the second was after a financial incentive to initiate antibiotics within four hours of triage was initiated.
After initiation of the four-hour rule, of the patients with an admitting diagnosis of CAP, significantly more patients received antibiotics within four hours of triage (66% versus 54%). However, the number of patients with abnormal chest X-ray findings associated with the diagnosis of CAP decreased from 28.5% to 20.6%, and the proportion of patients with a discharge diagnosis of CAP decreased from 75.9% to 58.9%.
The authors also used two diagnostic paradigms to make an independent diagnosis of CAP based on chart data. With the less rigorous independent analysis 44.7% of patients actually had CAP prior to the four-hour rule, and this fell to 36% after the four-hour rule. Using a more rigorous definition, only 32.7% of patients actually had CAP prior to initiation of the four-hour rule, and this fell to 27%.
There was no difference in length of stay or ICU transfers between the two analysis periods. The authors concluded that a four-hour rule increases premature diagnosis of CAP, presumably because providers felt compelled to initiate antibiotics before they had complete clinical data.
This tendency was associated with misuse and overuse of antibiotics, and increased laboratory testing, such as blood cultures, which had to be obtained before antibiotics were initiated. The authors emphasized the importance of reimbursement-associated quality measures creating incentives to treat the right patients for the correct diagnosis, and the potential harmful consequences of applying a quality-driven protocol to the wrong patient.
They suggest a six-hour rule would decrease the misdiagnosis of CAP. They also feel eliminating a mandatory time frame and requiring only that the first dose of antibiotics be administered in the ED will further ameliorate these effects.
Bottom line: Mandatory administration of antibiotics to patients with suspected CAP within four hours of triage increases the percentage of patients who receive antibiotics within four hours, but also increases the rate of misdiagnosis of CAP, inappropriate administration of antibiotics, and increased use of some laboratory services.
Citation: Kanwar M, Brar N, Khatib R, et al. Misdiagnosis of community-acquired pneumonia and inappropriate utilization of antibiotics: side effects of the 4-hour antibiotic administration rule. Chest. 2007 Jun;131(6):1865-1869.
Does prophylactic cardiac revascularization benefit patients undergoing vascular surgery?
Background: American College of Cardiology/American Heart Association Guidelines recommend referral for patients with multiple cardiac risk factors for non-invasive cardiac stress testing prior to surgery and prophylactic revascularization in high-risk patients. The authors performed a pilot analysis to determine how many patients would be needed to prospectively validate this recommendation in those with more significant ischemic cardiac disease.
Study design: Randomized controlled pilot study of 1,880 consecutive patients undergoing elective vascular surgery
Setting: Brazil, Belgium, the Netherlands, Italy, Serbia, and Montenegro
Synopsis: This was a pilot study to determine the necessary power to prove or disprove the benefit of the recommendation for cardiac revascularization in high-risk patients before major vascular surgery.
Prior research had shown that prophylactic revascularization is not of demonstrable benefit in this cohort. However, the majority of the patients in this previous trial had two-vessel disease and preserved left ventricular function. This study examined a sicker cohort of patients with more significant coronary artery disease and depressed left ventricular function.
This pilot screened all patients undergoing high-risk vascular surgery. All patients with three or more risk factors underwent non-invasive evaluation for cardiac ischemia. Patients with extensive ischemia were randomized to invasive evaluation and revascularization as appropriate or non-invasive management. Both arms received optimal medical management.
Prophylactic revascularization did not improve 30-day outcome after vascular surgery, demonstrated no difference in perioperative cardiac events, and found no difference in all-cause mortality or nonfatal myocardial infarction. Similarly, there was no evidence of long-term (at one year) difference between groups. The sample size needed to definitively establish that coronary revascularization is superior to medical therapy would be 300 patients per arm. That would require screening 9,000 patients.
Bottom line: Prophylactic revascularization has no clear benefit for high-risk patients undergoing vascular surgery, but a much larger sample size would be required to definitively prove or disprove benefit.
Citation: Poldermans D, Schouten O, Vidakovic R, et al. Clinical randomized trial to evaluate the safety of a noninvasive approach in high-risk patients undergoing major vascular surgery: the DECREASE-V pilot study. J. Am Coll Cardiol. 2007;49(17):1763-1769.
How Does Aspirin Resistance Affect Patients with Coronary Artery Disease?
Background: Although aspirin is used to decrease the risk of ischemic events, up to 45% of patients do not derive adequate anti-platelet activity. Few prospective studies have used laboratory-measured aspirin resistance to assess clinical outcomes.
Study design: Blinded cohort
Setting: Patients affiliated with Queen Mary Hospital, the University of Hong Kong.
Synopsis: Aspirin-induced platelet inhibition was measured quantitatively on 468 patients with stable coronary artery disease who take 80-325 mg of aspirin per day. The study found 128 patients were aspirin resistant. Aspirin resistance was more prevalent with increased age, female gender, renal insufficiency, anemia, and with use of low-dose aspirin. At follow up, aspirin-resistant patients were more likely to develop a primary outcome event: cardiovascular deaths, myocardial infarction, stroke, transient ischemic attack, and unstable angina. Aspirin resistance was an independent risk factor for developing the aforementioned outcomes, as are diabetes, prior myocardial infarction, and low hemoglobin.
Bottom line: Aspirin resistance, as defined by an aggregation-based assay, is associated with adverse outcomes in patients with stable coronary artery disease.
Citation: Chen W, Cheng X, Lee PY, et al. Aspirin resistance and adverse clinical events in patients with coronary artery disease. Am J Med. 2007 Jul;120(7):631-635.
Which Agents Best Prevent Venous Thromboembolism?
Background: Pulmonary emboli have been linked to 10% of in-hospital deaths. There continues to be a strong emphasis on prevention. Unfractionated heparin (UFH), low-molecular-weight heparin (LMWH), and selective factor Xa inhibitors are used for prophylaxis.
Study design: A meta-analysis of randomized controlled trials
Synopsis: The meta-analysis included 36 studies of hospitalized medical patients that compared UFH with control, LMWH with control, LMWH with UFH, and a selective factor Xa inhibitor with a placebo.
When each was compared with a control, UFH and LMWH were associated with a decreased risk of deep venous thrombosis (DVT) (risk ratio=0.33; 0.56) and pulmonary embolism (PE) (risk ratio=0.64; 0.37). Compared with control, LMWH three times daily was more effective than twice-daily dosing (risk ratio=0.27, 0.52). Through direct comparison of UFH and LMWH, LMWH was shown to have decreased DVT risk (risk ratio=0.68) and fewer injection site hematomas (risk ratio=0.47).
Neither UFH nor LMWH reduced mortality. LMWH and UFH were associated with significantly more bleeding events than control, but this increased risk was significant only for minor bleeding.
Bottom line: LMWH appears to have greater efficacy than UFH as a prophylactic agent against DVT/PE. If UFH is used, three times daily dosing is preferred.
Citation: Wein L, Wein S, Haas SJ, et al. Pharmacological venous thromboembolism prophylaxis in hospitalized medical patients. Arch Intern Med. 2007;167(14):1476-1486.
What Is the Association Between Antipsychotic Drugs and Mortality?
Background: Atypical antipsychotics prescribed off-label for problematic behaviors in dementia have been associated with risks including diabetes, stroke, and increased mortality. This resulted in the FDA placing a “black box” warning on atypical antipsychotics used for dementia. Subsequent studies have suggested that conventional antipsychotics are perhaps even more problematic.
Study Design: Retrospective cohort study
Synopsis: This trial found a small but significant increase in the risk of death in patients taking an antipsychotic medication.
The adjusted hazard ratio for death with the use of atypical antipsychotics in community dwelling patients with dementia was 1.3 (confidence interval 1.02-1.70). Similar to prior research, the authors found that conventional antipsychotics carried a higher risk than atypical agents.
Patients in long-term care settings also suffered increased risk compared with community dwelling patients. Interestingly, the increased risk of death was apparent after as little as a month of treatment.
As with all retrospective observational cohort trials, there remains the risk that an unanticipated confounding factor could skew the data and create a false association. However, the findings of this research support prior concerns that antipsychotics carry risk of increased mortality. This research bolsters the argument that these agents should not be used lightly or without full discussion of risks and benefits with the patient and/or proxy.
Bottom line: Antipsychotic agents used in patients with dementia may create increased risk of death. Potential benefit needs to be carefully weighted against this serious harm.
Citation: Gill S, Bronskill SE, Normand SL, et al. Antipsychotic drug use and mortality in older adults with dementia. Ann Intern Med. 2007 June 5;146(11):775-786.
Does Combination Therapy Help Prevent Serious Vascular Ischemic Events?
Background: Peripheral arterial disease (PAD) manifests as claudication and limb ischemia affecting 8.5 million Americans. Atherosclerotic disease in the periphery also reflects increased risk for ischemic events in the coronary and cranial circulations. Both antiplatelet agents and anticoagulation will decrease the probability of thrombus formation, although this must be weighed against bleeding risk.
Study design: Randomized, open-label, multicenter trial
Setting: Eighty centers in Europe, Asia, Australia, and North America
Synopsis: This trial randomized more than 2,000 patients with PAD to treatment with antiplatelet therapy (aspirin, ticlopidine, or clopidogrel) with or without additional anticoagulation.
During the next 3.5 years serious vascular events occurred at approximately the same rate in both combination and monotherapy groups (15.9% versus 17.4%, p=0.37). There was no significant difference between the occurrence of the composite ischemic endpoints or any of the individual endpoints. There was, however, a significantly higher rate of both moderate and life-threatening bleeding in the combination therapy group.
The 4% risk of life-threatening hemorrhage in the combination group exceeded the 1.2% rate of the monotherapy group creating a relative risk for bleeding of 3.4.
This trial demonstrates that for patients with PAD on antiplatelet therapy, the increased rate of bleeding without significant added benefit makes addition of warfarin inadvisable.1 Evidence of utility of combination therapy from studies in other arterial systems provides mixed results.2-4 Based on the results of this study, combination therapy cannot be advocated if the primary symptoms are from PAD.
Bottom line: This study provides further evidence that more is not always better when it comes to preventing thrombosis and ischemia in the peripheral arterial system. Antiplatelet agents are preferable for PAD to combination antiplatelet plus anticoagulation.
Citations:
- The Warfarin Antiplatelet Vascular Evaluation Trial Investigators. Oral anticoagulant and antiplatelet therapy and peripheral arterial disease. N Engl J Med. 2007 Jul 19;357(3):217-227.
- Hurlen M, Abdelnoor M, Smith P, et al. Warfarin, aspirin, or both after myocardial infarction. N Engl J Med. 2002 Sep 26;347(13):969-974.
- Mohr JP, Thompson JL, Lazar RM, et al. A comparison of warfarin and aspirin for the prevention of recurrent ischemic stroke. N Engl J Med. 2001 Nov 15;345(20):1444-1451.
- The ESPRIT Study Group. Medium intensity oral anticoagulants versus aspirin after cerebral ischaemia of arterial origin (ESPRIT): a randomised controlled trial. Lancet Neurol. 2007 Feb;6:115-124.
Does Transient Atrial Fibrillation Increase Stroke Risk After ST-Elevation Myocardial Infarction?
Background: Prior research has demonstrated that 2.1% of patients will suffer a stroke in the year following a heart attack. Persistent and paroxysmal atrial fibrillation (AF) are well recognized as risk factors for stroke, but the significance of transient ischemia-induced AF is less clear.
Study design: Retrospective cohort study
Setting: Queen Mary Hospital, Hong Kong
Synopsis: The study involved patients admitted for acute inferior ST-segment-elevation myocardial infarction (MI) with preserved left ventricular ejection fraction.
Transient AF that had converted back to normal sinus rhythm by discharge was observed in 14% of patients after the MI. Over the next three years the transient AF patients were 15 times more likely than those who remained in sinus rhythm during the index hospitalization to have recurrent AF (34% versus 2%). Despite antiplatelet therapy in both groups, ischemic stroke developed in 22% of patients who had transient AF following their MI, compared with only 4% in patients who did not (HR 5.1, confidence interval 2.4-11.2). Cerebrovascular accidents generally occurred simultaneously with recurrence of paroxysmal AF.1-2
The finding that patients with transient-ischemia-induced AF represents a group with markedly higher risk of ischemic stroke is compelling. It suggests that these patients may be candidates for combined antiplatelet and anticoagulant therapy. Trials of combined therapy following MI demonstrate that this strategy reduces the rate of recurrent cardiac ischemia, stroke, or death but does carry significantly increased risk of bleeding.3-4
Bottom line: The presence of transient AF following MI represents a significant risk factor for the development of subsequent paroxysmal AF. These patients have a five-fold increased risk of ischemic stroke over the next three years and should be considered for combined antiplatelet and anticoagulant therapy.
Citations:
- Chung-Wah S, Man-Hong J, Hee-Hwa H, et al. Transient atrial fibrillation complicating acute inferior myocardial infarction: implications for future risk of ischemic stroke. Chest. 2007 Mar 30;132(1):44-49.
- Witt BJ, Ballman KV, Brown RD Jr., Meverden RA, Jacobsen SJ, Roger VL. The incidence of stroke after myocardial infarction: a meta-analysis. Am J. Med. 2006;119(4):354 e1-9.
- Van Es RF, Jonker J, Verheugt F, et al. Aspirin and Coumadin after acute coronary syndromes (the ASPECT-2 study): a randomised controlled trial. Lancet. 2002 Jul 13;360(9327):109-113.
- Hurlen M, Abdelnoor M, Smith P, et al. Warfarin, aspirin, or both after myocardial infarction. N Engl J Med. 2002 Sep 26;347(13):969-974. TH
Renewal Made Easy
Effective April 1, SHM migrated from the fiscal-year renewal process that exists in many medical societies. Now, all members who wish to continue their membership must renew 12 months from the time they joined or last renewed.
As members will recall, SHM’s previous fiscal-year (or calendar-year) renewal process meant dues paid between July 1 and June 30 applied to the current membership year, regardless of the date of joining or renewal. Because full payment could be made in January or February and required again a few months later, this did not sit well with SHM or—more importantly—its members.
Why make the change? Two reasons:
- Fairness. Each membership payment should equal 12 months of member benefits; and
- Simplicity. It will be easier for members to plan for renewal and budget accordingly.
Chapter Summary
Western Massachusetts

JOIN THE SHM TEAM
Interested in being a part of an SHM committee or task force? Now’s your chance. Nominations are open for SHM’s committees and task forces. This is your opportunity to help shape the future of SHM and the hospital medicine movement.
To nominate yourself, visit the SHM Web site, www.hospitalmedicine.org, and click on “About SHM,” then click “Committees.” Here, you will see a full listing of committees, as well as task forces and their current members.
For each committee you would like to serve on, please submit your name and a one-to-two paragraph statement about why you are qualified or interested. E-mail this information to Joi Seabrooks at jseabrooks@hospitalmedicine.org by Dec. 7. Appointments will be made by early February, take effect in April 2008, and last one year.
In the short term, this change means little for current members as long as they renew within the grace period. In the long term, members will receive an expiration date with their payment so they know they’re getting a full year’s worth of benefits.
It’s never too late to join or renew. Whether your membership has lapsed in the past year, two years, or five, renewing is as easy as a phone call or access to the Internet. SHM membership representatives can be reached by calling toll free (800) 843-3360, or by visiting www.joinshm.org. If you’re not sure of your membership status, have questions about membership or the new renewal process, or general feedback as an SHM member, please e-mail membership@hospitalmedicine.org.
Lessons for Leaders
SHM hosted another sold-out Leadership Academy at the Marriott Riverwalk in San Antonio, Texas, Nov. 5-8. The meeting attracted more than 170 hospital medicine leaders for the Level I and Level II courses.
The Leadership Academy Level I was designed to provide leaders in hospital medicine the skills and resources to lead and manage programs. Small group sessions gave attendees a chance to interact with faculty and share personal experiences from their own institutions.
Jack Silversin, DMD, DrPh, president of the consulting firm Amicus in Cambridge, Mass., presented his well-known “broken squares” demonstration to teach the group to work together to learn effective communication. This course allowed attendees to evaluate personal leadership strengths and weaknesses and apply them to everyday leadership and management challenges.
The Level II course focused on discussions about culture change, negotiation skills, and finance. Level II faculty member Leonard Marcus, PhD, described how “meta-leadership” in hospital medicine links individuals through their leader’s vision to create enthusiastic followers. Dr. Marcus is founding director of the Program for Health Care Negotiation and Conflict Resolution at the Harvard School of Public Health. Mike Guthrie, MD, MBA, focused his presentation on finance and taught participants concepts and tools for mastering the case for quality improvement and performance management. Dr. Guthrie is executive-in-residence at the University of Colorado Denver School of Business.
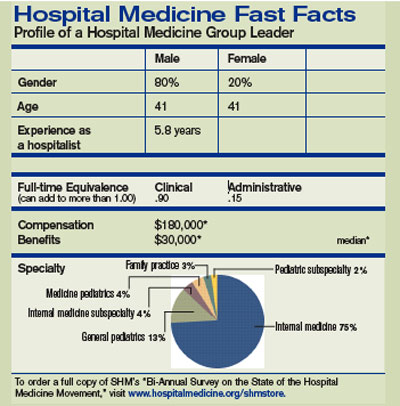
This course is a must-have for those who want to expand upon leadership skills learned in Level I or for those who have an MBA and want to improve their leadership in clinical care.
The skills discussed in this session are essential to developing and implementing quality improvement programs, patient safety initiatives, and other programs to make system changes that improve patient care. Don’t miss out on the next opportunity to attend Level II.
Leadership Academy Level I and II were jam-packed with relevant materials and tools applicable to business and the real world.
This is an outstanding opportunity for those beginning their leadership journey or those wanting to take their skills to the next level.
Don’t miss the next opportunity to become a leader in hospital medicine. The next meeting will take place Feb. 5-8, 2008, at the Loews Lake Las Vegas Resort in Las Vegas. Visit www.hospitalmedicine.org/leadership or call (800) 843-3360 for more information.
SHM BEHIND THE SCENES
The SHM team seeks your feedback at fall conferences
By Todd Von Deak

During my years in association management, I have seen time and time again how easy it is—and how dangerous it can be—to lose touch with your membership. If you truly want to deliver a high-quality product to all who belong to your organization, it is not enough to just read letters or listen to your most active members who serve on committees.
SHM places high value on maintaining a strong connection to all members. To that end, we employ a variety of feedback mechanisms that range from ensuring that all staff have the opportunity to interact with members on the phone, to fielding regular surveys that solicit feedback on a variety of topics.
Each fall, we do something that can easily go unnoticed. But it’s crucial to maintaining a strong connection to the community we serve. Over a four-month span, our staff and volunteer leaders will participate in 10 to 12 hospital medicine conferences ranging from Vancouver, Canada, to Savannah, Ga.
At these conferences, you are likely to find us in the exhibit hall staffing an SHM display. Other times, a physician making a presentation about some facet of hospital medicine will represent us and include a couple of slides about the latest news from within SHM.
No matter our role at a conference, our goal is the same. Whether we’re at an event for one or four days, we want to talk with as many people as possible about everything going on within hospital medicine.
We’re also anxious to hear the latest from the “front lines” and learn new ways we can improve our products and services to better serve your needs. To that end, we keep detailed statistics about the issues you raise and questions you ask when you visit our booth. These metrics are shared with executive management so they have the benefit of direct feedback.
Sure, these events are about signing up new members, selling copies of popular publications, and encouraging registrations for upcoming events. If we didn’t do these things, our dues would be higher.
These events are just as much about making sure we don’t lose touch with the very reason that we all come to work each day: You. You can’t replace the opportunity to look people in the eye, thank them for their support, and hear firsthand how you can make a difference for them personally and professionally.
Next time you’re attending a conference, please take a moment to see if SHM is an exhibitor. If we are, I hope you’ll visit our booth and let us know what’s on your mind and how SHM can continue to improve what we offer.
If you know of an event where hospital medicine is a hot topic and you think we’d benefit from attending, I’d love to hear from you. My e-mail is tvd@hospitalmedicine.org. TH
Effective April 1, SHM migrated from the fiscal-year renewal process that exists in many medical societies. Now, all members who wish to continue their membership must renew 12 months from the time they joined or last renewed.
As members will recall, SHM’s previous fiscal-year (or calendar-year) renewal process meant dues paid between July 1 and June 30 applied to the current membership year, regardless of the date of joining or renewal. Because full payment could be made in January or February and required again a few months later, this did not sit well with SHM or—more importantly—its members.
Why make the change? Two reasons:
- Fairness. Each membership payment should equal 12 months of member benefits; and
- Simplicity. It will be easier for members to plan for renewal and budget accordingly.
Chapter Summary
Western Massachusetts
JOIN THE SHM TEAM
Interested in being a part of an SHM committee or task force? Now’s your chance. Nominations are open for SHM’s committees and task forces. This is your opportunity to help shape the future of SHM and the hospital medicine movement.
To nominate yourself, visit the SHM Web site, www.hospitalmedicine.org, and click on “About SHM,” then click “Committees.” Here, you will see a full listing of committees, as well as task forces and their current members.
For each committee you would like to serve on, please submit your name and a one-to-two paragraph statement about why you are qualified or interested. E-mail this information to Joi Seabrooks at jseabrooks@hospitalmedicine.org by Dec. 7. Appointments will be made by early February, take effect in April 2008, and last one year.
In the short term, this change means little for current members as long as they renew within the grace period. In the long term, members will receive an expiration date with their payment so they know they’re getting a full year’s worth of benefits.
It’s never too late to join or renew. Whether your membership has lapsed in the past year, two years, or five, renewing is as easy as a phone call or access to the Internet. SHM membership representatives can be reached by calling toll free (800) 843-3360, or by visiting www.joinshm.org. If you’re not sure of your membership status, have questions about membership or the new renewal process, or general feedback as an SHM member, please e-mail membership@hospitalmedicine.org.
Lessons for Leaders
SHM hosted another sold-out Leadership Academy at the Marriott Riverwalk in San Antonio, Texas, Nov. 5-8. The meeting attracted more than 170 hospital medicine leaders for the Level I and Level II courses.
The Leadership Academy Level I was designed to provide leaders in hospital medicine the skills and resources to lead and manage programs. Small group sessions gave attendees a chance to interact with faculty and share personal experiences from their own institutions.
Jack Silversin, DMD, DrPh, president of the consulting firm Amicus in Cambridge, Mass., presented his well-known “broken squares” demonstration to teach the group to work together to learn effective communication. This course allowed attendees to evaluate personal leadership strengths and weaknesses and apply them to everyday leadership and management challenges.
The Level II course focused on discussions about culture change, negotiation skills, and finance. Level II faculty member Leonard Marcus, PhD, described how “meta-leadership” in hospital medicine links individuals through their leader’s vision to create enthusiastic followers. Dr. Marcus is founding director of the Program for Health Care Negotiation and Conflict Resolution at the Harvard School of Public Health. Mike Guthrie, MD, MBA, focused his presentation on finance and taught participants concepts and tools for mastering the case for quality improvement and performance management. Dr. Guthrie is executive-in-residence at the University of Colorado Denver School of Business.
This course is a must-have for those who want to expand upon leadership skills learned in Level I or for those who have an MBA and want to improve their leadership in clinical care.
The skills discussed in this session are essential to developing and implementing quality improvement programs, patient safety initiatives, and other programs to make system changes that improve patient care. Don’t miss out on the next opportunity to attend Level II.
Leadership Academy Level I and II were jam-packed with relevant materials and tools applicable to business and the real world.
This is an outstanding opportunity for those beginning their leadership journey or those wanting to take their skills to the next level.
Don’t miss the next opportunity to become a leader in hospital medicine. The next meeting will take place Feb. 5-8, 2008, at the Loews Lake Las Vegas Resort in Las Vegas. Visit www.hospitalmedicine.org/leadership or call (800) 843-3360 for more information.
SHM BEHIND THE SCENES
The SHM team seeks your feedback at fall conferences
By Todd Von Deak
During my years in association management, I have seen time and time again how easy it is—and how dangerous it can be—to lose touch with your membership. If you truly want to deliver a high-quality product to all who belong to your organization, it is not enough to just read letters or listen to your most active members who serve on committees.
SHM places high value on maintaining a strong connection to all members. To that end, we employ a variety of feedback mechanisms that range from ensuring that all staff have the opportunity to interact with members on the phone, to fielding regular surveys that solicit feedback on a variety of topics.
Each fall, we do something that can easily go unnoticed. But it’s crucial to maintaining a strong connection to the community we serve. Over a four-month span, our staff and volunteer leaders will participate in 10 to 12 hospital medicine conferences ranging from Vancouver, Canada, to Savannah, Ga.
At these conferences, you are likely to find us in the exhibit hall staffing an SHM display. Other times, a physician making a presentation about some facet of hospital medicine will represent us and include a couple of slides about the latest news from within SHM.
No matter our role at a conference, our goal is the same. Whether we’re at an event for one or four days, we want to talk with as many people as possible about everything going on within hospital medicine.
We’re also anxious to hear the latest from the “front lines” and learn new ways we can improve our products and services to better serve your needs. To that end, we keep detailed statistics about the issues you raise and questions you ask when you visit our booth. These metrics are shared with executive management so they have the benefit of direct feedback.
Sure, these events are about signing up new members, selling copies of popular publications, and encouraging registrations for upcoming events. If we didn’t do these things, our dues would be higher.
These events are just as much about making sure we don’t lose touch with the very reason that we all come to work each day: You. You can’t replace the opportunity to look people in the eye, thank them for their support, and hear firsthand how you can make a difference for them personally and professionally.
Next time you’re attending a conference, please take a moment to see if SHM is an exhibitor. If we are, I hope you’ll visit our booth and let us know what’s on your mind and how SHM can continue to improve what we offer.
If you know of an event where hospital medicine is a hot topic and you think we’d benefit from attending, I’d love to hear from you. My e-mail is tvd@hospitalmedicine.org. TH
Effective April 1, SHM migrated from the fiscal-year renewal process that exists in many medical societies. Now, all members who wish to continue their membership must renew 12 months from the time they joined or last renewed.
As members will recall, SHM’s previous fiscal-year (or calendar-year) renewal process meant dues paid between July 1 and June 30 applied to the current membership year, regardless of the date of joining or renewal. Because full payment could be made in January or February and required again a few months later, this did not sit well with SHM or—more importantly—its members.
Why make the change? Two reasons:
- Fairness. Each membership payment should equal 12 months of member benefits; and
- Simplicity. It will be easier for members to plan for renewal and budget accordingly.
Chapter Summary
Western Massachusetts
JOIN THE SHM TEAM
Interested in being a part of an SHM committee or task force? Now’s your chance. Nominations are open for SHM’s committees and task forces. This is your opportunity to help shape the future of SHM and the hospital medicine movement.
To nominate yourself, visit the SHM Web site, www.hospitalmedicine.org, and click on “About SHM,” then click “Committees.” Here, you will see a full listing of committees, as well as task forces and their current members.
For each committee you would like to serve on, please submit your name and a one-to-two paragraph statement about why you are qualified or interested. E-mail this information to Joi Seabrooks at jseabrooks@hospitalmedicine.org by Dec. 7. Appointments will be made by early February, take effect in April 2008, and last one year.
In the short term, this change means little for current members as long as they renew within the grace period. In the long term, members will receive an expiration date with their payment so they know they’re getting a full year’s worth of benefits.
It’s never too late to join or renew. Whether your membership has lapsed in the past year, two years, or five, renewing is as easy as a phone call or access to the Internet. SHM membership representatives can be reached by calling toll free (800) 843-3360, or by visiting www.joinshm.org. If you’re not sure of your membership status, have questions about membership or the new renewal process, or general feedback as an SHM member, please e-mail membership@hospitalmedicine.org.
Lessons for Leaders
SHM hosted another sold-out Leadership Academy at the Marriott Riverwalk in San Antonio, Texas, Nov. 5-8. The meeting attracted more than 170 hospital medicine leaders for the Level I and Level II courses.
The Leadership Academy Level I was designed to provide leaders in hospital medicine the skills and resources to lead and manage programs. Small group sessions gave attendees a chance to interact with faculty and share personal experiences from their own institutions.
Jack Silversin, DMD, DrPh, president of the consulting firm Amicus in Cambridge, Mass., presented his well-known “broken squares” demonstration to teach the group to work together to learn effective communication. This course allowed attendees to evaluate personal leadership strengths and weaknesses and apply them to everyday leadership and management challenges.
The Level II course focused on discussions about culture change, negotiation skills, and finance. Level II faculty member Leonard Marcus, PhD, described how “meta-leadership” in hospital medicine links individuals through their leader’s vision to create enthusiastic followers. Dr. Marcus is founding director of the Program for Health Care Negotiation and Conflict Resolution at the Harvard School of Public Health. Mike Guthrie, MD, MBA, focused his presentation on finance and taught participants concepts and tools for mastering the case for quality improvement and performance management. Dr. Guthrie is executive-in-residence at the University of Colorado Denver School of Business.
This course is a must-have for those who want to expand upon leadership skills learned in Level I or for those who have an MBA and want to improve their leadership in clinical care.
The skills discussed in this session are essential to developing and implementing quality improvement programs, patient safety initiatives, and other programs to make system changes that improve patient care. Don’t miss out on the next opportunity to attend Level II.
Leadership Academy Level I and II were jam-packed with relevant materials and tools applicable to business and the real world.
This is an outstanding opportunity for those beginning their leadership journey or those wanting to take their skills to the next level.
Don’t miss the next opportunity to become a leader in hospital medicine. The next meeting will take place Feb. 5-8, 2008, at the Loews Lake Las Vegas Resort in Las Vegas. Visit www.hospitalmedicine.org/leadership or call (800) 843-3360 for more information.
SHM BEHIND THE SCENES
The SHM team seeks your feedback at fall conferences
By Todd Von Deak
During my years in association management, I have seen time and time again how easy it is—and how dangerous it can be—to lose touch with your membership. If you truly want to deliver a high-quality product to all who belong to your organization, it is not enough to just read letters or listen to your most active members who serve on committees.
SHM places high value on maintaining a strong connection to all members. To that end, we employ a variety of feedback mechanisms that range from ensuring that all staff have the opportunity to interact with members on the phone, to fielding regular surveys that solicit feedback on a variety of topics.
Each fall, we do something that can easily go unnoticed. But it’s crucial to maintaining a strong connection to the community we serve. Over a four-month span, our staff and volunteer leaders will participate in 10 to 12 hospital medicine conferences ranging from Vancouver, Canada, to Savannah, Ga.
At these conferences, you are likely to find us in the exhibit hall staffing an SHM display. Other times, a physician making a presentation about some facet of hospital medicine will represent us and include a couple of slides about the latest news from within SHM.
No matter our role at a conference, our goal is the same. Whether we’re at an event for one or four days, we want to talk with as many people as possible about everything going on within hospital medicine.
We’re also anxious to hear the latest from the “front lines” and learn new ways we can improve our products and services to better serve your needs. To that end, we keep detailed statistics about the issues you raise and questions you ask when you visit our booth. These metrics are shared with executive management so they have the benefit of direct feedback.
Sure, these events are about signing up new members, selling copies of popular publications, and encouraging registrations for upcoming events. If we didn’t do these things, our dues would be higher.
These events are just as much about making sure we don’t lose touch with the very reason that we all come to work each day: You. You can’t replace the opportunity to look people in the eye, thank them for their support, and hear firsthand how you can make a difference for them personally and professionally.
Next time you’re attending a conference, please take a moment to see if SHM is an exhibitor. If we are, I hope you’ll visit our booth and let us know what’s on your mind and how SHM can continue to improve what we offer.
If you know of an event where hospital medicine is a hot topic and you think we’d benefit from attending, I’d love to hear from you. My e-mail is tvd@hospitalmedicine.org. TH
Video Interpreters Help Hospitals, Patients Connect
Twenty years ago, when Andrew Panos’ brother was involved in a car crash during a vacation in Puerto Vallarta, Mexico, there were no interpretation services available at the hospital where he was taken.
When the family was finally able to get him to Los Angeles, doctors concluded that if he had stayed in Mexico another eight hours he would have died from blood poisoning.
This experience—and the realization that even in his hometown of Columbus, Ohio, there was a serious need for fast, accurate healthcare interpretation services—prompted Andrew Panos to create the Language Access Network (LAN), a face-to-face live audio-video interpretation service, in 2003.
The system, My Accessible Real-Time Trusted Interpreter (MARTTI) is available in 23 hospitals. The system centralizes video interpretation into a center staffed by medically trained interpreter. In a hospital subscribing to the service, a provider can call LAN’s center in Columbus, Ohio, 24 hours a day, seven days a week. Users can choose among 150 languages, including a range of Chinese dialects and American Sign Language, and access an on-screen interpreter.
To use the system, a hospital purchases a block of minutes each month; charges are incurred when interpretations are sought.
“Some people have referred to it as the OnStar of interpreting,” says Panos, referring to the vehicle security system. “They are finding it more affordable than the cost of having on-site interpreters or calling an agency and having to pay a two-hour minimum and then having a wait time of upward of an hour.”
LAN’s system is a boon for hospitals that deal daily with Americans with Disabilities Act compliance.
“For instance, in New York they’re demanding that interpreters be provided within 10 minutes,” Panos says. “Having an American Sign Language interpreter in that short a time has really put quite a burden on their hospitals. With our system, since it is available with the push of a button, the result has been amazing.”
At Boston Medical Center (BMC), implementing MARTTI has meant synchronizing the institution’s wireless system with LAN’s system.
“It’s been a marriage of the two,” says Oscar Arocha, director of interpreter services and guest support services at BMC. Its 44 full-time interpreters were already providing in-person interpreting wherever possible. Then the hospital began telephone interpretation, and has since installed MARTTI units.
It was crucial to Arocha and BMC’s administrators that the service be available wirelessly so video units could be wheeled from place to place. Desktop units are also available from LAN.
“The user turns the video unit on and waits two or three seconds for the operator to come up on screen,” says Arocha. “You ask for the language you want, and they connect you within seconds to minutes, depending on the requested language.”
If the requested language or dialect is not one available on video, LAN automatically seeks an interpreter who connects via audio.
At Texas Children’s Hospital in Houston, a pilot program with the LAN system was set to go live in the emergency centers Nov. 1. Hospitalists and other providers can use this system in addition to personal and commercial telephone interpreters.
Yong S. Han, MD, a hospitalist at that institution, hopes the service enhances communication with patients and families. “Given that we have adopted family-centered rounding, this will also allow everyone to hear the conversation,” he says. “Additionally, it is pretty cumbersome and problematic switching the phone between the patient and the provider, so MARTTI should allow improvements in this arena.”
Information about the LAN system is available at www.languageaccessnetwork.com. TH
Andrea Sattinger is a medical journalist based in North Carolina
Twenty years ago, when Andrew Panos’ brother was involved in a car crash during a vacation in Puerto Vallarta, Mexico, there were no interpretation services available at the hospital where he was taken.
When the family was finally able to get him to Los Angeles, doctors concluded that if he had stayed in Mexico another eight hours he would have died from blood poisoning.
This experience—and the realization that even in his hometown of Columbus, Ohio, there was a serious need for fast, accurate healthcare interpretation services—prompted Andrew Panos to create the Language Access Network (LAN), a face-to-face live audio-video interpretation service, in 2003.
The system, My Accessible Real-Time Trusted Interpreter (MARTTI) is available in 23 hospitals. The system centralizes video interpretation into a center staffed by medically trained interpreter. In a hospital subscribing to the service, a provider can call LAN’s center in Columbus, Ohio, 24 hours a day, seven days a week. Users can choose among 150 languages, including a range of Chinese dialects and American Sign Language, and access an on-screen interpreter.
To use the system, a hospital purchases a block of minutes each month; charges are incurred when interpretations are sought.
“Some people have referred to it as the OnStar of interpreting,” says Panos, referring to the vehicle security system. “They are finding it more affordable than the cost of having on-site interpreters or calling an agency and having to pay a two-hour minimum and then having a wait time of upward of an hour.”
LAN’s system is a boon for hospitals that deal daily with Americans with Disabilities Act compliance.
“For instance, in New York they’re demanding that interpreters be provided within 10 minutes,” Panos says. “Having an American Sign Language interpreter in that short a time has really put quite a burden on their hospitals. With our system, since it is available with the push of a button, the result has been amazing.”
At Boston Medical Center (BMC), implementing MARTTI has meant synchronizing the institution’s wireless system with LAN’s system.
“It’s been a marriage of the two,” says Oscar Arocha, director of interpreter services and guest support services at BMC. Its 44 full-time interpreters were already providing in-person interpreting wherever possible. Then the hospital began telephone interpretation, and has since installed MARTTI units.
It was crucial to Arocha and BMC’s administrators that the service be available wirelessly so video units could be wheeled from place to place. Desktop units are also available from LAN.
“The user turns the video unit on and waits two or three seconds for the operator to come up on screen,” says Arocha. “You ask for the language you want, and they connect you within seconds to minutes, depending on the requested language.”
If the requested language or dialect is not one available on video, LAN automatically seeks an interpreter who connects via audio.
At Texas Children’s Hospital in Houston, a pilot program with the LAN system was set to go live in the emergency centers Nov. 1. Hospitalists and other providers can use this system in addition to personal and commercial telephone interpreters.
Yong S. Han, MD, a hospitalist at that institution, hopes the service enhances communication with patients and families. “Given that we have adopted family-centered rounding, this will also allow everyone to hear the conversation,” he says. “Additionally, it is pretty cumbersome and problematic switching the phone between the patient and the provider, so MARTTI should allow improvements in this arena.”
Information about the LAN system is available at www.languageaccessnetwork.com. TH
Andrea Sattinger is a medical journalist based in North Carolina
Twenty years ago, when Andrew Panos’ brother was involved in a car crash during a vacation in Puerto Vallarta, Mexico, there were no interpretation services available at the hospital where he was taken.
When the family was finally able to get him to Los Angeles, doctors concluded that if he had stayed in Mexico another eight hours he would have died from blood poisoning.
This experience—and the realization that even in his hometown of Columbus, Ohio, there was a serious need for fast, accurate healthcare interpretation services—prompted Andrew Panos to create the Language Access Network (LAN), a face-to-face live audio-video interpretation service, in 2003.
The system, My Accessible Real-Time Trusted Interpreter (MARTTI) is available in 23 hospitals. The system centralizes video interpretation into a center staffed by medically trained interpreter. In a hospital subscribing to the service, a provider can call LAN’s center in Columbus, Ohio, 24 hours a day, seven days a week. Users can choose among 150 languages, including a range of Chinese dialects and American Sign Language, and access an on-screen interpreter.
To use the system, a hospital purchases a block of minutes each month; charges are incurred when interpretations are sought.
“Some people have referred to it as the OnStar of interpreting,” says Panos, referring to the vehicle security system. “They are finding it more affordable than the cost of having on-site interpreters or calling an agency and having to pay a two-hour minimum and then having a wait time of upward of an hour.”
LAN’s system is a boon for hospitals that deal daily with Americans with Disabilities Act compliance.
“For instance, in New York they’re demanding that interpreters be provided within 10 minutes,” Panos says. “Having an American Sign Language interpreter in that short a time has really put quite a burden on their hospitals. With our system, since it is available with the push of a button, the result has been amazing.”
At Boston Medical Center (BMC), implementing MARTTI has meant synchronizing the institution’s wireless system with LAN’s system.
“It’s been a marriage of the two,” says Oscar Arocha, director of interpreter services and guest support services at BMC. Its 44 full-time interpreters were already providing in-person interpreting wherever possible. Then the hospital began telephone interpretation, and has since installed MARTTI units.
It was crucial to Arocha and BMC’s administrators that the service be available wirelessly so video units could be wheeled from place to place. Desktop units are also available from LAN.
“The user turns the video unit on and waits two or three seconds for the operator to come up on screen,” says Arocha. “You ask for the language you want, and they connect you within seconds to minutes, depending on the requested language.”
If the requested language or dialect is not one available on video, LAN automatically seeks an interpreter who connects via audio.
At Texas Children’s Hospital in Houston, a pilot program with the LAN system was set to go live in the emergency centers Nov. 1. Hospitalists and other providers can use this system in addition to personal and commercial telephone interpreters.
Yong S. Han, MD, a hospitalist at that institution, hopes the service enhances communication with patients and families. “Given that we have adopted family-centered rounding, this will also allow everyone to hear the conversation,” he says. “Additionally, it is pretty cumbersome and problematic switching the phone between the patient and the provider, so MARTTI should allow improvements in this arena.”
Information about the LAN system is available at www.languageaccessnetwork.com. TH
Andrea Sattinger is a medical journalist based in North Carolina
IMPORTED CARE
In this first of a two-part series, we examine the implications of international medical graduates (IMGs) in hospital medicine groups, and explore how hospitalist group leaders can improve communications and integrate them into their medicine teams. Part 2 will feature stories from hospitalist IMGs as they establish themselves as professionals in their communities.
International medical graduates (IMGs) comprise 25% of the total U.S. physician workforce.1 Despite post-9/11 barriers to immigration, the number of IMGs entering internal medical residencies has risen in recent years.
In 2006, more than 6,500 physicians who graduated medical school in foreign countries entered accredited residency programs, according to the Association of American Medical Colleges. U.S.-born residents who have attended medical school in another country account for approximately 25% of the total IMGs in training.
Further, the proportion of foreign-educated residents who will go into primary care is higher than for U.S. medical graduates. In 2006, 50% of the physicians training in internal medicine residency programs were IMGs.
What do these trends mean for hospital medicine? In light of projected physician shortages IMGs will continue to be a vital part of the physician workforce.2 Because internal medicine is a primary feeder of hospital medicine, it’s likely many hospital medicine programs will also continue to see an increase in hospitalists who are IMGs.
Hoops, Hurdles, and Visas

The J-1 visa was set up as an educational exchange program and carries with it a requirement that the graduate return to his or her native country upon completion of residency. However, a waiver of the requirement to return to their country of origin can be obtained if the physicians agree to begin practice in a Health Professional Shortage Area.
These service areas are determined using a scoring system based on four variables: the ratio of primary medical care physicians per 1,000 population, infant mortality rates, percentage of the population with incomes below the federal poverty level, and percentage of the population over 65. The vast majority of J-1 waivers are administered through “Conrad 30” programs administered by individual states and the District of Columbia.
In recent years, AAMC’s Center for Workforce Studies has observed a shift to the H1-B, or temporary worker visa, allowing hospitals and group practices to hire IMGs in areas where there are physician shortages. This visa is employer-specific, and some hospitalist programs have become involved in helping their applicants secure this visa.
Visa issues present a range of financial, legal and personal hurdles for the IMG. In addition to obtaining legal entry into the country, IMGs applying to U.S. residency programs must obtain ECGMG certification, a multistep process that includes:
- Graduating from a medical school listed in the World Directory of Medical Schools;
- Obtaining a license to practice medicine within their own country;
- Passing the medical science examination (Step 1 and 2 of the United States Medical Licensing Examination);
- Passing the ECFMG English test or Test of English as a Foreign Language; and
- Passing the Clinical Skills Assessment component of the USMLE.
An IMG can apply for lawful permanent resident status based on a job offer, provided that he or she has passed parts 1 and 2 of the National Board of Medical Examiners examination, and has fulfilled the other ECFMG certification requirements.
For more information, visit the Web sites of the Accreditation Council for Graduate Medical Education (www.acgme.org) and the Educational Commission for Foreign Medical Graduates (www.ecfmg.org).—GH
Image - © POWERED BY LIGHT/ALAN SPENCER / ALAMY
What the Trends Show
“International medical school graduates have been and continue to be a major source of physicians in the U.S.,” says Edward Salsberg, director, Center for Workforce Studies at the Association of American Medical Colleges.
According to a survey this year in Health Affairs of IMG trends since 1981, most IMGs working in the United States come from India, the Philippines, Mexico, Pakistan, China, and the Republic of Korea. When starting full-time employment, most IMGs tend to gravitate to the East Coast, the Midwest (particularly Illinois, Ohio, and Michigan), and California.
Although the overall percentage of IMGs in the United States has remained about the same, more U.S. citizens graduate from medical schools outside this country, according to Salsberg. Noncitizen IMGs are gravitating toward the H1-B visa for foreign-born professionals for a duration of not more than six years instead of J-1, or exchange visitor visas.
A slightly higher percent of IMGs go into primary care. “International medical graduates have tended to go into the specialties that U.S. graduates were less interested in entering,” Salsberg notes. “They fill gaps because many are willing to go into some specialties in order to get into the U.S.”
Location, Location, Location
Entering residency, obtaining fellowships, and embarking on the practice of medicine all pose challenges for the foreign-born IMG. Throughout their residencies and into practice, IMGs can face biased perceptions from peers, attending physicians, and patients—especially if English has not been their primary language.
Rachel George, MD, regional medical director for Cogent Healthcare, is an international medical graduate, who received her medical degree from JJM Medical College in Kamataka, India. She observes that the challenges for IMGs and hospital medicine groups often depend on the predominant cultural mix of the surrounding community, as well as the hospital community culture.
For example, one program Dr. George oversees is situated within a culturally diverse community near Los Angeles. “Almost any international medical grad can go there, do very well, and be very comfortable, just because the rest of the community is very comfortable with international grads,” she says. However, the first employment for many IMGs here on J-1 visa waivers may be in medically underserved areas, which tend to be rural areas.
“When you go to those places, I think communication becomes much more of a challenge because people in the local area may not be used to interacting with people of different cultures with different accents,” Dr. George says. In some of those cases, Cogent has sent physicians to English classes to help improve communication skills.
Perception versus Reality
Dr. George notes that international medical graduates often face the perception that they are not as good as American graduates.
Much of this perception may be related to an IMG’s lack of English fluency, she says. But those familiar with the certification process for IMGs know they face multiple difficulties to attain the status of a practicing physician in this country.
“It might actually be harder for an international medical grad to be able to practice in this country,” notes Dr. George. “Your scores almost have to be twice as good as the scores of the American grad standing next to you to get into residency. Fellowships are also extremely difficult to obtain. Foreign medical grads have to jump through a lot more hoops to get into the system. And because of that, we actually probably have the cream of the crop here.”
For Salsberg, credentials count. “A graduate of an LCME [Liaison Committee for Medical Education]-accredited medical school provides a high degree of assurance to a residency program director that the physician has received a comprehensive, solid medical education,” Salsberg says. “This is not to suggest that foreign IMGs are not well prepared: Many of the IMGs that we’re getting now are really among the best and the brightest in the world.”

—Rachel George, MD, regional medical director for Cogent Healthcare
Issues that Surface
Program directors of ACGME-accredited residency programs rely on certification by the Educational Commission for Foreign Medical Graduates (ECGMG) to ensure that their prospective residents have met standards of eligibility.
ECGMG certification is also a prerequisite required by most states for licensure to practice medicine. Vijay Rajput, MD, associate professor of medicine and program director of Internal Medicine Residency at UMDNJ-Robert Wood Johnson Medical School in Camden, N.J., and senior hospitalist with Cooper Health System, acknowledges that depending upon their country of origin, IMGs may have difficulties becoming acculturated when it comes time to start practicing medicine. During his time as a residency program director, Dr. Rajput has encountered residents who have problems with hierarchical issues. “A resident may come from a part of the world where they do not like to take orders from women,” he says. “It will be difficult for them to work with peers who are women.”
Hospitalist directors need to exercise good judgment when hiring new members of their team, and ascertain the prospective candidate’s bedside skills with language, communication, and cultural competency, says Dr. Rajput. He believes that evaluation of residents’ interpersonal communications skills varies from program to program.
The “hard skills” pertaining to the resident’s breadth of medical knowledge and technological expertise are easily evaluated by in-service and board examinations, as well as procedures tests. However, the “soft skills” of communication, professionalism, and interpersonal skills are not as easily evaluated.
He suggests hospital program medical directors speak with program directors to glean important information about the candidates’ interpersonal skills, including areas where they might need improvement.
“I think the hospitalist director will have to recognize their own community and the cultural, language, and communication issues in their own hospital’s patient population and then acclimatize their younger hospitalists, providing specific training as part of CME,” Dr. Rajput advises. “The hospitalist director has to keep his or her eyes open and see whether their IMG might need extra training—whether it’s in cultural competencies or ethical principles—because even in our country there are different cultural issues in each community.”
Dr. Rajput, in collaboration with Gerry Whalen, MD, a former vice president at ECFMG, has conducted a pilot acculturation project for the past two years. It entails a one-day program for 40 to 50 IMG participants to acquaint them with challenges they will likely face. This “snapshot” provides an overview of Western medicine’s ethics, bedside skills, insurance issues, and peer-relationship issues.
Pave the Way
Experts suggest various ways leaders of hospital medicine groups can address perception and communication challenges when they surface.
IMGs can be encouraged, for instance, to open their dialogue when meeting patients for the first time by telling them they are welcome to ask questions if there are words or terms they do not understand. In addition, says Dr. George, IMGs can slow the pace of their conversation to be better understood.
Perhaps more important is how the hospital and the practice group introduce new members of the team to their communities. Dr. George advocates a hospital-wide announcement when a new physician joins the hospital medicine team. It’s important that the hospital clearly communicates to the hospital staff and the community at large that the IMG is a “well-trained physician, is highly regarded and respected, has good credentials, was chosen very carefully, and will be a great addition to the team.”
Communications consultant Douglas Leonard, PhD, advised Richard H. Bailey, MD, medical director of Inpatient Care and Hospitalist Services at Saint Clare’s Hospital in Wausau, Wis., to create a brochure to introduce new members of the hospitalist team. Dr. Bailey leads a team made up entirely of hospitalists who are foreign-born IMGs. He had received complaints about his hospitalists’ English skills from other specialists at the hospital and hired Dr. Leonard to perform a needs assessment of his team and other staff members with whom they interface.
Dr. Leonard found that nursing staff, because they liked the hospitalists and wanted to help them, had begun to act as interpreters between physicians and patients.
“Because these hospitalists had such good attitudes, the staff had learned to understand their accents and had really made an effort to work with these doctors effectively,” Dr. Leonard reports. Part of that effort was that nurses would often step in to interpret for the hospitalists when patients could not understand their accents.
Dr. Leonard recommended that the hospitalists become better communicators with patients—even if that means softening their accents—and that they avoid reliance on nurses interpreting with their patients. The latter, says Dr. Leonard, “makes the hospitalists seem like second-class citizens in the world of doctoring.” Although the nurses were happy to provide the service, he says “the hospitalists have got to establish their own ability to communicate with their patients.”
In a case like this, the medical director can work with hospital administration to provide language training. Dr. Bailey has been exploring the possibility of working with local outside resources, including a local technical college, for this service.
The technical college is willing to schedule classes at night or when the hospitalists overlap on changing shifts. In addition, “Classes might alternate with on-site, one-to-one coaching sessions in speaking skills,” says Dr. Leonard.
Two-Way Street
IMGs will continue to be a valuable resource and an increasing presence in hospitalist programs. The challenge for hospital medicine group leaders is to ensure that their talents are nurtured and respected.
Dr. Bailey sees his job as that of champion and advocate for his team. For one member of his team, he solicited involvement from his congressman to help resolve complications with visa and immigration issues.
He has also seen tensions erupt when his hospitalists interact with other physicians or patients who have misperceptions about their medical skills. “I’d put my physicians up against anybody—they just don’t speak as well,” he says.
There are times when Dr. Bailey becomes concerned about the welfare of his team. “My job as medical director is to create an environment in which they can be successful—and that’s a two-way street,” he says. “That means I have to help them to be able to communicate, but it also means that I have to back them up when their professional competency is being questioned by preconceived notions about their language and their accents.”
Dr. Rajput underscores this message. “Acculturation is a two-way street,” he agrees. “As international doctors get acculturated, we as a society also need to adjust and help these well-trained physicians to understand us as well. In the interests of providing the best possible patient care, education and training will be needed for both sets of stakeholders [the IMG physicians and their employers].” TH
Gretchen Henkel is a frequent contributor to The Hospitalist.
References
- Hart LG, Skillman SM, Fordyce M, et al. International medical graduate physicians in the United States: changes since 1981. Health Aff. 2007 July/August;26(4):1159-1169.
- Association of American Medical Colleges. Help wanted: more U.S. doctors. Available online at www.aamc.org/workforce/helpwanted.pdf. Last accessed Sept. 11, 2007.
In this first of a two-part series, we examine the implications of international medical graduates (IMGs) in hospital medicine groups, and explore how hospitalist group leaders can improve communications and integrate them into their medicine teams. Part 2 will feature stories from hospitalist IMGs as they establish themselves as professionals in their communities.
International medical graduates (IMGs) comprise 25% of the total U.S. physician workforce.1 Despite post-9/11 barriers to immigration, the number of IMGs entering internal medical residencies has risen in recent years.
In 2006, more than 6,500 physicians who graduated medical school in foreign countries entered accredited residency programs, according to the Association of American Medical Colleges. U.S.-born residents who have attended medical school in another country account for approximately 25% of the total IMGs in training.
Further, the proportion of foreign-educated residents who will go into primary care is higher than for U.S. medical graduates. In 2006, 50% of the physicians training in internal medicine residency programs were IMGs.
What do these trends mean for hospital medicine? In light of projected physician shortages IMGs will continue to be a vital part of the physician workforce.2 Because internal medicine is a primary feeder of hospital medicine, it’s likely many hospital medicine programs will also continue to see an increase in hospitalists who are IMGs.
Hoops, Hurdles, and Visas
The J-1 visa was set up as an educational exchange program and carries with it a requirement that the graduate return to his or her native country upon completion of residency. However, a waiver of the requirement to return to their country of origin can be obtained if the physicians agree to begin practice in a Health Professional Shortage Area.
These service areas are determined using a scoring system based on four variables: the ratio of primary medical care physicians per 1,000 population, infant mortality rates, percentage of the population with incomes below the federal poverty level, and percentage of the population over 65. The vast majority of J-1 waivers are administered through “Conrad 30” programs administered by individual states and the District of Columbia.
In recent years, AAMC’s Center for Workforce Studies has observed a shift to the H1-B, or temporary worker visa, allowing hospitals and group practices to hire IMGs in areas where there are physician shortages. This visa is employer-specific, and some hospitalist programs have become involved in helping their applicants secure this visa.
Visa issues present a range of financial, legal and personal hurdles for the IMG. In addition to obtaining legal entry into the country, IMGs applying to U.S. residency programs must obtain ECGMG certification, a multistep process that includes:
- Graduating from a medical school listed in the World Directory of Medical Schools;
- Obtaining a license to practice medicine within their own country;
- Passing the medical science examination (Step 1 and 2 of the United States Medical Licensing Examination);
- Passing the ECFMG English test or Test of English as a Foreign Language; and
- Passing the Clinical Skills Assessment component of the USMLE.
An IMG can apply for lawful permanent resident status based on a job offer, provided that he or she has passed parts 1 and 2 of the National Board of Medical Examiners examination, and has fulfilled the other ECFMG certification requirements.
For more information, visit the Web sites of the Accreditation Council for Graduate Medical Education (www.acgme.org) and the Educational Commission for Foreign Medical Graduates (www.ecfmg.org).—GH
Image - © POWERED BY LIGHT/ALAN SPENCER / ALAMY
What the Trends Show
“International medical school graduates have been and continue to be a major source of physicians in the U.S.,” says Edward Salsberg, director, Center for Workforce Studies at the Association of American Medical Colleges.
According to a survey this year in Health Affairs of IMG trends since 1981, most IMGs working in the United States come from India, the Philippines, Mexico, Pakistan, China, and the Republic of Korea. When starting full-time employment, most IMGs tend to gravitate to the East Coast, the Midwest (particularly Illinois, Ohio, and Michigan), and California.
Although the overall percentage of IMGs in the United States has remained about the same, more U.S. citizens graduate from medical schools outside this country, according to Salsberg. Noncitizen IMGs are gravitating toward the H1-B visa for foreign-born professionals for a duration of not more than six years instead of J-1, or exchange visitor visas.
A slightly higher percent of IMGs go into primary care. “International medical graduates have tended to go into the specialties that U.S. graduates were less interested in entering,” Salsberg notes. “They fill gaps because many are willing to go into some specialties in order to get into the U.S.”
Location, Location, Location
Entering residency, obtaining fellowships, and embarking on the practice of medicine all pose challenges for the foreign-born IMG. Throughout their residencies and into practice, IMGs can face biased perceptions from peers, attending physicians, and patients—especially if English has not been their primary language.
Rachel George, MD, regional medical director for Cogent Healthcare, is an international medical graduate, who received her medical degree from JJM Medical College in Kamataka, India. She observes that the challenges for IMGs and hospital medicine groups often depend on the predominant cultural mix of the surrounding community, as well as the hospital community culture.
For example, one program Dr. George oversees is situated within a culturally diverse community near Los Angeles. “Almost any international medical grad can go there, do very well, and be very comfortable, just because the rest of the community is very comfortable with international grads,” she says. However, the first employment for many IMGs here on J-1 visa waivers may be in medically underserved areas, which tend to be rural areas.
“When you go to those places, I think communication becomes much more of a challenge because people in the local area may not be used to interacting with people of different cultures with different accents,” Dr. George says. In some of those cases, Cogent has sent physicians to English classes to help improve communication skills.
Perception versus Reality
Dr. George notes that international medical graduates often face the perception that they are not as good as American graduates.
Much of this perception may be related to an IMG’s lack of English fluency, she says. But those familiar with the certification process for IMGs know they face multiple difficulties to attain the status of a practicing physician in this country.
“It might actually be harder for an international medical grad to be able to practice in this country,” notes Dr. George. “Your scores almost have to be twice as good as the scores of the American grad standing next to you to get into residency. Fellowships are also extremely difficult to obtain. Foreign medical grads have to jump through a lot more hoops to get into the system. And because of that, we actually probably have the cream of the crop here.”
For Salsberg, credentials count. “A graduate of an LCME [Liaison Committee for Medical Education]-accredited medical school provides a high degree of assurance to a residency program director that the physician has received a comprehensive, solid medical education,” Salsberg says. “This is not to suggest that foreign IMGs are not well prepared: Many of the IMGs that we’re getting now are really among the best and the brightest in the world.”
—Rachel George, MD, regional medical director for Cogent Healthcare
Issues that Surface
Program directors of ACGME-accredited residency programs rely on certification by the Educational Commission for Foreign Medical Graduates (ECGMG) to ensure that their prospective residents have met standards of eligibility.
ECGMG certification is also a prerequisite required by most states for licensure to practice medicine. Vijay Rajput, MD, associate professor of medicine and program director of Internal Medicine Residency at UMDNJ-Robert Wood Johnson Medical School in Camden, N.J., and senior hospitalist with Cooper Health System, acknowledges that depending upon their country of origin, IMGs may have difficulties becoming acculturated when it comes time to start practicing medicine. During his time as a residency program director, Dr. Rajput has encountered residents who have problems with hierarchical issues. “A resident may come from a part of the world where they do not like to take orders from women,” he says. “It will be difficult for them to work with peers who are women.”
Hospitalist directors need to exercise good judgment when hiring new members of their team, and ascertain the prospective candidate’s bedside skills with language, communication, and cultural competency, says Dr. Rajput. He believes that evaluation of residents’ interpersonal communications skills varies from program to program.
The “hard skills” pertaining to the resident’s breadth of medical knowledge and technological expertise are easily evaluated by in-service and board examinations, as well as procedures tests. However, the “soft skills” of communication, professionalism, and interpersonal skills are not as easily evaluated.
He suggests hospital program medical directors speak with program directors to glean important information about the candidates’ interpersonal skills, including areas where they might need improvement.
“I think the hospitalist director will have to recognize their own community and the cultural, language, and communication issues in their own hospital’s patient population and then acclimatize their younger hospitalists, providing specific training as part of CME,” Dr. Rajput advises. “The hospitalist director has to keep his or her eyes open and see whether their IMG might need extra training—whether it’s in cultural competencies or ethical principles—because even in our country there are different cultural issues in each community.”
Dr. Rajput, in collaboration with Gerry Whalen, MD, a former vice president at ECFMG, has conducted a pilot acculturation project for the past two years. It entails a one-day program for 40 to 50 IMG participants to acquaint them with challenges they will likely face. This “snapshot” provides an overview of Western medicine’s ethics, bedside skills, insurance issues, and peer-relationship issues.
Pave the Way
Experts suggest various ways leaders of hospital medicine groups can address perception and communication challenges when they surface.
IMGs can be encouraged, for instance, to open their dialogue when meeting patients for the first time by telling them they are welcome to ask questions if there are words or terms they do not understand. In addition, says Dr. George, IMGs can slow the pace of their conversation to be better understood.
Perhaps more important is how the hospital and the practice group introduce new members of the team to their communities. Dr. George advocates a hospital-wide announcement when a new physician joins the hospital medicine team. It’s important that the hospital clearly communicates to the hospital staff and the community at large that the IMG is a “well-trained physician, is highly regarded and respected, has good credentials, was chosen very carefully, and will be a great addition to the team.”
Communications consultant Douglas Leonard, PhD, advised Richard H. Bailey, MD, medical director of Inpatient Care and Hospitalist Services at Saint Clare’s Hospital in Wausau, Wis., to create a brochure to introduce new members of the hospitalist team. Dr. Bailey leads a team made up entirely of hospitalists who are foreign-born IMGs. He had received complaints about his hospitalists’ English skills from other specialists at the hospital and hired Dr. Leonard to perform a needs assessment of his team and other staff members with whom they interface.
Dr. Leonard found that nursing staff, because they liked the hospitalists and wanted to help them, had begun to act as interpreters between physicians and patients.
“Because these hospitalists had such good attitudes, the staff had learned to understand their accents and had really made an effort to work with these doctors effectively,” Dr. Leonard reports. Part of that effort was that nurses would often step in to interpret for the hospitalists when patients could not understand their accents.
Dr. Leonard recommended that the hospitalists become better communicators with patients—even if that means softening their accents—and that they avoid reliance on nurses interpreting with their patients. The latter, says Dr. Leonard, “makes the hospitalists seem like second-class citizens in the world of doctoring.” Although the nurses were happy to provide the service, he says “the hospitalists have got to establish their own ability to communicate with their patients.”
In a case like this, the medical director can work with hospital administration to provide language training. Dr. Bailey has been exploring the possibility of working with local outside resources, including a local technical college, for this service.
The technical college is willing to schedule classes at night or when the hospitalists overlap on changing shifts. In addition, “Classes might alternate with on-site, one-to-one coaching sessions in speaking skills,” says Dr. Leonard.
Two-Way Street
IMGs will continue to be a valuable resource and an increasing presence in hospitalist programs. The challenge for hospital medicine group leaders is to ensure that their talents are nurtured and respected.
Dr. Bailey sees his job as that of champion and advocate for his team. For one member of his team, he solicited involvement from his congressman to help resolve complications with visa and immigration issues.
He has also seen tensions erupt when his hospitalists interact with other physicians or patients who have misperceptions about their medical skills. “I’d put my physicians up against anybody—they just don’t speak as well,” he says.
There are times when Dr. Bailey becomes concerned about the welfare of his team. “My job as medical director is to create an environment in which they can be successful—and that’s a two-way street,” he says. “That means I have to help them to be able to communicate, but it also means that I have to back them up when their professional competency is being questioned by preconceived notions about their language and their accents.”
Dr. Rajput underscores this message. “Acculturation is a two-way street,” he agrees. “As international doctors get acculturated, we as a society also need to adjust and help these well-trained physicians to understand us as well. In the interests of providing the best possible patient care, education and training will be needed for both sets of stakeholders [the IMG physicians and their employers].” TH
Gretchen Henkel is a frequent contributor to The Hospitalist.
References
- Hart LG, Skillman SM, Fordyce M, et al. International medical graduate physicians in the United States: changes since 1981. Health Aff. 2007 July/August;26(4):1159-1169.
- Association of American Medical Colleges. Help wanted: more U.S. doctors. Available online at www.aamc.org/workforce/helpwanted.pdf. Last accessed Sept. 11, 2007.
In this first of a two-part series, we examine the implications of international medical graduates (IMGs) in hospital medicine groups, and explore how hospitalist group leaders can improve communications and integrate them into their medicine teams. Part 2 will feature stories from hospitalist IMGs as they establish themselves as professionals in their communities.
International medical graduates (IMGs) comprise 25% of the total U.S. physician workforce.1 Despite post-9/11 barriers to immigration, the number of IMGs entering internal medical residencies has risen in recent years.
In 2006, more than 6,500 physicians who graduated medical school in foreign countries entered accredited residency programs, according to the Association of American Medical Colleges. U.S.-born residents who have attended medical school in another country account for approximately 25% of the total IMGs in training.
Further, the proportion of foreign-educated residents who will go into primary care is higher than for U.S. medical graduates. In 2006, 50% of the physicians training in internal medicine residency programs were IMGs.
What do these trends mean for hospital medicine? In light of projected physician shortages IMGs will continue to be a vital part of the physician workforce.2 Because internal medicine is a primary feeder of hospital medicine, it’s likely many hospital medicine programs will also continue to see an increase in hospitalists who are IMGs.
Hoops, Hurdles, and Visas
The J-1 visa was set up as an educational exchange program and carries with it a requirement that the graduate return to his or her native country upon completion of residency. However, a waiver of the requirement to return to their country of origin can be obtained if the physicians agree to begin practice in a Health Professional Shortage Area.
These service areas are determined using a scoring system based on four variables: the ratio of primary medical care physicians per 1,000 population, infant mortality rates, percentage of the population with incomes below the federal poverty level, and percentage of the population over 65. The vast majority of J-1 waivers are administered through “Conrad 30” programs administered by individual states and the District of Columbia.
In recent years, AAMC’s Center for Workforce Studies has observed a shift to the H1-B, or temporary worker visa, allowing hospitals and group practices to hire IMGs in areas where there are physician shortages. This visa is employer-specific, and some hospitalist programs have become involved in helping their applicants secure this visa.
Visa issues present a range of financial, legal and personal hurdles for the IMG. In addition to obtaining legal entry into the country, IMGs applying to U.S. residency programs must obtain ECGMG certification, a multistep process that includes:
- Graduating from a medical school listed in the World Directory of Medical Schools;
- Obtaining a license to practice medicine within their own country;
- Passing the medical science examination (Step 1 and 2 of the United States Medical Licensing Examination);
- Passing the ECFMG English test or Test of English as a Foreign Language; and
- Passing the Clinical Skills Assessment component of the USMLE.
An IMG can apply for lawful permanent resident status based on a job offer, provided that he or she has passed parts 1 and 2 of the National Board of Medical Examiners examination, and has fulfilled the other ECFMG certification requirements.
For more information, visit the Web sites of the Accreditation Council for Graduate Medical Education (www.acgme.org) and the Educational Commission for Foreign Medical Graduates (www.ecfmg.org).—GH
Image - © POWERED BY LIGHT/ALAN SPENCER / ALAMY
What the Trends Show
“International medical school graduates have been and continue to be a major source of physicians in the U.S.,” says Edward Salsberg, director, Center for Workforce Studies at the Association of American Medical Colleges.
According to a survey this year in Health Affairs of IMG trends since 1981, most IMGs working in the United States come from India, the Philippines, Mexico, Pakistan, China, and the Republic of Korea. When starting full-time employment, most IMGs tend to gravitate to the East Coast, the Midwest (particularly Illinois, Ohio, and Michigan), and California.
Although the overall percentage of IMGs in the United States has remained about the same, more U.S. citizens graduate from medical schools outside this country, according to Salsberg. Noncitizen IMGs are gravitating toward the H1-B visa for foreign-born professionals for a duration of not more than six years instead of J-1, or exchange visitor visas.
A slightly higher percent of IMGs go into primary care. “International medical graduates have tended to go into the specialties that U.S. graduates were less interested in entering,” Salsberg notes. “They fill gaps because many are willing to go into some specialties in order to get into the U.S.”
Location, Location, Location
Entering residency, obtaining fellowships, and embarking on the practice of medicine all pose challenges for the foreign-born IMG. Throughout their residencies and into practice, IMGs can face biased perceptions from peers, attending physicians, and patients—especially if English has not been their primary language.
Rachel George, MD, regional medical director for Cogent Healthcare, is an international medical graduate, who received her medical degree from JJM Medical College in Kamataka, India. She observes that the challenges for IMGs and hospital medicine groups often depend on the predominant cultural mix of the surrounding community, as well as the hospital community culture.
For example, one program Dr. George oversees is situated within a culturally diverse community near Los Angeles. “Almost any international medical grad can go there, do very well, and be very comfortable, just because the rest of the community is very comfortable with international grads,” she says. However, the first employment for many IMGs here on J-1 visa waivers may be in medically underserved areas, which tend to be rural areas.
“When you go to those places, I think communication becomes much more of a challenge because people in the local area may not be used to interacting with people of different cultures with different accents,” Dr. George says. In some of those cases, Cogent has sent physicians to English classes to help improve communication skills.
Perception versus Reality
Dr. George notes that international medical graduates often face the perception that they are not as good as American graduates.
Much of this perception may be related to an IMG’s lack of English fluency, she says. But those familiar with the certification process for IMGs know they face multiple difficulties to attain the status of a practicing physician in this country.
“It might actually be harder for an international medical grad to be able to practice in this country,” notes Dr. George. “Your scores almost have to be twice as good as the scores of the American grad standing next to you to get into residency. Fellowships are also extremely difficult to obtain. Foreign medical grads have to jump through a lot more hoops to get into the system. And because of that, we actually probably have the cream of the crop here.”
For Salsberg, credentials count. “A graduate of an LCME [Liaison Committee for Medical Education]-accredited medical school provides a high degree of assurance to a residency program director that the physician has received a comprehensive, solid medical education,” Salsberg says. “This is not to suggest that foreign IMGs are not well prepared: Many of the IMGs that we’re getting now are really among the best and the brightest in the world.”
—Rachel George, MD, regional medical director for Cogent Healthcare
Issues that Surface
Program directors of ACGME-accredited residency programs rely on certification by the Educational Commission for Foreign Medical Graduates (ECGMG) to ensure that their prospective residents have met standards of eligibility.
ECGMG certification is also a prerequisite required by most states for licensure to practice medicine. Vijay Rajput, MD, associate professor of medicine and program director of Internal Medicine Residency at UMDNJ-Robert Wood Johnson Medical School in Camden, N.J., and senior hospitalist with Cooper Health System, acknowledges that depending upon their country of origin, IMGs may have difficulties becoming acculturated when it comes time to start practicing medicine. During his time as a residency program director, Dr. Rajput has encountered residents who have problems with hierarchical issues. “A resident may come from a part of the world where they do not like to take orders from women,” he says. “It will be difficult for them to work with peers who are women.”
Hospitalist directors need to exercise good judgment when hiring new members of their team, and ascertain the prospective candidate’s bedside skills with language, communication, and cultural competency, says Dr. Rajput. He believes that evaluation of residents’ interpersonal communications skills varies from program to program.
The “hard skills” pertaining to the resident’s breadth of medical knowledge and technological expertise are easily evaluated by in-service and board examinations, as well as procedures tests. However, the “soft skills” of communication, professionalism, and interpersonal skills are not as easily evaluated.
He suggests hospital program medical directors speak with program directors to glean important information about the candidates’ interpersonal skills, including areas where they might need improvement.
“I think the hospitalist director will have to recognize their own community and the cultural, language, and communication issues in their own hospital’s patient population and then acclimatize their younger hospitalists, providing specific training as part of CME,” Dr. Rajput advises. “The hospitalist director has to keep his or her eyes open and see whether their IMG might need extra training—whether it’s in cultural competencies or ethical principles—because even in our country there are different cultural issues in each community.”
Dr. Rajput, in collaboration with Gerry Whalen, MD, a former vice president at ECFMG, has conducted a pilot acculturation project for the past two years. It entails a one-day program for 40 to 50 IMG participants to acquaint them with challenges they will likely face. This “snapshot” provides an overview of Western medicine’s ethics, bedside skills, insurance issues, and peer-relationship issues.
Pave the Way
Experts suggest various ways leaders of hospital medicine groups can address perception and communication challenges when they surface.
IMGs can be encouraged, for instance, to open their dialogue when meeting patients for the first time by telling them they are welcome to ask questions if there are words or terms they do not understand. In addition, says Dr. George, IMGs can slow the pace of their conversation to be better understood.
Perhaps more important is how the hospital and the practice group introduce new members of the team to their communities. Dr. George advocates a hospital-wide announcement when a new physician joins the hospital medicine team. It’s important that the hospital clearly communicates to the hospital staff and the community at large that the IMG is a “well-trained physician, is highly regarded and respected, has good credentials, was chosen very carefully, and will be a great addition to the team.”
Communications consultant Douglas Leonard, PhD, advised Richard H. Bailey, MD, medical director of Inpatient Care and Hospitalist Services at Saint Clare’s Hospital in Wausau, Wis., to create a brochure to introduce new members of the hospitalist team. Dr. Bailey leads a team made up entirely of hospitalists who are foreign-born IMGs. He had received complaints about his hospitalists’ English skills from other specialists at the hospital and hired Dr. Leonard to perform a needs assessment of his team and other staff members with whom they interface.
Dr. Leonard found that nursing staff, because they liked the hospitalists and wanted to help them, had begun to act as interpreters between physicians and patients.
“Because these hospitalists had such good attitudes, the staff had learned to understand their accents and had really made an effort to work with these doctors effectively,” Dr. Leonard reports. Part of that effort was that nurses would often step in to interpret for the hospitalists when patients could not understand their accents.
Dr. Leonard recommended that the hospitalists become better communicators with patients—even if that means softening their accents—and that they avoid reliance on nurses interpreting with their patients. The latter, says Dr. Leonard, “makes the hospitalists seem like second-class citizens in the world of doctoring.” Although the nurses were happy to provide the service, he says “the hospitalists have got to establish their own ability to communicate with their patients.”
In a case like this, the medical director can work with hospital administration to provide language training. Dr. Bailey has been exploring the possibility of working with local outside resources, including a local technical college, for this service.
The technical college is willing to schedule classes at night or when the hospitalists overlap on changing shifts. In addition, “Classes might alternate with on-site, one-to-one coaching sessions in speaking skills,” says Dr. Leonard.
Two-Way Street
IMGs will continue to be a valuable resource and an increasing presence in hospitalist programs. The challenge for hospital medicine group leaders is to ensure that their talents are nurtured and respected.
Dr. Bailey sees his job as that of champion and advocate for his team. For one member of his team, he solicited involvement from his congressman to help resolve complications with visa and immigration issues.
He has also seen tensions erupt when his hospitalists interact with other physicians or patients who have misperceptions about their medical skills. “I’d put my physicians up against anybody—they just don’t speak as well,” he says.
There are times when Dr. Bailey becomes concerned about the welfare of his team. “My job as medical director is to create an environment in which they can be successful—and that’s a two-way street,” he says. “That means I have to help them to be able to communicate, but it also means that I have to back them up when their professional competency is being questioned by preconceived notions about their language and their accents.”
Dr. Rajput underscores this message. “Acculturation is a two-way street,” he agrees. “As international doctors get acculturated, we as a society also need to adjust and help these well-trained physicians to understand us as well. In the interests of providing the best possible patient care, education and training will be needed for both sets of stakeholders [the IMG physicians and their employers].” TH
Gretchen Henkel is a frequent contributor to The Hospitalist.
References
- Hart LG, Skillman SM, Fordyce M, et al. International medical graduate physicians in the United States: changes since 1981. Health Aff. 2007 July/August;26(4):1159-1169.
- Association of American Medical Colleges. Help wanted: more U.S. doctors. Available online at www.aamc.org/workforce/helpwanted.pdf. Last accessed Sept. 11, 2007.
ADVICE ON THE RUN
Everyone has been there. You’re making rounds in the hospital and another physician taps you on the shoulder and says, “Can I ask you something?” He then gives the details and diagnosis of a patient’s condition and asks, “What would you suggest?”
Or maybe you stop the cardiologist in the hall to run your planned treatment of a particularly perplexing case by him.
These encounters—called curbside consultations—happen everywhere: hallways, cocktail parties, weddings, parking lots, and, increasingly, on the Internet.
As hospitalists increase their presence, they expose themselves to more curbside consultations—and the risks they entail. The practice is fraught with minefields that can turn the best of intentions into a potential medical and legal nightmare.
The term curbside consults implies opportunity—and hospitalists are most available to other hospitalists as they work in the hospital. In return, hospitalists have a greater opportunity to ask questions of other specialists without even picking up a telephone. A combination of geography and opportunity puts hospitalists at increasingly greater risk.
“We’re so accessible to other doctors in the hospital,” says Janet Nagamine, MD, chair of SHM’s Hospital Quality and Patient Safety committee and a hospitalist at Kaiser Permanente Santa Clara Medical Center in California. “I think we get more requests for informal consultations because we are there. It’s so easy for another physician to tap you on the shoulder and ask what you think about a patient’s condition or treatment. I am more frequently the giver of information than the receiver because it is so easy for a physician to tap me on the shoulder and ask my opinion.”
Proximity also presents an increased opportunity for hospitalists to seek a curbside consult from another physician in the hall. “I think hospitalists are more likely to ask for help from specialists they see in the hospital because hospitalists are generalists and can see a wide variety of conditions in the hospital,” says Clifford Zwillich, MD, professor of medicine at the University of Colorado and a hospitalist at the Denver Veterans Affairs Medical Center.
—Janet Nagamine, MD, chair of SHM’s Hospital Quality and Patient Safety committee and hospitalist, Kaiser Permanente Santa Clara Medical Center (Calif.)
Widespread Practice
In an April 2006 study in the Journal of the Medical Library Association, hospitalists reported that they seek a curbside consultation for a variety of reasons. These include:
- Confirm what they already know;
- Get quick answers to a question;
- Continue their medical education;
- Determine if a formal consultation is called for;
- Negotiate an appropriate course of treatment for a particular patient;
- Spread the emotional risk during a difficult case;
- Create or sustain camaraderie with physician colleges;
- Find like thinkers among their physician colleagues;
- Monitor their own knowledge; and
- Obtain help to get out of a difficult situation.
Hospitalists who provide curbside consultations reported doing so to provide good patient care, fulfill professional obligations, serve doctors, and encourage formal referrals.
Another study reported that 70% of primary care hospitalists and 68% of subspecialists surveyed participated in at least one informal consult in the previous week.
Critics say an enormous number of hospitalists put themselves at risk and potentially jeopardize patient care by taking part in these consultations. These dangers seem to increase when the consultation veers from the general educational question to advice on treating a specific patient.
“Medical errors are potentially a lot higher in curbside consultations because much is lost in translation,” Dr. Zwillich explains. “When a curbside is used as a substitute for the physician seeing the patient, it can result in an incorrect diagnosis and medical errors.”
Dr. Zwillich is concerned because a physician can give the best treatment advice, but if the underlying diagnosis is wrong patients can be harmed. Because curbsides are quick, one physician doesn’t know if the other physician is leaving out something critical or even if the underlying diagnosis is correct. “By taking a curbside consult, you are giving up your opportunity to make an alternative diagnosis,” Dr. Zwillich says.
When giving advice on a specific patient nothing beats a formal consultation in which the patient is seen and a complete history is taken, he says: “The best care is given at the bedside.”
Legal Liability
Dr. Nagamine also fears the risk hospitalists take for a medical malpractice lawsuit. “My biggest concern is when hospitalists don’t recognize the risk they take on,” she says. “We shouldn’t take a curbside consult without knowing the risks.”
Traditionally, medical malpractice liability for curbside consultations has hinged on an established physician-patient relationship, generally limited to hospitalists seeing a patient. “Courts have been reluctant to extend liability to specialists consulted informally by the patient’s primary physician,” writes Kim Baker, JD, a healthcare attorney with Williams Kastner, in Seattle, Wash., in an analysis of court rulings.
However, courts are allowing suits to proceed against the consulting hospitalist, trying to decide whether a physician-patient relationship existed—and if so whether the [consulting] physician’s advice led to the alleged malpractice. Particularly relevant to hospitalists is the legal question of whether a pre-existing contract between the consulting physician and the hospital creates a physician-patient relationship with patients in that hospital. On this question courts have been mixed. In other cases, liability turned on whether the consultant physician went beyond giving general advice to participating in the patient’s care.
Courts are continually revising their rulings and may change the way they interpret a physician-patient relationship. Baker cautions that this may be a trend with curbside consults. She says trial attorneys are continually trying to find ways to bring more hospitalists into a suit. Baker sees a “discernible shift away from the longstanding policy that favors physician’s expectations over those of patients when determining whether a particular physician owed a duty of care to a particular patient.” She warns that hospitalists who engage in informal consults “may be at greater risk for medical malpractice liability.”
Can’t Stop Lawsuits
The reality of a litigious society is that even if you aren’t liable for malpractice you can still be sued. Attorneys routinely “paper the hospital,” naming in a suit everyone who came in contact with a patient or gave advice on his treatment, says Robin Diamond, MSN, JD, vice president of patient safety at The Doctors Company, Napa, Calif., a professional liability insurer of hospitalists and other hospitalists.
“Even if you have no responsibility, you still have to go through all the pain, expense, and heartache of getting yourself dismissed from the suit,” she explains. “What makes the curbside consultation easy and convenient for the consulting physician is what turns it into a legal nightmare for both of them.” Because the consult is on the run, the consulting physician may not give all the information that reveals the whole clinical picture.
So far The Doctors Company hasn’t seen a significant number of lawsuits against hospitalists—but this could increase as the subspecialty grows, Diamond says. The closest example she knows of is a pending case in which a hospitalist is being sued for advice he gave in a consult in an emergency department.
Two things concern Diamond most about curbside consults. The first is that because there is no documentation in a curbside consult, the physician giving advice cannot prove later what was said. Insurers worry that because there is no documentation of curbside consults it can be one physician’s word against the other’s if the case goes to court. There can be disagreements about what was said, when, and the advice given—and no way to prove who is right, she says.
Her second area of concern is when the conversation goes from general to specific. A physician is easier to defend if it can be proved that the question asked was general and didn’t have a specific application or sharing of clinical expertise. If a specific patient and a specific history is discussed, courts could establish that this constituted a formal consultation and established a patient-physician relationship. They could also establish that the consulting physician relied on the recommendation, which harmed the patient, Diamond says.
Despite the dangers, are hospitalists likely to stop doing curbside consultations? Even the critics answer with a resounding “no.” They say such consults are a fact of life.
“Curbsides are a part of our professional community of care,” Dr. Zwillich says. “It’s good to ask advice of other hospitalists. The danger comes when a curbside is used as a substitute for a needed full consultation.”
Dr. Nagamine thinks curbside consultations are a good way for hospitalists to continue their medical education. “In the hospital setting, many knowledgeable hospitalists are nearby, and you can learn a lot from them. I don’t think that’s bad or wrong,” she says. “The biggest problem we have is not asking for help when you’re not sure. I’m all for making it easy for hospitalists to ask for advice when they are not sure. But I’m in favor of full consultations when appropriate.”
Safer Consults
If hospitalists are going to participate in curbside consults they can make them safer by following this advice: Tread carefully, keep it general, think before you speak, and consider documenting what you say. And never hesitate to ask to see the patient.
Keep the curbside consultation general and brief: Curbside consultations may be safer when they are more general and used for the physician’s general education, experts agree. It’s when the discussion gets complex or about a specific patient that it’s time to think before you speak and be cautious.
Diamond says it is probably safe to say to another physician: “This is what I just saw. Have you ever seen it before?” But once the question goes from there to asking the physician what he or she did in such a case, “That’s when you’ve got to say, ‘Wait a minute, this is becoming so complex that it would be better if we did a formal consult.’ ”
Consider the risk of being wrong: “You have to ask yourself what is the downside—or the risk—of the question you’re asking,” Dr. Nagamine says. “If you know you’re going to order some tests and want to know which one to do first, this is far less risky than [deciding] if … we admit someone to the hospital or send him home.” In the first case there’s probably not much risk because you can order other tests if the first ones don’t give you the results you need. But in the second, if you send someone home and you are wrong, you can cause harm, she explains.
Dr. Nagamine also recommends considering the seriousness of the patient’s condition. Patients rarely die from a rash but can if you’re wrong about chest pain, for example.
“You need to ask yourself, ‘What’s the complexity of the case and the downside of being wrong and what, exactly [is my colleague] asking me?’ ” she says.
Ask specific questions: “Think very carefully about whether the situation is appropriate for a curbside consultation,” Dr. Nagamine cautions. “Ask probing questions that assure you that the correct and complete information was gathered. What is the quality of the information you’re being given?” If you don’t have complete faith in the ability of the physician asking you for a consult, it’s best to see the patient, she says.
Consider facts not given: Diamond recommends the hospitalists consider the facts not given before deciding to give advice in a curbside consultation. The physician asking for the consult is going to give the information he feels is important at the time. He may have left out or discounted important facts about the patient’s history. Ask “What am I not getting here?” she recommends.
Don’t hesitate to ask to see the patient: Dr. Nagamine urges hospitalists not to refrain from asking to see the patient involved. “Many times I feel like the other physician really wants me to see the patient but doesn’t want to bother me. I find they are relieved when I suggest that I see the patient,” she says. “Other times hospitalists don’t like to admit they are in over their heads and ask for help. In many cases when I see the patient I’m glad I did.”
Document the conversation: The Doctors Company recommends hospitalists document curbside consultations. “Keep a brief record of it in a memo to yourself, “ Diamond says. However, that can be a Catch-22. “If you end up in court you have to supply all the information you have. So we say that if it gets to the point that you feel like you need to document a curbside consult, you need to bump it up to a formal consultation.”
Know your responsibilities to the hospital: For those hospitalists who work at more than one hospital, Diamond recommends you make sure you are following hospital protocol and not doing more than the hospital expects from you. Some hospitalists think it’s their responsibility to take a curbside consult from a facility’s hospitalists, and it may not be the case. All hospitals don’t have the same expectations of hospitalists, she says.
Dr. Nagamine thinks the stakes are higher for hospitalists taking curbside consultations because hospitalized patients are usually sicker than in an office setting. So the hospitalist may need to be even more cautious. TH
Barbara Dillard is a medical journalist based in Chicago.
Resources
- Manian FA. Curbside consultations: a closer look at a common practice. JAMA. 1996;275(22):145-147.
- Perley CM. Physician use of the curbside consultation to address information needs. J Med Libr Assoc. 2006 April;94(2);137-144.
- Pearson SD, Moreno R, Trnka Y. Informal consultations provided to general internists by the gastroenterology department of an HMO. J Gen Intern Med. 1998 July;13(7):435-438.
Everyone has been there. You’re making rounds in the hospital and another physician taps you on the shoulder and says, “Can I ask you something?” He then gives the details and diagnosis of a patient’s condition and asks, “What would you suggest?”
Or maybe you stop the cardiologist in the hall to run your planned treatment of a particularly perplexing case by him.
These encounters—called curbside consultations—happen everywhere: hallways, cocktail parties, weddings, parking lots, and, increasingly, on the Internet.
As hospitalists increase their presence, they expose themselves to more curbside consultations—and the risks they entail. The practice is fraught with minefields that can turn the best of intentions into a potential medical and legal nightmare.
The term curbside consults implies opportunity—and hospitalists are most available to other hospitalists as they work in the hospital. In return, hospitalists have a greater opportunity to ask questions of other specialists without even picking up a telephone. A combination of geography and opportunity puts hospitalists at increasingly greater risk.
“We’re so accessible to other doctors in the hospital,” says Janet Nagamine, MD, chair of SHM’s Hospital Quality and Patient Safety committee and a hospitalist at Kaiser Permanente Santa Clara Medical Center in California. “I think we get more requests for informal consultations because we are there. It’s so easy for another physician to tap you on the shoulder and ask what you think about a patient’s condition or treatment. I am more frequently the giver of information than the receiver because it is so easy for a physician to tap me on the shoulder and ask my opinion.”
Proximity also presents an increased opportunity for hospitalists to seek a curbside consult from another physician in the hall. “I think hospitalists are more likely to ask for help from specialists they see in the hospital because hospitalists are generalists and can see a wide variety of conditions in the hospital,” says Clifford Zwillich, MD, professor of medicine at the University of Colorado and a hospitalist at the Denver Veterans Affairs Medical Center.
—Janet Nagamine, MD, chair of SHM’s Hospital Quality and Patient Safety committee and hospitalist, Kaiser Permanente Santa Clara Medical Center (Calif.)
Widespread Practice
In an April 2006 study in the Journal of the Medical Library Association, hospitalists reported that they seek a curbside consultation for a variety of reasons. These include:
- Confirm what they already know;
- Get quick answers to a question;
- Continue their medical education;
- Determine if a formal consultation is called for;
- Negotiate an appropriate course of treatment for a particular patient;
- Spread the emotional risk during a difficult case;
- Create or sustain camaraderie with physician colleges;
- Find like thinkers among their physician colleagues;
- Monitor their own knowledge; and
- Obtain help to get out of a difficult situation.
Hospitalists who provide curbside consultations reported doing so to provide good patient care, fulfill professional obligations, serve doctors, and encourage formal referrals.
Another study reported that 70% of primary care hospitalists and 68% of subspecialists surveyed participated in at least one informal consult in the previous week.
Critics say an enormous number of hospitalists put themselves at risk and potentially jeopardize patient care by taking part in these consultations. These dangers seem to increase when the consultation veers from the general educational question to advice on treating a specific patient.
“Medical errors are potentially a lot higher in curbside consultations because much is lost in translation,” Dr. Zwillich explains. “When a curbside is used as a substitute for the physician seeing the patient, it can result in an incorrect diagnosis and medical errors.”
Dr. Zwillich is concerned because a physician can give the best treatment advice, but if the underlying diagnosis is wrong patients can be harmed. Because curbsides are quick, one physician doesn’t know if the other physician is leaving out something critical or even if the underlying diagnosis is correct. “By taking a curbside consult, you are giving up your opportunity to make an alternative diagnosis,” Dr. Zwillich says.
When giving advice on a specific patient nothing beats a formal consultation in which the patient is seen and a complete history is taken, he says: “The best care is given at the bedside.”
Legal Liability
Dr. Nagamine also fears the risk hospitalists take for a medical malpractice lawsuit. “My biggest concern is when hospitalists don’t recognize the risk they take on,” she says. “We shouldn’t take a curbside consult without knowing the risks.”
Traditionally, medical malpractice liability for curbside consultations has hinged on an established physician-patient relationship, generally limited to hospitalists seeing a patient. “Courts have been reluctant to extend liability to specialists consulted informally by the patient’s primary physician,” writes Kim Baker, JD, a healthcare attorney with Williams Kastner, in Seattle, Wash., in an analysis of court rulings.
However, courts are allowing suits to proceed against the consulting hospitalist, trying to decide whether a physician-patient relationship existed—and if so whether the [consulting] physician’s advice led to the alleged malpractice. Particularly relevant to hospitalists is the legal question of whether a pre-existing contract between the consulting physician and the hospital creates a physician-patient relationship with patients in that hospital. On this question courts have been mixed. In other cases, liability turned on whether the consultant physician went beyond giving general advice to participating in the patient’s care.
Courts are continually revising their rulings and may change the way they interpret a physician-patient relationship. Baker cautions that this may be a trend with curbside consults. She says trial attorneys are continually trying to find ways to bring more hospitalists into a suit. Baker sees a “discernible shift away from the longstanding policy that favors physician’s expectations over those of patients when determining whether a particular physician owed a duty of care to a particular patient.” She warns that hospitalists who engage in informal consults “may be at greater risk for medical malpractice liability.”
Can’t Stop Lawsuits
The reality of a litigious society is that even if you aren’t liable for malpractice you can still be sued. Attorneys routinely “paper the hospital,” naming in a suit everyone who came in contact with a patient or gave advice on his treatment, says Robin Diamond, MSN, JD, vice president of patient safety at The Doctors Company, Napa, Calif., a professional liability insurer of hospitalists and other hospitalists.
“Even if you have no responsibility, you still have to go through all the pain, expense, and heartache of getting yourself dismissed from the suit,” she explains. “What makes the curbside consultation easy and convenient for the consulting physician is what turns it into a legal nightmare for both of them.” Because the consult is on the run, the consulting physician may not give all the information that reveals the whole clinical picture.
So far The Doctors Company hasn’t seen a significant number of lawsuits against hospitalists—but this could increase as the subspecialty grows, Diamond says. The closest example she knows of is a pending case in which a hospitalist is being sued for advice he gave in a consult in an emergency department.
Two things concern Diamond most about curbside consults. The first is that because there is no documentation in a curbside consult, the physician giving advice cannot prove later what was said. Insurers worry that because there is no documentation of curbside consults it can be one physician’s word against the other’s if the case goes to court. There can be disagreements about what was said, when, and the advice given—and no way to prove who is right, she says.
Her second area of concern is when the conversation goes from general to specific. A physician is easier to defend if it can be proved that the question asked was general and didn’t have a specific application or sharing of clinical expertise. If a specific patient and a specific history is discussed, courts could establish that this constituted a formal consultation and established a patient-physician relationship. They could also establish that the consulting physician relied on the recommendation, which harmed the patient, Diamond says.
Despite the dangers, are hospitalists likely to stop doing curbside consultations? Even the critics answer with a resounding “no.” They say such consults are a fact of life.
“Curbsides are a part of our professional community of care,” Dr. Zwillich says. “It’s good to ask advice of other hospitalists. The danger comes when a curbside is used as a substitute for a needed full consultation.”
Dr. Nagamine thinks curbside consultations are a good way for hospitalists to continue their medical education. “In the hospital setting, many knowledgeable hospitalists are nearby, and you can learn a lot from them. I don’t think that’s bad or wrong,” she says. “The biggest problem we have is not asking for help when you’re not sure. I’m all for making it easy for hospitalists to ask for advice when they are not sure. But I’m in favor of full consultations when appropriate.”
Safer Consults
If hospitalists are going to participate in curbside consults they can make them safer by following this advice: Tread carefully, keep it general, think before you speak, and consider documenting what you say. And never hesitate to ask to see the patient.
Keep the curbside consultation general and brief: Curbside consultations may be safer when they are more general and used for the physician’s general education, experts agree. It’s when the discussion gets complex or about a specific patient that it’s time to think before you speak and be cautious.
Diamond says it is probably safe to say to another physician: “This is what I just saw. Have you ever seen it before?” But once the question goes from there to asking the physician what he or she did in such a case, “That’s when you’ve got to say, ‘Wait a minute, this is becoming so complex that it would be better if we did a formal consult.’ ”
Consider the risk of being wrong: “You have to ask yourself what is the downside—or the risk—of the question you’re asking,” Dr. Nagamine says. “If you know you’re going to order some tests and want to know which one to do first, this is far less risky than [deciding] if … we admit someone to the hospital or send him home.” In the first case there’s probably not much risk because you can order other tests if the first ones don’t give you the results you need. But in the second, if you send someone home and you are wrong, you can cause harm, she explains.
Dr. Nagamine also recommends considering the seriousness of the patient’s condition. Patients rarely die from a rash but can if you’re wrong about chest pain, for example.
“You need to ask yourself, ‘What’s the complexity of the case and the downside of being wrong and what, exactly [is my colleague] asking me?’ ” she says.
Ask specific questions: “Think very carefully about whether the situation is appropriate for a curbside consultation,” Dr. Nagamine cautions. “Ask probing questions that assure you that the correct and complete information was gathered. What is the quality of the information you’re being given?” If you don’t have complete faith in the ability of the physician asking you for a consult, it’s best to see the patient, she says.
Consider facts not given: Diamond recommends the hospitalists consider the facts not given before deciding to give advice in a curbside consultation. The physician asking for the consult is going to give the information he feels is important at the time. He may have left out or discounted important facts about the patient’s history. Ask “What am I not getting here?” she recommends.
Don’t hesitate to ask to see the patient: Dr. Nagamine urges hospitalists not to refrain from asking to see the patient involved. “Many times I feel like the other physician really wants me to see the patient but doesn’t want to bother me. I find they are relieved when I suggest that I see the patient,” she says. “Other times hospitalists don’t like to admit they are in over their heads and ask for help. In many cases when I see the patient I’m glad I did.”
Document the conversation: The Doctors Company recommends hospitalists document curbside consultations. “Keep a brief record of it in a memo to yourself, “ Diamond says. However, that can be a Catch-22. “If you end up in court you have to supply all the information you have. So we say that if it gets to the point that you feel like you need to document a curbside consult, you need to bump it up to a formal consultation.”
Know your responsibilities to the hospital: For those hospitalists who work at more than one hospital, Diamond recommends you make sure you are following hospital protocol and not doing more than the hospital expects from you. Some hospitalists think it’s their responsibility to take a curbside consult from a facility’s hospitalists, and it may not be the case. All hospitals don’t have the same expectations of hospitalists, she says.
Dr. Nagamine thinks the stakes are higher for hospitalists taking curbside consultations because hospitalized patients are usually sicker than in an office setting. So the hospitalist may need to be even more cautious. TH
Barbara Dillard is a medical journalist based in Chicago.
Resources
- Manian FA. Curbside consultations: a closer look at a common practice. JAMA. 1996;275(22):145-147.
- Perley CM. Physician use of the curbside consultation to address information needs. J Med Libr Assoc. 2006 April;94(2);137-144.
- Pearson SD, Moreno R, Trnka Y. Informal consultations provided to general internists by the gastroenterology department of an HMO. J Gen Intern Med. 1998 July;13(7):435-438.
Everyone has been there. You’re making rounds in the hospital and another physician taps you on the shoulder and says, “Can I ask you something?” He then gives the details and diagnosis of a patient’s condition and asks, “What would you suggest?”
Or maybe you stop the cardiologist in the hall to run your planned treatment of a particularly perplexing case by him.
These encounters—called curbside consultations—happen everywhere: hallways, cocktail parties, weddings, parking lots, and, increasingly, on the Internet.
As hospitalists increase their presence, they expose themselves to more curbside consultations—and the risks they entail. The practice is fraught with minefields that can turn the best of intentions into a potential medical and legal nightmare.
The term curbside consults implies opportunity—and hospitalists are most available to other hospitalists as they work in the hospital. In return, hospitalists have a greater opportunity to ask questions of other specialists without even picking up a telephone. A combination of geography and opportunity puts hospitalists at increasingly greater risk.
“We’re so accessible to other doctors in the hospital,” says Janet Nagamine, MD, chair of SHM’s Hospital Quality and Patient Safety committee and a hospitalist at Kaiser Permanente Santa Clara Medical Center in California. “I think we get more requests for informal consultations because we are there. It’s so easy for another physician to tap you on the shoulder and ask what you think about a patient’s condition or treatment. I am more frequently the giver of information than the receiver because it is so easy for a physician to tap me on the shoulder and ask my opinion.”
Proximity also presents an increased opportunity for hospitalists to seek a curbside consult from another physician in the hall. “I think hospitalists are more likely to ask for help from specialists they see in the hospital because hospitalists are generalists and can see a wide variety of conditions in the hospital,” says Clifford Zwillich, MD, professor of medicine at the University of Colorado and a hospitalist at the Denver Veterans Affairs Medical Center.
—Janet Nagamine, MD, chair of SHM’s Hospital Quality and Patient Safety committee and hospitalist, Kaiser Permanente Santa Clara Medical Center (Calif.)
Widespread Practice
In an April 2006 study in the Journal of the Medical Library Association, hospitalists reported that they seek a curbside consultation for a variety of reasons. These include:
- Confirm what they already know;
- Get quick answers to a question;
- Continue their medical education;
- Determine if a formal consultation is called for;
- Negotiate an appropriate course of treatment for a particular patient;
- Spread the emotional risk during a difficult case;
- Create or sustain camaraderie with physician colleges;
- Find like thinkers among their physician colleagues;
- Monitor their own knowledge; and
- Obtain help to get out of a difficult situation.
Hospitalists who provide curbside consultations reported doing so to provide good patient care, fulfill professional obligations, serve doctors, and encourage formal referrals.
Another study reported that 70% of primary care hospitalists and 68% of subspecialists surveyed participated in at least one informal consult in the previous week.
Critics say an enormous number of hospitalists put themselves at risk and potentially jeopardize patient care by taking part in these consultations. These dangers seem to increase when the consultation veers from the general educational question to advice on treating a specific patient.
“Medical errors are potentially a lot higher in curbside consultations because much is lost in translation,” Dr. Zwillich explains. “When a curbside is used as a substitute for the physician seeing the patient, it can result in an incorrect diagnosis and medical errors.”
Dr. Zwillich is concerned because a physician can give the best treatment advice, but if the underlying diagnosis is wrong patients can be harmed. Because curbsides are quick, one physician doesn’t know if the other physician is leaving out something critical or even if the underlying diagnosis is correct. “By taking a curbside consult, you are giving up your opportunity to make an alternative diagnosis,” Dr. Zwillich says.
When giving advice on a specific patient nothing beats a formal consultation in which the patient is seen and a complete history is taken, he says: “The best care is given at the bedside.”
Legal Liability
Dr. Nagamine also fears the risk hospitalists take for a medical malpractice lawsuit. “My biggest concern is when hospitalists don’t recognize the risk they take on,” she says. “We shouldn’t take a curbside consult without knowing the risks.”
Traditionally, medical malpractice liability for curbside consultations has hinged on an established physician-patient relationship, generally limited to hospitalists seeing a patient. “Courts have been reluctant to extend liability to specialists consulted informally by the patient’s primary physician,” writes Kim Baker, JD, a healthcare attorney with Williams Kastner, in Seattle, Wash., in an analysis of court rulings.
However, courts are allowing suits to proceed against the consulting hospitalist, trying to decide whether a physician-patient relationship existed—and if so whether the [consulting] physician’s advice led to the alleged malpractice. Particularly relevant to hospitalists is the legal question of whether a pre-existing contract between the consulting physician and the hospital creates a physician-patient relationship with patients in that hospital. On this question courts have been mixed. In other cases, liability turned on whether the consultant physician went beyond giving general advice to participating in the patient’s care.
Courts are continually revising their rulings and may change the way they interpret a physician-patient relationship. Baker cautions that this may be a trend with curbside consults. She says trial attorneys are continually trying to find ways to bring more hospitalists into a suit. Baker sees a “discernible shift away from the longstanding policy that favors physician’s expectations over those of patients when determining whether a particular physician owed a duty of care to a particular patient.” She warns that hospitalists who engage in informal consults “may be at greater risk for medical malpractice liability.”
Can’t Stop Lawsuits
The reality of a litigious society is that even if you aren’t liable for malpractice you can still be sued. Attorneys routinely “paper the hospital,” naming in a suit everyone who came in contact with a patient or gave advice on his treatment, says Robin Diamond, MSN, JD, vice president of patient safety at The Doctors Company, Napa, Calif., a professional liability insurer of hospitalists and other hospitalists.
“Even if you have no responsibility, you still have to go through all the pain, expense, and heartache of getting yourself dismissed from the suit,” she explains. “What makes the curbside consultation easy and convenient for the consulting physician is what turns it into a legal nightmare for both of them.” Because the consult is on the run, the consulting physician may not give all the information that reveals the whole clinical picture.
So far The Doctors Company hasn’t seen a significant number of lawsuits against hospitalists—but this could increase as the subspecialty grows, Diamond says. The closest example she knows of is a pending case in which a hospitalist is being sued for advice he gave in a consult in an emergency department.
Two things concern Diamond most about curbside consults. The first is that because there is no documentation in a curbside consult, the physician giving advice cannot prove later what was said. Insurers worry that because there is no documentation of curbside consults it can be one physician’s word against the other’s if the case goes to court. There can be disagreements about what was said, when, and the advice given—and no way to prove who is right, she says.
Her second area of concern is when the conversation goes from general to specific. A physician is easier to defend if it can be proved that the question asked was general and didn’t have a specific application or sharing of clinical expertise. If a specific patient and a specific history is discussed, courts could establish that this constituted a formal consultation and established a patient-physician relationship. They could also establish that the consulting physician relied on the recommendation, which harmed the patient, Diamond says.
Despite the dangers, are hospitalists likely to stop doing curbside consultations? Even the critics answer with a resounding “no.” They say such consults are a fact of life.
“Curbsides are a part of our professional community of care,” Dr. Zwillich says. “It’s good to ask advice of other hospitalists. The danger comes when a curbside is used as a substitute for a needed full consultation.”
Dr. Nagamine thinks curbside consultations are a good way for hospitalists to continue their medical education. “In the hospital setting, many knowledgeable hospitalists are nearby, and you can learn a lot from them. I don’t think that’s bad or wrong,” she says. “The biggest problem we have is not asking for help when you’re not sure. I’m all for making it easy for hospitalists to ask for advice when they are not sure. But I’m in favor of full consultations when appropriate.”
Safer Consults
If hospitalists are going to participate in curbside consults they can make them safer by following this advice: Tread carefully, keep it general, think before you speak, and consider documenting what you say. And never hesitate to ask to see the patient.
Keep the curbside consultation general and brief: Curbside consultations may be safer when they are more general and used for the physician’s general education, experts agree. It’s when the discussion gets complex or about a specific patient that it’s time to think before you speak and be cautious.
Diamond says it is probably safe to say to another physician: “This is what I just saw. Have you ever seen it before?” But once the question goes from there to asking the physician what he or she did in such a case, “That’s when you’ve got to say, ‘Wait a minute, this is becoming so complex that it would be better if we did a formal consult.’ ”
Consider the risk of being wrong: “You have to ask yourself what is the downside—or the risk—of the question you’re asking,” Dr. Nagamine says. “If you know you’re going to order some tests and want to know which one to do first, this is far less risky than [deciding] if … we admit someone to the hospital or send him home.” In the first case there’s probably not much risk because you can order other tests if the first ones don’t give you the results you need. But in the second, if you send someone home and you are wrong, you can cause harm, she explains.
Dr. Nagamine also recommends considering the seriousness of the patient’s condition. Patients rarely die from a rash but can if you’re wrong about chest pain, for example.
“You need to ask yourself, ‘What’s the complexity of the case and the downside of being wrong and what, exactly [is my colleague] asking me?’ ” she says.
Ask specific questions: “Think very carefully about whether the situation is appropriate for a curbside consultation,” Dr. Nagamine cautions. “Ask probing questions that assure you that the correct and complete information was gathered. What is the quality of the information you’re being given?” If you don’t have complete faith in the ability of the physician asking you for a consult, it’s best to see the patient, she says.
Consider facts not given: Diamond recommends the hospitalists consider the facts not given before deciding to give advice in a curbside consultation. The physician asking for the consult is going to give the information he feels is important at the time. He may have left out or discounted important facts about the patient’s history. Ask “What am I not getting here?” she recommends.
Don’t hesitate to ask to see the patient: Dr. Nagamine urges hospitalists not to refrain from asking to see the patient involved. “Many times I feel like the other physician really wants me to see the patient but doesn’t want to bother me. I find they are relieved when I suggest that I see the patient,” she says. “Other times hospitalists don’t like to admit they are in over their heads and ask for help. In many cases when I see the patient I’m glad I did.”
Document the conversation: The Doctors Company recommends hospitalists document curbside consultations. “Keep a brief record of it in a memo to yourself, “ Diamond says. However, that can be a Catch-22. “If you end up in court you have to supply all the information you have. So we say that if it gets to the point that you feel like you need to document a curbside consult, you need to bump it up to a formal consultation.”
Know your responsibilities to the hospital: For those hospitalists who work at more than one hospital, Diamond recommends you make sure you are following hospital protocol and not doing more than the hospital expects from you. Some hospitalists think it’s their responsibility to take a curbside consult from a facility’s hospitalists, and it may not be the case. All hospitals don’t have the same expectations of hospitalists, she says.
Dr. Nagamine thinks the stakes are higher for hospitalists taking curbside consultations because hospitalized patients are usually sicker than in an office setting. So the hospitalist may need to be even more cautious. TH
Barbara Dillard is a medical journalist based in Chicago.
Resources
- Manian FA. Curbside consultations: a closer look at a common practice. JAMA. 1996;275(22):145-147.
- Perley CM. Physician use of the curbside consultation to address information needs. J Med Libr Assoc. 2006 April;94(2);137-144.
- Pearson SD, Moreno R, Trnka Y. Informal consultations provided to general internists by the gastroenterology department of an HMO. J Gen Intern Med. 1998 July;13(7):435-438.