User login
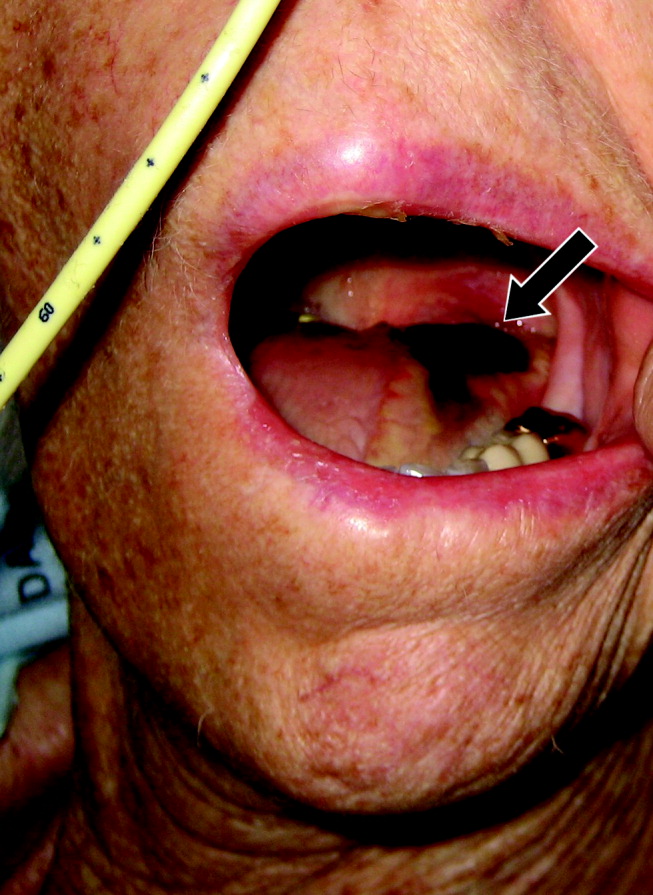
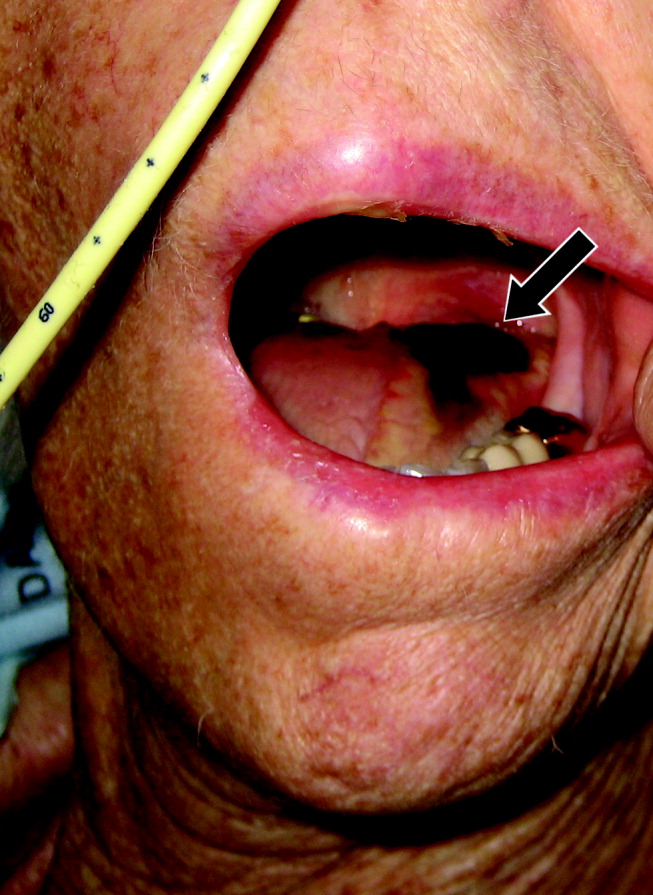
Tongue necrosis from temporal arteritis
A 77‐year‐old woman with hypothyroidism presented with a 2‐week history of head, neck, jaw, and tongue pain. She had also developed slurred speech and difficulty chewing. On examination she had a temperature of 38.0C. She was without neurological deficits. However, she did have difficulty protruding her tongue, which had a cyanotic appearance and was painful. Laboratory findings showed an erythrocyte sedimentation rate of 68 mm/hr. Temporal arteritis was suspected, and the patient was started on corticosteroids. A subsequent temporal artery biopsy revealed inflammation and thrombus formation consistent with temporal arteritis. On hospital day 3, she developed unilateral ischemia in her tongue, which eventually became necrotic (Fig. 1). Although tongue necrosis is rare, temporal arteritis is the most frequent cause. It is usually unilateral and caused by compromised blood supply as a result of vasculitis in one of the lingual arteries. Other causes of tongue necrosis such as embolus, abscess, syphilis, tongue carcinoma, and Hodgkin's disease should be excluded.1, 2 Although necrotic tongue tissue must sometimes be extensively debrided or resected, our patient required minimal debridement. At follow‐up 1 month later, she was recovering at home with ongoing speech therapy and a corticosteroid taper.
- ,,.Lingual infarction: a review of the literature.Ann Vasc Surg.1992;6:450–452.
- ,.The ESR in the diagnosis and management of the polymyalgia rheumatica/giant cell arteritis syndrome.Ann Rheum Dis.1983;42:168–170.
A 77‐year‐old woman with hypothyroidism presented with a 2‐week history of head, neck, jaw, and tongue pain. She had also developed slurred speech and difficulty chewing. On examination she had a temperature of 38.0C. She was without neurological deficits. However, she did have difficulty protruding her tongue, which had a cyanotic appearance and was painful. Laboratory findings showed an erythrocyte sedimentation rate of 68 mm/hr. Temporal arteritis was suspected, and the patient was started on corticosteroids. A subsequent temporal artery biopsy revealed inflammation and thrombus formation consistent with temporal arteritis. On hospital day 3, she developed unilateral ischemia in her tongue, which eventually became necrotic (Fig. 1). Although tongue necrosis is rare, temporal arteritis is the most frequent cause. It is usually unilateral and caused by compromised blood supply as a result of vasculitis in one of the lingual arteries. Other causes of tongue necrosis such as embolus, abscess, syphilis, tongue carcinoma, and Hodgkin's disease should be excluded.1, 2 Although necrotic tongue tissue must sometimes be extensively debrided or resected, our patient required minimal debridement. At follow‐up 1 month later, she was recovering at home with ongoing speech therapy and a corticosteroid taper.
A 77‐year‐old woman with hypothyroidism presented with a 2‐week history of head, neck, jaw, and tongue pain. She had also developed slurred speech and difficulty chewing. On examination she had a temperature of 38.0C. She was without neurological deficits. However, she did have difficulty protruding her tongue, which had a cyanotic appearance and was painful. Laboratory findings showed an erythrocyte sedimentation rate of 68 mm/hr. Temporal arteritis was suspected, and the patient was started on corticosteroids. A subsequent temporal artery biopsy revealed inflammation and thrombus formation consistent with temporal arteritis. On hospital day 3, she developed unilateral ischemia in her tongue, which eventually became necrotic (Fig. 1). Although tongue necrosis is rare, temporal arteritis is the most frequent cause. It is usually unilateral and caused by compromised blood supply as a result of vasculitis in one of the lingual arteries. Other causes of tongue necrosis such as embolus, abscess, syphilis, tongue carcinoma, and Hodgkin's disease should be excluded.1, 2 Although necrotic tongue tissue must sometimes be extensively debrided or resected, our patient required minimal debridement. At follow‐up 1 month later, she was recovering at home with ongoing speech therapy and a corticosteroid taper.
- ,,.Lingual infarction: a review of the literature.Ann Vasc Surg.1992;6:450–452.
- ,.The ESR in the diagnosis and management of the polymyalgia rheumatica/giant cell arteritis syndrome.Ann Rheum Dis.1983;42:168–170.
- ,,.Lingual infarction: a review of the literature.Ann Vasc Surg.1992;6:450–452.
- ,.The ESR in the diagnosis and management of the polymyalgia rheumatica/giant cell arteritis syndrome.Ann Rheum Dis.1983;42:168–170.
Linezolid‐ and vancomycin‐resistant Enterococcus faecium endocarditis: Successful treatment with tigecycline and daptomycin
Enterococci are a leading cause of endocarditis and nosocomial infections. Vancomycin‐resistant enterococci (VRE) emerged in the 1980s and now represent most nosocomial isolates in the United States. The first case of VRE endocarditis was reported in 1996.1 Although increasing enterococcal antibiotic resistance has prompted increasing reliance on newer antibiotics,2 a recent review of VRE endocarditis noted that survival rates were similar to those for vancomycin‐sensitive enterococcal endocarditis.1 Cure was achieved in several patients with bacteriostatic agents in the absence of valve replacement, but no patients were infected with truly linezolid‐resistant organisms. This case of linezolid‐resistant VRE endocarditis represents the first reported cure of infective endocarditis with a tigecycline‐containing regimen.
CASE REPORT
A 62‐year‐old man presented with hypoglycemia and delirium. His medical history included diabetes mellitus, coronary and peripheral arterial disease, and end‐stage renal disease. He had had endocarditis of an unknown type 12 years prior to admission. He had recently developed septic shock because of a Candida parapsilosis, Enterobacter cloacae, and Staphylococcus epidermidis infection of a peripherally inserted central catheter (PICC) and received 14 days of vancomycin, meropenem, and fluconazole administered through a new PICC. This catheter was not removed, and 39 days after completion of the antibiotic therapy, he developed hypoglycemia, which was attributed to weight loss without adjustment of his insulin regimen. He was afebrile; examination revealed a new 3/6 holosystolic murmur radiating to the axilla. There were no other stigmata of infective endocarditis, and his PICC and arteriovenous fistula sites appeared normal. Delirium resolved after administration of intravenous glucose.
E. faecium grew from all 6 initial blood cultures. A transesophageal echocardiogram revealed a new 3‐mm mitral valve vegetation with perforation and severe regurgitation. He had definite endocarditis on the basis of 2 major criteria.3 He was given vancomycin (1 g IV, then administered by levels), then switched to linezolid (600 mg orally every 12 hours), and finally tigecycline (100 mg IV followed by 50 mg IV every 12 hours) plus daptomycin (6 mg/kg IV every 48 hours) as further sensitivity data became available.
The organism was resistant to ampicillin, chloramphenicol, and linezolid (MIC > 20 g/mL), as well as vancomycin (MIC > 50 g/mL), quinupristin/dalfopristin (MIC 2.5 g/mL), and gentamicin (MIC > 200 g/mL), and demonstrated high‐level streptomycin resistance (>2000 g/mL). It was intermediate to doxycycline (MIC 5 g/mL). It was susceptible to daptomycin (MIC 4 g/mL) and tigecycline (MIC 0.06 g/mL).
Blood cultures done on hospital days 1, 4, 6, and 7 (day 1 of tigecycline) were positive, and multiple cultures were negative from day 10 on. Because of the lack of experience with tigecycline in infective endocarditis, unrevascularized left‐main coronary artery disease, and severe mitral regurgitation, the patient was advised to undergo valve replacement and coronary artery bypass surgery after antibiotic therapy. Because he feared surgical complications, he refused and received 70 days of tigecycline plus daptomycin therapy, which was complicated only by nausea. He remained clinically well and had negative blood cultures 16 weeks after completion of therapy.
DISCUSSION
Tigecycline, the first available glycylcycline, is a minocycline‐derived antibiotic that remains active in the presence of the ribosomal modifications and efflux pumps that mediate tetracycline resistance. Thus, it possesses broad‐spectrum bacteriostatic activity, including activity against VRE. A PubMed search revealed no published data about the use of tigecycline for endocarditis in humans. However, tetracyclines have been used to treat endocarditis due to such organisms as Bartonella, Coxiella burnetti, or methicillin‐resistant Staphylococcus aureus (MRSA), frequently for prolonged courses. Tetracyclines were combined with other antibiotics in 5 published cases of VRE endocarditis. All patients survived; 3 were cured with the tetracycline regimen and 2 with other antimicrobials.1 In animal models of endocarditis, tigecycline stabilized vegetation counts of E. faecalis and reduced vegetation counts of MRSA and 1 strain of E. faecium.4
Daptomycin, the first available cyclic lipopeptide, kills by nonlytic depolarization of the bacterial cell membrane. In a recent study, daptomycin was non‐inferior to vancomycin or antistaphylococcal penicillins for S. aureus bacteremia or endocarditis. Although a few patients had left‐sided endocarditis, only 1 of them experienced a successful outcome with daptomycin therapy, and daptomycin displayed a trend toward higher rates of persistent or relapsing infection.5 Less evidence supports the use of daptomycin for serious enterococcal infections.2 One report noted the deaths of 6 of 10 patients treated with daptomycin for VRE bacteremia, including both patients with endocarditis.6 Daptomycin was used successfully in a case of VRE endocarditis in combination with gentamicin and rifampin for 11 weeks1 and at least 6 other reported cases of VRE bacteremia.7, 8
In summary, despite tigecycline's lack of bactericidal activity or proven efficacy in endocarditis, daptomycin's prior performance in VRE bacteremia, and the isolate's borderline daptomycin susceptibility, prolonged combination therapy resulted in a cure of VRE endocarditis. This success extends the experience with using both agents in the treatment of resistant infections. As linezolid‐resistant VRE and other resistant pathogens become more common, the need for research on treatment options becomes more urgent, and familiarity with novel and lesser‐used antibiotics becomes more crucial for hospitalists.
- ,.Endocarditis due to vancomycin‐resistant enterococci: case report and review of the literature.Clin Infect Dis.2005;41:1134–1142.
- ,.Approaches to vancomycin resistant enterococci.Curr Opin Infect Dis.2004;17:541–547.
- ,,, et al.Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis.Clin Infect Dis.2000;4:633–638.
- ,,, et al.Activity and diffusion of tigecycline (GAR‐936) in experimental enterococcal endocarditis.Antimicrob Agents Chemother.2003;47:216–222.
- ,,, et al.Daptomycin versus standard therapy for bacteremia and endocarditis caused by staphylococcus aureus.New Engl J Med.2006;355:653–665.
- ,,.Daptomycin for the treatment of gram‐positive bacteremia and infective endocarditis: a retrospective case series of 31 patients.Pharmacotherapy.2006;26:347–352.
- ,,,,.Daptomycin in the treatment of vancomycin‐resistant Enterococcus faecium bacteremia in neutropenic patients.J Infect.2007;54:567–571.
- ,,,,.Daptomycin for the treatment of vancomycin resistant Enterococcus faecium bacteremia.Scand J Infect Dis.2006;38:290–292.
Enterococci are a leading cause of endocarditis and nosocomial infections. Vancomycin‐resistant enterococci (VRE) emerged in the 1980s and now represent most nosocomial isolates in the United States. The first case of VRE endocarditis was reported in 1996.1 Although increasing enterococcal antibiotic resistance has prompted increasing reliance on newer antibiotics,2 a recent review of VRE endocarditis noted that survival rates were similar to those for vancomycin‐sensitive enterococcal endocarditis.1 Cure was achieved in several patients with bacteriostatic agents in the absence of valve replacement, but no patients were infected with truly linezolid‐resistant organisms. This case of linezolid‐resistant VRE endocarditis represents the first reported cure of infective endocarditis with a tigecycline‐containing regimen.
CASE REPORT
A 62‐year‐old man presented with hypoglycemia and delirium. His medical history included diabetes mellitus, coronary and peripheral arterial disease, and end‐stage renal disease. He had had endocarditis of an unknown type 12 years prior to admission. He had recently developed septic shock because of a Candida parapsilosis, Enterobacter cloacae, and Staphylococcus epidermidis infection of a peripherally inserted central catheter (PICC) and received 14 days of vancomycin, meropenem, and fluconazole administered through a new PICC. This catheter was not removed, and 39 days after completion of the antibiotic therapy, he developed hypoglycemia, which was attributed to weight loss without adjustment of his insulin regimen. He was afebrile; examination revealed a new 3/6 holosystolic murmur radiating to the axilla. There were no other stigmata of infective endocarditis, and his PICC and arteriovenous fistula sites appeared normal. Delirium resolved after administration of intravenous glucose.
E. faecium grew from all 6 initial blood cultures. A transesophageal echocardiogram revealed a new 3‐mm mitral valve vegetation with perforation and severe regurgitation. He had definite endocarditis on the basis of 2 major criteria.3 He was given vancomycin (1 g IV, then administered by levels), then switched to linezolid (600 mg orally every 12 hours), and finally tigecycline (100 mg IV followed by 50 mg IV every 12 hours) plus daptomycin (6 mg/kg IV every 48 hours) as further sensitivity data became available.
The organism was resistant to ampicillin, chloramphenicol, and linezolid (MIC > 20 g/mL), as well as vancomycin (MIC > 50 g/mL), quinupristin/dalfopristin (MIC 2.5 g/mL), and gentamicin (MIC > 200 g/mL), and demonstrated high‐level streptomycin resistance (>2000 g/mL). It was intermediate to doxycycline (MIC 5 g/mL). It was susceptible to daptomycin (MIC 4 g/mL) and tigecycline (MIC 0.06 g/mL).
Blood cultures done on hospital days 1, 4, 6, and 7 (day 1 of tigecycline) were positive, and multiple cultures were negative from day 10 on. Because of the lack of experience with tigecycline in infective endocarditis, unrevascularized left‐main coronary artery disease, and severe mitral regurgitation, the patient was advised to undergo valve replacement and coronary artery bypass surgery after antibiotic therapy. Because he feared surgical complications, he refused and received 70 days of tigecycline plus daptomycin therapy, which was complicated only by nausea. He remained clinically well and had negative blood cultures 16 weeks after completion of therapy.
DISCUSSION
Tigecycline, the first available glycylcycline, is a minocycline‐derived antibiotic that remains active in the presence of the ribosomal modifications and efflux pumps that mediate tetracycline resistance. Thus, it possesses broad‐spectrum bacteriostatic activity, including activity against VRE. A PubMed search revealed no published data about the use of tigecycline for endocarditis in humans. However, tetracyclines have been used to treat endocarditis due to such organisms as Bartonella, Coxiella burnetti, or methicillin‐resistant Staphylococcus aureus (MRSA), frequently for prolonged courses. Tetracyclines were combined with other antibiotics in 5 published cases of VRE endocarditis. All patients survived; 3 were cured with the tetracycline regimen and 2 with other antimicrobials.1 In animal models of endocarditis, tigecycline stabilized vegetation counts of E. faecalis and reduced vegetation counts of MRSA and 1 strain of E. faecium.4
Daptomycin, the first available cyclic lipopeptide, kills by nonlytic depolarization of the bacterial cell membrane. In a recent study, daptomycin was non‐inferior to vancomycin or antistaphylococcal penicillins for S. aureus bacteremia or endocarditis. Although a few patients had left‐sided endocarditis, only 1 of them experienced a successful outcome with daptomycin therapy, and daptomycin displayed a trend toward higher rates of persistent or relapsing infection.5 Less evidence supports the use of daptomycin for serious enterococcal infections.2 One report noted the deaths of 6 of 10 patients treated with daptomycin for VRE bacteremia, including both patients with endocarditis.6 Daptomycin was used successfully in a case of VRE endocarditis in combination with gentamicin and rifampin for 11 weeks1 and at least 6 other reported cases of VRE bacteremia.7, 8
In summary, despite tigecycline's lack of bactericidal activity or proven efficacy in endocarditis, daptomycin's prior performance in VRE bacteremia, and the isolate's borderline daptomycin susceptibility, prolonged combination therapy resulted in a cure of VRE endocarditis. This success extends the experience with using both agents in the treatment of resistant infections. As linezolid‐resistant VRE and other resistant pathogens become more common, the need for research on treatment options becomes more urgent, and familiarity with novel and lesser‐used antibiotics becomes more crucial for hospitalists.
Enterococci are a leading cause of endocarditis and nosocomial infections. Vancomycin‐resistant enterococci (VRE) emerged in the 1980s and now represent most nosocomial isolates in the United States. The first case of VRE endocarditis was reported in 1996.1 Although increasing enterococcal antibiotic resistance has prompted increasing reliance on newer antibiotics,2 a recent review of VRE endocarditis noted that survival rates were similar to those for vancomycin‐sensitive enterococcal endocarditis.1 Cure was achieved in several patients with bacteriostatic agents in the absence of valve replacement, but no patients were infected with truly linezolid‐resistant organisms. This case of linezolid‐resistant VRE endocarditis represents the first reported cure of infective endocarditis with a tigecycline‐containing regimen.
CASE REPORT
A 62‐year‐old man presented with hypoglycemia and delirium. His medical history included diabetes mellitus, coronary and peripheral arterial disease, and end‐stage renal disease. He had had endocarditis of an unknown type 12 years prior to admission. He had recently developed septic shock because of a Candida parapsilosis, Enterobacter cloacae, and Staphylococcus epidermidis infection of a peripherally inserted central catheter (PICC) and received 14 days of vancomycin, meropenem, and fluconazole administered through a new PICC. This catheter was not removed, and 39 days after completion of the antibiotic therapy, he developed hypoglycemia, which was attributed to weight loss without adjustment of his insulin regimen. He was afebrile; examination revealed a new 3/6 holosystolic murmur radiating to the axilla. There were no other stigmata of infective endocarditis, and his PICC and arteriovenous fistula sites appeared normal. Delirium resolved after administration of intravenous glucose.
E. faecium grew from all 6 initial blood cultures. A transesophageal echocardiogram revealed a new 3‐mm mitral valve vegetation with perforation and severe regurgitation. He had definite endocarditis on the basis of 2 major criteria.3 He was given vancomycin (1 g IV, then administered by levels), then switched to linezolid (600 mg orally every 12 hours), and finally tigecycline (100 mg IV followed by 50 mg IV every 12 hours) plus daptomycin (6 mg/kg IV every 48 hours) as further sensitivity data became available.
The organism was resistant to ampicillin, chloramphenicol, and linezolid (MIC > 20 g/mL), as well as vancomycin (MIC > 50 g/mL), quinupristin/dalfopristin (MIC 2.5 g/mL), and gentamicin (MIC > 200 g/mL), and demonstrated high‐level streptomycin resistance (>2000 g/mL). It was intermediate to doxycycline (MIC 5 g/mL). It was susceptible to daptomycin (MIC 4 g/mL) and tigecycline (MIC 0.06 g/mL).
Blood cultures done on hospital days 1, 4, 6, and 7 (day 1 of tigecycline) were positive, and multiple cultures were negative from day 10 on. Because of the lack of experience with tigecycline in infective endocarditis, unrevascularized left‐main coronary artery disease, and severe mitral regurgitation, the patient was advised to undergo valve replacement and coronary artery bypass surgery after antibiotic therapy. Because he feared surgical complications, he refused and received 70 days of tigecycline plus daptomycin therapy, which was complicated only by nausea. He remained clinically well and had negative blood cultures 16 weeks after completion of therapy.
DISCUSSION
Tigecycline, the first available glycylcycline, is a minocycline‐derived antibiotic that remains active in the presence of the ribosomal modifications and efflux pumps that mediate tetracycline resistance. Thus, it possesses broad‐spectrum bacteriostatic activity, including activity against VRE. A PubMed search revealed no published data about the use of tigecycline for endocarditis in humans. However, tetracyclines have been used to treat endocarditis due to such organisms as Bartonella, Coxiella burnetti, or methicillin‐resistant Staphylococcus aureus (MRSA), frequently for prolonged courses. Tetracyclines were combined with other antibiotics in 5 published cases of VRE endocarditis. All patients survived; 3 were cured with the tetracycline regimen and 2 with other antimicrobials.1 In animal models of endocarditis, tigecycline stabilized vegetation counts of E. faecalis and reduced vegetation counts of MRSA and 1 strain of E. faecium.4
Daptomycin, the first available cyclic lipopeptide, kills by nonlytic depolarization of the bacterial cell membrane. In a recent study, daptomycin was non‐inferior to vancomycin or antistaphylococcal penicillins for S. aureus bacteremia or endocarditis. Although a few patients had left‐sided endocarditis, only 1 of them experienced a successful outcome with daptomycin therapy, and daptomycin displayed a trend toward higher rates of persistent or relapsing infection.5 Less evidence supports the use of daptomycin for serious enterococcal infections.2 One report noted the deaths of 6 of 10 patients treated with daptomycin for VRE bacteremia, including both patients with endocarditis.6 Daptomycin was used successfully in a case of VRE endocarditis in combination with gentamicin and rifampin for 11 weeks1 and at least 6 other reported cases of VRE bacteremia.7, 8
In summary, despite tigecycline's lack of bactericidal activity or proven efficacy in endocarditis, daptomycin's prior performance in VRE bacteremia, and the isolate's borderline daptomycin susceptibility, prolonged combination therapy resulted in a cure of VRE endocarditis. This success extends the experience with using both agents in the treatment of resistant infections. As linezolid‐resistant VRE and other resistant pathogens become more common, the need for research on treatment options becomes more urgent, and familiarity with novel and lesser‐used antibiotics becomes more crucial for hospitalists.
- ,.Endocarditis due to vancomycin‐resistant enterococci: case report and review of the literature.Clin Infect Dis.2005;41:1134–1142.
- ,.Approaches to vancomycin resistant enterococci.Curr Opin Infect Dis.2004;17:541–547.
- ,,, et al.Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis.Clin Infect Dis.2000;4:633–638.
- ,,, et al.Activity and diffusion of tigecycline (GAR‐936) in experimental enterococcal endocarditis.Antimicrob Agents Chemother.2003;47:216–222.
- ,,, et al.Daptomycin versus standard therapy for bacteremia and endocarditis caused by staphylococcus aureus.New Engl J Med.2006;355:653–665.
- ,,.Daptomycin for the treatment of gram‐positive bacteremia and infective endocarditis: a retrospective case series of 31 patients.Pharmacotherapy.2006;26:347–352.
- ,,,,.Daptomycin in the treatment of vancomycin‐resistant Enterococcus faecium bacteremia in neutropenic patients.J Infect.2007;54:567–571.
- ,,,,.Daptomycin for the treatment of vancomycin resistant Enterococcus faecium bacteremia.Scand J Infect Dis.2006;38:290–292.
- ,.Endocarditis due to vancomycin‐resistant enterococci: case report and review of the literature.Clin Infect Dis.2005;41:1134–1142.
- ,.Approaches to vancomycin resistant enterococci.Curr Opin Infect Dis.2004;17:541–547.
- ,,, et al.Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis.Clin Infect Dis.2000;4:633–638.
- ,,, et al.Activity and diffusion of tigecycline (GAR‐936) in experimental enterococcal endocarditis.Antimicrob Agents Chemother.2003;47:216–222.
- ,,, et al.Daptomycin versus standard therapy for bacteremia and endocarditis caused by staphylococcus aureus.New Engl J Med.2006;355:653–665.
- ,,.Daptomycin for the treatment of gram‐positive bacteremia and infective endocarditis: a retrospective case series of 31 patients.Pharmacotherapy.2006;26:347–352.
- ,,,,.Daptomycin in the treatment of vancomycin‐resistant Enterococcus faecium bacteremia in neutropenic patients.J Infect.2007;54:567–571.
- ,,,,.Daptomycin for the treatment of vancomycin resistant Enterococcus faecium bacteremia.Scand J Infect Dis.2006;38:290–292.
Fishing for a Diagnosis
A 54‐year‐old man with hypertension and type 2 diabetes mellitus entered the Chest Pain Evaluation Unit of a teaching hospital after 12 hours of intermittent thoracic discomfort. The pain began during dinner and was sharp, bandlike, and located beneath the sternum and across the entire chest. He had dyspnea but no diaphoresis or nausea. A recumbent position relieved the pain after dinner, but it recurred during the night and again the following morning. He did not smoke and had no family history of coronary artery disease.
A useful approach in evaluating acute chest pain is to employ a hierarchical differential diagnosis that emphasizes life‐threatening disorders requiring prompt recognition and intervention. Most prominent are cardiac ischemia, pericardial tamponade, pneumothorax, pulmonary embolus, esophageal rupture, and aortic dissection. The concurrent dyspnea and retrosternal location and intermittent nature of the pain that this patient has are consistent with myocardial ischemia, but the sharp quality of the pain and the relief gained by being recumbent are atypical. Pain with pericarditis is characteristically pleuritic and often worse when lying down. The pain of pneumothorax is typically unilateral, not intermittent, and unlikely to improve with recumbency. Although pain during eating suggests the possibility of an esophageal source, spontaneous rupture usually follows vomiting. The pain is typically continuous and severe. The pain of pulmonary embolism may be unilateral and pleuritic but often is more diffuse. Relief by recumbency is unusual, but the intermittent nature could suggest recurrent emboli. The patient has a history of hypertension, which predisposes him to aortic dissection, in which the pain is typically sharp, continuous, and severe but occasionally intermittent. Among numerous less urgent diagnoses are esophagitis and thoracic diabetic radiculopathy.
Important features to look for during this patient's examination include: disappearance of the radial pulse during inhalation, a simple screening test that is insensitive but very specific for pericardial tamponade; elevated neck veins, which can occur with tension pneumothorax, massive pulmonary embolism, and pericardial tamponade; pericardial and pleural friction rubs; discrepant blood pressures in the 2 arms, sometimes a sign of aortic dissection; local thoracic tenderness from chest wall disorders; and sensory examination of the chest surface, which is often abnormal in diabetic thoracic radiculopathy. Given this patient's age and history of diabetes, I am most concerned about myocardial ischemia. The most appropriate diagnostic tests include an electrocardiogram and a chest radiograph.
The patient appeared apprehensive but reported no pain. He had a temperature of 36.0 C, heart rate of 95 beats/minute, blood pressure of 138/77 mm Hg, respiratory rate of 16/minute, and oxygen saturation of 99% while breathing ambient air. Blood pressures were equal in both arms. Jugular venous distention was absent, and the lung and cardiac examinations had normal results. His pain did not increase on chest wall palpation. Examination of the abdomen, extremities, and the neurologic system showed normal results.
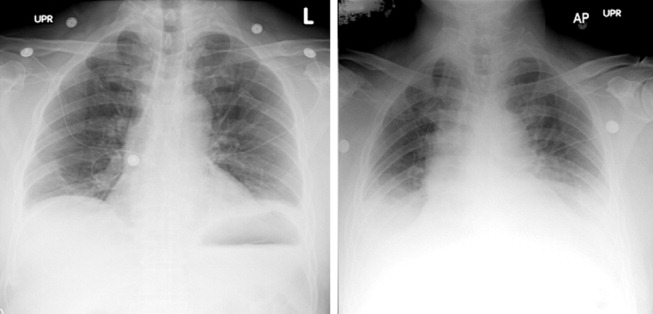
The results of laboratory tests showed a leukocyte count of 12,700/cm3, with 85% neutrophils, 8% lymphocytes, 6% monocytes, and 1% eosinophils. The hematocrit was 45%, and the platelet count was 172,000/cm3. The results of his chemistry panel were remarkable only for a glucose of 225 mg/dL. An electrocardiogram (ECG) showed a normal sinus rhythm and left anterior fascicular block without acute ST‐ or T‐wave changes. Prior ECGs were unavailable. An anteroposterior radiograph disclosed low lung volumes and bibasilar opacities. No pleural effusion was noted. Serial serum troponin and creatine kinase levels were normal. A Tc‐99m tetrofosmin cardiac nuclear perfusion test performed at rest demonstrated a moderate area of mildly decreased uptake along the inferior wall extending to the apex. An exercise treadmill test, terminated after 1 minute, 45 seconds because of chest pain, provoked no ECG changes diagnostic of ischemic disease.
The absence of elevated jugular venous pressure virtually eliminates pericardial tamponade as a diagnosis, and the chest film excludes pneumothorax. The intermittent nature of the chest pain, the absence on the chest radiograph of such findings as mediastinal gas, left pneumothorax, or hydropneumothorax, and the lack of a predisposing cause make esophageal rupture unlikely. Pulmonary emboli remain a consideration despite the normal oxygen saturation because there is no hypoxemia in a substantial minority of such cases. The normal cardiac enzyme levels and the lack of significant changes on the ECG exclude that a myocardial infarction has recently occurred, but cardiac ischemia remains a possibility, especially because the patient had chest pain on exercise and the nuclear scan indicated diminished blood flow to the inferior left ventricle. Aortic dissection still lurks as a possibility. The inferior wall abnormalities seen on the scan could result from dissection into the right coronary artery, which is more frequently involved than the left, or compression of it by an enlarged aorta, but they also may be artifacts. The leukocytosis may be a nonspecific response to stress but could indicate, although unlikely, infections such as mediastinitis from esophageal rupture or bacterial aortitis.
A conscientious clinician would repeat the history, reexamine the patient, and scrutinize the chest film to determine what the bilateral opacities represent. Given the story so far, however, I might consider a thoracic computed tomography (CT) angiogram because I am most concerned about pulmonary emboli and aortic dissection.
On hospital day 3, the patient had worsening dyspnea and persistent chest pain. His temperature was 39.3C, and his oxygen saturation decreased to 89% while breathing room air. Repeat chest radiography showed new bilateral pleural effusions and increased bibasilar opacification (Fig. 1). His leukocyte count was 19,000/cm3, with 88% neutrophils, 6% lymphocytes, 5% monocytes, and 1% eosinophils. Care was transferred from the chest pain team to an inpatient general medicine ward team. A pulmonary CT angiogram showed no large central clots but suggested emboli in the right superior subsegmental artery and a right upper lobe subsegmental artery. Bilateral pleural effusions were observed, as were bilateral pleural‐based atelectasis or infiltrates in the lower lungs. A hiatal hernia was noted, but no aortic dissection. The patient received supplemental oxygen, intravenous levofloxacin, and unfractionated heparin by continuous infusion.
Without other information, I will assume that the fever is part of the patient's original disease and not a nosocomial infection or drug fever. At this point, a crucial part of the evaluation is examining the CT scan with experienced radiologists to determine whether the abnormalities noted are genuinely convincing for pulmonary emboli. If the findings are equivocal, the next step might be a pulmonary angiogram or the indirect approach of evaluating the leg veins with ultrasound, reasoning that the presence of proximal leg vein thromboses would require anticoagulation in any event.
The patient's worsening chest pain and hypoxemia are consistent with multiple pulmonary emboli. Bilateral pleural effusions and leukocytosis can occur but are uncommon. Because of the fever, another possibility is septic pulmonary emboli, but he has no evidence of suppurative thrombophlebitis of the peripheral veins, apparent infection elsewhere, or previous intravenous drug abuse causing right‐sided endocarditis. An alternative diagnosis is infection of an initially bland pulmonary infarct.
An important consideration is a thoracentesis, depending on how persuasive the CT diagnosis of pulmonary embolism is and the size of the pleural effusions. It should be done before instituting antimicrobial therapy, which may decrease the yield of the cultures, and before starting heparin, which increases the risk of bleeding and occasionally causes a substantial, even fatal hemothorax.
The patient's oxygenation and dyspnea did not improve. Over the next day, he repeatedly mentioned that swallowing, particularly solid foods, worsened his chest pain. He had a temperature of 39.9C, a heart rate of 121 beats/minute, blood pressure of 149/94 mm Hg, a respiratory rate of 28/minute, and oxygen saturation of 93% while breathing 40% oxygen. He had inspiratory splinting, percussive dullness at both lung bases, and distant heart sounds. A contrast esophagogram showed distal narrowing that prevented solid contrast from passing, but no hiatal hernia. Blood and urine cultures obtained before antibiotic therapy were sterile. Duplex ultrasonography of bilateral lower extremities showed no evidence of deep venous thrombosis. A pulmonary angiogram revealed no emboli, and heparin was discontinued. Bilateral thoracentesis yielded grossly bloody fluid. Repeat chest CT (Fig. 2) demonstrated large bilateral effusions, a new large pericardial effusion, and a prominence at the gastroesophageal junction more concerning for a soft‐tissue mass than for a hiatal hernia, although the quality of the study was suboptimal because of an absence of oral contrast.

The CT scan suggests a paraesophageal abscess from an esophageal rupture. As mentioned earlier, if rupture occurs spontaneously, it typically follows retching or vomiting and is called Boerhaave's syndrome. Another consideration is a rupture secondary to an external insult, such as trauma or ingestion of a caustic substance. In evaluating these possibilities, the patient should have been asked 4 questions at the initial interview that I neglected to explicitly highlight earlier. First, what was he eating when he developed the chest pain? Second, did the pain begin during swallowing? Third, did he have previous symptoms suggesting an esophageal disorder such as dysphagia, odynophagia, or heartburn? These might indicate a cancer that could perforate or another problem such as a stricture or disordered esophageal motility that might have caused a swallowed item to lodge in the esophagus. Finally, did he have retching or vomiting? Though not routinely part of the review of systems, the former 2 questions are an appropriate history‐prompted line of questioning of a patient with onset of chest pain while eating.
At this point, a reasonable approach would be an esophagoscopy to delineate any intraluminal problems, such as a cancer or a foreign body. The apparent obstruction seen on barium swallow may be from extrinsic pressure from a paraesophageal abscess. The patient should receive broad‐spectrum antimicrobial therapy effective against oral anaerobes. Although occasionally patients recover with antibiotics alone, surgery is usually required. I am surprised that the original CT scan did not show evidence of an esophageal perforation. Possibly, the hiatal hernia was a paraesophageal abscess poorly characterized because of the lack of oral contrast.
The team, concerned about esophageal perforation, began the patient on intravenous clindamycin. The patient underwent video‐assisted thoracoscopic drainage, which yielded a moderate amount of turbid, bloody fluid from each hemithorax. The pericardium contained approximately 500 cm3 of turbid fluid. Gram stain and culture of these fluids were negative. No esophageal or mediastinal mass was noted during surgery. Intraoperative esophagogastroduodenoscopy with endoscopic ultrasound showed a healing linear mucosal tear in the distal esophagus (Fig. 3) as well as air/fluid collection in the esophageal soft tissue (not shown).

On further questioning postoperatively, the patient reported eating bony fish during the dinner when he first experienced chest pain. The patient received a 21‐day course of oral clindamycin and completely recovered. Five weeks later, a chest CT showed decreased distal esophageal thickening and no mediastinal air.
COMMENTARY
Esophageal perforation is an uncommon but life‐threatening cause of chest pain. In most series iatrogenic injury accounts for more than 70% of cases, whereas most of the other cases have spontaneous (5%20%) or traumatic (4%10%) causes (Table 1).14 Perforation as a complication of ingesting fish bones, although rare, is well described and continues to be reported.57
| Etiology | Percent |
|---|---|
| |
| Iatrogenic | 45%77% |
| Rigid or flexible endoscopy, balloon dilation, Blakemore tube, sclerotherapy, operative injury | |
| Increased intraesophageal pressure (Boerhaave's syndrome) | 5%20% |
| Vomiting or retching, weightlifting, childbirth | |
| Traumatic | 4%10% |
| Penetrating or blunt injury to neck or chest | |
| Ingestion | 0%12% |
| Foreign body, toxic or caustic substance | |
| Miscellaneous | 0%5% |
| Malignancy, Barrett's esophagus, infection, aortic dissection | |
Diagnosis of esophageal perforation secondary to a foreign body may be difficult because of the considerable overlap of symptoms with other causes of chest pain and failure to consider this infrequent condition in the absence of a classic history of retching. To diagnose such a disease, physicians must gather data from various sourcesespecially the history, physical examination, and medical recordformulate hypotheses, integrate results from diagnostic tests, and then assess the importance of the available information in the context of a differential diagnosis. Incorrectly evaluating or failing to obtain essential data can lead to incorrect or delayed diagnoses.
In This Patient's Evaluation, What Prevented Prompt Recognition of Esophageal Perforation?
The critical misstep was an incomplete history, both on arrival and when the patient was transferred to a second team. The presence of risk factors for coronary artery disease led the providers to first consider myocardial ischemia. They failed to ask crucial questions about the onset of the painwhen it occurred during the meal and what he was eatingeven when the patient later complained of odynophagia. As a result of the incomplete history, the providers, puzzled by the patient's ongoing and evolving symptoms, ordered numerous unnecessary diagnostic tests that gave false‐positive results, leading to potentially harmful treatment including anticoagulation. The discussant mentions that the preferred response to a puzzling clinical situation is to return to the bedside and repeat the history, reexamine the patient, and reevaluate available informationsimple steps that can often resolve diagnostic dilemmas.
There is ongoing concern that the history‐taking and physical examination skills of clinicians are in decline.814 Many speculate this is in part due to reliance on increasingly sophisticated diagnostic tests. Providers may overly rely on modern diagnostic tests because of their familiarity with the sensitivity and specificity of such tests, fear of malpractice litigation, diminishing opportunity to elucidate the complete history and physical exam, or lack of confidence in their history‐taking and examination skills.814 Although the rapid development and implementation of advanced diagnostic technologies have had a significant impact on diagnostic accuracy, the estimated rate of disease misdiagnosis remains elevated at 24%.1518 In contrast to technology‐based testing, the history and physical provide an inexpensive, safe, and effective means of at arriving at a correct diagnosis. In outpatient medical visits the history and physical, when completely elicited, result in a correct diagnosis of up to 70%90% of patients.8, 19, 20 Even for illnesses whose diagnosis requires confirmation by a diagnostic test, the definitive test can only be selected after a sufficient history and exam provide an assessment of the pretest probability of disease.
In evaluating chest pain there is an additional potential factor that diminishes reliance on bedside assessment. Modern quality assurance measures and chest pain units encourage clinicians to evaluate patients with chest pain quickly because any delay diminishes the benefits of therapies for acute coronary syndromes. In the emergency room, these patients find themselves on a rapidly moving diagnostic conveyor belt, an approach that is efficient and appropriate given the high prevalence of coronary disease but that also contributes to inattentiveness and error for patients with unusual diagnoses.
How Could Clinicians in Our Case Use Bedside Evidence to Help Differentiate Our Patient?
For most patients with chest pain there is no finding that would change diagnostic probabilities enough to take them off the diagnostic conveyor belt. Nevertheless, several bedside findings can help providers to rank‐order a differential diagnosis, thereby improving the sequence in which diagnostic testing is done. For patients with chest pain the ECG has the highest predictive ability of all studied history, physical exam, and ECG findings (Table 2).21 A history of sharp and positional pain descriptors diminishes the probability of myocardial ischemia.21 Unfortunately, no history, exam, or ECG feature is sensitive enough, either alone or in combination, to effectively rule out myocardial ischemia.
| Finding | Positive LR* |
|---|---|
| Myocardial ischemia | |
| ST segment elevation or Q wave | 22 |
| S3 gallop, blood pressure < 100 mm Hg, or ST segment depression | 3.0 |
| Sharp or positional pain | 0.3 |
| Pulmonary embolism | |
| Low clinical probability | 0.2 |
| Medium clinical probability | 1.8 |
| High clinical probability | 17.1 |
| Aortic dissection | |
| Tearing or ripping pain | 10.8 |
| Focal neurologic deficits | 6.633 |
| Ipsilateral versus contralateral pulse deficit | 5.7 |
| Cardiac tamponade | |
| Pulsus paradoxus > 12 mm Hg | 5.9 |
| Esophageal perforation | |
| Dysphagia, odynophagia, retching, vomiting, or subcutaneous emphysema | ? |
The history and exam can also facilitate differentiation of noncoronary causes of life‐threatening chest pain. The dismal performance of individual bedside findings for pulmonary embolism is what led to development of quantitative D‐dimer assays and objective methods based on bedside evaluation, including the widely used Wells Score.22 This score can be used to classify patients as having low, medium, and high risk of pulmonary embolism, facilitating management decisions after diagnostic imaging is obtained.23 Fewer than half of all patients with thoracic aortic dissection have classic exam findings; however, when present, they can appropriately raise the probability of dissection higher on the differential diagnosis.24 Importantly, no history or exam finding argues against dissection.24 Most patients with cardiac tamponade will have elevated jugular venous pressure (76%100%); however, poor interobserver agreement about this finding may decrease its detection.11, 25, 26 As the discussant notes, total paradox, defined as the palpable pulse disappearing with inspiration, is an insensitive test for tamponade, present in only 23% of patients with the disorder. In contrast, an inspiratory drop in systolic blood pressure of more than 12 mm Hg should prompt consideration for tamponade.11, 26 Commonly taught features of esophageal perforation, including chest pain, dysphagia, odynophagia, prior retching or vomiting, subcutaneous emphysema, dyspnea, and pleural effusions, vary in their reported sensitivity, but their specificity is virtually never reported.27
Like most patients with chest pain, our patient lacked all these symptoms and signs, arguing for myocardial ischemia, although he had a few signs that argued against it (sharp and positional chest pain). After the initial CXR and ECG, further testing with cardiac biomarkers was appropriate, but a fundamental error was made in not returning to the patient's bedside to repeat the interview and examination after the cardiac biomarkers were found to be normal. Had this been done, several cluesdysphagia, onset of pain with eating bony fish, and feverwould have pushed esophageal perforation to the top of the differential diagnosis. Subsequent testing would have led to the correct diagnosis and avoided a potentially harmful diagnostic fishing expedition.
Take‐Home Points
-
Esophageal perforation is an uncommon but life‐threatening cause of chest pain that is difficult to diagnose because of its nonspecific symptoms.
-
An accurate and complete history and exam can reveal signs and symptoms that influence the likelihood of each life‐threatening cause of chest pain. Evaluating patients for these features is vital to the rank ordering of a differential diagnosis and the selection of appropriate diagnostic tests.
-
There is no substitute for repeating the history, reexamining the patient, and reevaluating available information when confronted with a confusing constellation of symptoms.
Acknowledgements
The authors thank Steve McGee for his thoughtful review and comments on the manuscript.
- ,.Esophageal perforations: a 15 year experience.Am J Surg.1982;143:495–503.
- ,,.Esophageal perforation: emphasis on management.Ann Thorac Surg.1996;61:1447–1451; discussion1451–1452.
- ,,,,,.Evolving options in the management of esophageal perforation.Ann Thorac Surg.2004;77:1475–1783.
- ,.Personal management of 57 consecutive patients with esophageal perforation.Am J Surg.2004;187:58–63.
- ,,,,.Perforation of the oesophagus and aorta after eating fish: an unusual cause of chest pain.Emerg Med J.2003;20:385–386.
- ,,,.Esophageal perforation and mediastinitis from fish bone ingestion.South Med J.2003;96:516–520.
- ,,,.A 73‐year‐old man with chest pain 4 days after a fish dinner.Chest.2004;126:294–297.
- ,.The science of the art of the clinical examination.JAMA.1992;267:2650–2652.
- .Clinical skills in the 21st century.Arch Intern Med.1994;154:22–24.
- ,.Pulmonary auscultatory skills during training in internal medicine and family practice.Am J Respir Crit Care Med.1999;159:1119–1124.
- .Evidence‐Based Physical Diagnosis.Philadelphia, PA:Saunders;2001.
- .Simple is beautiful: the neglected power of simple tests.Arch Intern Med.2004;164:2198–2200.
- ,.Pearls and pitfalls in patient care: need to revive traditional clinical values.Am J Med Sci.2004;327:79–85.
- ,. Physical diagnosis: a lost art? Agency for Health Research and Quality. WebM75:29–40.
- .Low‐tech autopsies in the era of high‐tech medicine: continued value for quality assurance and patient safety.JAMA.1998;280:1273–1274.
- ,,,.Has misdiagnosis of appendicitis decreased over time? A population‐based analysis.JAMA.2001;286:1748–1753.
- ,,,.Changes in rates of autopsy‐detected diagnostic errors over time: a systematic review.JAMA.2003;289:2849–2856.
- .Diagnostic Process.J Coll Gen Pract.1963;54:579–589.
- .The importance of the history in the medical clinic and the cost of unnecessary tests.Am Heart J.1980;100:928–931.
- ,.Bedside diagnosis of coronary artery disease: a systematic review.Am J Med.2004;117:334–343.
- ,,, et al.Use of a clinical model for safe management of patients with suspected pulmonary embolism.Ann Intern Med.1998;129:997–1005.
- ,,, et al.Diagnostic pathways in acute pulmonary embolism: recommendations of the PIOPED II investigators.Am J Med.2006;119:1048–1055.
- .Does this patient have an acute thoracic aortic dissection?JAMA.2002;287:2262–2272.
- ,.The rational clinical examination. Does this patient have abnormal central venous pressure?JAMA.1996;275:630–634.
- ,,,.Does this patient with a pericardial effusion have cardiac tamponade?JAMA.2007;297:1810–1818.
- ,.Spontaneous esophageal rupture: a frequently missed diagnosis.Am Surg.1999;65:449–452.
A 54‐year‐old man with hypertension and type 2 diabetes mellitus entered the Chest Pain Evaluation Unit of a teaching hospital after 12 hours of intermittent thoracic discomfort. The pain began during dinner and was sharp, bandlike, and located beneath the sternum and across the entire chest. He had dyspnea but no diaphoresis or nausea. A recumbent position relieved the pain after dinner, but it recurred during the night and again the following morning. He did not smoke and had no family history of coronary artery disease.
A useful approach in evaluating acute chest pain is to employ a hierarchical differential diagnosis that emphasizes life‐threatening disorders requiring prompt recognition and intervention. Most prominent are cardiac ischemia, pericardial tamponade, pneumothorax, pulmonary embolus, esophageal rupture, and aortic dissection. The concurrent dyspnea and retrosternal location and intermittent nature of the pain that this patient has are consistent with myocardial ischemia, but the sharp quality of the pain and the relief gained by being recumbent are atypical. Pain with pericarditis is characteristically pleuritic and often worse when lying down. The pain of pneumothorax is typically unilateral, not intermittent, and unlikely to improve with recumbency. Although pain during eating suggests the possibility of an esophageal source, spontaneous rupture usually follows vomiting. The pain is typically continuous and severe. The pain of pulmonary embolism may be unilateral and pleuritic but often is more diffuse. Relief by recumbency is unusual, but the intermittent nature could suggest recurrent emboli. The patient has a history of hypertension, which predisposes him to aortic dissection, in which the pain is typically sharp, continuous, and severe but occasionally intermittent. Among numerous less urgent diagnoses are esophagitis and thoracic diabetic radiculopathy.
Important features to look for during this patient's examination include: disappearance of the radial pulse during inhalation, a simple screening test that is insensitive but very specific for pericardial tamponade; elevated neck veins, which can occur with tension pneumothorax, massive pulmonary embolism, and pericardial tamponade; pericardial and pleural friction rubs; discrepant blood pressures in the 2 arms, sometimes a sign of aortic dissection; local thoracic tenderness from chest wall disorders; and sensory examination of the chest surface, which is often abnormal in diabetic thoracic radiculopathy. Given this patient's age and history of diabetes, I am most concerned about myocardial ischemia. The most appropriate diagnostic tests include an electrocardiogram and a chest radiograph.
The patient appeared apprehensive but reported no pain. He had a temperature of 36.0 C, heart rate of 95 beats/minute, blood pressure of 138/77 mm Hg, respiratory rate of 16/minute, and oxygen saturation of 99% while breathing ambient air. Blood pressures were equal in both arms. Jugular venous distention was absent, and the lung and cardiac examinations had normal results. His pain did not increase on chest wall palpation. Examination of the abdomen, extremities, and the neurologic system showed normal results.
The results of laboratory tests showed a leukocyte count of 12,700/cm3, with 85% neutrophils, 8% lymphocytes, 6% monocytes, and 1% eosinophils. The hematocrit was 45%, and the platelet count was 172,000/cm3. The results of his chemistry panel were remarkable only for a glucose of 225 mg/dL. An electrocardiogram (ECG) showed a normal sinus rhythm and left anterior fascicular block without acute ST‐ or T‐wave changes. Prior ECGs were unavailable. An anteroposterior radiograph disclosed low lung volumes and bibasilar opacities. No pleural effusion was noted. Serial serum troponin and creatine kinase levels were normal. A Tc‐99m tetrofosmin cardiac nuclear perfusion test performed at rest demonstrated a moderate area of mildly decreased uptake along the inferior wall extending to the apex. An exercise treadmill test, terminated after 1 minute, 45 seconds because of chest pain, provoked no ECG changes diagnostic of ischemic disease.
The absence of elevated jugular venous pressure virtually eliminates pericardial tamponade as a diagnosis, and the chest film excludes pneumothorax. The intermittent nature of the chest pain, the absence on the chest radiograph of such findings as mediastinal gas, left pneumothorax, or hydropneumothorax, and the lack of a predisposing cause make esophageal rupture unlikely. Pulmonary emboli remain a consideration despite the normal oxygen saturation because there is no hypoxemia in a substantial minority of such cases. The normal cardiac enzyme levels and the lack of significant changes on the ECG exclude that a myocardial infarction has recently occurred, but cardiac ischemia remains a possibility, especially because the patient had chest pain on exercise and the nuclear scan indicated diminished blood flow to the inferior left ventricle. Aortic dissection still lurks as a possibility. The inferior wall abnormalities seen on the scan could result from dissection into the right coronary artery, which is more frequently involved than the left, or compression of it by an enlarged aorta, but they also may be artifacts. The leukocytosis may be a nonspecific response to stress but could indicate, although unlikely, infections such as mediastinitis from esophageal rupture or bacterial aortitis.
A conscientious clinician would repeat the history, reexamine the patient, and scrutinize the chest film to determine what the bilateral opacities represent. Given the story so far, however, I might consider a thoracic computed tomography (CT) angiogram because I am most concerned about pulmonary emboli and aortic dissection.
On hospital day 3, the patient had worsening dyspnea and persistent chest pain. His temperature was 39.3C, and his oxygen saturation decreased to 89% while breathing room air. Repeat chest radiography showed new bilateral pleural effusions and increased bibasilar opacification (Fig. 1). His leukocyte count was 19,000/cm3, with 88% neutrophils, 6% lymphocytes, 5% monocytes, and 1% eosinophils. Care was transferred from the chest pain team to an inpatient general medicine ward team. A pulmonary CT angiogram showed no large central clots but suggested emboli in the right superior subsegmental artery and a right upper lobe subsegmental artery. Bilateral pleural effusions were observed, as were bilateral pleural‐based atelectasis or infiltrates in the lower lungs. A hiatal hernia was noted, but no aortic dissection. The patient received supplemental oxygen, intravenous levofloxacin, and unfractionated heparin by continuous infusion.
Without other information, I will assume that the fever is part of the patient's original disease and not a nosocomial infection or drug fever. At this point, a crucial part of the evaluation is examining the CT scan with experienced radiologists to determine whether the abnormalities noted are genuinely convincing for pulmonary emboli. If the findings are equivocal, the next step might be a pulmonary angiogram or the indirect approach of evaluating the leg veins with ultrasound, reasoning that the presence of proximal leg vein thromboses would require anticoagulation in any event.
The patient's worsening chest pain and hypoxemia are consistent with multiple pulmonary emboli. Bilateral pleural effusions and leukocytosis can occur but are uncommon. Because of the fever, another possibility is septic pulmonary emboli, but he has no evidence of suppurative thrombophlebitis of the peripheral veins, apparent infection elsewhere, or previous intravenous drug abuse causing right‐sided endocarditis. An alternative diagnosis is infection of an initially bland pulmonary infarct.
An important consideration is a thoracentesis, depending on how persuasive the CT diagnosis of pulmonary embolism is and the size of the pleural effusions. It should be done before instituting antimicrobial therapy, which may decrease the yield of the cultures, and before starting heparin, which increases the risk of bleeding and occasionally causes a substantial, even fatal hemothorax.
The patient's oxygenation and dyspnea did not improve. Over the next day, he repeatedly mentioned that swallowing, particularly solid foods, worsened his chest pain. He had a temperature of 39.9C, a heart rate of 121 beats/minute, blood pressure of 149/94 mm Hg, a respiratory rate of 28/minute, and oxygen saturation of 93% while breathing 40% oxygen. He had inspiratory splinting, percussive dullness at both lung bases, and distant heart sounds. A contrast esophagogram showed distal narrowing that prevented solid contrast from passing, but no hiatal hernia. Blood and urine cultures obtained before antibiotic therapy were sterile. Duplex ultrasonography of bilateral lower extremities showed no evidence of deep venous thrombosis. A pulmonary angiogram revealed no emboli, and heparin was discontinued. Bilateral thoracentesis yielded grossly bloody fluid. Repeat chest CT (Fig. 2) demonstrated large bilateral effusions, a new large pericardial effusion, and a prominence at the gastroesophageal junction more concerning for a soft‐tissue mass than for a hiatal hernia, although the quality of the study was suboptimal because of an absence of oral contrast.
The CT scan suggests a paraesophageal abscess from an esophageal rupture. As mentioned earlier, if rupture occurs spontaneously, it typically follows retching or vomiting and is called Boerhaave's syndrome. Another consideration is a rupture secondary to an external insult, such as trauma or ingestion of a caustic substance. In evaluating these possibilities, the patient should have been asked 4 questions at the initial interview that I neglected to explicitly highlight earlier. First, what was he eating when he developed the chest pain? Second, did the pain begin during swallowing? Third, did he have previous symptoms suggesting an esophageal disorder such as dysphagia, odynophagia, or heartburn? These might indicate a cancer that could perforate or another problem such as a stricture or disordered esophageal motility that might have caused a swallowed item to lodge in the esophagus. Finally, did he have retching or vomiting? Though not routinely part of the review of systems, the former 2 questions are an appropriate history‐prompted line of questioning of a patient with onset of chest pain while eating.
At this point, a reasonable approach would be an esophagoscopy to delineate any intraluminal problems, such as a cancer or a foreign body. The apparent obstruction seen on barium swallow may be from extrinsic pressure from a paraesophageal abscess. The patient should receive broad‐spectrum antimicrobial therapy effective against oral anaerobes. Although occasionally patients recover with antibiotics alone, surgery is usually required. I am surprised that the original CT scan did not show evidence of an esophageal perforation. Possibly, the hiatal hernia was a paraesophageal abscess poorly characterized because of the lack of oral contrast.
The team, concerned about esophageal perforation, began the patient on intravenous clindamycin. The patient underwent video‐assisted thoracoscopic drainage, which yielded a moderate amount of turbid, bloody fluid from each hemithorax. The pericardium contained approximately 500 cm3 of turbid fluid. Gram stain and culture of these fluids were negative. No esophageal or mediastinal mass was noted during surgery. Intraoperative esophagogastroduodenoscopy with endoscopic ultrasound showed a healing linear mucosal tear in the distal esophagus (Fig. 3) as well as air/fluid collection in the esophageal soft tissue (not shown).
On further questioning postoperatively, the patient reported eating bony fish during the dinner when he first experienced chest pain. The patient received a 21‐day course of oral clindamycin and completely recovered. Five weeks later, a chest CT showed decreased distal esophageal thickening and no mediastinal air.
COMMENTARY
Esophageal perforation is an uncommon but life‐threatening cause of chest pain. In most series iatrogenic injury accounts for more than 70% of cases, whereas most of the other cases have spontaneous (5%20%) or traumatic (4%10%) causes (Table 1).14 Perforation as a complication of ingesting fish bones, although rare, is well described and continues to be reported.57
| Etiology | Percent |
|---|---|
| |
| Iatrogenic | 45%77% |
| Rigid or flexible endoscopy, balloon dilation, Blakemore tube, sclerotherapy, operative injury | |
| Increased intraesophageal pressure (Boerhaave's syndrome) | 5%20% |
| Vomiting or retching, weightlifting, childbirth | |
| Traumatic | 4%10% |
| Penetrating or blunt injury to neck or chest | |
| Ingestion | 0%12% |
| Foreign body, toxic or caustic substance | |
| Miscellaneous | 0%5% |
| Malignancy, Barrett's esophagus, infection, aortic dissection | |
Diagnosis of esophageal perforation secondary to a foreign body may be difficult because of the considerable overlap of symptoms with other causes of chest pain and failure to consider this infrequent condition in the absence of a classic history of retching. To diagnose such a disease, physicians must gather data from various sourcesespecially the history, physical examination, and medical recordformulate hypotheses, integrate results from diagnostic tests, and then assess the importance of the available information in the context of a differential diagnosis. Incorrectly evaluating or failing to obtain essential data can lead to incorrect or delayed diagnoses.
In This Patient's Evaluation, What Prevented Prompt Recognition of Esophageal Perforation?
The critical misstep was an incomplete history, both on arrival and when the patient was transferred to a second team. The presence of risk factors for coronary artery disease led the providers to first consider myocardial ischemia. They failed to ask crucial questions about the onset of the painwhen it occurred during the meal and what he was eatingeven when the patient later complained of odynophagia. As a result of the incomplete history, the providers, puzzled by the patient's ongoing and evolving symptoms, ordered numerous unnecessary diagnostic tests that gave false‐positive results, leading to potentially harmful treatment including anticoagulation. The discussant mentions that the preferred response to a puzzling clinical situation is to return to the bedside and repeat the history, reexamine the patient, and reevaluate available informationsimple steps that can often resolve diagnostic dilemmas.
There is ongoing concern that the history‐taking and physical examination skills of clinicians are in decline.814 Many speculate this is in part due to reliance on increasingly sophisticated diagnostic tests. Providers may overly rely on modern diagnostic tests because of their familiarity with the sensitivity and specificity of such tests, fear of malpractice litigation, diminishing opportunity to elucidate the complete history and physical exam, or lack of confidence in their history‐taking and examination skills.814 Although the rapid development and implementation of advanced diagnostic technologies have had a significant impact on diagnostic accuracy, the estimated rate of disease misdiagnosis remains elevated at 24%.1518 In contrast to technology‐based testing, the history and physical provide an inexpensive, safe, and effective means of at arriving at a correct diagnosis. In outpatient medical visits the history and physical, when completely elicited, result in a correct diagnosis of up to 70%90% of patients.8, 19, 20 Even for illnesses whose diagnosis requires confirmation by a diagnostic test, the definitive test can only be selected after a sufficient history and exam provide an assessment of the pretest probability of disease.
In evaluating chest pain there is an additional potential factor that diminishes reliance on bedside assessment. Modern quality assurance measures and chest pain units encourage clinicians to evaluate patients with chest pain quickly because any delay diminishes the benefits of therapies for acute coronary syndromes. In the emergency room, these patients find themselves on a rapidly moving diagnostic conveyor belt, an approach that is efficient and appropriate given the high prevalence of coronary disease but that also contributes to inattentiveness and error for patients with unusual diagnoses.
How Could Clinicians in Our Case Use Bedside Evidence to Help Differentiate Our Patient?
For most patients with chest pain there is no finding that would change diagnostic probabilities enough to take them off the diagnostic conveyor belt. Nevertheless, several bedside findings can help providers to rank‐order a differential diagnosis, thereby improving the sequence in which diagnostic testing is done. For patients with chest pain the ECG has the highest predictive ability of all studied history, physical exam, and ECG findings (Table 2).21 A history of sharp and positional pain descriptors diminishes the probability of myocardial ischemia.21 Unfortunately, no history, exam, or ECG feature is sensitive enough, either alone or in combination, to effectively rule out myocardial ischemia.
| Finding | Positive LR* |
|---|---|
| Myocardial ischemia | |
| ST segment elevation or Q wave | 22 |
| S3 gallop, blood pressure < 100 mm Hg, or ST segment depression | 3.0 |
| Sharp or positional pain | 0.3 |
| Pulmonary embolism | |
| Low clinical probability | 0.2 |
| Medium clinical probability | 1.8 |
| High clinical probability | 17.1 |
| Aortic dissection | |
| Tearing or ripping pain | 10.8 |
| Focal neurologic deficits | 6.633 |
| Ipsilateral versus contralateral pulse deficit | 5.7 |
| Cardiac tamponade | |
| Pulsus paradoxus > 12 mm Hg | 5.9 |
| Esophageal perforation | |
| Dysphagia, odynophagia, retching, vomiting, or subcutaneous emphysema | ? |
The history and exam can also facilitate differentiation of noncoronary causes of life‐threatening chest pain. The dismal performance of individual bedside findings for pulmonary embolism is what led to development of quantitative D‐dimer assays and objective methods based on bedside evaluation, including the widely used Wells Score.22 This score can be used to classify patients as having low, medium, and high risk of pulmonary embolism, facilitating management decisions after diagnostic imaging is obtained.23 Fewer than half of all patients with thoracic aortic dissection have classic exam findings; however, when present, they can appropriately raise the probability of dissection higher on the differential diagnosis.24 Importantly, no history or exam finding argues against dissection.24 Most patients with cardiac tamponade will have elevated jugular venous pressure (76%100%); however, poor interobserver agreement about this finding may decrease its detection.11, 25, 26 As the discussant notes, total paradox, defined as the palpable pulse disappearing with inspiration, is an insensitive test for tamponade, present in only 23% of patients with the disorder. In contrast, an inspiratory drop in systolic blood pressure of more than 12 mm Hg should prompt consideration for tamponade.11, 26 Commonly taught features of esophageal perforation, including chest pain, dysphagia, odynophagia, prior retching or vomiting, subcutaneous emphysema, dyspnea, and pleural effusions, vary in their reported sensitivity, but their specificity is virtually never reported.27
Like most patients with chest pain, our patient lacked all these symptoms and signs, arguing for myocardial ischemia, although he had a few signs that argued against it (sharp and positional chest pain). After the initial CXR and ECG, further testing with cardiac biomarkers was appropriate, but a fundamental error was made in not returning to the patient's bedside to repeat the interview and examination after the cardiac biomarkers were found to be normal. Had this been done, several cluesdysphagia, onset of pain with eating bony fish, and feverwould have pushed esophageal perforation to the top of the differential diagnosis. Subsequent testing would have led to the correct diagnosis and avoided a potentially harmful diagnostic fishing expedition.
Take‐Home Points
-
Esophageal perforation is an uncommon but life‐threatening cause of chest pain that is difficult to diagnose because of its nonspecific symptoms.
-
An accurate and complete history and exam can reveal signs and symptoms that influence the likelihood of each life‐threatening cause of chest pain. Evaluating patients for these features is vital to the rank ordering of a differential diagnosis and the selection of appropriate diagnostic tests.
-
There is no substitute for repeating the history, reexamining the patient, and reevaluating available information when confronted with a confusing constellation of symptoms.
Acknowledgements
The authors thank Steve McGee for his thoughtful review and comments on the manuscript.
A 54‐year‐old man with hypertension and type 2 diabetes mellitus entered the Chest Pain Evaluation Unit of a teaching hospital after 12 hours of intermittent thoracic discomfort. The pain began during dinner and was sharp, bandlike, and located beneath the sternum and across the entire chest. He had dyspnea but no diaphoresis or nausea. A recumbent position relieved the pain after dinner, but it recurred during the night and again the following morning. He did not smoke and had no family history of coronary artery disease.
A useful approach in evaluating acute chest pain is to employ a hierarchical differential diagnosis that emphasizes life‐threatening disorders requiring prompt recognition and intervention. Most prominent are cardiac ischemia, pericardial tamponade, pneumothorax, pulmonary embolus, esophageal rupture, and aortic dissection. The concurrent dyspnea and retrosternal location and intermittent nature of the pain that this patient has are consistent with myocardial ischemia, but the sharp quality of the pain and the relief gained by being recumbent are atypical. Pain with pericarditis is characteristically pleuritic and often worse when lying down. The pain of pneumothorax is typically unilateral, not intermittent, and unlikely to improve with recumbency. Although pain during eating suggests the possibility of an esophageal source, spontaneous rupture usually follows vomiting. The pain is typically continuous and severe. The pain of pulmonary embolism may be unilateral and pleuritic but often is more diffuse. Relief by recumbency is unusual, but the intermittent nature could suggest recurrent emboli. The patient has a history of hypertension, which predisposes him to aortic dissection, in which the pain is typically sharp, continuous, and severe but occasionally intermittent. Among numerous less urgent diagnoses are esophagitis and thoracic diabetic radiculopathy.
Important features to look for during this patient's examination include: disappearance of the radial pulse during inhalation, a simple screening test that is insensitive but very specific for pericardial tamponade; elevated neck veins, which can occur with tension pneumothorax, massive pulmonary embolism, and pericardial tamponade; pericardial and pleural friction rubs; discrepant blood pressures in the 2 arms, sometimes a sign of aortic dissection; local thoracic tenderness from chest wall disorders; and sensory examination of the chest surface, which is often abnormal in diabetic thoracic radiculopathy. Given this patient's age and history of diabetes, I am most concerned about myocardial ischemia. The most appropriate diagnostic tests include an electrocardiogram and a chest radiograph.
The patient appeared apprehensive but reported no pain. He had a temperature of 36.0 C, heart rate of 95 beats/minute, blood pressure of 138/77 mm Hg, respiratory rate of 16/minute, and oxygen saturation of 99% while breathing ambient air. Blood pressures were equal in both arms. Jugular venous distention was absent, and the lung and cardiac examinations had normal results. His pain did not increase on chest wall palpation. Examination of the abdomen, extremities, and the neurologic system showed normal results.
The results of laboratory tests showed a leukocyte count of 12,700/cm3, with 85% neutrophils, 8% lymphocytes, 6% monocytes, and 1% eosinophils. The hematocrit was 45%, and the platelet count was 172,000/cm3. The results of his chemistry panel were remarkable only for a glucose of 225 mg/dL. An electrocardiogram (ECG) showed a normal sinus rhythm and left anterior fascicular block without acute ST‐ or T‐wave changes. Prior ECGs were unavailable. An anteroposterior radiograph disclosed low lung volumes and bibasilar opacities. No pleural effusion was noted. Serial serum troponin and creatine kinase levels were normal. A Tc‐99m tetrofosmin cardiac nuclear perfusion test performed at rest demonstrated a moderate area of mildly decreased uptake along the inferior wall extending to the apex. An exercise treadmill test, terminated after 1 minute, 45 seconds because of chest pain, provoked no ECG changes diagnostic of ischemic disease.
The absence of elevated jugular venous pressure virtually eliminates pericardial tamponade as a diagnosis, and the chest film excludes pneumothorax. The intermittent nature of the chest pain, the absence on the chest radiograph of such findings as mediastinal gas, left pneumothorax, or hydropneumothorax, and the lack of a predisposing cause make esophageal rupture unlikely. Pulmonary emboli remain a consideration despite the normal oxygen saturation because there is no hypoxemia in a substantial minority of such cases. The normal cardiac enzyme levels and the lack of significant changes on the ECG exclude that a myocardial infarction has recently occurred, but cardiac ischemia remains a possibility, especially because the patient had chest pain on exercise and the nuclear scan indicated diminished blood flow to the inferior left ventricle. Aortic dissection still lurks as a possibility. The inferior wall abnormalities seen on the scan could result from dissection into the right coronary artery, which is more frequently involved than the left, or compression of it by an enlarged aorta, but they also may be artifacts. The leukocytosis may be a nonspecific response to stress but could indicate, although unlikely, infections such as mediastinitis from esophageal rupture or bacterial aortitis.
A conscientious clinician would repeat the history, reexamine the patient, and scrutinize the chest film to determine what the bilateral opacities represent. Given the story so far, however, I might consider a thoracic computed tomography (CT) angiogram because I am most concerned about pulmonary emboli and aortic dissection.
On hospital day 3, the patient had worsening dyspnea and persistent chest pain. His temperature was 39.3C, and his oxygen saturation decreased to 89% while breathing room air. Repeat chest radiography showed new bilateral pleural effusions and increased bibasilar opacification (Fig. 1). His leukocyte count was 19,000/cm3, with 88% neutrophils, 6% lymphocytes, 5% monocytes, and 1% eosinophils. Care was transferred from the chest pain team to an inpatient general medicine ward team. A pulmonary CT angiogram showed no large central clots but suggested emboli in the right superior subsegmental artery and a right upper lobe subsegmental artery. Bilateral pleural effusions were observed, as were bilateral pleural‐based atelectasis or infiltrates in the lower lungs. A hiatal hernia was noted, but no aortic dissection. The patient received supplemental oxygen, intravenous levofloxacin, and unfractionated heparin by continuous infusion.
Without other information, I will assume that the fever is part of the patient's original disease and not a nosocomial infection or drug fever. At this point, a crucial part of the evaluation is examining the CT scan with experienced radiologists to determine whether the abnormalities noted are genuinely convincing for pulmonary emboli. If the findings are equivocal, the next step might be a pulmonary angiogram or the indirect approach of evaluating the leg veins with ultrasound, reasoning that the presence of proximal leg vein thromboses would require anticoagulation in any event.
The patient's worsening chest pain and hypoxemia are consistent with multiple pulmonary emboli. Bilateral pleural effusions and leukocytosis can occur but are uncommon. Because of the fever, another possibility is septic pulmonary emboli, but he has no evidence of suppurative thrombophlebitis of the peripheral veins, apparent infection elsewhere, or previous intravenous drug abuse causing right‐sided endocarditis. An alternative diagnosis is infection of an initially bland pulmonary infarct.
An important consideration is a thoracentesis, depending on how persuasive the CT diagnosis of pulmonary embolism is and the size of the pleural effusions. It should be done before instituting antimicrobial therapy, which may decrease the yield of the cultures, and before starting heparin, which increases the risk of bleeding and occasionally causes a substantial, even fatal hemothorax.
The patient's oxygenation and dyspnea did not improve. Over the next day, he repeatedly mentioned that swallowing, particularly solid foods, worsened his chest pain. He had a temperature of 39.9C, a heart rate of 121 beats/minute, blood pressure of 149/94 mm Hg, a respiratory rate of 28/minute, and oxygen saturation of 93% while breathing 40% oxygen. He had inspiratory splinting, percussive dullness at both lung bases, and distant heart sounds. A contrast esophagogram showed distal narrowing that prevented solid contrast from passing, but no hiatal hernia. Blood and urine cultures obtained before antibiotic therapy were sterile. Duplex ultrasonography of bilateral lower extremities showed no evidence of deep venous thrombosis. A pulmonary angiogram revealed no emboli, and heparin was discontinued. Bilateral thoracentesis yielded grossly bloody fluid. Repeat chest CT (Fig. 2) demonstrated large bilateral effusions, a new large pericardial effusion, and a prominence at the gastroesophageal junction more concerning for a soft‐tissue mass than for a hiatal hernia, although the quality of the study was suboptimal because of an absence of oral contrast.
The CT scan suggests a paraesophageal abscess from an esophageal rupture. As mentioned earlier, if rupture occurs spontaneously, it typically follows retching or vomiting and is called Boerhaave's syndrome. Another consideration is a rupture secondary to an external insult, such as trauma or ingestion of a caustic substance. In evaluating these possibilities, the patient should have been asked 4 questions at the initial interview that I neglected to explicitly highlight earlier. First, what was he eating when he developed the chest pain? Second, did the pain begin during swallowing? Third, did he have previous symptoms suggesting an esophageal disorder such as dysphagia, odynophagia, or heartburn? These might indicate a cancer that could perforate or another problem such as a stricture or disordered esophageal motility that might have caused a swallowed item to lodge in the esophagus. Finally, did he have retching or vomiting? Though not routinely part of the review of systems, the former 2 questions are an appropriate history‐prompted line of questioning of a patient with onset of chest pain while eating.
At this point, a reasonable approach would be an esophagoscopy to delineate any intraluminal problems, such as a cancer or a foreign body. The apparent obstruction seen on barium swallow may be from extrinsic pressure from a paraesophageal abscess. The patient should receive broad‐spectrum antimicrobial therapy effective against oral anaerobes. Although occasionally patients recover with antibiotics alone, surgery is usually required. I am surprised that the original CT scan did not show evidence of an esophageal perforation. Possibly, the hiatal hernia was a paraesophageal abscess poorly characterized because of the lack of oral contrast.
The team, concerned about esophageal perforation, began the patient on intravenous clindamycin. The patient underwent video‐assisted thoracoscopic drainage, which yielded a moderate amount of turbid, bloody fluid from each hemithorax. The pericardium contained approximately 500 cm3 of turbid fluid. Gram stain and culture of these fluids were negative. No esophageal or mediastinal mass was noted during surgery. Intraoperative esophagogastroduodenoscopy with endoscopic ultrasound showed a healing linear mucosal tear in the distal esophagus (Fig. 3) as well as air/fluid collection in the esophageal soft tissue (not shown).
On further questioning postoperatively, the patient reported eating bony fish during the dinner when he first experienced chest pain. The patient received a 21‐day course of oral clindamycin and completely recovered. Five weeks later, a chest CT showed decreased distal esophageal thickening and no mediastinal air.
COMMENTARY
Esophageal perforation is an uncommon but life‐threatening cause of chest pain. In most series iatrogenic injury accounts for more than 70% of cases, whereas most of the other cases have spontaneous (5%20%) or traumatic (4%10%) causes (Table 1).14 Perforation as a complication of ingesting fish bones, although rare, is well described and continues to be reported.57
| Etiology | Percent |
|---|---|
| |
| Iatrogenic | 45%77% |
| Rigid or flexible endoscopy, balloon dilation, Blakemore tube, sclerotherapy, operative injury | |
| Increased intraesophageal pressure (Boerhaave's syndrome) | 5%20% |
| Vomiting or retching, weightlifting, childbirth | |
| Traumatic | 4%10% |
| Penetrating or blunt injury to neck or chest | |
| Ingestion | 0%12% |
| Foreign body, toxic or caustic substance | |
| Miscellaneous | 0%5% |
| Malignancy, Barrett's esophagus, infection, aortic dissection | |
Diagnosis of esophageal perforation secondary to a foreign body may be difficult because of the considerable overlap of symptoms with other causes of chest pain and failure to consider this infrequent condition in the absence of a classic history of retching. To diagnose such a disease, physicians must gather data from various sourcesespecially the history, physical examination, and medical recordformulate hypotheses, integrate results from diagnostic tests, and then assess the importance of the available information in the context of a differential diagnosis. Incorrectly evaluating or failing to obtain essential data can lead to incorrect or delayed diagnoses.
In This Patient's Evaluation, What Prevented Prompt Recognition of Esophageal Perforation?
The critical misstep was an incomplete history, both on arrival and when the patient was transferred to a second team. The presence of risk factors for coronary artery disease led the providers to first consider myocardial ischemia. They failed to ask crucial questions about the onset of the painwhen it occurred during the meal and what he was eatingeven when the patient later complained of odynophagia. As a result of the incomplete history, the providers, puzzled by the patient's ongoing and evolving symptoms, ordered numerous unnecessary diagnostic tests that gave false‐positive results, leading to potentially harmful treatment including anticoagulation. The discussant mentions that the preferred response to a puzzling clinical situation is to return to the bedside and repeat the history, reexamine the patient, and reevaluate available informationsimple steps that can often resolve diagnostic dilemmas.
There is ongoing concern that the history‐taking and physical examination skills of clinicians are in decline.814 Many speculate this is in part due to reliance on increasingly sophisticated diagnostic tests. Providers may overly rely on modern diagnostic tests because of their familiarity with the sensitivity and specificity of such tests, fear of malpractice litigation, diminishing opportunity to elucidate the complete history and physical exam, or lack of confidence in their history‐taking and examination skills.814 Although the rapid development and implementation of advanced diagnostic technologies have had a significant impact on diagnostic accuracy, the estimated rate of disease misdiagnosis remains elevated at 24%.1518 In contrast to technology‐based testing, the history and physical provide an inexpensive, safe, and effective means of at arriving at a correct diagnosis. In outpatient medical visits the history and physical, when completely elicited, result in a correct diagnosis of up to 70%90% of patients.8, 19, 20 Even for illnesses whose diagnosis requires confirmation by a diagnostic test, the definitive test can only be selected after a sufficient history and exam provide an assessment of the pretest probability of disease.
In evaluating chest pain there is an additional potential factor that diminishes reliance on bedside assessment. Modern quality assurance measures and chest pain units encourage clinicians to evaluate patients with chest pain quickly because any delay diminishes the benefits of therapies for acute coronary syndromes. In the emergency room, these patients find themselves on a rapidly moving diagnostic conveyor belt, an approach that is efficient and appropriate given the high prevalence of coronary disease but that also contributes to inattentiveness and error for patients with unusual diagnoses.
How Could Clinicians in Our Case Use Bedside Evidence to Help Differentiate Our Patient?
For most patients with chest pain there is no finding that would change diagnostic probabilities enough to take them off the diagnostic conveyor belt. Nevertheless, several bedside findings can help providers to rank‐order a differential diagnosis, thereby improving the sequence in which diagnostic testing is done. For patients with chest pain the ECG has the highest predictive ability of all studied history, physical exam, and ECG findings (Table 2).21 A history of sharp and positional pain descriptors diminishes the probability of myocardial ischemia.21 Unfortunately, no history, exam, or ECG feature is sensitive enough, either alone or in combination, to effectively rule out myocardial ischemia.
| Finding | Positive LR* |
|---|---|
| Myocardial ischemia | |
| ST segment elevation or Q wave | 22 |
| S3 gallop, blood pressure < 100 mm Hg, or ST segment depression | 3.0 |
| Sharp or positional pain | 0.3 |
| Pulmonary embolism | |
| Low clinical probability | 0.2 |
| Medium clinical probability | 1.8 |
| High clinical probability | 17.1 |
| Aortic dissection | |
| Tearing or ripping pain | 10.8 |
| Focal neurologic deficits | 6.633 |
| Ipsilateral versus contralateral pulse deficit | 5.7 |
| Cardiac tamponade | |
| Pulsus paradoxus > 12 mm Hg | 5.9 |
| Esophageal perforation | |
| Dysphagia, odynophagia, retching, vomiting, or subcutaneous emphysema | ? |
The history and exam can also facilitate differentiation of noncoronary causes of life‐threatening chest pain. The dismal performance of individual bedside findings for pulmonary embolism is what led to development of quantitative D‐dimer assays and objective methods based on bedside evaluation, including the widely used Wells Score.22 This score can be used to classify patients as having low, medium, and high risk of pulmonary embolism, facilitating management decisions after diagnostic imaging is obtained.23 Fewer than half of all patients with thoracic aortic dissection have classic exam findings; however, when present, they can appropriately raise the probability of dissection higher on the differential diagnosis.24 Importantly, no history or exam finding argues against dissection.24 Most patients with cardiac tamponade will have elevated jugular venous pressure (76%100%); however, poor interobserver agreement about this finding may decrease its detection.11, 25, 26 As the discussant notes, total paradox, defined as the palpable pulse disappearing with inspiration, is an insensitive test for tamponade, present in only 23% of patients with the disorder. In contrast, an inspiratory drop in systolic blood pressure of more than 12 mm Hg should prompt consideration for tamponade.11, 26 Commonly taught features of esophageal perforation, including chest pain, dysphagia, odynophagia, prior retching or vomiting, subcutaneous emphysema, dyspnea, and pleural effusions, vary in their reported sensitivity, but their specificity is virtually never reported.27
Like most patients with chest pain, our patient lacked all these symptoms and signs, arguing for myocardial ischemia, although he had a few signs that argued against it (sharp and positional chest pain). After the initial CXR and ECG, further testing with cardiac biomarkers was appropriate, but a fundamental error was made in not returning to the patient's bedside to repeat the interview and examination after the cardiac biomarkers were found to be normal. Had this been done, several cluesdysphagia, onset of pain with eating bony fish, and feverwould have pushed esophageal perforation to the top of the differential diagnosis. Subsequent testing would have led to the correct diagnosis and avoided a potentially harmful diagnostic fishing expedition.
Take‐Home Points
-
Esophageal perforation is an uncommon but life‐threatening cause of chest pain that is difficult to diagnose because of its nonspecific symptoms.
-
An accurate and complete history and exam can reveal signs and symptoms that influence the likelihood of each life‐threatening cause of chest pain. Evaluating patients for these features is vital to the rank ordering of a differential diagnosis and the selection of appropriate diagnostic tests.
-
There is no substitute for repeating the history, reexamining the patient, and reevaluating available information when confronted with a confusing constellation of symptoms.
Acknowledgements
The authors thank Steve McGee for his thoughtful review and comments on the manuscript.
- ,.Esophageal perforations: a 15 year experience.Am J Surg.1982;143:495–503.
- ,,.Esophageal perforation: emphasis on management.Ann Thorac Surg.1996;61:1447–1451; discussion1451–1452.
- ,,,,,.Evolving options in the management of esophageal perforation.Ann Thorac Surg.2004;77:1475–1783.
- ,.Personal management of 57 consecutive patients with esophageal perforation.Am J Surg.2004;187:58–63.
- ,,,,.Perforation of the oesophagus and aorta after eating fish: an unusual cause of chest pain.Emerg Med J.2003;20:385–386.
- ,,,.Esophageal perforation and mediastinitis from fish bone ingestion.South Med J.2003;96:516–520.
- ,,,.A 73‐year‐old man with chest pain 4 days after a fish dinner.Chest.2004;126:294–297.
- ,.The science of the art of the clinical examination.JAMA.1992;267:2650–2652.
- .Clinical skills in the 21st century.Arch Intern Med.1994;154:22–24.
- ,.Pulmonary auscultatory skills during training in internal medicine and family practice.Am J Respir Crit Care Med.1999;159:1119–1124.
- .Evidence‐Based Physical Diagnosis.Philadelphia, PA:Saunders;2001.
- .Simple is beautiful: the neglected power of simple tests.Arch Intern Med.2004;164:2198–2200.
- ,.Pearls and pitfalls in patient care: need to revive traditional clinical values.Am J Med Sci.2004;327:79–85.
- ,. Physical diagnosis: a lost art? Agency for Health Research and Quality. WebM75:29–40.
- .Low‐tech autopsies in the era of high‐tech medicine: continued value for quality assurance and patient safety.JAMA.1998;280:1273–1274.
- ,,,.Has misdiagnosis of appendicitis decreased over time? A population‐based analysis.JAMA.2001;286:1748–1753.
- ,,,.Changes in rates of autopsy‐detected diagnostic errors over time: a systematic review.JAMA.2003;289:2849–2856.
- .Diagnostic Process.J Coll Gen Pract.1963;54:579–589.
- .The importance of the history in the medical clinic and the cost of unnecessary tests.Am Heart J.1980;100:928–931.
- ,.Bedside diagnosis of coronary artery disease: a systematic review.Am J Med.2004;117:334–343.
- ,,, et al.Use of a clinical model for safe management of patients with suspected pulmonary embolism.Ann Intern Med.1998;129:997–1005.
- ,,, et al.Diagnostic pathways in acute pulmonary embolism: recommendations of the PIOPED II investigators.Am J Med.2006;119:1048–1055.
- .Does this patient have an acute thoracic aortic dissection?JAMA.2002;287:2262–2272.
- ,.The rational clinical examination. Does this patient have abnormal central venous pressure?JAMA.1996;275:630–634.
- ,,,.Does this patient with a pericardial effusion have cardiac tamponade?JAMA.2007;297:1810–1818.
- ,.Spontaneous esophageal rupture: a frequently missed diagnosis.Am Surg.1999;65:449–452.
- ,.Esophageal perforations: a 15 year experience.Am J Surg.1982;143:495–503.
- ,,.Esophageal perforation: emphasis on management.Ann Thorac Surg.1996;61:1447–1451; discussion1451–1452.
- ,,,,,.Evolving options in the management of esophageal perforation.Ann Thorac Surg.2004;77:1475–1783.
- ,.Personal management of 57 consecutive patients with esophageal perforation.Am J Surg.2004;187:58–63.
- ,,,,.Perforation of the oesophagus and aorta after eating fish: an unusual cause of chest pain.Emerg Med J.2003;20:385–386.
- ,,,.Esophageal perforation and mediastinitis from fish bone ingestion.South Med J.2003;96:516–520.
- ,,,.A 73‐year‐old man with chest pain 4 days after a fish dinner.Chest.2004;126:294–297.
- ,.The science of the art of the clinical examination.JAMA.1992;267:2650–2652.
- .Clinical skills in the 21st century.Arch Intern Med.1994;154:22–24.
- ,.Pulmonary auscultatory skills during training in internal medicine and family practice.Am J Respir Crit Care Med.1999;159:1119–1124.
- .Evidence‐Based Physical Diagnosis.Philadelphia, PA:Saunders;2001.
- .Simple is beautiful: the neglected power of simple tests.Arch Intern Med.2004;164:2198–2200.
- ,.Pearls and pitfalls in patient care: need to revive traditional clinical values.Am J Med Sci.2004;327:79–85.
- ,. Physical diagnosis: a lost art? Agency for Health Research and Quality. WebM75:29–40.
- .Low‐tech autopsies in the era of high‐tech medicine: continued value for quality assurance and patient safety.JAMA.1998;280:1273–1274.
- ,,,.Has misdiagnosis of appendicitis decreased over time? A population‐based analysis.JAMA.2001;286:1748–1753.
- ,,,.Changes in rates of autopsy‐detected diagnostic errors over time: a systematic review.JAMA.2003;289:2849–2856.
- .Diagnostic Process.J Coll Gen Pract.1963;54:579–589.
- .The importance of the history in the medical clinic and the cost of unnecessary tests.Am Heart J.1980;100:928–931.
- ,.Bedside diagnosis of coronary artery disease: a systematic review.Am J Med.2004;117:334–343.
- ,,, et al.Use of a clinical model for safe management of patients with suspected pulmonary embolism.Ann Intern Med.1998;129:997–1005.
- ,,, et al.Diagnostic pathways in acute pulmonary embolism: recommendations of the PIOPED II investigators.Am J Med.2006;119:1048–1055.
- .Does this patient have an acute thoracic aortic dissection?JAMA.2002;287:2262–2272.
- ,.The rational clinical examination. Does this patient have abnormal central venous pressure?JAMA.1996;275:630–634.
- ,,,.Does this patient with a pericardial effusion have cardiac tamponade?JAMA.2007;297:1810–1818.
- ,.Spontaneous esophageal rupture: a frequently missed diagnosis.Am Surg.1999;65:449–452.
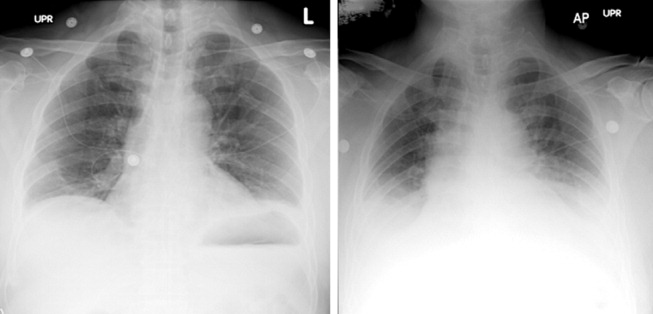
“Non‐Heart‐Beating” Organ Donation
In April 2003 the Health Resources and Services Administration of the U.S. Department of Health and Human Services (DHHS) announced the formation of the Organ Donation Breakthrough Collaborative (ODBC).1 The Organ Donation Breakthrough Collaborative created 58 national donation service areas (DSAs) to organize the transplant community across the United States. Each of the 58 organ procurement organizations (OPOs) is joined to a regional transplant center or centers and donor hospitals to form a DSA. The ODBC's goal is to achieve a cadaveric organ donation rate of 75% or higher from hospitals within each DSA.2
A requirement for organ donation from patients facing imminent or cardiac death has been introduced to increase the supply of transplantable organs and shorten the waiting time for transplantation candidates.35 This type of organ donation represents a significant source of organs required for future expansion of transplantation practice in the United States. The requirement for donation in imminent or cardiac death is implemented through the collaboration of the Advisory Committee on Organ Transplantation of the DHHS (Table 1), the Centers for Medicare & Medicaid Services (CMS), and the Joint Commission on Accreditation of Healthcare Organizations (JCAHO).3, 57 The organ donor pool of those facing imminent or cardiac death has also been expanded to include neurologically intact patients who may not fulfill brain death criteria before withdrawal of life support.4, 8, 9
| State law (year)* | |
|---|---|
| |
| Uniform Anatomical Gift Act (1968) | Any 18‐year‐old with a sound mind may donate his or her body after death to be used for medical research or as a source of transplantable tissues and organs and barring others from overriding a donor's decision to make an anatomical gift. |
| Amendment (1987) | Minors who can apply for a driver's license are empowered to make anatomical gifts, but either parent can revoke the gift if the minor dies before the age of 18. |
| Revision (2006) | Declaration of a gift does not require any witnesses. |
| Amendment (2007) | Document of a gift or donor registry is sufficient for the removal of organs, which means an OPO does not need consent of the spouse or the family. |
| Enables an OPO to gain access to documents of gifts in donor registries, medical records, and records of a state motor vehicle department. | |
| Facilitates donations by expanding the list of those who may make an anatomical gift for another individual who has not declared a preference for or against donation. | |
| Permits removal of organs by medical personnel without explicit consent from a potential donor or from a relative of the donor, so long as the appropriate medical personnel or authorities have made a reasonable effort to discover any objection by the donor or the donor's family. | |
| Require hospitals to notify an OPO or third party designated by the OPO of an individual whose death is imminent or who has died in the hospital in order to increase donation opportunity. | |
| Gives an OPO the right to inspect a patient's medical records. | |
| Measures necessary to ensure the medical suitability of a part not be withdrawn while an examination is being made to determine whether an individual who has been referred to OPO has a part that could be the subject of an anatomical gift. If, following such an examination, it is determined by the OPO that the individual has a part that could be the subject of an anatomical gift, the individual is a prospective donor under this act unless the individual had signed a refusal. | |
| Forbids the buying and selling of organs. | |
| Measures necessary to ensure the medical suitability of an organ for transplantation or therapy may not be withheld or withdrawn from a prospective donor who has an advance health‐care directive or declaration unless the directive or declaration expressly provides to the contrary. The section presumes that for prospective donors the desire to save lives by making an anatomical gift trumps the desire to have life support systems withheld or withdrawn. Individuals who desire to overcome this presumption can do so by express language in their advance health‐care directive or declaration. | |
| Uniform Determination of Death Act (1981) | An individual who has sustained either (1) irreversible cessation of circulatory and respiratory functions, or (2) irreversible cessation of all functions of the entire brain including the brain stem is dead. A determination of death must be made in accordance with accepted medical standards. |
| Federal laws | |
| National Organ Transplant Act (1984) | Calls for a unified transplant network to be operated by a private, nonprofit organization under federal contract and the establishment of a Task Force in Organ Procurement and Transplantation and an Organ Procurement and Transplantation Registry. |
| Public Health and Welfare Act Title 42 USC (1999) | |
| Section 273 | Establishes guidelines to be a qualified OPO that can receive federal grants. |
| Section 274 | Establishes the OPTN & Scientific Registry for Transplantation. |
| Federal regulations | |
| Title Code 42 CFR Part 121 (1999) | Lists regulations of the OPTN final rule. |
| Explains the OPTN structure. | |
| Lists the policy that the OPTN board of directors is responsible for developing. | |
| Explains rules that an OPTN member must obey when including a person on the organ waiting list. | |
| Describes the requirements and tests for determining the suitability of donated organs. | |
| Explains how the OPTN identifies an organ recipient, allocates the organ, and transports it to the recipient. | |
| Describes how the board of directors should develop allocation policies to guarantee they are both efficient and just and allocation performance goals to ensure the best possible use and most equitable allocation of organs. | |
| Lists designated transplant program requirements. | |
| Describes how the HHS conducts reviews and evaluations and enforces rules. | |
| Describes the recording and reporting requirements of the various groups involved in the transplantation process. | |
| Establishes the Advisory Committee on Organ Transplantation (ACOT), which advises the HHS secretary on organ donation, procurement, allocation, and transplantation The HHS secretary may ask for ACOT's opinion of proposed OPTN policies. | |
| Title Code 42 CFR Parts 413, 441, 486 and 498 (2006) | Lists regulations of the OPO final rule. |
| Establishes new conditions for coverage for OPOs that include multiple new outcome and process performance measures based on organ donor potential and other related factors in each donation service area of qualified OPOs. | |
The President's Council on Bioethics independently evaluated the issues surrounding deceased organ donation and procurement.10 The President's Council on Bioethics has expressed major concerns about several issues pertinent to cardiac or imminent death organ donation that have not been addressed explicitly by the bodies that have made recommendations for reforming or expanding that type of organ donation in the United States. The debate on organ procurement in imminent or cardiac death has come to the forefront because of doubts about its ethical appropriateness and acceptance within the medical profession and the community at large. This review focuses on the serious issues related to organ procurement from patients facing imminent or cardiac death.
Organ Procurement and the Dead Donor Rule
Organ procurement is only permitted when the donor is already dead (ie, the dead donor rule), and the act of organ recovery cannot have been the immediate act to cause that death.10, 11 There are 2 criteria for death as defined in the Uniform Determination of Death Act (UDDA; Table 1): an individual who has sustained irreversible cessation of either (1) circulatory and respiratory functions or (2) all functions of the entire brain, including the brain stem, is considered dead and this determination of death must have been made in accordance with accepted medical standards.12 When organs are procured from an individual in whom all brain function has ceased but normal cardiac pump activity is continuing, it is referred to as heart‐beating organ donation. Organ procurement after cessation of cardiac pump activity and cardiorespiratory functions is referred to as non‐heart‐beating organ donation (NHBOD). Organ procurement from an individual in imminent or cardiac death is considered NHBOD.
Non‐heart‐beating organ donors can be neurologically intact and do not fulfill the brain death criterion prior to cessation of cardiac pump activity. In response to this dilemma, the University of Pittsburgh Medical Centre developed a protocol for donation of organs that permitted their procurement from patients who were pulseless and apneic for 2 minutes and did not fulfill brain criteria and who had previously given consent for organ donation.13 Because it is uncertain if cessation of cardiorespiratory function is irreversible after only a short time, the Institute of Medicine (IOM) extended the time required for pulselessness and apnea from 2 to 5 minutes before permitting organ procurement.14 Waiting longer than 5 minutes for the determination of death would compromise the quality of procured organs because of warm ischemia time and would influence the functioning of grafts in transplant recipients.
One of the pivotal assumptions for NHBOD acceptance is that 5 minutes of pulselessness and apnea eliminates the possibility that the procurement process itself could be the cause of death and fulfills the dead donor rule.14, 15 The cardiorespiratory death criteria were derived from observations that did not evaluate delayed autoresuscitation (spontaneous return of circulation) or simultaneous cessation of brain electrical activity (as recorded in brain death).1618 The death criteria applied for organ procurement must also comply with the irreversibility requirement of the UDDA.11, 12
The true incidence, temporal characteristics, and predictors of autoresuscitation in humans remain unknown because of underreporting in the literature. However, there have been case reports of autoresuscitation with return of neurologic function (also called the Lazarus phenomenon) after 10 minutes of cardiac asystole.19, 20 Maleck et al. and Adhiyaman et al. described autoresuscitation 5 minutes or longer after cardiorespiratory arrest in 44% and 50% of the published case reports, respectively.19, 20 Although cardiac asystole leads to the loss of arterial pulse pressure, circulatory arterial mean pressure is maintained in diastole by arteriolar vasomotor tone. The relaxation (diastole) phase systemic arterial to venous pressure gradient provides the perfusion pressure for vital organs and the spontaneous return of circulation after circulatory arrest.21 It is likely that autoresuscitation occurs because of the persistence of circulatory vasomotor tone after cessation of cardiac function. The time course of systemic vascular tone after circulatory arrest has not been well characterized in humans. However, the IOM criteria did not account for the incidence of delayed autoresuscitation in humans even though the Maastricht protocol (developed by the University of Zurich, Zurich, Switzerland) acknowledged this phenomenon and required at least 10 minutes to elapse after cardiorespiratory arrest before starting organ procurement.22 The 10‐minute waiting time did not compromise the quality of the organs procured.
The cardiorespiratory death criteria for organ procurement also ignore cardiac electrical activity (such as pulseless electrical activity or ventricular fibrillation) on an electrocardiogram. Research with cardiac ultrasonography and indwelling arterial catheters confirms that pulseless cardiac electrical activity can be associated with cardiac mechanical contractions, although these contractions are too weak to be detected by blood pressure monitoring.23 The presence of cardiac electrical activity on an electrocardiogram can also increase the likelihood that delayed autoresuscitation will occur.19, 20 Furthermore, whether there is brain electrical activity or neurologic function when cardiac electrical activity is still observed on an electrocardiogram remains unknown.24 It can be argued that donors who have already suffered severe neurologic injury cannot have meaningful neurologic function at the time of cardiorespiratory death. However, the presence of brain activity becomes relevant for organ donors with intact neurologic and brain function prior to cardiorespiratory arrest when only cardiorespiratory criteria for organ procurement are being used.4, 8, 9
In situ circulatory support with extracorporeal perfusion in organ donors has also refuted that cardiorespiratory arrest for 5 minutes fulfills the UDDA requirement because reversibility can occur during the procurement process. In situ extracorporeal perfusion is initiated 5 minutes after cardiorespiratory arrest of donors in order to preserve organs for procurement.25 Coronary and cerebral reperfusion can lead to the return of cardiac and neurologic functions (also called reanimation) of donors during the procurement process. Mechanical occlusion of the aortic arch and pharmacological agents are required to suppress donor reanimation during organ procurement.26 Martin et al. documented that in situ extracorporeal perfusion returned full neurologic and cardiac function 25 minute after cardiorespiratory arrest that occurred outside the hospital.27 Similar observations of full neurologic recovery and survival to hospital discharge were reported after in situ extracorporeal perfusion for in‐hospital cardiorespiratory arrest.28 These observations confirm that the time required for irreversible loss of neurologic function after cessation of circulation is much longer than the 25 minutes of cardiorespiratory arrest required to begin the process of organ procurement in NHBOD.
The incidence of donor reanimation during procurement is unknown because its reporting violates the dead donor rule and can create legal concerns.11 It can be argued that reanimation of organ donors is irrelevant because it does not mean survival. However, the occurrence of reanimation invalidates the premise that the cardiorespiratory criteria for organ procurement comply with the uniform determination of death. Others have accepted the inaccuracy of these criteria for determining death for procurement of organs from deceased donors and proposed abandoning the dead donor rule in order to permit recovery of transplantable organs before death.29
In the face of the uncertainty in determining death and in response to a media and marketing campaign by organ procurement organizations (OPOs) to promote public enrollment in deceased organ donation, the transplant community renamed NHBOD cardiac death organ donation.30, 31 The use of the term cardiac death is scientifically inaccurate and perhaps misleading. This term is used to denote the cessation of circulation and cardiac pump activity. The term cardiac death can be misinterpreted as meaning the heart has irreversibly ceased at the time of procurement, thus contradicting the scientific evidence for spontaneous resumption of cardiac function and autoresuscitation.19, 20 Alternatively, the use of this term can falsely imply that neurologic activity or brain stem function has ceased irreversibly after loss of cardiac activity, when scientific evidence suggests that brain stem function can remain after cardiac arrest.32
Consent for Organ Donation
Several state laws and federal regulations have been enacted to ensure that organ donation and transplantation practice comply with the ethical and legal standards of society (Table 1). The current regulations require hospitals across the United States to provde regional OPOs with early notification of all patients whose deaths are imminent before life support has been withdrawn so that discussion of organ donation with surrogate decision makers can be initiated independently and consent obtained.3, 5, 9 The Organ Donation Breakthrough Collaborative has set a goal of each OPO accomplishing a target organ donation rate of 75% or higher at local hospitals within an assigned donation service area (DSA).1, 2, 5 The financial and administrative incentives for the OPO to achieve that target organ donation rate have introduced undisclosed conflict within the donation consent process.33 Self‐serving bias of OPOs can influence whether pertinent information necessary for surrogate decision makers to provide informed consent is disclosed.34 As an example of this bias, alternative options for care and palliation may be discussed with surrogate decision makers with less enthusiasm than are the benefits and altruistic notion of organ donation. In obtaining donation consent, OPOs often avoid disclosing details of perimortem interventions performed on donors that are required for successful procurement of transplantable organs.10, 34, 35 After receiving consent for organ donation, OPO staffs also assume the responsibility of planning donor medical care and treatment pathways essential for maintaining organ viability and of preparing for subsequent procurement.5, 36 In essence, the care of the dying patient is guided by a team whose primary interest is the preservation of organs until procurement has been accomplished.
The Uniform Anatomical Gift Act (UAGA) assigns explicit priority to the donor's expressed intent so that consent for organ donation becomes irrevocable and does not require the consent or concurrence of any person after the donor's death (Table 1).9, 37 The donor's authorization to donate, recorded on an organ donor card, the individual's driver's license, or a donor registry, becomes a legally binding advance directive. The UAGA amendment enables OPOs to procure organs without family consent and in certain instances after family refusal to donate.37
Other consent options for organ donation from deceased donors have been proposed to maximize OPO recovery of transplantable organs in the United States (Table 2).8 The IOM has considered presumed consent for organ donation as a favorable option.8 Presumed consent means the default option is consent to donation, that if an individual has not expressly rejected donation, that individual is considered to have consented to organ donation. Legislative enactment of presumed consent enables OPOs to avoid the potential for surrogates to deny consent for donation, thus increasing the pool of future organ donors. The revised UAGA replaces nondonation with the intent to donate organs as the default option. In the default option, all measures necessary to ensure the medical suitability of an organ for transplantation can not be withheld or withdrawn until the OPO has determined medical suitability of the individual as a prospective donor (Table 1). The default option overrides the expression of intent in a declaration or advance health‐care directives not to have life prolonged by withholding or withdrawing life support system unless the individual has expressed refusal of donation (Tables 1 and 2). The revised UAGA presumes that for prospective donors the desire to save lives by making an anatomical gift trumps the desire to have life support systems withheld or withdrawn. Mandated consent (or conscription) has also been proposed for recovery of cadaveric organs (Table 2).38 Under mandated consent, consent for organ donation is automatic from all deceased individuals; therefore, OPOs would not require or request consent because removal of all needed transplantable cadaveric organs would be compulsory. OPO staffs would no longer have to discuss organ procurement from potential donors with family members or other surrogates. An alternative form of donation consent is mandated choice, which requires each individual to decide in advance either to agree to organ donation or to refuse it. Mandated choice is the IOM's least favorite option because it would require extensive public informational programs on organ donation to facilitate individual choices and decision making (Table 2).8
| Type | Description |
|---|---|
| Requested (expressed) consent | An individual is asked to voluntarily agree to organ donation. |
| Presumed (implied) consent | Unless an individual has expressly refused to donate organs, the default option is agreement to donate organs. |
| Mandated consent (conscription) | An individual is not required to decide on organ donation before death, and there is an automatic right to procure organs from any and all deceased individuals. |
| Mandated choice | An individual must choose between 2 options before death: agreement or refusal to donate organs. |
End‐of‐Life Care
Quality of end‐of‐life (EOL) care for an organ donor, as for any individual whose treatment is being withdrawn, is considered the highest priority of care and must not be compromised by the donation process. Yet no studies have investigated the impact of organ donation on the quality of EOL care in NHBOD.35 Previous reports have criticized the quality of EOL care offered to dying patients in intensive care units (ICUs).39, 40 Many of these patients are undergoing withdrawal of life support in anticipation of death and are considered candidates for NHBOD. The Robert Wood Johnson Foundation (RWJF) Critical Care End‐Of‐Life Peer Workgroup developed 53 EOL quality indicators to standardize and measure the quality of EOL care.41 These quality indicators, organized in 7 domains, focus on delivering patient‐ and family‐centered care and facilitating a good death experience in the ICU (Table 3).
| Domains of comprehensive quality indicators of EOLC (n = 53)41 | Abbreviated quality indicators of EOLC (n = 18)46 |
|---|---|
| |
| Patient and family‐centered decision making (n = 13) | |
| Recognize the patient and family as the unit of care | |
| Assess the patient's and family's decision‐making style and preferences | |
| Address conflicts in decision making within the family | |
| Assess, together with appropriate clinical consultants, the patient's capacity to participate in decision making about treatment and document assessment | Assessment of the patient's decisional capacity |
| Initiate advance care planning with the patient and family | |
| Clarify and document the status of the patient's advance directive | Documentation of the presence and, if present, contents of advance directives |
| Identify the healthcare proxy or surrogate decision maker | Documentation of a surrogate decision maker within 24 hours of admission |
| Clarify and document resuscitation orders | |
| Assure patients and families that decision making by the health care team will incorporate their preferences | |
| Follow ethical and legal guidelines for patients who lack both capacity to make decisions and a surrogate decision maker | |
| Establish and document clear, realistic, and appropriate goals of care in consultation with the patient and family | Documentation of the goals of care |
| Help the patient and family assess the benefits and burdens of alternative treatment choices as the patient's condition changes | |
| Forgo life‐sustaining treatments in a way that ensures patient and family preferences are elicited and respected | |
| Communication within the team and with patients and families (n = 10) | |
| Meet as interdisciplinary team to discuss the patient's condition, clarify goals of treatment, and identify the patient's and family's needs and preferences | Documentation of a timely interdisciplinary clinicianfamily conference |
| Address conflicts among the clinical team before meeting with the patient and/or family | |
| Utilize expert clinical, ethical, and spiritual consultants when appropriate | |
| Recognize the adaptations in communication strategy required for patients and families according to the chronic versus acute nature of the illness, cultural and spiritual differences, and other influences | |
| Meet with the patient and/or family on a regular basis to review patient's status and to answer questions | Documentation of timely physician communication with the family |
| Communicate all information to the patient and family, including distressing news, in a clear, sensitive, unhurried manner and in an appropriate setting | |
| Clarify the patient's and family's understanding of the patient's condition and goals of care at the beginning and end of each meeting | |
| Designate primary clinical liaison(s) who will communicate with the family daily | |
| Identify a family member who will serve as the contact person for the family | |
| Prepare the patient and family for the dying process | |
| Continuity of care (n = 3) | |
| Maximize continuity of care across clinicians, consultants, and settings | |
| Orient new clinicians to the status of the patient and family | Transmission of key information with transfer of the patient out of the ICU |
| Policy for continuity of nursing services | |
| Prepare the patient and/or family for a change of clinician(s) and introduce new clinicians | |
| Emotional and practical support for patients and families (n = 8) | |
| Elicit and attend to the needs of the dying person and his/her family | |
| Distribute written material (booklet) for families that includes orientation to the ICU environment and open visitation guidelines, logistical information (nearby hotels, banks, restaurants, directions), listings of financial consultation services, and bereavement programs and resources | Open visitation policy for family members |
| Facilitate strengthening of patientfamily relationships and communication | |
| Maximize privacy of the patient and family | |
| Value and support the patient's and family's cultural traditions | |
| Arrange for social support for patients who do not have family or friends | Documentation that psychosocial support has been offered |
| Distribute written material (booklet) containing essential logistical information and listings of financial consultation services and bereavement support programs/resources | |
| Support family members through the patient's death and their bereavement | |
| Symptom management and comfort care (n = 10) | |
| Emphasize the comprehensive comfort care that will be provided to the patient rather than the removal of life‐sustaining treatments | |
| Institute and use uniform quantitative symptom assessment scales appropriate for communicative and noncommunicative patients on a routine basis | Documentation of pain assessment |
| Documentation of respiratory distress assessment | |
| Standardize and follow best clinical practices for symptom management | Protocol for analgesia/sedation in terminal withdrawal of mechanical ventilation |
| Appropriate medications available during withdrawal of mechanical ventilation | |
| Use nonpharmacologic as well as pharmacologic measures to maximize comfort as appropriate and desired by the patient and family | |
| Reassess and document symptoms following interventions | Documentation of pain management |
| Documentation of respiratory distress management | |
| Know and follow best clinical practices for withdrawing life‐sustaining treatments to avoid patient and family distress | |
| Eliminate unnecessary tests and procedures (laboratory work, weights, routine vital signs) and only maintain intravenous catheters for symptom management when life support is being withdrawn | |
| Minimize noxious stimuli (monitors, strong lights) | |
| Attend to patient's appearance and hygiene | |
| Ensure family's and/or clinician's presence so the patient is not dying alone | |
| Spiritual support for patients and families (n = 3) | |
| Assess and document spiritual needs of the patient and family on an ongoing basis | Documentation that spiritual support was offered |
| Encourage access to spiritual resources | |
| Elicit and facilitate spiritual and cultural practices that the patient and family find comforting | |
| Emotional and organizational support for ICU clinicians (n = 6) | |
| Support health care team colleagues caring for dying patients | Opportunity to review experience of caring for dying patients by ICU clinicians |
| Adjust nursing staff and medical rotation schedules to maximize continuity of care providers for dying patients | |
| Communicate regularly with interdisciplinary team about goals of care | |
| Establish a staff support group, based on the input and needs of ICU staff and experienced group facilitators, and integrate meeting times into the routine of the ICU | |
| Enlist palliative care experts, pastoral care representatives, and other consultants to teach and model aspects of EOLC | |
| Facilitate rituals for the staff to mark the death of patients | |
| Strategies to improve EOLC and provide a good death42, 43 | |
| EOL care quality monitoring | |
| Making environmental changes to promote dying with dignity | |
| Managing patients' pain and discomfort | |
| Knowing and following patients' wishes for end‐of‐life care | |
| Bereavement program or service | |
| Regular meetings of senior ICU physician and nurse with patients' families | |
| Training of ICU clinicians in end‐of‐life communication skills | |
| Role modeling and supervision of trainees by clinicians experienced in end‐of‐life care | |
| Formal mechanism for emotional support of staff caring for dying patients | |
| Access to palliative care consultants | |
| Training of ICU clinicians in symptom management | |
| Scheduling staff to promote continuity of care for dying patients | |
| Formal system for scaled assessment and charting of patients' symptoms | |
| Method to help resolve differences about appropriate care goals | |
| Resources to accommodate diversity among patients/families at the end of life | |
| Access to clinical ethics consultants | |
| Regular pastoral care visits to the ICU | |
In a subsequent U.S. survey, the Critical Care Peer Workgroup of the Promoting Excellence in End‐of‐Life Care Project reported that more than 75% of ICUs were still not monitoring the quality of EOL care.42 The survey also identified multiple barriers to optimal EOL care found in most ICUs. The study group proposed several strategies to overcome these barriers and improve the quality of EOL care (Table 3).42, 43 It can also be inferred from the survey findings that most ICUs are unprepared and lack the necessary tools to appropriately inform patients and families of the trade‐off in EOL care for NHBOD. The President's Council for Bioethics has also warned that NHBOD can transform EOL care from a peaceful dignified death into a profanely high‐tech death experience for donors' families.10
Several aspects of medical care that are neither palliative nor beneficial are performed for donor management for NHBOD and can explain the feared transformation of the death experience. The revised UAGA reaffirms that all measures necessary to ensure the medical suitability of an organ for transplantation cannot be withheld or withdrawn from the prospective donor and overrides the expression of intent by a prospective donor in either a declaration or advance health‐care directive not to have life prolonged by use of life support systems (Table 1).9 The 2007 amendment to revised UAGA section 21 recognizes the conflict between all measures necessary to ensure organs viability for transplantation and appropriate EOL care and requires the attending physician and OPO to resolve the conflict with the prospective donor or surrogate decision‐maker.9
OPOs apply donor management critical pathways to potential organ donors in order to maintain organ viability for successful execution of organ procurement.36 The University of Wisconsin developed a protocol and an evaluation tool to determine the eligibility of potential candidates for NHBOD.44 The protocol entails temporary discontinuation of mechanical ventilation for a trial of spontaneous respiration lasting up to 10 minutes to determine the likelihood of cardiorespiratory death within 60‐90 minutes of the withdrawal of life support. Those patients predicted by the University of Wisconsin evaluation tool to survive a longer time are not candidates for NHBOD and are transferred to palliative care. Those patients who meet the necessary criteria of the University of Wisconsin evaluation tool become candidates for NHBOD and undergo additional antemortem testing, invasive vascular instrumentation, and infusion of medications essential for organ preservation.36 The instrumentation and medications used for organ preservation can also expedite death on withdrawal of life support.45 Other interventions (such as circulatory support with invasive and noninvasive devices, extracorporeal perfusion and oxygenation, endotracheal reintubation, mechanical ventilation, and bronchoscopy) are performed when cardiorespiratory death is pronounced in order to maintain organ viability and can inadvertently reanimate the donor during the procurement process.26
The process of obtaining donation consent and subsequent donor management protocols for NHBOD deviate from more than 60% of the RWJF quality indicators recommended for optimal EOL care.35, 36, 41 Therefore, NHBOD can have a profound impact on the quality of EOL care. There has been a recent proposal to abbreviate the original RWJF quality indicators to include 14 of the 53 (26%) original quality indicators described for optimal EOL care in the ICU (Table 3).46 Many of the quality indicators expected to be negatively affected by NHBOD are not included in the proposal for an abbreviated list. There has been a concern that the application of an abbreviated rather than a comprehensive metrics for EOL care can portray an incomplete assessment and perhaps misinform donors and their families about the potential trade‐off in EOL care. The President's Council on Bioethics has emphasized that comprehensive evaluation of the quality of EOL care is an ethical imperative so that families can decide if the trade‐off is acceptable for organ donation.10 Deciding to donate organs at the end of life can be stressful for many families, and therefore they must be fully informed of the possible consequences. Posttraumatic stress disorders, anxiety, depression, and decreased quality of life have been reported in the deceased's family members who shared in stressful EOL decisions.47 Posttraumatic stress disorders have been reported in family members of deceased organ donors.48 Organ‐focused behavior by professionals requesting consent for organ donation and ambivalent decision making by family members appeared to increase the risk of relatives of deceased donors subsequently developing traumatic memories and stress disorders. The processes required for successful accomplishment of donation consent and subsequent organ recovery can interfere with many of the interventions that lessen the burden of bereavement of relatives of ICU decedents.49
The variability in decision making by health care providers about medical futility and EOL care has been given as a reason for concern about the implementation of NHBOD.50 The variability of EOL practice raises the possibility of conflicted decision making on medical futility within institutions that have transplant programs.50 Ethical conflicts and moral distress have been reported among health care providers who were directly involved in organ procurement in NHBOD.51 The pressure to recover transplantable organs from NHBOD candidates has been associated with health care professionals' perception of euthanasia and premature determination of medical futility and withdrawal of life support. The long‐term psychological impact of NHBOD practice on caregivers, health care providers, and professionals remains unknown.
CONCLUSIONS
In conclusion, NHBOD influences medical care at critical time points to maximize the procurement of transplantable organs and minimize their warm ischemia time with negative consequences on the EOL care for the prospective donors and their families (see Figure 1).
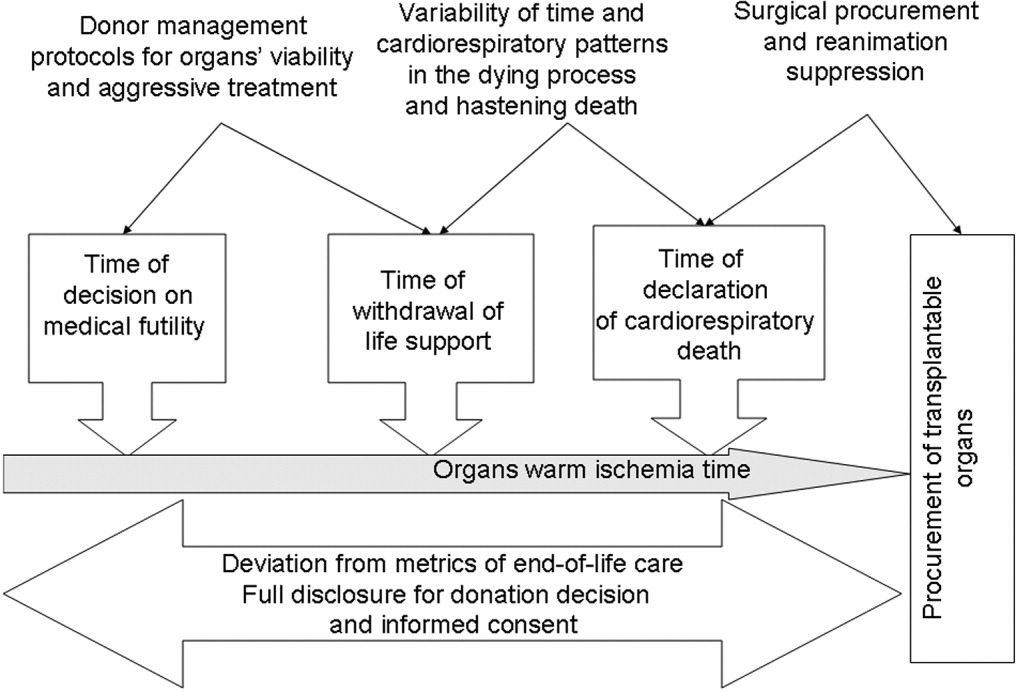
Mandatory implementation of NHBOD in the face of difficulties surrounding the quality of EOL care for donors raises concern across the medical profession and community. There is a need for better scientific validation of the timing of organ procurement to ensure that organ recovery is not the irreversible event defining death in NHBOD. The desire of OPOs or their affiliates to maximize recovery of transplantable organs introduces self‐serving bias into obtaining consent for organ donation and violates the basic tenet of true informed consent. The use of comprehensive quality indicators of EOL care will help to determine the impact of NHBOD on donors, families, caregivers, and health care providers.
- ,,, et al.Organ donation and utilization, 1995‐2004: Entering the collaborative era.Am J Transplant.2006;6:1101–1110.
- U.S. Department of Health and Human Servcies—Organ Donation and Transplant Breakthrough Collaborative. Measurement strategy: Organ Donation and Transplant Breakthrough Collaborative. Available at: http://www.organdonationnow.org/. Accessed December 15,2006.
- U.S. Department of Health and Human Services Advisory Committee on Organ Transplantation. Consensus Recommendations to the HHS Secretary. Available at: http://www.organdonor.gov/research/acot.htm. Accessed January 30,2007.
- ,,, et al.Report of a National Conference on Donation after Cardiac Death.Am J Transplant.2006;6:281–291.
- Centers for Medicare and Medicaid Services, Department of Health and Human Services.Medicare and Medicaid Programs. Conditions for coverage for organ procurement organizations (OPOs); final rule.Federal Register.2006;71:30981–31054.
- [JCAHO] Joint Commission on Accreditation of Healthcare Organizations. Health care at the crossroads: strategies for narrowing the organ donation gap and protecting patients. Available at: http://www.jointcommission.org/PublicPolicy/organ_donation.htm. Accessed January 30,2007.
- [JCAHO] Joint Commission on Accreditation of Healthcare Organizations.Revisions to Standard LD.3.110.Jt Comm Perspect.2006;26:7.
- Committee on Increasing Rates of Organ Donation‐Board on Health Sciences Policy‐Institute of Medicine.Organ Donation: Opportunities for Action.Washington, DC:National Academies Press;2006.
- National Conference of Commissioners on Uniform State Laws. Revised Uniform Anatomical Gift Act (2006) and Amendment to Section 21 (2007). http://www.law.upenn.edu/bll/ulc/uaga/2006final.htm and http://www.anatomicalgiftact.org/DesktopDefault.aspx?tabindex=0
In April 2003 the Health Resources and Services Administration of the U.S. Department of Health and Human Services (DHHS) announced the formation of the Organ Donation Breakthrough Collaborative (ODBC).1 The Organ Donation Breakthrough Collaborative created 58 national donation service areas (DSAs) to organize the transplant community across the United States. Each of the 58 organ procurement organizations (OPOs) is joined to a regional transplant center or centers and donor hospitals to form a DSA. The ODBC's goal is to achieve a cadaveric organ donation rate of 75% or higher from hospitals within each DSA.2
A requirement for organ donation from patients facing imminent or cardiac death has been introduced to increase the supply of transplantable organs and shorten the waiting time for transplantation candidates.35 This type of organ donation represents a significant source of organs required for future expansion of transplantation practice in the United States. The requirement for donation in imminent or cardiac death is implemented through the collaboration of the Advisory Committee on Organ Transplantation of the DHHS (Table 1), the Centers for Medicare & Medicaid Services (CMS), and the Joint Commission on Accreditation of Healthcare Organizations (JCAHO).3, 57 The organ donor pool of those facing imminent or cardiac death has also been expanded to include neurologically intact patients who may not fulfill brain death criteria before withdrawal of life support.4, 8, 9
| State law (year)* | |
|---|---|
| |
| Uniform Anatomical Gift Act (1968) | Any 18‐year‐old with a sound mind may donate his or her body after death to be used for medical research or as a source of transplantable tissues and organs and barring others from overriding a donor's decision to make an anatomical gift. |
| Amendment (1987) | Minors who can apply for a driver's license are empowered to make anatomical gifts, but either parent can revoke the gift if the minor dies before the age of 18. |
| Revision (2006) | Declaration of a gift does not require any witnesses. |
| Amendment (2007) | Document of a gift or donor registry is sufficient for the removal of organs, which means an OPO does not need consent of the spouse or the family. |
| Enables an OPO to gain access to documents of gifts in donor registries, medical records, and records of a state motor vehicle department. | |
| Facilitates donations by expanding the list of those who may make an anatomical gift for another individual who has not declared a preference for or against donation. | |
| Permits removal of organs by medical personnel without explicit consent from a potential donor or from a relative of the donor, so long as the appropriate medical personnel or authorities have made a reasonable effort to discover any objection by the donor or the donor's family. | |
| Require hospitals to notify an OPO or third party designated by the OPO of an individual whose death is imminent or who has died in the hospital in order to increase donation opportunity. | |
| Gives an OPO the right to inspect a patient's medical records. | |
| Measures necessary to ensure the medical suitability of a part not be withdrawn while an examination is being made to determine whether an individual who has been referred to OPO has a part that could be the subject of an anatomical gift. If, following such an examination, it is determined by the OPO that the individual has a part that could be the subject of an anatomical gift, the individual is a prospective donor under this act unless the individual had signed a refusal. | |
| Forbids the buying and selling of organs. | |
| Measures necessary to ensure the medical suitability of an organ for transplantation or therapy may not be withheld or withdrawn from a prospective donor who has an advance health‐care directive or declaration unless the directive or declaration expressly provides to the contrary. The section presumes that for prospective donors the desire to save lives by making an anatomical gift trumps the desire to have life support systems withheld or withdrawn. Individuals who desire to overcome this presumption can do so by express language in their advance health‐care directive or declaration. | |
| Uniform Determination of Death Act (1981) | An individual who has sustained either (1) irreversible cessation of circulatory and respiratory functions, or (2) irreversible cessation of all functions of the entire brain including the brain stem is dead. A determination of death must be made in accordance with accepted medical standards. |
| Federal laws | |
| National Organ Transplant Act (1984) | Calls for a unified transplant network to be operated by a private, nonprofit organization under federal contract and the establishment of a Task Force in Organ Procurement and Transplantation and an Organ Procurement and Transplantation Registry. |
| Public Health and Welfare Act Title 42 USC (1999) | |
| Section 273 | Establishes guidelines to be a qualified OPO that can receive federal grants. |
| Section 274 | Establishes the OPTN & Scientific Registry for Transplantation. |
| Federal regulations | |
| Title Code 42 CFR Part 121 (1999) | Lists regulations of the OPTN final rule. |
| Explains the OPTN structure. | |
| Lists the policy that the OPTN board of directors is responsible for developing. | |
| Explains rules that an OPTN member must obey when including a person on the organ waiting list. | |
| Describes the requirements and tests for determining the suitability of donated organs. | |
| Explains how the OPTN identifies an organ recipient, allocates the organ, and transports it to the recipient. | |
| Describes how the board of directors should develop allocation policies to guarantee they are both efficient and just and allocation performance goals to ensure the best possible use and most equitable allocation of organs. | |
| Lists designated transplant program requirements. | |
| Describes how the HHS conducts reviews and evaluations and enforces rules. | |
| Describes the recording and reporting requirements of the various groups involved in the transplantation process. | |
| Establishes the Advisory Committee on Organ Transplantation (ACOT), which advises the HHS secretary on organ donation, procurement, allocation, and transplantation The HHS secretary may ask for ACOT's opinion of proposed OPTN policies. | |
| Title Code 42 CFR Parts 413, 441, 486 and 498 (2006) | Lists regulations of the OPO final rule. |
| Establishes new conditions for coverage for OPOs that include multiple new outcome and process performance measures based on organ donor potential and other related factors in each donation service area of qualified OPOs. | |
The President's Council on Bioethics independently evaluated the issues surrounding deceased organ donation and procurement.10 The President's Council on Bioethics has expressed major concerns about several issues pertinent to cardiac or imminent death organ donation that have not been addressed explicitly by the bodies that have made recommendations for reforming or expanding that type of organ donation in the United States. The debate on organ procurement in imminent or cardiac death has come to the forefront because of doubts about its ethical appropriateness and acceptance within the medical profession and the community at large. This review focuses on the serious issues related to organ procurement from patients facing imminent or cardiac death.
Organ Procurement and the Dead Donor Rule
Organ procurement is only permitted when the donor is already dead (ie, the dead donor rule), and the act of organ recovery cannot have been the immediate act to cause that death.10, 11 There are 2 criteria for death as defined in the Uniform Determination of Death Act (UDDA; Table 1): an individual who has sustained irreversible cessation of either (1) circulatory and respiratory functions or (2) all functions of the entire brain, including the brain stem, is considered dead and this determination of death must have been made in accordance with accepted medical standards.12 When organs are procured from an individual in whom all brain function has ceased but normal cardiac pump activity is continuing, it is referred to as heart‐beating organ donation. Organ procurement after cessation of cardiac pump activity and cardiorespiratory functions is referred to as non‐heart‐beating organ donation (NHBOD). Organ procurement from an individual in imminent or cardiac death is considered NHBOD.
Non‐heart‐beating organ donors can be neurologically intact and do not fulfill the brain death criterion prior to cessation of cardiac pump activity. In response to this dilemma, the University of Pittsburgh Medical Centre developed a protocol for donation of organs that permitted their procurement from patients who were pulseless and apneic for 2 minutes and did not fulfill brain criteria and who had previously given consent for organ donation.13 Because it is uncertain if cessation of cardiorespiratory function is irreversible after only a short time, the Institute of Medicine (IOM) extended the time required for pulselessness and apnea from 2 to 5 minutes before permitting organ procurement.14 Waiting longer than 5 minutes for the determination of death would compromise the quality of procured organs because of warm ischemia time and would influence the functioning of grafts in transplant recipients.
One of the pivotal assumptions for NHBOD acceptance is that 5 minutes of pulselessness and apnea eliminates the possibility that the procurement process itself could be the cause of death and fulfills the dead donor rule.14, 15 The cardiorespiratory death criteria were derived from observations that did not evaluate delayed autoresuscitation (spontaneous return of circulation) or simultaneous cessation of brain electrical activity (as recorded in brain death).1618 The death criteria applied for organ procurement must also comply with the irreversibility requirement of the UDDA.11, 12
The true incidence, temporal characteristics, and predictors of autoresuscitation in humans remain unknown because of underreporting in the literature. However, there have been case reports of autoresuscitation with return of neurologic function (also called the Lazarus phenomenon) after 10 minutes of cardiac asystole.19, 20 Maleck et al. and Adhiyaman et al. described autoresuscitation 5 minutes or longer after cardiorespiratory arrest in 44% and 50% of the published case reports, respectively.19, 20 Although cardiac asystole leads to the loss of arterial pulse pressure, circulatory arterial mean pressure is maintained in diastole by arteriolar vasomotor tone. The relaxation (diastole) phase systemic arterial to venous pressure gradient provides the perfusion pressure for vital organs and the spontaneous return of circulation after circulatory arrest.21 It is likely that autoresuscitation occurs because of the persistence of circulatory vasomotor tone after cessation of cardiac function. The time course of systemic vascular tone after circulatory arrest has not been well characterized in humans. However, the IOM criteria did not account for the incidence of delayed autoresuscitation in humans even though the Maastricht protocol (developed by the University of Zurich, Zurich, Switzerland) acknowledged this phenomenon and required at least 10 minutes to elapse after cardiorespiratory arrest before starting organ procurement.22 The 10‐minute waiting time did not compromise the quality of the organs procured.
The cardiorespiratory death criteria for organ procurement also ignore cardiac electrical activity (such as pulseless electrical activity or ventricular fibrillation) on an electrocardiogram. Research with cardiac ultrasonography and indwelling arterial catheters confirms that pulseless cardiac electrical activity can be associated with cardiac mechanical contractions, although these contractions are too weak to be detected by blood pressure monitoring.23 The presence of cardiac electrical activity on an electrocardiogram can also increase the likelihood that delayed autoresuscitation will occur.19, 20 Furthermore, whether there is brain electrical activity or neurologic function when cardiac electrical activity is still observed on an electrocardiogram remains unknown.24 It can be argued that donors who have already suffered severe neurologic injury cannot have meaningful neurologic function at the time of cardiorespiratory death. However, the presence of brain activity becomes relevant for organ donors with intact neurologic and brain function prior to cardiorespiratory arrest when only cardiorespiratory criteria for organ procurement are being used.4, 8, 9
In situ circulatory support with extracorporeal perfusion in organ donors has also refuted that cardiorespiratory arrest for 5 minutes fulfills the UDDA requirement because reversibility can occur during the procurement process. In situ extracorporeal perfusion is initiated 5 minutes after cardiorespiratory arrest of donors in order to preserve organs for procurement.25 Coronary and cerebral reperfusion can lead to the return of cardiac and neurologic functions (also called reanimation) of donors during the procurement process. Mechanical occlusion of the aortic arch and pharmacological agents are required to suppress donor reanimation during organ procurement.26 Martin et al. documented that in situ extracorporeal perfusion returned full neurologic and cardiac function 25 minute after cardiorespiratory arrest that occurred outside the hospital.27 Similar observations of full neurologic recovery and survival to hospital discharge were reported after in situ extracorporeal perfusion for in‐hospital cardiorespiratory arrest.28 These observations confirm that the time required for irreversible loss of neurologic function after cessation of circulation is much longer than the 25 minutes of cardiorespiratory arrest required to begin the process of organ procurement in NHBOD.
The incidence of donor reanimation during procurement is unknown because its reporting violates the dead donor rule and can create legal concerns.11 It can be argued that reanimation of organ donors is irrelevant because it does not mean survival. However, the occurrence of reanimation invalidates the premise that the cardiorespiratory criteria for organ procurement comply with the uniform determination of death. Others have accepted the inaccuracy of these criteria for determining death for procurement of organs from deceased donors and proposed abandoning the dead donor rule in order to permit recovery of transplantable organs before death.29
In the face of the uncertainty in determining death and in response to a media and marketing campaign by organ procurement organizations (OPOs) to promote public enrollment in deceased organ donation, the transplant community renamed NHBOD cardiac death organ donation.30, 31 The use of the term cardiac death is scientifically inaccurate and perhaps misleading. This term is used to denote the cessation of circulation and cardiac pump activity. The term cardiac death can be misinterpreted as meaning the heart has irreversibly ceased at the time of procurement, thus contradicting the scientific evidence for spontaneous resumption of cardiac function and autoresuscitation.19, 20 Alternatively, the use of this term can falsely imply that neurologic activity or brain stem function has ceased irreversibly after loss of cardiac activity, when scientific evidence suggests that brain stem function can remain after cardiac arrest.32
Consent for Organ Donation
Several state laws and federal regulations have been enacted to ensure that organ donation and transplantation practice comply with the ethical and legal standards of society (Table 1). The current regulations require hospitals across the United States to provde regional OPOs with early notification of all patients whose deaths are imminent before life support has been withdrawn so that discussion of organ donation with surrogate decision makers can be initiated independently and consent obtained.3, 5, 9 The Organ Donation Breakthrough Collaborative has set a goal of each OPO accomplishing a target organ donation rate of 75% or higher at local hospitals within an assigned donation service area (DSA).1, 2, 5 The financial and administrative incentives for the OPO to achieve that target organ donation rate have introduced undisclosed conflict within the donation consent process.33 Self‐serving bias of OPOs can influence whether pertinent information necessary for surrogate decision makers to provide informed consent is disclosed.34 As an example of this bias, alternative options for care and palliation may be discussed with surrogate decision makers with less enthusiasm than are the benefits and altruistic notion of organ donation. In obtaining donation consent, OPOs often avoid disclosing details of perimortem interventions performed on donors that are required for successful procurement of transplantable organs.10, 34, 35 After receiving consent for organ donation, OPO staffs also assume the responsibility of planning donor medical care and treatment pathways essential for maintaining organ viability and of preparing for subsequent procurement.5, 36 In essence, the care of the dying patient is guided by a team whose primary interest is the preservation of organs until procurement has been accomplished.
The Uniform Anatomical Gift Act (UAGA) assigns explicit priority to the donor's expressed intent so that consent for organ donation becomes irrevocable and does not require the consent or concurrence of any person after the donor's death (Table 1).9, 37 The donor's authorization to donate, recorded on an organ donor card, the individual's driver's license, or a donor registry, becomes a legally binding advance directive. The UAGA amendment enables OPOs to procure organs without family consent and in certain instances after family refusal to donate.37
Other consent options for organ donation from deceased donors have been proposed to maximize OPO recovery of transplantable organs in the United States (Table 2).8 The IOM has considered presumed consent for organ donation as a favorable option.8 Presumed consent means the default option is consent to donation, that if an individual has not expressly rejected donation, that individual is considered to have consented to organ donation. Legislative enactment of presumed consent enables OPOs to avoid the potential for surrogates to deny consent for donation, thus increasing the pool of future organ donors. The revised UAGA replaces nondonation with the intent to donate organs as the default option. In the default option, all measures necessary to ensure the medical suitability of an organ for transplantation can not be withheld or withdrawn until the OPO has determined medical suitability of the individual as a prospective donor (Table 1). The default option overrides the expression of intent in a declaration or advance health‐care directives not to have life prolonged by withholding or withdrawing life support system unless the individual has expressed refusal of donation (Tables 1 and 2). The revised UAGA presumes that for prospective donors the desire to save lives by making an anatomical gift trumps the desire to have life support systems withheld or withdrawn. Mandated consent (or conscription) has also been proposed for recovery of cadaveric organs (Table 2).38 Under mandated consent, consent for organ donation is automatic from all deceased individuals; therefore, OPOs would not require or request consent because removal of all needed transplantable cadaveric organs would be compulsory. OPO staffs would no longer have to discuss organ procurement from potential donors with family members or other surrogates. An alternative form of donation consent is mandated choice, which requires each individual to decide in advance either to agree to organ donation or to refuse it. Mandated choice is the IOM's least favorite option because it would require extensive public informational programs on organ donation to facilitate individual choices and decision making (Table 2).8
| Type | Description |
|---|---|
| Requested (expressed) consent | An individual is asked to voluntarily agree to organ donation. |
| Presumed (implied) consent | Unless an individual has expressly refused to donate organs, the default option is agreement to donate organs. |
| Mandated consent (conscription) | An individual is not required to decide on organ donation before death, and there is an automatic right to procure organs from any and all deceased individuals. |
| Mandated choice | An individual must choose between 2 options before death: agreement or refusal to donate organs. |
End‐of‐Life Care
Quality of end‐of‐life (EOL) care for an organ donor, as for any individual whose treatment is being withdrawn, is considered the highest priority of care and must not be compromised by the donation process. Yet no studies have investigated the impact of organ donation on the quality of EOL care in NHBOD.35 Previous reports have criticized the quality of EOL care offered to dying patients in intensive care units (ICUs).39, 40 Many of these patients are undergoing withdrawal of life support in anticipation of death and are considered candidates for NHBOD. The Robert Wood Johnson Foundation (RWJF) Critical Care End‐Of‐Life Peer Workgroup developed 53 EOL quality indicators to standardize and measure the quality of EOL care.41 These quality indicators, organized in 7 domains, focus on delivering patient‐ and family‐centered care and facilitating a good death experience in the ICU (Table 3).
| Domains of comprehensive quality indicators of EOLC (n = 53)41 | Abbreviated quality indicators of EOLC (n = 18)46 |
|---|---|
| |
| Patient and family‐centered decision making (n = 13) | |
| Recognize the patient and family as the unit of care | |
| Assess the patient's and family's decision‐making style and preferences | |
| Address conflicts in decision making within the family | |
| Assess, together with appropriate clinical consultants, the patient's capacity to participate in decision making about treatment and document assessment | Assessment of the patient's decisional capacity |
| Initiate advance care planning with the patient and family | |
| Clarify and document the status of the patient's advance directive | Documentation of the presence and, if present, contents of advance directives |
| Identify the healthcare proxy or surrogate decision maker | Documentation of a surrogate decision maker within 24 hours of admission |
| Clarify and document resuscitation orders | |
| Assure patients and families that decision making by the health care team will incorporate their preferences | |
| Follow ethical and legal guidelines for patients who lack both capacity to make decisions and a surrogate decision maker | |
| Establish and document clear, realistic, and appropriate goals of care in consultation with the patient and family | Documentation of the goals of care |
| Help the patient and family assess the benefits and burdens of alternative treatment choices as the patient's condition changes | |
| Forgo life‐sustaining treatments in a way that ensures patient and family preferences are elicited and respected | |
| Communication within the team and with patients and families (n = 10) | |
| Meet as interdisciplinary team to discuss the patient's condition, clarify goals of treatment, and identify the patient's and family's needs and preferences | Documentation of a timely interdisciplinary clinicianfamily conference |
| Address conflicts among the clinical team before meeting with the patient and/or family | |
| Utilize expert clinical, ethical, and spiritual consultants when appropriate | |
| Recognize the adaptations in communication strategy required for patients and families according to the chronic versus acute nature of the illness, cultural and spiritual differences, and other influences | |
| Meet with the patient and/or family on a regular basis to review patient's status and to answer questions | Documentation of timely physician communication with the family |
| Communicate all information to the patient and family, including distressing news, in a clear, sensitive, unhurried manner and in an appropriate setting | |
| Clarify the patient's and family's understanding of the patient's condition and goals of care at the beginning and end of each meeting | |
| Designate primary clinical liaison(s) who will communicate with the family daily | |
| Identify a family member who will serve as the contact person for the family | |
| Prepare the patient and family for the dying process | |
| Continuity of care (n = 3) | |
| Maximize continuity of care across clinicians, consultants, and settings | |
| Orient new clinicians to the status of the patient and family | Transmission of key information with transfer of the patient out of the ICU |
| Policy for continuity of nursing services | |
| Prepare the patient and/or family for a change of clinician(s) and introduce new clinicians | |
| Emotional and practical support for patients and families (n = 8) | |
| Elicit and attend to the needs of the dying person and his/her family | |
| Distribute written material (booklet) for families that includes orientation to the ICU environment and open visitation guidelines, logistical information (nearby hotels, banks, restaurants, directions), listings of financial consultation services, and bereavement programs and resources | Open visitation policy for family members |
| Facilitate strengthening of patientfamily relationships and communication | |
| Maximize privacy of the patient and family | |
| Value and support the patient's and family's cultural traditions | |
| Arrange for social support for patients who do not have family or friends | Documentation that psychosocial support has been offered |
| Distribute written material (booklet) containing essential logistical information and listings of financial consultation services and bereavement support programs/resources | |
| Support family members through the patient's death and their bereavement | |
| Symptom management and comfort care (n = 10) | |
| Emphasize the comprehensive comfort care that will be provided to the patient rather than the removal of life‐sustaining treatments | |
| Institute and use uniform quantitative symptom assessment scales appropriate for communicative and noncommunicative patients on a routine basis | Documentation of pain assessment |
| Documentation of respiratory distress assessment | |
| Standardize and follow best clinical practices for symptom management | Protocol for analgesia/sedation in terminal withdrawal of mechanical ventilation |
| Appropriate medications available during withdrawal of mechanical ventilation | |
| Use nonpharmacologic as well as pharmacologic measures to maximize comfort as appropriate and desired by the patient and family | |
| Reassess and document symptoms following interventions | Documentation of pain management |
| Documentation of respiratory distress management | |
| Know and follow best clinical practices for withdrawing life‐sustaining treatments to avoid patient and family distress | |
| Eliminate unnecessary tests and procedures (laboratory work, weights, routine vital signs) and only maintain intravenous catheters for symptom management when life support is being withdrawn | |
| Minimize noxious stimuli (monitors, strong lights) | |
| Attend to patient's appearance and hygiene | |
| Ensure family's and/or clinician's presence so the patient is not dying alone | |
| Spiritual support for patients and families (n = 3) | |
| Assess and document spiritual needs of the patient and family on an ongoing basis | Documentation that spiritual support was offered |
| Encourage access to spiritual resources | |
| Elicit and facilitate spiritual and cultural practices that the patient and family find comforting | |
| Emotional and organizational support for ICU clinicians (n = 6) | |
| Support health care team colleagues caring for dying patients | Opportunity to review experience of caring for dying patients by ICU clinicians |
| Adjust nursing staff and medical rotation schedules to maximize continuity of care providers for dying patients | |
| Communicate regularly with interdisciplinary team about goals of care | |
| Establish a staff support group, based on the input and needs of ICU staff and experienced group facilitators, and integrate meeting times into the routine of the ICU | |
| Enlist palliative care experts, pastoral care representatives, and other consultants to teach and model aspects of EOLC | |
| Facilitate rituals for the staff to mark the death of patients | |
| Strategies to improve EOLC and provide a good death42, 43 | |
| EOL care quality monitoring | |
| Making environmental changes to promote dying with dignity | |
| Managing patients' pain and discomfort | |
| Knowing and following patients' wishes for end‐of‐life care | |
| Bereavement program or service | |
| Regular meetings of senior ICU physician and nurse with patients' families | |
| Training of ICU clinicians in end‐of‐life communication skills | |
| Role modeling and supervision of trainees by clinicians experienced in end‐of‐life care | |
| Formal mechanism for emotional support of staff caring for dying patients | |
| Access to palliative care consultants | |
| Training of ICU clinicians in symptom management | |
| Scheduling staff to promote continuity of care for dying patients | |
| Formal system for scaled assessment and charting of patients' symptoms | |
| Method to help resolve differences about appropriate care goals | |
| Resources to accommodate diversity among patients/families at the end of life | |
| Access to clinical ethics consultants | |
| Regular pastoral care visits to the ICU | |
In a subsequent U.S. survey, the Critical Care Peer Workgroup of the Promoting Excellence in End‐of‐Life Care Project reported that more than 75% of ICUs were still not monitoring the quality of EOL care.42 The survey also identified multiple barriers to optimal EOL care found in most ICUs. The study group proposed several strategies to overcome these barriers and improve the quality of EOL care (Table 3).42, 43 It can also be inferred from the survey findings that most ICUs are unprepared and lack the necessary tools to appropriately inform patients and families of the trade‐off in EOL care for NHBOD. The President's Council for Bioethics has also warned that NHBOD can transform EOL care from a peaceful dignified death into a profanely high‐tech death experience for donors' families.10
Several aspects of medical care that are neither palliative nor beneficial are performed for donor management for NHBOD and can explain the feared transformation of the death experience. The revised UAGA reaffirms that all measures necessary to ensure the medical suitability of an organ for transplantation cannot be withheld or withdrawn from the prospective donor and overrides the expression of intent by a prospective donor in either a declaration or advance health‐care directive not to have life prolonged by use of life support systems (Table 1).9 The 2007 amendment to revised UAGA section 21 recognizes the conflict between all measures necessary to ensure organs viability for transplantation and appropriate EOL care and requires the attending physician and OPO to resolve the conflict with the prospective donor or surrogate decision‐maker.9
OPOs apply donor management critical pathways to potential organ donors in order to maintain organ viability for successful execution of organ procurement.36 The University of Wisconsin developed a protocol and an evaluation tool to determine the eligibility of potential candidates for NHBOD.44 The protocol entails temporary discontinuation of mechanical ventilation for a trial of spontaneous respiration lasting up to 10 minutes to determine the likelihood of cardiorespiratory death within 60‐90 minutes of the withdrawal of life support. Those patients predicted by the University of Wisconsin evaluation tool to survive a longer time are not candidates for NHBOD and are transferred to palliative care. Those patients who meet the necessary criteria of the University of Wisconsin evaluation tool become candidates for NHBOD and undergo additional antemortem testing, invasive vascular instrumentation, and infusion of medications essential for organ preservation.36 The instrumentation and medications used for organ preservation can also expedite death on withdrawal of life support.45 Other interventions (such as circulatory support with invasive and noninvasive devices, extracorporeal perfusion and oxygenation, endotracheal reintubation, mechanical ventilation, and bronchoscopy) are performed when cardiorespiratory death is pronounced in order to maintain organ viability and can inadvertently reanimate the donor during the procurement process.26
The process of obtaining donation consent and subsequent donor management protocols for NHBOD deviate from more than 60% of the RWJF quality indicators recommended for optimal EOL care.35, 36, 41 Therefore, NHBOD can have a profound impact on the quality of EOL care. There has been a recent proposal to abbreviate the original RWJF quality indicators to include 14 of the 53 (26%) original quality indicators described for optimal EOL care in the ICU (Table 3).46 Many of the quality indicators expected to be negatively affected by NHBOD are not included in the proposal for an abbreviated list. There has been a concern that the application of an abbreviated rather than a comprehensive metrics for EOL care can portray an incomplete assessment and perhaps misinform donors and their families about the potential trade‐off in EOL care. The President's Council on Bioethics has emphasized that comprehensive evaluation of the quality of EOL care is an ethical imperative so that families can decide if the trade‐off is acceptable for organ donation.10 Deciding to donate organs at the end of life can be stressful for many families, and therefore they must be fully informed of the possible consequences. Posttraumatic stress disorders, anxiety, depression, and decreased quality of life have been reported in the deceased's family members who shared in stressful EOL decisions.47 Posttraumatic stress disorders have been reported in family members of deceased organ donors.48 Organ‐focused behavior by professionals requesting consent for organ donation and ambivalent decision making by family members appeared to increase the risk of relatives of deceased donors subsequently developing traumatic memories and stress disorders. The processes required for successful accomplishment of donation consent and subsequent organ recovery can interfere with many of the interventions that lessen the burden of bereavement of relatives of ICU decedents.49
The variability in decision making by health care providers about medical futility and EOL care has been given as a reason for concern about the implementation of NHBOD.50 The variability of EOL practice raises the possibility of conflicted decision making on medical futility within institutions that have transplant programs.50 Ethical conflicts and moral distress have been reported among health care providers who were directly involved in organ procurement in NHBOD.51 The pressure to recover transplantable organs from NHBOD candidates has been associated with health care professionals' perception of euthanasia and premature determination of medical futility and withdrawal of life support. The long‐term psychological impact of NHBOD practice on caregivers, health care providers, and professionals remains unknown.
CONCLUSIONS
In conclusion, NHBOD influences medical care at critical time points to maximize the procurement of transplantable organs and minimize their warm ischemia time with negative consequences on the EOL care for the prospective donors and their families (see Figure 1).
Mandatory implementation of NHBOD in the face of difficulties surrounding the quality of EOL care for donors raises concern across the medical profession and community. There is a need for better scientific validation of the timing of organ procurement to ensure that organ recovery is not the irreversible event defining death in NHBOD. The desire of OPOs or their affiliates to maximize recovery of transplantable organs introduces self‐serving bias into obtaining consent for organ donation and violates the basic tenet of true informed consent. The use of comprehensive quality indicators of EOL care will help to determine the impact of NHBOD on donors, families, caregivers, and health care providers.
In April 2003 the Health Resources and Services Administration of the U.S. Department of Health and Human Services (DHHS) announced the formation of the Organ Donation Breakthrough Collaborative (ODBC).1 The Organ Donation Breakthrough Collaborative created 58 national donation service areas (DSAs) to organize the transplant community across the United States. Each of the 58 organ procurement organizations (OPOs) is joined to a regional transplant center or centers and donor hospitals to form a DSA. The ODBC's goal is to achieve a cadaveric organ donation rate of 75% or higher from hospitals within each DSA.2
A requirement for organ donation from patients facing imminent or cardiac death has been introduced to increase the supply of transplantable organs and shorten the waiting time for transplantation candidates.35 This type of organ donation represents a significant source of organs required for future expansion of transplantation practice in the United States. The requirement for donation in imminent or cardiac death is implemented through the collaboration of the Advisory Committee on Organ Transplantation of the DHHS (Table 1), the Centers for Medicare & Medicaid Services (CMS), and the Joint Commission on Accreditation of Healthcare Organizations (JCAHO).3, 57 The organ donor pool of those facing imminent or cardiac death has also been expanded to include neurologically intact patients who may not fulfill brain death criteria before withdrawal of life support.4, 8, 9
| State law (year)* | |
|---|---|
| |
| Uniform Anatomical Gift Act (1968) | Any 18‐year‐old with a sound mind may donate his or her body after death to be used for medical research or as a source of transplantable tissues and organs and barring others from overriding a donor's decision to make an anatomical gift. |
| Amendment (1987) | Minors who can apply for a driver's license are empowered to make anatomical gifts, but either parent can revoke the gift if the minor dies before the age of 18. |
| Revision (2006) | Declaration of a gift does not require any witnesses. |
| Amendment (2007) | Document of a gift or donor registry is sufficient for the removal of organs, which means an OPO does not need consent of the spouse or the family. |
| Enables an OPO to gain access to documents of gifts in donor registries, medical records, and records of a state motor vehicle department. | |
| Facilitates donations by expanding the list of those who may make an anatomical gift for another individual who has not declared a preference for or against donation. | |
| Permits removal of organs by medical personnel without explicit consent from a potential donor or from a relative of the donor, so long as the appropriate medical personnel or authorities have made a reasonable effort to discover any objection by the donor or the donor's family. | |
| Require hospitals to notify an OPO or third party designated by the OPO of an individual whose death is imminent or who has died in the hospital in order to increase donation opportunity. | |
| Gives an OPO the right to inspect a patient's medical records. | |
| Measures necessary to ensure the medical suitability of a part not be withdrawn while an examination is being made to determine whether an individual who has been referred to OPO has a part that could be the subject of an anatomical gift. If, following such an examination, it is determined by the OPO that the individual has a part that could be the subject of an anatomical gift, the individual is a prospective donor under this act unless the individual had signed a refusal. | |
| Forbids the buying and selling of organs. | |
| Measures necessary to ensure the medical suitability of an organ for transplantation or therapy may not be withheld or withdrawn from a prospective donor who has an advance health‐care directive or declaration unless the directive or declaration expressly provides to the contrary. The section presumes that for prospective donors the desire to save lives by making an anatomical gift trumps the desire to have life support systems withheld or withdrawn. Individuals who desire to overcome this presumption can do so by express language in their advance health‐care directive or declaration. | |
| Uniform Determination of Death Act (1981) | An individual who has sustained either (1) irreversible cessation of circulatory and respiratory functions, or (2) irreversible cessation of all functions of the entire brain including the brain stem is dead. A determination of death must be made in accordance with accepted medical standards. |
| Federal laws | |
| National Organ Transplant Act (1984) | Calls for a unified transplant network to be operated by a private, nonprofit organization under federal contract and the establishment of a Task Force in Organ Procurement and Transplantation and an Organ Procurement and Transplantation Registry. |
| Public Health and Welfare Act Title 42 USC (1999) | |
| Section 273 | Establishes guidelines to be a qualified OPO that can receive federal grants. |
| Section 274 | Establishes the OPTN & Scientific Registry for Transplantation. |
| Federal regulations | |
| Title Code 42 CFR Part 121 (1999) | Lists regulations of the OPTN final rule. |
| Explains the OPTN structure. | |
| Lists the policy that the OPTN board of directors is responsible for developing. | |
| Explains rules that an OPTN member must obey when including a person on the organ waiting list. | |
| Describes the requirements and tests for determining the suitability of donated organs. | |
| Explains how the OPTN identifies an organ recipient, allocates the organ, and transports it to the recipient. | |
| Describes how the board of directors should develop allocation policies to guarantee they are both efficient and just and allocation performance goals to ensure the best possible use and most equitable allocation of organs. | |
| Lists designated transplant program requirements. | |
| Describes how the HHS conducts reviews and evaluations and enforces rules. | |
| Describes the recording and reporting requirements of the various groups involved in the transplantation process. | |
| Establishes the Advisory Committee on Organ Transplantation (ACOT), which advises the HHS secretary on organ donation, procurement, allocation, and transplantation The HHS secretary may ask for ACOT's opinion of proposed OPTN policies. | |
| Title Code 42 CFR Parts 413, 441, 486 and 498 (2006) | Lists regulations of the OPO final rule. |
| Establishes new conditions for coverage for OPOs that include multiple new outcome and process performance measures based on organ donor potential and other related factors in each donation service area of qualified OPOs. | |
The President's Council on Bioethics independently evaluated the issues surrounding deceased organ donation and procurement.10 The President's Council on Bioethics has expressed major concerns about several issues pertinent to cardiac or imminent death organ donation that have not been addressed explicitly by the bodies that have made recommendations for reforming or expanding that type of organ donation in the United States. The debate on organ procurement in imminent or cardiac death has come to the forefront because of doubts about its ethical appropriateness and acceptance within the medical profession and the community at large. This review focuses on the serious issues related to organ procurement from patients facing imminent or cardiac death.
Organ Procurement and the Dead Donor Rule
Organ procurement is only permitted when the donor is already dead (ie, the dead donor rule), and the act of organ recovery cannot have been the immediate act to cause that death.10, 11 There are 2 criteria for death as defined in the Uniform Determination of Death Act (UDDA; Table 1): an individual who has sustained irreversible cessation of either (1) circulatory and respiratory functions or (2) all functions of the entire brain, including the brain stem, is considered dead and this determination of death must have been made in accordance with accepted medical standards.12 When organs are procured from an individual in whom all brain function has ceased but normal cardiac pump activity is continuing, it is referred to as heart‐beating organ donation. Organ procurement after cessation of cardiac pump activity and cardiorespiratory functions is referred to as non‐heart‐beating organ donation (NHBOD). Organ procurement from an individual in imminent or cardiac death is considered NHBOD.
Non‐heart‐beating organ donors can be neurologically intact and do not fulfill the brain death criterion prior to cessation of cardiac pump activity. In response to this dilemma, the University of Pittsburgh Medical Centre developed a protocol for donation of organs that permitted their procurement from patients who were pulseless and apneic for 2 minutes and did not fulfill brain criteria and who had previously given consent for organ donation.13 Because it is uncertain if cessation of cardiorespiratory function is irreversible after only a short time, the Institute of Medicine (IOM) extended the time required for pulselessness and apnea from 2 to 5 minutes before permitting organ procurement.14 Waiting longer than 5 minutes for the determination of death would compromise the quality of procured organs because of warm ischemia time and would influence the functioning of grafts in transplant recipients.
One of the pivotal assumptions for NHBOD acceptance is that 5 minutes of pulselessness and apnea eliminates the possibility that the procurement process itself could be the cause of death and fulfills the dead donor rule.14, 15 The cardiorespiratory death criteria were derived from observations that did not evaluate delayed autoresuscitation (spontaneous return of circulation) or simultaneous cessation of brain electrical activity (as recorded in brain death).1618 The death criteria applied for organ procurement must also comply with the irreversibility requirement of the UDDA.11, 12
The true incidence, temporal characteristics, and predictors of autoresuscitation in humans remain unknown because of underreporting in the literature. However, there have been case reports of autoresuscitation with return of neurologic function (also called the Lazarus phenomenon) after 10 minutes of cardiac asystole.19, 20 Maleck et al. and Adhiyaman et al. described autoresuscitation 5 minutes or longer after cardiorespiratory arrest in 44% and 50% of the published case reports, respectively.19, 20 Although cardiac asystole leads to the loss of arterial pulse pressure, circulatory arterial mean pressure is maintained in diastole by arteriolar vasomotor tone. The relaxation (diastole) phase systemic arterial to venous pressure gradient provides the perfusion pressure for vital organs and the spontaneous return of circulation after circulatory arrest.21 It is likely that autoresuscitation occurs because of the persistence of circulatory vasomotor tone after cessation of cardiac function. The time course of systemic vascular tone after circulatory arrest has not been well characterized in humans. However, the IOM criteria did not account for the incidence of delayed autoresuscitation in humans even though the Maastricht protocol (developed by the University of Zurich, Zurich, Switzerland) acknowledged this phenomenon and required at least 10 minutes to elapse after cardiorespiratory arrest before starting organ procurement.22 The 10‐minute waiting time did not compromise the quality of the organs procured.
The cardiorespiratory death criteria for organ procurement also ignore cardiac electrical activity (such as pulseless electrical activity or ventricular fibrillation) on an electrocardiogram. Research with cardiac ultrasonography and indwelling arterial catheters confirms that pulseless cardiac electrical activity can be associated with cardiac mechanical contractions, although these contractions are too weak to be detected by blood pressure monitoring.23 The presence of cardiac electrical activity on an electrocardiogram can also increase the likelihood that delayed autoresuscitation will occur.19, 20 Furthermore, whether there is brain electrical activity or neurologic function when cardiac electrical activity is still observed on an electrocardiogram remains unknown.24 It can be argued that donors who have already suffered severe neurologic injury cannot have meaningful neurologic function at the time of cardiorespiratory death. However, the presence of brain activity becomes relevant for organ donors with intact neurologic and brain function prior to cardiorespiratory arrest when only cardiorespiratory criteria for organ procurement are being used.4, 8, 9
In situ circulatory support with extracorporeal perfusion in organ donors has also refuted that cardiorespiratory arrest for 5 minutes fulfills the UDDA requirement because reversibility can occur during the procurement process. In situ extracorporeal perfusion is initiated 5 minutes after cardiorespiratory arrest of donors in order to preserve organs for procurement.25 Coronary and cerebral reperfusion can lead to the return of cardiac and neurologic functions (also called reanimation) of donors during the procurement process. Mechanical occlusion of the aortic arch and pharmacological agents are required to suppress donor reanimation during organ procurement.26 Martin et al. documented that in situ extracorporeal perfusion returned full neurologic and cardiac function 25 minute after cardiorespiratory arrest that occurred outside the hospital.27 Similar observations of full neurologic recovery and survival to hospital discharge were reported after in situ extracorporeal perfusion for in‐hospital cardiorespiratory arrest.28 These observations confirm that the time required for irreversible loss of neurologic function after cessation of circulation is much longer than the 25 minutes of cardiorespiratory arrest required to begin the process of organ procurement in NHBOD.
The incidence of donor reanimation during procurement is unknown because its reporting violates the dead donor rule and can create legal concerns.11 It can be argued that reanimation of organ donors is irrelevant because it does not mean survival. However, the occurrence of reanimation invalidates the premise that the cardiorespiratory criteria for organ procurement comply with the uniform determination of death. Others have accepted the inaccuracy of these criteria for determining death for procurement of organs from deceased donors and proposed abandoning the dead donor rule in order to permit recovery of transplantable organs before death.29
In the face of the uncertainty in determining death and in response to a media and marketing campaign by organ procurement organizations (OPOs) to promote public enrollment in deceased organ donation, the transplant community renamed NHBOD cardiac death organ donation.30, 31 The use of the term cardiac death is scientifically inaccurate and perhaps misleading. This term is used to denote the cessation of circulation and cardiac pump activity. The term cardiac death can be misinterpreted as meaning the heart has irreversibly ceased at the time of procurement, thus contradicting the scientific evidence for spontaneous resumption of cardiac function and autoresuscitation.19, 20 Alternatively, the use of this term can falsely imply that neurologic activity or brain stem function has ceased irreversibly after loss of cardiac activity, when scientific evidence suggests that brain stem function can remain after cardiac arrest.32
Consent for Organ Donation
Several state laws and federal regulations have been enacted to ensure that organ donation and transplantation practice comply with the ethical and legal standards of society (Table 1). The current regulations require hospitals across the United States to provde regional OPOs with early notification of all patients whose deaths are imminent before life support has been withdrawn so that discussion of organ donation with surrogate decision makers can be initiated independently and consent obtained.3, 5, 9 The Organ Donation Breakthrough Collaborative has set a goal of each OPO accomplishing a target organ donation rate of 75% or higher at local hospitals within an assigned donation service area (DSA).1, 2, 5 The financial and administrative incentives for the OPO to achieve that target organ donation rate have introduced undisclosed conflict within the donation consent process.33 Self‐serving bias of OPOs can influence whether pertinent information necessary for surrogate decision makers to provide informed consent is disclosed.34 As an example of this bias, alternative options for care and palliation may be discussed with surrogate decision makers with less enthusiasm than are the benefits and altruistic notion of organ donation. In obtaining donation consent, OPOs often avoid disclosing details of perimortem interventions performed on donors that are required for successful procurement of transplantable organs.10, 34, 35 After receiving consent for organ donation, OPO staffs also assume the responsibility of planning donor medical care and treatment pathways essential for maintaining organ viability and of preparing for subsequent procurement.5, 36 In essence, the care of the dying patient is guided by a team whose primary interest is the preservation of organs until procurement has been accomplished.
The Uniform Anatomical Gift Act (UAGA) assigns explicit priority to the donor's expressed intent so that consent for organ donation becomes irrevocable and does not require the consent or concurrence of any person after the donor's death (Table 1).9, 37 The donor's authorization to donate, recorded on an organ donor card, the individual's driver's license, or a donor registry, becomes a legally binding advance directive. The UAGA amendment enables OPOs to procure organs without family consent and in certain instances after family refusal to donate.37
Other consent options for organ donation from deceased donors have been proposed to maximize OPO recovery of transplantable organs in the United States (Table 2).8 The IOM has considered presumed consent for organ donation as a favorable option.8 Presumed consent means the default option is consent to donation, that if an individual has not expressly rejected donation, that individual is considered to have consented to organ donation. Legislative enactment of presumed consent enables OPOs to avoid the potential for surrogates to deny consent for donation, thus increasing the pool of future organ donors. The revised UAGA replaces nondonation with the intent to donate organs as the default option. In the default option, all measures necessary to ensure the medical suitability of an organ for transplantation can not be withheld or withdrawn until the OPO has determined medical suitability of the individual as a prospective donor (Table 1). The default option overrides the expression of intent in a declaration or advance health‐care directives not to have life prolonged by withholding or withdrawing life support system unless the individual has expressed refusal of donation (Tables 1 and 2). The revised UAGA presumes that for prospective donors the desire to save lives by making an anatomical gift trumps the desire to have life support systems withheld or withdrawn. Mandated consent (or conscription) has also been proposed for recovery of cadaveric organs (Table 2).38 Under mandated consent, consent for organ donation is automatic from all deceased individuals; therefore, OPOs would not require or request consent because removal of all needed transplantable cadaveric organs would be compulsory. OPO staffs would no longer have to discuss organ procurement from potential donors with family members or other surrogates. An alternative form of donation consent is mandated choice, which requires each individual to decide in advance either to agree to organ donation or to refuse it. Mandated choice is the IOM's least favorite option because it would require extensive public informational programs on organ donation to facilitate individual choices and decision making (Table 2).8
| Type | Description |
|---|---|
| Requested (expressed) consent | An individual is asked to voluntarily agree to organ donation. |
| Presumed (implied) consent | Unless an individual has expressly refused to donate organs, the default option is agreement to donate organs. |
| Mandated consent (conscription) | An individual is not required to decide on organ donation before death, and there is an automatic right to procure organs from any and all deceased individuals. |
| Mandated choice | An individual must choose between 2 options before death: agreement or refusal to donate organs. |
End‐of‐Life Care
Quality of end‐of‐life (EOL) care for an organ donor, as for any individual whose treatment is being withdrawn, is considered the highest priority of care and must not be compromised by the donation process. Yet no studies have investigated the impact of organ donation on the quality of EOL care in NHBOD.35 Previous reports have criticized the quality of EOL care offered to dying patients in intensive care units (ICUs).39, 40 Many of these patients are undergoing withdrawal of life support in anticipation of death and are considered candidates for NHBOD. The Robert Wood Johnson Foundation (RWJF) Critical Care End‐Of‐Life Peer Workgroup developed 53 EOL quality indicators to standardize and measure the quality of EOL care.41 These quality indicators, organized in 7 domains, focus on delivering patient‐ and family‐centered care and facilitating a good death experience in the ICU (Table 3).
| Domains of comprehensive quality indicators of EOLC (n = 53)41 | Abbreviated quality indicators of EOLC (n = 18)46 |
|---|---|
| |
| Patient and family‐centered decision making (n = 13) | |
| Recognize the patient and family as the unit of care | |
| Assess the patient's and family's decision‐making style and preferences | |
| Address conflicts in decision making within the family | |
| Assess, together with appropriate clinical consultants, the patient's capacity to participate in decision making about treatment and document assessment | Assessment of the patient's decisional capacity |
| Initiate advance care planning with the patient and family | |
| Clarify and document the status of the patient's advance directive | Documentation of the presence and, if present, contents of advance directives |
| Identify the healthcare proxy or surrogate decision maker | Documentation of a surrogate decision maker within 24 hours of admission |
| Clarify and document resuscitation orders | |
| Assure patients and families that decision making by the health care team will incorporate their preferences | |
| Follow ethical and legal guidelines for patients who lack both capacity to make decisions and a surrogate decision maker | |
| Establish and document clear, realistic, and appropriate goals of care in consultation with the patient and family | Documentation of the goals of care |
| Help the patient and family assess the benefits and burdens of alternative treatment choices as the patient's condition changes | |
| Forgo life‐sustaining treatments in a way that ensures patient and family preferences are elicited and respected | |
| Communication within the team and with patients and families (n = 10) | |
| Meet as interdisciplinary team to discuss the patient's condition, clarify goals of treatment, and identify the patient's and family's needs and preferences | Documentation of a timely interdisciplinary clinicianfamily conference |
| Address conflicts among the clinical team before meeting with the patient and/or family | |
| Utilize expert clinical, ethical, and spiritual consultants when appropriate | |
| Recognize the adaptations in communication strategy required for patients and families according to the chronic versus acute nature of the illness, cultural and spiritual differences, and other influences | |
| Meet with the patient and/or family on a regular basis to review patient's status and to answer questions | Documentation of timely physician communication with the family |
| Communicate all information to the patient and family, including distressing news, in a clear, sensitive, unhurried manner and in an appropriate setting | |
| Clarify the patient's and family's understanding of the patient's condition and goals of care at the beginning and end of each meeting | |
| Designate primary clinical liaison(s) who will communicate with the family daily | |
| Identify a family member who will serve as the contact person for the family | |
| Prepare the patient and family for the dying process | |
| Continuity of care (n = 3) | |
| Maximize continuity of care across clinicians, consultants, and settings | |
| Orient new clinicians to the status of the patient and family | Transmission of key information with transfer of the patient out of the ICU |
| Policy for continuity of nursing services | |
| Prepare the patient and/or family for a change of clinician(s) and introduce new clinicians | |
| Emotional and practical support for patients and families (n = 8) | |
| Elicit and attend to the needs of the dying person and his/her family | |
| Distribute written material (booklet) for families that includes orientation to the ICU environment and open visitation guidelines, logistical information (nearby hotels, banks, restaurants, directions), listings of financial consultation services, and bereavement programs and resources | Open visitation policy for family members |
| Facilitate strengthening of patientfamily relationships and communication | |
| Maximize privacy of the patient and family | |
| Value and support the patient's and family's cultural traditions | |
| Arrange for social support for patients who do not have family or friends | Documentation that psychosocial support has been offered |
| Distribute written material (booklet) containing essential logistical information and listings of financial consultation services and bereavement support programs/resources | |
| Support family members through the patient's death and their bereavement | |
| Symptom management and comfort care (n = 10) | |
| Emphasize the comprehensive comfort care that will be provided to the patient rather than the removal of life‐sustaining treatments | |
| Institute and use uniform quantitative symptom assessment scales appropriate for communicative and noncommunicative patients on a routine basis | Documentation of pain assessment |
| Documentation of respiratory distress assessment | |
| Standardize and follow best clinical practices for symptom management | Protocol for analgesia/sedation in terminal withdrawal of mechanical ventilation |
| Appropriate medications available during withdrawal of mechanical ventilation | |
| Use nonpharmacologic as well as pharmacologic measures to maximize comfort as appropriate and desired by the patient and family | |
| Reassess and document symptoms following interventions | Documentation of pain management |
| Documentation of respiratory distress management | |
| Know and follow best clinical practices for withdrawing life‐sustaining treatments to avoid patient and family distress | |
| Eliminate unnecessary tests and procedures (laboratory work, weights, routine vital signs) and only maintain intravenous catheters for symptom management when life support is being withdrawn | |
| Minimize noxious stimuli (monitors, strong lights) | |
| Attend to patient's appearance and hygiene | |
| Ensure family's and/or clinician's presence so the patient is not dying alone | |
| Spiritual support for patients and families (n = 3) | |
| Assess and document spiritual needs of the patient and family on an ongoing basis | Documentation that spiritual support was offered |
| Encourage access to spiritual resources | |
| Elicit and facilitate spiritual and cultural practices that the patient and family find comforting | |
| Emotional and organizational support for ICU clinicians (n = 6) | |
| Support health care team colleagues caring for dying patients | Opportunity to review experience of caring for dying patients by ICU clinicians |
| Adjust nursing staff and medical rotation schedules to maximize continuity of care providers for dying patients | |
| Communicate regularly with interdisciplinary team about goals of care | |
| Establish a staff support group, based on the input and needs of ICU staff and experienced group facilitators, and integrate meeting times into the routine of the ICU | |
| Enlist palliative care experts, pastoral care representatives, and other consultants to teach and model aspects of EOLC | |
| Facilitate rituals for the staff to mark the death of patients | |
| Strategies to improve EOLC and provide a good death42, 43 | |
| EOL care quality monitoring | |
| Making environmental changes to promote dying with dignity | |
| Managing patients' pain and discomfort | |
| Knowing and following patients' wishes for end‐of‐life care | |
| Bereavement program or service | |
| Regular meetings of senior ICU physician and nurse with patients' families | |
| Training of ICU clinicians in end‐of‐life communication skills | |
| Role modeling and supervision of trainees by clinicians experienced in end‐of‐life care | |
| Formal mechanism for emotional support of staff caring for dying patients | |
| Access to palliative care consultants | |
| Training of ICU clinicians in symptom management | |
| Scheduling staff to promote continuity of care for dying patients | |
| Formal system for scaled assessment and charting of patients' symptoms | |
| Method to help resolve differences about appropriate care goals | |
| Resources to accommodate diversity among patients/families at the end of life | |
| Access to clinical ethics consultants | |
| Regular pastoral care visits to the ICU | |
In a subsequent U.S. survey, the Critical Care Peer Workgroup of the Promoting Excellence in End‐of‐Life Care Project reported that more than 75% of ICUs were still not monitoring the quality of EOL care.42 The survey also identified multiple barriers to optimal EOL care found in most ICUs. The study group proposed several strategies to overcome these barriers and improve the quality of EOL care (Table 3).42, 43 It can also be inferred from the survey findings that most ICUs are unprepared and lack the necessary tools to appropriately inform patients and families of the trade‐off in EOL care for NHBOD. The President's Council for Bioethics has also warned that NHBOD can transform EOL care from a peaceful dignified death into a profanely high‐tech death experience for donors' families.10
Several aspects of medical care that are neither palliative nor beneficial are performed for donor management for NHBOD and can explain the feared transformation of the death experience. The revised UAGA reaffirms that all measures necessary to ensure the medical suitability of an organ for transplantation cannot be withheld or withdrawn from the prospective donor and overrides the expression of intent by a prospective donor in either a declaration or advance health‐care directive not to have life prolonged by use of life support systems (Table 1).9 The 2007 amendment to revised UAGA section 21 recognizes the conflict between all measures necessary to ensure organs viability for transplantation and appropriate EOL care and requires the attending physician and OPO to resolve the conflict with the prospective donor or surrogate decision‐maker.9
OPOs apply donor management critical pathways to potential organ donors in order to maintain organ viability for successful execution of organ procurement.36 The University of Wisconsin developed a protocol and an evaluation tool to determine the eligibility of potential candidates for NHBOD.44 The protocol entails temporary discontinuation of mechanical ventilation for a trial of spontaneous respiration lasting up to 10 minutes to determine the likelihood of cardiorespiratory death within 60‐90 minutes of the withdrawal of life support. Those patients predicted by the University of Wisconsin evaluation tool to survive a longer time are not candidates for NHBOD and are transferred to palliative care. Those patients who meet the necessary criteria of the University of Wisconsin evaluation tool become candidates for NHBOD and undergo additional antemortem testing, invasive vascular instrumentation, and infusion of medications essential for organ preservation.36 The instrumentation and medications used for organ preservation can also expedite death on withdrawal of life support.45 Other interventions (such as circulatory support with invasive and noninvasive devices, extracorporeal perfusion and oxygenation, endotracheal reintubation, mechanical ventilation, and bronchoscopy) are performed when cardiorespiratory death is pronounced in order to maintain organ viability and can inadvertently reanimate the donor during the procurement process.26
The process of obtaining donation consent and subsequent donor management protocols for NHBOD deviate from more than 60% of the RWJF quality indicators recommended for optimal EOL care.35, 36, 41 Therefore, NHBOD can have a profound impact on the quality of EOL care. There has been a recent proposal to abbreviate the original RWJF quality indicators to include 14 of the 53 (26%) original quality indicators described for optimal EOL care in the ICU (Table 3).46 Many of the quality indicators expected to be negatively affected by NHBOD are not included in the proposal for an abbreviated list. There has been a concern that the application of an abbreviated rather than a comprehensive metrics for EOL care can portray an incomplete assessment and perhaps misinform donors and their families about the potential trade‐off in EOL care. The President's Council on Bioethics has emphasized that comprehensive evaluation of the quality of EOL care is an ethical imperative so that families can decide if the trade‐off is acceptable for organ donation.10 Deciding to donate organs at the end of life can be stressful for many families, and therefore they must be fully informed of the possible consequences. Posttraumatic stress disorders, anxiety, depression, and decreased quality of life have been reported in the deceased's family members who shared in stressful EOL decisions.47 Posttraumatic stress disorders have been reported in family members of deceased organ donors.48 Organ‐focused behavior by professionals requesting consent for organ donation and ambivalent decision making by family members appeared to increase the risk of relatives of deceased donors subsequently developing traumatic memories and stress disorders. The processes required for successful accomplishment of donation consent and subsequent organ recovery can interfere with many of the interventions that lessen the burden of bereavement of relatives of ICU decedents.49
The variability in decision making by health care providers about medical futility and EOL care has been given as a reason for concern about the implementation of NHBOD.50 The variability of EOL practice raises the possibility of conflicted decision making on medical futility within institutions that have transplant programs.50 Ethical conflicts and moral distress have been reported among health care providers who were directly involved in organ procurement in NHBOD.51 The pressure to recover transplantable organs from NHBOD candidates has been associated with health care professionals' perception of euthanasia and premature determination of medical futility and withdrawal of life support. The long‐term psychological impact of NHBOD practice on caregivers, health care providers, and professionals remains unknown.
CONCLUSIONS
In conclusion, NHBOD influences medical care at critical time points to maximize the procurement of transplantable organs and minimize their warm ischemia time with negative consequences on the EOL care for the prospective donors and their families (see Figure 1).
Mandatory implementation of NHBOD in the face of difficulties surrounding the quality of EOL care for donors raises concern across the medical profession and community. There is a need for better scientific validation of the timing of organ procurement to ensure that organ recovery is not the irreversible event defining death in NHBOD. The desire of OPOs or their affiliates to maximize recovery of transplantable organs introduces self‐serving bias into obtaining consent for organ donation and violates the basic tenet of true informed consent. The use of comprehensive quality indicators of EOL care will help to determine the impact of NHBOD on donors, families, caregivers, and health care providers.
- ,,, et al.Organ donation and utilization, 1995‐2004: Entering the collaborative era.Am J Transplant.2006;6:1101–1110.
- U.S. Department of Health and Human Servcies—Organ Donation and Transplant Breakthrough Collaborative. Measurement strategy: Organ Donation and Transplant Breakthrough Collaborative. Available at: http://www.organdonationnow.org/. Accessed December 15,2006.
- U.S. Department of Health and Human Services Advisory Committee on Organ Transplantation. Consensus Recommendations to the HHS Secretary. Available at: http://www.organdonor.gov/research/acot.htm. Accessed January 30,2007.
- ,,, et al.Report of a National Conference on Donation after Cardiac Death.Am J Transplant.2006;6:281–291.
- Centers for Medicare and Medicaid Services, Department of Health and Human Services.Medicare and Medicaid Programs. Conditions for coverage for organ procurement organizations (OPOs); final rule.Federal Register.2006;71:30981–31054.
- [JCAHO] Joint Commission on Accreditation of Healthcare Organizations. Health care at the crossroads: strategies for narrowing the organ donation gap and protecting patients. Available at: http://www.jointcommission.org/PublicPolicy/organ_donation.htm. Accessed January 30,2007.
- [JCAHO] Joint Commission on Accreditation of Healthcare Organizations.Revisions to Standard LD.3.110.Jt Comm Perspect.2006;26:7.
- Committee on Increasing Rates of Organ Donation‐Board on Health Sciences Policy‐Institute of Medicine.Organ Donation: Opportunities for Action.Washington, DC:National Academies Press;2006.
- National Conference of Commissioners on Uniform State Laws. Revised Uniform Anatomical Gift Act (2006) and Amendment to Section 21 (2007). http://www.law.upenn.edu/bll/ulc/uaga/2006final.htm and http://www.anatomicalgiftact.org/DesktopDefault.aspx?tabindex=0
- ,,, et al.Organ donation and utilization, 1995‐2004: Entering the collaborative era.Am J Transplant.2006;6:1101–1110.
- U.S. Department of Health and Human Servcies—Organ Donation and Transplant Breakthrough Collaborative. Measurement strategy: Organ Donation and Transplant Breakthrough Collaborative. Available at: http://www.organdonationnow.org/. Accessed December 15,2006.
- U.S. Department of Health and Human Services Advisory Committee on Organ Transplantation. Consensus Recommendations to the HHS Secretary. Available at: http://www.organdonor.gov/research/acot.htm. Accessed January 30,2007.
- ,,, et al.Report of a National Conference on Donation after Cardiac Death.Am J Transplant.2006;6:281–291.
- Centers for Medicare and Medicaid Services, Department of Health and Human Services.Medicare and Medicaid Programs. Conditions for coverage for organ procurement organizations (OPOs); final rule.Federal Register.2006;71:30981–31054.
- [JCAHO] Joint Commission on Accreditation of Healthcare Organizations. Health care at the crossroads: strategies for narrowing the organ donation gap and protecting patients. Available at: http://www.jointcommission.org/PublicPolicy/organ_donation.htm. Accessed January 30,2007.
- [JCAHO] Joint Commission on Accreditation of Healthcare Organizations.Revisions to Standard LD.3.110.Jt Comm Perspect.2006;26:7.
- Committee on Increasing Rates of Organ Donation‐Board on Health Sciences Policy‐Institute of Medicine.Organ Donation: Opportunities for Action.Washington, DC:National Academies Press;2006.
- National Conference of Commissioners on Uniform State Laws. Revised Uniform Anatomical Gift Act (2006) and Amendment to Section 21 (2007). http://www.law.upenn.edu/bll/ulc/uaga/2006final.htm and http://www.anatomicalgiftact.org/DesktopDefault.aspx?tabindex=0
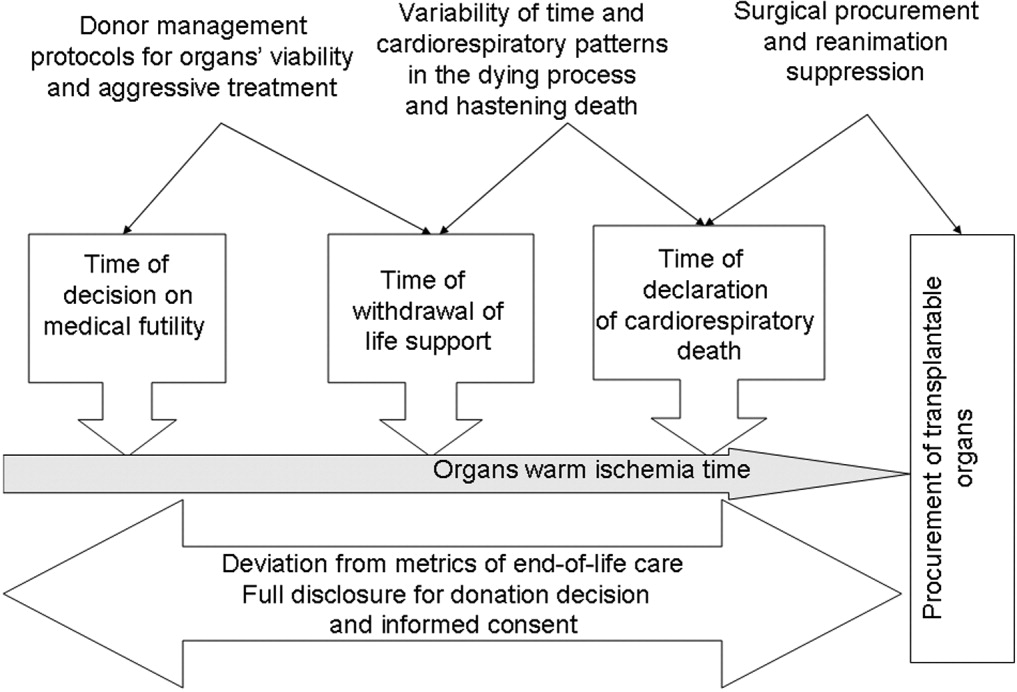
Barriers to Mobility During Hospitalization
The adverse outcomes associated with hospitalization of older patients, such as functional decline and increased nursing home placement, have been well documented.19 Low mobility, defined as being limited to a bed or chair, has also been associated with these adverse outcomes, even after controlling for severity of illness.10 Early ambulation has been a common practice for years following many types of orthopedic operations, including hip fracture repair and total joint replacement.11, 12 A recent study demonstrated that time to ambulation after surgery was an independent predictor of the development of postoperative complications such as pneumonia and delirium.13
In the early 1980s, early ambulation became the cornerstone of cardiac rehabilitation after acute myocardial infarction.14, 15 Until recently, with the exception of postmyocardial infarction, the use of early ambulation for patients admitted with medical illnesses has not been studied. In the last few years, researchers have begun to explore the use of early ambulation for patients after cardiac catheterization and for those admitted with deep‐vein thrombosis and pneumonia.1620 Although many of these studies have been small, they have found early ambulation not to be associated with worse outcomes. Indeed, a study of early ambulation for patients with community‐acquired pneumonia demonstrated decreased hospital costs and increased functional ability prior to discharge.20
Although the literature documents the adverse consequences associated with bed rest2123 and the beneficial effects of early ambulation, patients continue to spend a significant amount of their hospital stay limited to a bed or a chair. The prevalence of low mobility in older patients ranges from 23% to 33% during hospitalization for medical illness.9, 10 Despite the high prevalence and the associated adverse outcomes of low mobility among hospitalized older adults, the factors associated with low mobility in the hospital setting have not been systematically explored. Identification of such factors is the first step toward recognizing potentially modifiable factors and developing targeted interventions to improve hospital care.
We conceptualized a variety of factors or barriers that could potentially affect the level of mobility achieved by older hospitalized patients. Using professional experience and expert opinion, a conceptual model of potential barriers to mobility was developed (Fig. 1). As Figure 1 illustrates, the model has 4 major categories: patient‐related factors, including illness severity or comorbid conditions; treatment‐related factors such as catheters and intravenous lines; institution‐related factors such as nursing‐to‐patient ratio; and attitudinal factors related to perspectives on mobility and concerns about falling. This model was reviewed and feedback provided by a multidisciplinary group of colleagues including physicians, nurses, physical therapists, medical educators, and medical sociologists.
The objectives of this study were to employ qualitative methodology to identify and contextualize perceived barriers to mobility during hospitalization from the perspectives of older patients, their primary nurses, and their resident physicians; to compare and contrast the perceived barriers among these 3 groups; and to compare perceived barriers to mobility with our conceptual model.
METHODS
Setting and Patients
Patients aged 75 years admitted to the medical wards of the University Hospital either directly or through the Emergency Department were recruited for this study. In addition, the primary nurses and resident physicians of enrolled patients were also recruited because of their roles in providing hands‐on care to these patients in the university hospital setting. This project was supported in part by a VA Research Career Development Award and a training support grant from the Hartford Foundationfunded Southeast Center of Excellence in Geriatric Medicine. Written informed consent for participation was obtained from the patients, their nurses, and their resident physicians according to procedures approved by the Institutional Review Board of the University of Alabama at Birmingham. Recruitment was continued until no new barriers to hospital mobility were identified and data saturation was achieved. In all, 29 persons were enrolled: 10 patients, 10 nurses, and 9 physicians.
Patient exclusion criteria included factors that made it difficult for an individual to participate in the interview and to self‐report on mobility: (1) inability to be interviewed (ie, obtunded, aphasic), (2) a significant language barrier, requiring a translator, (3) Mini Mental State Examination Score24 < 16, (4) delirium at the time of the interview as documented by the Confusion Assessment Method (CAM)25, and (5) self‐reported inability to ambulate or transfer 2 weeks prior to hospital admission; Additional exclusion criteria were (6) previous enrollment in the study by the patient, the primary nurse, or the physician; and (7) refusal by patient, family, or physician to participate.
Questionnaire Development
A semistructured interview guide approach was used to encourage participants to discuss their perception of barriers to mobility during hospitalization. Pilot testing at a local retirement center was used to revise the initial patient questionnaire. Domains of inquiry were identified through the pilot testing and based on the conceptualized model (Fig. 1). These domains included attitudes toward mobility, expectations of care regarding walking/mobility, patient‐related factors that influence mobility, situational factors that influence mobility, and specific perceived barriers to mobility. Similar but not identical questions were used for patients and health care providers so answers could be compared between participant subgroups. For example, patients were asked, What might make it easier for you to get out of bed and walk more frequently or for longer periods than you are now? and health care providers were asked, What would make it easier for the patient to get out of bed and walk more frequently or for longer periods of time? Responses were categorized as being spontaneous or prompted depending on how the responses were elicited. Spontaneous responses about mobility barriers were elicited during general questioning about the hospital stay; for example: Tell me what you think about getting out of bed and moving around during this hospitalization? Prompted responses were elicited by asking a specific question about a potential barrier: Do you have any concerns about falling during your hospital stay?
Data Analysis
Interviews were conducted by the principal investigator (PI) between September 2004 and January 2005. Using an iterative approach, analysis began after the first interview with emerging themes being explored in subsequent interviews. All interviews were audiotaped and transcribed verbatim by a medical transcriptionist. Each participant was assigned a unique identifier. Interviews were reviewed by the PI to verify content. Participants were also given an opportunity to review the content of their interviews, with 76% choosing to do this. Using the grounded theory approach, an analytic technique that systematically analyzes raw interview data to generate hypotheses and develop theory; the data were analyzed by generating categories and themes.26
Interviews were independently reviewed and coded by the research assistant and the PI, with a third reviewer available to resolve disputes throughout the analyses. Initially, reviewers coded any item they believed to fit the category of barriers. Discrepancies between reviewers led to review of the original data to determine if the item could be considered a barrier. This process continued until the reviewers were in agreement about what to include as a barrier. Next, the themes generated by the coders were compared. Any discrepancies again led to review of the original data and revision of themes as indicated. This process continued until agreement was achieved for categories and themes between the coders for each of the 29 interviews. Independent themes were identified and counted and are presented as percentages for the purpose of comparing and contrasting between groups.
RESULTS
Fifty‐seven patients age 75 years were admitted to the medical service during the study period. Of those, 18 were excluded because they were too ill according to their physician (n = 6), had a nonmedical illness (n = 5), were discharged before being interviewed (n = 3), or were being cared for by a previously enrolled nurse or physician (n = 4). Of the 39 who were eligible for the study, 7 declined participation (6 patients, 1 physician), and data were lost for 3 as a result of technical difficulties with the tape recorder. A total of 29 participants had an interview transcribed: 10 patients, 10 nurses, and 9 physicians. As in other qualitative inquiries, data saturation was achieved after about 10 interviews,27 but we continued recruitment to permit comparison of themes identified by patients, nurses, and physicians.
Table 1 presents baseline characteristics of the patients. The mean age of the nurses was 34.9 9.9 years, all were female, and 60% were black. The mean age of the resident physicians was 29.1 2.2 years; 44% were female; and 78% were white, 22% were Latino, and none were black.
| Characteristic | Mean (SD) or N (%) |
|---|---|
| Age (years) | 84 (6.0) |
| Sex Male | 3 (30) |
| Female | 7 (70) |
| Race Black | 3 (30) |
| White | 7 (70) |
| Mini Mental State Examination score | 24 (3.3) |
| Number of comorbidities | 6 (2.3) |
| Number of medications at admission | 9 (2.3) |
Figure 2 presents barriers most frequently noted by participants. These barriers were similar among the 3 groups for symptoms and hospital‐related factors like catheters and lack of staff. Lack of patient motivation, lack of ambulatory devices, and medical reasons necessitating bed rest were reported more frequently by health care providers than by patients. On admission, 40% of patients had bed rest ordered. By hospital day 3, all patients had out‐of‐bed orders, and 70% had had physical therapy ordered.
Symptoms
Symptoms were spontaneously mentioned by 97% of participants (28 of 29) as a cause of limited mobility, with weakness cited most frequently: I know it is going to be painful (to walk). My head swims. This side of my all up and down to my toes is weak. When that comes, you kind of be scared. Pain and fatigue were also mentioned by more than 35% of all participants. Although 42% of health care providers (8 of 19) identified dyspnea or shortness of breath as a barrier, no patients reported this symptom as a barrier.
Medical Devices
When asked directly about the impact of urinary catheters and intravenous lines, most patients expressed the belief that the device could either be disconnected or carried and therefore was not a barrier: They can take that off [the catheter] and hook it on the wall. Only 30% of the patients described their mobility as hampered by the medical devices, and only 1 patient (10%) spontaneously indicated the catheter was a barrier: I have had that catheter hooked up to me until today. That was a relief to get that outI couldn't hardly do nothing with that.
In contrast, most health care providers (89%) believed medical devices adversely affected mobility. However, only 32% spontaneously noted the IV or catheter was a barrier, with the other 67% requiring prompting to consider the medical devices as barriers. The rationale for this belief varied widely. Some providers focused on the impact of the patient having to push the IV pole: They get tangled, they hurt when they are mobilized. You have to push the little cart, so patients actually need some assistance. Other providers mentioned the impact of a patient's medical devices on the nurse's ability to assist patients out of bed: I hate to say it, but I think on some days, it does [affect mobility]. You have patients who have TPN and blood and Foleys and chest tubes, you are probably less likely to [get people out of bed]. One physician commented on a less obvious impact of catheters: Some people might be embarrassed to walk around with that Foley catheter.
Need for Assistance and Lack of Staff
Patients, nurses, and physicians alike spontaneously identified the patient's need for assistance with ambulation as a barrier. This observation was frequently followed by comments about staff shortages and time constraints that limited the availability of staff to assist patients with ambulation. The impact of a perceived lack of staff was expressed differently by patients and health care providers. Patients frequently talked about not wanting to bother the nurses: I know it would be good for me, but I just don't want to impose upon them; I try not to worry the girls to take me walking because they have their own patients. Health care providers focused on the variety of other nursing duties that tended to take precedence over helping patients with mobility: I just don't think the nurses have time. They are too busy doing other things to walk their patients up and down the hallway. I think if you really want your patient up walking down the hall, you need to have a relative help them or physical therapy. Among staff, the most frequently mentioned solution was to refer patients to physical therapy, a strategy endorsed equally by nurses and physicians: That is why we try to encourage the doctors to order physical therapy, because we don't have time to ambulate patients in the hallway like the doctor expects.
Lack of Ambulatory Devices
The nurses frequently mentioned the absence of ambulatory devices to assist patients with walking. Nurses also expressed concern about the ability of patients to walk safely without such devices: Sometimes if a patient requires a lot of help, then I think you really need to involve physical therapy to ensure the safety of the person getting up. Because a lot of times you are limited with equipment that you need and they [physical therapists] have that equipment to make sure they don't fall. No physicians and only 1 patient cited lack of ambulatory devices as a barrier to mobility.
Fear of a Patient Falling
The potential for a fall during a hospital stay was of concern for more than 75% of the participants, with physicians spontaneously expressing concern for falls as a perceived barrier more frequently than did patients or nurses: I probably don't encourage her to move as much as I should. And when I do, I tell her to be sure to have someone with her when she is getting up. I am probably a little more protective because I am afraid she might fall. Another physician stated, I think nurses in general would prefer the patient to stay in bed. I believe they perceive it as a risk for falls and a risk for pulling out their IVs or any other medical device, and it is probably not viewed as an important factor in someone who is recovering from an illness. Another physician noted fall prevention was a secondary reason for limited mobility but also expressed the idea that bed rest was easier than mobility: While they are in bed they are not giving trouble to anybody. It is less work and, second, because of liability issues in terms of patients falling and hurting themselves while they are in the hospital. I think everybody is very concerned with that, but I think mainly because it is less work. Although 68% of health care providers spontaneously noted falls as a barrier to mobility, only 1 patient spontaneously verbalized this concern. However, with prompting to consider falls a barrier, 60% of patients stated falls were a potential barrier: As old as I am, your legs don't last long and they give away. It would be dangerous because I haven't got the strength. Now, since I've fallen, yes, I have to be careful.
Lack of Patient Motivation
Lack of patient motivation was mentioned by 50% of the nurses and 78% of the physicians and was often linked to a patient's age: I just think he is older now, and he is not as motivated as younger people are, and he has been through so much. I just don't think he wants to do it. I don't know if it is because it is the elderly or because they just seem more stubborn. They are sometimes more content to stay in the bed, and you have to really stress to them to get up. However, none of the patients indicated a lack of motivation was the reason for not getting out of bed. Indeed, they commented on the staff's apparent lack of interest or their perception that the staff did not consider increased mobility important: I don't believe they are going to get me out of bed while I am here. If I said I really needed to get out of bed, they try to do what you want them to do. But evidently they don't think it is that important.
Hospital Environment
Although not frequently mentioned, issues of an environment not conducive to mobility did emerge as a theme. Several patients expressed this environmental barrier as a difficulty with the hospital gowns that are required garb during a hospital stay. One patient wrote the following additional thoughts after reviewing her transcript: Gowns lead to embarrassing moments, are designed for benefit of staff, not patients. This sentiment was echoed by a physician who, when queried about the impact of gowns, responded, I think the gown exposes the patient a lot and they might feel embarrassed to go around. And outside the hospital room, nobody wants to be perceived as sick and draw attention. Finally, 2 physicians commented on the lack of chairs in the room and the physical setup of the room not encouraging mobility: I think that patients, when they are in the hospital, they feel they are supposed to be in bed. And they are more comfortable there and a lot of times they can see the TV better.
DISCUSSION
Many of the barriers described in the original conceptual model (Fig. 1) were cited by participants from all 3 groups: patients, nurses and physicians. These included patient‐related factors like symptoms and need for assistance, concern about falls, and lack of staff to assist with ambulation. Although attitudes toward mobility were cited in the model and by participants, there was significant disagreement between the 3 groups about the cause of the attitudinal barrier. Health care providers cited lack of patient motivation, whereas patients perceived health care providers as not being interested in mobility or viewing it as important. Health care providers frequently employed stereotypes to describe the potential reasons for the perceived attitudes toward mobility, often linking lack of motivation or interest in getting out of bed to patients being old. Patients linked the lack of importance attached to mobility to the numerous duties of staff members and believed that assistance with mobility was less important than other duties. Physicians and nurses were both more likely than patients to mention factors like urinary catheters, intravenous lines, and other medical reasons that necessitated bed rest. Although more than half the nurses commented on the lack of ambulatory devices for ambulation, no physicians and only 1 patient perceived this lack to be a barrier.
The model presented appears to have face validity, with participants citing many of the factors originally identified as barriers to mobility. The original model did not include consideration of environmental factors such as the number of chairs in the room or the location of the television. Such environmental factors can be conceptualized as institution‐related factors.
In addition, the impact of physician activity orders for bed rest was not specifically discussed by participants, although 45% of participants did comment on the need for bed rest because of a medical condition. A review of the medical records for activity orders indicated 40% of the patients initially had orders for bed rest. Another recent study demonstrated 33% of older patients were on bed rest at some point during their hospital stay10 and should be retained in the model as a treatment‐related consideration.
Several barriers noted in the original model and by participants may not be modifiable, such as comorbid conditions and illness severity. But other perceived barriers may be, and recognition of these factors present potential targets for a future multicomponent intervention to enhance hospital mobility. This multicomponent approach has been highly successful for geriatric syndromes like falls28 and delirium.29
During hospitalization, a focus on early removal of catheters and intravenous lines may encourage mobility. In a recent study absence of a urinary catheter was a predictor of patients with activity limitations regaining ambulatory ability while hospitalized.30 Availability of ambulatory devices may allow nurses to ambulate patients without consulting physical therapy. Another potential solution would be a hospitalwide walking program. The feasibility of a walking program was demonstrated in a small pilot study at a community‐based hospital using specially trained transporters to walk ward patients during slow periods. These periods included nights and weekends, when patients were more likely to be available and when physical therapy was often not present. On average, participants spent 2.4 days in the program, with an average of 5.6 walks per patient. However, additional research is needed, as the study was too small to demonstrate the effects of the walking program on length of stay or functional decline.31
Other barriers, while potentially modifiable, may be more difficult to address and may involve changing the culture of the hospital. For instance, concern about falls was a common theme, echoed by all 3 groups. Physicians were the most likely to spontaneously mention falls as a concern. The nurses shared this concern, frequently citing the use of bed rails as a part of their fall protocol, despite available literature demonstrating that this approach was not efficacious.3234 Nurses also consistently reported asking patients to call for help to ambulate, yet both patients and nurses noted a lack of nursing time to assist with ambulation. The default solution providers reported using was utilizing physical therapists, who were available to walk with patients only once or twice a day. Research on the best methods to prevent falls during hospitalization is limited. Given the current medicolegal environment and the emphasis on fall prevention by the Joint Commission on Accreditation of Healthcare Organizations and other government entities, it is not surprising that bed rest and mobility limitation are being used as a method of minimizing falls. Until data about successful fall‐prevention strategies are available, minimization of mobility may remain the default solution.
Strengths of the present study include the use of qualitative methods to explore potential barriers to mobility, a method that allows participants to describe in their own words their attitudes, beliefs, and expectations about mobility during hospitalization. Face‐to‐face interviewing of the 3 major groups involved in the hospital experience (patients, nurses, and physicians) facilitated the collection of detailed contextualized information on factors expected to affect a patient's level of mobility during hospitalization. This enabled hypothesis generation and sensitization to issues that need further quantitative investigation with larger groups.
The study also had several limitations. First, only resident physicians were included, and their answers may not reflect the opinions of other, more experienced physicians. However, resident physicians were chosen for this study because they play important roles in delivering hands‐on care in teaching hospitals and would need to be involved in any future interventions designed to enhanced patient mobility. Second, a sample size of 29 participants, approximately 10 persons in each group, may not reflect the thinking of those throughout the hospital. However, sampling was continued until no new themes or barriers emerged, and major themes emerged consistently throughout the interviews with all 3 groups. Interviews were conducted at a large, urban university hospital, and so results may not be generalizable to smaller community hospitals. Last, although the 3 major groupspatients, nurses, and physicianswere included in the interviews, the opinions of other stakeholders who may have had perspectives on mobility such as family members were not solicited and may need to be incorporated into the model.
This study presents the perceived barriers to mobility from the perspectives of patients their nurses and physicians. The modifiable and nonmodifiable factors that might affect mobility during hospitalization that made up the original theoretical model were consistent with the barriers cited by the participants. Importantly, this research has led to the identification of other barriers such as environmental factors that may also influence the mobility of older patients. This research has provided insights into potentially modifiable factors of the well‐documented phenomenon of low mobility of hospitalized older persons10 and identified several targets for a multicomponent intervention to minimize low mobility. Possible interventions include a progressive walking program initiated early in the hospital stay, provision of assistive devices to patients who need them, and early removal of catheters and intravenous lines. Further research is needed to explore other factors associated with low mobility, such as specific medical conditions for which bed rest may be ordered, and to evaluate the impact that specific interventions may have on the mobility of older persons during hospitalization.
Acknowledgements
The authors are indebted to the patients, nurses, and resident physicians at University Hospital who participated in the study; to Stephanie Stone, MBA, for her invaluable assistance with study execution; and to Robert H. Brown, MDiv, for his critical review of the manuscript.
APPENDIX
Questionnaire Guide for Patients
Attitudes toward Mobility
Tell me how much walking do you do at home when you are not sick.
Do you leave your bedroom when you are at home? Do you need help to do this?
Do you go out of the house when you are at home? Do you need help to do this?
Do you go out of your neighborhood when you are at home? Do you need help to do this?
Tell me what you think about getting out of bed and moving around during this hospitalization? Do you think it is a good idea or a bad one?
How important do you believe it is for you to rest while you are in the hospital? Why did you choose that answer?
How important do you believe it is for you to walk while you are in the hospital? Why did you choose that answer?
Do you believe it to be dangerous for you to get up out of bed and walk? Why or why not?
Do you think your doctor wants you to get out of bed and walk? Why or why not?
Do you think your nurse wants you to get out of bed and walk? Why or why not?
Expectations of Care about Walking/Mobility
Can you tell me what you believe the nurse is supposed to do for you while you are in the hospital?
When you leave the hospital, do you believe you will be able to walk on your own, or will you need help?
Needs help: Why do you believe you will need help? What type of help will you need?
No help needed: Why do you believe you will not need help?
When you leave the hospital, do you believe you will be able to care for yourself, or will you need help? Needs help: Why do you believe you will need help? What type of help will you need?
No help needed: Why do you believe you will not need help?
If you needed help, who would be available to help you when you go home?
Person Factors That Influence Mobility
Tell me about the illness that brought you into the hospital.
How serious do you believe your illness to be? Why do you believe that?
How easy will it be for you to get better from this illness? Why do you believe that?
Situational Factors That Influence Mobility
Do you have any thoughts about what might make it easier for you to get out of bed and walk more frequently or for longer periods than you are now?
If you decided to go to the bathroom, would you call for help?
Why did you choose that answer?
Perceived Barriers
Tell me what, if anything, would prevent you from getting out of bed and walking during your hospital stay?
Do you have any concerns about falling during your hospital stay?
Are there other factors that influence if you will walk during your hospitalization that I haven't asked about?
New Questions
As this is a qualitative study, if participants bring up new topics that have not been previously explored with the questionnaire guide, these questions will be added to the questionnaire. Future participants will be asked the new questions.
- ,,.Predictors of functional decline in hospitalized elderly patients: a systematic review.J Gerontol Med Sci.2002;57A:M569–M577.
- ,,, et al.Loss of independence in activities of daily living in older adults hospitalized with medical illnesses: increased vulnerability with age.J Am Geriatr Soc.2003;51:451–458.
- ,,, et al.Functional outcomes of acute medical illness and hospitalization in older persons.Arch Intern Med.1996;156:645–652.
- ,,,,.Effect of a geriatric consultation team on functional status of elderly hospitalized patients.Ann Intern Med.1989;110:79–84.
- ,,, et al.Functional disability in the hospitalized elderly.JAMA.1982;248:847–850.
- ,,, et al.Predictors of immediate and 6‐month outcomes in hospitalized elderly patients.J Am Geriatr Soc.1988;36:775–783.
- ,,.Adverse consequences of hospitalization in the elderly.Soc Sci Med.1982;16:1033–1038.
- ,.Complications of illness in geriatric patients in hospital.J Chronic Dis.1966;19:307–313.
- ,,,,.The provision of physical activity to hospitalized elderly patients.Arch Intern Med.1991;151:2452–2456.
- ,,.Prevalence and outcomes of low mobility in hospitalized older patients.J Am Geriatr Soc.2004;52:1263–1270.
- ,,.Cost effectiveness of accelerated rehabilitation after proximal femoral fracture.J Clin Epidemiol.1994;47:1307–1313.
- ,,,,.Early inpatient rehabilitation after elective hip and knee arthroplasty.JAMA.1998;279:847–852.
- ,,,,.Time to ambulation after hip fracture surgery: relation to hospitalization outcomes.J Gerontol.2003;58A:1042–1045.
- ,,, et al.Controlled trial of early mobilization and discharge from hospital in uncomplicated myocardial infarction.Lancet.1971;2:1359–1360.
- ,,,,.Value of early ambulation in patients with and without complications after acute myocardial infarction.N Engl J Med.1975;292:719–722.
- ,,.Bed rest: a potentially harmful treatment needing more careful evaluation.Lancet.1999;354:1229–1233.
- ,,, et al.Early ambulation after 5 French diagnostic cardiac catheterization: results of a multicenter trial.J Am Coll Cardiol.1990;15:1475–1483.
- ,,, et al.Position and mobilisation post‐angiography study (PAMPAS): a comparison of 4.5 hours and 2.5 hours bed rest.Hear.2003;89:447–448.
- ,,, et al.Bed rest or ambulation in the initial treatment of patients with acute deep vein thrombosis or pulmonary embolism: findings from the RIETE Registry.Chest.2005;127:1631–1636.
- ,,,,.Early mobilization of patients hospitalized with community‐acquired pneumonia.Chest.2003;124:883–889.
- .Hazards of hospitalization of the elderly.Ann Intern Med.1993;118:219–223.
- ,.Physiology and complications of bedrest.J Am Geriatr Soc.1988;36:1047–1054.
- ,.Hospital‐associated deconditioning and dysfunction.J Am Geriatr Soc.1991;39:220–222.
- ,,.“Mini‐mental state.” A practical method for grading the cognitive status of patients for the clinician.J Psychiatr Rev.1975;12:189–198.
- ,,,,,.Clarifying confusion: the confusion assessment method. A new method for detection of delirium.Ann Intern Med.1990;113:941–948.
- ,.The Discovery of Grounded Theory. Strategies for Qualitative Research.Chicago, IL:Aldine;1967.
- ,,.How many interviews are enough?Field Methods.2006;18:59–82.
- ,,, et al.A multifactorial intervention to reduce the risk of falling among elderly people living in the community.N Engl J Med.1994;331:821–827.
- ,,, et al.A multicomponent intervention to prevent delirium in hospitalized older patients.N Engl J Med.1999;340:669–676.
- ,,,.Predictors of regaining ambulatory ability during hospitalization.J Hosp Med.2006;1:277–284.
- ,,.Walking for Wellness: a collaborative program to maintain mobility in hospitalized older adults.Geriatr Nurs.2004;25:242–245.
- ,,.Use of restraints and bed rails in a British hospital.J Am Geriatr Soc.1996;44:1086–1088.
- ,,.An analysis of falls in the hospital: can we do without bedrails?J Am Geriatr Soc.1999;47:529–31.
- ,,,.Side rail use and bed‐related outcomes among nursing home residents.J Am Geriatr Soc.2002;50:90–96.
The adverse outcomes associated with hospitalization of older patients, such as functional decline and increased nursing home placement, have been well documented.19 Low mobility, defined as being limited to a bed or chair, has also been associated with these adverse outcomes, even after controlling for severity of illness.10 Early ambulation has been a common practice for years following many types of orthopedic operations, including hip fracture repair and total joint replacement.11, 12 A recent study demonstrated that time to ambulation after surgery was an independent predictor of the development of postoperative complications such as pneumonia and delirium.13
In the early 1980s, early ambulation became the cornerstone of cardiac rehabilitation after acute myocardial infarction.14, 15 Until recently, with the exception of postmyocardial infarction, the use of early ambulation for patients admitted with medical illnesses has not been studied. In the last few years, researchers have begun to explore the use of early ambulation for patients after cardiac catheterization and for those admitted with deep‐vein thrombosis and pneumonia.1620 Although many of these studies have been small, they have found early ambulation not to be associated with worse outcomes. Indeed, a study of early ambulation for patients with community‐acquired pneumonia demonstrated decreased hospital costs and increased functional ability prior to discharge.20
Although the literature documents the adverse consequences associated with bed rest2123 and the beneficial effects of early ambulation, patients continue to spend a significant amount of their hospital stay limited to a bed or a chair. The prevalence of low mobility in older patients ranges from 23% to 33% during hospitalization for medical illness.9, 10 Despite the high prevalence and the associated adverse outcomes of low mobility among hospitalized older adults, the factors associated with low mobility in the hospital setting have not been systematically explored. Identification of such factors is the first step toward recognizing potentially modifiable factors and developing targeted interventions to improve hospital care.
We conceptualized a variety of factors or barriers that could potentially affect the level of mobility achieved by older hospitalized patients. Using professional experience and expert opinion, a conceptual model of potential barriers to mobility was developed (Fig. 1). As Figure 1 illustrates, the model has 4 major categories: patient‐related factors, including illness severity or comorbid conditions; treatment‐related factors such as catheters and intravenous lines; institution‐related factors such as nursing‐to‐patient ratio; and attitudinal factors related to perspectives on mobility and concerns about falling. This model was reviewed and feedback provided by a multidisciplinary group of colleagues including physicians, nurses, physical therapists, medical educators, and medical sociologists.
The objectives of this study were to employ qualitative methodology to identify and contextualize perceived barriers to mobility during hospitalization from the perspectives of older patients, their primary nurses, and their resident physicians; to compare and contrast the perceived barriers among these 3 groups; and to compare perceived barriers to mobility with our conceptual model.
METHODS
Setting and Patients
Patients aged 75 years admitted to the medical wards of the University Hospital either directly or through the Emergency Department were recruited for this study. In addition, the primary nurses and resident physicians of enrolled patients were also recruited because of their roles in providing hands‐on care to these patients in the university hospital setting. This project was supported in part by a VA Research Career Development Award and a training support grant from the Hartford Foundationfunded Southeast Center of Excellence in Geriatric Medicine. Written informed consent for participation was obtained from the patients, their nurses, and their resident physicians according to procedures approved by the Institutional Review Board of the University of Alabama at Birmingham. Recruitment was continued until no new barriers to hospital mobility were identified and data saturation was achieved. In all, 29 persons were enrolled: 10 patients, 10 nurses, and 9 physicians.
Patient exclusion criteria included factors that made it difficult for an individual to participate in the interview and to self‐report on mobility: (1) inability to be interviewed (ie, obtunded, aphasic), (2) a significant language barrier, requiring a translator, (3) Mini Mental State Examination Score24 < 16, (4) delirium at the time of the interview as documented by the Confusion Assessment Method (CAM)25, and (5) self‐reported inability to ambulate or transfer 2 weeks prior to hospital admission; Additional exclusion criteria were (6) previous enrollment in the study by the patient, the primary nurse, or the physician; and (7) refusal by patient, family, or physician to participate.
Questionnaire Development
A semistructured interview guide approach was used to encourage participants to discuss their perception of barriers to mobility during hospitalization. Pilot testing at a local retirement center was used to revise the initial patient questionnaire. Domains of inquiry were identified through the pilot testing and based on the conceptualized model (Fig. 1). These domains included attitudes toward mobility, expectations of care regarding walking/mobility, patient‐related factors that influence mobility, situational factors that influence mobility, and specific perceived barriers to mobility. Similar but not identical questions were used for patients and health care providers so answers could be compared between participant subgroups. For example, patients were asked, What might make it easier for you to get out of bed and walk more frequently or for longer periods than you are now? and health care providers were asked, What would make it easier for the patient to get out of bed and walk more frequently or for longer periods of time? Responses were categorized as being spontaneous or prompted depending on how the responses were elicited. Spontaneous responses about mobility barriers were elicited during general questioning about the hospital stay; for example: Tell me what you think about getting out of bed and moving around during this hospitalization? Prompted responses were elicited by asking a specific question about a potential barrier: Do you have any concerns about falling during your hospital stay?
Data Analysis
Interviews were conducted by the principal investigator (PI) between September 2004 and January 2005. Using an iterative approach, analysis began after the first interview with emerging themes being explored in subsequent interviews. All interviews were audiotaped and transcribed verbatim by a medical transcriptionist. Each participant was assigned a unique identifier. Interviews were reviewed by the PI to verify content. Participants were also given an opportunity to review the content of their interviews, with 76% choosing to do this. Using the grounded theory approach, an analytic technique that systematically analyzes raw interview data to generate hypotheses and develop theory; the data were analyzed by generating categories and themes.26
Interviews were independently reviewed and coded by the research assistant and the PI, with a third reviewer available to resolve disputes throughout the analyses. Initially, reviewers coded any item they believed to fit the category of barriers. Discrepancies between reviewers led to review of the original data to determine if the item could be considered a barrier. This process continued until the reviewers were in agreement about what to include as a barrier. Next, the themes generated by the coders were compared. Any discrepancies again led to review of the original data and revision of themes as indicated. This process continued until agreement was achieved for categories and themes between the coders for each of the 29 interviews. Independent themes were identified and counted and are presented as percentages for the purpose of comparing and contrasting between groups.
RESULTS
Fifty‐seven patients age 75 years were admitted to the medical service during the study period. Of those, 18 were excluded because they were too ill according to their physician (n = 6), had a nonmedical illness (n = 5), were discharged before being interviewed (n = 3), or were being cared for by a previously enrolled nurse or physician (n = 4). Of the 39 who were eligible for the study, 7 declined participation (6 patients, 1 physician), and data were lost for 3 as a result of technical difficulties with the tape recorder. A total of 29 participants had an interview transcribed: 10 patients, 10 nurses, and 9 physicians. As in other qualitative inquiries, data saturation was achieved after about 10 interviews,27 but we continued recruitment to permit comparison of themes identified by patients, nurses, and physicians.
Table 1 presents baseline characteristics of the patients. The mean age of the nurses was 34.9 9.9 years, all were female, and 60% were black. The mean age of the resident physicians was 29.1 2.2 years; 44% were female; and 78% were white, 22% were Latino, and none were black.
| Characteristic | Mean (SD) or N (%) |
|---|---|
| Age (years) | 84 (6.0) |
| Sex Male | 3 (30) |
| Female | 7 (70) |
| Race Black | 3 (30) |
| White | 7 (70) |
| Mini Mental State Examination score | 24 (3.3) |
| Number of comorbidities | 6 (2.3) |
| Number of medications at admission | 9 (2.3) |
Figure 2 presents barriers most frequently noted by participants. These barriers were similar among the 3 groups for symptoms and hospital‐related factors like catheters and lack of staff. Lack of patient motivation, lack of ambulatory devices, and medical reasons necessitating bed rest were reported more frequently by health care providers than by patients. On admission, 40% of patients had bed rest ordered. By hospital day 3, all patients had out‐of‐bed orders, and 70% had had physical therapy ordered.
Symptoms
Symptoms were spontaneously mentioned by 97% of participants (28 of 29) as a cause of limited mobility, with weakness cited most frequently: I know it is going to be painful (to walk). My head swims. This side of my all up and down to my toes is weak. When that comes, you kind of be scared. Pain and fatigue were also mentioned by more than 35% of all participants. Although 42% of health care providers (8 of 19) identified dyspnea or shortness of breath as a barrier, no patients reported this symptom as a barrier.
Medical Devices
When asked directly about the impact of urinary catheters and intravenous lines, most patients expressed the belief that the device could either be disconnected or carried and therefore was not a barrier: They can take that off [the catheter] and hook it on the wall. Only 30% of the patients described their mobility as hampered by the medical devices, and only 1 patient (10%) spontaneously indicated the catheter was a barrier: I have had that catheter hooked up to me until today. That was a relief to get that outI couldn't hardly do nothing with that.
In contrast, most health care providers (89%) believed medical devices adversely affected mobility. However, only 32% spontaneously noted the IV or catheter was a barrier, with the other 67% requiring prompting to consider the medical devices as barriers. The rationale for this belief varied widely. Some providers focused on the impact of the patient having to push the IV pole: They get tangled, they hurt when they are mobilized. You have to push the little cart, so patients actually need some assistance. Other providers mentioned the impact of a patient's medical devices on the nurse's ability to assist patients out of bed: I hate to say it, but I think on some days, it does [affect mobility]. You have patients who have TPN and blood and Foleys and chest tubes, you are probably less likely to [get people out of bed]. One physician commented on a less obvious impact of catheters: Some people might be embarrassed to walk around with that Foley catheter.
Need for Assistance and Lack of Staff
Patients, nurses, and physicians alike spontaneously identified the patient's need for assistance with ambulation as a barrier. This observation was frequently followed by comments about staff shortages and time constraints that limited the availability of staff to assist patients with ambulation. The impact of a perceived lack of staff was expressed differently by patients and health care providers. Patients frequently talked about not wanting to bother the nurses: I know it would be good for me, but I just don't want to impose upon them; I try not to worry the girls to take me walking because they have their own patients. Health care providers focused on the variety of other nursing duties that tended to take precedence over helping patients with mobility: I just don't think the nurses have time. They are too busy doing other things to walk their patients up and down the hallway. I think if you really want your patient up walking down the hall, you need to have a relative help them or physical therapy. Among staff, the most frequently mentioned solution was to refer patients to physical therapy, a strategy endorsed equally by nurses and physicians: That is why we try to encourage the doctors to order physical therapy, because we don't have time to ambulate patients in the hallway like the doctor expects.
Lack of Ambulatory Devices
The nurses frequently mentioned the absence of ambulatory devices to assist patients with walking. Nurses also expressed concern about the ability of patients to walk safely without such devices: Sometimes if a patient requires a lot of help, then I think you really need to involve physical therapy to ensure the safety of the person getting up. Because a lot of times you are limited with equipment that you need and they [physical therapists] have that equipment to make sure they don't fall. No physicians and only 1 patient cited lack of ambulatory devices as a barrier to mobility.
Fear of a Patient Falling
The potential for a fall during a hospital stay was of concern for more than 75% of the participants, with physicians spontaneously expressing concern for falls as a perceived barrier more frequently than did patients or nurses: I probably don't encourage her to move as much as I should. And when I do, I tell her to be sure to have someone with her when she is getting up. I am probably a little more protective because I am afraid she might fall. Another physician stated, I think nurses in general would prefer the patient to stay in bed. I believe they perceive it as a risk for falls and a risk for pulling out their IVs or any other medical device, and it is probably not viewed as an important factor in someone who is recovering from an illness. Another physician noted fall prevention was a secondary reason for limited mobility but also expressed the idea that bed rest was easier than mobility: While they are in bed they are not giving trouble to anybody. It is less work and, second, because of liability issues in terms of patients falling and hurting themselves while they are in the hospital. I think everybody is very concerned with that, but I think mainly because it is less work. Although 68% of health care providers spontaneously noted falls as a barrier to mobility, only 1 patient spontaneously verbalized this concern. However, with prompting to consider falls a barrier, 60% of patients stated falls were a potential barrier: As old as I am, your legs don't last long and they give away. It would be dangerous because I haven't got the strength. Now, since I've fallen, yes, I have to be careful.
Lack of Patient Motivation
Lack of patient motivation was mentioned by 50% of the nurses and 78% of the physicians and was often linked to a patient's age: I just think he is older now, and he is not as motivated as younger people are, and he has been through so much. I just don't think he wants to do it. I don't know if it is because it is the elderly or because they just seem more stubborn. They are sometimes more content to stay in the bed, and you have to really stress to them to get up. However, none of the patients indicated a lack of motivation was the reason for not getting out of bed. Indeed, they commented on the staff's apparent lack of interest or their perception that the staff did not consider increased mobility important: I don't believe they are going to get me out of bed while I am here. If I said I really needed to get out of bed, they try to do what you want them to do. But evidently they don't think it is that important.
Hospital Environment
Although not frequently mentioned, issues of an environment not conducive to mobility did emerge as a theme. Several patients expressed this environmental barrier as a difficulty with the hospital gowns that are required garb during a hospital stay. One patient wrote the following additional thoughts after reviewing her transcript: Gowns lead to embarrassing moments, are designed for benefit of staff, not patients. This sentiment was echoed by a physician who, when queried about the impact of gowns, responded, I think the gown exposes the patient a lot and they might feel embarrassed to go around. And outside the hospital room, nobody wants to be perceived as sick and draw attention. Finally, 2 physicians commented on the lack of chairs in the room and the physical setup of the room not encouraging mobility: I think that patients, when they are in the hospital, they feel they are supposed to be in bed. And they are more comfortable there and a lot of times they can see the TV better.
DISCUSSION
Many of the barriers described in the original conceptual model (Fig. 1) were cited by participants from all 3 groups: patients, nurses and physicians. These included patient‐related factors like symptoms and need for assistance, concern about falls, and lack of staff to assist with ambulation. Although attitudes toward mobility were cited in the model and by participants, there was significant disagreement between the 3 groups about the cause of the attitudinal barrier. Health care providers cited lack of patient motivation, whereas patients perceived health care providers as not being interested in mobility or viewing it as important. Health care providers frequently employed stereotypes to describe the potential reasons for the perceived attitudes toward mobility, often linking lack of motivation or interest in getting out of bed to patients being old. Patients linked the lack of importance attached to mobility to the numerous duties of staff members and believed that assistance with mobility was less important than other duties. Physicians and nurses were both more likely than patients to mention factors like urinary catheters, intravenous lines, and other medical reasons that necessitated bed rest. Although more than half the nurses commented on the lack of ambulatory devices for ambulation, no physicians and only 1 patient perceived this lack to be a barrier.
The model presented appears to have face validity, with participants citing many of the factors originally identified as barriers to mobility. The original model did not include consideration of environmental factors such as the number of chairs in the room or the location of the television. Such environmental factors can be conceptualized as institution‐related factors.
In addition, the impact of physician activity orders for bed rest was not specifically discussed by participants, although 45% of participants did comment on the need for bed rest because of a medical condition. A review of the medical records for activity orders indicated 40% of the patients initially had orders for bed rest. Another recent study demonstrated 33% of older patients were on bed rest at some point during their hospital stay10 and should be retained in the model as a treatment‐related consideration.
Several barriers noted in the original model and by participants may not be modifiable, such as comorbid conditions and illness severity. But other perceived barriers may be, and recognition of these factors present potential targets for a future multicomponent intervention to enhance hospital mobility. This multicomponent approach has been highly successful for geriatric syndromes like falls28 and delirium.29
During hospitalization, a focus on early removal of catheters and intravenous lines may encourage mobility. In a recent study absence of a urinary catheter was a predictor of patients with activity limitations regaining ambulatory ability while hospitalized.30 Availability of ambulatory devices may allow nurses to ambulate patients without consulting physical therapy. Another potential solution would be a hospitalwide walking program. The feasibility of a walking program was demonstrated in a small pilot study at a community‐based hospital using specially trained transporters to walk ward patients during slow periods. These periods included nights and weekends, when patients were more likely to be available and when physical therapy was often not present. On average, participants spent 2.4 days in the program, with an average of 5.6 walks per patient. However, additional research is needed, as the study was too small to demonstrate the effects of the walking program on length of stay or functional decline.31
Other barriers, while potentially modifiable, may be more difficult to address and may involve changing the culture of the hospital. For instance, concern about falls was a common theme, echoed by all 3 groups. Physicians were the most likely to spontaneously mention falls as a concern. The nurses shared this concern, frequently citing the use of bed rails as a part of their fall protocol, despite available literature demonstrating that this approach was not efficacious.3234 Nurses also consistently reported asking patients to call for help to ambulate, yet both patients and nurses noted a lack of nursing time to assist with ambulation. The default solution providers reported using was utilizing physical therapists, who were available to walk with patients only once or twice a day. Research on the best methods to prevent falls during hospitalization is limited. Given the current medicolegal environment and the emphasis on fall prevention by the Joint Commission on Accreditation of Healthcare Organizations and other government entities, it is not surprising that bed rest and mobility limitation are being used as a method of minimizing falls. Until data about successful fall‐prevention strategies are available, minimization of mobility may remain the default solution.
Strengths of the present study include the use of qualitative methods to explore potential barriers to mobility, a method that allows participants to describe in their own words their attitudes, beliefs, and expectations about mobility during hospitalization. Face‐to‐face interviewing of the 3 major groups involved in the hospital experience (patients, nurses, and physicians) facilitated the collection of detailed contextualized information on factors expected to affect a patient's level of mobility during hospitalization. This enabled hypothesis generation and sensitization to issues that need further quantitative investigation with larger groups.
The study also had several limitations. First, only resident physicians were included, and their answers may not reflect the opinions of other, more experienced physicians. However, resident physicians were chosen for this study because they play important roles in delivering hands‐on care in teaching hospitals and would need to be involved in any future interventions designed to enhanced patient mobility. Second, a sample size of 29 participants, approximately 10 persons in each group, may not reflect the thinking of those throughout the hospital. However, sampling was continued until no new themes or barriers emerged, and major themes emerged consistently throughout the interviews with all 3 groups. Interviews were conducted at a large, urban university hospital, and so results may not be generalizable to smaller community hospitals. Last, although the 3 major groupspatients, nurses, and physicianswere included in the interviews, the opinions of other stakeholders who may have had perspectives on mobility such as family members were not solicited and may need to be incorporated into the model.
This study presents the perceived barriers to mobility from the perspectives of patients their nurses and physicians. The modifiable and nonmodifiable factors that might affect mobility during hospitalization that made up the original theoretical model were consistent with the barriers cited by the participants. Importantly, this research has led to the identification of other barriers such as environmental factors that may also influence the mobility of older patients. This research has provided insights into potentially modifiable factors of the well‐documented phenomenon of low mobility of hospitalized older persons10 and identified several targets for a multicomponent intervention to minimize low mobility. Possible interventions include a progressive walking program initiated early in the hospital stay, provision of assistive devices to patients who need them, and early removal of catheters and intravenous lines. Further research is needed to explore other factors associated with low mobility, such as specific medical conditions for which bed rest may be ordered, and to evaluate the impact that specific interventions may have on the mobility of older persons during hospitalization.
Acknowledgements
The authors are indebted to the patients, nurses, and resident physicians at University Hospital who participated in the study; to Stephanie Stone, MBA, for her invaluable assistance with study execution; and to Robert H. Brown, MDiv, for his critical review of the manuscript.
APPENDIX
Questionnaire Guide for Patients
Attitudes toward Mobility
Tell me how much walking do you do at home when you are not sick.
Do you leave your bedroom when you are at home? Do you need help to do this?
Do you go out of the house when you are at home? Do you need help to do this?
Do you go out of your neighborhood when you are at home? Do you need help to do this?
Tell me what you think about getting out of bed and moving around during this hospitalization? Do you think it is a good idea or a bad one?
How important do you believe it is for you to rest while you are in the hospital? Why did you choose that answer?
How important do you believe it is for you to walk while you are in the hospital? Why did you choose that answer?
Do you believe it to be dangerous for you to get up out of bed and walk? Why or why not?
Do you think your doctor wants you to get out of bed and walk? Why or why not?
Do you think your nurse wants you to get out of bed and walk? Why or why not?
Expectations of Care about Walking/Mobility
Can you tell me what you believe the nurse is supposed to do for you while you are in the hospital?
When you leave the hospital, do you believe you will be able to walk on your own, or will you need help?
Needs help: Why do you believe you will need help? What type of help will you need?
No help needed: Why do you believe you will not need help?
When you leave the hospital, do you believe you will be able to care for yourself, or will you need help? Needs help: Why do you believe you will need help? What type of help will you need?
No help needed: Why do you believe you will not need help?
If you needed help, who would be available to help you when you go home?
Person Factors That Influence Mobility
Tell me about the illness that brought you into the hospital.
How serious do you believe your illness to be? Why do you believe that?
How easy will it be for you to get better from this illness? Why do you believe that?
Situational Factors That Influence Mobility
Do you have any thoughts about what might make it easier for you to get out of bed and walk more frequently or for longer periods than you are now?
If you decided to go to the bathroom, would you call for help?
Why did you choose that answer?
Perceived Barriers
Tell me what, if anything, would prevent you from getting out of bed and walking during your hospital stay?
Do you have any concerns about falling during your hospital stay?
Are there other factors that influence if you will walk during your hospitalization that I haven't asked about?
New Questions
As this is a qualitative study, if participants bring up new topics that have not been previously explored with the questionnaire guide, these questions will be added to the questionnaire. Future participants will be asked the new questions.
The adverse outcomes associated with hospitalization of older patients, such as functional decline and increased nursing home placement, have been well documented.19 Low mobility, defined as being limited to a bed or chair, has also been associated with these adverse outcomes, even after controlling for severity of illness.10 Early ambulation has been a common practice for years following many types of orthopedic operations, including hip fracture repair and total joint replacement.11, 12 A recent study demonstrated that time to ambulation after surgery was an independent predictor of the development of postoperative complications such as pneumonia and delirium.13
In the early 1980s, early ambulation became the cornerstone of cardiac rehabilitation after acute myocardial infarction.14, 15 Until recently, with the exception of postmyocardial infarction, the use of early ambulation for patients admitted with medical illnesses has not been studied. In the last few years, researchers have begun to explore the use of early ambulation for patients after cardiac catheterization and for those admitted with deep‐vein thrombosis and pneumonia.1620 Although many of these studies have been small, they have found early ambulation not to be associated with worse outcomes. Indeed, a study of early ambulation for patients with community‐acquired pneumonia demonstrated decreased hospital costs and increased functional ability prior to discharge.20
Although the literature documents the adverse consequences associated with bed rest2123 and the beneficial effects of early ambulation, patients continue to spend a significant amount of their hospital stay limited to a bed or a chair. The prevalence of low mobility in older patients ranges from 23% to 33% during hospitalization for medical illness.9, 10 Despite the high prevalence and the associated adverse outcomes of low mobility among hospitalized older adults, the factors associated with low mobility in the hospital setting have not been systematically explored. Identification of such factors is the first step toward recognizing potentially modifiable factors and developing targeted interventions to improve hospital care.
We conceptualized a variety of factors or barriers that could potentially affect the level of mobility achieved by older hospitalized patients. Using professional experience and expert opinion, a conceptual model of potential barriers to mobility was developed (Fig. 1). As Figure 1 illustrates, the model has 4 major categories: patient‐related factors, including illness severity or comorbid conditions; treatment‐related factors such as catheters and intravenous lines; institution‐related factors such as nursing‐to‐patient ratio; and attitudinal factors related to perspectives on mobility and concerns about falling. This model was reviewed and feedback provided by a multidisciplinary group of colleagues including physicians, nurses, physical therapists, medical educators, and medical sociologists.
The objectives of this study were to employ qualitative methodology to identify and contextualize perceived barriers to mobility during hospitalization from the perspectives of older patients, their primary nurses, and their resident physicians; to compare and contrast the perceived barriers among these 3 groups; and to compare perceived barriers to mobility with our conceptual model.
METHODS
Setting and Patients
Patients aged 75 years admitted to the medical wards of the University Hospital either directly or through the Emergency Department were recruited for this study. In addition, the primary nurses and resident physicians of enrolled patients were also recruited because of their roles in providing hands‐on care to these patients in the university hospital setting. This project was supported in part by a VA Research Career Development Award and a training support grant from the Hartford Foundationfunded Southeast Center of Excellence in Geriatric Medicine. Written informed consent for participation was obtained from the patients, their nurses, and their resident physicians according to procedures approved by the Institutional Review Board of the University of Alabama at Birmingham. Recruitment was continued until no new barriers to hospital mobility were identified and data saturation was achieved. In all, 29 persons were enrolled: 10 patients, 10 nurses, and 9 physicians.
Patient exclusion criteria included factors that made it difficult for an individual to participate in the interview and to self‐report on mobility: (1) inability to be interviewed (ie, obtunded, aphasic), (2) a significant language barrier, requiring a translator, (3) Mini Mental State Examination Score24 < 16, (4) delirium at the time of the interview as documented by the Confusion Assessment Method (CAM)25, and (5) self‐reported inability to ambulate or transfer 2 weeks prior to hospital admission; Additional exclusion criteria were (6) previous enrollment in the study by the patient, the primary nurse, or the physician; and (7) refusal by patient, family, or physician to participate.
Questionnaire Development
A semistructured interview guide approach was used to encourage participants to discuss their perception of barriers to mobility during hospitalization. Pilot testing at a local retirement center was used to revise the initial patient questionnaire. Domains of inquiry were identified through the pilot testing and based on the conceptualized model (Fig. 1). These domains included attitudes toward mobility, expectations of care regarding walking/mobility, patient‐related factors that influence mobility, situational factors that influence mobility, and specific perceived barriers to mobility. Similar but not identical questions were used for patients and health care providers so answers could be compared between participant subgroups. For example, patients were asked, What might make it easier for you to get out of bed and walk more frequently or for longer periods than you are now? and health care providers were asked, What would make it easier for the patient to get out of bed and walk more frequently or for longer periods of time? Responses were categorized as being spontaneous or prompted depending on how the responses were elicited. Spontaneous responses about mobility barriers were elicited during general questioning about the hospital stay; for example: Tell me what you think about getting out of bed and moving around during this hospitalization? Prompted responses were elicited by asking a specific question about a potential barrier: Do you have any concerns about falling during your hospital stay?
Data Analysis
Interviews were conducted by the principal investigator (PI) between September 2004 and January 2005. Using an iterative approach, analysis began after the first interview with emerging themes being explored in subsequent interviews. All interviews were audiotaped and transcribed verbatim by a medical transcriptionist. Each participant was assigned a unique identifier. Interviews were reviewed by the PI to verify content. Participants were also given an opportunity to review the content of their interviews, with 76% choosing to do this. Using the grounded theory approach, an analytic technique that systematically analyzes raw interview data to generate hypotheses and develop theory; the data were analyzed by generating categories and themes.26
Interviews were independently reviewed and coded by the research assistant and the PI, with a third reviewer available to resolve disputes throughout the analyses. Initially, reviewers coded any item they believed to fit the category of barriers. Discrepancies between reviewers led to review of the original data to determine if the item could be considered a barrier. This process continued until the reviewers were in agreement about what to include as a barrier. Next, the themes generated by the coders were compared. Any discrepancies again led to review of the original data and revision of themes as indicated. This process continued until agreement was achieved for categories and themes between the coders for each of the 29 interviews. Independent themes were identified and counted and are presented as percentages for the purpose of comparing and contrasting between groups.
RESULTS
Fifty‐seven patients age 75 years were admitted to the medical service during the study period. Of those, 18 were excluded because they were too ill according to their physician (n = 6), had a nonmedical illness (n = 5), were discharged before being interviewed (n = 3), or were being cared for by a previously enrolled nurse or physician (n = 4). Of the 39 who were eligible for the study, 7 declined participation (6 patients, 1 physician), and data were lost for 3 as a result of technical difficulties with the tape recorder. A total of 29 participants had an interview transcribed: 10 patients, 10 nurses, and 9 physicians. As in other qualitative inquiries, data saturation was achieved after about 10 interviews,27 but we continued recruitment to permit comparison of themes identified by patients, nurses, and physicians.
Table 1 presents baseline characteristics of the patients. The mean age of the nurses was 34.9 9.9 years, all were female, and 60% were black. The mean age of the resident physicians was 29.1 2.2 years; 44% were female; and 78% were white, 22% were Latino, and none were black.
| Characteristic | Mean (SD) or N (%) |
|---|---|
| Age (years) | 84 (6.0) |
| Sex Male | 3 (30) |
| Female | 7 (70) |
| Race Black | 3 (30) |
| White | 7 (70) |
| Mini Mental State Examination score | 24 (3.3) |
| Number of comorbidities | 6 (2.3) |
| Number of medications at admission | 9 (2.3) |
Figure 2 presents barriers most frequently noted by participants. These barriers were similar among the 3 groups for symptoms and hospital‐related factors like catheters and lack of staff. Lack of patient motivation, lack of ambulatory devices, and medical reasons necessitating bed rest were reported more frequently by health care providers than by patients. On admission, 40% of patients had bed rest ordered. By hospital day 3, all patients had out‐of‐bed orders, and 70% had had physical therapy ordered.
Symptoms
Symptoms were spontaneously mentioned by 97% of participants (28 of 29) as a cause of limited mobility, with weakness cited most frequently: I know it is going to be painful (to walk). My head swims. This side of my all up and down to my toes is weak. When that comes, you kind of be scared. Pain and fatigue were also mentioned by more than 35% of all participants. Although 42% of health care providers (8 of 19) identified dyspnea or shortness of breath as a barrier, no patients reported this symptom as a barrier.
Medical Devices
When asked directly about the impact of urinary catheters and intravenous lines, most patients expressed the belief that the device could either be disconnected or carried and therefore was not a barrier: They can take that off [the catheter] and hook it on the wall. Only 30% of the patients described their mobility as hampered by the medical devices, and only 1 patient (10%) spontaneously indicated the catheter was a barrier: I have had that catheter hooked up to me until today. That was a relief to get that outI couldn't hardly do nothing with that.
In contrast, most health care providers (89%) believed medical devices adversely affected mobility. However, only 32% spontaneously noted the IV or catheter was a barrier, with the other 67% requiring prompting to consider the medical devices as barriers. The rationale for this belief varied widely. Some providers focused on the impact of the patient having to push the IV pole: They get tangled, they hurt when they are mobilized. You have to push the little cart, so patients actually need some assistance. Other providers mentioned the impact of a patient's medical devices on the nurse's ability to assist patients out of bed: I hate to say it, but I think on some days, it does [affect mobility]. You have patients who have TPN and blood and Foleys and chest tubes, you are probably less likely to [get people out of bed]. One physician commented on a less obvious impact of catheters: Some people might be embarrassed to walk around with that Foley catheter.
Need for Assistance and Lack of Staff
Patients, nurses, and physicians alike spontaneously identified the patient's need for assistance with ambulation as a barrier. This observation was frequently followed by comments about staff shortages and time constraints that limited the availability of staff to assist patients with ambulation. The impact of a perceived lack of staff was expressed differently by patients and health care providers. Patients frequently talked about not wanting to bother the nurses: I know it would be good for me, but I just don't want to impose upon them; I try not to worry the girls to take me walking because they have their own patients. Health care providers focused on the variety of other nursing duties that tended to take precedence over helping patients with mobility: I just don't think the nurses have time. They are too busy doing other things to walk their patients up and down the hallway. I think if you really want your patient up walking down the hall, you need to have a relative help them or physical therapy. Among staff, the most frequently mentioned solution was to refer patients to physical therapy, a strategy endorsed equally by nurses and physicians: That is why we try to encourage the doctors to order physical therapy, because we don't have time to ambulate patients in the hallway like the doctor expects.
Lack of Ambulatory Devices
The nurses frequently mentioned the absence of ambulatory devices to assist patients with walking. Nurses also expressed concern about the ability of patients to walk safely without such devices: Sometimes if a patient requires a lot of help, then I think you really need to involve physical therapy to ensure the safety of the person getting up. Because a lot of times you are limited with equipment that you need and they [physical therapists] have that equipment to make sure they don't fall. No physicians and only 1 patient cited lack of ambulatory devices as a barrier to mobility.
Fear of a Patient Falling
The potential for a fall during a hospital stay was of concern for more than 75% of the participants, with physicians spontaneously expressing concern for falls as a perceived barrier more frequently than did patients or nurses: I probably don't encourage her to move as much as I should. And when I do, I tell her to be sure to have someone with her when she is getting up. I am probably a little more protective because I am afraid she might fall. Another physician stated, I think nurses in general would prefer the patient to stay in bed. I believe they perceive it as a risk for falls and a risk for pulling out their IVs or any other medical device, and it is probably not viewed as an important factor in someone who is recovering from an illness. Another physician noted fall prevention was a secondary reason for limited mobility but also expressed the idea that bed rest was easier than mobility: While they are in bed they are not giving trouble to anybody. It is less work and, second, because of liability issues in terms of patients falling and hurting themselves while they are in the hospital. I think everybody is very concerned with that, but I think mainly because it is less work. Although 68% of health care providers spontaneously noted falls as a barrier to mobility, only 1 patient spontaneously verbalized this concern. However, with prompting to consider falls a barrier, 60% of patients stated falls were a potential barrier: As old as I am, your legs don't last long and they give away. It would be dangerous because I haven't got the strength. Now, since I've fallen, yes, I have to be careful.
Lack of Patient Motivation
Lack of patient motivation was mentioned by 50% of the nurses and 78% of the physicians and was often linked to a patient's age: I just think he is older now, and he is not as motivated as younger people are, and he has been through so much. I just don't think he wants to do it. I don't know if it is because it is the elderly or because they just seem more stubborn. They are sometimes more content to stay in the bed, and you have to really stress to them to get up. However, none of the patients indicated a lack of motivation was the reason for not getting out of bed. Indeed, they commented on the staff's apparent lack of interest or their perception that the staff did not consider increased mobility important: I don't believe they are going to get me out of bed while I am here. If I said I really needed to get out of bed, they try to do what you want them to do. But evidently they don't think it is that important.
Hospital Environment
Although not frequently mentioned, issues of an environment not conducive to mobility did emerge as a theme. Several patients expressed this environmental barrier as a difficulty with the hospital gowns that are required garb during a hospital stay. One patient wrote the following additional thoughts after reviewing her transcript: Gowns lead to embarrassing moments, are designed for benefit of staff, not patients. This sentiment was echoed by a physician who, when queried about the impact of gowns, responded, I think the gown exposes the patient a lot and they might feel embarrassed to go around. And outside the hospital room, nobody wants to be perceived as sick and draw attention. Finally, 2 physicians commented on the lack of chairs in the room and the physical setup of the room not encouraging mobility: I think that patients, when they are in the hospital, they feel they are supposed to be in bed. And they are more comfortable there and a lot of times they can see the TV better.
DISCUSSION
Many of the barriers described in the original conceptual model (Fig. 1) were cited by participants from all 3 groups: patients, nurses and physicians. These included patient‐related factors like symptoms and need for assistance, concern about falls, and lack of staff to assist with ambulation. Although attitudes toward mobility were cited in the model and by participants, there was significant disagreement between the 3 groups about the cause of the attitudinal barrier. Health care providers cited lack of patient motivation, whereas patients perceived health care providers as not being interested in mobility or viewing it as important. Health care providers frequently employed stereotypes to describe the potential reasons for the perceived attitudes toward mobility, often linking lack of motivation or interest in getting out of bed to patients being old. Patients linked the lack of importance attached to mobility to the numerous duties of staff members and believed that assistance with mobility was less important than other duties. Physicians and nurses were both more likely than patients to mention factors like urinary catheters, intravenous lines, and other medical reasons that necessitated bed rest. Although more than half the nurses commented on the lack of ambulatory devices for ambulation, no physicians and only 1 patient perceived this lack to be a barrier.
The model presented appears to have face validity, with participants citing many of the factors originally identified as barriers to mobility. The original model did not include consideration of environmental factors such as the number of chairs in the room or the location of the television. Such environmental factors can be conceptualized as institution‐related factors.
In addition, the impact of physician activity orders for bed rest was not specifically discussed by participants, although 45% of participants did comment on the need for bed rest because of a medical condition. A review of the medical records for activity orders indicated 40% of the patients initially had orders for bed rest. Another recent study demonstrated 33% of older patients were on bed rest at some point during their hospital stay10 and should be retained in the model as a treatment‐related consideration.
Several barriers noted in the original model and by participants may not be modifiable, such as comorbid conditions and illness severity. But other perceived barriers may be, and recognition of these factors present potential targets for a future multicomponent intervention to enhance hospital mobility. This multicomponent approach has been highly successful for geriatric syndromes like falls28 and delirium.29
During hospitalization, a focus on early removal of catheters and intravenous lines may encourage mobility. In a recent study absence of a urinary catheter was a predictor of patients with activity limitations regaining ambulatory ability while hospitalized.30 Availability of ambulatory devices may allow nurses to ambulate patients without consulting physical therapy. Another potential solution would be a hospitalwide walking program. The feasibility of a walking program was demonstrated in a small pilot study at a community‐based hospital using specially trained transporters to walk ward patients during slow periods. These periods included nights and weekends, when patients were more likely to be available and when physical therapy was often not present. On average, participants spent 2.4 days in the program, with an average of 5.6 walks per patient. However, additional research is needed, as the study was too small to demonstrate the effects of the walking program on length of stay or functional decline.31
Other barriers, while potentially modifiable, may be more difficult to address and may involve changing the culture of the hospital. For instance, concern about falls was a common theme, echoed by all 3 groups. Physicians were the most likely to spontaneously mention falls as a concern. The nurses shared this concern, frequently citing the use of bed rails as a part of their fall protocol, despite available literature demonstrating that this approach was not efficacious.3234 Nurses also consistently reported asking patients to call for help to ambulate, yet both patients and nurses noted a lack of nursing time to assist with ambulation. The default solution providers reported using was utilizing physical therapists, who were available to walk with patients only once or twice a day. Research on the best methods to prevent falls during hospitalization is limited. Given the current medicolegal environment and the emphasis on fall prevention by the Joint Commission on Accreditation of Healthcare Organizations and other government entities, it is not surprising that bed rest and mobility limitation are being used as a method of minimizing falls. Until data about successful fall‐prevention strategies are available, minimization of mobility may remain the default solution.
Strengths of the present study include the use of qualitative methods to explore potential barriers to mobility, a method that allows participants to describe in their own words their attitudes, beliefs, and expectations about mobility during hospitalization. Face‐to‐face interviewing of the 3 major groups involved in the hospital experience (patients, nurses, and physicians) facilitated the collection of detailed contextualized information on factors expected to affect a patient's level of mobility during hospitalization. This enabled hypothesis generation and sensitization to issues that need further quantitative investigation with larger groups.
The study also had several limitations. First, only resident physicians were included, and their answers may not reflect the opinions of other, more experienced physicians. However, resident physicians were chosen for this study because they play important roles in delivering hands‐on care in teaching hospitals and would need to be involved in any future interventions designed to enhanced patient mobility. Second, a sample size of 29 participants, approximately 10 persons in each group, may not reflect the thinking of those throughout the hospital. However, sampling was continued until no new themes or barriers emerged, and major themes emerged consistently throughout the interviews with all 3 groups. Interviews were conducted at a large, urban university hospital, and so results may not be generalizable to smaller community hospitals. Last, although the 3 major groupspatients, nurses, and physicianswere included in the interviews, the opinions of other stakeholders who may have had perspectives on mobility such as family members were not solicited and may need to be incorporated into the model.
This study presents the perceived barriers to mobility from the perspectives of patients their nurses and physicians. The modifiable and nonmodifiable factors that might affect mobility during hospitalization that made up the original theoretical model were consistent with the barriers cited by the participants. Importantly, this research has led to the identification of other barriers such as environmental factors that may also influence the mobility of older patients. This research has provided insights into potentially modifiable factors of the well‐documented phenomenon of low mobility of hospitalized older persons10 and identified several targets for a multicomponent intervention to minimize low mobility. Possible interventions include a progressive walking program initiated early in the hospital stay, provision of assistive devices to patients who need them, and early removal of catheters and intravenous lines. Further research is needed to explore other factors associated with low mobility, such as specific medical conditions for which bed rest may be ordered, and to evaluate the impact that specific interventions may have on the mobility of older persons during hospitalization.
Acknowledgements
The authors are indebted to the patients, nurses, and resident physicians at University Hospital who participated in the study; to Stephanie Stone, MBA, for her invaluable assistance with study execution; and to Robert H. Brown, MDiv, for his critical review of the manuscript.
APPENDIX
Questionnaire Guide for Patients
Attitudes toward Mobility
Tell me how much walking do you do at home when you are not sick.
Do you leave your bedroom when you are at home? Do you need help to do this?
Do you go out of the house when you are at home? Do you need help to do this?
Do you go out of your neighborhood when you are at home? Do you need help to do this?
Tell me what you think about getting out of bed and moving around during this hospitalization? Do you think it is a good idea or a bad one?
How important do you believe it is for you to rest while you are in the hospital? Why did you choose that answer?
How important do you believe it is for you to walk while you are in the hospital? Why did you choose that answer?
Do you believe it to be dangerous for you to get up out of bed and walk? Why or why not?
Do you think your doctor wants you to get out of bed and walk? Why or why not?
Do you think your nurse wants you to get out of bed and walk? Why or why not?
Expectations of Care about Walking/Mobility
Can you tell me what you believe the nurse is supposed to do for you while you are in the hospital?
When you leave the hospital, do you believe you will be able to walk on your own, or will you need help?
Needs help: Why do you believe you will need help? What type of help will you need?
No help needed: Why do you believe you will not need help?
When you leave the hospital, do you believe you will be able to care for yourself, or will you need help? Needs help: Why do you believe you will need help? What type of help will you need?
No help needed: Why do you believe you will not need help?
If you needed help, who would be available to help you when you go home?
Person Factors That Influence Mobility
Tell me about the illness that brought you into the hospital.
How serious do you believe your illness to be? Why do you believe that?
How easy will it be for you to get better from this illness? Why do you believe that?
Situational Factors That Influence Mobility
Do you have any thoughts about what might make it easier for you to get out of bed and walk more frequently or for longer periods than you are now?
If you decided to go to the bathroom, would you call for help?
Why did you choose that answer?
Perceived Barriers
Tell me what, if anything, would prevent you from getting out of bed and walking during your hospital stay?
Do you have any concerns about falling during your hospital stay?
Are there other factors that influence if you will walk during your hospitalization that I haven't asked about?
New Questions
As this is a qualitative study, if participants bring up new topics that have not been previously explored with the questionnaire guide, these questions will be added to the questionnaire. Future participants will be asked the new questions.
- ,,.Predictors of functional decline in hospitalized elderly patients: a systematic review.J Gerontol Med Sci.2002;57A:M569–M577.
- ,,, et al.Loss of independence in activities of daily living in older adults hospitalized with medical illnesses: increased vulnerability with age.J Am Geriatr Soc.2003;51:451–458.
- ,,, et al.Functional outcomes of acute medical illness and hospitalization in older persons.Arch Intern Med.1996;156:645–652.
- ,,,,.Effect of a geriatric consultation team on functional status of elderly hospitalized patients.Ann Intern Med.1989;110:79–84.
- ,,, et al.Functional disability in the hospitalized elderly.JAMA.1982;248:847–850.
- ,,, et al.Predictors of immediate and 6‐month outcomes in hospitalized elderly patients.J Am Geriatr Soc.1988;36:775–783.
- ,,.Adverse consequences of hospitalization in the elderly.Soc Sci Med.1982;16:1033–1038.
- ,.Complications of illness in geriatric patients in hospital.J Chronic Dis.1966;19:307–313.
- ,,,,.The provision of physical activity to hospitalized elderly patients.Arch Intern Med.1991;151:2452–2456.
- ,,.Prevalence and outcomes of low mobility in hospitalized older patients.J Am Geriatr Soc.2004;52:1263–1270.
- ,,.Cost effectiveness of accelerated rehabilitation after proximal femoral fracture.J Clin Epidemiol.1994;47:1307–1313.
- ,,,,.Early inpatient rehabilitation after elective hip and knee arthroplasty.JAMA.1998;279:847–852.
- ,,,,.Time to ambulation after hip fracture surgery: relation to hospitalization outcomes.J Gerontol.2003;58A:1042–1045.
- ,,, et al.Controlled trial of early mobilization and discharge from hospital in uncomplicated myocardial infarction.Lancet.1971;2:1359–1360.
- ,,,,.Value of early ambulation in patients with and without complications after acute myocardial infarction.N Engl J Med.1975;292:719–722.
- ,,.Bed rest: a potentially harmful treatment needing more careful evaluation.Lancet.1999;354:1229–1233.
- ,,, et al.Early ambulation after 5 French diagnostic cardiac catheterization: results of a multicenter trial.J Am Coll Cardiol.1990;15:1475–1483.
- ,,, et al.Position and mobilisation post‐angiography study (PAMPAS): a comparison of 4.5 hours and 2.5 hours bed rest.Hear.2003;89:447–448.
- ,,, et al.Bed rest or ambulation in the initial treatment of patients with acute deep vein thrombosis or pulmonary embolism: findings from the RIETE Registry.Chest.2005;127:1631–1636.
- ,,,,.Early mobilization of patients hospitalized with community‐acquired pneumonia.Chest.2003;124:883–889.
- .Hazards of hospitalization of the elderly.Ann Intern Med.1993;118:219–223.
- ,.Physiology and complications of bedrest.J Am Geriatr Soc.1988;36:1047–1054.
- ,.Hospital‐associated deconditioning and dysfunction.J Am Geriatr Soc.1991;39:220–222.
- ,,.“Mini‐mental state.” A practical method for grading the cognitive status of patients for the clinician.J Psychiatr Rev.1975;12:189–198.
- ,,,,,.Clarifying confusion: the confusion assessment method. A new method for detection of delirium.Ann Intern Med.1990;113:941–948.
- ,.The Discovery of Grounded Theory. Strategies for Qualitative Research.Chicago, IL:Aldine;1967.
- ,,.How many interviews are enough?Field Methods.2006;18:59–82.
- ,,, et al.A multifactorial intervention to reduce the risk of falling among elderly people living in the community.N Engl J Med.1994;331:821–827.
- ,,, et al.A multicomponent intervention to prevent delirium in hospitalized older patients.N Engl J Med.1999;340:669–676.
- ,,,.Predictors of regaining ambulatory ability during hospitalization.J Hosp Med.2006;1:277–284.
- ,,.Walking for Wellness: a collaborative program to maintain mobility in hospitalized older adults.Geriatr Nurs.2004;25:242–245.
- ,,.Use of restraints and bed rails in a British hospital.J Am Geriatr Soc.1996;44:1086–1088.
- ,,.An analysis of falls in the hospital: can we do without bedrails?J Am Geriatr Soc.1999;47:529–31.
- ,,,.Side rail use and bed‐related outcomes among nursing home residents.J Am Geriatr Soc.2002;50:90–96.
- ,,.Predictors of functional decline in hospitalized elderly patients: a systematic review.J Gerontol Med Sci.2002;57A:M569–M577.
- ,,, et al.Loss of independence in activities of daily living in older adults hospitalized with medical illnesses: increased vulnerability with age.J Am Geriatr Soc.2003;51:451–458.
- ,,, et al.Functional outcomes of acute medical illness and hospitalization in older persons.Arch Intern Med.1996;156:645–652.
- ,,,,.Effect of a geriatric consultation team on functional status of elderly hospitalized patients.Ann Intern Med.1989;110:79–84.
- ,,, et al.Functional disability in the hospitalized elderly.JAMA.1982;248:847–850.
- ,,, et al.Predictors of immediate and 6‐month outcomes in hospitalized elderly patients.J Am Geriatr Soc.1988;36:775–783.
- ,,.Adverse consequences of hospitalization in the elderly.Soc Sci Med.1982;16:1033–1038.
- ,.Complications of illness in geriatric patients in hospital.J Chronic Dis.1966;19:307–313.
- ,,,,.The provision of physical activity to hospitalized elderly patients.Arch Intern Med.1991;151:2452–2456.
- ,,.Prevalence and outcomes of low mobility in hospitalized older patients.J Am Geriatr Soc.2004;52:1263–1270.
- ,,.Cost effectiveness of accelerated rehabilitation after proximal femoral fracture.J Clin Epidemiol.1994;47:1307–1313.
- ,,,,.Early inpatient rehabilitation after elective hip and knee arthroplasty.JAMA.1998;279:847–852.
- ,,,,.Time to ambulation after hip fracture surgery: relation to hospitalization outcomes.J Gerontol.2003;58A:1042–1045.
- ,,, et al.Controlled trial of early mobilization and discharge from hospital in uncomplicated myocardial infarction.Lancet.1971;2:1359–1360.
- ,,,,.Value of early ambulation in patients with and without complications after acute myocardial infarction.N Engl J Med.1975;292:719–722.
- ,,.Bed rest: a potentially harmful treatment needing more careful evaluation.Lancet.1999;354:1229–1233.
- ,,, et al.Early ambulation after 5 French diagnostic cardiac catheterization: results of a multicenter trial.J Am Coll Cardiol.1990;15:1475–1483.
- ,,, et al.Position and mobilisation post‐angiography study (PAMPAS): a comparison of 4.5 hours and 2.5 hours bed rest.Hear.2003;89:447–448.
- ,,, et al.Bed rest or ambulation in the initial treatment of patients with acute deep vein thrombosis or pulmonary embolism: findings from the RIETE Registry.Chest.2005;127:1631–1636.
- ,,,,.Early mobilization of patients hospitalized with community‐acquired pneumonia.Chest.2003;124:883–889.
- .Hazards of hospitalization of the elderly.Ann Intern Med.1993;118:219–223.
- ,.Physiology and complications of bedrest.J Am Geriatr Soc.1988;36:1047–1054.
- ,.Hospital‐associated deconditioning and dysfunction.J Am Geriatr Soc.1991;39:220–222.
- ,,.“Mini‐mental state.” A practical method for grading the cognitive status of patients for the clinician.J Psychiatr Rev.1975;12:189–198.
- ,,,,,.Clarifying confusion: the confusion assessment method. A new method for detection of delirium.Ann Intern Med.1990;113:941–948.
- ,.The Discovery of Grounded Theory. Strategies for Qualitative Research.Chicago, IL:Aldine;1967.
- ,,.How many interviews are enough?Field Methods.2006;18:59–82.
- ,,, et al.A multifactorial intervention to reduce the risk of falling among elderly people living in the community.N Engl J Med.1994;331:821–827.
- ,,, et al.A multicomponent intervention to prevent delirium in hospitalized older patients.N Engl J Med.1999;340:669–676.
- ,,,.Predictors of regaining ambulatory ability during hospitalization.J Hosp Med.2006;1:277–284.
- ,,.Walking for Wellness: a collaborative program to maintain mobility in hospitalized older adults.Geriatr Nurs.2004;25:242–245.
- ,,.Use of restraints and bed rails in a British hospital.J Am Geriatr Soc.1996;44:1086–1088.
- ,,.An analysis of falls in the hospital: can we do without bedrails?J Am Geriatr Soc.1999;47:529–31.
- ,,,.Side rail use and bed‐related outcomes among nursing home residents.J Am Geriatr Soc.2002;50:90–96.
Copyright © 2007 Society of Hospital Medicine
Sign‐Out within the Electronic Medical Record
The delivery of safe, high‐quality care to hospitalized patients depends on effective communication among providers.1, 2 Inpatients may receive care from a number of specialists in addition to their primary hospital physicians, and each provider may practice in a group that transfers care of individual patients among its members. This issue is exacerbated in teaching hospitals because fellows, residents, and interns make frequent transfers of care because of work‐hour rules.3, 4 Finally, teams of physician providers making management decisions must effectively communicate with other members of the care team, such as nurses, dieticians, and social workers, who also may be part of a group practice involving transfers. A patient hospitalized for just a few days in a modern hospital may receive care from dozens of providers and be the subject of multiple transfers of care, or handoffs, that require effective communication. Therefore, as part of its 2006 National Patient Safety Goals,5 the Joint Commission on Accreditation of Health Care Organizations (JCAHO) now requires that each hospital implement a standardized, structured approach to transfers of care.
Transfers of care have been shown to be a source of medical errors and adverse patient outcomes.2, 6, 7 In many cases, the critical information necessary to avert medical errors exists but is not available in real time to providers.6
Traditionally, provider teams have relied on the patient chart, in concert with direct patient evaluation, to provide the information to guide decision making during a hospitalization. Unfortunately, the structure of the chart in most hospitals has evolved little over the past 80 years810 and remains organized so that information is more easily filed than retrieved, read, or summarized.811 Typically, electronic medical records (EMRs) mimic the appearance of paper records and include similar organizational flaws.12 As a result, many providers have created ad hoc informational systems, separate from the chart, designed to track a patient's progress over time and to facilitate transfers of care. These sign‐out systems, which are intended to complement verbal sign‐out between providers,1315 range in complexity from simple handwritten index cards16 to adapted spreadsheets, PDA systems,17, 18 and more complex data systems (eg, FileMaker Pro)19 and often contain crucial information not found elsewhere in the medical record.20, 21
Although sign‐out systems are crucial to patient safety, they have several drawbacks. First, ad‐hoc informational systems may not be standardized, resulting in content and accuracy that vary among providers.22 These systems may fail to identify critical elements of a patient's condition, promoting ineffective communication and placing the patient at increased risk of adverse events.7, 13, 23
These observations underscore the need for a standardized patient‐tracking instrument that can distill crucial patient information, enhance communication, support transfers, improve efficiency, and enhance continuity of patient care.
We aimed to develop an integrated, problem‐based patient‐tracking tool as part of our hospital's EMR. The tool, SynopSIS, supports patient tracking, transfers of care (ie, sign‐outs), and daily rounds.
METHODS
Setting
The study took place at a 547‐bed adult and pediatric tertiary‐care university‐based teaching hospital with 2 campuses at the University of California, San Francisco, Medical Center (UCSFMC).
PROGRAM DESCRIPTION
Development and Design
A multidisciplinary team of practicing residents and attending physicians, information technology leaders, software engineers, and experts in medical communication and sign‐out developed the SynopSIS tool. We reviewed the literature to incorporate key design elements of other successfully implemented information transfer systems.24, 25
We conducted a formal review of existing patient‐tracking and sign‐out systems at our hospital to characterize provider work practices, with an emphasis on the specific information requirements of different specialties. A needs assessment of current sign‐out processes at UCSFMC was conducted by personal interviews with a chief resident or representative of each of the 18 Accreditation Council of Graduate Medical Education (ACGME) accredited residency programs through the dean's office of Graduate Medical Education. This needs assessment revealed that the majority of the programs did not have a standardized mechanism for sign‐out. Although most did use a written format for sign‐out, the actual type of written format varied from handwritten cards to databases using a variety of programs including Filemaker Pro, Microsoft Excel, and Microsoft Word. When asked what could improve the sign‐out system for their program, they most often responded that it would be having a standardized computerized sign‐out system in the hospital.26
During the design and pilot phase, we presented each SynopSIS function to an advisory committee of more than 50 trainees in medical, surgical, and pediatric general and subspecialty fields. Their input shaped the information content and presentation of our tool. In addition, we discussed the tool with the attending‐physician advisory group that oversees the implementation of clinical information systems in our hospital system.
Conceptual Model
We developed this conceptual model by integrating existing scholarship and input from stakeholders at our institution. First, we reviewed existing literature on documentation and transfers of care. Next, we conducted several focus group sessions with our EMR Residents' Advisory Group to conceptualize work flow and handoff needs for hospital physicians across specialties. We arrived at this model after several iterations of feedback from providers.
SynopSIS maps patient data available in the EMR to each of the 3 main functions according to type of clinical decisions supported by that function (Fig. 1). For example, data needed for effective patient tracking, such as likely functional status, are required to make decisions over the course of a patient's hospitalization. Similarly, data needed for sign‐out are used to make decisions over the course of a shift, typically overnight; and data needed for morning rounds are used to make decisions for the day. Although the information required for each function overlaps considerably, there are specialized data elements unique to each function.
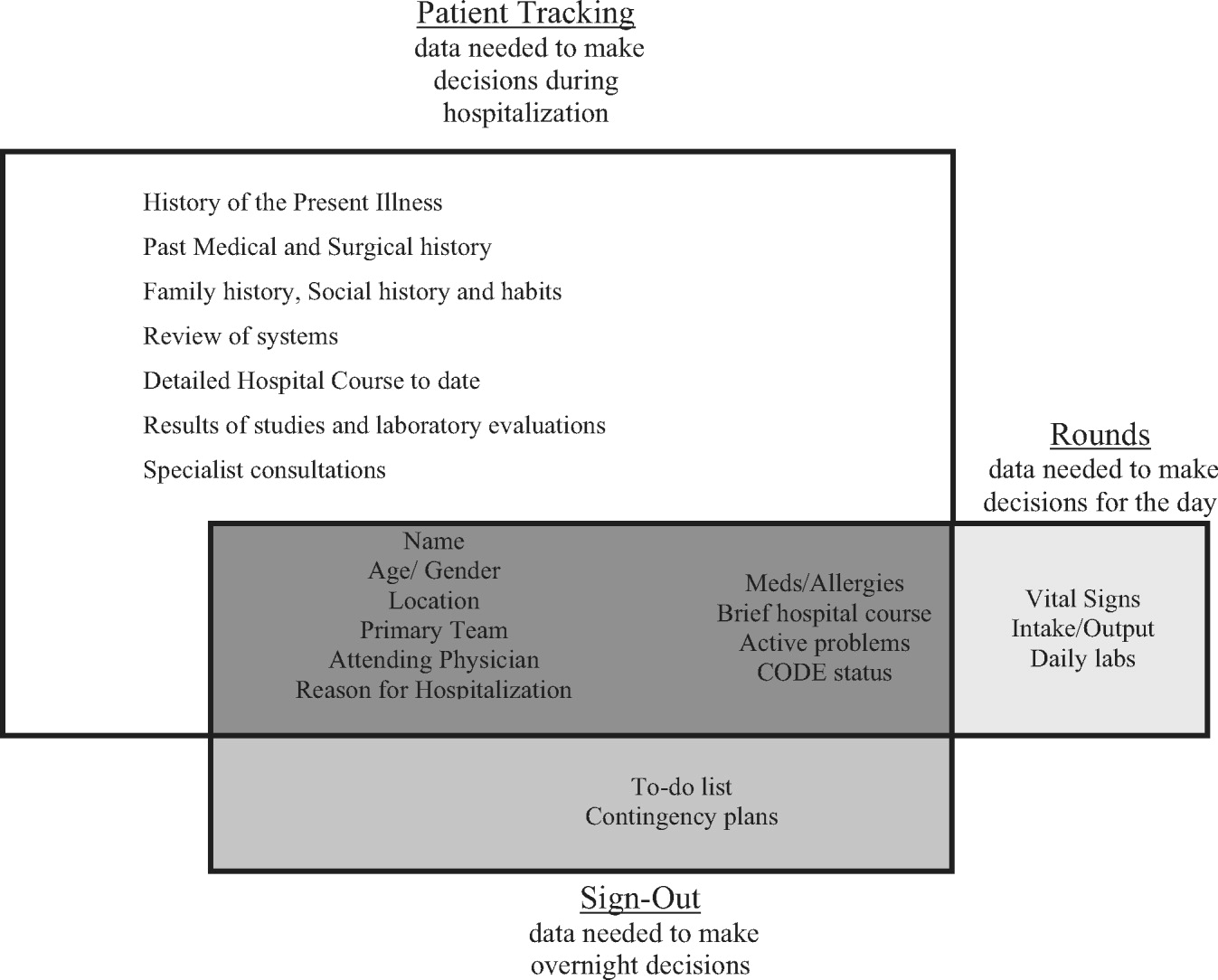
Description of Functionality
SynopSIS is integrated with our hospital's EMR, General Electric (GE) Centricity Enterprise. The physician interface for SynopSIS is shown in Figure 2. After selecting a patient from a list corresponding to a given inpatient service (eg, Medicine Team B), the user selects the menu option to view the SynopSIS screen, which provides an at a glance overview of the patient's current condition. Different fields on the screen support each of SynopSIS's 3 main functions. At the top, the patient's demographic and registration information is displayed, including name, location, age, medical record number, and attending physician. Below are fields viewable and editable by users of the EMR. The Admission Diagnosis/Course and Problem List fields support patient tracking and allow a receiving physician to understand the reason for the patient's admission, the overall course of the illness, and the current active problems. The problem list is entered by the primary hospital physician. The Anticipated Problems/To Do List field supports the sign‐out function from which providers can coordinate care‐related activities and make contingency plans for anticipated events. The patients' most recent laboratory results and vital signs are displayed on the lower left of the screen for easy reference during face‐to‐face physician sign‐outs. Finally, the CODE status, Allergies, and Medications fields allow efficient tracking of information. Temporarily, until the pharmacy component of the EMR goes into use, the primary hospital physician will enter and update the medications. When the pharmacy is linked to the EMR, medications will be added directly from the inpatient pharmacy records to the EMR‐linked sign‐out tool.
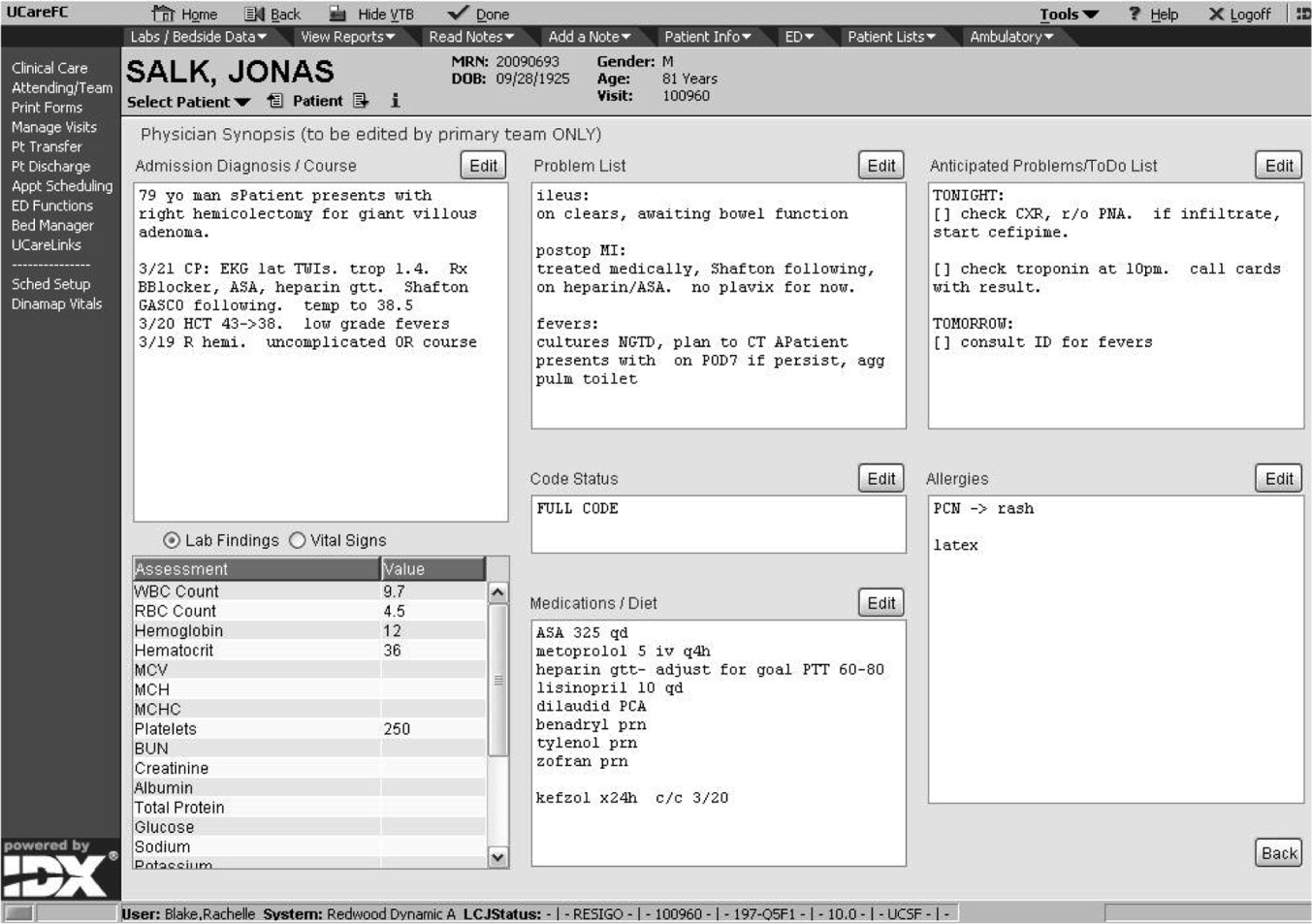
This on‐screen SynopSIS view is distinct from the summary screen typically seen in EMRs, including vendor‐based and the Veterans' Affairs systems. For instance, the Veterans' Affairs summary screen incorporates clinical and nonclinical data, including demographic and payment information, upcoming appointments, and patient‐specific information such as allergies. Moreover, it is not editable by primary hospital physicians. Unlike a summary screen, which collates select patient information from other parts of the EMR, SynopSIS is specific to the current acute hospitalization and includes information not found elsewhere in the medical record.
To support rounding, SynopSIS gathers and presents data from the EMR in a printed Rounds Report (Fig. 3). The report is generated for all patients assigned to an inpatient service (eg, Medicine Team B) and emphasizes clarity and brevity using a format validated in the medical literature.24, 25 Each patient's report covers one fourth of a standard 8‐by‐11‐inch landscape‐printed page. The top half of each of these quarter‐page patient reports displays data stored in SynopSIS's interface and summarizes the patient's illness and the course of that illness. The lower half displays vital signs, intake/output, and laboratory data over the 24 hours from the time of printing. The most recent value and the range over the previous 24 hours of all vital signs are displayed. Intake/output totals are listed together with a structured breakdown. Laboratory results for the past 24 hours are listed with the most immediate prior values, allowing providers to discern trends. We envision providers obtaining a rounds report on arrival each day before examining their patients.
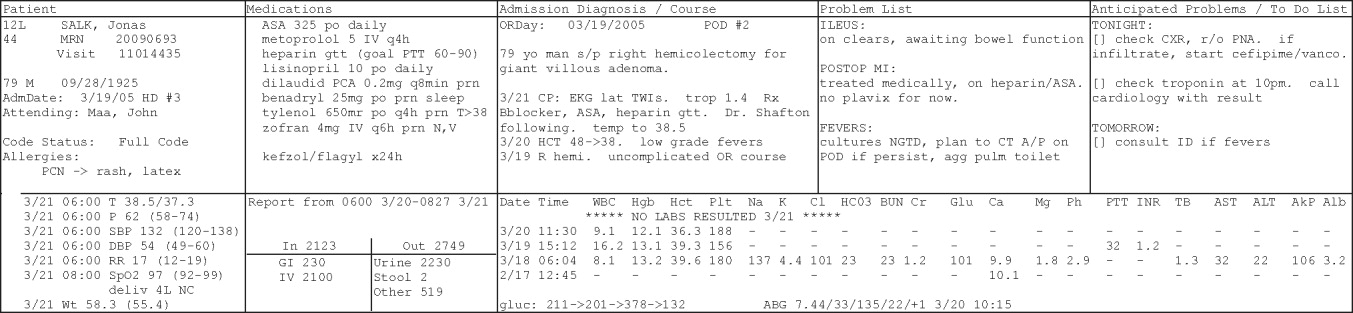
Importantly, although SynopSIS is part of the patient's medical record, physician users may change or overwrite the data in any field. This ability is a critical feature of the toolthe focus is on providing an interpretable snapshot of the patient. Data may be removed as their importance lessens or as the patient's condition changes, which contrasts with unchangeable documentation geared for alternative purposes, such as billing or medical‐legal requirements. Deleted data are saved in the medical record and are viewable by audit.
Program Evaluation
We have planned a postimplementation evaluation for SynopSIS. Each of the 3 functions (patient tracking, rounding, and care transitions) will be assessed separately. We will explore rounding efficiency and quality by survey and through direct observation. We plan to assess the percentage of time spent on direct patient care versus gathering patient data during morning rounds. We adapted elements of SynopSIS from UWCores, an existing sign‐out application in place at the University of Washington.24, 25 In a randomized trial, UWCores was shown to improve indicators of quality of care (more time spent with patients on rounds, fewer patients missed on rounds) and rounding efficiency (less time prerounding and rounding).25 For evaluation, we plan to use a previously published instrument25 in an online survey of SynopSIS users to assess perceived changes in the quality of sign‐out, providerprovider communication, and patient continuity of care. We intend to measure daily use of SynopSIS by primary providers, covering providers, and consulting physicians in order to assess its impact on each patient's care plan. We hypothesize that primary hospital physicians will access SynopSIS at least 3 times daily: on arrival at the hospital, after rounding, and prior to handoffs. We also plan to investigate whether consulting physicians will view SynopSIS daily rather than obtaining patient data such as labs and vital signs from separate parts of the EMR. Finally, we hypothesize that SynopSIS may facilitate initiation of appropriate discharge planning earlier in a patient's hospital course because it is viewable by nursing, care management, and social work personnel. Importantly, we will implement SynopSIS after the EMR gains universal use at our hospital. We will then wait for a washout following the EMR implementation in order to avoid confounding with the effects of the EMR. We will then be able to separate the effects of this tool from the effects of the EMR. Our EMR does not offer a function comparable to the rounds report or sign‐out tool in SynopSIS.
In addition to this quantitative evaluation process, we plan to solicit feedback from SynopSIS users in focus groups, including physicians at all levels of training as well as nonphysicians. We will use this information to revise SynopSIS according to the users' needs and to tailor the application to diverse specialty services.
DISCUSSION
Several systems have been developed to enhance communication among providers and to support the transfer of care of hospitalized patients.13, 14, 16, 19, 24, 25 We have developed a tool to support patient tracking, sign‐out, and rounding that incorporates key elements of previously designed systems and may improve communication among providers. SynopSIS helps to fulfill the 2006 JCAHO accreditation requirement for standardized communication for transfers of care when used with appropriate verbal communication, including an opportunity to ask and respond to questions.5 Research from other safety‐oriented industries recommends standardized information transfer, which SynopSIS will provide.20 What is innovative about SynopSIS is that it is not a stand‐alone system, but an integrated part of the EMR.
Currently, fewer than 5% of hospitals have an electronic sign‐out tool linked to hospital information systems27; therefore, SynopSIS has great potential for dissemination. In technical terms, this tool was coded by GE and could be readily adopted by any other GE Centricity Enterprise customer. Moreover, the conceptual model, the design strategy, and the critical system elements should be relevant to effective patient tracking, sign‐out, and rounding across different IT platforms.
Despite its strengths, the SynopSIS system has several limitations. First, appropriate transfer of care is a learned process that incorporates well‐described provider and system elements.15, 21, 2830 This tool cannot perform sign‐out; it makes up one part of an effective sign‐out process. As our institution implements SynopSIS, we will also proceed with educational efforts and infrastructure to improve the sign‐out process. Second, although data can be overwritten, prior screen versions are archived in the database. Because SynopSIS is part of the medical record, users may omit sensitive or clinically useful information because of medical‐legal concerns, such as sensitive family dynamics or patient behavioral issues that providers may be reluctant to document in the patient chart. Currently, such information is conveyed verbally during sign‐out. Third, as information gathering and transfer become more automated, informal person‐to‐person interactions among providers (eg, physicians and nurses) may erode. However, we expect that SynopSIS actually will enhance the quality of this communication because it places them on the same page. Finally, SynopSIS generates paper reports that must be disposed of in accordance with standards of patient confidentiality.
We believe that SynopSIS will improve the quality of care through several mechanisms. Because this single‐screen summary will be available to all members of a patients' care team, it is possible that SynopSIS will enable providers to share management plans more readily. Although nursing and care management do not use SynopSIS for their own handoffs, they have clamored for the ability to view it. In addition, rotating providers can readily assume care of an unfamiliar patient. By automating data‐gathering tasks, SynopSIS may foster efficiency and increase time with patients during rounds. For trainee providers in particular, such increased efficiency should allow more time for education and alleviate some of the pressures of duty‐hour compliance. Most important, SynopSIS frees the EMR from emulating the historic paper chart as its method of supporting clinical work flow and communication. That paradigm does not harness the power of today's EMR databases and integration capabilities31 and creates extra work through interruptive work flow and redundant effort.32 With SynopSIS reengineering, instead of providers having to serve the needs of the chart, the chart serves the needs of providers and patients.
Future clinical documentation and EMR systems should focus on provider work flow to improve quality and efficiency in patient care. Moreover, involving providers, including residents, in system design fosters innovation and optimally applies information technology to supporting clinical practice.
Acknowledgements
The authors acknowledge Harry Wong, Chutima Assapimonwait, and Vern Rogers for programming the application. Deborah G. Airo edited the manuscript.
- ,,.Crew resource managment and its applications in medicine. Making health care safer: A critical analysis of patient safety practices. Evidence report/technology assessment2001. AHRQ publication 01‐E058(43).
- ,.Internal Bleeding: The Truth behind America's Terrifying Epidemic of Medical Mistakes.New York, NY:Rugged Land;2004.
- ,,.New requirements for resident duty hours.JAMA.2002;288:1112–1124.
- ,,,.The impact of a regulation restricting medical house staff working hours on the quality of patient care.JAMA.1993;269:374–378.
- Joint Commission 2006 National Patient Safety Goals Implementation Expectations.2005. Available at: http://www.jcaho.org/accredited+organizations/patient+safety/06_npsg_ie.pdf.
- ,,.Gaps in the continuity of care and progress on patient safety.BMJ.2000;320:791–794.
- ,,,,.Does housestaff discontinuity of care increase the risk for preventable adverse events?Ann Intern Med.1994;121:866–872.
- .The problem‐oriented record—its organizing principles and its structure.League Exch.1975 (103):3–6.
- .The problem oriented record as a basic tool in medical education, patient care and clinical research.Ann Clin Res.1971;3(3):131–134.
- .Medical records, patient care, and medical education.Ir J Med Sci.1964;17:271–282.
- ,,, et al.Creating a note classification scheme for a multi‐institutional electronic medical record.AMIA Annu Symp Proc.2003:968.
- ,,,,,.Impacts of computerized physician documentation in a teaching hospital: perceptions of faculty and resident physicians.J Am Med Inform Assoc.2004;11:300–309.
- ,,,,.Using a computerized sign‐out program to improve continuity of inpatient care and prevent adverse events.Jt Comm J Qual Improv.1998;24(2):77–87.
- ,.Signing out patients for off‐hours coverage: comparison of manual and computer‐aided methods.Proc Annu Symp Comput Appl Med Care.1992:114–118.
- ,,,,.Managing discontinuity in academic medical centers: strategies for a safe and effective resident sign‐out.J Hosp Med.2006;1:257–266.
- ,,.Utility of a standardized sign‐out card for new medical interns.J Gen Intern Med.1996;11:753–755.
- ,,.The potential role of IT in supporting the work of junior doctors.J R Coll Physicians Lond.2000;34:366–370.
- ,,,.Electronic Sign‐out using a personal digital assistant.Psychiatr Serv.2001;52(2):173–174.
- .“Doctor's notes”: a computerized method for managing inpatient care.Fam Med.1988;20:223–224.
- ,,,,.Handoff strategies in settings with high consequences for failure: lessons for health care operations.Int J Qual Health Care.2004;16(2):125–132.
- ,,, et al.Understanding patient‐centered care in the context of total quality management and continuous quality improvement.Jt Comm J Qual Improv.1994;20(3):152–161.
- ,,.Utility of a standardized sign‐out card for new medical interns.J Gen Intern Med.1996;11:753–755.
- ,,,.Post‐call transfer of resident responsibility: its effect on patient care.J Gen Intern Med.1990;5:501–505.
- ,,,.Organizing the transfer of patient care information: the development of a computerized resident sign‐out system.Surgery.2004;136(1):5–13.
- ,,,,.A randomized, controlled trial evaluating the impact of a computerized rounding and sign‐out system on continuity of care and resident work hours.J Am Coll Surg.2005;200:538–545.
- .UCSFMC sign‐out needs assessment [personal communication].2007.
- ,.Is 80 the cost of saving lives? Reduced duty hours, errors, and cost.J Gen Intern Med.2005;20:969–970.
- ,,.Intern curriculum: the impact of a focused training program on the process and content of sign‐out out patients. Harvard Medical School Education Day2004.
- .When conversation is better than computation.J Am Med Inform Assoc.2000;7:277–286.
- ,.Communication behaviours in a hospital setting: an observational study.BMJ.1998;316:673–676.
- ,,,.Integration and beyond: linking information from disparate sources and into workflow.J Am Med Inform Assoc.2000;7(2):135–145.
- .Update on the electronic medical record.Otolaryngol Clin North Am.2002;35:1223–1236, vii.
The delivery of safe, high‐quality care to hospitalized patients depends on effective communication among providers.1, 2 Inpatients may receive care from a number of specialists in addition to their primary hospital physicians, and each provider may practice in a group that transfers care of individual patients among its members. This issue is exacerbated in teaching hospitals because fellows, residents, and interns make frequent transfers of care because of work‐hour rules.3, 4 Finally, teams of physician providers making management decisions must effectively communicate with other members of the care team, such as nurses, dieticians, and social workers, who also may be part of a group practice involving transfers. A patient hospitalized for just a few days in a modern hospital may receive care from dozens of providers and be the subject of multiple transfers of care, or handoffs, that require effective communication. Therefore, as part of its 2006 National Patient Safety Goals,5 the Joint Commission on Accreditation of Health Care Organizations (JCAHO) now requires that each hospital implement a standardized, structured approach to transfers of care.
Transfers of care have been shown to be a source of medical errors and adverse patient outcomes.2, 6, 7 In many cases, the critical information necessary to avert medical errors exists but is not available in real time to providers.6
Traditionally, provider teams have relied on the patient chart, in concert with direct patient evaluation, to provide the information to guide decision making during a hospitalization. Unfortunately, the structure of the chart in most hospitals has evolved little over the past 80 years810 and remains organized so that information is more easily filed than retrieved, read, or summarized.811 Typically, electronic medical records (EMRs) mimic the appearance of paper records and include similar organizational flaws.12 As a result, many providers have created ad hoc informational systems, separate from the chart, designed to track a patient's progress over time and to facilitate transfers of care. These sign‐out systems, which are intended to complement verbal sign‐out between providers,1315 range in complexity from simple handwritten index cards16 to adapted spreadsheets, PDA systems,17, 18 and more complex data systems (eg, FileMaker Pro)19 and often contain crucial information not found elsewhere in the medical record.20, 21
Although sign‐out systems are crucial to patient safety, they have several drawbacks. First, ad‐hoc informational systems may not be standardized, resulting in content and accuracy that vary among providers.22 These systems may fail to identify critical elements of a patient's condition, promoting ineffective communication and placing the patient at increased risk of adverse events.7, 13, 23
These observations underscore the need for a standardized patient‐tracking instrument that can distill crucial patient information, enhance communication, support transfers, improve efficiency, and enhance continuity of patient care.
We aimed to develop an integrated, problem‐based patient‐tracking tool as part of our hospital's EMR. The tool, SynopSIS, supports patient tracking, transfers of care (ie, sign‐outs), and daily rounds.
METHODS
Setting
The study took place at a 547‐bed adult and pediatric tertiary‐care university‐based teaching hospital with 2 campuses at the University of California, San Francisco, Medical Center (UCSFMC).
PROGRAM DESCRIPTION
Development and Design
A multidisciplinary team of practicing residents and attending physicians, information technology leaders, software engineers, and experts in medical communication and sign‐out developed the SynopSIS tool. We reviewed the literature to incorporate key design elements of other successfully implemented information transfer systems.24, 25
We conducted a formal review of existing patient‐tracking and sign‐out systems at our hospital to characterize provider work practices, with an emphasis on the specific information requirements of different specialties. A needs assessment of current sign‐out processes at UCSFMC was conducted by personal interviews with a chief resident or representative of each of the 18 Accreditation Council of Graduate Medical Education (ACGME) accredited residency programs through the dean's office of Graduate Medical Education. This needs assessment revealed that the majority of the programs did not have a standardized mechanism for sign‐out. Although most did use a written format for sign‐out, the actual type of written format varied from handwritten cards to databases using a variety of programs including Filemaker Pro, Microsoft Excel, and Microsoft Word. When asked what could improve the sign‐out system for their program, they most often responded that it would be having a standardized computerized sign‐out system in the hospital.26
During the design and pilot phase, we presented each SynopSIS function to an advisory committee of more than 50 trainees in medical, surgical, and pediatric general and subspecialty fields. Their input shaped the information content and presentation of our tool. In addition, we discussed the tool with the attending‐physician advisory group that oversees the implementation of clinical information systems in our hospital system.
Conceptual Model
We developed this conceptual model by integrating existing scholarship and input from stakeholders at our institution. First, we reviewed existing literature on documentation and transfers of care. Next, we conducted several focus group sessions with our EMR Residents' Advisory Group to conceptualize work flow and handoff needs for hospital physicians across specialties. We arrived at this model after several iterations of feedback from providers.
SynopSIS maps patient data available in the EMR to each of the 3 main functions according to type of clinical decisions supported by that function (Fig. 1). For example, data needed for effective patient tracking, such as likely functional status, are required to make decisions over the course of a patient's hospitalization. Similarly, data needed for sign‐out are used to make decisions over the course of a shift, typically overnight; and data needed for morning rounds are used to make decisions for the day. Although the information required for each function overlaps considerably, there are specialized data elements unique to each function.
Description of Functionality
SynopSIS is integrated with our hospital's EMR, General Electric (GE) Centricity Enterprise. The physician interface for SynopSIS is shown in Figure 2. After selecting a patient from a list corresponding to a given inpatient service (eg, Medicine Team B), the user selects the menu option to view the SynopSIS screen, which provides an at a glance overview of the patient's current condition. Different fields on the screen support each of SynopSIS's 3 main functions. At the top, the patient's demographic and registration information is displayed, including name, location, age, medical record number, and attending physician. Below are fields viewable and editable by users of the EMR. The Admission Diagnosis/Course and Problem List fields support patient tracking and allow a receiving physician to understand the reason for the patient's admission, the overall course of the illness, and the current active problems. The problem list is entered by the primary hospital physician. The Anticipated Problems/To Do List field supports the sign‐out function from which providers can coordinate care‐related activities and make contingency plans for anticipated events. The patients' most recent laboratory results and vital signs are displayed on the lower left of the screen for easy reference during face‐to‐face physician sign‐outs. Finally, the CODE status, Allergies, and Medications fields allow efficient tracking of information. Temporarily, until the pharmacy component of the EMR goes into use, the primary hospital physician will enter and update the medications. When the pharmacy is linked to the EMR, medications will be added directly from the inpatient pharmacy records to the EMR‐linked sign‐out tool.
This on‐screen SynopSIS view is distinct from the summary screen typically seen in EMRs, including vendor‐based and the Veterans' Affairs systems. For instance, the Veterans' Affairs summary screen incorporates clinical and nonclinical data, including demographic and payment information, upcoming appointments, and patient‐specific information such as allergies. Moreover, it is not editable by primary hospital physicians. Unlike a summary screen, which collates select patient information from other parts of the EMR, SynopSIS is specific to the current acute hospitalization and includes information not found elsewhere in the medical record.
To support rounding, SynopSIS gathers and presents data from the EMR in a printed Rounds Report (Fig. 3). The report is generated for all patients assigned to an inpatient service (eg, Medicine Team B) and emphasizes clarity and brevity using a format validated in the medical literature.24, 25 Each patient's report covers one fourth of a standard 8‐by‐11‐inch landscape‐printed page. The top half of each of these quarter‐page patient reports displays data stored in SynopSIS's interface and summarizes the patient's illness and the course of that illness. The lower half displays vital signs, intake/output, and laboratory data over the 24 hours from the time of printing. The most recent value and the range over the previous 24 hours of all vital signs are displayed. Intake/output totals are listed together with a structured breakdown. Laboratory results for the past 24 hours are listed with the most immediate prior values, allowing providers to discern trends. We envision providers obtaining a rounds report on arrival each day before examining their patients.
Importantly, although SynopSIS is part of the patient's medical record, physician users may change or overwrite the data in any field. This ability is a critical feature of the toolthe focus is on providing an interpretable snapshot of the patient. Data may be removed as their importance lessens or as the patient's condition changes, which contrasts with unchangeable documentation geared for alternative purposes, such as billing or medical‐legal requirements. Deleted data are saved in the medical record and are viewable by audit.
Program Evaluation
We have planned a postimplementation evaluation for SynopSIS. Each of the 3 functions (patient tracking, rounding, and care transitions) will be assessed separately. We will explore rounding efficiency and quality by survey and through direct observation. We plan to assess the percentage of time spent on direct patient care versus gathering patient data during morning rounds. We adapted elements of SynopSIS from UWCores, an existing sign‐out application in place at the University of Washington.24, 25 In a randomized trial, UWCores was shown to improve indicators of quality of care (more time spent with patients on rounds, fewer patients missed on rounds) and rounding efficiency (less time prerounding and rounding).25 For evaluation, we plan to use a previously published instrument25 in an online survey of SynopSIS users to assess perceived changes in the quality of sign‐out, providerprovider communication, and patient continuity of care. We intend to measure daily use of SynopSIS by primary providers, covering providers, and consulting physicians in order to assess its impact on each patient's care plan. We hypothesize that primary hospital physicians will access SynopSIS at least 3 times daily: on arrival at the hospital, after rounding, and prior to handoffs. We also plan to investigate whether consulting physicians will view SynopSIS daily rather than obtaining patient data such as labs and vital signs from separate parts of the EMR. Finally, we hypothesize that SynopSIS may facilitate initiation of appropriate discharge planning earlier in a patient's hospital course because it is viewable by nursing, care management, and social work personnel. Importantly, we will implement SynopSIS after the EMR gains universal use at our hospital. We will then wait for a washout following the EMR implementation in order to avoid confounding with the effects of the EMR. We will then be able to separate the effects of this tool from the effects of the EMR. Our EMR does not offer a function comparable to the rounds report or sign‐out tool in SynopSIS.
In addition to this quantitative evaluation process, we plan to solicit feedback from SynopSIS users in focus groups, including physicians at all levels of training as well as nonphysicians. We will use this information to revise SynopSIS according to the users' needs and to tailor the application to diverse specialty services.
DISCUSSION
Several systems have been developed to enhance communication among providers and to support the transfer of care of hospitalized patients.13, 14, 16, 19, 24, 25 We have developed a tool to support patient tracking, sign‐out, and rounding that incorporates key elements of previously designed systems and may improve communication among providers. SynopSIS helps to fulfill the 2006 JCAHO accreditation requirement for standardized communication for transfers of care when used with appropriate verbal communication, including an opportunity to ask and respond to questions.5 Research from other safety‐oriented industries recommends standardized information transfer, which SynopSIS will provide.20 What is innovative about SynopSIS is that it is not a stand‐alone system, but an integrated part of the EMR.
Currently, fewer than 5% of hospitals have an electronic sign‐out tool linked to hospital information systems27; therefore, SynopSIS has great potential for dissemination. In technical terms, this tool was coded by GE and could be readily adopted by any other GE Centricity Enterprise customer. Moreover, the conceptual model, the design strategy, and the critical system elements should be relevant to effective patient tracking, sign‐out, and rounding across different IT platforms.
Despite its strengths, the SynopSIS system has several limitations. First, appropriate transfer of care is a learned process that incorporates well‐described provider and system elements.15, 21, 2830 This tool cannot perform sign‐out; it makes up one part of an effective sign‐out process. As our institution implements SynopSIS, we will also proceed with educational efforts and infrastructure to improve the sign‐out process. Second, although data can be overwritten, prior screen versions are archived in the database. Because SynopSIS is part of the medical record, users may omit sensitive or clinically useful information because of medical‐legal concerns, such as sensitive family dynamics or patient behavioral issues that providers may be reluctant to document in the patient chart. Currently, such information is conveyed verbally during sign‐out. Third, as information gathering and transfer become more automated, informal person‐to‐person interactions among providers (eg, physicians and nurses) may erode. However, we expect that SynopSIS actually will enhance the quality of this communication because it places them on the same page. Finally, SynopSIS generates paper reports that must be disposed of in accordance with standards of patient confidentiality.
We believe that SynopSIS will improve the quality of care through several mechanisms. Because this single‐screen summary will be available to all members of a patients' care team, it is possible that SynopSIS will enable providers to share management plans more readily. Although nursing and care management do not use SynopSIS for their own handoffs, they have clamored for the ability to view it. In addition, rotating providers can readily assume care of an unfamiliar patient. By automating data‐gathering tasks, SynopSIS may foster efficiency and increase time with patients during rounds. For trainee providers in particular, such increased efficiency should allow more time for education and alleviate some of the pressures of duty‐hour compliance. Most important, SynopSIS frees the EMR from emulating the historic paper chart as its method of supporting clinical work flow and communication. That paradigm does not harness the power of today's EMR databases and integration capabilities31 and creates extra work through interruptive work flow and redundant effort.32 With SynopSIS reengineering, instead of providers having to serve the needs of the chart, the chart serves the needs of providers and patients.
Future clinical documentation and EMR systems should focus on provider work flow to improve quality and efficiency in patient care. Moreover, involving providers, including residents, in system design fosters innovation and optimally applies information technology to supporting clinical practice.
Acknowledgements
The authors acknowledge Harry Wong, Chutima Assapimonwait, and Vern Rogers for programming the application. Deborah G. Airo edited the manuscript.
The delivery of safe, high‐quality care to hospitalized patients depends on effective communication among providers.1, 2 Inpatients may receive care from a number of specialists in addition to their primary hospital physicians, and each provider may practice in a group that transfers care of individual patients among its members. This issue is exacerbated in teaching hospitals because fellows, residents, and interns make frequent transfers of care because of work‐hour rules.3, 4 Finally, teams of physician providers making management decisions must effectively communicate with other members of the care team, such as nurses, dieticians, and social workers, who also may be part of a group practice involving transfers. A patient hospitalized for just a few days in a modern hospital may receive care from dozens of providers and be the subject of multiple transfers of care, or handoffs, that require effective communication. Therefore, as part of its 2006 National Patient Safety Goals,5 the Joint Commission on Accreditation of Health Care Organizations (JCAHO) now requires that each hospital implement a standardized, structured approach to transfers of care.
Transfers of care have been shown to be a source of medical errors and adverse patient outcomes.2, 6, 7 In many cases, the critical information necessary to avert medical errors exists but is not available in real time to providers.6
Traditionally, provider teams have relied on the patient chart, in concert with direct patient evaluation, to provide the information to guide decision making during a hospitalization. Unfortunately, the structure of the chart in most hospitals has evolved little over the past 80 years810 and remains organized so that information is more easily filed than retrieved, read, or summarized.811 Typically, electronic medical records (EMRs) mimic the appearance of paper records and include similar organizational flaws.12 As a result, many providers have created ad hoc informational systems, separate from the chart, designed to track a patient's progress over time and to facilitate transfers of care. These sign‐out systems, which are intended to complement verbal sign‐out between providers,1315 range in complexity from simple handwritten index cards16 to adapted spreadsheets, PDA systems,17, 18 and more complex data systems (eg, FileMaker Pro)19 and often contain crucial information not found elsewhere in the medical record.20, 21
Although sign‐out systems are crucial to patient safety, they have several drawbacks. First, ad‐hoc informational systems may not be standardized, resulting in content and accuracy that vary among providers.22 These systems may fail to identify critical elements of a patient's condition, promoting ineffective communication and placing the patient at increased risk of adverse events.7, 13, 23
These observations underscore the need for a standardized patient‐tracking instrument that can distill crucial patient information, enhance communication, support transfers, improve efficiency, and enhance continuity of patient care.
We aimed to develop an integrated, problem‐based patient‐tracking tool as part of our hospital's EMR. The tool, SynopSIS, supports patient tracking, transfers of care (ie, sign‐outs), and daily rounds.
METHODS
Setting
The study took place at a 547‐bed adult and pediatric tertiary‐care university‐based teaching hospital with 2 campuses at the University of California, San Francisco, Medical Center (UCSFMC).
PROGRAM DESCRIPTION
Development and Design
A multidisciplinary team of practicing residents and attending physicians, information technology leaders, software engineers, and experts in medical communication and sign‐out developed the SynopSIS tool. We reviewed the literature to incorporate key design elements of other successfully implemented information transfer systems.24, 25
We conducted a formal review of existing patient‐tracking and sign‐out systems at our hospital to characterize provider work practices, with an emphasis on the specific information requirements of different specialties. A needs assessment of current sign‐out processes at UCSFMC was conducted by personal interviews with a chief resident or representative of each of the 18 Accreditation Council of Graduate Medical Education (ACGME) accredited residency programs through the dean's office of Graduate Medical Education. This needs assessment revealed that the majority of the programs did not have a standardized mechanism for sign‐out. Although most did use a written format for sign‐out, the actual type of written format varied from handwritten cards to databases using a variety of programs including Filemaker Pro, Microsoft Excel, and Microsoft Word. When asked what could improve the sign‐out system for their program, they most often responded that it would be having a standardized computerized sign‐out system in the hospital.26
During the design and pilot phase, we presented each SynopSIS function to an advisory committee of more than 50 trainees in medical, surgical, and pediatric general and subspecialty fields. Their input shaped the information content and presentation of our tool. In addition, we discussed the tool with the attending‐physician advisory group that oversees the implementation of clinical information systems in our hospital system.
Conceptual Model
We developed this conceptual model by integrating existing scholarship and input from stakeholders at our institution. First, we reviewed existing literature on documentation and transfers of care. Next, we conducted several focus group sessions with our EMR Residents' Advisory Group to conceptualize work flow and handoff needs for hospital physicians across specialties. We arrived at this model after several iterations of feedback from providers.
SynopSIS maps patient data available in the EMR to each of the 3 main functions according to type of clinical decisions supported by that function (Fig. 1). For example, data needed for effective patient tracking, such as likely functional status, are required to make decisions over the course of a patient's hospitalization. Similarly, data needed for sign‐out are used to make decisions over the course of a shift, typically overnight; and data needed for morning rounds are used to make decisions for the day. Although the information required for each function overlaps considerably, there are specialized data elements unique to each function.
Description of Functionality
SynopSIS is integrated with our hospital's EMR, General Electric (GE) Centricity Enterprise. The physician interface for SynopSIS is shown in Figure 2. After selecting a patient from a list corresponding to a given inpatient service (eg, Medicine Team B), the user selects the menu option to view the SynopSIS screen, which provides an at a glance overview of the patient's current condition. Different fields on the screen support each of SynopSIS's 3 main functions. At the top, the patient's demographic and registration information is displayed, including name, location, age, medical record number, and attending physician. Below are fields viewable and editable by users of the EMR. The Admission Diagnosis/Course and Problem List fields support patient tracking and allow a receiving physician to understand the reason for the patient's admission, the overall course of the illness, and the current active problems. The problem list is entered by the primary hospital physician. The Anticipated Problems/To Do List field supports the sign‐out function from which providers can coordinate care‐related activities and make contingency plans for anticipated events. The patients' most recent laboratory results and vital signs are displayed on the lower left of the screen for easy reference during face‐to‐face physician sign‐outs. Finally, the CODE status, Allergies, and Medications fields allow efficient tracking of information. Temporarily, until the pharmacy component of the EMR goes into use, the primary hospital physician will enter and update the medications. When the pharmacy is linked to the EMR, medications will be added directly from the inpatient pharmacy records to the EMR‐linked sign‐out tool.
This on‐screen SynopSIS view is distinct from the summary screen typically seen in EMRs, including vendor‐based and the Veterans' Affairs systems. For instance, the Veterans' Affairs summary screen incorporates clinical and nonclinical data, including demographic and payment information, upcoming appointments, and patient‐specific information such as allergies. Moreover, it is not editable by primary hospital physicians. Unlike a summary screen, which collates select patient information from other parts of the EMR, SynopSIS is specific to the current acute hospitalization and includes information not found elsewhere in the medical record.
To support rounding, SynopSIS gathers and presents data from the EMR in a printed Rounds Report (Fig. 3). The report is generated for all patients assigned to an inpatient service (eg, Medicine Team B) and emphasizes clarity and brevity using a format validated in the medical literature.24, 25 Each patient's report covers one fourth of a standard 8‐by‐11‐inch landscape‐printed page. The top half of each of these quarter‐page patient reports displays data stored in SynopSIS's interface and summarizes the patient's illness and the course of that illness. The lower half displays vital signs, intake/output, and laboratory data over the 24 hours from the time of printing. The most recent value and the range over the previous 24 hours of all vital signs are displayed. Intake/output totals are listed together with a structured breakdown. Laboratory results for the past 24 hours are listed with the most immediate prior values, allowing providers to discern trends. We envision providers obtaining a rounds report on arrival each day before examining their patients.
Importantly, although SynopSIS is part of the patient's medical record, physician users may change or overwrite the data in any field. This ability is a critical feature of the toolthe focus is on providing an interpretable snapshot of the patient. Data may be removed as their importance lessens or as the patient's condition changes, which contrasts with unchangeable documentation geared for alternative purposes, such as billing or medical‐legal requirements. Deleted data are saved in the medical record and are viewable by audit.
Program Evaluation
We have planned a postimplementation evaluation for SynopSIS. Each of the 3 functions (patient tracking, rounding, and care transitions) will be assessed separately. We will explore rounding efficiency and quality by survey and through direct observation. We plan to assess the percentage of time spent on direct patient care versus gathering patient data during morning rounds. We adapted elements of SynopSIS from UWCores, an existing sign‐out application in place at the University of Washington.24, 25 In a randomized trial, UWCores was shown to improve indicators of quality of care (more time spent with patients on rounds, fewer patients missed on rounds) and rounding efficiency (less time prerounding and rounding).25 For evaluation, we plan to use a previously published instrument25 in an online survey of SynopSIS users to assess perceived changes in the quality of sign‐out, providerprovider communication, and patient continuity of care. We intend to measure daily use of SynopSIS by primary providers, covering providers, and consulting physicians in order to assess its impact on each patient's care plan. We hypothesize that primary hospital physicians will access SynopSIS at least 3 times daily: on arrival at the hospital, after rounding, and prior to handoffs. We also plan to investigate whether consulting physicians will view SynopSIS daily rather than obtaining patient data such as labs and vital signs from separate parts of the EMR. Finally, we hypothesize that SynopSIS may facilitate initiation of appropriate discharge planning earlier in a patient's hospital course because it is viewable by nursing, care management, and social work personnel. Importantly, we will implement SynopSIS after the EMR gains universal use at our hospital. We will then wait for a washout following the EMR implementation in order to avoid confounding with the effects of the EMR. We will then be able to separate the effects of this tool from the effects of the EMR. Our EMR does not offer a function comparable to the rounds report or sign‐out tool in SynopSIS.
In addition to this quantitative evaluation process, we plan to solicit feedback from SynopSIS users in focus groups, including physicians at all levels of training as well as nonphysicians. We will use this information to revise SynopSIS according to the users' needs and to tailor the application to diverse specialty services.
DISCUSSION
Several systems have been developed to enhance communication among providers and to support the transfer of care of hospitalized patients.13, 14, 16, 19, 24, 25 We have developed a tool to support patient tracking, sign‐out, and rounding that incorporates key elements of previously designed systems and may improve communication among providers. SynopSIS helps to fulfill the 2006 JCAHO accreditation requirement for standardized communication for transfers of care when used with appropriate verbal communication, including an opportunity to ask and respond to questions.5 Research from other safety‐oriented industries recommends standardized information transfer, which SynopSIS will provide.20 What is innovative about SynopSIS is that it is not a stand‐alone system, but an integrated part of the EMR.
Currently, fewer than 5% of hospitals have an electronic sign‐out tool linked to hospital information systems27; therefore, SynopSIS has great potential for dissemination. In technical terms, this tool was coded by GE and could be readily adopted by any other GE Centricity Enterprise customer. Moreover, the conceptual model, the design strategy, and the critical system elements should be relevant to effective patient tracking, sign‐out, and rounding across different IT platforms.
Despite its strengths, the SynopSIS system has several limitations. First, appropriate transfer of care is a learned process that incorporates well‐described provider and system elements.15, 21, 2830 This tool cannot perform sign‐out; it makes up one part of an effective sign‐out process. As our institution implements SynopSIS, we will also proceed with educational efforts and infrastructure to improve the sign‐out process. Second, although data can be overwritten, prior screen versions are archived in the database. Because SynopSIS is part of the medical record, users may omit sensitive or clinically useful information because of medical‐legal concerns, such as sensitive family dynamics or patient behavioral issues that providers may be reluctant to document in the patient chart. Currently, such information is conveyed verbally during sign‐out. Third, as information gathering and transfer become more automated, informal person‐to‐person interactions among providers (eg, physicians and nurses) may erode. However, we expect that SynopSIS actually will enhance the quality of this communication because it places them on the same page. Finally, SynopSIS generates paper reports that must be disposed of in accordance with standards of patient confidentiality.
We believe that SynopSIS will improve the quality of care through several mechanisms. Because this single‐screen summary will be available to all members of a patients' care team, it is possible that SynopSIS will enable providers to share management plans more readily. Although nursing and care management do not use SynopSIS for their own handoffs, they have clamored for the ability to view it. In addition, rotating providers can readily assume care of an unfamiliar patient. By automating data‐gathering tasks, SynopSIS may foster efficiency and increase time with patients during rounds. For trainee providers in particular, such increased efficiency should allow more time for education and alleviate some of the pressures of duty‐hour compliance. Most important, SynopSIS frees the EMR from emulating the historic paper chart as its method of supporting clinical work flow and communication. That paradigm does not harness the power of today's EMR databases and integration capabilities31 and creates extra work through interruptive work flow and redundant effort.32 With SynopSIS reengineering, instead of providers having to serve the needs of the chart, the chart serves the needs of providers and patients.
Future clinical documentation and EMR systems should focus on provider work flow to improve quality and efficiency in patient care. Moreover, involving providers, including residents, in system design fosters innovation and optimally applies information technology to supporting clinical practice.
Acknowledgements
The authors acknowledge Harry Wong, Chutima Assapimonwait, and Vern Rogers for programming the application. Deborah G. Airo edited the manuscript.
- ,,.Crew resource managment and its applications in medicine. Making health care safer: A critical analysis of patient safety practices. Evidence report/technology assessment2001. AHRQ publication 01‐E058(43).
- ,.Internal Bleeding: The Truth behind America's Terrifying Epidemic of Medical Mistakes.New York, NY:Rugged Land;2004.
- ,,.New requirements for resident duty hours.JAMA.2002;288:1112–1124.
- ,,,.The impact of a regulation restricting medical house staff working hours on the quality of patient care.JAMA.1993;269:374–378.
- Joint Commission 2006 National Patient Safety Goals Implementation Expectations.2005. Available at: http://www.jcaho.org/accredited+organizations/patient+safety/06_npsg_ie.pdf.
- ,,.Gaps in the continuity of care and progress on patient safety.BMJ.2000;320:791–794.
- ,,,,.Does housestaff discontinuity of care increase the risk for preventable adverse events?Ann Intern Med.1994;121:866–872.
- .The problem‐oriented record—its organizing principles and its structure.League Exch.1975 (103):3–6.
- .The problem oriented record as a basic tool in medical education, patient care and clinical research.Ann Clin Res.1971;3(3):131–134.
- .Medical records, patient care, and medical education.Ir J Med Sci.1964;17:271–282.
- ,,, et al.Creating a note classification scheme for a multi‐institutional electronic medical record.AMIA Annu Symp Proc.2003:968.
- ,,,,,.Impacts of computerized physician documentation in a teaching hospital: perceptions of faculty and resident physicians.J Am Med Inform Assoc.2004;11:300–309.
- ,,,,.Using a computerized sign‐out program to improve continuity of inpatient care and prevent adverse events.Jt Comm J Qual Improv.1998;24(2):77–87.
- ,.Signing out patients for off‐hours coverage: comparison of manual and computer‐aided methods.Proc Annu Symp Comput Appl Med Care.1992:114–118.
- ,,,,.Managing discontinuity in academic medical centers: strategies for a safe and effective resident sign‐out.J Hosp Med.2006;1:257–266.
- ,,.Utility of a standardized sign‐out card for new medical interns.J Gen Intern Med.1996;11:753–755.
- ,,.The potential role of IT in supporting the work of junior doctors.J R Coll Physicians Lond.2000;34:366–370.
- ,,,.Electronic Sign‐out using a personal digital assistant.Psychiatr Serv.2001;52(2):173–174.
- .“Doctor's notes”: a computerized method for managing inpatient care.Fam Med.1988;20:223–224.
- ,,,,.Handoff strategies in settings with high consequences for failure: lessons for health care operations.Int J Qual Health Care.2004;16(2):125–132.
- ,,, et al.Understanding patient‐centered care in the context of total quality management and continuous quality improvement.Jt Comm J Qual Improv.1994;20(3):152–161.
- ,,.Utility of a standardized sign‐out card for new medical interns.J Gen Intern Med.1996;11:753–755.
- ,,,.Post‐call transfer of resident responsibility: its effect on patient care.J Gen Intern Med.1990;5:501–505.
- ,,,.Organizing the transfer of patient care information: the development of a computerized resident sign‐out system.Surgery.2004;136(1):5–13.
- ,,,,.A randomized, controlled trial evaluating the impact of a computerized rounding and sign‐out system on continuity of care and resident work hours.J Am Coll Surg.2005;200:538–545.
- .UCSFMC sign‐out needs assessment [personal communication].2007.
- ,.Is 80 the cost of saving lives? Reduced duty hours, errors, and cost.J Gen Intern Med.2005;20:969–970.
- ,,.Intern curriculum: the impact of a focused training program on the process and content of sign‐out out patients. Harvard Medical School Education Day2004.
- .When conversation is better than computation.J Am Med Inform Assoc.2000;7:277–286.
- ,.Communication behaviours in a hospital setting: an observational study.BMJ.1998;316:673–676.
- ,,,.Integration and beyond: linking information from disparate sources and into workflow.J Am Med Inform Assoc.2000;7(2):135–145.
- .Update on the electronic medical record.Otolaryngol Clin North Am.2002;35:1223–1236, vii.
- ,,.Crew resource managment and its applications in medicine. Making health care safer: A critical analysis of patient safety practices. Evidence report/technology assessment2001. AHRQ publication 01‐E058(43).
- ,.Internal Bleeding: The Truth behind America's Terrifying Epidemic of Medical Mistakes.New York, NY:Rugged Land;2004.
- ,,.New requirements for resident duty hours.JAMA.2002;288:1112–1124.
- ,,,.The impact of a regulation restricting medical house staff working hours on the quality of patient care.JAMA.1993;269:374–378.
- Joint Commission 2006 National Patient Safety Goals Implementation Expectations.2005. Available at: http://www.jcaho.org/accredited+organizations/patient+safety/06_npsg_ie.pdf.
- ,,.Gaps in the continuity of care and progress on patient safety.BMJ.2000;320:791–794.
- ,,,,.Does housestaff discontinuity of care increase the risk for preventable adverse events?Ann Intern Med.1994;121:866–872.
- .The problem‐oriented record—its organizing principles and its structure.League Exch.1975 (103):3–6.
- .The problem oriented record as a basic tool in medical education, patient care and clinical research.Ann Clin Res.1971;3(3):131–134.
- .Medical records, patient care, and medical education.Ir J Med Sci.1964;17:271–282.
- ,,, et al.Creating a note classification scheme for a multi‐institutional electronic medical record.AMIA Annu Symp Proc.2003:968.
- ,,,,,.Impacts of computerized physician documentation in a teaching hospital: perceptions of faculty and resident physicians.J Am Med Inform Assoc.2004;11:300–309.
- ,,,,.Using a computerized sign‐out program to improve continuity of inpatient care and prevent adverse events.Jt Comm J Qual Improv.1998;24(2):77–87.
- ,.Signing out patients for off‐hours coverage: comparison of manual and computer‐aided methods.Proc Annu Symp Comput Appl Med Care.1992:114–118.
- ,,,,.Managing discontinuity in academic medical centers: strategies for a safe and effective resident sign‐out.J Hosp Med.2006;1:257–266.
- ,,.Utility of a standardized sign‐out card for new medical interns.J Gen Intern Med.1996;11:753–755.
- ,,.The potential role of IT in supporting the work of junior doctors.J R Coll Physicians Lond.2000;34:366–370.
- ,,,.Electronic Sign‐out using a personal digital assistant.Psychiatr Serv.2001;52(2):173–174.
- .“Doctor's notes”: a computerized method for managing inpatient care.Fam Med.1988;20:223–224.
- ,,,,.Handoff strategies in settings with high consequences for failure: lessons for health care operations.Int J Qual Health Care.2004;16(2):125–132.
- ,,, et al.Understanding patient‐centered care in the context of total quality management and continuous quality improvement.Jt Comm J Qual Improv.1994;20(3):152–161.
- ,,.Utility of a standardized sign‐out card for new medical interns.J Gen Intern Med.1996;11:753–755.
- ,,,.Post‐call transfer of resident responsibility: its effect on patient care.J Gen Intern Med.1990;5:501–505.
- ,,,.Organizing the transfer of patient care information: the development of a computerized resident sign‐out system.Surgery.2004;136(1):5–13.
- ,,,,.A randomized, controlled trial evaluating the impact of a computerized rounding and sign‐out system on continuity of care and resident work hours.J Am Coll Surg.2005;200:538–545.
- .UCSFMC sign‐out needs assessment [personal communication].2007.
- ,.Is 80 the cost of saving lives? Reduced duty hours, errors, and cost.J Gen Intern Med.2005;20:969–970.
- ,,.Intern curriculum: the impact of a focused training program on the process and content of sign‐out out patients. Harvard Medical School Education Day2004.
- .When conversation is better than computation.J Am Med Inform Assoc.2000;7:277–286.
- ,.Communication behaviours in a hospital setting: an observational study.BMJ.1998;316:673–676.
- ,,,.Integration and beyond: linking information from disparate sources and into workflow.J Am Med Inform Assoc.2000;7(2):135–145.
- .Update on the electronic medical record.Otolaryngol Clin North Am.2002;35:1223–1236, vii.
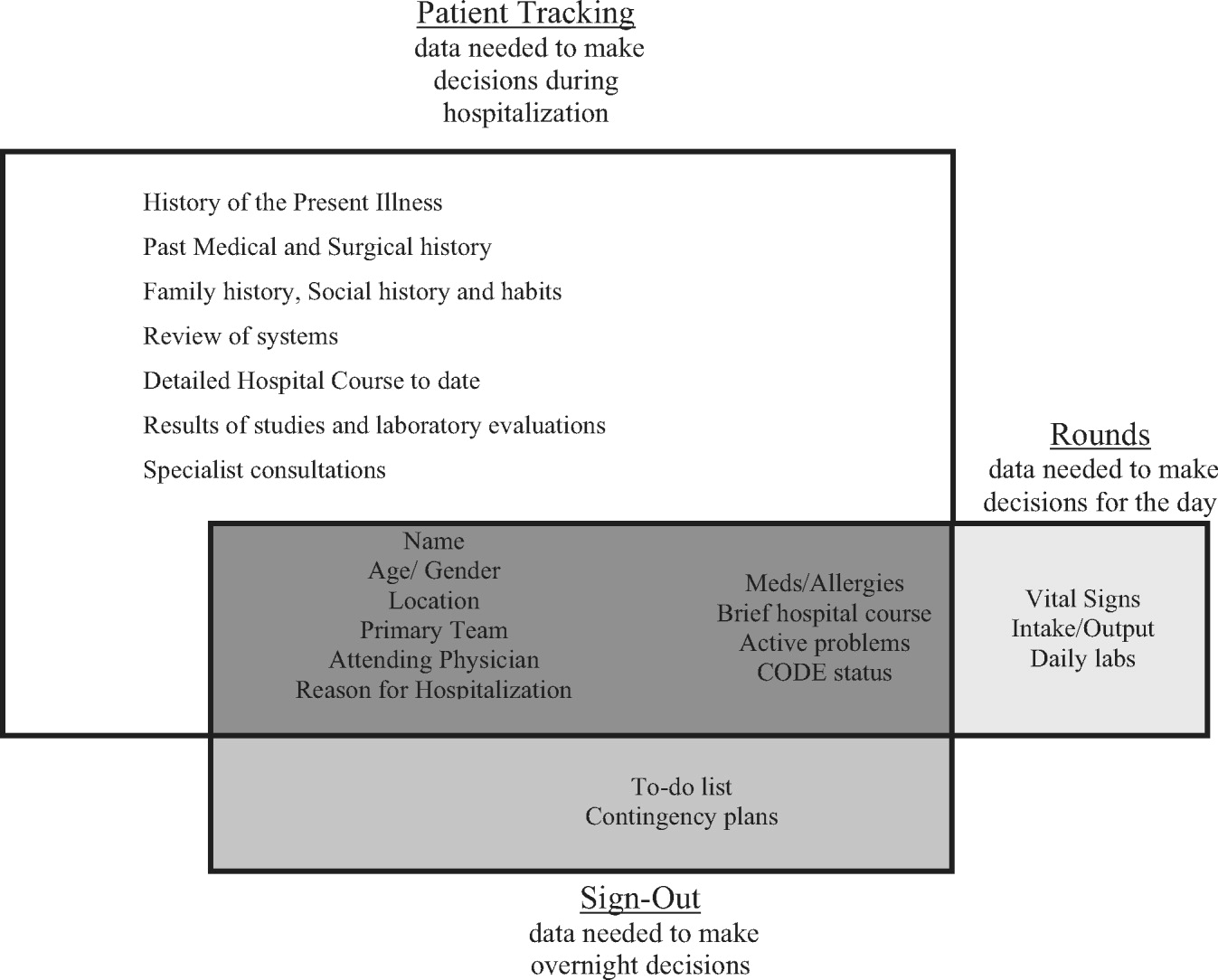
Barriers to Mobility During Hospitalization
Institute of Medicine (IOM) reports1, 2 have estimated that between 44,000 and 98,000 patients die every year in hospitals because of iatrogenic errors of omission and commission. More people die in a year from medical errors than from car accidents (43,458), breast cancer (42,297), or AIDS (16,515).3 The IOM report recommended a goal of a 50% reduction in errors over the next 5 years.4 Since publication of these reports, a great deal of interest has been focused on how to make our hospitals safer.5, 6 Times of transitions in care (eg, from home to hospital, from emergency department to hospital, from the intensive care unit to the general ward) have been identified as opportune times to improve continuity and thus to decrease errors.
The hospital discharge process is often nonstandardized and frequently marked by poor quality.7 One in five hospital discharges is complicated by adverse events within 30 days, many of which lead to visits to emergency departments (EDs) and rehospitalization.810 Nationally, approximately 25% of hospitalized patients are readmitted within 90 days, often because of errors resulting from discontinuity and fragmentation of care at discharge, which exposes patients to iatrogenic risk and raises costs.11, 12 Low health literacy rates, lack of coordination in the handoff from the hospital to community care, gaps in social supports, and the absence of physician follow‐up after discharge place patients at high risk of rehospitalization.1315 Increasingly, as hospitalists provide more inpatient care, it is difficult for primary care physicians to be aware of all the complexities of a hospitalization.16
Studying the hospital discharge process provides an opportunity to learn more about its complexities,17 which could then be used to standardize the process and focus on those interventions that reduce the number of medical errors and resulting adverse events. However, to date, few studies have described the essential components of the discharge process, and no studies have focused on the discharge process from the point of view of the hospitalized patient. Therefore, a qualitative study was conducted in order to understand the phenomenon of frequent rehospitalization from the perspective of the discharged patient and to determine if activities at the time of discharge could be designed to reduce the number of adverse events and rehospitalizations.
METHODS
The larger study of which this work is a part examined the transition from inpatient service at a large inner‐city hospital to community care in order to lead to the development of an intervention to improve the discharge process. Qualitative research stresses the socially constructed nature of reality, and qualitative researchers seek to answer questions that stress how social experience is created and given meaning.18 Qualitative interviewing permits the researcher to understand the world as seen by the respondent within the context of the respondent's everyday life.19 Learning from the experiences of patients hospitalized more than once in a 6‐month period will help to identify their perceptions and beliefs about their disease and discharge instructions and assist additional interventions that could prevent rehospitalization.
Sample
Semistructured, open‐ended interviews were conducted with 21 patients during their hospital stay at Boston Medical Center. To be eligible for the study, a patient had to receive medical care through a health center affiliated with Boston Health Net, a network of community health centers serving primarily low‐income patients, and had to have been hospitalized on at least 1 additional occasion in the previous 6 months. Each day during the interview period the Boston Health Net nurse identified all patients previously admitted within 6 months and contacted the interviewer with the names and room numbers of those patients. The interviewer (M.S.) approached potential participants in their hospital rooms and obtained informed consent at the time of the interview. If the patient agreed, the interview was conducted at that time. If the patient was not available at that time, the interviewer made at least 2 attempts to visit the patient at a convenient time. The interviews were conducted on 17 days of a 4‐month period with no more than 2 interviews completed a day. The participants ranged in age from 18 to 79; 10 respondents were male, and 11 were female. All were English speaking. The mean age of the 20 patients who provided demographic information was 45.55 years, and the median age was 47 years. Nine of the participants reported their racial or ethnic identities as white (5 male, 3 female), 3 as black (2 male, 1 female), 4 as African American (1 male, 3 female); 1 as Latina; 1 as Hispanic (male), 1 as Spanish (male), and 1 as mixed (female). One male and 1 female participant provided no race or ethnic identity. Two participants were excluded from the study because they did not speak English, and 2 were excluded because they were unable to speak due to their medical conditions. Interviews were audiotaped, but full names were not used on the tape. Only subject code numbers were used to identify respondents. The discharge records of each participant were reviewed for consistency with that participant's descriptions of his or her condition. The study was approved by the Institutional Review Board of Boston University Medical Center.
Interview Guide
To help assure collection of comparable qualitative data, an interview guide listed specific questions and topics to be covered in a particular order in the interview. Questions were drawn in part from a pilot test of interviewing patients on the inpatient service rehospitalized within 90 days of the previous admission.17 Interviews assessed continuity of care after discharge, need for and availability of social support, and the participant's ability to obtain follow‐up medical care. The interview script consisted of open‐ended questions about events leading up to the current hospitalization, previous hospitalizations, instructions received the last time discharged, home situation, and ability to attend medical appointments, and participant feedback on the discharge process was requested. Follow‐up questions were asked based on a patient's responses to these questions. Interviews lasted between 20 and 45 minutes.
Analysis
The interview tapes were transcribed by a subcontracted transcriber, and the transcripts were checked for accuracy by the interviewer. Each interview was evaluated according to a set of thematic codes developed by 2 qualitative researchers (L.S. and M.S.). The codes represent categories or themes found in the data, and the appropriate codes were attached to their corresponding sections of text. To improve interrater reliability in coding, the 2 qualitative researchers coded 3 interviews, reviewed the codes, and, once it was clear that they both understood the coding scheme, coded the interviews. They resolved any problem cases and checked each other's work throughout the coding process to ensure that each interview was coded correctly. The findings were analyzed to explore whether there were linkages between and among particular themes. The discharge records of all patients were reviewed in order to compare the discharge notes about each patient's condition with that patient's own description of his or her condition and treatment.
RESULTS
All the patients who participated in this study were able to describe their medical condition and the reasons they were admitted to the hospital. Almost all, 20 of the 21 participants, were rehospitalized for the same primary diagnosis. For 5 of these 20 participants, length of time since the last hospitalization was 5‐6 months (4 for diabetes control, 1 for a lupus erythematosus flare); for 4 participants time since last hospitalization was between 6 weeks and 2 months (1 because of a fall, 1 because of seizures, 1 with hypertension, and 1 with SOB); for 8 participants time since last hospitalization was between 3 weeks and 1 month (2 with kidney disease, 2 with seizures, and 1 each with chronic obstructive pulmonary disease, sickle cell disease, PVD, and alcoholic gastritis), and for 3 participants time since last hospitalization was 1‐2 weeks (1 each with abdominal pain, alcohol intoxication, and lower gastrointestinal bleed). The principal diagnosis in a patient's discharge records matched that participant's description. Participants also described the discharge instructions they received. Although some did not report the brand names of the medications they were taking, all reports of the types of medications being taken or the conditions for which the medications were prescribed were consistent with discharge summaries. Although none of the participants incorrectly reported a medication or condition to the interviewer, a few did not provide information about every medication or condition. In 1 case the discharge summary noted medications for bipolar disorder and mental illness; in 2 cases medications were prescribed for depression. None of these participants mentioned these conditions or medications to the interviewer. One patient talked about stress and depression, but nothing was written about these issues in the discharge record.
For participants in this study, difficult life circumstances posed a greater barrier to recuperation than did lack of medical knowledge. The interviews conducted in this study illustrate the personal and social impact of disease that resulted in rehospitalization.
Discharge and Medical Knowledge
During discharge, transition care processes can fail at many points.20 These include: communication of the care plan, reconciliation of current and initial medication regimens, transportation of the patient, follow‐up care with a provider, and preparation of patient and caregiver for maintaining the patient's regimen.4, 2022 Participants in this study identified some of these and other factors as constituting barriers to effective care transitions.
At discharge, 7 participants were advised by physicians to change their diets or refrain from tobacco or alcohol use. Participants clearly understood the instructions and could give detailed accounts of diet changes they were supposed to make or explain the reasons tobacco or alcohol use caused or exacerbated their diseases. A diabetic whose discharge instructions included diet change listed sweet ones, starchy oneswith a lot of carbohydrates as foods she is not supposed to eat, wherease others described the links between alcohol use and adverse health: In my mind, I think that alcohol is a way out.But I know that it, that it's not.And so, the pancreatitis develops.
Lack of understanding about their medical condition or of knowledge about procedures to be followed was not evident in this population. Instead, recuperation was compromised by factors such as distress, substance use, support for medical and basic needs, and limitations in the availability of transportation to medical appointments. Many participants reported not receiving necessary rest as a result of needing to work or care for young children.
Crises and Coping: Distress
Despite understanding needed behavior changes, almost half the participants explained how difficult life circumstances and gaps in ongoing care or support made it impossible for them to follow medical advice.
Almost half the participants described themselves as being stressed, sad, or depressed. Their explanations indicate a relationship between distress and subsequent behaviors that exacerbated their conditions.
Of 3 self‐described alcoholics, one, a 52‐year‐old white man rehospitalized for alcohol related seizures, had relapsed after the deaths of his mother and his girlfriend. He explained, Well, after my girlfriend died, I really started to hit the bottle. Another, an unemployed 45‐year‐old black woman, lacked stable housing and at the time of the interview lived with a heavy drinker. She said that when I get stressed out, the first thing I want to do is go run to the [liquor] store. The third self‐described alcoholic, a 62‐year‐old white man, reported drinking because of lack of regular treatment for chronic depression:
My problem is has to do with stress and depression, which is what I'm gonna try to deal with this time. 'Cause that'scontributed to me getting so depressed I justjust started drinking again. I justnext time it'll kill me. So. That's almosta kind of a suicide wish, I guess.I know it's gonna kill me if I keep drinking.I think I need to get into something. Butthere'sI don't know if you call it substance abuse, butI think it's related todeep depression, which is not necessarily substance abuse, but it canI'm sure there's some relationship.
Similarly, the experiences of participants with diabetes illustrate clearly how depression contributed to undermining their ability to follow their doctors' recommendations. For example, an 18‐year‐old African American teenager rehospitalized for diabetes control discussed her inability to maintain her physician‐recommended diet:
Like when I'm stressed out.I get depressed and, umI give up. Just don't wanna do it anymore. It's not [that] I don't want to, I can't. I just can't do it I, when I got home, I actually did good! I actually really did good. I was eating salads. I did go on a diet. I ate salads, grilled food, and things like that. I took my medicine. I started loggin', like writin' everything down in a book. I wrote down what I ate every day, what my blood sugar was, and how much medicine I took. I was doin' good. But then I got depressed, and I stopped doin' it.
Continuity of Condition Management
Participants expressed a need after discharge for help at home, although in most cases, the help they reported needing did not require medical knowledge or technical skills.
Skilled Care
Few participants reported needing and/or receiving visiting nurse services; even in these cases, some of the responsibility for care fell to family members. Their health suffered because they lacked sufficient access to visiting nurse services or other needed support. A 42‐year‐old Latina diabetic with kidney infection described a visiting nurse's unsuccessful attempt to teach her husband how to change her catheter:
They try to show, 'cause before? I don't got the catheter, they're comin' in my house, in the morning? You know, put the catheter into my bladder, and they come back before me go to sleep, they try to show my husband how to do it, but he can't [CHUCKLES LIGHTLY], you know, he can't.So thethe doctor decide to leave the catheter there.
Basic Need Care
For most participants, the posthospital assistance needed did not require medical expertise. In the period after their last hospitalization, most participants needed assistance with daily chores such as cleaning, cooking, child care, and driving; they turned to friends and family members to meet these needs. However, because no family member was capable of providing full‐time care during recuperation, some participants were unable to follow advice from physicians about resting or refraining from certain activities. A 67‐year‐old African American man whose foot ulcers kept him from walking explained that during his recuperation he had to stay in the same place for 8 hours while his brother worked:
Oh, maybe if I had to go to the bathroom or something, I can'tbut for the most part, I guess I had things set upwhere I didn't, you know, where I didn't moveI just set my things up to keep me from movin' all day. I'd set my food up and everything else, little sandwich and all that. So, there wasn't anything aboutyou know, worrying about movin'or getting hungry, I guess.
None of the participants were able to pay for support services such as housecleaning or in‐home care, and all relied on busy friends and family members to meet their needs.
The experiences of 3 single mothers with health conditions characterized by debilitating chronic pain illustrate how very different access to supportive family members affected their ability to seek care and follow medical instructions as well as how child care responsibilities compromised their recuperation. One, a 20‐year‐old African American woman hospitalized for polycystic kidney disease, described situations during which the intensity of the pain did not permit her to do basic household chores. At those times she relied on her 5‐year‐old son:
Hehe actually knows how to sweep, he knows how to wash dishes. At 5 and a half, he surprised me, but [CHUCKLES] he can wash dishes, so. He has to get up on a chair, but he can wash 'em.
As a result of needing more care than was available, she traveled south to stay with her mother, who was unable to leave work to come to Boston:
I took the bus because my son has sickle cell trait, so they told me from day one it's not really good for him to fly on a plane? So, I had to take himit took like 20 hoursyou know, stoppin' here, stoppin' there, like, pullin' my bags and stuff, so it put me in more pain than I was in.
Another, a 24‐year‐old of mixed background chronically hospitalized with sickle cell pain crises, delayed medical treatment because of lack of child care:
There's been times that I have had to wait till I could find somebody to watch my kids, to even come to the hospital.There's been times thatuh, it'd be a while before I could get anybody, so instead of me coming to the hospital, I have to wait at home, in a lot of pain.I would have to waitany time between 5 hours to 2 days before I could find somebody to watch my kids.
This pattern of child care interfering with recovery continued after leaving the hospital:
The minute I get home it'd be nice to have somebody to watch the kids, so I could at least recuperate for like 24 hours before I have to take care of thingsI would have to usually just go home and just get right to it.
The experience of a third, a 29‐year‐old African American woman with systemic lupus erythematosus, illustrates the ways in which family support can ease the burden of illness. This participant relocated to be close to her mother, aunt, and cousins, all of whom cared for her children when she is in the hospital:
When I was in [NEIGHBORING STATE] it was terrible'cause my, my kids wasn't goin' to school, 'cause I couldn't get up to get them dressed and wake them up. My daughter almost got kept back and stuff. It was real hardand it wasn't good, you know, that they could justrun through the house rampant, do whatever they want and not be supervised.So that was very dangerous, too. And then, it put like, it put a strain on my oldest, my daughter
She contrasted this with her current situation in which family members cared for her children when she is in the hospital or sick at home:
Like, this morningthey took the kids to school for me and everything. Made 'em breakfast, made sure they was dressed right this morningMy mother picked them up from school this afternoon.
Transportation to Appointments
Travel to follow‐up appointments was difficult for many participants. Almost half reported taking public transportation to appointments; the others either drove themselves, were driven by relatives or friends, or paid for taxis. Those relying on public transportation were more likely than others to miss appointments because of transportation issues if they did not feel well:
Depending how I feel. If I feel all right, I'll take the bus; if not, I'll get a taxi or I'll just won't show up. I would borrow a bus pass or somethin', you know, from [HIS NAME] is Joebecause I would make, like, evening appointments. Um, because my sickle cell tends to act up if it's coldSo, if it's really cold, I don't go.
As one 55‐year‐old white woman who has seizures summed up the matter of traveling by bus when not feeling well, You do what you have to do!
DISCUSSION AND CONCLUSIONS
The hospital discharge process has been identified as a time when sources of error occur that result in rehospitalization. Many factors that adversely affect care transitions apply to the hospital discharge process, including preparation of the patient and caregiver, communication of the care plan, changes in the medication regimen, transportation of the patient, scheduling of follow‐up care, and availability of advance care directives.20 Patients with low socioeconomic status have been found to be especially vulnerable after discharge. A 1989 telephone survey of 6455 patients recently discharged from hospitals in the United States found that low socioeconomic status and poor patient health were independent predictors of patient problems after discharge.21 A nationwide telephone survey of 1800 recently discharged patients and their care partners also revealed that low socioeconomic status and poor patient health status were associated with problems experienced by care partners.22
High rates of unnecessary rehospitalization have been shown to be related to poorly managed discharge processes.23 Although some factors identified in other studies of care transition did influence the rehospitalization of participants in this study; others did not. Transportation and follow‐up care greatly affected rehospitalization, whereas health literacy had a minimal effect. Fifteen of 20 participants were readmitted within weeks up to 2 months for the same primary diagnosis, yet they understood their medical conditions and knew the procedures to be followed. Having a chronic illness may have affected their understanding of their disease because they had received teaching over time. However, for most participants in this studyinner‐city, minority, low‐income patientsfactors beyond the discharge process affected their rehospitalization. Difficult life circumstances and gaps in ongoing care or support resulted in distress and behavior that exacerbated their conditions. Participants lacked social and emotional support that would have enabled them to prioritize maintaining their health.
Although there is not a universally accepted definition of the concept of social support, it is generally understood that it involves emotional connection and caring24 and occurs in a relationship in which the person providing the support is equipped to respond to a wide variety of needs ranging from practical assistance to counseling and encouragement based on the concerns or life circumstances of the patient. Qualitative studies of social support interventions demonstrate the ways in which having a dependable person to whom a patient can turn for encouragement, information, and practical assistance improves the patient's ability to maintain health regimens and manage chronic pain. An intervention in which nurses made weekly telephone contact with low‐income pregnant smokers helped these patients manage numerous stressors and, in some cases, reduce their tobacco use.25 A support group for women with chronic pain helped participants learn practical strategies for reducing pain and reduced isolation and emotional distress about their conditions.26 A study of consumer experiences of transition care27 found that the most valued institutions were those in which providers from one facility thoroughly communicated a patient's medical and treatment history to providers in another; also important was involving the consumer in medical decision making, preparing the consumer to actively participate in his or her own care, and attending to individual needs and preferences.
This study had several limitations, including reliance on participants' reports of their conditions and experiences with medical staff at a time when they were rehospitalized. In the vulnerable position of being hospitalized, participants may have been reluctant to have complaints about their hospital experiences tape‐recorded. All participants reported positive experiences with hospital staff during the formal interview. Two participants reported negative experiences with hospital staff after the audio‐recorder was turned off and the interview concluded. Other limitations of the hospital setting include limited privacy. Either a roommate was present during the interview or the interview was interrupted by a visit from a hospital staff person or a telephone call. Participants were asked to recall events that for some had occurred several months before the interview, introducing the possibility of inaccurate recall. To address these limitations, we compared interview transcripts to discharge summaries in order to assess any inconsistencies that may have resulted from this lack of privacy. The differences between summaries and patient self‐reports were that 2 participants did not report illicit substance use and 2 did not report psychiatric conditions. Despite these limitations, conducting this study in a hospital setting allowed investigators access to a highly vulnerable population that would be most affected by improvements in the discharge process. Given the difficulties many participants reported in getting to appointments, it is unlikely that a study conducted outside the hospital setting would have effectively reached this population.
These results support the findings in this study that life circumstances outside the hospital can be as important to recovery as institutional coordination of medical care. Although the stresses described by the low‐income patients in this study may not directly cause subsequent illness, their experiences clearly demonstrate the ways in which stresses make it difficult or impossible to attain sufficient rest to heal, maintain the behavioral change necessary to improve health, and follow instructions given by clinicians at the time of discharge. Interventions targeting low‐income patients thus are more likely to succeed if they include provisions for social support and assist patients in easing the burden of daily responsibilities. Effective transition care includes support that may not be explicitly medical, but without which participants lack the stability to fully recuperate. Without the possibility of taking a break from household or parenting responsibilities, it is difficult to rest enough to truly recover. The descriptions of extreme measures taken in order to obtain needed support illustrate how recuperation was compromised by both family responsibilities and lack of flexibility in caregiver work schedules. Distress, particularly depression, further contributed to poor health and undermined the ability to follow doctors' recommendations and discharge plans.
Discharge interventions that explicitly assess requirements for social support and connect patients with agencies or volunteer groups that call or visit those recuperating, provide meals on wheels, or offer other services such as light cleaning or shopping can address the complex circumstances that result in poor health and chronic rehospitalization. This study has identified the crucial role social support plays in getting and staying well.
Acknowledgements
The authors thank Maria Rizzo DePaoli MSW and Cornelia Walsh RN for assistance with logistics of the study.
- ,.Excess length of stay, charges, and mortality attributable to medical injuries during hospitalization.JAMA.2003;290:1868–1874.
- ,,,Institute of Medicine (U.S.).Committee on Quality of Health Care in America.To Err Is Human: Building a Safer Health System.Washington, DC:National Academy Press:2000.
- Centers for Disease Control and Prevention (National Center for Health Statistics).Births and deaths: preliminary data for 1998.Nat Vit Stat Rep.1999:47.
- Institute of Medicine (U.S.).Committee on Quality of Health Care in America.Crossing the Quality Chasm: a New Health System for the 21st Century.Washington, DC:National Academy Press;2001.
- AHRQ's Patient Safety Initiative: Building Foundations, Reducing Risk. Interim Report to the Senate Committee on Appropriations, AHRQ Publication No. 04‐RG005.Rockville, MD:Agency for Healthcare Research and Quality;2003. Available at: http://www.ahrq.gov/qual/pscongrpt/.
- ,,,,,.Patient safety at time of discharge—an example of a multifaceted process evaluation. In:Henriksen K,Battles JB,Marks ES,Lewin DI, editors. Advances in Patient Safety: from Research to Implementation. Vol.2,Concepts and methodology. AHRQ Publication No. 05‐0021‐2.Rockville, MD:Agency for Healthcare Research and Quality;2005.
- ,,.Dissemination of discharge summaries. Not reaching follow‐up physicians.Can Fam Physician.2002;48:737–742.
- ,,,,.The incidence and severity of adverse events affecting patients after discharge from the hospital.Ann Intern Med.2003;138(3):161–167.
- ,,, et al.Adverse events among medical patients after discharge from hospital.CMAJ.2004;170:345–349.
- ,,, et al.Adverse drug reactions as cause of admission to hospital: prospective analysis of 18 820 patients.BMJ.2004;329:15–19.
- and.Hospital readmissions in the Medicare population.N Engl J Med.1984;311:1349–1353.
- and.Factors predicting readmission of older general medicine patients.J Gen Intern Med.1991;6:389–393.
- ,,,.Delayed access to health care: risk factors, reasons and consequences.Ann Intern Med.1991;114:325–331.
- ,,,,,.Impact of socioeconomic status on hospital use in New York City.Health Aff (Millwood).1993 Spring;12(1):162–173.
- ,,.The impact of patient socioeconomic status and other social factors on readmission: a prospective study in four Massachusetts hospitals.Inquiry.1994;31(2):163–172.
- ,,,.Primary care physician attitudes regarding communication with hospitalists.Dis Mon.2002;48(4):218–229.
- ,,,,,.Patient safety at time of discharge: an example of a multifaceted process evaluation.Washington, DC:AHRQ Patient Safety 2 Volume Site;2004.
- ,.Entering the field of qualitative research. In:Denzin NK,Lincoln YS, eds.Handbook of Qualitative Research.Newbury Park, CA:Sage;1994.
- ,.The workers' compensation system: worker friend or foe?Am J Ind Med.2004;45:338–345.
- .Falling through the cracks: challenges and opportunities for improving transitional care for persons with continuous complex care needs.J Am Geriatr Soc.2003;51:549–555.
- ,,,,.Carepartner experiences with hospital care.Med Care.1999;37:33–38.
- ,,.Patients' and caregivers' transition from hospital to home. Needs and recommendations.Home Health Care Serv Q.1998;17:27–48.
- ,,, et al.Patients evaluate their hospital care: A national survey.Health Aff.1991;10:254.
- ,,.Defining social support in context: a necessary step in improving research, intervention, and practice.Qual Health Res.2004;14:942–960.
- .Telephone social support or nursing presence? Analysis of a nursing intervention.Qual Health Res.2005;15(1):19–29.
- ...Encountering the continuing challenges for women with chronic pain: recovery through recognition.Qual Health Res.2003;13:491–509.
- ,.Understanding coordination of care from the consumer's perspective in a regional health system.Health Serv Res.2002;37:1031–1054.
Institute of Medicine (IOM) reports1, 2 have estimated that between 44,000 and 98,000 patients die every year in hospitals because of iatrogenic errors of omission and commission. More people die in a year from medical errors than from car accidents (43,458), breast cancer (42,297), or AIDS (16,515).3 The IOM report recommended a goal of a 50% reduction in errors over the next 5 years.4 Since publication of these reports, a great deal of interest has been focused on how to make our hospitals safer.5, 6 Times of transitions in care (eg, from home to hospital, from emergency department to hospital, from the intensive care unit to the general ward) have been identified as opportune times to improve continuity and thus to decrease errors.
The hospital discharge process is often nonstandardized and frequently marked by poor quality.7 One in five hospital discharges is complicated by adverse events within 30 days, many of which lead to visits to emergency departments (EDs) and rehospitalization.810 Nationally, approximately 25% of hospitalized patients are readmitted within 90 days, often because of errors resulting from discontinuity and fragmentation of care at discharge, which exposes patients to iatrogenic risk and raises costs.11, 12 Low health literacy rates, lack of coordination in the handoff from the hospital to community care, gaps in social supports, and the absence of physician follow‐up after discharge place patients at high risk of rehospitalization.1315 Increasingly, as hospitalists provide more inpatient care, it is difficult for primary care physicians to be aware of all the complexities of a hospitalization.16
Studying the hospital discharge process provides an opportunity to learn more about its complexities,17 which could then be used to standardize the process and focus on those interventions that reduce the number of medical errors and resulting adverse events. However, to date, few studies have described the essential components of the discharge process, and no studies have focused on the discharge process from the point of view of the hospitalized patient. Therefore, a qualitative study was conducted in order to understand the phenomenon of frequent rehospitalization from the perspective of the discharged patient and to determine if activities at the time of discharge could be designed to reduce the number of adverse events and rehospitalizations.
METHODS
The larger study of which this work is a part examined the transition from inpatient service at a large inner‐city hospital to community care in order to lead to the development of an intervention to improve the discharge process. Qualitative research stresses the socially constructed nature of reality, and qualitative researchers seek to answer questions that stress how social experience is created and given meaning.18 Qualitative interviewing permits the researcher to understand the world as seen by the respondent within the context of the respondent's everyday life.19 Learning from the experiences of patients hospitalized more than once in a 6‐month period will help to identify their perceptions and beliefs about their disease and discharge instructions and assist additional interventions that could prevent rehospitalization.
Sample
Semistructured, open‐ended interviews were conducted with 21 patients during their hospital stay at Boston Medical Center. To be eligible for the study, a patient had to receive medical care through a health center affiliated with Boston Health Net, a network of community health centers serving primarily low‐income patients, and had to have been hospitalized on at least 1 additional occasion in the previous 6 months. Each day during the interview period the Boston Health Net nurse identified all patients previously admitted within 6 months and contacted the interviewer with the names and room numbers of those patients. The interviewer (M.S.) approached potential participants in their hospital rooms and obtained informed consent at the time of the interview. If the patient agreed, the interview was conducted at that time. If the patient was not available at that time, the interviewer made at least 2 attempts to visit the patient at a convenient time. The interviews were conducted on 17 days of a 4‐month period with no more than 2 interviews completed a day. The participants ranged in age from 18 to 79; 10 respondents were male, and 11 were female. All were English speaking. The mean age of the 20 patients who provided demographic information was 45.55 years, and the median age was 47 years. Nine of the participants reported their racial or ethnic identities as white (5 male, 3 female), 3 as black (2 male, 1 female), 4 as African American (1 male, 3 female); 1 as Latina; 1 as Hispanic (male), 1 as Spanish (male), and 1 as mixed (female). One male and 1 female participant provided no race or ethnic identity. Two participants were excluded from the study because they did not speak English, and 2 were excluded because they were unable to speak due to their medical conditions. Interviews were audiotaped, but full names were not used on the tape. Only subject code numbers were used to identify respondents. The discharge records of each participant were reviewed for consistency with that participant's descriptions of his or her condition. The study was approved by the Institutional Review Board of Boston University Medical Center.
Interview Guide
To help assure collection of comparable qualitative data, an interview guide listed specific questions and topics to be covered in a particular order in the interview. Questions were drawn in part from a pilot test of interviewing patients on the inpatient service rehospitalized within 90 days of the previous admission.17 Interviews assessed continuity of care after discharge, need for and availability of social support, and the participant's ability to obtain follow‐up medical care. The interview script consisted of open‐ended questions about events leading up to the current hospitalization, previous hospitalizations, instructions received the last time discharged, home situation, and ability to attend medical appointments, and participant feedback on the discharge process was requested. Follow‐up questions were asked based on a patient's responses to these questions. Interviews lasted between 20 and 45 minutes.
Analysis
The interview tapes were transcribed by a subcontracted transcriber, and the transcripts were checked for accuracy by the interviewer. Each interview was evaluated according to a set of thematic codes developed by 2 qualitative researchers (L.S. and M.S.). The codes represent categories or themes found in the data, and the appropriate codes were attached to their corresponding sections of text. To improve interrater reliability in coding, the 2 qualitative researchers coded 3 interviews, reviewed the codes, and, once it was clear that they both understood the coding scheme, coded the interviews. They resolved any problem cases and checked each other's work throughout the coding process to ensure that each interview was coded correctly. The findings were analyzed to explore whether there were linkages between and among particular themes. The discharge records of all patients were reviewed in order to compare the discharge notes about each patient's condition with that patient's own description of his or her condition and treatment.
RESULTS
All the patients who participated in this study were able to describe their medical condition and the reasons they were admitted to the hospital. Almost all, 20 of the 21 participants, were rehospitalized for the same primary diagnosis. For 5 of these 20 participants, length of time since the last hospitalization was 5‐6 months (4 for diabetes control, 1 for a lupus erythematosus flare); for 4 participants time since last hospitalization was between 6 weeks and 2 months (1 because of a fall, 1 because of seizures, 1 with hypertension, and 1 with SOB); for 8 participants time since last hospitalization was between 3 weeks and 1 month (2 with kidney disease, 2 with seizures, and 1 each with chronic obstructive pulmonary disease, sickle cell disease, PVD, and alcoholic gastritis), and for 3 participants time since last hospitalization was 1‐2 weeks (1 each with abdominal pain, alcohol intoxication, and lower gastrointestinal bleed). The principal diagnosis in a patient's discharge records matched that participant's description. Participants also described the discharge instructions they received. Although some did not report the brand names of the medications they were taking, all reports of the types of medications being taken or the conditions for which the medications were prescribed were consistent with discharge summaries. Although none of the participants incorrectly reported a medication or condition to the interviewer, a few did not provide information about every medication or condition. In 1 case the discharge summary noted medications for bipolar disorder and mental illness; in 2 cases medications were prescribed for depression. None of these participants mentioned these conditions or medications to the interviewer. One patient talked about stress and depression, but nothing was written about these issues in the discharge record.
For participants in this study, difficult life circumstances posed a greater barrier to recuperation than did lack of medical knowledge. The interviews conducted in this study illustrate the personal and social impact of disease that resulted in rehospitalization.
Discharge and Medical Knowledge
During discharge, transition care processes can fail at many points.20 These include: communication of the care plan, reconciliation of current and initial medication regimens, transportation of the patient, follow‐up care with a provider, and preparation of patient and caregiver for maintaining the patient's regimen.4, 2022 Participants in this study identified some of these and other factors as constituting barriers to effective care transitions.
At discharge, 7 participants were advised by physicians to change their diets or refrain from tobacco or alcohol use. Participants clearly understood the instructions and could give detailed accounts of diet changes they were supposed to make or explain the reasons tobacco or alcohol use caused or exacerbated their diseases. A diabetic whose discharge instructions included diet change listed sweet ones, starchy oneswith a lot of carbohydrates as foods she is not supposed to eat, wherease others described the links between alcohol use and adverse health: In my mind, I think that alcohol is a way out.But I know that it, that it's not.And so, the pancreatitis develops.
Lack of understanding about their medical condition or of knowledge about procedures to be followed was not evident in this population. Instead, recuperation was compromised by factors such as distress, substance use, support for medical and basic needs, and limitations in the availability of transportation to medical appointments. Many participants reported not receiving necessary rest as a result of needing to work or care for young children.
Crises and Coping: Distress
Despite understanding needed behavior changes, almost half the participants explained how difficult life circumstances and gaps in ongoing care or support made it impossible for them to follow medical advice.
Almost half the participants described themselves as being stressed, sad, or depressed. Their explanations indicate a relationship between distress and subsequent behaviors that exacerbated their conditions.
Of 3 self‐described alcoholics, one, a 52‐year‐old white man rehospitalized for alcohol related seizures, had relapsed after the deaths of his mother and his girlfriend. He explained, Well, after my girlfriend died, I really started to hit the bottle. Another, an unemployed 45‐year‐old black woman, lacked stable housing and at the time of the interview lived with a heavy drinker. She said that when I get stressed out, the first thing I want to do is go run to the [liquor] store. The third self‐described alcoholic, a 62‐year‐old white man, reported drinking because of lack of regular treatment for chronic depression:
My problem is has to do with stress and depression, which is what I'm gonna try to deal with this time. 'Cause that'scontributed to me getting so depressed I justjust started drinking again. I justnext time it'll kill me. So. That's almosta kind of a suicide wish, I guess.I know it's gonna kill me if I keep drinking.I think I need to get into something. Butthere'sI don't know if you call it substance abuse, butI think it's related todeep depression, which is not necessarily substance abuse, but it canI'm sure there's some relationship.
Similarly, the experiences of participants with diabetes illustrate clearly how depression contributed to undermining their ability to follow their doctors' recommendations. For example, an 18‐year‐old African American teenager rehospitalized for diabetes control discussed her inability to maintain her physician‐recommended diet:
Like when I'm stressed out.I get depressed and, umI give up. Just don't wanna do it anymore. It's not [that] I don't want to, I can't. I just can't do it I, when I got home, I actually did good! I actually really did good. I was eating salads. I did go on a diet. I ate salads, grilled food, and things like that. I took my medicine. I started loggin', like writin' everything down in a book. I wrote down what I ate every day, what my blood sugar was, and how much medicine I took. I was doin' good. But then I got depressed, and I stopped doin' it.
Continuity of Condition Management
Participants expressed a need after discharge for help at home, although in most cases, the help they reported needing did not require medical knowledge or technical skills.
Skilled Care
Few participants reported needing and/or receiving visiting nurse services; even in these cases, some of the responsibility for care fell to family members. Their health suffered because they lacked sufficient access to visiting nurse services or other needed support. A 42‐year‐old Latina diabetic with kidney infection described a visiting nurse's unsuccessful attempt to teach her husband how to change her catheter:
They try to show, 'cause before? I don't got the catheter, they're comin' in my house, in the morning? You know, put the catheter into my bladder, and they come back before me go to sleep, they try to show my husband how to do it, but he can't [CHUCKLES LIGHTLY], you know, he can't.So thethe doctor decide to leave the catheter there.
Basic Need Care
For most participants, the posthospital assistance needed did not require medical expertise. In the period after their last hospitalization, most participants needed assistance with daily chores such as cleaning, cooking, child care, and driving; they turned to friends and family members to meet these needs. However, because no family member was capable of providing full‐time care during recuperation, some participants were unable to follow advice from physicians about resting or refraining from certain activities. A 67‐year‐old African American man whose foot ulcers kept him from walking explained that during his recuperation he had to stay in the same place for 8 hours while his brother worked:
Oh, maybe if I had to go to the bathroom or something, I can'tbut for the most part, I guess I had things set upwhere I didn't, you know, where I didn't moveI just set my things up to keep me from movin' all day. I'd set my food up and everything else, little sandwich and all that. So, there wasn't anything aboutyou know, worrying about movin'or getting hungry, I guess.
None of the participants were able to pay for support services such as housecleaning or in‐home care, and all relied on busy friends and family members to meet their needs.
The experiences of 3 single mothers with health conditions characterized by debilitating chronic pain illustrate how very different access to supportive family members affected their ability to seek care and follow medical instructions as well as how child care responsibilities compromised their recuperation. One, a 20‐year‐old African American woman hospitalized for polycystic kidney disease, described situations during which the intensity of the pain did not permit her to do basic household chores. At those times she relied on her 5‐year‐old son:
Hehe actually knows how to sweep, he knows how to wash dishes. At 5 and a half, he surprised me, but [CHUCKLES] he can wash dishes, so. He has to get up on a chair, but he can wash 'em.
As a result of needing more care than was available, she traveled south to stay with her mother, who was unable to leave work to come to Boston:
I took the bus because my son has sickle cell trait, so they told me from day one it's not really good for him to fly on a plane? So, I had to take himit took like 20 hoursyou know, stoppin' here, stoppin' there, like, pullin' my bags and stuff, so it put me in more pain than I was in.
Another, a 24‐year‐old of mixed background chronically hospitalized with sickle cell pain crises, delayed medical treatment because of lack of child care:
There's been times that I have had to wait till I could find somebody to watch my kids, to even come to the hospital.There's been times thatuh, it'd be a while before I could get anybody, so instead of me coming to the hospital, I have to wait at home, in a lot of pain.I would have to waitany time between 5 hours to 2 days before I could find somebody to watch my kids.
This pattern of child care interfering with recovery continued after leaving the hospital:
The minute I get home it'd be nice to have somebody to watch the kids, so I could at least recuperate for like 24 hours before I have to take care of thingsI would have to usually just go home and just get right to it.
The experience of a third, a 29‐year‐old African American woman with systemic lupus erythematosus, illustrates the ways in which family support can ease the burden of illness. This participant relocated to be close to her mother, aunt, and cousins, all of whom cared for her children when she is in the hospital:
When I was in [NEIGHBORING STATE] it was terrible'cause my, my kids wasn't goin' to school, 'cause I couldn't get up to get them dressed and wake them up. My daughter almost got kept back and stuff. It was real hardand it wasn't good, you know, that they could justrun through the house rampant, do whatever they want and not be supervised.So that was very dangerous, too. And then, it put like, it put a strain on my oldest, my daughter
She contrasted this with her current situation in which family members cared for her children when she is in the hospital or sick at home:
Like, this morningthey took the kids to school for me and everything. Made 'em breakfast, made sure they was dressed right this morningMy mother picked them up from school this afternoon.
Transportation to Appointments
Travel to follow‐up appointments was difficult for many participants. Almost half reported taking public transportation to appointments; the others either drove themselves, were driven by relatives or friends, or paid for taxis. Those relying on public transportation were more likely than others to miss appointments because of transportation issues if they did not feel well:
Depending how I feel. If I feel all right, I'll take the bus; if not, I'll get a taxi or I'll just won't show up. I would borrow a bus pass or somethin', you know, from [HIS NAME] is Joebecause I would make, like, evening appointments. Um, because my sickle cell tends to act up if it's coldSo, if it's really cold, I don't go.
As one 55‐year‐old white woman who has seizures summed up the matter of traveling by bus when not feeling well, You do what you have to do!
DISCUSSION AND CONCLUSIONS
The hospital discharge process has been identified as a time when sources of error occur that result in rehospitalization. Many factors that adversely affect care transitions apply to the hospital discharge process, including preparation of the patient and caregiver, communication of the care plan, changes in the medication regimen, transportation of the patient, scheduling of follow‐up care, and availability of advance care directives.20 Patients with low socioeconomic status have been found to be especially vulnerable after discharge. A 1989 telephone survey of 6455 patients recently discharged from hospitals in the United States found that low socioeconomic status and poor patient health were independent predictors of patient problems after discharge.21 A nationwide telephone survey of 1800 recently discharged patients and their care partners also revealed that low socioeconomic status and poor patient health status were associated with problems experienced by care partners.22
High rates of unnecessary rehospitalization have been shown to be related to poorly managed discharge processes.23 Although some factors identified in other studies of care transition did influence the rehospitalization of participants in this study; others did not. Transportation and follow‐up care greatly affected rehospitalization, whereas health literacy had a minimal effect. Fifteen of 20 participants were readmitted within weeks up to 2 months for the same primary diagnosis, yet they understood their medical conditions and knew the procedures to be followed. Having a chronic illness may have affected their understanding of their disease because they had received teaching over time. However, for most participants in this studyinner‐city, minority, low‐income patientsfactors beyond the discharge process affected their rehospitalization. Difficult life circumstances and gaps in ongoing care or support resulted in distress and behavior that exacerbated their conditions. Participants lacked social and emotional support that would have enabled them to prioritize maintaining their health.
Although there is not a universally accepted definition of the concept of social support, it is generally understood that it involves emotional connection and caring24 and occurs in a relationship in which the person providing the support is equipped to respond to a wide variety of needs ranging from practical assistance to counseling and encouragement based on the concerns or life circumstances of the patient. Qualitative studies of social support interventions demonstrate the ways in which having a dependable person to whom a patient can turn for encouragement, information, and practical assistance improves the patient's ability to maintain health regimens and manage chronic pain. An intervention in which nurses made weekly telephone contact with low‐income pregnant smokers helped these patients manage numerous stressors and, in some cases, reduce their tobacco use.25 A support group for women with chronic pain helped participants learn practical strategies for reducing pain and reduced isolation and emotional distress about their conditions.26 A study of consumer experiences of transition care27 found that the most valued institutions were those in which providers from one facility thoroughly communicated a patient's medical and treatment history to providers in another; also important was involving the consumer in medical decision making, preparing the consumer to actively participate in his or her own care, and attending to individual needs and preferences.
This study had several limitations, including reliance on participants' reports of their conditions and experiences with medical staff at a time when they were rehospitalized. In the vulnerable position of being hospitalized, participants may have been reluctant to have complaints about their hospital experiences tape‐recorded. All participants reported positive experiences with hospital staff during the formal interview. Two participants reported negative experiences with hospital staff after the audio‐recorder was turned off and the interview concluded. Other limitations of the hospital setting include limited privacy. Either a roommate was present during the interview or the interview was interrupted by a visit from a hospital staff person or a telephone call. Participants were asked to recall events that for some had occurred several months before the interview, introducing the possibility of inaccurate recall. To address these limitations, we compared interview transcripts to discharge summaries in order to assess any inconsistencies that may have resulted from this lack of privacy. The differences between summaries and patient self‐reports were that 2 participants did not report illicit substance use and 2 did not report psychiatric conditions. Despite these limitations, conducting this study in a hospital setting allowed investigators access to a highly vulnerable population that would be most affected by improvements in the discharge process. Given the difficulties many participants reported in getting to appointments, it is unlikely that a study conducted outside the hospital setting would have effectively reached this population.
These results support the findings in this study that life circumstances outside the hospital can be as important to recovery as institutional coordination of medical care. Although the stresses described by the low‐income patients in this study may not directly cause subsequent illness, their experiences clearly demonstrate the ways in which stresses make it difficult or impossible to attain sufficient rest to heal, maintain the behavioral change necessary to improve health, and follow instructions given by clinicians at the time of discharge. Interventions targeting low‐income patients thus are more likely to succeed if they include provisions for social support and assist patients in easing the burden of daily responsibilities. Effective transition care includes support that may not be explicitly medical, but without which participants lack the stability to fully recuperate. Without the possibility of taking a break from household or parenting responsibilities, it is difficult to rest enough to truly recover. The descriptions of extreme measures taken in order to obtain needed support illustrate how recuperation was compromised by both family responsibilities and lack of flexibility in caregiver work schedules. Distress, particularly depression, further contributed to poor health and undermined the ability to follow doctors' recommendations and discharge plans.
Discharge interventions that explicitly assess requirements for social support and connect patients with agencies or volunteer groups that call or visit those recuperating, provide meals on wheels, or offer other services such as light cleaning or shopping can address the complex circumstances that result in poor health and chronic rehospitalization. This study has identified the crucial role social support plays in getting and staying well.
Acknowledgements
The authors thank Maria Rizzo DePaoli MSW and Cornelia Walsh RN for assistance with logistics of the study.
Institute of Medicine (IOM) reports1, 2 have estimated that between 44,000 and 98,000 patients die every year in hospitals because of iatrogenic errors of omission and commission. More people die in a year from medical errors than from car accidents (43,458), breast cancer (42,297), or AIDS (16,515).3 The IOM report recommended a goal of a 50% reduction in errors over the next 5 years.4 Since publication of these reports, a great deal of interest has been focused on how to make our hospitals safer.5, 6 Times of transitions in care (eg, from home to hospital, from emergency department to hospital, from the intensive care unit to the general ward) have been identified as opportune times to improve continuity and thus to decrease errors.
The hospital discharge process is often nonstandardized and frequently marked by poor quality.7 One in five hospital discharges is complicated by adverse events within 30 days, many of which lead to visits to emergency departments (EDs) and rehospitalization.810 Nationally, approximately 25% of hospitalized patients are readmitted within 90 days, often because of errors resulting from discontinuity and fragmentation of care at discharge, which exposes patients to iatrogenic risk and raises costs.11, 12 Low health literacy rates, lack of coordination in the handoff from the hospital to community care, gaps in social supports, and the absence of physician follow‐up after discharge place patients at high risk of rehospitalization.1315 Increasingly, as hospitalists provide more inpatient care, it is difficult for primary care physicians to be aware of all the complexities of a hospitalization.16
Studying the hospital discharge process provides an opportunity to learn more about its complexities,17 which could then be used to standardize the process and focus on those interventions that reduce the number of medical errors and resulting adverse events. However, to date, few studies have described the essential components of the discharge process, and no studies have focused on the discharge process from the point of view of the hospitalized patient. Therefore, a qualitative study was conducted in order to understand the phenomenon of frequent rehospitalization from the perspective of the discharged patient and to determine if activities at the time of discharge could be designed to reduce the number of adverse events and rehospitalizations.
METHODS
The larger study of which this work is a part examined the transition from inpatient service at a large inner‐city hospital to community care in order to lead to the development of an intervention to improve the discharge process. Qualitative research stresses the socially constructed nature of reality, and qualitative researchers seek to answer questions that stress how social experience is created and given meaning.18 Qualitative interviewing permits the researcher to understand the world as seen by the respondent within the context of the respondent's everyday life.19 Learning from the experiences of patients hospitalized more than once in a 6‐month period will help to identify their perceptions and beliefs about their disease and discharge instructions and assist additional interventions that could prevent rehospitalization.
Sample
Semistructured, open‐ended interviews were conducted with 21 patients during their hospital stay at Boston Medical Center. To be eligible for the study, a patient had to receive medical care through a health center affiliated with Boston Health Net, a network of community health centers serving primarily low‐income patients, and had to have been hospitalized on at least 1 additional occasion in the previous 6 months. Each day during the interview period the Boston Health Net nurse identified all patients previously admitted within 6 months and contacted the interviewer with the names and room numbers of those patients. The interviewer (M.S.) approached potential participants in their hospital rooms and obtained informed consent at the time of the interview. If the patient agreed, the interview was conducted at that time. If the patient was not available at that time, the interviewer made at least 2 attempts to visit the patient at a convenient time. The interviews were conducted on 17 days of a 4‐month period with no more than 2 interviews completed a day. The participants ranged in age from 18 to 79; 10 respondents were male, and 11 were female. All were English speaking. The mean age of the 20 patients who provided demographic information was 45.55 years, and the median age was 47 years. Nine of the participants reported their racial or ethnic identities as white (5 male, 3 female), 3 as black (2 male, 1 female), 4 as African American (1 male, 3 female); 1 as Latina; 1 as Hispanic (male), 1 as Spanish (male), and 1 as mixed (female). One male and 1 female participant provided no race or ethnic identity. Two participants were excluded from the study because they did not speak English, and 2 were excluded because they were unable to speak due to their medical conditions. Interviews were audiotaped, but full names were not used on the tape. Only subject code numbers were used to identify respondents. The discharge records of each participant were reviewed for consistency with that participant's descriptions of his or her condition. The study was approved by the Institutional Review Board of Boston University Medical Center.
Interview Guide
To help assure collection of comparable qualitative data, an interview guide listed specific questions and topics to be covered in a particular order in the interview. Questions were drawn in part from a pilot test of interviewing patients on the inpatient service rehospitalized within 90 days of the previous admission.17 Interviews assessed continuity of care after discharge, need for and availability of social support, and the participant's ability to obtain follow‐up medical care. The interview script consisted of open‐ended questions about events leading up to the current hospitalization, previous hospitalizations, instructions received the last time discharged, home situation, and ability to attend medical appointments, and participant feedback on the discharge process was requested. Follow‐up questions were asked based on a patient's responses to these questions. Interviews lasted between 20 and 45 minutes.
Analysis
The interview tapes were transcribed by a subcontracted transcriber, and the transcripts were checked for accuracy by the interviewer. Each interview was evaluated according to a set of thematic codes developed by 2 qualitative researchers (L.S. and M.S.). The codes represent categories or themes found in the data, and the appropriate codes were attached to their corresponding sections of text. To improve interrater reliability in coding, the 2 qualitative researchers coded 3 interviews, reviewed the codes, and, once it was clear that they both understood the coding scheme, coded the interviews. They resolved any problem cases and checked each other's work throughout the coding process to ensure that each interview was coded correctly. The findings were analyzed to explore whether there were linkages between and among particular themes. The discharge records of all patients were reviewed in order to compare the discharge notes about each patient's condition with that patient's own description of his or her condition and treatment.
RESULTS
All the patients who participated in this study were able to describe their medical condition and the reasons they were admitted to the hospital. Almost all, 20 of the 21 participants, were rehospitalized for the same primary diagnosis. For 5 of these 20 participants, length of time since the last hospitalization was 5‐6 months (4 for diabetes control, 1 for a lupus erythematosus flare); for 4 participants time since last hospitalization was between 6 weeks and 2 months (1 because of a fall, 1 because of seizures, 1 with hypertension, and 1 with SOB); for 8 participants time since last hospitalization was between 3 weeks and 1 month (2 with kidney disease, 2 with seizures, and 1 each with chronic obstructive pulmonary disease, sickle cell disease, PVD, and alcoholic gastritis), and for 3 participants time since last hospitalization was 1‐2 weeks (1 each with abdominal pain, alcohol intoxication, and lower gastrointestinal bleed). The principal diagnosis in a patient's discharge records matched that participant's description. Participants also described the discharge instructions they received. Although some did not report the brand names of the medications they were taking, all reports of the types of medications being taken or the conditions for which the medications were prescribed were consistent with discharge summaries. Although none of the participants incorrectly reported a medication or condition to the interviewer, a few did not provide information about every medication or condition. In 1 case the discharge summary noted medications for bipolar disorder and mental illness; in 2 cases medications were prescribed for depression. None of these participants mentioned these conditions or medications to the interviewer. One patient talked about stress and depression, but nothing was written about these issues in the discharge record.
For participants in this study, difficult life circumstances posed a greater barrier to recuperation than did lack of medical knowledge. The interviews conducted in this study illustrate the personal and social impact of disease that resulted in rehospitalization.
Discharge and Medical Knowledge
During discharge, transition care processes can fail at many points.20 These include: communication of the care plan, reconciliation of current and initial medication regimens, transportation of the patient, follow‐up care with a provider, and preparation of patient and caregiver for maintaining the patient's regimen.4, 2022 Participants in this study identified some of these and other factors as constituting barriers to effective care transitions.
At discharge, 7 participants were advised by physicians to change their diets or refrain from tobacco or alcohol use. Participants clearly understood the instructions and could give detailed accounts of diet changes they were supposed to make or explain the reasons tobacco or alcohol use caused or exacerbated their diseases. A diabetic whose discharge instructions included diet change listed sweet ones, starchy oneswith a lot of carbohydrates as foods she is not supposed to eat, wherease others described the links between alcohol use and adverse health: In my mind, I think that alcohol is a way out.But I know that it, that it's not.And so, the pancreatitis develops.
Lack of understanding about their medical condition or of knowledge about procedures to be followed was not evident in this population. Instead, recuperation was compromised by factors such as distress, substance use, support for medical and basic needs, and limitations in the availability of transportation to medical appointments. Many participants reported not receiving necessary rest as a result of needing to work or care for young children.
Crises and Coping: Distress
Despite understanding needed behavior changes, almost half the participants explained how difficult life circumstances and gaps in ongoing care or support made it impossible for them to follow medical advice.
Almost half the participants described themselves as being stressed, sad, or depressed. Their explanations indicate a relationship between distress and subsequent behaviors that exacerbated their conditions.
Of 3 self‐described alcoholics, one, a 52‐year‐old white man rehospitalized for alcohol related seizures, had relapsed after the deaths of his mother and his girlfriend. He explained, Well, after my girlfriend died, I really started to hit the bottle. Another, an unemployed 45‐year‐old black woman, lacked stable housing and at the time of the interview lived with a heavy drinker. She said that when I get stressed out, the first thing I want to do is go run to the [liquor] store. The third self‐described alcoholic, a 62‐year‐old white man, reported drinking because of lack of regular treatment for chronic depression:
My problem is has to do with stress and depression, which is what I'm gonna try to deal with this time. 'Cause that'scontributed to me getting so depressed I justjust started drinking again. I justnext time it'll kill me. So. That's almosta kind of a suicide wish, I guess.I know it's gonna kill me if I keep drinking.I think I need to get into something. Butthere'sI don't know if you call it substance abuse, butI think it's related todeep depression, which is not necessarily substance abuse, but it canI'm sure there's some relationship.
Similarly, the experiences of participants with diabetes illustrate clearly how depression contributed to undermining their ability to follow their doctors' recommendations. For example, an 18‐year‐old African American teenager rehospitalized for diabetes control discussed her inability to maintain her physician‐recommended diet:
Like when I'm stressed out.I get depressed and, umI give up. Just don't wanna do it anymore. It's not [that] I don't want to, I can't. I just can't do it I, when I got home, I actually did good! I actually really did good. I was eating salads. I did go on a diet. I ate salads, grilled food, and things like that. I took my medicine. I started loggin', like writin' everything down in a book. I wrote down what I ate every day, what my blood sugar was, and how much medicine I took. I was doin' good. But then I got depressed, and I stopped doin' it.
Continuity of Condition Management
Participants expressed a need after discharge for help at home, although in most cases, the help they reported needing did not require medical knowledge or technical skills.
Skilled Care
Few participants reported needing and/or receiving visiting nurse services; even in these cases, some of the responsibility for care fell to family members. Their health suffered because they lacked sufficient access to visiting nurse services or other needed support. A 42‐year‐old Latina diabetic with kidney infection described a visiting nurse's unsuccessful attempt to teach her husband how to change her catheter:
They try to show, 'cause before? I don't got the catheter, they're comin' in my house, in the morning? You know, put the catheter into my bladder, and they come back before me go to sleep, they try to show my husband how to do it, but he can't [CHUCKLES LIGHTLY], you know, he can't.So thethe doctor decide to leave the catheter there.
Basic Need Care
For most participants, the posthospital assistance needed did not require medical expertise. In the period after their last hospitalization, most participants needed assistance with daily chores such as cleaning, cooking, child care, and driving; they turned to friends and family members to meet these needs. However, because no family member was capable of providing full‐time care during recuperation, some participants were unable to follow advice from physicians about resting or refraining from certain activities. A 67‐year‐old African American man whose foot ulcers kept him from walking explained that during his recuperation he had to stay in the same place for 8 hours while his brother worked:
Oh, maybe if I had to go to the bathroom or something, I can'tbut for the most part, I guess I had things set upwhere I didn't, you know, where I didn't moveI just set my things up to keep me from movin' all day. I'd set my food up and everything else, little sandwich and all that. So, there wasn't anything aboutyou know, worrying about movin'or getting hungry, I guess.
None of the participants were able to pay for support services such as housecleaning or in‐home care, and all relied on busy friends and family members to meet their needs.
The experiences of 3 single mothers with health conditions characterized by debilitating chronic pain illustrate how very different access to supportive family members affected their ability to seek care and follow medical instructions as well as how child care responsibilities compromised their recuperation. One, a 20‐year‐old African American woman hospitalized for polycystic kidney disease, described situations during which the intensity of the pain did not permit her to do basic household chores. At those times she relied on her 5‐year‐old son:
Hehe actually knows how to sweep, he knows how to wash dishes. At 5 and a half, he surprised me, but [CHUCKLES] he can wash dishes, so. He has to get up on a chair, but he can wash 'em.
As a result of needing more care than was available, she traveled south to stay with her mother, who was unable to leave work to come to Boston:
I took the bus because my son has sickle cell trait, so they told me from day one it's not really good for him to fly on a plane? So, I had to take himit took like 20 hoursyou know, stoppin' here, stoppin' there, like, pullin' my bags and stuff, so it put me in more pain than I was in.
Another, a 24‐year‐old of mixed background chronically hospitalized with sickle cell pain crises, delayed medical treatment because of lack of child care:
There's been times that I have had to wait till I could find somebody to watch my kids, to even come to the hospital.There's been times thatuh, it'd be a while before I could get anybody, so instead of me coming to the hospital, I have to wait at home, in a lot of pain.I would have to waitany time between 5 hours to 2 days before I could find somebody to watch my kids.
This pattern of child care interfering with recovery continued after leaving the hospital:
The minute I get home it'd be nice to have somebody to watch the kids, so I could at least recuperate for like 24 hours before I have to take care of thingsI would have to usually just go home and just get right to it.
The experience of a third, a 29‐year‐old African American woman with systemic lupus erythematosus, illustrates the ways in which family support can ease the burden of illness. This participant relocated to be close to her mother, aunt, and cousins, all of whom cared for her children when she is in the hospital:
When I was in [NEIGHBORING STATE] it was terrible'cause my, my kids wasn't goin' to school, 'cause I couldn't get up to get them dressed and wake them up. My daughter almost got kept back and stuff. It was real hardand it wasn't good, you know, that they could justrun through the house rampant, do whatever they want and not be supervised.So that was very dangerous, too. And then, it put like, it put a strain on my oldest, my daughter
She contrasted this with her current situation in which family members cared for her children when she is in the hospital or sick at home:
Like, this morningthey took the kids to school for me and everything. Made 'em breakfast, made sure they was dressed right this morningMy mother picked them up from school this afternoon.
Transportation to Appointments
Travel to follow‐up appointments was difficult for many participants. Almost half reported taking public transportation to appointments; the others either drove themselves, were driven by relatives or friends, or paid for taxis. Those relying on public transportation were more likely than others to miss appointments because of transportation issues if they did not feel well:
Depending how I feel. If I feel all right, I'll take the bus; if not, I'll get a taxi or I'll just won't show up. I would borrow a bus pass or somethin', you know, from [HIS NAME] is Joebecause I would make, like, evening appointments. Um, because my sickle cell tends to act up if it's coldSo, if it's really cold, I don't go.
As one 55‐year‐old white woman who has seizures summed up the matter of traveling by bus when not feeling well, You do what you have to do!
DISCUSSION AND CONCLUSIONS
The hospital discharge process has been identified as a time when sources of error occur that result in rehospitalization. Many factors that adversely affect care transitions apply to the hospital discharge process, including preparation of the patient and caregiver, communication of the care plan, changes in the medication regimen, transportation of the patient, scheduling of follow‐up care, and availability of advance care directives.20 Patients with low socioeconomic status have been found to be especially vulnerable after discharge. A 1989 telephone survey of 6455 patients recently discharged from hospitals in the United States found that low socioeconomic status and poor patient health were independent predictors of patient problems after discharge.21 A nationwide telephone survey of 1800 recently discharged patients and their care partners also revealed that low socioeconomic status and poor patient health status were associated with problems experienced by care partners.22
High rates of unnecessary rehospitalization have been shown to be related to poorly managed discharge processes.23 Although some factors identified in other studies of care transition did influence the rehospitalization of participants in this study; others did not. Transportation and follow‐up care greatly affected rehospitalization, whereas health literacy had a minimal effect. Fifteen of 20 participants were readmitted within weeks up to 2 months for the same primary diagnosis, yet they understood their medical conditions and knew the procedures to be followed. Having a chronic illness may have affected their understanding of their disease because they had received teaching over time. However, for most participants in this studyinner‐city, minority, low‐income patientsfactors beyond the discharge process affected their rehospitalization. Difficult life circumstances and gaps in ongoing care or support resulted in distress and behavior that exacerbated their conditions. Participants lacked social and emotional support that would have enabled them to prioritize maintaining their health.
Although there is not a universally accepted definition of the concept of social support, it is generally understood that it involves emotional connection and caring24 and occurs in a relationship in which the person providing the support is equipped to respond to a wide variety of needs ranging from practical assistance to counseling and encouragement based on the concerns or life circumstances of the patient. Qualitative studies of social support interventions demonstrate the ways in which having a dependable person to whom a patient can turn for encouragement, information, and practical assistance improves the patient's ability to maintain health regimens and manage chronic pain. An intervention in which nurses made weekly telephone contact with low‐income pregnant smokers helped these patients manage numerous stressors and, in some cases, reduce their tobacco use.25 A support group for women with chronic pain helped participants learn practical strategies for reducing pain and reduced isolation and emotional distress about their conditions.26 A study of consumer experiences of transition care27 found that the most valued institutions were those in which providers from one facility thoroughly communicated a patient's medical and treatment history to providers in another; also important was involving the consumer in medical decision making, preparing the consumer to actively participate in his or her own care, and attending to individual needs and preferences.
This study had several limitations, including reliance on participants' reports of their conditions and experiences with medical staff at a time when they were rehospitalized. In the vulnerable position of being hospitalized, participants may have been reluctant to have complaints about their hospital experiences tape‐recorded. All participants reported positive experiences with hospital staff during the formal interview. Two participants reported negative experiences with hospital staff after the audio‐recorder was turned off and the interview concluded. Other limitations of the hospital setting include limited privacy. Either a roommate was present during the interview or the interview was interrupted by a visit from a hospital staff person or a telephone call. Participants were asked to recall events that for some had occurred several months before the interview, introducing the possibility of inaccurate recall. To address these limitations, we compared interview transcripts to discharge summaries in order to assess any inconsistencies that may have resulted from this lack of privacy. The differences between summaries and patient self‐reports were that 2 participants did not report illicit substance use and 2 did not report psychiatric conditions. Despite these limitations, conducting this study in a hospital setting allowed investigators access to a highly vulnerable population that would be most affected by improvements in the discharge process. Given the difficulties many participants reported in getting to appointments, it is unlikely that a study conducted outside the hospital setting would have effectively reached this population.
These results support the findings in this study that life circumstances outside the hospital can be as important to recovery as institutional coordination of medical care. Although the stresses described by the low‐income patients in this study may not directly cause subsequent illness, their experiences clearly demonstrate the ways in which stresses make it difficult or impossible to attain sufficient rest to heal, maintain the behavioral change necessary to improve health, and follow instructions given by clinicians at the time of discharge. Interventions targeting low‐income patients thus are more likely to succeed if they include provisions for social support and assist patients in easing the burden of daily responsibilities. Effective transition care includes support that may not be explicitly medical, but without which participants lack the stability to fully recuperate. Without the possibility of taking a break from household or parenting responsibilities, it is difficult to rest enough to truly recover. The descriptions of extreme measures taken in order to obtain needed support illustrate how recuperation was compromised by both family responsibilities and lack of flexibility in caregiver work schedules. Distress, particularly depression, further contributed to poor health and undermined the ability to follow doctors' recommendations and discharge plans.
Discharge interventions that explicitly assess requirements for social support and connect patients with agencies or volunteer groups that call or visit those recuperating, provide meals on wheels, or offer other services such as light cleaning or shopping can address the complex circumstances that result in poor health and chronic rehospitalization. This study has identified the crucial role social support plays in getting and staying well.
Acknowledgements
The authors thank Maria Rizzo DePaoli MSW and Cornelia Walsh RN for assistance with logistics of the study.
- ,.Excess length of stay, charges, and mortality attributable to medical injuries during hospitalization.JAMA.2003;290:1868–1874.
- ,,,Institute of Medicine (U.S.).Committee on Quality of Health Care in America.To Err Is Human: Building a Safer Health System.Washington, DC:National Academy Press:2000.
- Centers for Disease Control and Prevention (National Center for Health Statistics).Births and deaths: preliminary data for 1998.Nat Vit Stat Rep.1999:47.
- Institute of Medicine (U.S.).Committee on Quality of Health Care in America.Crossing the Quality Chasm: a New Health System for the 21st Century.Washington, DC:National Academy Press;2001.
- AHRQ's Patient Safety Initiative: Building Foundations, Reducing Risk. Interim Report to the Senate Committee on Appropriations, AHRQ Publication No. 04‐RG005.Rockville, MD:Agency for Healthcare Research and Quality;2003. Available at: http://www.ahrq.gov/qual/pscongrpt/.
- ,,,,,.Patient safety at time of discharge—an example of a multifaceted process evaluation. In:Henriksen K,Battles JB,Marks ES,Lewin DI, editors. Advances in Patient Safety: from Research to Implementation. Vol.2,Concepts and methodology. AHRQ Publication No. 05‐0021‐2.Rockville, MD:Agency for Healthcare Research and Quality;2005.
- ,,.Dissemination of discharge summaries. Not reaching follow‐up physicians.Can Fam Physician.2002;48:737–742.
- ,,,,.The incidence and severity of adverse events affecting patients after discharge from the hospital.Ann Intern Med.2003;138(3):161–167.
- ,,, et al.Adverse events among medical patients after discharge from hospital.CMAJ.2004;170:345–349.
- ,,, et al.Adverse drug reactions as cause of admission to hospital: prospective analysis of 18 820 patients.BMJ.2004;329:15–19.
- and.Hospital readmissions in the Medicare population.N Engl J Med.1984;311:1349–1353.
- and.Factors predicting readmission of older general medicine patients.J Gen Intern Med.1991;6:389–393.
- ,,,.Delayed access to health care: risk factors, reasons and consequences.Ann Intern Med.1991;114:325–331.
- ,,,,,.Impact of socioeconomic status on hospital use in New York City.Health Aff (Millwood).1993 Spring;12(1):162–173.
- ,,.The impact of patient socioeconomic status and other social factors on readmission: a prospective study in four Massachusetts hospitals.Inquiry.1994;31(2):163–172.
- ,,,.Primary care physician attitudes regarding communication with hospitalists.Dis Mon.2002;48(4):218–229.
- ,,,,,.Patient safety at time of discharge: an example of a multifaceted process evaluation.Washington, DC:AHRQ Patient Safety 2 Volume Site;2004.
- ,.Entering the field of qualitative research. In:Denzin NK,Lincoln YS, eds.Handbook of Qualitative Research.Newbury Park, CA:Sage;1994.
- ,.The workers' compensation system: worker friend or foe?Am J Ind Med.2004;45:338–345.
- .Falling through the cracks: challenges and opportunities for improving transitional care for persons with continuous complex care needs.J Am Geriatr Soc.2003;51:549–555.
- ,,,,.Carepartner experiences with hospital care.Med Care.1999;37:33–38.
- ,,.Patients' and caregivers' transition from hospital to home. Needs and recommendations.Home Health Care Serv Q.1998;17:27–48.
- ,,, et al.Patients evaluate their hospital care: A national survey.Health Aff.1991;10:254.
- ,,.Defining social support in context: a necessary step in improving research, intervention, and practice.Qual Health Res.2004;14:942–960.
- .Telephone social support or nursing presence? Analysis of a nursing intervention.Qual Health Res.2005;15(1):19–29.
- ...Encountering the continuing challenges for women with chronic pain: recovery through recognition.Qual Health Res.2003;13:491–509.
- ,.Understanding coordination of care from the consumer's perspective in a regional health system.Health Serv Res.2002;37:1031–1054.
- ,.Excess length of stay, charges, and mortality attributable to medical injuries during hospitalization.JAMA.2003;290:1868–1874.
- ,,,Institute of Medicine (U.S.).Committee on Quality of Health Care in America.To Err Is Human: Building a Safer Health System.Washington, DC:National Academy Press:2000.
- Centers for Disease Control and Prevention (National Center for Health Statistics).Births and deaths: preliminary data for 1998.Nat Vit Stat Rep.1999:47.
- Institute of Medicine (U.S.).Committee on Quality of Health Care in America.Crossing the Quality Chasm: a New Health System for the 21st Century.Washington, DC:National Academy Press;2001.
- AHRQ's Patient Safety Initiative: Building Foundations, Reducing Risk. Interim Report to the Senate Committee on Appropriations, AHRQ Publication No. 04‐RG005.Rockville, MD:Agency for Healthcare Research and Quality;2003. Available at: http://www.ahrq.gov/qual/pscongrpt/.
- ,,,,,.Patient safety at time of discharge—an example of a multifaceted process evaluation. In:Henriksen K,Battles JB,Marks ES,Lewin DI, editors. Advances in Patient Safety: from Research to Implementation. Vol.2,Concepts and methodology. AHRQ Publication No. 05‐0021‐2.Rockville, MD:Agency for Healthcare Research and Quality;2005.
- ,,.Dissemination of discharge summaries. Not reaching follow‐up physicians.Can Fam Physician.2002;48:737–742.
- ,,,,.The incidence and severity of adverse events affecting patients after discharge from the hospital.Ann Intern Med.2003;138(3):161–167.
- ,,, et al.Adverse events among medical patients after discharge from hospital.CMAJ.2004;170:345–349.
- ,,, et al.Adverse drug reactions as cause of admission to hospital: prospective analysis of 18 820 patients.BMJ.2004;329:15–19.
- and.Hospital readmissions in the Medicare population.N Engl J Med.1984;311:1349–1353.
- and.Factors predicting readmission of older general medicine patients.J Gen Intern Med.1991;6:389–393.
- ,,,.Delayed access to health care: risk factors, reasons and consequences.Ann Intern Med.1991;114:325–331.
- ,,,,,.Impact of socioeconomic status on hospital use in New York City.Health Aff (Millwood).1993 Spring;12(1):162–173.
- ,,.The impact of patient socioeconomic status and other social factors on readmission: a prospective study in four Massachusetts hospitals.Inquiry.1994;31(2):163–172.
- ,,,.Primary care physician attitudes regarding communication with hospitalists.Dis Mon.2002;48(4):218–229.
- ,,,,,.Patient safety at time of discharge: an example of a multifaceted process evaluation.Washington, DC:AHRQ Patient Safety 2 Volume Site;2004.
- ,.Entering the field of qualitative research. In:Denzin NK,Lincoln YS, eds.Handbook of Qualitative Research.Newbury Park, CA:Sage;1994.
- ,.The workers' compensation system: worker friend or foe?Am J Ind Med.2004;45:338–345.
- .Falling through the cracks: challenges and opportunities for improving transitional care for persons with continuous complex care needs.J Am Geriatr Soc.2003;51:549–555.
- ,,,,.Carepartner experiences with hospital care.Med Care.1999;37:33–38.
- ,,.Patients' and caregivers' transition from hospital to home. Needs and recommendations.Home Health Care Serv Q.1998;17:27–48.
- ,,, et al.Patients evaluate their hospital care: A national survey.Health Aff.1991;10:254.
- ,,.Defining social support in context: a necessary step in improving research, intervention, and practice.Qual Health Res.2004;14:942–960.
- .Telephone social support or nursing presence? Analysis of a nursing intervention.Qual Health Res.2005;15(1):19–29.
- ...Encountering the continuing challenges for women with chronic pain: recovery through recognition.Qual Health Res.2003;13:491–509.
- ,.Understanding coordination of care from the consumer's perspective in a regional health system.Health Serv Res.2002;37:1031–1054.
Copyright © 2007 Society of Hospital Medicine
Transitions of Care at Hospital Discharge
As the counterpart to hospital admission, hospital discharge is a necessary process experienced by each living patient. For all patients except those being transferred to a continuing care facility, discharge is a period of transition from hospital to home that involves a transfer in responsibility from the inpatient provider or hospitalist to the patient and primary care physician (PCP).1 Prescription medications are commonly altered at this transition point, with patients asked to discontinue some medications, switch to a new dosage schedule of others, or begin new treatments.2, 3 Self‐care responsibilities also increase in number and importance, presenting new challenges for patients and their families as they return home.4 Under these circumstances, ineffective planning and coordination of care can undermine patient satisfaction, facilitate adverse events, and contribute to more frequent hospital readmissions.58
Following hospital discharge nearly half (49%) of hospitalized patients experience at least 1 medical error in medication continuity, diagnostic workup, or test follow‐up.7 It has been reported that 19%23% of patients suffer an adverse event, most frequently an adverse drug event (ADE).911 Half of ADEs are considered preventable or ameliorable (ie, their severity or duration could have been decreased). Most errors and adverse events in this setting result from a breakdown in communication between the hospital team and the patient or primary care physician.10
To promote more effective care transitions, The Joint Commission now requires accredited facilities to accurately and completely reconcile medications across the continuum of care.12 The Society of Hospital Medicine recently published recommendations for the discharge of elderly patients.13 The joint Society of Hospital MedicineSociety of General Internal Medicine Continuity of Care Task Force also recently published a systematic review with recommendations for improving the handoff of patient information at discharge.14 Apart from these reports, however, it is uncommon to find evidence‐based recommendations for hospital discharge applicable to a broad range of patients.15 This review highlights several important challenges for physicians who seek to provide high‐quality care during hospital discharge and the subsequent period of transition. Based on the best available evidence, recommendations are also provided for how to improve communication and facilitate the care transition for adult inpatients returning home.
INPATIENTOUTPATIENT PHYSICIAN DISCONTINUITY
Traditionally, primary care physicians have admitted their own patients, provided hospital care (in addition to seeing outpatients during the day), and followed patients after discharge. Under this model, continuity of care has been preserved; however, this method of care has faltered under the weight of inpatients and outpatients with more severe illnesses, rapid technological advancements, managed care pressuring outpatient physicians to see more patients, and a thrust toward reduced hospital costs and length of stay.16 Increases in the efficiency and quality of hospital care have accompanied a new reliance on the field of hospital medicine, while allowing PCPs to focus on outpatient care.1719 With more than 14,000 hospitalists currently practicing in the United States and 25,000 anticipated to be practicing by 2010, transfer of care from hospital‐based providers to PCPs has become increasingly common at discharge.20
Patient discharge summaries are the most common means of communication between inpatient and outpatient providers. However, numerous studies have shown that discharge summaries often fail to provide important administrative and medical information, such as the primary diagnosis, results of abnormal diagnostics, details about the hospital course, follow‐up plans, whether laboratory test results are pending, and patient or family counseling.14 Summaries also may not arrive in a timely manner and sometimes may not reach the PCP at all.2123
At the time patients first follow up with their PCPs after hospitalization, discharge summaries have not yet arrived about 75% of the time,22, 24, 25 restricting the PCPs' ability to provide adequate follow‐up care in 24% of hospital follow‐up visits, according to one study.26 In another investigation, PCPs reported being unaware of 62% of the pending test results that returned after discharge, of which 37% were considered actionable.27
Improving Physician Information Transfer and Continuity
To improve information transfer from hospitalist to PCP, attention must be paid to the content, format, and timely delivery of discharge information (Table 1).14 Surveys of primary care physicians suggest the following information should be included in discharge summaries: diagnoses, abnormal physical findings, important test results, discharge medications, follow‐up arrangements made and appointments that still need to be made, counseling provided to the patient and family, and tests still pending at discharge.24, 2833 These domains are consistent with Joint Commission guidelines for discharge summaries,34 and the inclusion of a detailed medication list and pending test results also has implications for patient safety.911, 27
| Challenge | Recommended approaches |
|---|---|
| Inpatientoutpatient physician discontinuity | When possible, involve the primary care physician (PCP) in discharge planning and work together to develop a follow‐up plan |
| At minimum, communicate the following to the PCP on the day of discharge: diagnoses, medications, results of procedures, pending tests, follow‐up arrangements, and suggested next steps | |
| Provide the PCP with a detailed discharge summary within 1 week | |
| In discharge summaries include: diagnoses, abnormal physical findings, important test results, discharge medications with rationale for new or changed medications, follow‐up arrangements made, counseling provided to the patient and family, and tasks to be completed (eg, appointments that still need to be made and tests that require follow‐up) | |
| Follow a structured template with subheadings in discharge communications | |
| When possible, use health information technology to create and disseminate discharge summaries | |
| Changes and discrepancies in medication regimen | Obtain a complete medication history by asking patients about: medications taken at different times of day; medications prescribed by different physicians; nonoral medications; over‐the‐counter products; dosage, indication, length of therapy, and timing of last dose of all drugs; allergies; and adherence |
| Compare and reconcile medication information obtained from patient and caregiver reports, patient lists, prescription bottles, medical records, and pharmacy records | |
| Display preadmission medication list prominently in the chart | |
| Reconcile medications at all care transitions, including admission, intrahospital transfer, and discharge | |
| Communicate complete and accurate medication information to the next provider at discharge, including indications for new medications and reasons for any changes | |
| When possible, partner with clinical pharmacists to manage medication information and reconciliation, especially for high‐risk patients | |
| Self‐care responsibilities and social support | Use multidisciplinary discharge planning teams to assess the needs of patients and their families |
| Arrange a specific follow‐up appointment prior to discharge | |
| Contact patients by telephone a few days after discharge to assess questions, symptoms, and medication‐related issues | |
| Order home health services when indicated | |
| Consider home visits for frail elderly patients | |
| Ineffective physicianpatient communication | Focus discharge counseling on informing patients of major diagnoses, medication changes, dates of follow‐up appointments, self‐care instructions, and who to contact if problems develop |
| Ensure that staff members communicate consistent instructions | |
| For high‐volume conditions, consider using audiovisual recordings for discharge education, combined with an opportunity for additional counseling and questions | |
| Use trained interpreters when a language gap exists | |
| Provide simply written materials that include illustrations when possible to reinforce verbal instructions | |
| Ensure patients and family members comprehend key points by asking them to teach back the information in their own words and demonstrate any self‐care behaviors | |
| Encourage patients and family members to ask questions through an open‐ended invitation like, What questions do you have? instead of Do you have any questions? |
Because many patients follow up with their PCPs within a few days of discharge, it becomes important to provide the PCPs with some information about the hospitalization on the day of discharge. This can be accomplished via a quick telephone call, fax, or e‐mail update to the PCP.24, 35 Important things to include in this communiqu are the discharge diagnosis, medications, results of procedures, pending test results, follow‐up arrangements, and suggested next steps. Within 1 week, a detailed discharge summary should have been received.26, 33, 36 As electronic medical records become more widely available, computer‐generated summaries offer a way to more quickly and completely highlight the key elements of the hospitalization, and they are ready for delivery sooner than traditional dictated summaries.37 Additionally, all forms of discharge summariescomputer‐generated, handwritten, and dictatedshould include subheadings to better organize and present the information instead of unstructured narrative summaries.38
There is increasing interest in moving away from the traditional 1‐way transfer of information about a hospitalization toward a 2‐way dialogue between hospitalist and primary care physician.39 Preferences about how to do this will vary among physicians. One strategy might be to provide the PCP with the hospitalist's contact information and encouraging questions about the hospitalization. Another approach would involve contacting the PCP during the discharge planning process to exchange information about the patient, provide an opportunity for the PCP to ask questions about the hospitalization, and formulate a cohesive plan for follow‐up, particularly about contingency planning (ie, what is most likely to go wrong and what should be done about it) and specific follow‐up needs (ie, what tasks should be accomplished at the first postdischarge visit).
CHANGES AND DISCREPANCIES IN THE MEDICATION REGIMEN
Medication errors make up a large portion of the adverse events patients may experience in the period following hospital discharge.7 In fact, errors during the ordering of admission or discharge medications make up almost half of all hospital medication errors.4043 At transition points such as admission and discharge, errors are often associated with changes in the medication regimen, including discrepancies between the new set of medication orders and what the patient was taking previously. In 2 recent studies, 54% of patients experienced at least 1 unintended medication discrepancy on admission to the hospital, and 39%‐45% of these discrepancies were considered a potential threat to the patient.44, 45
At discharge, differences between the prescribed medication regimen and the prehospital regimen may exist for several reasons. First, physicians may not obtain a comprehensive and accurate medication history at the time of admission.46 The medication history elicited from the patient at hospital admission is often affected by health literacy, language barriers, current health status, medication‐history interviewing skills, and time constraints.47 Physicians may not consult other important sources of medication information, including family members, prescription lists or bottles, and community pharmacy records. The most common error in the admission medication history is omitting a medication taken at home.46 Additionally, several providers, including a physician, a nurse, and an inpatient pharmacist, may independently take medication histories for the same patient. These multiple accounts lead to discrepancies that are rarely recognized or corrected.
Second, a patient's medication regimen can be significantly altered several times during a hospitalization. Acute illness may cause physicians to hold certain medications, discontinue others, or change prescribed doses during hospitalization.48 In addition, at most hospitals closed drug formularies necessitate automatic substitution of 1 medication for another drug in the same class during the patient's hospital stay.49 Changes from long‐acting to short‐acting medications are also routinely made in the name of tighter control (eg, of blood pressure). One study of hospitalized elders found that 40% of all admission medications had been discontinued by discharge and that 45% of all discharge medications were newly started during the hospitalization.3
Finally, at discharge, the current medication regimen needs to be reconciled with the preadmission medication regimen in a thoughtful manner.2 This includes resuming medications held or modified at admission for clinical reasons, resuming medications that were substituted in the hospital for formulary or pharmacokinetic reasons, and stopping newly started medications that were only required during the hospitalization (eg, for prevention of venous thromboembolism or stress ulcers).50 It is difficult, even in hospitals with advanced electronic health information systems, to prompt physicians to make these necessary changes. In a recent study, unexplained discrepancies between the preadmission medication list and discharge medication orders were noted in 49% of hospital discharges.51 Errors in discharge medication reconciliation may subsequently increase the risk of postdischarge ADEs.51
Medication Reconciliation and Education
An optimal strategy for obtaining a complete medication history may include asking patients about the following: a typical day and what medications are taken at different times of day; whether prescriptions come from more than 1 doctor; medications not taken orally (eg, inhalers, patches); dosages and indications for all medications; length of therapy and timing of last dose; over‐the‐counter products, herbals, vitamins, and supplements used and vaccinations received; allergies; and number of doses missed in the last week (Table 1).5254 Forms are also available to help patients maintain a list of current medications.5557
Ideally, the process of obtaining a medication history involves integration of information from several sources, including patient and caregiver recollections, patient‐provided lists of medications, prescription bottles, outpatient medical records, and prescription refill information from community pharmacies.58, 59 Any discrepancies in the information obtained should be explicitly resolved with the patient and/or caregiver. Assistance from a pharmacist or the patient's PCP may also be required.
Once the preadmission medication regimen is confirmed, it should be entered on a standardized form and placed in a prominent place in the chart. This list should then be compared against the patient's medication orders at admission, throughout the hospital stay, and at discharge.12 The planned action for each of these medications (eg, continue at same dose/route/frequency, substitute) should be made explicit. At discharge, this preadmission list also needs to be compared with the current hospital medications in order to create a coherent set of discharge orders.
Staff responsibilities for obtaining and documenting an accurate list of preadmission medications and reconciling medications at admission, transfer, and discharge should be well defined and based on the resources available at each institution. Redundant work (eg, multiple personnel independently taking a medication history) should be replaced by interdisciplinary communication (ie, a member of the team confirming the accuracy of a list obtained by another member of the team). When discrepancies are found (eg, between preadmission and discharge medications), reconciliation requires correction of unintentional discrepancies and appropriate documentation of intentional changes.60
Because a patient's medications change frequently during the transitions of admission, intrahospital transfer, and discharge, reconciliation is an active and ongoing process that aims to ensure the patient is receiving the correct medication regimen at all times. Reconciliation also allows for a review of the safety and appropriateness of the regimen and discontinuation of any unsuitable or needless medications.61, 62
Finally, a comprehensive list of a patient's medications should be reported to the next service provider when the patient is referred or transferred to another setting, service, practitioner, or level of care within or outside the organization. Avoiding overarching orders such as continue home medications and resume all medications becomes crucial to patient safety during transitions in care. At discharge, physicians should provide patients with a complete list of medications to be taken at home with indications and instructions for administration written in everyday language. Physicians should also highlight the results of medication reconciliation by pointing out any changes from the preadmission regimen, especially medications that are at home but should no longer be taken.
Ultimately, physicians have the duty to ensure that correct and complete medication information is provided. However, to achieve optimal results, physicians should partner with clinical pharmacists when possible. Pharmacists have been formally educated about and are experienced at taking medication histories, which may make them the ideal individuals to interview newly admitted patients about their medication histories.63 Unfortunately, according to a recent survey, pharmacists perform admission drug histories in only 5% of U.S. hospitals and provide drug therapy counseling in just 49% of U.S. hospitals.64 Patients who are elderly, have limited literacy skills, take more than 5 medications daily, or take high‐risk medications such as insulin, warfarin, cardiovascular drugs (including antiarrhythmics), inhalers, antiseizure medications, eye medications, analgesics, oral hypoglycemics, oral methotrexate, and immunosuppressants may require additional counseling or pharmacist involvement for effective reconciliation.10, 65, 66
Although the evidence supporting medication reconciliation is limited, it is convincing enough to support carrying out such reconciliations. In 1 investigation, when the nursing staff obtained and pharmacists verified orders for home medications, the accuracy of admission medication orders increased from 40% to 95%.67 In another work, in which there was pharmacist‐led medication reconciliation, significant discrepancies were found in approximately 25% of patients' medication histories and admission orders.45 In the absence of pharmacist intervention, the authors predicted that 22% of the discrepancies could have caused some form of patient harm during hospitalization and that 59% of the discrepancies might have contributed to an adverse event if the error continued after discharge.45 Others report that orders were changed as a result of reconciliation for 94% of patients being transferred out of the intensive care unit.2 Finally, in a randomized controlled trial of a pharmacist intervention at discharge in which medication reconciliation was the most common action performed, after 30 days preventable ADEs were detected in 11% of control patients and 1% of intervention patients. Medication discrepancy was the cause of half the preventable ADEs in the control group.51
SELF‐CARE RESPONSIBILITIES AND SOCIAL SUPPORT
Compounding the difficulties at discharge are the economic pressures on our health care system, causing patients to be released from the hospital quicker and sicker than ever before.68 The scope of care provided to patients also undergoes a major shift at discharge. Multidisciplinary providers no longer continually review the health status and needs of patients; instead, patients must follow up with their outpatient physician over a period of days to weeks. In the interim, the patients themselves are responsible for administering new medications, participating in physical therapy, and tracking their own symptoms to see if they are worsening. For many patients, sufficient social and family support is not available to help perform these activities effectively. Unfortunately, hospital personnel often inaccurately assess patients' functional status and overestimate patients' knowledge of required self‐care activities.69
Providing Adequate Medical and Social Support
A multidisciplinary discharge planning team can facilitate proper assessments of the social needs of patients and their families (Table 1).7072 This team is often composed of a nurse case manager and a social worker but may also include a physical therapist, an occupational therapist, a pharmacist, and other health care providers. Following discussion with a patient and the patient's family, the team may suggest home health services during the transition home to supplement available medical support,73 or they may decide that discharge to a rehabilitation or skilled nursing facility is more appropriate.
In addition, follow‐up should be arranged prior to discharge. Patients who are given a set appointment are more likely to show up for their follow‐up visits than are those who are simply asked to call and arrange their own visits.74 Typically, follow‐up with the PCP should be conducted within 2 weeks of hospital discharge. However, depending on a patient's functional status, pending test results, and need for medication monitoring or follow‐up testing, this may need to take place sooner. Interestingly, research indicates that follow‐up appointments with the inpatient provider can result in a lower combined rate of readmission and 30‐day mortality.75 Thus, hospitalists may consider operating a hospitalist‐staffed follow‐up clinic, especially for patients without a regular PCP.
Telephone follow‐up conducted a few days after discharge can also be an effective means of bridging the inpatientoutpatient transition.35 Such follow‐up provides a chance to attend to any patient questions, new or concerning symptoms, and medication‐related issues (eg, not filling the discharge medications or difficulty comprehending the new medication regimen).76 A physician, physician assistant, advanced practice nurse, registered nurse, pharmacist, or care manager can effectively carry out this telephone follow‐up. No matter who telephones, the caller must be aware of the patient's recent course of events as well as the care plan decided at discharge. Published evidence indicates that telephone follow‐up fosters patient satisfaction, increases medication adherence, decreases preventable ADEs, and decreases the number of subsequent emergency room visits and hospital readmissions,51, 77, 78 although not all evaluations have demonstrated benefit.79 As with medication histories performed by pharmacists, limited resources may mean that such follow‐up be restricted to those patients at highest risk for readmission.
Home visits may be appropriate for certain patient populations, such as the frail elderly.80 Home visits enable a patient's daily needs and safety (eg, fall risk) to be assessed. They can also be a means of assessing medication safety and adherence by reviewing all prescription and over‐the‐counter products in the household.81 Close follow‐up of at‐risk or elderly patients after discharge can help to minimize hospital readmission and total health care costs.4, 8285
INEFFECTIVE PHYSICIANPATIENT COMMUNICATION
Physicianpatient communication is fundamental to the practice of medicine and is crucially important at discharge. However, several studies have demonstrated a disconnect between physician information giving and patient understanding.76, 9690 When providing instructions, physicians commonly use medical jargon and attempt to cover a wealth of information in a limited amount of time.69, 87 They also tend to rely on verbal instructions and fail to provide supplementary audiovisual materials (eg, educational handouts or videos) that could aid patient comprehension. Physicians may not point out important self‐care tasks that patients should carry out at home. The entire interaction may be rushed or seem rushed. Moreover, when physicians solicit questions from patients, they may only allow for yes/no responses by using statements like Any questions? or Do you have any questions? that make it easy for patients to simply respond, No. The encounter usually comes to an end without true confirmation of a patient's level of understanding or assessment of a patient's ability to perform the self‐care activities and medication management required on returning home.81
Adding to the challenges of effective physicianpatient communication is the large number of adult Americans (more than 90 million) who have limited functional literacy skills.91, 92 Such patients typically have difficulty reading and understanding medical instructions, medication labels, and appointment slips.9396 Not surprisingly, patients with limited literacy skills know less about their chronic illnesses and how to manage their diseases.97 Having low literacy is also linked to increased use of emergency department services, a higher risk of hospitalization, and higher health care costs.9799 Patients with limited English proficiency have similar or even greater challenges and also have longer stays in the hospital.100
More Effective PhysicianPatient Communication
Discharge counseling should concentrate on the few key points that are of the greatest interest and the most importance to patients: major diagnoses, medication changes, dates of follow‐up appointments, self‐care instructions, and who to contact if problems develop (Table 1).101 Furthermore, these key instructions should be reinforced by other hospital staff, including nurses and pharmacists. For common conditions (eg, high‐volume cardiac procedures), offering standardized audiovisual instructions can be both efficient and worthwhile if used in conjunction with questionanswer sessions.102 In the event that physicians and hospital staff cannot fluently communicate in a patient's language, it is essential to engage trained interpreters, not rely on rudimentary language skills, the patient's family, or other ad hoc ways to communicate.103
Because patients are unlikely to fully remember verbal instructions at discharge, it is helpful to provide patients and family members with written materials to take home in order to reinforce important self‐care instructions.76, 87 These materials, written at a 5th‐ to 8th‐grade reading level, should outline key information in a simple format with little or no medical jargon. Illustrated materials are often better comprehended and subsequently remembered by patients.104, 105 If preprinted illustrated materials are not on hand, then physicians can convey key points by drawing simple pictures.
Confirming patient comprehension with the teach‐back method is perhaps the most important step in effectively communicating discharge instructions.106 With this method, patients are asked to repeat back what they understand from the discharge instructions. Application of this simple technique is advocated as one of the most effective means of improving patient safety.107, 108 Patients should also be asked to demonstrate any new self‐care tasks that they will be required to carry out at home, such as using an inhaler or administering a subcutaneous injection.
Last, The Joint Commission recently created a National Patent Safety Goal to encourage the active involvement of patients and their families in the patient's own care.12 This charge requires that physicians offer ample time for patients and their family members to ask questions. Physicians should avoid questions with yes/no responses and instead invite patient and family member questions in a more open‐ended manner (eg, What questions do you have?) to help ensure comprehension and comfort with the care plan.
CONCLUSIONS
The transition from hospital to home is a vulnerable period of discontinuity and potential adverse events. Hospitalists and other inpatient providers should not view discharge as an end to their obligation to patients but rather should attempt to promote a safe and efficient transition of care. Hospitalists can play an important role in bridging the gap between inpatient and outpatient care through appropriate discharge planning and effective communication with patients, their family members, and outpatient physicians.
Acknowledgements
The authors thank Marra Katz for her editorial assistance in the preparation of this manuscript
- .Whither continuity of care?N Engl J Med.1999;340:1362–1363.
- ,,, et al.Medication reconciliation: a practical tool to reduce the risk of medication errors.J Crit Care.2003;18(4):201–205.
- ,,,.Influence of hospitalization on drug therapy in the elderly.J Am Geriatr Soc.1989;37:679–683.
- ,,,,,.Preparing patients and caregivers to participate in care delivered across settings: the Care Transitions Intervention.J Am Geriatr Soc.2004;52:1817–1825.
- ,,.Predictors of elder and family caregiver satisfaction with discharge planning.J Cardiovasc Nurs.2000;14(3):76–87.
- ,.Discharge planning and continuity of care for aged people: indicators of satisfaction and implications for practice.Aust J Adv Nurs.1998;16(1):7–13.
- ,,,.Medical errors related to discontinuity of care from an inpatient to an outpatient setting.J Gen Intern Med.2003;18:646–651.
- ,,.Assessing the quality of preparation for posthospital care from the patient's perspective: the care transitions measure.Med Care.2005;43(3):246–255.
- ,,, et al.Adverse events among medical patients after discharge from hospital.CMAJ.2004;170:345–349.
- ,,,,.The incidence and severity of adverse events affecting patients after discharge from the hospital.Ann Intern Med.2003;138:161–167.
- ,,,,.Adverse drug events occurring following hospital discharge.J Gen Intern Med.2005;20:317–323.
- The Joint Commission. Joint Commission National Patient Safety Goals. Available at: http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/. Accessed July 17,2006.
- ,,, et al.Transition of care for hospitalized elderly patients ‐ Development of a discharge checklist for hospitalists.J Hosp Med.2006;1:354–360.
- ,,,,,.Deficits in communication and information transfer between hospital‐based and primary care physicians: implications for patient safety and continuity of care.JAMA.2007;297:831–841.
- Agency for Healthcare Research and Quality. National Guideline Clearinghouse. Available at: http://www.guideline.gov. Accessed January 3,2007.
- ,.The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335:514–517.
- .Hospitalists in the United States—mission accomplished or work in progress?N Engl J Med.2004;350:1935–1936.
- .The evolution of the hospitalist model in the United States.Med Clin North Am2002;86(4):687–706.
- ,.The hospitalist movement 5 years later.JAMA.2002;287:487–494.
- Society of Hospital Medicine. Growth of hospital medicine nationwide. Available at: http://www.hospitalmedicine.org/Content/NavigationMenu/Media/GrowthofHospitalMedicineNationwide/Growth_of_Hospital_M.htm. Accessed July 17,2006.
- ,,,,.Quality assessment of discharge letters in a French university hospital.Int J Health Care Qual Assur Inc Leadersh Health Serv.1998;11(2‐3):90–95.
- ,,.Dissemination of discharge summaries. Not reaching follow‐up physicians.Can Fam Physician.2002;48:737–742.
- ,.Quality assessment of a discharge summary system.CMAJ.1995;152:1437–1442.
- ,,,.Primary care physician attitudes regarding communication with hospitalists.Am J Med.2001;111(9B):15S–20S.
- ,,,.Effect of discharge summary availability during post‐discharge visits on hospital readmission.J Gen Intern Med.2002;17(3):186–192.
- .Study of discharge communications from hospital doctors to an inner London general practice.J R Coll Gen Pract.1987;37:494–495.
- ,,, et al.Patient safety concerns arising from test results that return after hospital discharge.Ann Intern Med.2005;143(2):121–128.
- ,,.Communication between general practitioners and consultants: what should their letters contain?BMJ1992;304(6830):821–824.
- ,,,.Written communication from specialists to general practitioners in cancer care. What are the expectations and how are they met?Scand J Prim Health Care.1998;16(3):154–159.
- ,.Improving the continuity of care between general practitioners and public hospitals.Med J Aust.1994;161:656–659.
- ,.Towards better discharge summaries: brevity and structure.West Engl Med J.1991;106(2):40–41,55.
- ,,.Content of a discharge summary from a medical ward: views of general practitioners and hospital doctors.J R Coll Physicians Lond.1995;29:307–310.
- ,.What is necessary for high‐quality discharge summaries?Am J Med Qual.1999;14(4):160–169.
- The Joint Commission.Standard IM.6.10. Hospital Accreditation Standards.Oakbrook Terrace, IL:The Joint Commission;2006:338–340.
- .The importance of postdischarge telephone follow‐up for hospitalists: a view from the trenches.Am J Med.2001;111(9B):43S–44S.
- ,,,.The quality of communication between hospitals and general practitioners: an assessment.J Qual Clin Pract.1998;18:241–247.
- ,,,.Dictated versus database‐generated discharge summaries: a randomized clinical trial.CMAJ.1999;160:319–326.
- ,,,.Standardized or narrative discharge summaries. Which do family physicians prefer?Can Fam Physician.1998;44:62–69.
- ,.Moving from information transfer to information exchange in health and health care.Soc Sci Med.2003;56:449–464.
- ,,, et al.The costs of adverse drug events in hospitalized patients.Adverse Drug Events Prevention Study Group.JAMA.1997;277:307–311.
- ,,, et al.Systems analysis of adverse drug events.ADE Prevention Study Group.JAMA.1995;274(1):35–43.
- ,,, et al.Incidence of adverse drug events and potential adverse drug events. Implications for prevention.ADE Prevention Study Group.JAMA.1995;274(1):29–34.
- ,.Medication errors in hospitalized cardiovascular patients.Arch Intern Med.2003;163:1461–1466.
- ,,, et al.Unintended medication discrepancies at the time of hospital admission.Arch Intern Med.2005;165:424–429.
- ,,,,,.Reconciliation of discrepancies in medication histories and admission orders of newly hospitalized patients.Am J Health Syst Pharm.2004;61:1689–1695.
- ,,,,,.Frequency, type and clinical importance of medication history errors at admission to hospital: a systematic review.CMAJ.2005;173:510–515.
- ,,,,.Medication reconciliation in the acute care setting: opportunity and challenge for nursing.J Nurs Care Qual.2005;20(2):95–98.
- ,,.The adverse effects of hospitalization on drug regimens.Arch Intern Med.1991;151:1562–1564.
- ,,,,.Prevalence and cost savings of therapeutic interchange among U.S. hospitals.Am J Health Syst Pharm.2002;59:529–533.
- ,,, et al.Medication reconciliation: are we meeting the requirements?JCOM.2006;13:441–444.
- ,,, et al.Role of pharmacist counseling in preventing adverse drug events after hospitalization.Arch Intern Med.2006;166:565–571.
- ,.Effectiveness of a pharmacist‐acquired medication history in promoting patient safety.Am J Health Syst Pharm.2002;59:2221–2225.
- .Ensuring continuity of care and accuracy of patients' medication history on hospital admission.Am J Health Syst Pharm.2002;59:1054–1055.
- ,,,.Current methods used to teach the medication history interview to doctor of pharmacy students.Am J Pharm Educ.2002;66(Summer):103–107.
- AARP. My Personal Medication Record. Available at: http://assets.aarp.org/www.aarp.org_/articles/learntech/wellbeing/medication‐record.pdf. Accessed October 20,2006.
- AARP. Mi registro de medicacion. Available at: http://assets.aarp.org/www.aarp.org_/articles/health/docs/PersonalMedRecordSP.pdf. Accessed October 20,2006.
- Institute for Safe Medication Practices. Available at: http://www.ismp.org. Accessed September 8,2006.
- ,,.Parents as partners in obtaining the medication history.J Am Med Inform Assoc.2005;12:299–305.
- ,,.Medication history on internal medicine wards: assessment of extra information collected from second drug interviews and GP lists.Pharmacoepidemiology Drug Saf.2003;12:491–498.
- Medication Discrepancy Tool. Available at: http://www.caretransitions.org. Accessed July 28,2005.
- ,,,,,.Updating the Beers criteria for potentially inappropriate medication use in older adults: results of a US consensus panel of experts.Arch Intern Med.2003;163:2716–2724.
- .Using the NO TEARS tool for medication review.BMJ2004;329(7463):434.
- ,,,.Clinical pharmacists and inpatient medical care: a systematic review.Arch Intern Med.2006;166:955–964.
- ,.Clinical pharmacy services, pharmacy staffing, and adverse drug reactions in United States hospitals.Pharmacotherapy.2006;26:735–747.
- ,,, et al.Adverse drug events in ambulatory care.N Engl J Med.2003;348:1556–1564.
- MA Coalition for the Prevention of Medical Errors. Reconciling medications. Recommended practices. Available at: http://www.macoalition.org/documents/RecMedPractices.pdf. Accessed July 27,2005.
- ,.OSF healthcare's journey in patient safety.Qual Manag Health Care.2004;13(1):53–59.
- ,,, et al.Prospective payment system and impairment at discharge. The ‘quicker‐and‐sicker’ story revisited.JAMA.1990;264:1980–1983.
- ,,,,,.Discharge planning: comparison of patients and nurses' perceptions of patients following hospital discharge.Image J Nurs Sch.1996;28(2):143–147.
- ,,,.The Care Transitions Intervention: results of a randomized controlled trial.Arch Intern Med.2006;166:1822–1828.
- ,,,,,.Comprehensive discharge planning with postdischarge support for older patients with congestive heart failure: a meta‐analysis.JAMA.2004;291:1358–1367.
- ,,,.Discharge planning from hospital to home.Cochrane Database Syst Rev.2006;4.
- .Falling through the cracks: challenges and opportunities for improving transitional care for persons with continuous complex care needs.J Am Geriatr Soc.2003;51:549–555.
- .The best way to improve emergency department follow‐up is actually to give the patient a specific appointment.J Gen Intern Med.2006;21:398; author reply398.
- ,,,.Continuity of care and patient outcomes after hospital discharge.J Gen Intern Med.2004;19:624–631.
- ,.Patients' understanding of their treatment plans and diagnosis at discharge.Mayo Clin Proc.2005;80:991–994.
- ,,,.The impact of follow‐up telephone calls to patients after hospitalization.Am J Med.2001;111(9B):26S–30S.
- ,.The impact of clinical pharmacists' consultations on geriatric patients' compliance and medical care use: a randomized controlled trial.Gerontologist.1994;34:307–315.
- ,.Telephone follow‐up, initiated by a hospital‐based health professional, for postdischarge problems in patients discharged from hospital to home.Cochrane Database Syst Rev.2007;1.
- ,,, et al.Geriatric home assessment after hospital discharge.J Am Geriatr Soc.1994;42:1229–1234.
- ,.Uncovering a multitude of sins: medication management in the home post acute hospitalisation among the chronically ill.Aust N Z J Med.1999;29(2):220–227.
- ,,, et al.Comprehensive discharge planning and home follow‐up of hospitalized elders: a randomized clinical trial.JAMA.1999;281:613–620.
- ,,,.The cost‐effectiveness of intensive postdischarge care. A randomized trial.Med Care.1988;26:1092–1102.
- ,,,,.The effects of aftercare on chronic patients and frail elderly patients when discharged from hospital: a systematic review.J Adv Nurs.1998;27:1076–1086.
- ,,,,,.A multidisciplinary intervention to prevent the readmission of elderly patients with congestive heart failure.N Engl J Med.1995;333:1190–1195.
- ,,.Medication education of acutely hospitalized older patients.J Gen Intern Med.1999;14:610–616.
- ,,, et al.Patient‐physician communication at hospital discharge and patients' understanding of the postdischarge treatment plan.Arch Intern Med.1997;157:1026–1030.
- ,,.Patient understanding of commonly used medical vocabulary.J Fam Pract.1987;25:176–178.
- .The understanding of medical terminology used in printed health education materials.Heal Educ J.1979;38:111–121.
- ,,,,.The gap between patient reading comprehension and the readability of patient education materials.J Fam Pract.1990;31:533–538.
- ,,. National Assessment of Adult Literacy (NAAL). A first look at the literacy of America's adults in the 21st century. Available at: http://nces.ed.gov/naal. Accessed May 2,2006.
- ,,,.Adult Literacy in America: A First Look at the Findings of the National Adult Literacy Survey.Washington, DC:National Center for Education Statistics, U.S. Department of Education;1993.
- ,,,.The role of health literacy in patient‐physician communication.Fam Med.2002;34:383–389.
- American Medical Association Council on Scientific Affairs.Health literacy.JAMA.1999;281:552–557.
- National Work Group on Literacy and Health.Communicating with patients who have limited literacy skills.J Fam Pract.1998;46:168–176.
- ,.Communicating with patients who cannot read.N Engl J Med.1997;337:272–274.
- ,,,,.Literacy and health outcomes: a systematic review of the literature.J Gen Intern Med.2004;19:1129–1139.
- ,,.The impact of low health literacy on the medical costs of Medicare managed care enrollees.Am J Med.2005;118:371–377.
- ,,,.Health literacy and the risk of hospital admission.J Gen Intern Med.1998;13:791–798.
- ,,, et al.The effect of English language proficiency on length of stay and in‐hospital mortality.J Gen Intern Med.2004;19(3):221–228.
- ,,, et al.Effects of a structured patient‐centered discharge interview on patients' knowledge about their medications.Am J Med.2004;117:563–568.
- ,,.Effects of a videotape information intervention at discharge on diet and exercise compliance after coronary artery bypass surgery.J Cardiopulm Rehab.1999;19(3):170–177.
- .The impact of medical interpreter services on the quality of health care: a systematic review.Med Care Res Rev.2005;62(3):255–299.
- ,,.Use of pictorial aids in medication instructions: a review of the literature.Am J Health Syst Pharm.2006;63:2391–2397.
- ,,,.The role of pictures in improving health communication: A review of research on attention, comprehension, recall, and adherence.Patient Educ Couns.2006;61(2):173–190.
- ,,, et al.Closing the loop. Physician communication with diabetic patients who have low health literacy.Arch Intern Med.2003;163:83–90.
- National Quality Forum.Safe Practices for Better Healthcare,2003; Washington, DC.
- Shojania KG, Duncan BW, McDonald KM, Wachter RM, eds.Making Healthcare Safer: A Critical Analysis of Patient Safety Practices. Evidence Report No. 43 from the Agency for Healthcare Research and Quality. AHRQ Publication No. 01‐E058;2001.
As the counterpart to hospital admission, hospital discharge is a necessary process experienced by each living patient. For all patients except those being transferred to a continuing care facility, discharge is a period of transition from hospital to home that involves a transfer in responsibility from the inpatient provider or hospitalist to the patient and primary care physician (PCP).1 Prescription medications are commonly altered at this transition point, with patients asked to discontinue some medications, switch to a new dosage schedule of others, or begin new treatments.2, 3 Self‐care responsibilities also increase in number and importance, presenting new challenges for patients and their families as they return home.4 Under these circumstances, ineffective planning and coordination of care can undermine patient satisfaction, facilitate adverse events, and contribute to more frequent hospital readmissions.58
Following hospital discharge nearly half (49%) of hospitalized patients experience at least 1 medical error in medication continuity, diagnostic workup, or test follow‐up.7 It has been reported that 19%23% of patients suffer an adverse event, most frequently an adverse drug event (ADE).911 Half of ADEs are considered preventable or ameliorable (ie, their severity or duration could have been decreased). Most errors and adverse events in this setting result from a breakdown in communication between the hospital team and the patient or primary care physician.10
To promote more effective care transitions, The Joint Commission now requires accredited facilities to accurately and completely reconcile medications across the continuum of care.12 The Society of Hospital Medicine recently published recommendations for the discharge of elderly patients.13 The joint Society of Hospital MedicineSociety of General Internal Medicine Continuity of Care Task Force also recently published a systematic review with recommendations for improving the handoff of patient information at discharge.14 Apart from these reports, however, it is uncommon to find evidence‐based recommendations for hospital discharge applicable to a broad range of patients.15 This review highlights several important challenges for physicians who seek to provide high‐quality care during hospital discharge and the subsequent period of transition. Based on the best available evidence, recommendations are also provided for how to improve communication and facilitate the care transition for adult inpatients returning home.
INPATIENTOUTPATIENT PHYSICIAN DISCONTINUITY
Traditionally, primary care physicians have admitted their own patients, provided hospital care (in addition to seeing outpatients during the day), and followed patients after discharge. Under this model, continuity of care has been preserved; however, this method of care has faltered under the weight of inpatients and outpatients with more severe illnesses, rapid technological advancements, managed care pressuring outpatient physicians to see more patients, and a thrust toward reduced hospital costs and length of stay.16 Increases in the efficiency and quality of hospital care have accompanied a new reliance on the field of hospital medicine, while allowing PCPs to focus on outpatient care.1719 With more than 14,000 hospitalists currently practicing in the United States and 25,000 anticipated to be practicing by 2010, transfer of care from hospital‐based providers to PCPs has become increasingly common at discharge.20
Patient discharge summaries are the most common means of communication between inpatient and outpatient providers. However, numerous studies have shown that discharge summaries often fail to provide important administrative and medical information, such as the primary diagnosis, results of abnormal diagnostics, details about the hospital course, follow‐up plans, whether laboratory test results are pending, and patient or family counseling.14 Summaries also may not arrive in a timely manner and sometimes may not reach the PCP at all.2123
At the time patients first follow up with their PCPs after hospitalization, discharge summaries have not yet arrived about 75% of the time,22, 24, 25 restricting the PCPs' ability to provide adequate follow‐up care in 24% of hospital follow‐up visits, according to one study.26 In another investigation, PCPs reported being unaware of 62% of the pending test results that returned after discharge, of which 37% were considered actionable.27
Improving Physician Information Transfer and Continuity
To improve information transfer from hospitalist to PCP, attention must be paid to the content, format, and timely delivery of discharge information (Table 1).14 Surveys of primary care physicians suggest the following information should be included in discharge summaries: diagnoses, abnormal physical findings, important test results, discharge medications, follow‐up arrangements made and appointments that still need to be made, counseling provided to the patient and family, and tests still pending at discharge.24, 2833 These domains are consistent with Joint Commission guidelines for discharge summaries,34 and the inclusion of a detailed medication list and pending test results also has implications for patient safety.911, 27
| Challenge | Recommended approaches |
|---|---|
| Inpatientoutpatient physician discontinuity | When possible, involve the primary care physician (PCP) in discharge planning and work together to develop a follow‐up plan |
| At minimum, communicate the following to the PCP on the day of discharge: diagnoses, medications, results of procedures, pending tests, follow‐up arrangements, and suggested next steps | |
| Provide the PCP with a detailed discharge summary within 1 week | |
| In discharge summaries include: diagnoses, abnormal physical findings, important test results, discharge medications with rationale for new or changed medications, follow‐up arrangements made, counseling provided to the patient and family, and tasks to be completed (eg, appointments that still need to be made and tests that require follow‐up) | |
| Follow a structured template with subheadings in discharge communications | |
| When possible, use health information technology to create and disseminate discharge summaries | |
| Changes and discrepancies in medication regimen | Obtain a complete medication history by asking patients about: medications taken at different times of day; medications prescribed by different physicians; nonoral medications; over‐the‐counter products; dosage, indication, length of therapy, and timing of last dose of all drugs; allergies; and adherence |
| Compare and reconcile medication information obtained from patient and caregiver reports, patient lists, prescription bottles, medical records, and pharmacy records | |
| Display preadmission medication list prominently in the chart | |
| Reconcile medications at all care transitions, including admission, intrahospital transfer, and discharge | |
| Communicate complete and accurate medication information to the next provider at discharge, including indications for new medications and reasons for any changes | |
| When possible, partner with clinical pharmacists to manage medication information and reconciliation, especially for high‐risk patients | |
| Self‐care responsibilities and social support | Use multidisciplinary discharge planning teams to assess the needs of patients and their families |
| Arrange a specific follow‐up appointment prior to discharge | |
| Contact patients by telephone a few days after discharge to assess questions, symptoms, and medication‐related issues | |
| Order home health services when indicated | |
| Consider home visits for frail elderly patients | |
| Ineffective physicianpatient communication | Focus discharge counseling on informing patients of major diagnoses, medication changes, dates of follow‐up appointments, self‐care instructions, and who to contact if problems develop |
| Ensure that staff members communicate consistent instructions | |
| For high‐volume conditions, consider using audiovisual recordings for discharge education, combined with an opportunity for additional counseling and questions | |
| Use trained interpreters when a language gap exists | |
| Provide simply written materials that include illustrations when possible to reinforce verbal instructions | |
| Ensure patients and family members comprehend key points by asking them to teach back the information in their own words and demonstrate any self‐care behaviors | |
| Encourage patients and family members to ask questions through an open‐ended invitation like, What questions do you have? instead of Do you have any questions? |
Because many patients follow up with their PCPs within a few days of discharge, it becomes important to provide the PCPs with some information about the hospitalization on the day of discharge. This can be accomplished via a quick telephone call, fax, or e‐mail update to the PCP.24, 35 Important things to include in this communiqu are the discharge diagnosis, medications, results of procedures, pending test results, follow‐up arrangements, and suggested next steps. Within 1 week, a detailed discharge summary should have been received.26, 33, 36 As electronic medical records become more widely available, computer‐generated summaries offer a way to more quickly and completely highlight the key elements of the hospitalization, and they are ready for delivery sooner than traditional dictated summaries.37 Additionally, all forms of discharge summariescomputer‐generated, handwritten, and dictatedshould include subheadings to better organize and present the information instead of unstructured narrative summaries.38
There is increasing interest in moving away from the traditional 1‐way transfer of information about a hospitalization toward a 2‐way dialogue between hospitalist and primary care physician.39 Preferences about how to do this will vary among physicians. One strategy might be to provide the PCP with the hospitalist's contact information and encouraging questions about the hospitalization. Another approach would involve contacting the PCP during the discharge planning process to exchange information about the patient, provide an opportunity for the PCP to ask questions about the hospitalization, and formulate a cohesive plan for follow‐up, particularly about contingency planning (ie, what is most likely to go wrong and what should be done about it) and specific follow‐up needs (ie, what tasks should be accomplished at the first postdischarge visit).
CHANGES AND DISCREPANCIES IN THE MEDICATION REGIMEN
Medication errors make up a large portion of the adverse events patients may experience in the period following hospital discharge.7 In fact, errors during the ordering of admission or discharge medications make up almost half of all hospital medication errors.4043 At transition points such as admission and discharge, errors are often associated with changes in the medication regimen, including discrepancies between the new set of medication orders and what the patient was taking previously. In 2 recent studies, 54% of patients experienced at least 1 unintended medication discrepancy on admission to the hospital, and 39%‐45% of these discrepancies were considered a potential threat to the patient.44, 45
At discharge, differences between the prescribed medication regimen and the prehospital regimen may exist for several reasons. First, physicians may not obtain a comprehensive and accurate medication history at the time of admission.46 The medication history elicited from the patient at hospital admission is often affected by health literacy, language barriers, current health status, medication‐history interviewing skills, and time constraints.47 Physicians may not consult other important sources of medication information, including family members, prescription lists or bottles, and community pharmacy records. The most common error in the admission medication history is omitting a medication taken at home.46 Additionally, several providers, including a physician, a nurse, and an inpatient pharmacist, may independently take medication histories for the same patient. These multiple accounts lead to discrepancies that are rarely recognized or corrected.
Second, a patient's medication regimen can be significantly altered several times during a hospitalization. Acute illness may cause physicians to hold certain medications, discontinue others, or change prescribed doses during hospitalization.48 In addition, at most hospitals closed drug formularies necessitate automatic substitution of 1 medication for another drug in the same class during the patient's hospital stay.49 Changes from long‐acting to short‐acting medications are also routinely made in the name of tighter control (eg, of blood pressure). One study of hospitalized elders found that 40% of all admission medications had been discontinued by discharge and that 45% of all discharge medications were newly started during the hospitalization.3
Finally, at discharge, the current medication regimen needs to be reconciled with the preadmission medication regimen in a thoughtful manner.2 This includes resuming medications held or modified at admission for clinical reasons, resuming medications that were substituted in the hospital for formulary or pharmacokinetic reasons, and stopping newly started medications that were only required during the hospitalization (eg, for prevention of venous thromboembolism or stress ulcers).50 It is difficult, even in hospitals with advanced electronic health information systems, to prompt physicians to make these necessary changes. In a recent study, unexplained discrepancies between the preadmission medication list and discharge medication orders were noted in 49% of hospital discharges.51 Errors in discharge medication reconciliation may subsequently increase the risk of postdischarge ADEs.51
Medication Reconciliation and Education
An optimal strategy for obtaining a complete medication history may include asking patients about the following: a typical day and what medications are taken at different times of day; whether prescriptions come from more than 1 doctor; medications not taken orally (eg, inhalers, patches); dosages and indications for all medications; length of therapy and timing of last dose; over‐the‐counter products, herbals, vitamins, and supplements used and vaccinations received; allergies; and number of doses missed in the last week (Table 1).5254 Forms are also available to help patients maintain a list of current medications.5557
Ideally, the process of obtaining a medication history involves integration of information from several sources, including patient and caregiver recollections, patient‐provided lists of medications, prescription bottles, outpatient medical records, and prescription refill information from community pharmacies.58, 59 Any discrepancies in the information obtained should be explicitly resolved with the patient and/or caregiver. Assistance from a pharmacist or the patient's PCP may also be required.
Once the preadmission medication regimen is confirmed, it should be entered on a standardized form and placed in a prominent place in the chart. This list should then be compared against the patient's medication orders at admission, throughout the hospital stay, and at discharge.12 The planned action for each of these medications (eg, continue at same dose/route/frequency, substitute) should be made explicit. At discharge, this preadmission list also needs to be compared with the current hospital medications in order to create a coherent set of discharge orders.
Staff responsibilities for obtaining and documenting an accurate list of preadmission medications and reconciling medications at admission, transfer, and discharge should be well defined and based on the resources available at each institution. Redundant work (eg, multiple personnel independently taking a medication history) should be replaced by interdisciplinary communication (ie, a member of the team confirming the accuracy of a list obtained by another member of the team). When discrepancies are found (eg, between preadmission and discharge medications), reconciliation requires correction of unintentional discrepancies and appropriate documentation of intentional changes.60
Because a patient's medications change frequently during the transitions of admission, intrahospital transfer, and discharge, reconciliation is an active and ongoing process that aims to ensure the patient is receiving the correct medication regimen at all times. Reconciliation also allows for a review of the safety and appropriateness of the regimen and discontinuation of any unsuitable or needless medications.61, 62
Finally, a comprehensive list of a patient's medications should be reported to the next service provider when the patient is referred or transferred to another setting, service, practitioner, or level of care within or outside the organization. Avoiding overarching orders such as continue home medications and resume all medications becomes crucial to patient safety during transitions in care. At discharge, physicians should provide patients with a complete list of medications to be taken at home with indications and instructions for administration written in everyday language. Physicians should also highlight the results of medication reconciliation by pointing out any changes from the preadmission regimen, especially medications that are at home but should no longer be taken.
Ultimately, physicians have the duty to ensure that correct and complete medication information is provided. However, to achieve optimal results, physicians should partner with clinical pharmacists when possible. Pharmacists have been formally educated about and are experienced at taking medication histories, which may make them the ideal individuals to interview newly admitted patients about their medication histories.63 Unfortunately, according to a recent survey, pharmacists perform admission drug histories in only 5% of U.S. hospitals and provide drug therapy counseling in just 49% of U.S. hospitals.64 Patients who are elderly, have limited literacy skills, take more than 5 medications daily, or take high‐risk medications such as insulin, warfarin, cardiovascular drugs (including antiarrhythmics), inhalers, antiseizure medications, eye medications, analgesics, oral hypoglycemics, oral methotrexate, and immunosuppressants may require additional counseling or pharmacist involvement for effective reconciliation.10, 65, 66
Although the evidence supporting medication reconciliation is limited, it is convincing enough to support carrying out such reconciliations. In 1 investigation, when the nursing staff obtained and pharmacists verified orders for home medications, the accuracy of admission medication orders increased from 40% to 95%.67 In another work, in which there was pharmacist‐led medication reconciliation, significant discrepancies were found in approximately 25% of patients' medication histories and admission orders.45 In the absence of pharmacist intervention, the authors predicted that 22% of the discrepancies could have caused some form of patient harm during hospitalization and that 59% of the discrepancies might have contributed to an adverse event if the error continued after discharge.45 Others report that orders were changed as a result of reconciliation for 94% of patients being transferred out of the intensive care unit.2 Finally, in a randomized controlled trial of a pharmacist intervention at discharge in which medication reconciliation was the most common action performed, after 30 days preventable ADEs were detected in 11% of control patients and 1% of intervention patients. Medication discrepancy was the cause of half the preventable ADEs in the control group.51
SELF‐CARE RESPONSIBILITIES AND SOCIAL SUPPORT
Compounding the difficulties at discharge are the economic pressures on our health care system, causing patients to be released from the hospital quicker and sicker than ever before.68 The scope of care provided to patients also undergoes a major shift at discharge. Multidisciplinary providers no longer continually review the health status and needs of patients; instead, patients must follow up with their outpatient physician over a period of days to weeks. In the interim, the patients themselves are responsible for administering new medications, participating in physical therapy, and tracking their own symptoms to see if they are worsening. For many patients, sufficient social and family support is not available to help perform these activities effectively. Unfortunately, hospital personnel often inaccurately assess patients' functional status and overestimate patients' knowledge of required self‐care activities.69
Providing Adequate Medical and Social Support
A multidisciplinary discharge planning team can facilitate proper assessments of the social needs of patients and their families (Table 1).7072 This team is often composed of a nurse case manager and a social worker but may also include a physical therapist, an occupational therapist, a pharmacist, and other health care providers. Following discussion with a patient and the patient's family, the team may suggest home health services during the transition home to supplement available medical support,73 or they may decide that discharge to a rehabilitation or skilled nursing facility is more appropriate.
In addition, follow‐up should be arranged prior to discharge. Patients who are given a set appointment are more likely to show up for their follow‐up visits than are those who are simply asked to call and arrange their own visits.74 Typically, follow‐up with the PCP should be conducted within 2 weeks of hospital discharge. However, depending on a patient's functional status, pending test results, and need for medication monitoring or follow‐up testing, this may need to take place sooner. Interestingly, research indicates that follow‐up appointments with the inpatient provider can result in a lower combined rate of readmission and 30‐day mortality.75 Thus, hospitalists may consider operating a hospitalist‐staffed follow‐up clinic, especially for patients without a regular PCP.
Telephone follow‐up conducted a few days after discharge can also be an effective means of bridging the inpatientoutpatient transition.35 Such follow‐up provides a chance to attend to any patient questions, new or concerning symptoms, and medication‐related issues (eg, not filling the discharge medications or difficulty comprehending the new medication regimen).76 A physician, physician assistant, advanced practice nurse, registered nurse, pharmacist, or care manager can effectively carry out this telephone follow‐up. No matter who telephones, the caller must be aware of the patient's recent course of events as well as the care plan decided at discharge. Published evidence indicates that telephone follow‐up fosters patient satisfaction, increases medication adherence, decreases preventable ADEs, and decreases the number of subsequent emergency room visits and hospital readmissions,51, 77, 78 although not all evaluations have demonstrated benefit.79 As with medication histories performed by pharmacists, limited resources may mean that such follow‐up be restricted to those patients at highest risk for readmission.
Home visits may be appropriate for certain patient populations, such as the frail elderly.80 Home visits enable a patient's daily needs and safety (eg, fall risk) to be assessed. They can also be a means of assessing medication safety and adherence by reviewing all prescription and over‐the‐counter products in the household.81 Close follow‐up of at‐risk or elderly patients after discharge can help to minimize hospital readmission and total health care costs.4, 8285
INEFFECTIVE PHYSICIANPATIENT COMMUNICATION
Physicianpatient communication is fundamental to the practice of medicine and is crucially important at discharge. However, several studies have demonstrated a disconnect between physician information giving and patient understanding.76, 9690 When providing instructions, physicians commonly use medical jargon and attempt to cover a wealth of information in a limited amount of time.69, 87 They also tend to rely on verbal instructions and fail to provide supplementary audiovisual materials (eg, educational handouts or videos) that could aid patient comprehension. Physicians may not point out important self‐care tasks that patients should carry out at home. The entire interaction may be rushed or seem rushed. Moreover, when physicians solicit questions from patients, they may only allow for yes/no responses by using statements like Any questions? or Do you have any questions? that make it easy for patients to simply respond, No. The encounter usually comes to an end without true confirmation of a patient's level of understanding or assessment of a patient's ability to perform the self‐care activities and medication management required on returning home.81
Adding to the challenges of effective physicianpatient communication is the large number of adult Americans (more than 90 million) who have limited functional literacy skills.91, 92 Such patients typically have difficulty reading and understanding medical instructions, medication labels, and appointment slips.9396 Not surprisingly, patients with limited literacy skills know less about their chronic illnesses and how to manage their diseases.97 Having low literacy is also linked to increased use of emergency department services, a higher risk of hospitalization, and higher health care costs.9799 Patients with limited English proficiency have similar or even greater challenges and also have longer stays in the hospital.100
More Effective PhysicianPatient Communication
Discharge counseling should concentrate on the few key points that are of the greatest interest and the most importance to patients: major diagnoses, medication changes, dates of follow‐up appointments, self‐care instructions, and who to contact if problems develop (Table 1).101 Furthermore, these key instructions should be reinforced by other hospital staff, including nurses and pharmacists. For common conditions (eg, high‐volume cardiac procedures), offering standardized audiovisual instructions can be both efficient and worthwhile if used in conjunction with questionanswer sessions.102 In the event that physicians and hospital staff cannot fluently communicate in a patient's language, it is essential to engage trained interpreters, not rely on rudimentary language skills, the patient's family, or other ad hoc ways to communicate.103
Because patients are unlikely to fully remember verbal instructions at discharge, it is helpful to provide patients and family members with written materials to take home in order to reinforce important self‐care instructions.76, 87 These materials, written at a 5th‐ to 8th‐grade reading level, should outline key information in a simple format with little or no medical jargon. Illustrated materials are often better comprehended and subsequently remembered by patients.104, 105 If preprinted illustrated materials are not on hand, then physicians can convey key points by drawing simple pictures.
Confirming patient comprehension with the teach‐back method is perhaps the most important step in effectively communicating discharge instructions.106 With this method, patients are asked to repeat back what they understand from the discharge instructions. Application of this simple technique is advocated as one of the most effective means of improving patient safety.107, 108 Patients should also be asked to demonstrate any new self‐care tasks that they will be required to carry out at home, such as using an inhaler or administering a subcutaneous injection.
Last, The Joint Commission recently created a National Patent Safety Goal to encourage the active involvement of patients and their families in the patient's own care.12 This charge requires that physicians offer ample time for patients and their family members to ask questions. Physicians should avoid questions with yes/no responses and instead invite patient and family member questions in a more open‐ended manner (eg, What questions do you have?) to help ensure comprehension and comfort with the care plan.
CONCLUSIONS
The transition from hospital to home is a vulnerable period of discontinuity and potential adverse events. Hospitalists and other inpatient providers should not view discharge as an end to their obligation to patients but rather should attempt to promote a safe and efficient transition of care. Hospitalists can play an important role in bridging the gap between inpatient and outpatient care through appropriate discharge planning and effective communication with patients, their family members, and outpatient physicians.
Acknowledgements
The authors thank Marra Katz for her editorial assistance in the preparation of this manuscript
As the counterpart to hospital admission, hospital discharge is a necessary process experienced by each living patient. For all patients except those being transferred to a continuing care facility, discharge is a period of transition from hospital to home that involves a transfer in responsibility from the inpatient provider or hospitalist to the patient and primary care physician (PCP).1 Prescription medications are commonly altered at this transition point, with patients asked to discontinue some medications, switch to a new dosage schedule of others, or begin new treatments.2, 3 Self‐care responsibilities also increase in number and importance, presenting new challenges for patients and their families as they return home.4 Under these circumstances, ineffective planning and coordination of care can undermine patient satisfaction, facilitate adverse events, and contribute to more frequent hospital readmissions.58
Following hospital discharge nearly half (49%) of hospitalized patients experience at least 1 medical error in medication continuity, diagnostic workup, or test follow‐up.7 It has been reported that 19%23% of patients suffer an adverse event, most frequently an adverse drug event (ADE).911 Half of ADEs are considered preventable or ameliorable (ie, their severity or duration could have been decreased). Most errors and adverse events in this setting result from a breakdown in communication between the hospital team and the patient or primary care physician.10
To promote more effective care transitions, The Joint Commission now requires accredited facilities to accurately and completely reconcile medications across the continuum of care.12 The Society of Hospital Medicine recently published recommendations for the discharge of elderly patients.13 The joint Society of Hospital MedicineSociety of General Internal Medicine Continuity of Care Task Force also recently published a systematic review with recommendations for improving the handoff of patient information at discharge.14 Apart from these reports, however, it is uncommon to find evidence‐based recommendations for hospital discharge applicable to a broad range of patients.15 This review highlights several important challenges for physicians who seek to provide high‐quality care during hospital discharge and the subsequent period of transition. Based on the best available evidence, recommendations are also provided for how to improve communication and facilitate the care transition for adult inpatients returning home.
INPATIENTOUTPATIENT PHYSICIAN DISCONTINUITY
Traditionally, primary care physicians have admitted their own patients, provided hospital care (in addition to seeing outpatients during the day), and followed patients after discharge. Under this model, continuity of care has been preserved; however, this method of care has faltered under the weight of inpatients and outpatients with more severe illnesses, rapid technological advancements, managed care pressuring outpatient physicians to see more patients, and a thrust toward reduced hospital costs and length of stay.16 Increases in the efficiency and quality of hospital care have accompanied a new reliance on the field of hospital medicine, while allowing PCPs to focus on outpatient care.1719 With more than 14,000 hospitalists currently practicing in the United States and 25,000 anticipated to be practicing by 2010, transfer of care from hospital‐based providers to PCPs has become increasingly common at discharge.20
Patient discharge summaries are the most common means of communication between inpatient and outpatient providers. However, numerous studies have shown that discharge summaries often fail to provide important administrative and medical information, such as the primary diagnosis, results of abnormal diagnostics, details about the hospital course, follow‐up plans, whether laboratory test results are pending, and patient or family counseling.14 Summaries also may not arrive in a timely manner and sometimes may not reach the PCP at all.2123
At the time patients first follow up with their PCPs after hospitalization, discharge summaries have not yet arrived about 75% of the time,22, 24, 25 restricting the PCPs' ability to provide adequate follow‐up care in 24% of hospital follow‐up visits, according to one study.26 In another investigation, PCPs reported being unaware of 62% of the pending test results that returned after discharge, of which 37% were considered actionable.27
Improving Physician Information Transfer and Continuity
To improve information transfer from hospitalist to PCP, attention must be paid to the content, format, and timely delivery of discharge information (Table 1).14 Surveys of primary care physicians suggest the following information should be included in discharge summaries: diagnoses, abnormal physical findings, important test results, discharge medications, follow‐up arrangements made and appointments that still need to be made, counseling provided to the patient and family, and tests still pending at discharge.24, 2833 These domains are consistent with Joint Commission guidelines for discharge summaries,34 and the inclusion of a detailed medication list and pending test results also has implications for patient safety.911, 27
| Challenge | Recommended approaches |
|---|---|
| Inpatientoutpatient physician discontinuity | When possible, involve the primary care physician (PCP) in discharge planning and work together to develop a follow‐up plan |
| At minimum, communicate the following to the PCP on the day of discharge: diagnoses, medications, results of procedures, pending tests, follow‐up arrangements, and suggested next steps | |
| Provide the PCP with a detailed discharge summary within 1 week | |
| In discharge summaries include: diagnoses, abnormal physical findings, important test results, discharge medications with rationale for new or changed medications, follow‐up arrangements made, counseling provided to the patient and family, and tasks to be completed (eg, appointments that still need to be made and tests that require follow‐up) | |
| Follow a structured template with subheadings in discharge communications | |
| When possible, use health information technology to create and disseminate discharge summaries | |
| Changes and discrepancies in medication regimen | Obtain a complete medication history by asking patients about: medications taken at different times of day; medications prescribed by different physicians; nonoral medications; over‐the‐counter products; dosage, indication, length of therapy, and timing of last dose of all drugs; allergies; and adherence |
| Compare and reconcile medication information obtained from patient and caregiver reports, patient lists, prescription bottles, medical records, and pharmacy records | |
| Display preadmission medication list prominently in the chart | |
| Reconcile medications at all care transitions, including admission, intrahospital transfer, and discharge | |
| Communicate complete and accurate medication information to the next provider at discharge, including indications for new medications and reasons for any changes | |
| When possible, partner with clinical pharmacists to manage medication information and reconciliation, especially for high‐risk patients | |
| Self‐care responsibilities and social support | Use multidisciplinary discharge planning teams to assess the needs of patients and their families |
| Arrange a specific follow‐up appointment prior to discharge | |
| Contact patients by telephone a few days after discharge to assess questions, symptoms, and medication‐related issues | |
| Order home health services when indicated | |
| Consider home visits for frail elderly patients | |
| Ineffective physicianpatient communication | Focus discharge counseling on informing patients of major diagnoses, medication changes, dates of follow‐up appointments, self‐care instructions, and who to contact if problems develop |
| Ensure that staff members communicate consistent instructions | |
| For high‐volume conditions, consider using audiovisual recordings for discharge education, combined with an opportunity for additional counseling and questions | |
| Use trained interpreters when a language gap exists | |
| Provide simply written materials that include illustrations when possible to reinforce verbal instructions | |
| Ensure patients and family members comprehend key points by asking them to teach back the information in their own words and demonstrate any self‐care behaviors | |
| Encourage patients and family members to ask questions through an open‐ended invitation like, What questions do you have? instead of Do you have any questions? |
Because many patients follow up with their PCPs within a few days of discharge, it becomes important to provide the PCPs with some information about the hospitalization on the day of discharge. This can be accomplished via a quick telephone call, fax, or e‐mail update to the PCP.24, 35 Important things to include in this communiqu are the discharge diagnosis, medications, results of procedures, pending test results, follow‐up arrangements, and suggested next steps. Within 1 week, a detailed discharge summary should have been received.26, 33, 36 As electronic medical records become more widely available, computer‐generated summaries offer a way to more quickly and completely highlight the key elements of the hospitalization, and they are ready for delivery sooner than traditional dictated summaries.37 Additionally, all forms of discharge summariescomputer‐generated, handwritten, and dictatedshould include subheadings to better organize and present the information instead of unstructured narrative summaries.38
There is increasing interest in moving away from the traditional 1‐way transfer of information about a hospitalization toward a 2‐way dialogue between hospitalist and primary care physician.39 Preferences about how to do this will vary among physicians. One strategy might be to provide the PCP with the hospitalist's contact information and encouraging questions about the hospitalization. Another approach would involve contacting the PCP during the discharge planning process to exchange information about the patient, provide an opportunity for the PCP to ask questions about the hospitalization, and formulate a cohesive plan for follow‐up, particularly about contingency planning (ie, what is most likely to go wrong and what should be done about it) and specific follow‐up needs (ie, what tasks should be accomplished at the first postdischarge visit).
CHANGES AND DISCREPANCIES IN THE MEDICATION REGIMEN
Medication errors make up a large portion of the adverse events patients may experience in the period following hospital discharge.7 In fact, errors during the ordering of admission or discharge medications make up almost half of all hospital medication errors.4043 At transition points such as admission and discharge, errors are often associated with changes in the medication regimen, including discrepancies between the new set of medication orders and what the patient was taking previously. In 2 recent studies, 54% of patients experienced at least 1 unintended medication discrepancy on admission to the hospital, and 39%‐45% of these discrepancies were considered a potential threat to the patient.44, 45
At discharge, differences between the prescribed medication regimen and the prehospital regimen may exist for several reasons. First, physicians may not obtain a comprehensive and accurate medication history at the time of admission.46 The medication history elicited from the patient at hospital admission is often affected by health literacy, language barriers, current health status, medication‐history interviewing skills, and time constraints.47 Physicians may not consult other important sources of medication information, including family members, prescription lists or bottles, and community pharmacy records. The most common error in the admission medication history is omitting a medication taken at home.46 Additionally, several providers, including a physician, a nurse, and an inpatient pharmacist, may independently take medication histories for the same patient. These multiple accounts lead to discrepancies that are rarely recognized or corrected.
Second, a patient's medication regimen can be significantly altered several times during a hospitalization. Acute illness may cause physicians to hold certain medications, discontinue others, or change prescribed doses during hospitalization.48 In addition, at most hospitals closed drug formularies necessitate automatic substitution of 1 medication for another drug in the same class during the patient's hospital stay.49 Changes from long‐acting to short‐acting medications are also routinely made in the name of tighter control (eg, of blood pressure). One study of hospitalized elders found that 40% of all admission medications had been discontinued by discharge and that 45% of all discharge medications were newly started during the hospitalization.3
Finally, at discharge, the current medication regimen needs to be reconciled with the preadmission medication regimen in a thoughtful manner.2 This includes resuming medications held or modified at admission for clinical reasons, resuming medications that were substituted in the hospital for formulary or pharmacokinetic reasons, and stopping newly started medications that were only required during the hospitalization (eg, for prevention of venous thromboembolism or stress ulcers).50 It is difficult, even in hospitals with advanced electronic health information systems, to prompt physicians to make these necessary changes. In a recent study, unexplained discrepancies between the preadmission medication list and discharge medication orders were noted in 49% of hospital discharges.51 Errors in discharge medication reconciliation may subsequently increase the risk of postdischarge ADEs.51
Medication Reconciliation and Education
An optimal strategy for obtaining a complete medication history may include asking patients about the following: a typical day and what medications are taken at different times of day; whether prescriptions come from more than 1 doctor; medications not taken orally (eg, inhalers, patches); dosages and indications for all medications; length of therapy and timing of last dose; over‐the‐counter products, herbals, vitamins, and supplements used and vaccinations received; allergies; and number of doses missed in the last week (Table 1).5254 Forms are also available to help patients maintain a list of current medications.5557
Ideally, the process of obtaining a medication history involves integration of information from several sources, including patient and caregiver recollections, patient‐provided lists of medications, prescription bottles, outpatient medical records, and prescription refill information from community pharmacies.58, 59 Any discrepancies in the information obtained should be explicitly resolved with the patient and/or caregiver. Assistance from a pharmacist or the patient's PCP may also be required.
Once the preadmission medication regimen is confirmed, it should be entered on a standardized form and placed in a prominent place in the chart. This list should then be compared against the patient's medication orders at admission, throughout the hospital stay, and at discharge.12 The planned action for each of these medications (eg, continue at same dose/route/frequency, substitute) should be made explicit. At discharge, this preadmission list also needs to be compared with the current hospital medications in order to create a coherent set of discharge orders.
Staff responsibilities for obtaining and documenting an accurate list of preadmission medications and reconciling medications at admission, transfer, and discharge should be well defined and based on the resources available at each institution. Redundant work (eg, multiple personnel independently taking a medication history) should be replaced by interdisciplinary communication (ie, a member of the team confirming the accuracy of a list obtained by another member of the team). When discrepancies are found (eg, between preadmission and discharge medications), reconciliation requires correction of unintentional discrepancies and appropriate documentation of intentional changes.60
Because a patient's medications change frequently during the transitions of admission, intrahospital transfer, and discharge, reconciliation is an active and ongoing process that aims to ensure the patient is receiving the correct medication regimen at all times. Reconciliation also allows for a review of the safety and appropriateness of the regimen and discontinuation of any unsuitable or needless medications.61, 62
Finally, a comprehensive list of a patient's medications should be reported to the next service provider when the patient is referred or transferred to another setting, service, practitioner, or level of care within or outside the organization. Avoiding overarching orders such as continue home medications and resume all medications becomes crucial to patient safety during transitions in care. At discharge, physicians should provide patients with a complete list of medications to be taken at home with indications and instructions for administration written in everyday language. Physicians should also highlight the results of medication reconciliation by pointing out any changes from the preadmission regimen, especially medications that are at home but should no longer be taken.
Ultimately, physicians have the duty to ensure that correct and complete medication information is provided. However, to achieve optimal results, physicians should partner with clinical pharmacists when possible. Pharmacists have been formally educated about and are experienced at taking medication histories, which may make them the ideal individuals to interview newly admitted patients about their medication histories.63 Unfortunately, according to a recent survey, pharmacists perform admission drug histories in only 5% of U.S. hospitals and provide drug therapy counseling in just 49% of U.S. hospitals.64 Patients who are elderly, have limited literacy skills, take more than 5 medications daily, or take high‐risk medications such as insulin, warfarin, cardiovascular drugs (including antiarrhythmics), inhalers, antiseizure medications, eye medications, analgesics, oral hypoglycemics, oral methotrexate, and immunosuppressants may require additional counseling or pharmacist involvement for effective reconciliation.10, 65, 66
Although the evidence supporting medication reconciliation is limited, it is convincing enough to support carrying out such reconciliations. In 1 investigation, when the nursing staff obtained and pharmacists verified orders for home medications, the accuracy of admission medication orders increased from 40% to 95%.67 In another work, in which there was pharmacist‐led medication reconciliation, significant discrepancies were found in approximately 25% of patients' medication histories and admission orders.45 In the absence of pharmacist intervention, the authors predicted that 22% of the discrepancies could have caused some form of patient harm during hospitalization and that 59% of the discrepancies might have contributed to an adverse event if the error continued after discharge.45 Others report that orders were changed as a result of reconciliation for 94% of patients being transferred out of the intensive care unit.2 Finally, in a randomized controlled trial of a pharmacist intervention at discharge in which medication reconciliation was the most common action performed, after 30 days preventable ADEs were detected in 11% of control patients and 1% of intervention patients. Medication discrepancy was the cause of half the preventable ADEs in the control group.51
SELF‐CARE RESPONSIBILITIES AND SOCIAL SUPPORT
Compounding the difficulties at discharge are the economic pressures on our health care system, causing patients to be released from the hospital quicker and sicker than ever before.68 The scope of care provided to patients also undergoes a major shift at discharge. Multidisciplinary providers no longer continually review the health status and needs of patients; instead, patients must follow up with their outpatient physician over a period of days to weeks. In the interim, the patients themselves are responsible for administering new medications, participating in physical therapy, and tracking their own symptoms to see if they are worsening. For many patients, sufficient social and family support is not available to help perform these activities effectively. Unfortunately, hospital personnel often inaccurately assess patients' functional status and overestimate patients' knowledge of required self‐care activities.69
Providing Adequate Medical and Social Support
A multidisciplinary discharge planning team can facilitate proper assessments of the social needs of patients and their families (Table 1).7072 This team is often composed of a nurse case manager and a social worker but may also include a physical therapist, an occupational therapist, a pharmacist, and other health care providers. Following discussion with a patient and the patient's family, the team may suggest home health services during the transition home to supplement available medical support,73 or they may decide that discharge to a rehabilitation or skilled nursing facility is more appropriate.
In addition, follow‐up should be arranged prior to discharge. Patients who are given a set appointment are more likely to show up for their follow‐up visits than are those who are simply asked to call and arrange their own visits.74 Typically, follow‐up with the PCP should be conducted within 2 weeks of hospital discharge. However, depending on a patient's functional status, pending test results, and need for medication monitoring or follow‐up testing, this may need to take place sooner. Interestingly, research indicates that follow‐up appointments with the inpatient provider can result in a lower combined rate of readmission and 30‐day mortality.75 Thus, hospitalists may consider operating a hospitalist‐staffed follow‐up clinic, especially for patients without a regular PCP.
Telephone follow‐up conducted a few days after discharge can also be an effective means of bridging the inpatientoutpatient transition.35 Such follow‐up provides a chance to attend to any patient questions, new or concerning symptoms, and medication‐related issues (eg, not filling the discharge medications or difficulty comprehending the new medication regimen).76 A physician, physician assistant, advanced practice nurse, registered nurse, pharmacist, or care manager can effectively carry out this telephone follow‐up. No matter who telephones, the caller must be aware of the patient's recent course of events as well as the care plan decided at discharge. Published evidence indicates that telephone follow‐up fosters patient satisfaction, increases medication adherence, decreases preventable ADEs, and decreases the number of subsequent emergency room visits and hospital readmissions,51, 77, 78 although not all evaluations have demonstrated benefit.79 As with medication histories performed by pharmacists, limited resources may mean that such follow‐up be restricted to those patients at highest risk for readmission.
Home visits may be appropriate for certain patient populations, such as the frail elderly.80 Home visits enable a patient's daily needs and safety (eg, fall risk) to be assessed. They can also be a means of assessing medication safety and adherence by reviewing all prescription and over‐the‐counter products in the household.81 Close follow‐up of at‐risk or elderly patients after discharge can help to minimize hospital readmission and total health care costs.4, 8285
INEFFECTIVE PHYSICIANPATIENT COMMUNICATION
Physicianpatient communication is fundamental to the practice of medicine and is crucially important at discharge. However, several studies have demonstrated a disconnect between physician information giving and patient understanding.76, 9690 When providing instructions, physicians commonly use medical jargon and attempt to cover a wealth of information in a limited amount of time.69, 87 They also tend to rely on verbal instructions and fail to provide supplementary audiovisual materials (eg, educational handouts or videos) that could aid patient comprehension. Physicians may not point out important self‐care tasks that patients should carry out at home. The entire interaction may be rushed or seem rushed. Moreover, when physicians solicit questions from patients, they may only allow for yes/no responses by using statements like Any questions? or Do you have any questions? that make it easy for patients to simply respond, No. The encounter usually comes to an end without true confirmation of a patient's level of understanding or assessment of a patient's ability to perform the self‐care activities and medication management required on returning home.81
Adding to the challenges of effective physicianpatient communication is the large number of adult Americans (more than 90 million) who have limited functional literacy skills.91, 92 Such patients typically have difficulty reading and understanding medical instructions, medication labels, and appointment slips.9396 Not surprisingly, patients with limited literacy skills know less about their chronic illnesses and how to manage their diseases.97 Having low literacy is also linked to increased use of emergency department services, a higher risk of hospitalization, and higher health care costs.9799 Patients with limited English proficiency have similar or even greater challenges and also have longer stays in the hospital.100
More Effective PhysicianPatient Communication
Discharge counseling should concentrate on the few key points that are of the greatest interest and the most importance to patients: major diagnoses, medication changes, dates of follow‐up appointments, self‐care instructions, and who to contact if problems develop (Table 1).101 Furthermore, these key instructions should be reinforced by other hospital staff, including nurses and pharmacists. For common conditions (eg, high‐volume cardiac procedures), offering standardized audiovisual instructions can be both efficient and worthwhile if used in conjunction with questionanswer sessions.102 In the event that physicians and hospital staff cannot fluently communicate in a patient's language, it is essential to engage trained interpreters, not rely on rudimentary language skills, the patient's family, or other ad hoc ways to communicate.103
Because patients are unlikely to fully remember verbal instructions at discharge, it is helpful to provide patients and family members with written materials to take home in order to reinforce important self‐care instructions.76, 87 These materials, written at a 5th‐ to 8th‐grade reading level, should outline key information in a simple format with little or no medical jargon. Illustrated materials are often better comprehended and subsequently remembered by patients.104, 105 If preprinted illustrated materials are not on hand, then physicians can convey key points by drawing simple pictures.
Confirming patient comprehension with the teach‐back method is perhaps the most important step in effectively communicating discharge instructions.106 With this method, patients are asked to repeat back what they understand from the discharge instructions. Application of this simple technique is advocated as one of the most effective means of improving patient safety.107, 108 Patients should also be asked to demonstrate any new self‐care tasks that they will be required to carry out at home, such as using an inhaler or administering a subcutaneous injection.
Last, The Joint Commission recently created a National Patent Safety Goal to encourage the active involvement of patients and their families in the patient's own care.12 This charge requires that physicians offer ample time for patients and their family members to ask questions. Physicians should avoid questions with yes/no responses and instead invite patient and family member questions in a more open‐ended manner (eg, What questions do you have?) to help ensure comprehension and comfort with the care plan.
CONCLUSIONS
The transition from hospital to home is a vulnerable period of discontinuity and potential adverse events. Hospitalists and other inpatient providers should not view discharge as an end to their obligation to patients but rather should attempt to promote a safe and efficient transition of care. Hospitalists can play an important role in bridging the gap between inpatient and outpatient care through appropriate discharge planning and effective communication with patients, their family members, and outpatient physicians.
Acknowledgements
The authors thank Marra Katz for her editorial assistance in the preparation of this manuscript
- .Whither continuity of care?N Engl J Med.1999;340:1362–1363.
- ,,, et al.Medication reconciliation: a practical tool to reduce the risk of medication errors.J Crit Care.2003;18(4):201–205.
- ,,,.Influence of hospitalization on drug therapy in the elderly.J Am Geriatr Soc.1989;37:679–683.
- ,,,,,.Preparing patients and caregivers to participate in care delivered across settings: the Care Transitions Intervention.J Am Geriatr Soc.2004;52:1817–1825.
- ,,.Predictors of elder and family caregiver satisfaction with discharge planning.J Cardiovasc Nurs.2000;14(3):76–87.
- ,.Discharge planning and continuity of care for aged people: indicators of satisfaction and implications for practice.Aust J Adv Nurs.1998;16(1):7–13.
- ,,,.Medical errors related to discontinuity of care from an inpatient to an outpatient setting.J Gen Intern Med.2003;18:646–651.
- ,,.Assessing the quality of preparation for posthospital care from the patient's perspective: the care transitions measure.Med Care.2005;43(3):246–255.
- ,,, et al.Adverse events among medical patients after discharge from hospital.CMAJ.2004;170:345–349.
- ,,,,.The incidence and severity of adverse events affecting patients after discharge from the hospital.Ann Intern Med.2003;138:161–167.
- ,,,,.Adverse drug events occurring following hospital discharge.J Gen Intern Med.2005;20:317–323.
- The Joint Commission. Joint Commission National Patient Safety Goals. Available at: http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/. Accessed July 17,2006.
- ,,, et al.Transition of care for hospitalized elderly patients ‐ Development of a discharge checklist for hospitalists.J Hosp Med.2006;1:354–360.
- ,,,,,.Deficits in communication and information transfer between hospital‐based and primary care physicians: implications for patient safety and continuity of care.JAMA.2007;297:831–841.
- Agency for Healthcare Research and Quality. National Guideline Clearinghouse. Available at: http://www.guideline.gov. Accessed January 3,2007.
- ,.The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335:514–517.
- .Hospitalists in the United States—mission accomplished or work in progress?N Engl J Med.2004;350:1935–1936.
- .The evolution of the hospitalist model in the United States.Med Clin North Am2002;86(4):687–706.
- ,.The hospitalist movement 5 years later.JAMA.2002;287:487–494.
- Society of Hospital Medicine. Growth of hospital medicine nationwide. Available at: http://www.hospitalmedicine.org/Content/NavigationMenu/Media/GrowthofHospitalMedicineNationwide/Growth_of_Hospital_M.htm. Accessed July 17,2006.
- ,,,,.Quality assessment of discharge letters in a French university hospital.Int J Health Care Qual Assur Inc Leadersh Health Serv.1998;11(2‐3):90–95.
- ,,.Dissemination of discharge summaries. Not reaching follow‐up physicians.Can Fam Physician.2002;48:737–742.
- ,.Quality assessment of a discharge summary system.CMAJ.1995;152:1437–1442.
- ,,,.Primary care physician attitudes regarding communication with hospitalists.Am J Med.2001;111(9B):15S–20S.
- ,,,.Effect of discharge summary availability during post‐discharge visits on hospital readmission.J Gen Intern Med.2002;17(3):186–192.
- .Study of discharge communications from hospital doctors to an inner London general practice.J R Coll Gen Pract.1987;37:494–495.
- ,,, et al.Patient safety concerns arising from test results that return after hospital discharge.Ann Intern Med.2005;143(2):121–128.
- ,,.Communication between general practitioners and consultants: what should their letters contain?BMJ1992;304(6830):821–824.
- ,,,.Written communication from specialists to general practitioners in cancer care. What are the expectations and how are they met?Scand J Prim Health Care.1998;16(3):154–159.
- ,.Improving the continuity of care between general practitioners and public hospitals.Med J Aust.1994;161:656–659.
- ,.Towards better discharge summaries: brevity and structure.West Engl Med J.1991;106(2):40–41,55.
- ,,.Content of a discharge summary from a medical ward: views of general practitioners and hospital doctors.J R Coll Physicians Lond.1995;29:307–310.
- ,.What is necessary for high‐quality discharge summaries?Am J Med Qual.1999;14(4):160–169.
- The Joint Commission.Standard IM.6.10. Hospital Accreditation Standards.Oakbrook Terrace, IL:The Joint Commission;2006:338–340.
- .The importance of postdischarge telephone follow‐up for hospitalists: a view from the trenches.Am J Med.2001;111(9B):43S–44S.
- ,,,.The quality of communication between hospitals and general practitioners: an assessment.J Qual Clin Pract.1998;18:241–247.
- ,,,.Dictated versus database‐generated discharge summaries: a randomized clinical trial.CMAJ.1999;160:319–326.
- ,,,.Standardized or narrative discharge summaries. Which do family physicians prefer?Can Fam Physician.1998;44:62–69.
- ,.Moving from information transfer to information exchange in health and health care.Soc Sci Med.2003;56:449–464.
- ,,, et al.The costs of adverse drug events in hospitalized patients.Adverse Drug Events Prevention Study Group.JAMA.1997;277:307–311.
- ,,, et al.Systems analysis of adverse drug events.ADE Prevention Study Group.JAMA.1995;274(1):35–43.
- ,,, et al.Incidence of adverse drug events and potential adverse drug events. Implications for prevention.ADE Prevention Study Group.JAMA.1995;274(1):29–34.
- ,.Medication errors in hospitalized cardiovascular patients.Arch Intern Med.2003;163:1461–1466.
- ,,, et al.Unintended medication discrepancies at the time of hospital admission.Arch Intern Med.2005;165:424–429.
- ,,,,,.Reconciliation of discrepancies in medication histories and admission orders of newly hospitalized patients.Am J Health Syst Pharm.2004;61:1689–1695.
- ,,,,,.Frequency, type and clinical importance of medication history errors at admission to hospital: a systematic review.CMAJ.2005;173:510–515.
- ,,,,.Medication reconciliation in the acute care setting: opportunity and challenge for nursing.J Nurs Care Qual.2005;20(2):95–98.
- ,,.The adverse effects of hospitalization on drug regimens.Arch Intern Med.1991;151:1562–1564.
- ,,,,.Prevalence and cost savings of therapeutic interchange among U.S. hospitals.Am J Health Syst Pharm.2002;59:529–533.
- ,,, et al.Medication reconciliation: are we meeting the requirements?JCOM.2006;13:441–444.
- ,,, et al.Role of pharmacist counseling in preventing adverse drug events after hospitalization.Arch Intern Med.2006;166:565–571.
- ,.Effectiveness of a pharmacist‐acquired medication history in promoting patient safety.Am J Health Syst Pharm.2002;59:2221–2225.
- .Ensuring continuity of care and accuracy of patients' medication history on hospital admission.Am J Health Syst Pharm.2002;59:1054–1055.
- ,,,.Current methods used to teach the medication history interview to doctor of pharmacy students.Am J Pharm Educ.2002;66(Summer):103–107.
- AARP. My Personal Medication Record. Available at: http://assets.aarp.org/www.aarp.org_/articles/learntech/wellbeing/medication‐record.pdf. Accessed October 20,2006.
- AARP. Mi registro de medicacion. Available at: http://assets.aarp.org/www.aarp.org_/articles/health/docs/PersonalMedRecordSP.pdf. Accessed October 20,2006.
- Institute for Safe Medication Practices. Available at: http://www.ismp.org. Accessed September 8,2006.
- ,,.Parents as partners in obtaining the medication history.J Am Med Inform Assoc.2005;12:299–305.
- ,,.Medication history on internal medicine wards: assessment of extra information collected from second drug interviews and GP lists.Pharmacoepidemiology Drug Saf.2003;12:491–498.
- Medication Discrepancy Tool. Available at: http://www.caretransitions.org. Accessed July 28,2005.
- ,,,,,.Updating the Beers criteria for potentially inappropriate medication use in older adults: results of a US consensus panel of experts.Arch Intern Med.2003;163:2716–2724.
- .Using the NO TEARS tool for medication review.BMJ2004;329(7463):434.
- ,,,.Clinical pharmacists and inpatient medical care: a systematic review.Arch Intern Med.2006;166:955–964.
- ,.Clinical pharmacy services, pharmacy staffing, and adverse drug reactions in United States hospitals.Pharmacotherapy.2006;26:735–747.
- ,,, et al.Adverse drug events in ambulatory care.N Engl J Med.2003;348:1556–1564.
- MA Coalition for the Prevention of Medical Errors. Reconciling medications. Recommended practices. Available at: http://www.macoalition.org/documents/RecMedPractices.pdf. Accessed July 27,2005.
- ,.OSF healthcare's journey in patient safety.Qual Manag Health Care.2004;13(1):53–59.
- ,,, et al.Prospective payment system and impairment at discharge. The ‘quicker‐and‐sicker’ story revisited.JAMA.1990;264:1980–1983.
- ,,,,,.Discharge planning: comparison of patients and nurses' perceptions of patients following hospital discharge.Image J Nurs Sch.1996;28(2):143–147.
- ,,,.The Care Transitions Intervention: results of a randomized controlled trial.Arch Intern Med.2006;166:1822–1828.
- ,,,,,.Comprehensive discharge planning with postdischarge support for older patients with congestive heart failure: a meta‐analysis.JAMA.2004;291:1358–1367.
- ,,,.Discharge planning from hospital to home.Cochrane Database Syst Rev.2006;4.
- .Falling through the cracks: challenges and opportunities for improving transitional care for persons with continuous complex care needs.J Am Geriatr Soc.2003;51:549–555.
- .The best way to improve emergency department follow‐up is actually to give the patient a specific appointment.J Gen Intern Med.2006;21:398; author reply398.
- ,,,.Continuity of care and patient outcomes after hospital discharge.J Gen Intern Med.2004;19:624–631.
- ,.Patients' understanding of their treatment plans and diagnosis at discharge.Mayo Clin Proc.2005;80:991–994.
- ,,,.The impact of follow‐up telephone calls to patients after hospitalization.Am J Med.2001;111(9B):26S–30S.
- ,.The impact of clinical pharmacists' consultations on geriatric patients' compliance and medical care use: a randomized controlled trial.Gerontologist.1994;34:307–315.
- ,.Telephone follow‐up, initiated by a hospital‐based health professional, for postdischarge problems in patients discharged from hospital to home.Cochrane Database Syst Rev.2007;1.
- ,,, et al.Geriatric home assessment after hospital discharge.J Am Geriatr Soc.1994;42:1229–1234.
- ,.Uncovering a multitude of sins: medication management in the home post acute hospitalisation among the chronically ill.Aust N Z J Med.1999;29(2):220–227.
- ,,, et al.Comprehensive discharge planning and home follow‐up of hospitalized elders: a randomized clinical trial.JAMA.1999;281:613–620.
- ,,,.The cost‐effectiveness of intensive postdischarge care. A randomized trial.Med Care.1988;26:1092–1102.
- ,,,,.The effects of aftercare on chronic patients and frail elderly patients when discharged from hospital: a systematic review.J Adv Nurs.1998;27:1076–1086.
- ,,,,,.A multidisciplinary intervention to prevent the readmission of elderly patients with congestive heart failure.N Engl J Med.1995;333:1190–1195.
- ,,.Medication education of acutely hospitalized older patients.J Gen Intern Med.1999;14:610–616.
- ,,, et al.Patient‐physician communication at hospital discharge and patients' understanding of the postdischarge treatment plan.Arch Intern Med.1997;157:1026–1030.
- ,,.Patient understanding of commonly used medical vocabulary.J Fam Pract.1987;25:176–178.
- .The understanding of medical terminology used in printed health education materials.Heal Educ J.1979;38:111–121.
- ,,,,.The gap between patient reading comprehension and the readability of patient education materials.J Fam Pract.1990;31:533–538.
- ,,. National Assessment of Adult Literacy (NAAL). A first look at the literacy of America's adults in the 21st century. Available at: http://nces.ed.gov/naal. Accessed May 2,2006.
- ,,,.Adult Literacy in America: A First Look at the Findings of the National Adult Literacy Survey.Washington, DC:National Center for Education Statistics, U.S. Department of Education;1993.
- ,,,.The role of health literacy in patient‐physician communication.Fam Med.2002;34:383–389.
- American Medical Association Council on Scientific Affairs.Health literacy.JAMA.1999;281:552–557.
- National Work Group on Literacy and Health.Communicating with patients who have limited literacy skills.J Fam Pract.1998;46:168–176.
- ,.Communicating with patients who cannot read.N Engl J Med.1997;337:272–274.
- ,,,,.Literacy and health outcomes: a systematic review of the literature.J Gen Intern Med.2004;19:1129–1139.
- ,,.The impact of low health literacy on the medical costs of Medicare managed care enrollees.Am J Med.2005;118:371–377.
- ,,,.Health literacy and the risk of hospital admission.J Gen Intern Med.1998;13:791–798.
- ,,, et al.The effect of English language proficiency on length of stay and in‐hospital mortality.J Gen Intern Med.2004;19(3):221–228.
- ,,, et al.Effects of a structured patient‐centered discharge interview on patients' knowledge about their medications.Am J Med.2004;117:563–568.
- ,,.Effects of a videotape information intervention at discharge on diet and exercise compliance after coronary artery bypass surgery.J Cardiopulm Rehab.1999;19(3):170–177.
- .The impact of medical interpreter services on the quality of health care: a systematic review.Med Care Res Rev.2005;62(3):255–299.
- ,,.Use of pictorial aids in medication instructions: a review of the literature.Am J Health Syst Pharm.2006;63:2391–2397.
- ,,,.The role of pictures in improving health communication: A review of research on attention, comprehension, recall, and adherence.Patient Educ Couns.2006;61(2):173–190.
- ,,, et al.Closing the loop. Physician communication with diabetic patients who have low health literacy.Arch Intern Med.2003;163:83–90.
- National Quality Forum.Safe Practices for Better Healthcare,2003; Washington, DC.
- Shojania KG, Duncan BW, McDonald KM, Wachter RM, eds.Making Healthcare Safer: A Critical Analysis of Patient Safety Practices. Evidence Report No. 43 from the Agency for Healthcare Research and Quality. AHRQ Publication No. 01‐E058;2001.
- .Whither continuity of care?N Engl J Med.1999;340:1362–1363.
- ,,, et al.Medication reconciliation: a practical tool to reduce the risk of medication errors.J Crit Care.2003;18(4):201–205.
- ,,,.Influence of hospitalization on drug therapy in the elderly.J Am Geriatr Soc.1989;37:679–683.
- ,,,,,.Preparing patients and caregivers to participate in care delivered across settings: the Care Transitions Intervention.J Am Geriatr Soc.2004;52:1817–1825.
- ,,.Predictors of elder and family caregiver satisfaction with discharge planning.J Cardiovasc Nurs.2000;14(3):76–87.
- ,.Discharge planning and continuity of care for aged people: indicators of satisfaction and implications for practice.Aust J Adv Nurs.1998;16(1):7–13.
- ,,,.Medical errors related to discontinuity of care from an inpatient to an outpatient setting.J Gen Intern Med.2003;18:646–651.
- ,,.Assessing the quality of preparation for posthospital care from the patient's perspective: the care transitions measure.Med Care.2005;43(3):246–255.
- ,,, et al.Adverse events among medical patients after discharge from hospital.CMAJ.2004;170:345–349.
- ,,,,.The incidence and severity of adverse events affecting patients after discharge from the hospital.Ann Intern Med.2003;138:161–167.
- ,,,,.Adverse drug events occurring following hospital discharge.J Gen Intern Med.2005;20:317–323.
- The Joint Commission. Joint Commission National Patient Safety Goals. Available at: http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/. Accessed July 17,2006.
- ,,, et al.Transition of care for hospitalized elderly patients ‐ Development of a discharge checklist for hospitalists.J Hosp Med.2006;1:354–360.
- ,,,,,.Deficits in communication and information transfer between hospital‐based and primary care physicians: implications for patient safety and continuity of care.JAMA.2007;297:831–841.
- Agency for Healthcare Research and Quality. National Guideline Clearinghouse. Available at: http://www.guideline.gov. Accessed January 3,2007.
- ,.The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335:514–517.
- .Hospitalists in the United States—mission accomplished or work in progress?N Engl J Med.2004;350:1935–1936.
- .The evolution of the hospitalist model in the United States.Med Clin North Am2002;86(4):687–706.
- ,.The hospitalist movement 5 years later.JAMA.2002;287:487–494.
- Society of Hospital Medicine. Growth of hospital medicine nationwide. Available at: http://www.hospitalmedicine.org/Content/NavigationMenu/Media/GrowthofHospitalMedicineNationwide/Growth_of_Hospital_M.htm. Accessed July 17,2006.
- ,,,,.Quality assessment of discharge letters in a French university hospital.Int J Health Care Qual Assur Inc Leadersh Health Serv.1998;11(2‐3):90–95.
- ,,.Dissemination of discharge summaries. Not reaching follow‐up physicians.Can Fam Physician.2002;48:737–742.
- ,.Quality assessment of a discharge summary system.CMAJ.1995;152:1437–1442.
- ,,,.Primary care physician attitudes regarding communication with hospitalists.Am J Med.2001;111(9B):15S–20S.
- ,,,.Effect of discharge summary availability during post‐discharge visits on hospital readmission.J Gen Intern Med.2002;17(3):186–192.
- .Study of discharge communications from hospital doctors to an inner London general practice.J R Coll Gen Pract.1987;37:494–495.
- ,,, et al.Patient safety concerns arising from test results that return after hospital discharge.Ann Intern Med.2005;143(2):121–128.
- ,,.Communication between general practitioners and consultants: what should their letters contain?BMJ1992;304(6830):821–824.
- ,,,.Written communication from specialists to general practitioners in cancer care. What are the expectations and how are they met?Scand J Prim Health Care.1998;16(3):154–159.
- ,.Improving the continuity of care between general practitioners and public hospitals.Med J Aust.1994;161:656–659.
- ,.Towards better discharge summaries: brevity and structure.West Engl Med J.1991;106(2):40–41,55.
- ,,.Content of a discharge summary from a medical ward: views of general practitioners and hospital doctors.J R Coll Physicians Lond.1995;29:307–310.
- ,.What is necessary for high‐quality discharge summaries?Am J Med Qual.1999;14(4):160–169.
- The Joint Commission.Standard IM.6.10. Hospital Accreditation Standards.Oakbrook Terrace, IL:The Joint Commission;2006:338–340.
- .The importance of postdischarge telephone follow‐up for hospitalists: a view from the trenches.Am J Med.2001;111(9B):43S–44S.
- ,,,.The quality of communication between hospitals and general practitioners: an assessment.J Qual Clin Pract.1998;18:241–247.
- ,,,.Dictated versus database‐generated discharge summaries: a randomized clinical trial.CMAJ.1999;160:319–326.
- ,,,.Standardized or narrative discharge summaries. Which do family physicians prefer?Can Fam Physician.1998;44:62–69.
- ,.Moving from information transfer to information exchange in health and health care.Soc Sci Med.2003;56:449–464.
- ,,, et al.The costs of adverse drug events in hospitalized patients.Adverse Drug Events Prevention Study Group.JAMA.1997;277:307–311.
- ,,, et al.Systems analysis of adverse drug events.ADE Prevention Study Group.JAMA.1995;274(1):35–43.
- ,,, et al.Incidence of adverse drug events and potential adverse drug events. Implications for prevention.ADE Prevention Study Group.JAMA.1995;274(1):29–34.
- ,.Medication errors in hospitalized cardiovascular patients.Arch Intern Med.2003;163:1461–1466.
- ,,, et al.Unintended medication discrepancies at the time of hospital admission.Arch Intern Med.2005;165:424–429.
- ,,,,,.Reconciliation of discrepancies in medication histories and admission orders of newly hospitalized patients.Am J Health Syst Pharm.2004;61:1689–1695.
- ,,,,,.Frequency, type and clinical importance of medication history errors at admission to hospital: a systematic review.CMAJ.2005;173:510–515.
- ,,,,.Medication reconciliation in the acute care setting: opportunity and challenge for nursing.J Nurs Care Qual.2005;20(2):95–98.
- ,,.The adverse effects of hospitalization on drug regimens.Arch Intern Med.1991;151:1562–1564.
- ,,,,.Prevalence and cost savings of therapeutic interchange among U.S. hospitals.Am J Health Syst Pharm.2002;59:529–533.
- ,,, et al.Medication reconciliation: are we meeting the requirements?JCOM.2006;13:441–444.
- ,,, et al.Role of pharmacist counseling in preventing adverse drug events after hospitalization.Arch Intern Med.2006;166:565–571.
- ,.Effectiveness of a pharmacist‐acquired medication history in promoting patient safety.Am J Health Syst Pharm.2002;59:2221–2225.
- .Ensuring continuity of care and accuracy of patients' medication history on hospital admission.Am J Health Syst Pharm.2002;59:1054–1055.
- ,,,.Current methods used to teach the medication history interview to doctor of pharmacy students.Am J Pharm Educ.2002;66(Summer):103–107.
- AARP. My Personal Medication Record. Available at: http://assets.aarp.org/www.aarp.org_/articles/learntech/wellbeing/medication‐record.pdf. Accessed October 20,2006.
- AARP. Mi registro de medicacion. Available at: http://assets.aarp.org/www.aarp.org_/articles/health/docs/PersonalMedRecordSP.pdf. Accessed October 20,2006.
- Institute for Safe Medication Practices. Available at: http://www.ismp.org. Accessed September 8,2006.
- ,,.Parents as partners in obtaining the medication history.J Am Med Inform Assoc.2005;12:299–305.
- ,,.Medication history on internal medicine wards: assessment of extra information collected from second drug interviews and GP lists.Pharmacoepidemiology Drug Saf.2003;12:491–498.
- Medication Discrepancy Tool. Available at: http://www.caretransitions.org. Accessed July 28,2005.
- ,,,,,.Updating the Beers criteria for potentially inappropriate medication use in older adults: results of a US consensus panel of experts.Arch Intern Med.2003;163:2716–2724.
- .Using the NO TEARS tool for medication review.BMJ2004;329(7463):434.
- ,,,.Clinical pharmacists and inpatient medical care: a systematic review.Arch Intern Med.2006;166:955–964.
- ,.Clinical pharmacy services, pharmacy staffing, and adverse drug reactions in United States hospitals.Pharmacotherapy.2006;26:735–747.
- ,,, et al.Adverse drug events in ambulatory care.N Engl J Med.2003;348:1556–1564.
- MA Coalition for the Prevention of Medical Errors. Reconciling medications. Recommended practices. Available at: http://www.macoalition.org/documents/RecMedPractices.pdf. Accessed July 27,2005.
- ,.OSF healthcare's journey in patient safety.Qual Manag Health Care.2004;13(1):53–59.
- ,,, et al.Prospective payment system and impairment at discharge. The ‘quicker‐and‐sicker’ story revisited.JAMA.1990;264:1980–1983.
- ,,,,,.Discharge planning: comparison of patients and nurses' perceptions of patients following hospital discharge.Image J Nurs Sch.1996;28(2):143–147.
- ,,,.The Care Transitions Intervention: results of a randomized controlled trial.Arch Intern Med.2006;166:1822–1828.
- ,,,,,.Comprehensive discharge planning with postdischarge support for older patients with congestive heart failure: a meta‐analysis.JAMA.2004;291:1358–1367.
- ,,,.Discharge planning from hospital to home.Cochrane Database Syst Rev.2006;4.
- .Falling through the cracks: challenges and opportunities for improving transitional care for persons with continuous complex care needs.J Am Geriatr Soc.2003;51:549–555.
- .The best way to improve emergency department follow‐up is actually to give the patient a specific appointment.J Gen Intern Med.2006;21:398; author reply398.
- ,,,.Continuity of care and patient outcomes after hospital discharge.J Gen Intern Med.2004;19:624–631.
- ,.Patients' understanding of their treatment plans and diagnosis at discharge.Mayo Clin Proc.2005;80:991–994.
- ,,,.The impact of follow‐up telephone calls to patients after hospitalization.Am J Med.2001;111(9B):26S–30S.
- ,.The impact of clinical pharmacists' consultations on geriatric patients' compliance and medical care use: a randomized controlled trial.Gerontologist.1994;34:307–315.
- ,.Telephone follow‐up, initiated by a hospital‐based health professional, for postdischarge problems in patients discharged from hospital to home.Cochrane Database Syst Rev.2007;1.
- ,,, et al.Geriatric home assessment after hospital discharge.J Am Geriatr Soc.1994;42:1229–1234.
- ,.Uncovering a multitude of sins: medication management in the home post acute hospitalisation among the chronically ill.Aust N Z J Med.1999;29(2):220–227.
- ,,, et al.Comprehensive discharge planning and home follow‐up of hospitalized elders: a randomized clinical trial.JAMA.1999;281:613–620.
- ,,,.The cost‐effectiveness of intensive postdischarge care. A randomized trial.Med Care.1988;26:1092–1102.
- ,,,,.The effects of aftercare on chronic patients and frail elderly patients when discharged from hospital: a systematic review.J Adv Nurs.1998;27:1076–1086.
- ,,,,,.A multidisciplinary intervention to prevent the readmission of elderly patients with congestive heart failure.N Engl J Med.1995;333:1190–1195.
- ,,.Medication education of acutely hospitalized older patients.J Gen Intern Med.1999;14:610–616.
- ,,, et al.Patient‐physician communication at hospital discharge and patients' understanding of the postdischarge treatment plan.Arch Intern Med.1997;157:1026–1030.
- ,,.Patient understanding of commonly used medical vocabulary.J Fam Pract.1987;25:176–178.
- .The understanding of medical terminology used in printed health education materials.Heal Educ J.1979;38:111–121.
- ,,,,.The gap between patient reading comprehension and the readability of patient education materials.J Fam Pract.1990;31:533–538.
- ,,. National Assessment of Adult Literacy (NAAL). A first look at the literacy of America's adults in the 21st century. Available at: http://nces.ed.gov/naal. Accessed May 2,2006.
- ,,,.Adult Literacy in America: A First Look at the Findings of the National Adult Literacy Survey.Washington, DC:National Center for Education Statistics, U.S. Department of Education;1993.
- ,,,.The role of health literacy in patient‐physician communication.Fam Med.2002;34:383–389.
- American Medical Association Council on Scientific Affairs.Health literacy.JAMA.1999;281:552–557.
- National Work Group on Literacy and Health.Communicating with patients who have limited literacy skills.J Fam Pract.1998;46:168–176.
- ,.Communicating with patients who cannot read.N Engl J Med.1997;337:272–274.
- ,,,,.Literacy and health outcomes: a systematic review of the literature.J Gen Intern Med.2004;19:1129–1139.
- ,,.The impact of low health literacy on the medical costs of Medicare managed care enrollees.Am J Med.2005;118:371–377.
- ,,,.Health literacy and the risk of hospital admission.J Gen Intern Med.1998;13:791–798.
- ,,, et al.The effect of English language proficiency on length of stay and in‐hospital mortality.J Gen Intern Med.2004;19(3):221–228.
- ,,, et al.Effects of a structured patient‐centered discharge interview on patients' knowledge about their medications.Am J Med.2004;117:563–568.
- ,,.Effects of a videotape information intervention at discharge on diet and exercise compliance after coronary artery bypass surgery.J Cardiopulm Rehab.1999;19(3):170–177.
- .The impact of medical interpreter services on the quality of health care: a systematic review.Med Care Res Rev.2005;62(3):255–299.
- ,,.Use of pictorial aids in medication instructions: a review of the literature.Am J Health Syst Pharm.2006;63:2391–2397.
- ,,,.The role of pictures in improving health communication: A review of research on attention, comprehension, recall, and adherence.Patient Educ Couns.2006;61(2):173–190.
- ,,, et al.Closing the loop. Physician communication with diabetic patients who have low health literacy.Arch Intern Med.2003;163:83–90.
- National Quality Forum.Safe Practices for Better Healthcare,2003; Washington, DC.
- Shojania KG, Duncan BW, McDonald KM, Wachter RM, eds.Making Healthcare Safer: A Critical Analysis of Patient Safety Practices. Evidence Report No. 43 from the Agency for Healthcare Research and Quality. AHRQ Publication No. 01‐E058;2001.
Editorial
As a hospital practitioner, you have undoubtedly experienced the frustration of witnessing how easily the excellent care you provide can unravel as the patient goes out the door. Patients are admitted acutely ill, and largely attributed to your clinical acumen, they are discharged tuned up and stable to return home. Days later, however, you may learn that your best‐laid discharge plans were not properly executed, and the patient returned with yet another exacerbation. Clearly this scenario represents a major setback for the patient and family caregivers. Possibly dismissed as another episode of patient noncompliance, such readmissions are now being recognized as system failures and reflect a discharge process that has been described as random events connected to highly variable actions with only a remote possibility of meeting implied expectations (Roger Resar, MD, Senior Fellow, Institute for Healthcare Improvement).
Once an area that received relatively little attention, transitions out of the hospital has been identified as a priority area in need of action by a confluence of recent research and national activities. Recognizing the expanding evidence for lapses in quality and safety, many esteemed organizations, including the Joint Commission, the Centers for Medicare and Medicaid Services and their accompanying Quality Improvement Organizations, the Institute for Healthcare Improvement, the Institute of Medicine, National Quality Forum, the Medicare Payment Advisory Committee, the American Board of Internal Medicine Foundation, the National Transitions of Care Coalition, the American College of Physicians, the Society for General Medicine, and the Society for Hospital Medicine, are currently focusing their efforts on how to optimize transitions. All have articulated the need for further clinical investigation that can offer greater insight into the nature of the problems that arise during this vulnerable period and what the potential solutions are.
In this edition of the Journal of Hospital Medicine, 3 teams of investigators have responded to this need, making timely, important, and unique contributions to advance the field.13 Specifically, each of these articles further raises awareness that a patient's transition out of the hospital often unfolds quickly in a fast‐paced, chaotic manner, placing many competing demands on clinicians, patients, and family caregivers. Not surprisingly, such competing demands can contribute to deficits in quality and safety. The authors of these studies all directly identify the central role of communication among clinicians as well as between patients and clinicians in ensuring successful handoffs, further affirming the Joint Commission's finding that inadequate communication is the leading cause of sentinel events.4 In this respect, communication is more than simply the transfer of information; rather, it involves the need to ensure comprehension and provide an opportunity to have a 2‐way dialogue. Importantly, these articles share a common approach in fostering our understanding of the perspective of patients and family caregivers with a particular focus on disadvantaged populations.
Kripalani and colleagues conducted a comprehensive review of the state of the science for those key hospital discharge issues that pertain to hospitalists. They identified a number of challenges including communication between hospital‐ and ambulatory‐based clinicians, medication reconciliation, timely hospital follow‐up, and engaging patients in self‐care. For each of these priority areas, the authors provide pragmatic recommendations for improving care that could be implemented within the current state of practice, either individually or as a bundle of interventions.
Recognizing that patients are often the only common thread across different sites of care, Strunin and colleagues demonstrate the value of including the voice of the patient in helping clinicians to understand the challenges and larger context in which they attempt to follow through with discharge instructions. Strunin et al. found that among a range of factors that contribute to adherence problems, many were nonmedical. Fortunately, a number of these are modifiable and point to the need to both prioritize recommendations to patients and to simplify them whenever possible. The authors' findings resonate with a growing literature that examines the hospital discharge process from the patient's perspective.510
Flacker and colleagues surveyed older patients to gain greater insights into their information needs at discharge. From a process standpoint, they demonstrated that a posthospital survey was feasible and acceptable to older patients. In and of itself, this finding has important implications in the context of national efforts aimed at implementing performance measurement and accompanying public reporting. It also may reflect patients' eagerness to be contacted after discharge; hospitalization is a major event in patients' lives, and attentive follow‐up is appreciated. The authors found that more than half of patients did not recall being asked about how they would care for themselves on returning home from the hospital. Although there may be a variety of explanations for this finding, it nevertheless points to an immediate area for intervention.
Collectively, these 3 articles set the stage for a proposed clinical investigation agenda aimed at optimizing transitions out of the hospital (see Table 1).
| 1. Greater recognition of the integral role of family caregivers |
| 2. Empirically define the appropriate follow‐up interval |
| 3. Define physician accountability for patients referred to home health on hospital discharge |
| 4. Delineate the role of the hospitalist in the advanced medical home |
| 5. Develop the ability to examine episodes of care |
These 5 recommendations have the potential to ensure that the gains patients make in our hospitals are maintained long after discharge.
-
Greater Recognition for the Integral Role of Family Caregivers. The patient and family caregivers should be integrated into health care professionals' efforts to improve care coordination across settings. Family caregivers have been silent partners in health care delivery, functioning as de facto care coordinators. During care handoffs, family caregivers make important contributions to ensuring quality, safety, and adherence to patient preferences; their role needs to be formally recognized and supported. An important initial step would be standardizing the approach to defining the types and intensity of the roles family caregivers play to facilitate improved communication. One proposed working definition is the FACED classification developed by one of the authors (E.C.). Modeled after the TNM system used in cancer, each letter of FACED refers to a different contribution made by a family caregiver: F = Financial; A = Advocacy; C = Care coordination; E = Emotional support; and D = Direct care provision. A simple numeric rating system could be developed whereby 0 = does not contribute in this area and 3 = makes significant contribution to this area. Such a straightforward approach would readily inform all members of the health care team about the caregivers' roles and capabilities and how they can optimally collaborate in the care plan.
-
Empirically Define Appropriate Follow‐Up Interval. At present, patients are given rather arbitrary and generic instructions for when to obtain follow‐up with their outpatient primary care physician or specialist. Surgical patients are often instructed to follow up with their surgeon, and yet most of the readmissions of these patients are attributable to medical conditions (personal communication, Steven Jencks, MD, Centers for Medicare and Medicaid Services). Furthermore, a significant number of discharged medical and surgical patients are readmitted to the hospital within 30 days without any outpatient contact with a health professional. One may envision an evidence‐based tiered approach whereby patients are assigned a hospital readmission risk score at the time of discharge that then determines the timing of their follow‐up appointment. Using this framework, the highest‐risk patients may be encouraged to receive follow‐up within 2472 hours, whereas lower‐risk patients may be able to wait 1421 days. Of course, there will need to be sufficient access to outpatient physicians, who will need to be available, to ensure the success of this strategy.
-
Define Physician Accountability for Patients Referred to Home Health on Hospital Discharge. Communication problems between the hospital and the home health care agency are a source of aggravation for both parties, not to mention patients. Typically, a hospitalist provides the initial order for services and then expects subsequent home care coordination to be managed by an outpatient physician. Unfortunately, in some cases the patient may not have an outpatient physician or the patient's primary physician may be unaware of the recent hospitalization and thus unwilling to assume management of an unfamiliar care plan. As a result, home care nurses often cannot identify a physician to respond to their questions or concerns. At the center of this problem lies a lack of understanding of where the responsibility of the ordering hospitalist ends and the outpatient physician assuming care begins. Recognizing the profound costs of failed home health care leading to hospital readmission, the nation's Quality Improvement Organizations launched a national campaign in 2006 to address this problem. Hospitalists should engage in this effort and not punt the entire responsibility to home health agenciesimagine if hospitals and hospitalists were financially penalized if a patient was readmitted.
-
Delineate the Role of the Hospitalist in the Advanced Medical Home. Modeled after a concept with origins in pediatrics, the American College of Physicians and American Academy of Family Physicians are promoting the advanced medical home as a new care model that aims to provide comprehensive ambulatory care with an explicit focus on care coordination.11 The Centers for Medicare and Medicaid Services is planning to initiate a demonstration of this approach. What has not been adequately underscored is how the advanced medical home will communicate essential clinical information with the hospitalist and what, if any, will be the role of the hospitalist in relation to a patient's medical home? Ideally, the medical home approach will alleviate many of the current access problems that impede timely follow‐up.
-
Develop Ability to Examine Episodes of Care. Patients with complex conditions often require care from different practitioners in multiple settings. From the vantage point of health care professionals, these may appear to occur as merely a string of individual interactions, including hospital admissions and discharges. However from the patient's perspective, the experience is more appropriately characterized as a journey across an aggregated episode of care. The National Quality Forum is currently exploring how to measure quality of care delivered across such an episode of care. Additionally, the Centers for Medicare and Medicaid Services is developing a new assessment tool that will transcend acute and postacute care settings, the Continuity Assessment Record and Evaluation (CARE). This tool will potentially enhance our ability to measure care across a predefined episode. Measurement can further pave the way for payment reform designed to align incentives toward higher‐quality care transitions. Currently, professional fees for coronary artery bypass grafting surgery are bundled across an episode, including hospital and posthospital care settings. Extending this approach to a wider array of conditions and services could encourage new perspectives on the timing of discharge and the use of posthospital care venues. For example, under bundled payment, incentives might support a plan to keep a patient in the hospital an extra 1 or 2 days in order to obviate a transfer to a skilled nursing facility and the concomitant risks of transfer‐related problems. Further, bundled payment may allow for the provision of additional services not currently covered, including transportation, as identified by Strunin and colleagues.3
Hospitalists are well positioned to offer leadership in these high‐leverage areas and thereby make a unique contribution to the quality and safety of care transitions. By so doing, they are poised to reaffirm their professionalism,12 ensuring that the excellent care that they provide in the hospital is sustained well into the future.
- ,,.Discharge information and older patients: do they get what they need?J Hosp Med.2007;2:291–296.
- ,,,.Promoting effective transitions of care at hospital discharge: a review of key issues for hospitalists.J Hosp Med.2007;2:314–323.
- ,,.Understanding rehospitalization risk: can the hospital discharge be modified to impact recurrent hospitalization.J Hosp Med.2007;2:297–304.
- The Joint Commission. Sentinel event statistics. Available at: http://www.jointcommission.org/SentinelEvents/Statistics/. Accessed August 7,2007.
- ,,.Patients' and caregivers' transition from hospital to home: needs and recommendations.Home Health Care Serv Q.1998;17:27–48.
- ,,,,.Carepartner experiences with hospital care.Med Care.1999;37:33–38.
- ,.Understanding coordination of care from the consumer's perspective in a regional health system.Health Serv Res.2002;37:1031–1054.
- ,,, et al.Development and testing of a measure designed to assess the quality of care transitions.Int J Integrated Care.2002;2:e02.
- .Rough crossings: family caregivers odysseys through the health care system.New York:United Hospital Fund of New York;1998.
- ,.Facilitating the transition out of the hospital. In:Gerteis M,Edgman‐Levitan S,Daley J,Delbanco T, editors.Through the Patient's Eyes: Understanding and Promoting Patient‐Centered Care.San Francisco:Jossey‐Bass;1993:204–223.
- ,,American College of Physicians. The advanced medical home: a patient‐centered, physician‐guided model of health care. p. 1–22. http://www.acponline.org/hpp/adv_med.pdf Accessed August 7,2007.
- Project of the ABIM Foundation A‐AFaEFoIM.Medical professionalism in the new millennium: a physician charter.Ann Intern Med.2002;136:243–246.
As a hospital practitioner, you have undoubtedly experienced the frustration of witnessing how easily the excellent care you provide can unravel as the patient goes out the door. Patients are admitted acutely ill, and largely attributed to your clinical acumen, they are discharged tuned up and stable to return home. Days later, however, you may learn that your best‐laid discharge plans were not properly executed, and the patient returned with yet another exacerbation. Clearly this scenario represents a major setback for the patient and family caregivers. Possibly dismissed as another episode of patient noncompliance, such readmissions are now being recognized as system failures and reflect a discharge process that has been described as random events connected to highly variable actions with only a remote possibility of meeting implied expectations (Roger Resar, MD, Senior Fellow, Institute for Healthcare Improvement).
Once an area that received relatively little attention, transitions out of the hospital has been identified as a priority area in need of action by a confluence of recent research and national activities. Recognizing the expanding evidence for lapses in quality and safety, many esteemed organizations, including the Joint Commission, the Centers for Medicare and Medicaid Services and their accompanying Quality Improvement Organizations, the Institute for Healthcare Improvement, the Institute of Medicine, National Quality Forum, the Medicare Payment Advisory Committee, the American Board of Internal Medicine Foundation, the National Transitions of Care Coalition, the American College of Physicians, the Society for General Medicine, and the Society for Hospital Medicine, are currently focusing their efforts on how to optimize transitions. All have articulated the need for further clinical investigation that can offer greater insight into the nature of the problems that arise during this vulnerable period and what the potential solutions are.
In this edition of the Journal of Hospital Medicine, 3 teams of investigators have responded to this need, making timely, important, and unique contributions to advance the field.13 Specifically, each of these articles further raises awareness that a patient's transition out of the hospital often unfolds quickly in a fast‐paced, chaotic manner, placing many competing demands on clinicians, patients, and family caregivers. Not surprisingly, such competing demands can contribute to deficits in quality and safety. The authors of these studies all directly identify the central role of communication among clinicians as well as between patients and clinicians in ensuring successful handoffs, further affirming the Joint Commission's finding that inadequate communication is the leading cause of sentinel events.4 In this respect, communication is more than simply the transfer of information; rather, it involves the need to ensure comprehension and provide an opportunity to have a 2‐way dialogue. Importantly, these articles share a common approach in fostering our understanding of the perspective of patients and family caregivers with a particular focus on disadvantaged populations.
Kripalani and colleagues conducted a comprehensive review of the state of the science for those key hospital discharge issues that pertain to hospitalists. They identified a number of challenges including communication between hospital‐ and ambulatory‐based clinicians, medication reconciliation, timely hospital follow‐up, and engaging patients in self‐care. For each of these priority areas, the authors provide pragmatic recommendations for improving care that could be implemented within the current state of practice, either individually or as a bundle of interventions.
Recognizing that patients are often the only common thread across different sites of care, Strunin and colleagues demonstrate the value of including the voice of the patient in helping clinicians to understand the challenges and larger context in which they attempt to follow through with discharge instructions. Strunin et al. found that among a range of factors that contribute to adherence problems, many were nonmedical. Fortunately, a number of these are modifiable and point to the need to both prioritize recommendations to patients and to simplify them whenever possible. The authors' findings resonate with a growing literature that examines the hospital discharge process from the patient's perspective.510
Flacker and colleagues surveyed older patients to gain greater insights into their information needs at discharge. From a process standpoint, they demonstrated that a posthospital survey was feasible and acceptable to older patients. In and of itself, this finding has important implications in the context of national efforts aimed at implementing performance measurement and accompanying public reporting. It also may reflect patients' eagerness to be contacted after discharge; hospitalization is a major event in patients' lives, and attentive follow‐up is appreciated. The authors found that more than half of patients did not recall being asked about how they would care for themselves on returning home from the hospital. Although there may be a variety of explanations for this finding, it nevertheless points to an immediate area for intervention.
Collectively, these 3 articles set the stage for a proposed clinical investigation agenda aimed at optimizing transitions out of the hospital (see Table 1).
| 1. Greater recognition of the integral role of family caregivers |
| 2. Empirically define the appropriate follow‐up interval |
| 3. Define physician accountability for patients referred to home health on hospital discharge |
| 4. Delineate the role of the hospitalist in the advanced medical home |
| 5. Develop the ability to examine episodes of care |
These 5 recommendations have the potential to ensure that the gains patients make in our hospitals are maintained long after discharge.
-
Greater Recognition for the Integral Role of Family Caregivers. The patient and family caregivers should be integrated into health care professionals' efforts to improve care coordination across settings. Family caregivers have been silent partners in health care delivery, functioning as de facto care coordinators. During care handoffs, family caregivers make important contributions to ensuring quality, safety, and adherence to patient preferences; their role needs to be formally recognized and supported. An important initial step would be standardizing the approach to defining the types and intensity of the roles family caregivers play to facilitate improved communication. One proposed working definition is the FACED classification developed by one of the authors (E.C.). Modeled after the TNM system used in cancer, each letter of FACED refers to a different contribution made by a family caregiver: F = Financial; A = Advocacy; C = Care coordination; E = Emotional support; and D = Direct care provision. A simple numeric rating system could be developed whereby 0 = does not contribute in this area and 3 = makes significant contribution to this area. Such a straightforward approach would readily inform all members of the health care team about the caregivers' roles and capabilities and how they can optimally collaborate in the care plan.
-
Empirically Define Appropriate Follow‐Up Interval. At present, patients are given rather arbitrary and generic instructions for when to obtain follow‐up with their outpatient primary care physician or specialist. Surgical patients are often instructed to follow up with their surgeon, and yet most of the readmissions of these patients are attributable to medical conditions (personal communication, Steven Jencks, MD, Centers for Medicare and Medicaid Services). Furthermore, a significant number of discharged medical and surgical patients are readmitted to the hospital within 30 days without any outpatient contact with a health professional. One may envision an evidence‐based tiered approach whereby patients are assigned a hospital readmission risk score at the time of discharge that then determines the timing of their follow‐up appointment. Using this framework, the highest‐risk patients may be encouraged to receive follow‐up within 2472 hours, whereas lower‐risk patients may be able to wait 1421 days. Of course, there will need to be sufficient access to outpatient physicians, who will need to be available, to ensure the success of this strategy.
-
Define Physician Accountability for Patients Referred to Home Health on Hospital Discharge. Communication problems between the hospital and the home health care agency are a source of aggravation for both parties, not to mention patients. Typically, a hospitalist provides the initial order for services and then expects subsequent home care coordination to be managed by an outpatient physician. Unfortunately, in some cases the patient may not have an outpatient physician or the patient's primary physician may be unaware of the recent hospitalization and thus unwilling to assume management of an unfamiliar care plan. As a result, home care nurses often cannot identify a physician to respond to their questions or concerns. At the center of this problem lies a lack of understanding of where the responsibility of the ordering hospitalist ends and the outpatient physician assuming care begins. Recognizing the profound costs of failed home health care leading to hospital readmission, the nation's Quality Improvement Organizations launched a national campaign in 2006 to address this problem. Hospitalists should engage in this effort and not punt the entire responsibility to home health agenciesimagine if hospitals and hospitalists were financially penalized if a patient was readmitted.
-
Delineate the Role of the Hospitalist in the Advanced Medical Home. Modeled after a concept with origins in pediatrics, the American College of Physicians and American Academy of Family Physicians are promoting the advanced medical home as a new care model that aims to provide comprehensive ambulatory care with an explicit focus on care coordination.11 The Centers for Medicare and Medicaid Services is planning to initiate a demonstration of this approach. What has not been adequately underscored is how the advanced medical home will communicate essential clinical information with the hospitalist and what, if any, will be the role of the hospitalist in relation to a patient's medical home? Ideally, the medical home approach will alleviate many of the current access problems that impede timely follow‐up.
-
Develop Ability to Examine Episodes of Care. Patients with complex conditions often require care from different practitioners in multiple settings. From the vantage point of health care professionals, these may appear to occur as merely a string of individual interactions, including hospital admissions and discharges. However from the patient's perspective, the experience is more appropriately characterized as a journey across an aggregated episode of care. The National Quality Forum is currently exploring how to measure quality of care delivered across such an episode of care. Additionally, the Centers for Medicare and Medicaid Services is developing a new assessment tool that will transcend acute and postacute care settings, the Continuity Assessment Record and Evaluation (CARE). This tool will potentially enhance our ability to measure care across a predefined episode. Measurement can further pave the way for payment reform designed to align incentives toward higher‐quality care transitions. Currently, professional fees for coronary artery bypass grafting surgery are bundled across an episode, including hospital and posthospital care settings. Extending this approach to a wider array of conditions and services could encourage new perspectives on the timing of discharge and the use of posthospital care venues. For example, under bundled payment, incentives might support a plan to keep a patient in the hospital an extra 1 or 2 days in order to obviate a transfer to a skilled nursing facility and the concomitant risks of transfer‐related problems. Further, bundled payment may allow for the provision of additional services not currently covered, including transportation, as identified by Strunin and colleagues.3
Hospitalists are well positioned to offer leadership in these high‐leverage areas and thereby make a unique contribution to the quality and safety of care transitions. By so doing, they are poised to reaffirm their professionalism,12 ensuring that the excellent care that they provide in the hospital is sustained well into the future.
As a hospital practitioner, you have undoubtedly experienced the frustration of witnessing how easily the excellent care you provide can unravel as the patient goes out the door. Patients are admitted acutely ill, and largely attributed to your clinical acumen, they are discharged tuned up and stable to return home. Days later, however, you may learn that your best‐laid discharge plans were not properly executed, and the patient returned with yet another exacerbation. Clearly this scenario represents a major setback for the patient and family caregivers. Possibly dismissed as another episode of patient noncompliance, such readmissions are now being recognized as system failures and reflect a discharge process that has been described as random events connected to highly variable actions with only a remote possibility of meeting implied expectations (Roger Resar, MD, Senior Fellow, Institute for Healthcare Improvement).
Once an area that received relatively little attention, transitions out of the hospital has been identified as a priority area in need of action by a confluence of recent research and national activities. Recognizing the expanding evidence for lapses in quality and safety, many esteemed organizations, including the Joint Commission, the Centers for Medicare and Medicaid Services and their accompanying Quality Improvement Organizations, the Institute for Healthcare Improvement, the Institute of Medicine, National Quality Forum, the Medicare Payment Advisory Committee, the American Board of Internal Medicine Foundation, the National Transitions of Care Coalition, the American College of Physicians, the Society for General Medicine, and the Society for Hospital Medicine, are currently focusing their efforts on how to optimize transitions. All have articulated the need for further clinical investigation that can offer greater insight into the nature of the problems that arise during this vulnerable period and what the potential solutions are.
In this edition of the Journal of Hospital Medicine, 3 teams of investigators have responded to this need, making timely, important, and unique contributions to advance the field.13 Specifically, each of these articles further raises awareness that a patient's transition out of the hospital often unfolds quickly in a fast‐paced, chaotic manner, placing many competing demands on clinicians, patients, and family caregivers. Not surprisingly, such competing demands can contribute to deficits in quality and safety. The authors of these studies all directly identify the central role of communication among clinicians as well as between patients and clinicians in ensuring successful handoffs, further affirming the Joint Commission's finding that inadequate communication is the leading cause of sentinel events.4 In this respect, communication is more than simply the transfer of information; rather, it involves the need to ensure comprehension and provide an opportunity to have a 2‐way dialogue. Importantly, these articles share a common approach in fostering our understanding of the perspective of patients and family caregivers with a particular focus on disadvantaged populations.
Kripalani and colleagues conducted a comprehensive review of the state of the science for those key hospital discharge issues that pertain to hospitalists. They identified a number of challenges including communication between hospital‐ and ambulatory‐based clinicians, medication reconciliation, timely hospital follow‐up, and engaging patients in self‐care. For each of these priority areas, the authors provide pragmatic recommendations for improving care that could be implemented within the current state of practice, either individually or as a bundle of interventions.
Recognizing that patients are often the only common thread across different sites of care, Strunin and colleagues demonstrate the value of including the voice of the patient in helping clinicians to understand the challenges and larger context in which they attempt to follow through with discharge instructions. Strunin et al. found that among a range of factors that contribute to adherence problems, many were nonmedical. Fortunately, a number of these are modifiable and point to the need to both prioritize recommendations to patients and to simplify them whenever possible. The authors' findings resonate with a growing literature that examines the hospital discharge process from the patient's perspective.510
Flacker and colleagues surveyed older patients to gain greater insights into their information needs at discharge. From a process standpoint, they demonstrated that a posthospital survey was feasible and acceptable to older patients. In and of itself, this finding has important implications in the context of national efforts aimed at implementing performance measurement and accompanying public reporting. It also may reflect patients' eagerness to be contacted after discharge; hospitalization is a major event in patients' lives, and attentive follow‐up is appreciated. The authors found that more than half of patients did not recall being asked about how they would care for themselves on returning home from the hospital. Although there may be a variety of explanations for this finding, it nevertheless points to an immediate area for intervention.
Collectively, these 3 articles set the stage for a proposed clinical investigation agenda aimed at optimizing transitions out of the hospital (see Table 1).
| 1. Greater recognition of the integral role of family caregivers |
| 2. Empirically define the appropriate follow‐up interval |
| 3. Define physician accountability for patients referred to home health on hospital discharge |
| 4. Delineate the role of the hospitalist in the advanced medical home |
| 5. Develop the ability to examine episodes of care |
These 5 recommendations have the potential to ensure that the gains patients make in our hospitals are maintained long after discharge.
-
Greater Recognition for the Integral Role of Family Caregivers. The patient and family caregivers should be integrated into health care professionals' efforts to improve care coordination across settings. Family caregivers have been silent partners in health care delivery, functioning as de facto care coordinators. During care handoffs, family caregivers make important contributions to ensuring quality, safety, and adherence to patient preferences; their role needs to be formally recognized and supported. An important initial step would be standardizing the approach to defining the types and intensity of the roles family caregivers play to facilitate improved communication. One proposed working definition is the FACED classification developed by one of the authors (E.C.). Modeled after the TNM system used in cancer, each letter of FACED refers to a different contribution made by a family caregiver: F = Financial; A = Advocacy; C = Care coordination; E = Emotional support; and D = Direct care provision. A simple numeric rating system could be developed whereby 0 = does not contribute in this area and 3 = makes significant contribution to this area. Such a straightforward approach would readily inform all members of the health care team about the caregivers' roles and capabilities and how they can optimally collaborate in the care plan.
-
Empirically Define Appropriate Follow‐Up Interval. At present, patients are given rather arbitrary and generic instructions for when to obtain follow‐up with their outpatient primary care physician or specialist. Surgical patients are often instructed to follow up with their surgeon, and yet most of the readmissions of these patients are attributable to medical conditions (personal communication, Steven Jencks, MD, Centers for Medicare and Medicaid Services). Furthermore, a significant number of discharged medical and surgical patients are readmitted to the hospital within 30 days without any outpatient contact with a health professional. One may envision an evidence‐based tiered approach whereby patients are assigned a hospital readmission risk score at the time of discharge that then determines the timing of their follow‐up appointment. Using this framework, the highest‐risk patients may be encouraged to receive follow‐up within 2472 hours, whereas lower‐risk patients may be able to wait 1421 days. Of course, there will need to be sufficient access to outpatient physicians, who will need to be available, to ensure the success of this strategy.
-
Define Physician Accountability for Patients Referred to Home Health on Hospital Discharge. Communication problems between the hospital and the home health care agency are a source of aggravation for both parties, not to mention patients. Typically, a hospitalist provides the initial order for services and then expects subsequent home care coordination to be managed by an outpatient physician. Unfortunately, in some cases the patient may not have an outpatient physician or the patient's primary physician may be unaware of the recent hospitalization and thus unwilling to assume management of an unfamiliar care plan. As a result, home care nurses often cannot identify a physician to respond to their questions or concerns. At the center of this problem lies a lack of understanding of where the responsibility of the ordering hospitalist ends and the outpatient physician assuming care begins. Recognizing the profound costs of failed home health care leading to hospital readmission, the nation's Quality Improvement Organizations launched a national campaign in 2006 to address this problem. Hospitalists should engage in this effort and not punt the entire responsibility to home health agenciesimagine if hospitals and hospitalists were financially penalized if a patient was readmitted.
-
Delineate the Role of the Hospitalist in the Advanced Medical Home. Modeled after a concept with origins in pediatrics, the American College of Physicians and American Academy of Family Physicians are promoting the advanced medical home as a new care model that aims to provide comprehensive ambulatory care with an explicit focus on care coordination.11 The Centers for Medicare and Medicaid Services is planning to initiate a demonstration of this approach. What has not been adequately underscored is how the advanced medical home will communicate essential clinical information with the hospitalist and what, if any, will be the role of the hospitalist in relation to a patient's medical home? Ideally, the medical home approach will alleviate many of the current access problems that impede timely follow‐up.
-
Develop Ability to Examine Episodes of Care. Patients with complex conditions often require care from different practitioners in multiple settings. From the vantage point of health care professionals, these may appear to occur as merely a string of individual interactions, including hospital admissions and discharges. However from the patient's perspective, the experience is more appropriately characterized as a journey across an aggregated episode of care. The National Quality Forum is currently exploring how to measure quality of care delivered across such an episode of care. Additionally, the Centers for Medicare and Medicaid Services is developing a new assessment tool that will transcend acute and postacute care settings, the Continuity Assessment Record and Evaluation (CARE). This tool will potentially enhance our ability to measure care across a predefined episode. Measurement can further pave the way for payment reform designed to align incentives toward higher‐quality care transitions. Currently, professional fees for coronary artery bypass grafting surgery are bundled across an episode, including hospital and posthospital care settings. Extending this approach to a wider array of conditions and services could encourage new perspectives on the timing of discharge and the use of posthospital care venues. For example, under bundled payment, incentives might support a plan to keep a patient in the hospital an extra 1 or 2 days in order to obviate a transfer to a skilled nursing facility and the concomitant risks of transfer‐related problems. Further, bundled payment may allow for the provision of additional services not currently covered, including transportation, as identified by Strunin and colleagues.3
Hospitalists are well positioned to offer leadership in these high‐leverage areas and thereby make a unique contribution to the quality and safety of care transitions. By so doing, they are poised to reaffirm their professionalism,12 ensuring that the excellent care that they provide in the hospital is sustained well into the future.
- ,,.Discharge information and older patients: do they get what they need?J Hosp Med.2007;2:291–296.
- ,,,.Promoting effective transitions of care at hospital discharge: a review of key issues for hospitalists.J Hosp Med.2007;2:314–323.
- ,,.Understanding rehospitalization risk: can the hospital discharge be modified to impact recurrent hospitalization.J Hosp Med.2007;2:297–304.
- The Joint Commission. Sentinel event statistics. Available at: http://www.jointcommission.org/SentinelEvents/Statistics/. Accessed August 7,2007.
- ,,.Patients' and caregivers' transition from hospital to home: needs and recommendations.Home Health Care Serv Q.1998;17:27–48.
- ,,,,.Carepartner experiences with hospital care.Med Care.1999;37:33–38.
- ,.Understanding coordination of care from the consumer's perspective in a regional health system.Health Serv Res.2002;37:1031–1054.
- ,,, et al.Development and testing of a measure designed to assess the quality of care transitions.Int J Integrated Care.2002;2:e02.
- .Rough crossings: family caregivers odysseys through the health care system.New York:United Hospital Fund of New York;1998.
- ,.Facilitating the transition out of the hospital. In:Gerteis M,Edgman‐Levitan S,Daley J,Delbanco T, editors.Through the Patient's Eyes: Understanding and Promoting Patient‐Centered Care.San Francisco:Jossey‐Bass;1993:204–223.
- ,,American College of Physicians. The advanced medical home: a patient‐centered, physician‐guided model of health care. p. 1–22. http://www.acponline.org/hpp/adv_med.pdf Accessed August 7,2007.
- Project of the ABIM Foundation A‐AFaEFoIM.Medical professionalism in the new millennium: a physician charter.Ann Intern Med.2002;136:243–246.
- ,,.Discharge information and older patients: do they get what they need?J Hosp Med.2007;2:291–296.
- ,,,.Promoting effective transitions of care at hospital discharge: a review of key issues for hospitalists.J Hosp Med.2007;2:314–323.
- ,,.Understanding rehospitalization risk: can the hospital discharge be modified to impact recurrent hospitalization.J Hosp Med.2007;2:297–304.
- The Joint Commission. Sentinel event statistics. Available at: http://www.jointcommission.org/SentinelEvents/Statistics/. Accessed August 7,2007.
- ,,.Patients' and caregivers' transition from hospital to home: needs and recommendations.Home Health Care Serv Q.1998;17:27–48.
- ,,,,.Carepartner experiences with hospital care.Med Care.1999;37:33–38.
- ,.Understanding coordination of care from the consumer's perspective in a regional health system.Health Serv Res.2002;37:1031–1054.
- ,,, et al.Development and testing of a measure designed to assess the quality of care transitions.Int J Integrated Care.2002;2:e02.
- .Rough crossings: family caregivers odysseys through the health care system.New York:United Hospital Fund of New York;1998.
- ,.Facilitating the transition out of the hospital. In:Gerteis M,Edgman‐Levitan S,Daley J,Delbanco T, editors.Through the Patient's Eyes: Understanding and Promoting Patient‐Centered Care.San Francisco:Jossey‐Bass;1993:204–223.
- ,,American College of Physicians. The advanced medical home: a patient‐centered, physician‐guided model of health care. p. 1–22. http://www.acponline.org/hpp/adv_med.pdf Accessed August 7,2007.
- Project of the ABIM Foundation A‐AFaEFoIM.Medical professionalism in the new millennium: a physician charter.Ann Intern Med.2002;136:243–246.
FDA clears first rapid test to screen for bacterial contamination in platelets
The US Food and Drug Administration (FDA) has cleared for marketing the first rapid test to detect bacterial contamination in leukoreduced apheresis platelets prior to transfusion.
The platelet pan genera detection (PGD) test system is a disposable test strip for use in a hospital transfusion service setting.
It is intended to supplement current quality control testing methods of platelets following collection.
The clearance of this test is a significant advancement in detecting bacterial contamination of platelets, according to Jesse L. Goodman, MD, MPH, director of the FDA’s Center for Biologics Evaluation and Research.
“In half an hour, a sample is prepared, processed, and read, providing an additional assurance that the product is free from harmful bacteria,” Dr Goodman said.
Bacterial contamination of platelets is the leading infectious cause of transfusion-related patient fatalities. The risk of a patient receiving a transfusion contaminated with bacteria is 1 in 5,000, far greater than the risk of transmitting hepatitis C (1 in 1.6 million) or HIV (1 in 1.9 million).
To reduce the risk of transfusing contaminated platelets, blood centers culture samples of the platelets 24 hours after the donation. The culture is read within 48 hours of donation, and contaminated units are discarded.
However, there is a possibility that the number of bacteria present at the time of culture may be so low that bacteria are not detected due to sampling limitations.
Rapid testing of platelets using the platelet PGD test system permits units of platelets to be retested at a time closer to their use. Although the test system is less sensitive than standard cultures, it is done later in storage when bacteria, if present, have multiplied and are therefore easier to detect.
The platelet PGD test system was developed by Verax Biomedica Inc., Worcester, Massachusetts. ![]()
The US Food and Drug Administration (FDA) has cleared for marketing the first rapid test to detect bacterial contamination in leukoreduced apheresis platelets prior to transfusion.
The platelet pan genera detection (PGD) test system is a disposable test strip for use in a hospital transfusion service setting.
It is intended to supplement current quality control testing methods of platelets following collection.
The clearance of this test is a significant advancement in detecting bacterial contamination of platelets, according to Jesse L. Goodman, MD, MPH, director of the FDA’s Center for Biologics Evaluation and Research.
“In half an hour, a sample is prepared, processed, and read, providing an additional assurance that the product is free from harmful bacteria,” Dr Goodman said.
Bacterial contamination of platelets is the leading infectious cause of transfusion-related patient fatalities. The risk of a patient receiving a transfusion contaminated with bacteria is 1 in 5,000, far greater than the risk of transmitting hepatitis C (1 in 1.6 million) or HIV (1 in 1.9 million).
To reduce the risk of transfusing contaminated platelets, blood centers culture samples of the platelets 24 hours after the donation. The culture is read within 48 hours of donation, and contaminated units are discarded.
However, there is a possibility that the number of bacteria present at the time of culture may be so low that bacteria are not detected due to sampling limitations.
Rapid testing of platelets using the platelet PGD test system permits units of platelets to be retested at a time closer to their use. Although the test system is less sensitive than standard cultures, it is done later in storage when bacteria, if present, have multiplied and are therefore easier to detect.
The platelet PGD test system was developed by Verax Biomedica Inc., Worcester, Massachusetts. ![]()
The US Food and Drug Administration (FDA) has cleared for marketing the first rapid test to detect bacterial contamination in leukoreduced apheresis platelets prior to transfusion.
The platelet pan genera detection (PGD) test system is a disposable test strip for use in a hospital transfusion service setting.
It is intended to supplement current quality control testing methods of platelets following collection.
The clearance of this test is a significant advancement in detecting bacterial contamination of platelets, according to Jesse L. Goodman, MD, MPH, director of the FDA’s Center for Biologics Evaluation and Research.
“In half an hour, a sample is prepared, processed, and read, providing an additional assurance that the product is free from harmful bacteria,” Dr Goodman said.
Bacterial contamination of platelets is the leading infectious cause of transfusion-related patient fatalities. The risk of a patient receiving a transfusion contaminated with bacteria is 1 in 5,000, far greater than the risk of transmitting hepatitis C (1 in 1.6 million) or HIV (1 in 1.9 million).
To reduce the risk of transfusing contaminated platelets, blood centers culture samples of the platelets 24 hours after the donation. The culture is read within 48 hours of donation, and contaminated units are discarded.
However, there is a possibility that the number of bacteria present at the time of culture may be so low that bacteria are not detected due to sampling limitations.
Rapid testing of platelets using the platelet PGD test system permits units of platelets to be retested at a time closer to their use. Although the test system is less sensitive than standard cultures, it is done later in storage when bacteria, if present, have multiplied and are therefore easier to detect.
The platelet PGD test system was developed by Verax Biomedica Inc., Worcester, Massachusetts. ![]()