User login
The Boutique Lure

The Boutique Lure
Question: I recently received a brochure in the mail about a hospital that caters only to cardiac patients. While I think this job sounds intriguing, I’m concerned that this may be a boutique hospital. What do you think of the movement toward boutique hospitals? Do you think they are ethical?
Curious in Boston
Dr. Hospitalist responds: Boutique or specialty hospitals have been hotly debated among healthcare policymakers over the past few years. Compared with the number of general hospitals, the numbers of specialty hospitals—typically those that focus on cardiac, orthopedic, surgical, and women’s procedures—are small.
A Government Accounting Office (GAO) report in 2003 identified 100 such hospitals in the country. More than two-thirds of the hospitals are in seven states (Arizona, California, Kansas, Oklahoma, Louisiana, South Dakota, and Texas).
The GAO found that compared with general hospitals, specialty hospitals are “much less likely to have emergency departments, treated smaller percentages of Medicaid patients and derived a smaller share of their revenues from inpatient services.” Although small, this is a growing segment of the healthcare industry.
Specialty hospitals are controversial because many are for-profit and often owned by some of the physicians who work at the hospital. Specialty hospital supporters believe competition between specialty and general hospitals for services can lower costs and improve care.
A 2005 Medicare Payment Advisory Commission study found that physician-owned specialty hospitals decreased lengths of stay but didn’t lower costs for Medicare patients.
In general, specialty hospitals treated less-severe cases and tended to have lower numbers of Medicaid patients than community hospitals.
Specialty care hospital critics are concerned that specialty hospitals take care of the most profitable patients (those who are less ill) and leave the general hospital with the sicker patients who incur higher costs.
They fear growing numbers of specialty hospitals will make it financially difficult for general hospitals to meet all of a community’s needs, including charity care and emergency services.
Critics are also concerned that physician ownership of specialty hospitals could affect physicians’ clinical behavior by driving inappropriate referrals.
You may remember that the federal Stark law (named after Rep. Peter Stark, D-Calif.) generally prohibits physicians from referring Medicare patients for healthcare services to facilities where they have financial interests.
This law was enacted after several studies demonstrated that physicians with ownership interest in clinical laboratories, diagnostic imaging centers, and physical therapy providers made more referrals to these centers and ordered more services at higher costs.
The Stark law lets physicians who have an ownership interest in an entire hospital and are authorized to perform services there to refer patients to that hospital.
As you consider this opportunity, further investigate the risks, benefits, and potential effect of the specialty hospital on your community and our healthcare system.
Holiday Dilemma
Question: I just took over scheduling for our hospitalist group. I’ve been practicing nearly two years and am wondering how to staff holidays. I’m finding it difficult handling the multiple requests for Thanksgiving, Christmas, and New Year’s Eve. Do you know of any innovative scheduling techniques?
Schedule Grinch in Philadelphia
Dr. Hospitalist responds: Congratulations on your new responsibility! I write this with my tongue firmly planted in my cheek. As you now realize, completing the schedule is not easy.
Unfortunately, most hospitalists don’t recognize the enormous challenge one faces in filling the schedule until they are given the task.
Unless you were a chief medical resident, you probably didn’t learn or practice scheduling in the course of your medical training. Inevitably, everyone wants and expects to get their choice of days off. Of course, that is rarely possible.
How do you make everyone happy? It is important to recognize that making everyone happy every time is not possible. But it is possible and important to be fair to everyone all the time. There are some steps you can take to ensure the scheduling process is fair.
The first step is to set appropriate expectations. It is critical for the group leader and the staff member making the schedule to help each group member understand the enormous challenges that come with scheduling.
Providers who understand the difficulties of scheduling will be more understanding and accommodating in their requests.
The second step is to establish and clearly state the rules of engagement. For example, be explicit in explaining the rules for submitting requests and the deadline for requests. Avoid misconceptions by stating when the final schedule will be revealed.
The last step is to clearly state how to handle requests for schedule changes. Many hospitalist groups keep track of who works which holidays so the distribution of work on holidays is fair from year to year.
I have one last suggestion. Consider rotating the job of scheduling so everyone understands firsthand the challenges of the job. To entice people to assume this responsibility, the job should come with remuneration—either salary support and/or preference in choosing their own holiday schedule.
Of course, recognize that not everyone will want the job or be good at it. An effective group leader helps individuals identify opportunities and helps them succeed.
Foreign Medical Grads
Question: What’s your opinion on the effect of foreign medical graduates in the U.S.?
IMG in Cincinnati
Dr. Hospitalist responds: The U.S. healthcare system would be quite different without foreign (aka international) medical graduates (IMGs), who play important clinical, educational, administrative, and research roles.
Some physicians and patients believe medical education outside this country is inferior. In some cases, they are correct—in others, they could not be more wrong. Medical education outside this country varies in standards and curricula.
Many people are not aware that IMGs who wish to enter an Accreditation Council for Graduate Medical Education residency of fellowship program in the United States must have Educational Commission for Foreign Medical Graduates (ECFMG) certification. ECFMG certification requires the applicant to pass a series of examinations, including United States Medical Licensing Examination (USMLE) Steps 1 and 2.
ECFMG certification is also required before an applicant can take Step 3 of the USMLE and is required before a physician can obtain an unrestricted license to practice medicine in the United States.
I suspect some IMGs face discrimination in this country because some may speak with an accent. But truth be told, the United States healthcare system could not exist without the contributions made by IMGs. TH
The Boutique Lure
Question: I recently received a brochure in the mail about a hospital that caters only to cardiac patients. While I think this job sounds intriguing, I’m concerned that this may be a boutique hospital. What do you think of the movement toward boutique hospitals? Do you think they are ethical?
Curious in Boston
Dr. Hospitalist responds: Boutique or specialty hospitals have been hotly debated among healthcare policymakers over the past few years. Compared with the number of general hospitals, the numbers of specialty hospitals—typically those that focus on cardiac, orthopedic, surgical, and women’s procedures—are small.
A Government Accounting Office (GAO) report in 2003 identified 100 such hospitals in the country. More than two-thirds of the hospitals are in seven states (Arizona, California, Kansas, Oklahoma, Louisiana, South Dakota, and Texas).
The GAO found that compared with general hospitals, specialty hospitals are “much less likely to have emergency departments, treated smaller percentages of Medicaid patients and derived a smaller share of their revenues from inpatient services.” Although small, this is a growing segment of the healthcare industry.
Specialty hospitals are controversial because many are for-profit and often owned by some of the physicians who work at the hospital. Specialty hospital supporters believe competition between specialty and general hospitals for services can lower costs and improve care.
A 2005 Medicare Payment Advisory Commission study found that physician-owned specialty hospitals decreased lengths of stay but didn’t lower costs for Medicare patients.
In general, specialty hospitals treated less-severe cases and tended to have lower numbers of Medicaid patients than community hospitals.
Specialty care hospital critics are concerned that specialty hospitals take care of the most profitable patients (those who are less ill) and leave the general hospital with the sicker patients who incur higher costs.
They fear growing numbers of specialty hospitals will make it financially difficult for general hospitals to meet all of a community’s needs, including charity care and emergency services.
Critics are also concerned that physician ownership of specialty hospitals could affect physicians’ clinical behavior by driving inappropriate referrals.
You may remember that the federal Stark law (named after Rep. Peter Stark, D-Calif.) generally prohibits physicians from referring Medicare patients for healthcare services to facilities where they have financial interests.
This law was enacted after several studies demonstrated that physicians with ownership interest in clinical laboratories, diagnostic imaging centers, and physical therapy providers made more referrals to these centers and ordered more services at higher costs.
The Stark law lets physicians who have an ownership interest in an entire hospital and are authorized to perform services there to refer patients to that hospital.
As you consider this opportunity, further investigate the risks, benefits, and potential effect of the specialty hospital on your community and our healthcare system.
Holiday Dilemma
Question: I just took over scheduling for our hospitalist group. I’ve been practicing nearly two years and am wondering how to staff holidays. I’m finding it difficult handling the multiple requests for Thanksgiving, Christmas, and New Year’s Eve. Do you know of any innovative scheduling techniques?
Schedule Grinch in Philadelphia
Dr. Hospitalist responds: Congratulations on your new responsibility! I write this with my tongue firmly planted in my cheek. As you now realize, completing the schedule is not easy.
Unfortunately, most hospitalists don’t recognize the enormous challenge one faces in filling the schedule until they are given the task.
Unless you were a chief medical resident, you probably didn’t learn or practice scheduling in the course of your medical training. Inevitably, everyone wants and expects to get their choice of days off. Of course, that is rarely possible.
How do you make everyone happy? It is important to recognize that making everyone happy every time is not possible. But it is possible and important to be fair to everyone all the time. There are some steps you can take to ensure the scheduling process is fair.
The first step is to set appropriate expectations. It is critical for the group leader and the staff member making the schedule to help each group member understand the enormous challenges that come with scheduling.
Providers who understand the difficulties of scheduling will be more understanding and accommodating in their requests.
The second step is to establish and clearly state the rules of engagement. For example, be explicit in explaining the rules for submitting requests and the deadline for requests. Avoid misconceptions by stating when the final schedule will be revealed.
The last step is to clearly state how to handle requests for schedule changes. Many hospitalist groups keep track of who works which holidays so the distribution of work on holidays is fair from year to year.
I have one last suggestion. Consider rotating the job of scheduling so everyone understands firsthand the challenges of the job. To entice people to assume this responsibility, the job should come with remuneration—either salary support and/or preference in choosing their own holiday schedule.
Of course, recognize that not everyone will want the job or be good at it. An effective group leader helps individuals identify opportunities and helps them succeed.
Foreign Medical Grads
Question: What’s your opinion on the effect of foreign medical graduates in the U.S.?
IMG in Cincinnati
Dr. Hospitalist responds: The U.S. healthcare system would be quite different without foreign (aka international) medical graduates (IMGs), who play important clinical, educational, administrative, and research roles.
Some physicians and patients believe medical education outside this country is inferior. In some cases, they are correct—in others, they could not be more wrong. Medical education outside this country varies in standards and curricula.
Many people are not aware that IMGs who wish to enter an Accreditation Council for Graduate Medical Education residency of fellowship program in the United States must have Educational Commission for Foreign Medical Graduates (ECFMG) certification. ECFMG certification requires the applicant to pass a series of examinations, including United States Medical Licensing Examination (USMLE) Steps 1 and 2.
ECFMG certification is also required before an applicant can take Step 3 of the USMLE and is required before a physician can obtain an unrestricted license to practice medicine in the United States.
I suspect some IMGs face discrimination in this country because some may speak with an accent. But truth be told, the United States healthcare system could not exist without the contributions made by IMGs. TH
The Boutique Lure
Question: I recently received a brochure in the mail about a hospital that caters only to cardiac patients. While I think this job sounds intriguing, I’m concerned that this may be a boutique hospital. What do you think of the movement toward boutique hospitals? Do you think they are ethical?
Curious in Boston
Dr. Hospitalist responds: Boutique or specialty hospitals have been hotly debated among healthcare policymakers over the past few years. Compared with the number of general hospitals, the numbers of specialty hospitals—typically those that focus on cardiac, orthopedic, surgical, and women’s procedures—are small.
A Government Accounting Office (GAO) report in 2003 identified 100 such hospitals in the country. More than two-thirds of the hospitals are in seven states (Arizona, California, Kansas, Oklahoma, Louisiana, South Dakota, and Texas).
The GAO found that compared with general hospitals, specialty hospitals are “much less likely to have emergency departments, treated smaller percentages of Medicaid patients and derived a smaller share of their revenues from inpatient services.” Although small, this is a growing segment of the healthcare industry.
Specialty hospitals are controversial because many are for-profit and often owned by some of the physicians who work at the hospital. Specialty hospital supporters believe competition between specialty and general hospitals for services can lower costs and improve care.
A 2005 Medicare Payment Advisory Commission study found that physician-owned specialty hospitals decreased lengths of stay but didn’t lower costs for Medicare patients.
In general, specialty hospitals treated less-severe cases and tended to have lower numbers of Medicaid patients than community hospitals.
Specialty care hospital critics are concerned that specialty hospitals take care of the most profitable patients (those who are less ill) and leave the general hospital with the sicker patients who incur higher costs.
They fear growing numbers of specialty hospitals will make it financially difficult for general hospitals to meet all of a community’s needs, including charity care and emergency services.
Critics are also concerned that physician ownership of specialty hospitals could affect physicians’ clinical behavior by driving inappropriate referrals.
You may remember that the federal Stark law (named after Rep. Peter Stark, D-Calif.) generally prohibits physicians from referring Medicare patients for healthcare services to facilities where they have financial interests.
This law was enacted after several studies demonstrated that physicians with ownership interest in clinical laboratories, diagnostic imaging centers, and physical therapy providers made more referrals to these centers and ordered more services at higher costs.
The Stark law lets physicians who have an ownership interest in an entire hospital and are authorized to perform services there to refer patients to that hospital.
As you consider this opportunity, further investigate the risks, benefits, and potential effect of the specialty hospital on your community and our healthcare system.
Holiday Dilemma
Question: I just took over scheduling for our hospitalist group. I’ve been practicing nearly two years and am wondering how to staff holidays. I’m finding it difficult handling the multiple requests for Thanksgiving, Christmas, and New Year’s Eve. Do you know of any innovative scheduling techniques?
Schedule Grinch in Philadelphia
Dr. Hospitalist responds: Congratulations on your new responsibility! I write this with my tongue firmly planted in my cheek. As you now realize, completing the schedule is not easy.
Unfortunately, most hospitalists don’t recognize the enormous challenge one faces in filling the schedule until they are given the task.
Unless you were a chief medical resident, you probably didn’t learn or practice scheduling in the course of your medical training. Inevitably, everyone wants and expects to get their choice of days off. Of course, that is rarely possible.
How do you make everyone happy? It is important to recognize that making everyone happy every time is not possible. But it is possible and important to be fair to everyone all the time. There are some steps you can take to ensure the scheduling process is fair.
The first step is to set appropriate expectations. It is critical for the group leader and the staff member making the schedule to help each group member understand the enormous challenges that come with scheduling.
Providers who understand the difficulties of scheduling will be more understanding and accommodating in their requests.
The second step is to establish and clearly state the rules of engagement. For example, be explicit in explaining the rules for submitting requests and the deadline for requests. Avoid misconceptions by stating when the final schedule will be revealed.
The last step is to clearly state how to handle requests for schedule changes. Many hospitalist groups keep track of who works which holidays so the distribution of work on holidays is fair from year to year.
I have one last suggestion. Consider rotating the job of scheduling so everyone understands firsthand the challenges of the job. To entice people to assume this responsibility, the job should come with remuneration—either salary support and/or preference in choosing their own holiday schedule.
Of course, recognize that not everyone will want the job or be good at it. An effective group leader helps individuals identify opportunities and helps them succeed.
Foreign Medical Grads
Question: What’s your opinion on the effect of foreign medical graduates in the U.S.?
IMG in Cincinnati
Dr. Hospitalist responds: The U.S. healthcare system would be quite different without foreign (aka international) medical graduates (IMGs), who play important clinical, educational, administrative, and research roles.
Some physicians and patients believe medical education outside this country is inferior. In some cases, they are correct—in others, they could not be more wrong. Medical education outside this country varies in standards and curricula.
Many people are not aware that IMGs who wish to enter an Accreditation Council for Graduate Medical Education residency of fellowship program in the United States must have Educational Commission for Foreign Medical Graduates (ECFMG) certification. ECFMG certification requires the applicant to pass a series of examinations, including United States Medical Licensing Examination (USMLE) Steps 1 and 2.
ECFMG certification is also required before an applicant can take Step 3 of the USMLE and is required before a physician can obtain an unrestricted license to practice medicine in the United States.
I suspect some IMGs face discrimination in this country because some may speak with an accent. But truth be told, the United States healthcare system could not exist without the contributions made by IMGs. TH
Haggle With the Hospital

Negotiating support from the hospital where you practice is one of the most critical skills you can learn. I am often asked, “How can our group prove our value to the hospital so we can get the support we need?” The best approach is the same whether you are a practice employed by the hospital or a separate legal entity that contracts with the hospital.
There are many valuable sources of guidance regarding the best way to negotiate any important agreement, including a book I recommend, Getting to Yes. I suggest you read such a book if you want to be a better negotiator. But here I want to highlight some features of negotiations between a hospital medicine practice and a hospital that such sources won’t specifically address.
Clearly this is complicated, and different situations call for different strategies. These are generalizations worth thinking about in any situation.
Know what is important to the hospital. I often hear hospitalists say, “We want to attend to the things that are important to the hospital, but we don’t know what those things are.” If that is really the case, the communication between the hospital and hospitalists must be awfully poor—and there is an opportunity for the hospitalists to improve it. It is worth the time and energy required to know what is on the mind of the hospital’s leadership. It may be as simple as having a person-to-person conversation with one or more hospital leaders about what they see as the institution’s most important goals—and how your practice could help achieve them. You need to be sure and understand the particulars at your hospital, but the topics below are on the mind of most executives.
Propose using additional funding to ensure adequate staffing, not raises for existing doctors. In the current environment of difficult recruiting, hospital executives are usually far more inclined to pay for increased staffing than worry about whether you need a raise just because you deserve it. So it is usually much more effective to tell the hospital, “Our practice needs more money so we can add doctors and more fully meet the demand for our services.” Much less effective is saying, “We [existing hospitalists] are working so hard that if we don’t get more money we’re going to quit.”
While the latter may be true, a hospital executive is much more likely to respond positively to paying for increased manpower so the existing doctors won’t have to continue working at unreasonably high workloads, rather than to providing money to support a raise for doctors already working unreasonably hard.
Propose additional resources to support quality improvement, and consider sharing some financial risk. Most hospital executives care about their hospital’s performance on quality measures and are willing to provide money to improve it. You might win more financial support if it is contingent on your group improving performance on quality measures.
You could propose that the hospital make additional money available to encourage and reward improved performance. You could even put existing financial support at risk and ask the hospital to match it. In other words, you could say you will contribute $5,000 or $10,000 of the money currently provided annually by the hospital per full-time equivalent hospitalist into a pool matched dollar for dollar (or some other ratio) by the hospital. Your group would get less total financial support (i.e., lose the funds put at risk) if quality doesn’t improve, but get more support if performance improved by an agreed-upon amount. A willingness to share financial risk demonstrates your commitment to success and can be compelling to the hospital.
Know your data. Hard data are far more effective than anecdotes when trying to convince the hospital of your practice’s value. Trumpet your successes, but remember that same executive will probably hear from 10 others in the same week that spending huge sums of money on their product or service will dramatically improve the hospital’s bottom line. If you’re trying to convince the hospital that every dollar spent to support your practice will provide an attractive return on investment, you need hard data to prove it.
It would be best if you could independently collect this data. But in most cases, you will have to rely on data the hospital has collected. It’s worthwhile to insist on routine reports (e.g., monthly, or no less than quarterly) from the hospital summarizing your group’s performance on quality and financial metrics (CMS core measures, patient satisfaction, cost per case). This data will be critical to you when you negotiate financial support from the hospital.
You should also have data about other hospitalist practices, such as results from the 2005-06 “SHM Survey of Hospitalist Productivity and Compensation” and other sources I discussed in a recent column (July 2007, p. 73). And if you’re able to get reliable data about other practices in your local marketplace (i.e., something more significant than just what you heard through the grapevine), be sure to share that information as well.
Agree to conditions carefully. Don’t agree to do things you would be unhappy doing just because it might help get more financial support from the hospital. Executives know it is bad business to pay people more money to get them to keep doing something they don’t want to do. Such an agreement usually leads to the hospitalists asking for more money each year to continue providing the service—and the quality of the service is often sub par if it’s something the hospitalists really don’t want to do (even if paid well to do it).
Stay focused on hospital performance—even in areas not specifically governed by your contractual relationship. Many or most hospitals that employ hospitalists assume all the financial risk for the practice. That is, the hospital agrees to make up the difference between collected professional fee revenue and the cost of operating the practice.
If the doctors underdocument and downcode, or are not compulsive about ensuring that their charges get to the billing agent, fee collections will suffer—and the hospital will end up having to pay more to support the practice.
If you are in such a situation, you should ensure that you’re helping to support optimal documentation, coding, billing, and collection practices—even if it won’t increase your paycheck but simply saves the hospital money. This will increase your chance of getting the hospital to increase financial support of your practice.
Remember your financial support isn’t a one-time negotiation; it is part of an ongoing relationship. In some negotiations, such as buying a car from a stranger, it seems reasonable to use any leverage most favorable for you. After all, you’re unlikely to ever interact with that person again. A hospitalist practice might compel the hospital to provide more support by threatening to quit suddenly. Yet it is usually a bad idea to do this because it can severely damage the long-term relationship.
Further, if you make it clear you’re going to quit unless you get more money, the hospital is in a tough spot. While the hospital may not want to lose you, any executive will realize that by making such a threat you probably aren’t committed to staying long even if you do get more financial support. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management-consulting firm. This column represents his views and is not intended to reflect an official position of SHM.
Negotiating support from the hospital where you practice is one of the most critical skills you can learn. I am often asked, “How can our group prove our value to the hospital so we can get the support we need?” The best approach is the same whether you are a practice employed by the hospital or a separate legal entity that contracts with the hospital.
There are many valuable sources of guidance regarding the best way to negotiate any important agreement, including a book I recommend, Getting to Yes. I suggest you read such a book if you want to be a better negotiator. But here I want to highlight some features of negotiations between a hospital medicine practice and a hospital that such sources won’t specifically address.
Clearly this is complicated, and different situations call for different strategies. These are generalizations worth thinking about in any situation.
Know what is important to the hospital. I often hear hospitalists say, “We want to attend to the things that are important to the hospital, but we don’t know what those things are.” If that is really the case, the communication between the hospital and hospitalists must be awfully poor—and there is an opportunity for the hospitalists to improve it. It is worth the time and energy required to know what is on the mind of the hospital’s leadership. It may be as simple as having a person-to-person conversation with one or more hospital leaders about what they see as the institution’s most important goals—and how your practice could help achieve them. You need to be sure and understand the particulars at your hospital, but the topics below are on the mind of most executives.
Propose using additional funding to ensure adequate staffing, not raises for existing doctors. In the current environment of difficult recruiting, hospital executives are usually far more inclined to pay for increased staffing than worry about whether you need a raise just because you deserve it. So it is usually much more effective to tell the hospital, “Our practice needs more money so we can add doctors and more fully meet the demand for our services.” Much less effective is saying, “We [existing hospitalists] are working so hard that if we don’t get more money we’re going to quit.”
While the latter may be true, a hospital executive is much more likely to respond positively to paying for increased manpower so the existing doctors won’t have to continue working at unreasonably high workloads, rather than to providing money to support a raise for doctors already working unreasonably hard.
Propose additional resources to support quality improvement, and consider sharing some financial risk. Most hospital executives care about their hospital’s performance on quality measures and are willing to provide money to improve it. You might win more financial support if it is contingent on your group improving performance on quality measures.
You could propose that the hospital make additional money available to encourage and reward improved performance. You could even put existing financial support at risk and ask the hospital to match it. In other words, you could say you will contribute $5,000 or $10,000 of the money currently provided annually by the hospital per full-time equivalent hospitalist into a pool matched dollar for dollar (or some other ratio) by the hospital. Your group would get less total financial support (i.e., lose the funds put at risk) if quality doesn’t improve, but get more support if performance improved by an agreed-upon amount. A willingness to share financial risk demonstrates your commitment to success and can be compelling to the hospital.
Know your data. Hard data are far more effective than anecdotes when trying to convince the hospital of your practice’s value. Trumpet your successes, but remember that same executive will probably hear from 10 others in the same week that spending huge sums of money on their product or service will dramatically improve the hospital’s bottom line. If you’re trying to convince the hospital that every dollar spent to support your practice will provide an attractive return on investment, you need hard data to prove it.
It would be best if you could independently collect this data. But in most cases, you will have to rely on data the hospital has collected. It’s worthwhile to insist on routine reports (e.g., monthly, or no less than quarterly) from the hospital summarizing your group’s performance on quality and financial metrics (CMS core measures, patient satisfaction, cost per case). This data will be critical to you when you negotiate financial support from the hospital.
You should also have data about other hospitalist practices, such as results from the 2005-06 “SHM Survey of Hospitalist Productivity and Compensation” and other sources I discussed in a recent column (July 2007, p. 73). And if you’re able to get reliable data about other practices in your local marketplace (i.e., something more significant than just what you heard through the grapevine), be sure to share that information as well.
Agree to conditions carefully. Don’t agree to do things you would be unhappy doing just because it might help get more financial support from the hospital. Executives know it is bad business to pay people more money to get them to keep doing something they don’t want to do. Such an agreement usually leads to the hospitalists asking for more money each year to continue providing the service—and the quality of the service is often sub par if it’s something the hospitalists really don’t want to do (even if paid well to do it).
Stay focused on hospital performance—even in areas not specifically governed by your contractual relationship. Many or most hospitals that employ hospitalists assume all the financial risk for the practice. That is, the hospital agrees to make up the difference between collected professional fee revenue and the cost of operating the practice.
If the doctors underdocument and downcode, or are not compulsive about ensuring that their charges get to the billing agent, fee collections will suffer—and the hospital will end up having to pay more to support the practice.
If you are in such a situation, you should ensure that you’re helping to support optimal documentation, coding, billing, and collection practices—even if it won’t increase your paycheck but simply saves the hospital money. This will increase your chance of getting the hospital to increase financial support of your practice.
Remember your financial support isn’t a one-time negotiation; it is part of an ongoing relationship. In some negotiations, such as buying a car from a stranger, it seems reasonable to use any leverage most favorable for you. After all, you’re unlikely to ever interact with that person again. A hospitalist practice might compel the hospital to provide more support by threatening to quit suddenly. Yet it is usually a bad idea to do this because it can severely damage the long-term relationship.
Further, if you make it clear you’re going to quit unless you get more money, the hospital is in a tough spot. While the hospital may not want to lose you, any executive will realize that by making such a threat you probably aren’t committed to staying long even if you do get more financial support. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management-consulting firm. This column represents his views and is not intended to reflect an official position of SHM.
Negotiating support from the hospital where you practice is one of the most critical skills you can learn. I am often asked, “How can our group prove our value to the hospital so we can get the support we need?” The best approach is the same whether you are a practice employed by the hospital or a separate legal entity that contracts with the hospital.
There are many valuable sources of guidance regarding the best way to negotiate any important agreement, including a book I recommend, Getting to Yes. I suggest you read such a book if you want to be a better negotiator. But here I want to highlight some features of negotiations between a hospital medicine practice and a hospital that such sources won’t specifically address.
Clearly this is complicated, and different situations call for different strategies. These are generalizations worth thinking about in any situation.
Know what is important to the hospital. I often hear hospitalists say, “We want to attend to the things that are important to the hospital, but we don’t know what those things are.” If that is really the case, the communication between the hospital and hospitalists must be awfully poor—and there is an opportunity for the hospitalists to improve it. It is worth the time and energy required to know what is on the mind of the hospital’s leadership. It may be as simple as having a person-to-person conversation with one or more hospital leaders about what they see as the institution’s most important goals—and how your practice could help achieve them. You need to be sure and understand the particulars at your hospital, but the topics below are on the mind of most executives.
Propose using additional funding to ensure adequate staffing, not raises for existing doctors. In the current environment of difficult recruiting, hospital executives are usually far more inclined to pay for increased staffing than worry about whether you need a raise just because you deserve it. So it is usually much more effective to tell the hospital, “Our practice needs more money so we can add doctors and more fully meet the demand for our services.” Much less effective is saying, “We [existing hospitalists] are working so hard that if we don’t get more money we’re going to quit.”
While the latter may be true, a hospital executive is much more likely to respond positively to paying for increased manpower so the existing doctors won’t have to continue working at unreasonably high workloads, rather than to providing money to support a raise for doctors already working unreasonably hard.
Propose additional resources to support quality improvement, and consider sharing some financial risk. Most hospital executives care about their hospital’s performance on quality measures and are willing to provide money to improve it. You might win more financial support if it is contingent on your group improving performance on quality measures.
You could propose that the hospital make additional money available to encourage and reward improved performance. You could even put existing financial support at risk and ask the hospital to match it. In other words, you could say you will contribute $5,000 or $10,000 of the money currently provided annually by the hospital per full-time equivalent hospitalist into a pool matched dollar for dollar (or some other ratio) by the hospital. Your group would get less total financial support (i.e., lose the funds put at risk) if quality doesn’t improve, but get more support if performance improved by an agreed-upon amount. A willingness to share financial risk demonstrates your commitment to success and can be compelling to the hospital.
Know your data. Hard data are far more effective than anecdotes when trying to convince the hospital of your practice’s value. Trumpet your successes, but remember that same executive will probably hear from 10 others in the same week that spending huge sums of money on their product or service will dramatically improve the hospital’s bottom line. If you’re trying to convince the hospital that every dollar spent to support your practice will provide an attractive return on investment, you need hard data to prove it.
It would be best if you could independently collect this data. But in most cases, you will have to rely on data the hospital has collected. It’s worthwhile to insist on routine reports (e.g., monthly, or no less than quarterly) from the hospital summarizing your group’s performance on quality and financial metrics (CMS core measures, patient satisfaction, cost per case). This data will be critical to you when you negotiate financial support from the hospital.
You should also have data about other hospitalist practices, such as results from the 2005-06 “SHM Survey of Hospitalist Productivity and Compensation” and other sources I discussed in a recent column (July 2007, p. 73). And if you’re able to get reliable data about other practices in your local marketplace (i.e., something more significant than just what you heard through the grapevine), be sure to share that information as well.
Agree to conditions carefully. Don’t agree to do things you would be unhappy doing just because it might help get more financial support from the hospital. Executives know it is bad business to pay people more money to get them to keep doing something they don’t want to do. Such an agreement usually leads to the hospitalists asking for more money each year to continue providing the service—and the quality of the service is often sub par if it’s something the hospitalists really don’t want to do (even if paid well to do it).
Stay focused on hospital performance—even in areas not specifically governed by your contractual relationship. Many or most hospitals that employ hospitalists assume all the financial risk for the practice. That is, the hospital agrees to make up the difference between collected professional fee revenue and the cost of operating the practice.
If the doctors underdocument and downcode, or are not compulsive about ensuring that their charges get to the billing agent, fee collections will suffer—and the hospital will end up having to pay more to support the practice.
If you are in such a situation, you should ensure that you’re helping to support optimal documentation, coding, billing, and collection practices—even if it won’t increase your paycheck but simply saves the hospital money. This will increase your chance of getting the hospital to increase financial support of your practice.
Remember your financial support isn’t a one-time negotiation; it is part of an ongoing relationship. In some negotiations, such as buying a car from a stranger, it seems reasonable to use any leverage most favorable for you. After all, you’re unlikely to ever interact with that person again. A hospitalist practice might compel the hospital to provide more support by threatening to quit suddenly. Yet it is usually a bad idea to do this because it can severely damage the long-term relationship.
Further, if you make it clear you’re going to quit unless you get more money, the hospital is in a tough spot. While the hospital may not want to lose you, any executive will realize that by making such a threat you probably aren’t committed to staying long even if you do get more financial support. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management-consulting firm. This column represents his views and is not intended to reflect an official position of SHM.
End-of-Life Predictions

The July 26 New England Journal of Medicine contained several articles of interest for hospitalists: A trial of steroids for bronchiolitis, mortality associated with type B aortic dissections, cardiovascular outcomes in patients using rofecoxib, implications of our social networks on obesity, and a terrific review of methicillin-resistant Staph aureus in soft-tissue infections.
But all these were trumped in the media by Oscar the cat.1
National Public Radio, CNN, Fox, and the BBC all covered the story about the cantankerous cat that could predict death in a community nursing home’s third-floor dementia unit with Grim Reaper-like proficiency. The 2-year-old cat was adopted and raised from kittenhood by staff members at the Steere House Nursing and Rehabilitation Center in Providence, R.I.
Nursing staff began noticing that Oscar would curl up in bed next to patients who had only hours to live. Oscar was so adept at predicting death that the nursing staff began using his prophesies to alert family members of an impending demise. Oscar rounds daily, waiting for closed doors to open when necessary and employing somewhat less-sophisticated methods than his human colleagues—namely observing and sniffing. However, this “cat scan” appears to serve as an unprecedented augur, accurately predicting the death of 25 nursing home residents.
Why all the fuss about this predictive puss in boots? To be sure it’s an intriguing story. But why does the public care so much that Oscar the cat can now be found in Wikipedia—and why should the average hospitalist care about a prognosticating cat?
The answer lies in the medical profession’s dreadful lack of ability to predict patients’ survival at the end of life. Multiple studies have shown physicians are terrible at predicting survival, most often in an overly optimistic manner. A paper in the British Medical Journal examined the ability of 343 doctors to estimate the survival of 468 patients at the time of referral to hospice.2 Only 20% of physicians were able to accurately prognosticate the time of death to within 33% of the actual survival. While median survival was 24 days doctors, on average, predicted patients would live 5.3 times longer than they did. Interestingly, the longer the doctor knew the patient the more likely they were to predict wrongly.
Most seriously ill patients value prognostic information more than they do information about therapeutic options. It is a central determinant in how patients and families make end-of-life decisions. The fact that we seem to systematically provide overly optimistic predictions has several important downstream effects.
Unduly optimistic predictions likely delay referral to palliative care providers and hospice. Doctors generally believe patients should receive hospice care for several months before death. However, patients typically receive this care for less than a month and in many cases only a few hours. Our inability to realistically predict survival most likely plays into this discrepancy and negatively affects our patients’ quality of life.
Second, our consistently overestimated predictions likely translate into patients making inappropriate or counterproductive end-of-life decisions.
We’ve all experienced the patient who continues to push for obviously futile care despite our attempts to nudge them toward a palliative approach. Yet it’s easy to see why patients who believe they have six months to live would push for more aggressive treatments. If they knew they had six weeks to live, they might choose more palliative options.
Finally, hospitalists are increasingly under the gun to decrease length of stay (LOS) and contain costs. It is estimated that more than 25% of Medicare costs (approximately $88 billion a year) are associated with care in the last year of life, much of it in the hospital. While several studies have shown that early palliative care intervention reduces LOS and cost of care, overly optimistic predictions make it less likely these timely referrals will be made.
The development of the hospitalist model, with its fractured approach to care, might provide an opportunity to improve end-of-life prognostication. Having a strong, long-lasting relationship with a patient appears to be an important predictor of inaccurate prognosis. It isn’t hard to imagine that a provider with a long relationship with a patient might have a more difficult time acknowledging a patient’s poor outcome or unwittingly be less likely to squelch a patient’s hope with a poor prognosis.
We can take advantage of the inherent discontinuities of the hospitalist model as well as the severity and immediacy of the patient’s acute illness to not only proffer an end-of-life prediction but contextualize it for the patient. This, of course, needs to be done in a sensitive manner that recognizes our brief role in their care and, as such, is most often best managed in concert with the patient’s primary care provider.
The promise of the hospital medicine movement is that we can do it better and cheaper. This is a tall order indeed. While the hospitalist model has improved efficiency and quality, future improvements will require us to adopt and develop new efficiencies and better systems of care.
It is in this vein that I believe we can and should be able to improve end-of-life care. An early salvo in this front can be a dedicated and systematic push to improve end-of-life prognostication and its myriad downstream effects. This will require a conscientious effort, more formal education, and better predictive tools. As hospitalists, we are perfectly positioned to lead these efforts. The other alternative may be to adopt more cats into our multidisciplinary team. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver and Health Sciences Center, where he serves as director of the Hospital Medicine Program, Inpatient Clinical Services in the Department of Medicine, and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Dosa DA. A day in the life of Oscar the cat. N Engl J Med. 2007;357(4):328-329.
- Christakis NA, Lamont EB. Extent and determinants of error in doctors’ prognoses in terminally ill patients: prospective cohort study. BMJ. 2000;320:469-472.
The July 26 New England Journal of Medicine contained several articles of interest for hospitalists: A trial of steroids for bronchiolitis, mortality associated with type B aortic dissections, cardiovascular outcomes in patients using rofecoxib, implications of our social networks on obesity, and a terrific review of methicillin-resistant Staph aureus in soft-tissue infections.
But all these were trumped in the media by Oscar the cat.1
National Public Radio, CNN, Fox, and the BBC all covered the story about the cantankerous cat that could predict death in a community nursing home’s third-floor dementia unit with Grim Reaper-like proficiency. The 2-year-old cat was adopted and raised from kittenhood by staff members at the Steere House Nursing and Rehabilitation Center in Providence, R.I.
Nursing staff began noticing that Oscar would curl up in bed next to patients who had only hours to live. Oscar was so adept at predicting death that the nursing staff began using his prophesies to alert family members of an impending demise. Oscar rounds daily, waiting for closed doors to open when necessary and employing somewhat less-sophisticated methods than his human colleagues—namely observing and sniffing. However, this “cat scan” appears to serve as an unprecedented augur, accurately predicting the death of 25 nursing home residents.
Why all the fuss about this predictive puss in boots? To be sure it’s an intriguing story. But why does the public care so much that Oscar the cat can now be found in Wikipedia—and why should the average hospitalist care about a prognosticating cat?
The answer lies in the medical profession’s dreadful lack of ability to predict patients’ survival at the end of life. Multiple studies have shown physicians are terrible at predicting survival, most often in an overly optimistic manner. A paper in the British Medical Journal examined the ability of 343 doctors to estimate the survival of 468 patients at the time of referral to hospice.2 Only 20% of physicians were able to accurately prognosticate the time of death to within 33% of the actual survival. While median survival was 24 days doctors, on average, predicted patients would live 5.3 times longer than they did. Interestingly, the longer the doctor knew the patient the more likely they were to predict wrongly.
Most seriously ill patients value prognostic information more than they do information about therapeutic options. It is a central determinant in how patients and families make end-of-life decisions. The fact that we seem to systematically provide overly optimistic predictions has several important downstream effects.
Unduly optimistic predictions likely delay referral to palliative care providers and hospice. Doctors generally believe patients should receive hospice care for several months before death. However, patients typically receive this care for less than a month and in many cases only a few hours. Our inability to realistically predict survival most likely plays into this discrepancy and negatively affects our patients’ quality of life.
Second, our consistently overestimated predictions likely translate into patients making inappropriate or counterproductive end-of-life decisions.
We’ve all experienced the patient who continues to push for obviously futile care despite our attempts to nudge them toward a palliative approach. Yet it’s easy to see why patients who believe they have six months to live would push for more aggressive treatments. If they knew they had six weeks to live, they might choose more palliative options.
Finally, hospitalists are increasingly under the gun to decrease length of stay (LOS) and contain costs. It is estimated that more than 25% of Medicare costs (approximately $88 billion a year) are associated with care in the last year of life, much of it in the hospital. While several studies have shown that early palliative care intervention reduces LOS and cost of care, overly optimistic predictions make it less likely these timely referrals will be made.
The development of the hospitalist model, with its fractured approach to care, might provide an opportunity to improve end-of-life prognostication. Having a strong, long-lasting relationship with a patient appears to be an important predictor of inaccurate prognosis. It isn’t hard to imagine that a provider with a long relationship with a patient might have a more difficult time acknowledging a patient’s poor outcome or unwittingly be less likely to squelch a patient’s hope with a poor prognosis.
We can take advantage of the inherent discontinuities of the hospitalist model as well as the severity and immediacy of the patient’s acute illness to not only proffer an end-of-life prediction but contextualize it for the patient. This, of course, needs to be done in a sensitive manner that recognizes our brief role in their care and, as such, is most often best managed in concert with the patient’s primary care provider.
The promise of the hospital medicine movement is that we can do it better and cheaper. This is a tall order indeed. While the hospitalist model has improved efficiency and quality, future improvements will require us to adopt and develop new efficiencies and better systems of care.
It is in this vein that I believe we can and should be able to improve end-of-life care. An early salvo in this front can be a dedicated and systematic push to improve end-of-life prognostication and its myriad downstream effects. This will require a conscientious effort, more formal education, and better predictive tools. As hospitalists, we are perfectly positioned to lead these efforts. The other alternative may be to adopt more cats into our multidisciplinary team. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver and Health Sciences Center, where he serves as director of the Hospital Medicine Program, Inpatient Clinical Services in the Department of Medicine, and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Dosa DA. A day in the life of Oscar the cat. N Engl J Med. 2007;357(4):328-329.
- Christakis NA, Lamont EB. Extent and determinants of error in doctors’ prognoses in terminally ill patients: prospective cohort study. BMJ. 2000;320:469-472.
The July 26 New England Journal of Medicine contained several articles of interest for hospitalists: A trial of steroids for bronchiolitis, mortality associated with type B aortic dissections, cardiovascular outcomes in patients using rofecoxib, implications of our social networks on obesity, and a terrific review of methicillin-resistant Staph aureus in soft-tissue infections.
But all these were trumped in the media by Oscar the cat.1
National Public Radio, CNN, Fox, and the BBC all covered the story about the cantankerous cat that could predict death in a community nursing home’s third-floor dementia unit with Grim Reaper-like proficiency. The 2-year-old cat was adopted and raised from kittenhood by staff members at the Steere House Nursing and Rehabilitation Center in Providence, R.I.
Nursing staff began noticing that Oscar would curl up in bed next to patients who had only hours to live. Oscar was so adept at predicting death that the nursing staff began using his prophesies to alert family members of an impending demise. Oscar rounds daily, waiting for closed doors to open when necessary and employing somewhat less-sophisticated methods than his human colleagues—namely observing and sniffing. However, this “cat scan” appears to serve as an unprecedented augur, accurately predicting the death of 25 nursing home residents.
Why all the fuss about this predictive puss in boots? To be sure it’s an intriguing story. But why does the public care so much that Oscar the cat can now be found in Wikipedia—and why should the average hospitalist care about a prognosticating cat?
The answer lies in the medical profession’s dreadful lack of ability to predict patients’ survival at the end of life. Multiple studies have shown physicians are terrible at predicting survival, most often in an overly optimistic manner. A paper in the British Medical Journal examined the ability of 343 doctors to estimate the survival of 468 patients at the time of referral to hospice.2 Only 20% of physicians were able to accurately prognosticate the time of death to within 33% of the actual survival. While median survival was 24 days doctors, on average, predicted patients would live 5.3 times longer than they did. Interestingly, the longer the doctor knew the patient the more likely they were to predict wrongly.
Most seriously ill patients value prognostic information more than they do information about therapeutic options. It is a central determinant in how patients and families make end-of-life decisions. The fact that we seem to systematically provide overly optimistic predictions has several important downstream effects.
Unduly optimistic predictions likely delay referral to palliative care providers and hospice. Doctors generally believe patients should receive hospice care for several months before death. However, patients typically receive this care for less than a month and in many cases only a few hours. Our inability to realistically predict survival most likely plays into this discrepancy and negatively affects our patients’ quality of life.
Second, our consistently overestimated predictions likely translate into patients making inappropriate or counterproductive end-of-life decisions.
We’ve all experienced the patient who continues to push for obviously futile care despite our attempts to nudge them toward a palliative approach. Yet it’s easy to see why patients who believe they have six months to live would push for more aggressive treatments. If they knew they had six weeks to live, they might choose more palliative options.
Finally, hospitalists are increasingly under the gun to decrease length of stay (LOS) and contain costs. It is estimated that more than 25% of Medicare costs (approximately $88 billion a year) are associated with care in the last year of life, much of it in the hospital. While several studies have shown that early palliative care intervention reduces LOS and cost of care, overly optimistic predictions make it less likely these timely referrals will be made.
The development of the hospitalist model, with its fractured approach to care, might provide an opportunity to improve end-of-life prognostication. Having a strong, long-lasting relationship with a patient appears to be an important predictor of inaccurate prognosis. It isn’t hard to imagine that a provider with a long relationship with a patient might have a more difficult time acknowledging a patient’s poor outcome or unwittingly be less likely to squelch a patient’s hope with a poor prognosis.
We can take advantage of the inherent discontinuities of the hospitalist model as well as the severity and immediacy of the patient’s acute illness to not only proffer an end-of-life prediction but contextualize it for the patient. This, of course, needs to be done in a sensitive manner that recognizes our brief role in their care and, as such, is most often best managed in concert with the patient’s primary care provider.
The promise of the hospital medicine movement is that we can do it better and cheaper. This is a tall order indeed. While the hospitalist model has improved efficiency and quality, future improvements will require us to adopt and develop new efficiencies and better systems of care.
It is in this vein that I believe we can and should be able to improve end-of-life care. An early salvo in this front can be a dedicated and systematic push to improve end-of-life prognostication and its myriad downstream effects. This will require a conscientious effort, more formal education, and better predictive tools. As hospitalists, we are perfectly positioned to lead these efforts. The other alternative may be to adopt more cats into our multidisciplinary team. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver and Health Sciences Center, where he serves as director of the Hospital Medicine Program, Inpatient Clinical Services in the Department of Medicine, and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Dosa DA. A day in the life of Oscar the cat. N Engl J Med. 2007;357(4):328-329.
- Christakis NA, Lamont EB. Extent and determinants of error in doctors’ prognoses in terminally ill patients: prospective cohort study. BMJ. 2000;320:469-472.
Information Deficits

If there is one thing most everyone in healthcare can agree on, it is that too often the information we need is not readily available.
Primary care physicians (PCP) complain that when recently hospitalized patients show up in their office—or, heaven forbid, call the first day after their hospital discharge—they don’t have their discharge information. We often hear that when hospitalists are called to admit an acutely ill patient information is sketchy or incomplete. We hear most hospitalized patients present not only as diagnostic challenges but as “unknowns” with insufficient history and medication information.
A 2006 study by the Common-wealth Fund found that in 32% of outpatient visits or referrals, crucial test results or clinical information were absent and consultation needed to be rescheduled.
In many ways the biggest knock on the hospitalist model is that, despite their better in-house availability, use of resources, or quality of care, hospitalists create another “interruption” in care coordination.
This “voltage drop” didn’t start with hospitalists. It has been around whenever patients are referred to specialists or for surgery—or most procedures, for that matter.
But hospitalists and SHM have seized on this perceived Achilles’ heel and formed coalitions to improve transitions of care and urge better care coordination. While working with many others in medicine, SHM also has had interesting discussions with key change agents not traditionally encountered in healthcare.
With grants from the John Hartford Foundation, SHM has developed state-of-the-art discharge planning tools available on the SHM Web site. And, SHM and Intel have discussed broader strategies for managing information.
In addition, I attended a recent American Hospital Association Leadership Summit and had lunch with Colin Powell, who is active at RevolutionHealth.com—the brainchild of AOL founder Steven Case.
One of RevolutionHealth.com’s projects is to create a widely used personal health record (PHR). This would be a Web database with the patient as the focal point. When a patient has a test, sees a physician, visits an ED, or is hospitalized, that information would flow into an updated record accessible by the patient or physician virtually anywhere, any time.
For hospitalists, this could be a source of complete, up-to-date medication lists, diagnoses, and test results. Hospitalists or case managers could update this PHR at discharge so it is immediately available to PCP or coverage partners, home healthcare providers, or a skilled nursing facility. This type of tool doesn’t require that every physician have an electronic medical record (EMR) and isn’t limited by interoperability issues.
Other strategies are gaining traction. At a recent conference on care coordination sponsored by the American Board of Internal Medicine Foundation (ABIM) in Montreal, Quebec, Canada, Chuck Kilo, MD, MPH, CEO of GreenField Health and The GreenField Group in Portland, Ore., showed how e-mail smoothes transitions and improves information flow.
Those in Dr. Kilo’s practice recognize that, while some professionals may have reservations about e-mails between patients and physicians, there seems less resistance to physicians and hospitals using e-mail to exchange information. With minimal expense and startup costs, PCPs can e-mail patients’ medication records, recent chart notes, and test results to a specialist for referral or a hospitalist for admission.
When the consultant or hospitalist is ready to provide information in the transition back to the PCP, e-mail is a quick solution. It’s not perfect, but it’s immediate. Certainly there are barriers to overcome: HIPAA issues are always important to resolve, and documents converted to PDFs don’t flow into an EMR. But this is a step forward.
These solutions get information to the point of decision when the patient is there and the acute need must be met. For those in the trenches this is good news—a great improvement on the hunt-and-peck paradigm.
In a broader strategic approach, SHM has advocated giving hospitalists a role in defining the standards and measures to be used in assessing performance in transitions of care. In July, SHM worked with the ABIM, the American College of Physicians, the Society of General Internal Medicine, the American Geriatrics Society, and the Agency for Healthcare Research and Quality to develop consensus on transitions-of-care standards. This group included most of the big players in the house of internal medicine as well as representatives from nursing, pharmacy, case management, home health, patients, and families. The American College of Emergency Physicians (ACEP) joined the discourse in August.
At the same time, SHM has been working with the American Medical Association’s Physician Consortium and the National Quality Forum to use standards conceived in consensus to develop measures for transitions of care. The measures would mark either stand-alone performance or performance with specific disease states (e.g., management of diabetes or acute heart failure).
Hospitalists will need resources and tools to give patients the best care and smoothest transitions (and score well on these measures). SHM has developed a Web-based quality-improvement resource room on transitions and continues to work with a broad coalition to improve the discharge process under our Hartford grant.
We add real value for our patients. But our job doesn’t end at the hospital door. Hospitalists recognize their obligation to patients as well those who will assume their care outside the hospital. Whether working on tools with Intel or RevolutionHealth or working with professional societies and organizations charged with developing performance standards and measures, hospitalists and SHM must take an active leadership role.
This is not easy stuff and can’t be solved in one meeting—or even one year.
A few years ago no one was talking much about patient safety, notes past SHM President Bob Wachter, MD, professor of medicine at the University of California, San Francisco, associate chairman of UCSF’s Department of Medicine, and chief of the Medical Service at UCSF Medical Center. That is, until the Institute of Medicine’s 2000 report “To Err Is Human: Building a Safer Health System” and some disastrous medical errors.
Transitions aren’t happening well, and care is sporadic and isolated. This is high on our agenda; SHM and hospitalists are willing to work with any group that will help all of us get closer to a solution. TH
Dr. Wellikson is the CEO of SHM.
If there is one thing most everyone in healthcare can agree on, it is that too often the information we need is not readily available.
Primary care physicians (PCP) complain that when recently hospitalized patients show up in their office—or, heaven forbid, call the first day after their hospital discharge—they don’t have their discharge information. We often hear that when hospitalists are called to admit an acutely ill patient information is sketchy or incomplete. We hear most hospitalized patients present not only as diagnostic challenges but as “unknowns” with insufficient history and medication information.
A 2006 study by the Common-wealth Fund found that in 32% of outpatient visits or referrals, crucial test results or clinical information were absent and consultation needed to be rescheduled.
In many ways the biggest knock on the hospitalist model is that, despite their better in-house availability, use of resources, or quality of care, hospitalists create another “interruption” in care coordination.
This “voltage drop” didn’t start with hospitalists. It has been around whenever patients are referred to specialists or for surgery—or most procedures, for that matter.
But hospitalists and SHM have seized on this perceived Achilles’ heel and formed coalitions to improve transitions of care and urge better care coordination. While working with many others in medicine, SHM also has had interesting discussions with key change agents not traditionally encountered in healthcare.
With grants from the John Hartford Foundation, SHM has developed state-of-the-art discharge planning tools available on the SHM Web site. And, SHM and Intel have discussed broader strategies for managing information.
In addition, I attended a recent American Hospital Association Leadership Summit and had lunch with Colin Powell, who is active at RevolutionHealth.com—the brainchild of AOL founder Steven Case.
One of RevolutionHealth.com’s projects is to create a widely used personal health record (PHR). This would be a Web database with the patient as the focal point. When a patient has a test, sees a physician, visits an ED, or is hospitalized, that information would flow into an updated record accessible by the patient or physician virtually anywhere, any time.
For hospitalists, this could be a source of complete, up-to-date medication lists, diagnoses, and test results. Hospitalists or case managers could update this PHR at discharge so it is immediately available to PCP or coverage partners, home healthcare providers, or a skilled nursing facility. This type of tool doesn’t require that every physician have an electronic medical record (EMR) and isn’t limited by interoperability issues.
Other strategies are gaining traction. At a recent conference on care coordination sponsored by the American Board of Internal Medicine Foundation (ABIM) in Montreal, Quebec, Canada, Chuck Kilo, MD, MPH, CEO of GreenField Health and The GreenField Group in Portland, Ore., showed how e-mail smoothes transitions and improves information flow.
Those in Dr. Kilo’s practice recognize that, while some professionals may have reservations about e-mails between patients and physicians, there seems less resistance to physicians and hospitals using e-mail to exchange information. With minimal expense and startup costs, PCPs can e-mail patients’ medication records, recent chart notes, and test results to a specialist for referral or a hospitalist for admission.
When the consultant or hospitalist is ready to provide information in the transition back to the PCP, e-mail is a quick solution. It’s not perfect, but it’s immediate. Certainly there are barriers to overcome: HIPAA issues are always important to resolve, and documents converted to PDFs don’t flow into an EMR. But this is a step forward.
These solutions get information to the point of decision when the patient is there and the acute need must be met. For those in the trenches this is good news—a great improvement on the hunt-and-peck paradigm.
In a broader strategic approach, SHM has advocated giving hospitalists a role in defining the standards and measures to be used in assessing performance in transitions of care. In July, SHM worked with the ABIM, the American College of Physicians, the Society of General Internal Medicine, the American Geriatrics Society, and the Agency for Healthcare Research and Quality to develop consensus on transitions-of-care standards. This group included most of the big players in the house of internal medicine as well as representatives from nursing, pharmacy, case management, home health, patients, and families. The American College of Emergency Physicians (ACEP) joined the discourse in August.
At the same time, SHM has been working with the American Medical Association’s Physician Consortium and the National Quality Forum to use standards conceived in consensus to develop measures for transitions of care. The measures would mark either stand-alone performance or performance with specific disease states (e.g., management of diabetes or acute heart failure).
Hospitalists will need resources and tools to give patients the best care and smoothest transitions (and score well on these measures). SHM has developed a Web-based quality-improvement resource room on transitions and continues to work with a broad coalition to improve the discharge process under our Hartford grant.
We add real value for our patients. But our job doesn’t end at the hospital door. Hospitalists recognize their obligation to patients as well those who will assume their care outside the hospital. Whether working on tools with Intel or RevolutionHealth or working with professional societies and organizations charged with developing performance standards and measures, hospitalists and SHM must take an active leadership role.
This is not easy stuff and can’t be solved in one meeting—or even one year.
A few years ago no one was talking much about patient safety, notes past SHM President Bob Wachter, MD, professor of medicine at the University of California, San Francisco, associate chairman of UCSF’s Department of Medicine, and chief of the Medical Service at UCSF Medical Center. That is, until the Institute of Medicine’s 2000 report “To Err Is Human: Building a Safer Health System” and some disastrous medical errors.
Transitions aren’t happening well, and care is sporadic and isolated. This is high on our agenda; SHM and hospitalists are willing to work with any group that will help all of us get closer to a solution. TH
Dr. Wellikson is the CEO of SHM.
If there is one thing most everyone in healthcare can agree on, it is that too often the information we need is not readily available.
Primary care physicians (PCP) complain that when recently hospitalized patients show up in their office—or, heaven forbid, call the first day after their hospital discharge—they don’t have their discharge information. We often hear that when hospitalists are called to admit an acutely ill patient information is sketchy or incomplete. We hear most hospitalized patients present not only as diagnostic challenges but as “unknowns” with insufficient history and medication information.
A 2006 study by the Common-wealth Fund found that in 32% of outpatient visits or referrals, crucial test results or clinical information were absent and consultation needed to be rescheduled.
In many ways the biggest knock on the hospitalist model is that, despite their better in-house availability, use of resources, or quality of care, hospitalists create another “interruption” in care coordination.
This “voltage drop” didn’t start with hospitalists. It has been around whenever patients are referred to specialists or for surgery—or most procedures, for that matter.
But hospitalists and SHM have seized on this perceived Achilles’ heel and formed coalitions to improve transitions of care and urge better care coordination. While working with many others in medicine, SHM also has had interesting discussions with key change agents not traditionally encountered in healthcare.
With grants from the John Hartford Foundation, SHM has developed state-of-the-art discharge planning tools available on the SHM Web site. And, SHM and Intel have discussed broader strategies for managing information.
In addition, I attended a recent American Hospital Association Leadership Summit and had lunch with Colin Powell, who is active at RevolutionHealth.com—the brainchild of AOL founder Steven Case.
One of RevolutionHealth.com’s projects is to create a widely used personal health record (PHR). This would be a Web database with the patient as the focal point. When a patient has a test, sees a physician, visits an ED, or is hospitalized, that information would flow into an updated record accessible by the patient or physician virtually anywhere, any time.
For hospitalists, this could be a source of complete, up-to-date medication lists, diagnoses, and test results. Hospitalists or case managers could update this PHR at discharge so it is immediately available to PCP or coverage partners, home healthcare providers, or a skilled nursing facility. This type of tool doesn’t require that every physician have an electronic medical record (EMR) and isn’t limited by interoperability issues.
Other strategies are gaining traction. At a recent conference on care coordination sponsored by the American Board of Internal Medicine Foundation (ABIM) in Montreal, Quebec, Canada, Chuck Kilo, MD, MPH, CEO of GreenField Health and The GreenField Group in Portland, Ore., showed how e-mail smoothes transitions and improves information flow.
Those in Dr. Kilo’s practice recognize that, while some professionals may have reservations about e-mails between patients and physicians, there seems less resistance to physicians and hospitals using e-mail to exchange information. With minimal expense and startup costs, PCPs can e-mail patients’ medication records, recent chart notes, and test results to a specialist for referral or a hospitalist for admission.
When the consultant or hospitalist is ready to provide information in the transition back to the PCP, e-mail is a quick solution. It’s not perfect, but it’s immediate. Certainly there are barriers to overcome: HIPAA issues are always important to resolve, and documents converted to PDFs don’t flow into an EMR. But this is a step forward.
These solutions get information to the point of decision when the patient is there and the acute need must be met. For those in the trenches this is good news—a great improvement on the hunt-and-peck paradigm.
In a broader strategic approach, SHM has advocated giving hospitalists a role in defining the standards and measures to be used in assessing performance in transitions of care. In July, SHM worked with the ABIM, the American College of Physicians, the Society of General Internal Medicine, the American Geriatrics Society, and the Agency for Healthcare Research and Quality to develop consensus on transitions-of-care standards. This group included most of the big players in the house of internal medicine as well as representatives from nursing, pharmacy, case management, home health, patients, and families. The American College of Emergency Physicians (ACEP) joined the discourse in August.
At the same time, SHM has been working with the American Medical Association’s Physician Consortium and the National Quality Forum to use standards conceived in consensus to develop measures for transitions of care. The measures would mark either stand-alone performance or performance with specific disease states (e.g., management of diabetes or acute heart failure).
Hospitalists will need resources and tools to give patients the best care and smoothest transitions (and score well on these measures). SHM has developed a Web-based quality-improvement resource room on transitions and continues to work with a broad coalition to improve the discharge process under our Hartford grant.
We add real value for our patients. But our job doesn’t end at the hospital door. Hospitalists recognize their obligation to patients as well those who will assume their care outside the hospital. Whether working on tools with Intel or RevolutionHealth or working with professional societies and organizations charged with developing performance standards and measures, hospitalists and SHM must take an active leadership role.
This is not easy stuff and can’t be solved in one meeting—or even one year.
A few years ago no one was talking much about patient safety, notes past SHM President Bob Wachter, MD, professor of medicine at the University of California, San Francisco, associate chairman of UCSF’s Department of Medicine, and chief of the Medical Service at UCSF Medical Center. That is, until the Institute of Medicine’s 2000 report “To Err Is Human: Building a Safer Health System” and some disastrous medical errors.
Transitions aren’t happening well, and care is sporadic and isolated. This is high on our agenda; SHM and hospitalists are willing to work with any group that will help all of us get closer to a solution. TH
Dr. Wellikson is the CEO of SHM.
Experts in the Elderly
The average young or middle-age person probably finds a hospital stay stressful, uncomfortable, and inconvenient. The experience can be strikingly more disruptive for a geriatric patient.
A frail elderly person can easily succumb to delirium, a fall, dehydration, polypharmacy, and deterioration in basic life skills, quickly turning even a routine hospitalization into a catastrophic downhill slide. But if a patient is lucky, she will be treated by a geriatric hospitalist—a physician who by training and temperament is uniquely suited to care for her.
Geriatric hospitalists bring heightened sensitivity and experience to treating and preventing the common syndromes that can overwhelm the elderly during hospitalizations. Fredrick Sherman, MD, FACP, medical director of Senior Health Partners and professor of geriatrics at the Mount Sinai School of Medicine in Manhattan, has been a geriatrician since the 1980s. He sees a great opportunity for hospitalist geriatricians to improve the metrics by which hospitalist programs are judged: reduced length of stay, bounceback, and morbidity. They do this, he says, with a unique blend of skills, mindset, and temperament.
“In one or two minutes at the bedside, a geriatric hospitalist can do a basic functional assessment of an elderly patient,” he says. “We can understand their ADL [activities of daily living] skills, mental status, and what resources we have to mobilize during the hospital stay and for a safe discharge plan. We don’t want to turn hospitalists into social workers, but geriatricians can teach them a body of knowledge to help them better understand and develop a holistic approach to elderly patients.”
How geriatricians work best, though, can be somewhat out of synch with hospital medicine’s fast pace. “Many hospitalists are younger and have been trained very recently,” Dr. Sherman says. “They quickly learn to take care of a 55-year-old with a [myocardial infarction], but they sometimes lack a global view of geriatric patients that is more a frame of mind than about the physician’s technical skills.”
Challenges Ahead
As hospital medicine groups integrate geriatricians into their ranks, they will have recruited major players invested in improving the care of hospitalized elderly patients. There’s a lot at stake in caring for them.
The Healthcare Cost and Utilization Project’s (HCUP) most recent figures of what hospitalizations of the elderly cost is staggering. Medicare patients account for 76% of public spending on hospital care. The costliest diagnoses for Medicare-paid hospitalizations are coronary arteriosclerosis ($44 billion), acute myocardial infarction ($31 billion), and heart failure ($29 billion). Further, 90% of elderly patients with osteoarthritis are hospitalized for elective hip or knee joint replacement therapy.
The expertise of board-certified hospitalist geriatricians will be hard to disseminate throughout the corps of hospitalists. Only a tiny fraction of the nation’s hospitalist programs claim special expertise in geriatrics. Researchers from the University of Colorado Health Sciences Center and the Mayo Clinic College of Medicine conducted a cross-sectional survey of the hospitalist community in 2003-2004 to determine the impact of the hospitalist movement on acute care geriatrics. They found:
- Out of 1,415 hospitalist programs, 11 reported geriatric innovations.
- Four developed core clinical activities, four used geriatric QI measures, three used comprehensive geriatric assessments, and two had specific protocols for elderly patients discharged to nursing facilities; and
- In terms of staffing, four had hospitalists with no special geriatric training, four employed fellowship-trained geriatricians, two had general hospitalists and geriatricians, and four used advanced practice nurses with and without geriatric training.1
Adding to the difficulty of building a cadre of geriatric hospitalists is the national paucity of geriatricians. According to the American Geriatrics Society (AGS), there were 9,000 board-certified geriatricians in 1998. A decade later there are 7,600—and the pipeline is narrow. Of 9,780 medical school graduates in 2004, only 321 were geriatricians. The AGS estimates that the United States needs 14,000 geriatricians now and 36,000 in 2030, when there will be an estimated 70 million adults 65 years and older.
But there’s hope. Hospital medicine programs, growing by leaps and bounds, offer a new career path for physicians interested in geriatrics. As the number of hospitalists continues to grow, there’s room for physicians to have an impact by staying tuned in to the special clinical, psychosocial, emotional, spiritual, and environmental needs of elderly patients.
The Breed
According to Leslie Libow, MD, distinguished clinical professor at the Jewish Home and Hospital of New York in Manhattan, physicians who pursue a career in geriatrics do so because they have the right psychological make-up to work with elderly people.
He should know. In 1968, Dr. Libow petitioned the American Board of Internal Medicine (ABIM) to recognize geriatrics as a sub-specialty of internal medicine. Shortly after ABIM recognition, Dr. Libow established a geriatric residency/fellowship at Mount Sinai—still a national leader in geriatric education.
Being a geriatric hospitalist allows physicians with a simpatico set of personality traits to thrive. One study of geriatricians who had been practicing for up to 25 years found that they shared these traits:
- Highly value enduring relationships;
- Enjoy making small but potent changes in their patients’ lives;
- Like to make a difference personally and for society;
- Prefer working in a multidisciplinary team;
- Prefer democratic, not autocratic, decision-making;
- Desire the intellectual challenges of geriatric medicine and like to teach; and
- Perceive that they have a distinct and different career path than other physicians.2
That essentially describes Purnima Joshi, chief of medicine, at Kaiser-Permanente Mid-Atlantic States at Washington Hospital Center in Washington, D.C. She directs a group of 12 hospitalists, is the group’s only geriatrician at the 800-bed tertiary care facility, and enjoys teaching residents about geriatric medicine. A family physician by trade, she was grandfathered into geriatrics in 1992 and recertified in 2002.
“I love working with the frail elderly and practicing Kaiser’s brand of medicine because I don’t do billing—I just treat patients,” Dr. Joshi says. Additionally, Kaiser simplifies record-keeping on inpatient and outpatient treatments and makes communicating with Kaiser’s outpatient doctors about post-discharge care smooth and efficient.
Dr. Joshi explains that being a geriatric hospitalist is different than specializing in general internal medicine because she customizes the approach for each patient—including tailoring therapies to life expectancy. “Guidelines and evidence-based medicine are fine and very important, and we use geriatric guidelines on our teaching service,” she says. “But geriatrics liberates your thinking as a doctor. You treat the whole person—a diabetic with three days to live, and a 90-year-old with delirium and decubitus ulcers.”
She calls herself a surrogate primary care physician, seeing 12 patients most days. She consults frequently with other hospitalists on their toughest geriatric issues and makes daily multidisciplinary rounds—with discharge planner, pharmacist, physical therapist, palliative care specialist, nurses, and resident in tow.
“We keep length of stay and guidelines in mind, but the patient is the center of my universe,” Dr. Joshi asserts. “I deliver holistic, patient-centered care and use gentle teaching tools for our residents. I have the luxury of taking time to see the patient and talk to them and their families. It’s wonderful.”
Dr. Joshi’s attitude toward her profession reflects a consistent national finding: Geriatricians rank No. 1 in nearly every study of physician career satisfaction, from the American Medical Association to the American Geriatrics Society.
Across the country, Alpesh Amin, MD, MBA, FACP, professor and chief of general internal medicine and executive director of the University of California at Irvine’s School of Medicine Hospitalist Service, is making the most of the two geriatricians on his 15-hospitalist team. Starting about eight years ago, Dr. Amin—also a member of SHM’s board of directors—turned to his hospitalist geriatricians for a host of services: geriatric assessments, co-management of psychiatric problems, perioperative consults, critical care, and palliative care consults.
“Geriatricians have such knowledge and insight into elderly patients to share with the other hospitalists,” says Dr. Amin. “That’s why they work well side by side with internal medicine and family medicine hospitalists. They keep us aware of issues in geriatrics and the literature on what works best with these patients.”
Knowing that geriatricians are scarce, Dr. Amin accesses their expertise by using a system that focuses team members’ attention on their knowledge. There are journal clubs, frequent consults, monthly meetings, teaching rounds, geriatric fellowships, and other opportunities that keep the geriatrician’s unique perspective front and center for other team members. “They are so in tune with issues related to delirium, polypharmacy, falls risk, etc.,” he says. “Our model incorporates that expertise, and it works very well. We truly work as a multidisciplinary team with ownership and accountability of the special needs of our geriatric patients.”
—Fredrick Sherman, MD, FACP, medical director of Senior Health Partners and professor of geriatrics at the Mount Sinai School of Medicine in Manhattan
A New Generation
The rapid growth of hospital medicine has encouraged new physicians to choose this career path.
Claudene George, MD, recently completed a two-year geriatric fellowship at Mount Sinai Hospital in New York City and is starting as a geriatric hospitalist at Montefiore Hospital in the Bronx. “Becoming a geriatrician sort of surprised me because I thought I’d go into internal medicine,” she says. “But I love the approach to caring for the whole person and communicating with their families.”
As part of her contract at Montefiore, she negotiated a half-day-per-week rotation at the hospital’s outpatient clinic—part of her commitment to being a well-rounded physician.
“The geriatric assessment up front is essential to find out what the patient’s and family’s goals of care are,” says Dr. George. “If they’re 80 years old and want to stay at home, we need to help them do that safely. That may mean linking them to the [visiting nurse service], a home aide, or adult day care.”
She points out that an inpatient stay also offers seniors the opportunity to be seen by subspecialists and do a lot in a short period of time. “As a hospitalist geriatrician you can see change almost immediately; you can have an impact,” she concludes.
As the hospitalist movement affords career opportunities to geriatricians, young physicians can obtain financial incentives to pursue a career in geriatrics. For instance, in 2006 South Carolina enacted a Geriatrician Loan Forgiveness program, helping physicians to repay up to $35,000 of medical school loans if they complete a geriatrics fellowship and practice in South Carolina for five years after completing medical training.
Victor Hirth, MD, medical director for the Division of Geriatric Services of Palmetto Health of Columbia, S.C., has recruited eight geriatric fellows, two of whom will be hospitalists. A recent recruit, Andres Leone, MD, went to medical school in Ecuador, recently completed a geriatric fellowship in South Carolina, and works as a hospitalist half time and at a free clinic for Hispanics half-time. “The flexibility to work as a hospitalist and in an outpatient clinic feels right to me,” says Dr. Leone.
While the number of geriatric hospitalists today is small, some predict their growing presence is inevitable.
“The baby boomers will deluge us, and they will demand so much more of hospitalists in the near future,” Dr. Sherman says. “They will have complicated issues and be very inquisitive geriatric patients.” TH
Marlene Piturro is a frequent contributor to The Hospitalist.
References
- Wald H, Huddleston J, Kramer A. Is there a geriatrician in the house? Geriatric care approaches in hospitalist programs. J Hosp Med. 2006 Jan;1(1):29-35.
- Shah U, Aung M, Chan S, et al. Do geriatricians stay in geriatrics? Gerontol Geriatr Educ. 2006;27(1):57-65.
The average young or middle-age person probably finds a hospital stay stressful, uncomfortable, and inconvenient. The experience can be strikingly more disruptive for a geriatric patient.
A frail elderly person can easily succumb to delirium, a fall, dehydration, polypharmacy, and deterioration in basic life skills, quickly turning even a routine hospitalization into a catastrophic downhill slide. But if a patient is lucky, she will be treated by a geriatric hospitalist—a physician who by training and temperament is uniquely suited to care for her.
Geriatric hospitalists bring heightened sensitivity and experience to treating and preventing the common syndromes that can overwhelm the elderly during hospitalizations. Fredrick Sherman, MD, FACP, medical director of Senior Health Partners and professor of geriatrics at the Mount Sinai School of Medicine in Manhattan, has been a geriatrician since the 1980s. He sees a great opportunity for hospitalist geriatricians to improve the metrics by which hospitalist programs are judged: reduced length of stay, bounceback, and morbidity. They do this, he says, with a unique blend of skills, mindset, and temperament.
“In one or two minutes at the bedside, a geriatric hospitalist can do a basic functional assessment of an elderly patient,” he says. “We can understand their ADL [activities of daily living] skills, mental status, and what resources we have to mobilize during the hospital stay and for a safe discharge plan. We don’t want to turn hospitalists into social workers, but geriatricians can teach them a body of knowledge to help them better understand and develop a holistic approach to elderly patients.”
How geriatricians work best, though, can be somewhat out of synch with hospital medicine’s fast pace. “Many hospitalists are younger and have been trained very recently,” Dr. Sherman says. “They quickly learn to take care of a 55-year-old with a [myocardial infarction], but they sometimes lack a global view of geriatric patients that is more a frame of mind than about the physician’s technical skills.”
Challenges Ahead
As hospital medicine groups integrate geriatricians into their ranks, they will have recruited major players invested in improving the care of hospitalized elderly patients. There’s a lot at stake in caring for them.
The Healthcare Cost and Utilization Project’s (HCUP) most recent figures of what hospitalizations of the elderly cost is staggering. Medicare patients account for 76% of public spending on hospital care. The costliest diagnoses for Medicare-paid hospitalizations are coronary arteriosclerosis ($44 billion), acute myocardial infarction ($31 billion), and heart failure ($29 billion). Further, 90% of elderly patients with osteoarthritis are hospitalized for elective hip or knee joint replacement therapy.
The expertise of board-certified hospitalist geriatricians will be hard to disseminate throughout the corps of hospitalists. Only a tiny fraction of the nation’s hospitalist programs claim special expertise in geriatrics. Researchers from the University of Colorado Health Sciences Center and the Mayo Clinic College of Medicine conducted a cross-sectional survey of the hospitalist community in 2003-2004 to determine the impact of the hospitalist movement on acute care geriatrics. They found:
- Out of 1,415 hospitalist programs, 11 reported geriatric innovations.
- Four developed core clinical activities, four used geriatric QI measures, three used comprehensive geriatric assessments, and two had specific protocols for elderly patients discharged to nursing facilities; and
- In terms of staffing, four had hospitalists with no special geriatric training, four employed fellowship-trained geriatricians, two had general hospitalists and geriatricians, and four used advanced practice nurses with and without geriatric training.1
Adding to the difficulty of building a cadre of geriatric hospitalists is the national paucity of geriatricians. According to the American Geriatrics Society (AGS), there were 9,000 board-certified geriatricians in 1998. A decade later there are 7,600—and the pipeline is narrow. Of 9,780 medical school graduates in 2004, only 321 were geriatricians. The AGS estimates that the United States needs 14,000 geriatricians now and 36,000 in 2030, when there will be an estimated 70 million adults 65 years and older.
But there’s hope. Hospital medicine programs, growing by leaps and bounds, offer a new career path for physicians interested in geriatrics. As the number of hospitalists continues to grow, there’s room for physicians to have an impact by staying tuned in to the special clinical, psychosocial, emotional, spiritual, and environmental needs of elderly patients.
The Breed
According to Leslie Libow, MD, distinguished clinical professor at the Jewish Home and Hospital of New York in Manhattan, physicians who pursue a career in geriatrics do so because they have the right psychological make-up to work with elderly people.
He should know. In 1968, Dr. Libow petitioned the American Board of Internal Medicine (ABIM) to recognize geriatrics as a sub-specialty of internal medicine. Shortly after ABIM recognition, Dr. Libow established a geriatric residency/fellowship at Mount Sinai—still a national leader in geriatric education.
Being a geriatric hospitalist allows physicians with a simpatico set of personality traits to thrive. One study of geriatricians who had been practicing for up to 25 years found that they shared these traits:
- Highly value enduring relationships;
- Enjoy making small but potent changes in their patients’ lives;
- Like to make a difference personally and for society;
- Prefer working in a multidisciplinary team;
- Prefer democratic, not autocratic, decision-making;
- Desire the intellectual challenges of geriatric medicine and like to teach; and
- Perceive that they have a distinct and different career path than other physicians.2
That essentially describes Purnima Joshi, chief of medicine, at Kaiser-Permanente Mid-Atlantic States at Washington Hospital Center in Washington, D.C. She directs a group of 12 hospitalists, is the group’s only geriatrician at the 800-bed tertiary care facility, and enjoys teaching residents about geriatric medicine. A family physician by trade, she was grandfathered into geriatrics in 1992 and recertified in 2002.
“I love working with the frail elderly and practicing Kaiser’s brand of medicine because I don’t do billing—I just treat patients,” Dr. Joshi says. Additionally, Kaiser simplifies record-keeping on inpatient and outpatient treatments and makes communicating with Kaiser’s outpatient doctors about post-discharge care smooth and efficient.
Dr. Joshi explains that being a geriatric hospitalist is different than specializing in general internal medicine because she customizes the approach for each patient—including tailoring therapies to life expectancy. “Guidelines and evidence-based medicine are fine and very important, and we use geriatric guidelines on our teaching service,” she says. “But geriatrics liberates your thinking as a doctor. You treat the whole person—a diabetic with three days to live, and a 90-year-old with delirium and decubitus ulcers.”
She calls herself a surrogate primary care physician, seeing 12 patients most days. She consults frequently with other hospitalists on their toughest geriatric issues and makes daily multidisciplinary rounds—with discharge planner, pharmacist, physical therapist, palliative care specialist, nurses, and resident in tow.
“We keep length of stay and guidelines in mind, but the patient is the center of my universe,” Dr. Joshi asserts. “I deliver holistic, patient-centered care and use gentle teaching tools for our residents. I have the luxury of taking time to see the patient and talk to them and their families. It’s wonderful.”
Dr. Joshi’s attitude toward her profession reflects a consistent national finding: Geriatricians rank No. 1 in nearly every study of physician career satisfaction, from the American Medical Association to the American Geriatrics Society.
Across the country, Alpesh Amin, MD, MBA, FACP, professor and chief of general internal medicine and executive director of the University of California at Irvine’s School of Medicine Hospitalist Service, is making the most of the two geriatricians on his 15-hospitalist team. Starting about eight years ago, Dr. Amin—also a member of SHM’s board of directors—turned to his hospitalist geriatricians for a host of services: geriatric assessments, co-management of psychiatric problems, perioperative consults, critical care, and palliative care consults.
“Geriatricians have such knowledge and insight into elderly patients to share with the other hospitalists,” says Dr. Amin. “That’s why they work well side by side with internal medicine and family medicine hospitalists. They keep us aware of issues in geriatrics and the literature on what works best with these patients.”
Knowing that geriatricians are scarce, Dr. Amin accesses their expertise by using a system that focuses team members’ attention on their knowledge. There are journal clubs, frequent consults, monthly meetings, teaching rounds, geriatric fellowships, and other opportunities that keep the geriatrician’s unique perspective front and center for other team members. “They are so in tune with issues related to delirium, polypharmacy, falls risk, etc.,” he says. “Our model incorporates that expertise, and it works very well. We truly work as a multidisciplinary team with ownership and accountability of the special needs of our geriatric patients.”
—Fredrick Sherman, MD, FACP, medical director of Senior Health Partners and professor of geriatrics at the Mount Sinai School of Medicine in Manhattan
A New Generation
The rapid growth of hospital medicine has encouraged new physicians to choose this career path.
Claudene George, MD, recently completed a two-year geriatric fellowship at Mount Sinai Hospital in New York City and is starting as a geriatric hospitalist at Montefiore Hospital in the Bronx. “Becoming a geriatrician sort of surprised me because I thought I’d go into internal medicine,” she says. “But I love the approach to caring for the whole person and communicating with their families.”
As part of her contract at Montefiore, she negotiated a half-day-per-week rotation at the hospital’s outpatient clinic—part of her commitment to being a well-rounded physician.
“The geriatric assessment up front is essential to find out what the patient’s and family’s goals of care are,” says Dr. George. “If they’re 80 years old and want to stay at home, we need to help them do that safely. That may mean linking them to the [visiting nurse service], a home aide, or adult day care.”
She points out that an inpatient stay also offers seniors the opportunity to be seen by subspecialists and do a lot in a short period of time. “As a hospitalist geriatrician you can see change almost immediately; you can have an impact,” she concludes.
As the hospitalist movement affords career opportunities to geriatricians, young physicians can obtain financial incentives to pursue a career in geriatrics. For instance, in 2006 South Carolina enacted a Geriatrician Loan Forgiveness program, helping physicians to repay up to $35,000 of medical school loans if they complete a geriatrics fellowship and practice in South Carolina for five years after completing medical training.
Victor Hirth, MD, medical director for the Division of Geriatric Services of Palmetto Health of Columbia, S.C., has recruited eight geriatric fellows, two of whom will be hospitalists. A recent recruit, Andres Leone, MD, went to medical school in Ecuador, recently completed a geriatric fellowship in South Carolina, and works as a hospitalist half time and at a free clinic for Hispanics half-time. “The flexibility to work as a hospitalist and in an outpatient clinic feels right to me,” says Dr. Leone.
While the number of geriatric hospitalists today is small, some predict their growing presence is inevitable.
“The baby boomers will deluge us, and they will demand so much more of hospitalists in the near future,” Dr. Sherman says. “They will have complicated issues and be very inquisitive geriatric patients.” TH
Marlene Piturro is a frequent contributor to The Hospitalist.
References
- Wald H, Huddleston J, Kramer A. Is there a geriatrician in the house? Geriatric care approaches in hospitalist programs. J Hosp Med. 2006 Jan;1(1):29-35.
- Shah U, Aung M, Chan S, et al. Do geriatricians stay in geriatrics? Gerontol Geriatr Educ. 2006;27(1):57-65.
The average young or middle-age person probably finds a hospital stay stressful, uncomfortable, and inconvenient. The experience can be strikingly more disruptive for a geriatric patient.
A frail elderly person can easily succumb to delirium, a fall, dehydration, polypharmacy, and deterioration in basic life skills, quickly turning even a routine hospitalization into a catastrophic downhill slide. But if a patient is lucky, she will be treated by a geriatric hospitalist—a physician who by training and temperament is uniquely suited to care for her.
Geriatric hospitalists bring heightened sensitivity and experience to treating and preventing the common syndromes that can overwhelm the elderly during hospitalizations. Fredrick Sherman, MD, FACP, medical director of Senior Health Partners and professor of geriatrics at the Mount Sinai School of Medicine in Manhattan, has been a geriatrician since the 1980s. He sees a great opportunity for hospitalist geriatricians to improve the metrics by which hospitalist programs are judged: reduced length of stay, bounceback, and morbidity. They do this, he says, with a unique blend of skills, mindset, and temperament.
“In one or two minutes at the bedside, a geriatric hospitalist can do a basic functional assessment of an elderly patient,” he says. “We can understand their ADL [activities of daily living] skills, mental status, and what resources we have to mobilize during the hospital stay and for a safe discharge plan. We don’t want to turn hospitalists into social workers, but geriatricians can teach them a body of knowledge to help them better understand and develop a holistic approach to elderly patients.”
How geriatricians work best, though, can be somewhat out of synch with hospital medicine’s fast pace. “Many hospitalists are younger and have been trained very recently,” Dr. Sherman says. “They quickly learn to take care of a 55-year-old with a [myocardial infarction], but they sometimes lack a global view of geriatric patients that is more a frame of mind than about the physician’s technical skills.”
Challenges Ahead
As hospital medicine groups integrate geriatricians into their ranks, they will have recruited major players invested in improving the care of hospitalized elderly patients. There’s a lot at stake in caring for them.
The Healthcare Cost and Utilization Project’s (HCUP) most recent figures of what hospitalizations of the elderly cost is staggering. Medicare patients account for 76% of public spending on hospital care. The costliest diagnoses for Medicare-paid hospitalizations are coronary arteriosclerosis ($44 billion), acute myocardial infarction ($31 billion), and heart failure ($29 billion). Further, 90% of elderly patients with osteoarthritis are hospitalized for elective hip or knee joint replacement therapy.
The expertise of board-certified hospitalist geriatricians will be hard to disseminate throughout the corps of hospitalists. Only a tiny fraction of the nation’s hospitalist programs claim special expertise in geriatrics. Researchers from the University of Colorado Health Sciences Center and the Mayo Clinic College of Medicine conducted a cross-sectional survey of the hospitalist community in 2003-2004 to determine the impact of the hospitalist movement on acute care geriatrics. They found:
- Out of 1,415 hospitalist programs, 11 reported geriatric innovations.
- Four developed core clinical activities, four used geriatric QI measures, three used comprehensive geriatric assessments, and two had specific protocols for elderly patients discharged to nursing facilities; and
- In terms of staffing, four had hospitalists with no special geriatric training, four employed fellowship-trained geriatricians, two had general hospitalists and geriatricians, and four used advanced practice nurses with and without geriatric training.1
Adding to the difficulty of building a cadre of geriatric hospitalists is the national paucity of geriatricians. According to the American Geriatrics Society (AGS), there were 9,000 board-certified geriatricians in 1998. A decade later there are 7,600—and the pipeline is narrow. Of 9,780 medical school graduates in 2004, only 321 were geriatricians. The AGS estimates that the United States needs 14,000 geriatricians now and 36,000 in 2030, when there will be an estimated 70 million adults 65 years and older.
But there’s hope. Hospital medicine programs, growing by leaps and bounds, offer a new career path for physicians interested in geriatrics. As the number of hospitalists continues to grow, there’s room for physicians to have an impact by staying tuned in to the special clinical, psychosocial, emotional, spiritual, and environmental needs of elderly patients.
The Breed
According to Leslie Libow, MD, distinguished clinical professor at the Jewish Home and Hospital of New York in Manhattan, physicians who pursue a career in geriatrics do so because they have the right psychological make-up to work with elderly people.
He should know. In 1968, Dr. Libow petitioned the American Board of Internal Medicine (ABIM) to recognize geriatrics as a sub-specialty of internal medicine. Shortly after ABIM recognition, Dr. Libow established a geriatric residency/fellowship at Mount Sinai—still a national leader in geriatric education.
Being a geriatric hospitalist allows physicians with a simpatico set of personality traits to thrive. One study of geriatricians who had been practicing for up to 25 years found that they shared these traits:
- Highly value enduring relationships;
- Enjoy making small but potent changes in their patients’ lives;
- Like to make a difference personally and for society;
- Prefer working in a multidisciplinary team;
- Prefer democratic, not autocratic, decision-making;
- Desire the intellectual challenges of geriatric medicine and like to teach; and
- Perceive that they have a distinct and different career path than other physicians.2
That essentially describes Purnima Joshi, chief of medicine, at Kaiser-Permanente Mid-Atlantic States at Washington Hospital Center in Washington, D.C. She directs a group of 12 hospitalists, is the group’s only geriatrician at the 800-bed tertiary care facility, and enjoys teaching residents about geriatric medicine. A family physician by trade, she was grandfathered into geriatrics in 1992 and recertified in 2002.
“I love working with the frail elderly and practicing Kaiser’s brand of medicine because I don’t do billing—I just treat patients,” Dr. Joshi says. Additionally, Kaiser simplifies record-keeping on inpatient and outpatient treatments and makes communicating with Kaiser’s outpatient doctors about post-discharge care smooth and efficient.
Dr. Joshi explains that being a geriatric hospitalist is different than specializing in general internal medicine because she customizes the approach for each patient—including tailoring therapies to life expectancy. “Guidelines and evidence-based medicine are fine and very important, and we use geriatric guidelines on our teaching service,” she says. “But geriatrics liberates your thinking as a doctor. You treat the whole person—a diabetic with three days to live, and a 90-year-old with delirium and decubitus ulcers.”
She calls herself a surrogate primary care physician, seeing 12 patients most days. She consults frequently with other hospitalists on their toughest geriatric issues and makes daily multidisciplinary rounds—with discharge planner, pharmacist, physical therapist, palliative care specialist, nurses, and resident in tow.
“We keep length of stay and guidelines in mind, but the patient is the center of my universe,” Dr. Joshi asserts. “I deliver holistic, patient-centered care and use gentle teaching tools for our residents. I have the luxury of taking time to see the patient and talk to them and their families. It’s wonderful.”
Dr. Joshi’s attitude toward her profession reflects a consistent national finding: Geriatricians rank No. 1 in nearly every study of physician career satisfaction, from the American Medical Association to the American Geriatrics Society.
Across the country, Alpesh Amin, MD, MBA, FACP, professor and chief of general internal medicine and executive director of the University of California at Irvine’s School of Medicine Hospitalist Service, is making the most of the two geriatricians on his 15-hospitalist team. Starting about eight years ago, Dr. Amin—also a member of SHM’s board of directors—turned to his hospitalist geriatricians for a host of services: geriatric assessments, co-management of psychiatric problems, perioperative consults, critical care, and palliative care consults.
“Geriatricians have such knowledge and insight into elderly patients to share with the other hospitalists,” says Dr. Amin. “That’s why they work well side by side with internal medicine and family medicine hospitalists. They keep us aware of issues in geriatrics and the literature on what works best with these patients.”
Knowing that geriatricians are scarce, Dr. Amin accesses their expertise by using a system that focuses team members’ attention on their knowledge. There are journal clubs, frequent consults, monthly meetings, teaching rounds, geriatric fellowships, and other opportunities that keep the geriatrician’s unique perspective front and center for other team members. “They are so in tune with issues related to delirium, polypharmacy, falls risk, etc.,” he says. “Our model incorporates that expertise, and it works very well. We truly work as a multidisciplinary team with ownership and accountability of the special needs of our geriatric patients.”
—Fredrick Sherman, MD, FACP, medical director of Senior Health Partners and professor of geriatrics at the Mount Sinai School of Medicine in Manhattan
A New Generation
The rapid growth of hospital medicine has encouraged new physicians to choose this career path.
Claudene George, MD, recently completed a two-year geriatric fellowship at Mount Sinai Hospital in New York City and is starting as a geriatric hospitalist at Montefiore Hospital in the Bronx. “Becoming a geriatrician sort of surprised me because I thought I’d go into internal medicine,” she says. “But I love the approach to caring for the whole person and communicating with their families.”
As part of her contract at Montefiore, she negotiated a half-day-per-week rotation at the hospital’s outpatient clinic—part of her commitment to being a well-rounded physician.
“The geriatric assessment up front is essential to find out what the patient’s and family’s goals of care are,” says Dr. George. “If they’re 80 years old and want to stay at home, we need to help them do that safely. That may mean linking them to the [visiting nurse service], a home aide, or adult day care.”
She points out that an inpatient stay also offers seniors the opportunity to be seen by subspecialists and do a lot in a short period of time. “As a hospitalist geriatrician you can see change almost immediately; you can have an impact,” she concludes.
As the hospitalist movement affords career opportunities to geriatricians, young physicians can obtain financial incentives to pursue a career in geriatrics. For instance, in 2006 South Carolina enacted a Geriatrician Loan Forgiveness program, helping physicians to repay up to $35,000 of medical school loans if they complete a geriatrics fellowship and practice in South Carolina for five years after completing medical training.
Victor Hirth, MD, medical director for the Division of Geriatric Services of Palmetto Health of Columbia, S.C., has recruited eight geriatric fellows, two of whom will be hospitalists. A recent recruit, Andres Leone, MD, went to medical school in Ecuador, recently completed a geriatric fellowship in South Carolina, and works as a hospitalist half time and at a free clinic for Hispanics half-time. “The flexibility to work as a hospitalist and in an outpatient clinic feels right to me,” says Dr. Leone.
While the number of geriatric hospitalists today is small, some predict their growing presence is inevitable.
“The baby boomers will deluge us, and they will demand so much more of hospitalists in the near future,” Dr. Sherman says. “They will have complicated issues and be very inquisitive geriatric patients.” TH
Marlene Piturro is a frequent contributor to The Hospitalist.
References
- Wald H, Huddleston J, Kramer A. Is there a geriatrician in the house? Geriatric care approaches in hospitalist programs. J Hosp Med. 2006 Jan;1(1):29-35.
- Shah U, Aung M, Chan S, et al. Do geriatricians stay in geriatrics? Gerontol Geriatr Educ. 2006;27(1):57-65.
Diagnose Misdiagnosis
This is the first of a two-part series examining medical errors. This article addresses thought processes hospitalists use that may lead to mistaken diagnoses. Part 2 will look at what healthcare corporations are doing to improve diagnoses and reduce errors.
When talking about tough diagnoses, academic hospitalist David Feinbloom, MD, recalls the story of a female patient seen by his hospitalist group whose diagnosis took some time to nail down.
This woman had been in and out of the hospital for several years with nonspecific abdominal pain and intermittent diarrhea. She had been seen by numerous doctors and tested extensively. Increasingly her doctors concluded that there was some psychiatric overlay—she was depressed or somatic.
“Patients like these are very common and often end up on the hospitalist service,” says Dr. Feinbloom, who works at Beth Israel Deaconess Medical Center in Boston.
But to Joseph Li, MD, director of the hospital medicine program at Beth Israel, this patient seemed normal. There was something about the symptoms she described that reminded him of a patient he had seen who had been diagnosed with a metastatic neuroendocrine tumor.
Although this patient’s past MRI had been negative, Dr. Li remembered that if you don’t perform the right MRI protocol, you’ll miss something. He asked the team to obtain a panel looking for specific markers and to repeat the MRI with the correct protocol. It was accepted as fact that there was no pathology to explain her symptoms but that she had had every test. He requested another gastrointestinal (GI) consult.
“It seemed so far out there, and then everything he said was completely correct,” says Dr. Feinbloom. “She had Zollinger-Ellison syndrome.”
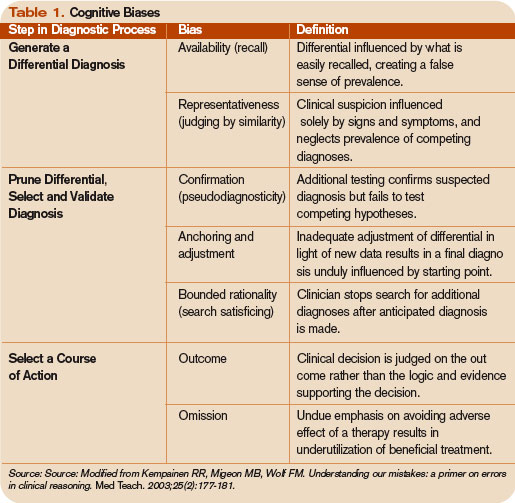
Clues from Sherlock
In his book How Doctors Think, Jerome Groopman, MD, discusses Sir Arthur Conan Doyle, physician and creator of the brilliant detective Sherlock Holmes. When it comes to solving crimes, Holmes’ superior observation and logic, intellectual prowess, and pristine reasoning help him observe and interpret the most obscure and arcane clues. He is, in the end, a consummate diagnostician.
One of the first rules a great diagnostician must follow is to not get boxed into one way of thinking, says Dr. Groopman, the Dina and Raphael Recanati chair of medicine at the Harvard Medical School and chief of experimental medicine at the Beth Israel Deaconess Medical Center, Boston. That is one of the downsides of a too-easy attachment to using clinical practice guidelines, he says.
“Guidelines are valuable reference points, but in order to use a guideline effectively, you have to have the correct diagnosis,” he says. “Studies over decades with hospitalized patients show that the misdiagnosis rate is at least 15% and hasn’t changed.1 A great deal of effort needs to be put into improving our accuracy in making diagnoses.”
Compared with other kinds of medical errors, diagnostic errors have not gotten a great deal of attention. The hospital patient safety movement has been more focused on preventing medication errors, surgical errors, handoff communications, nosocomial infections, falls, and blood clots.2 There have been few studies pertaining exclusively to diagnostic errors—but the topic is gaining headway.3
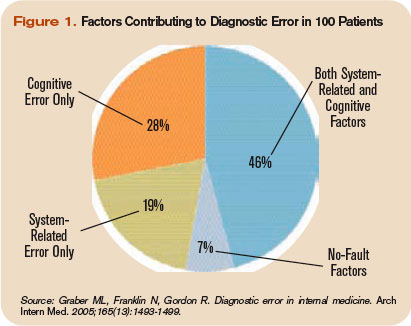
Think about Thinking
Diagnostic errors are usually multifactorial in origin and typically involve system-related and individual factors. The systems-based piece includes environmental and organizational factors. Medical researchers conclude the majority of diagnostic errors arise from flaws in physician thinking, not technical mistakes.
Cognitive errors involve instances where knowledge, data gathering, data processing, or verification (such as by lab testing) are faulty. Improving diagnostics will require better accountability by institutions and individuals. To do the latter, experts say, physicians would do well to familiarize themselves with their diagnostic weaknesses.
Thinking about thinking is the science of cognitive psychology and addresses the cognitive aspects of clinical reasoning underlying diagnostic decision-making. It is an area of study in which few medical professionals are versed. “Except for a few of these guys who trained in psych or were voices in the wilderness that have been largely ignored,” most physicians are unaware of the cognitive psychology literature, Dr. Groopman says.
Common biases and errors in clinical reasoning are presented in Table 1 (right).4,5 These are largely individual mistakes for which physicians traditionally have been accountable.

Patterns and Heuristics
The following factors contribute to how shortcuts are used: the pressures of working in medicine, the degrees of uncertainty a physician may feel, and the fact that hospitalists rarely have all the information they need about a patient.
“That’s just the nature of medicine,” says Dr. Groopman. “These shortcuts are natural ways of thinking under those conditions. They succeed about 85% of the time; they fail up to 10-20% of the time. The first thing we need to educate ourselves about is that this is how our minds work as doctors.”
Dr. Groopman and those he interviewed for his book have a razor-sharp overview of clinical practice within hospitals throughout the U.S. and Canada, including academic centers, community centers, affluent areas, suburbs, inner cities, and Native American reservations. But except for Pat Croskerry, MD, PhD, in the department of emergency medicine at Dalhousie University’s Queen Elizabeth II Health Sciences Center in Halifax, Nova Scotia, none of the experts he interviewed had rigorous training in cognitive science.
Although how to think is a priority in physicians’ training, how to think about one’s thinking is not.
“We are not given a vocabulary during medical training, or later through CME courses, in this emerging science—and yet this science involves how our mind works successfully and when we make mistakes,” Dr. Groopman says.
The data back this assertion. In a study of 100 cases of diagnostic error, 90 involved injury, including 33 deaths; 74% were attributed to errors in cognitive reasoning (see Figure 1, right).1 Failure to consider reasonable alternatives after an initial diagnosis was the most common cause. Other common causes included faulty context generation, misjudging the salience of findings, faulty perception, and errors connected with the use of heuristics. In this study, faulty or inadequate knowledge was uncommon.
Underlying contributions to error fell into three categories: “no fault,” system-related, and cognitive. Only seven cases reflected no-fault errors alone. In the remaining 93 cases, 548 errors were identified as system-related or cognitive factors (5.9 per case). System-related factors contributed to the diagnostic error in 65% of the cases and cognitive factors in 74%. The most common system-related factors involved problems with policies and procedures, inefficient processes, teamwork, and communication. The most common cognitive problems involved faulty synthesis.
Dr. Groopman believes it is important for physicians to be more introspective about the thinking patterns they employ and learn the traps to which they are susceptible. He also feels it is imperative to develop curricula at different stages of medical training so this new knowledge can be used to reduce error rates. Because the names for these traps can vary, the development of a universal and comprehensive taxonomy for classifying diagnostic errors is also needed.
“It’s impossible to be perfect; we’re never going to be 100%,” Dr. Groopman says. “But I deeply believe that it is quite feasible to think about your thinking and to assess how your mind came to a conclusion about a diagnosis and treatment plan.”
When phy-sicians think about errors in cognitive reasoning, they often focus on the “don’t-miss diagnoses” or the uncommon variant missed by recall or anchoring errors.
“When I reflect on the errors I have made, they mostly fall into the categories that Dr. Groopman describes in his book,” Dr. Feinbloom says. “Interestingly, the errors that I see most often stem from the fear of making an error of omission.”
It is paradoxical, but in order to ensure that no possible diagnosis is missed, doctors often feel the need to rule out all possible diagnoses.
“While it makes us feel that we are doing the best for our patients, this approach leads to an inordinate amount of unnecessary testing and potentially harmful interventions,” says Dr. Feinbloom. “Understanding how cognitive errors occur should allow us to be judicious in our approach, with the confidence to hold back when the diagnosis is clear, and push harder when we know that something does not fit.”
Emotional Dimension
Although many diagnostic errors are attributable to mistakes in thinking, emotions, and feelings—which may not be easy to detect or admit—also contribute to decision-making.
As hypothesized by noted neurologist and author Antonio Damasio in Descartes’ Error: Emotion, Reason, and the Human Brain, some feelings—visceral signals he calls somatic markers—deter us from or attract us to certain images and decisions.6 Remaining cognizant of those feelings helps clarify how they may inform a medical decision—for good and bad.
The emotional dimension of decision-making cannot be disregarded, says Dr. Groopman. “We need to take our emotional temperature; there are patients we like more and patients we like less,” he says. “There are times when we are tremendously motivated to succeed with a very complicated and daunting patient in the hospital, and there are times when we retreat from that for whatever psychological reason. Sometimes it’s fear of failure, sometimes it’s stereotyping. Regardless, we need to have a level of self-awareness.”
The stressful atmosphere of hospital-based medicine contributes to a high level of anxiety. “Physicians use a telegraphic language full of sound bytes with each other that may contribute to the way heuristics are passed from one generation of doctors to the next,” Dr. Groopman says. “That language is enormously powerful in guiding our thinking and the kinds of shortcuts that we use.”
Pitfalls in Reasoning
Of all the bias errors in clinical reasoning, two of the most influential on physicians are anchoring and attribution. Bound-ed rationality—the failure to continue considering reasonable alternatives after an initial diagnosis is reached—is also a pitfall. The difference between the latter and anchoring is whether the clinician adjusts the diagnosis when new data emerge.
Anchoring errors may arise from seizing the first bits of data and allowing them to guide all future questioning. “It happens every day,” says Dr. Feinbloom. “The diagnosis kind of feels right. There is something about the speed with which it comes to mind, the familiarity with the diagnosis in question, [that] reinforces your confidence.”
Dr. Feinbloom teaches his young trainees to trust no one. “I mean that in a good-hearted way,” he says. “Never assume what you’re told is accurate. You have to review everything yourself, interview the patient again; skepticism is a powerful tool.”
With the woman who was ultimately diagnosed with Zollinger-Ellison syndrome, Dr. Li’s skepticism paid off—and the hospitalist team benefited from deconstructing its clinical thinking to see where it went awry.
“If someone had gotten the gastrin level earlier,” says Dr. Feinbloom, “they would have caught it, but it was not on anyone’s radar. When imaging was negative, the team assumed it wasn’t a tumor.”
Lessons Learned
There are lots of lessons here, says Dr. Feinbloom. “You could spin it any one of five different ways with heuristic lessons, but what jumped out at me was that if you don’t know it, you don’t know it, and you can’t diagnose it,’’ he says. “And that gives you a sense of confidence that you’ve covered everything.”
No one had a familiarity with the subtle manifestations of that diagnosis until Dr. Li stepped in. “One lesson is that if you think the patient is on the up and up, and you haven’t yet made a diagnosis,” says Dr. Feinbloom, “it doesn’t mean there’s no diagnosis to be made.”
Dr. Li gives this lesson to his students this way: You may not have seen diagnosis X, but has diagnosis X seen you?
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Graber ML, Franklin N, Gordon R. Diagnostic error in internal medicine. Arch Intern Med. 2005;165(13):1493-1499.
- Wachter RM. Is ambulatory patient safety just like hospital safety, only without the ‘‘stat’’? Ann Intern Med. 2006;145(7):547-549.
- Schiff GD, Kim S, Abrams R, et al. Diagnosing diagnosis errors: lessons from a multi-institutional collaborative project. Rockville, MD: Agency for Healthcare Research and Quality (AHRQ Publication No.050021-2.); 2005.
- Kempainen RR, Migeon MB, Wolf FM. Understanding our mistakes: a primer on errors in clinical reasoning. Med Teach. 2003;25(2):177-181.
- Redelmeier DA. Improving patient care. The cognitive psychology of missed diagnoses. Ann Intern Med. 2005;142(2):115-120.
- Damasio AR. Descartes’ Error: Emotion, Reason, and the Human Brain. New York: GP Putnam’s Sons; 1995.
This is the first of a two-part series examining medical errors. This article addresses thought processes hospitalists use that may lead to mistaken diagnoses. Part 2 will look at what healthcare corporations are doing to improve diagnoses and reduce errors.
When talking about tough diagnoses, academic hospitalist David Feinbloom, MD, recalls the story of a female patient seen by his hospitalist group whose diagnosis took some time to nail down.
This woman had been in and out of the hospital for several years with nonspecific abdominal pain and intermittent diarrhea. She had been seen by numerous doctors and tested extensively. Increasingly her doctors concluded that there was some psychiatric overlay—she was depressed or somatic.
“Patients like these are very common and often end up on the hospitalist service,” says Dr. Feinbloom, who works at Beth Israel Deaconess Medical Center in Boston.
But to Joseph Li, MD, director of the hospital medicine program at Beth Israel, this patient seemed normal. There was something about the symptoms she described that reminded him of a patient he had seen who had been diagnosed with a metastatic neuroendocrine tumor.
Although this patient’s past MRI had been negative, Dr. Li remembered that if you don’t perform the right MRI protocol, you’ll miss something. He asked the team to obtain a panel looking for specific markers and to repeat the MRI with the correct protocol. It was accepted as fact that there was no pathology to explain her symptoms but that she had had every test. He requested another gastrointestinal (GI) consult.
“It seemed so far out there, and then everything he said was completely correct,” says Dr. Feinbloom. “She had Zollinger-Ellison syndrome.”
Clues from Sherlock
In his book How Doctors Think, Jerome Groopman, MD, discusses Sir Arthur Conan Doyle, physician and creator of the brilliant detective Sherlock Holmes. When it comes to solving crimes, Holmes’ superior observation and logic, intellectual prowess, and pristine reasoning help him observe and interpret the most obscure and arcane clues. He is, in the end, a consummate diagnostician.
One of the first rules a great diagnostician must follow is to not get boxed into one way of thinking, says Dr. Groopman, the Dina and Raphael Recanati chair of medicine at the Harvard Medical School and chief of experimental medicine at the Beth Israel Deaconess Medical Center, Boston. That is one of the downsides of a too-easy attachment to using clinical practice guidelines, he says.
“Guidelines are valuable reference points, but in order to use a guideline effectively, you have to have the correct diagnosis,” he says. “Studies over decades with hospitalized patients show that the misdiagnosis rate is at least 15% and hasn’t changed.1 A great deal of effort needs to be put into improving our accuracy in making diagnoses.”
Compared with other kinds of medical errors, diagnostic errors have not gotten a great deal of attention. The hospital patient safety movement has been more focused on preventing medication errors, surgical errors, handoff communications, nosocomial infections, falls, and blood clots.2 There have been few studies pertaining exclusively to diagnostic errors—but the topic is gaining headway.3
Think about Thinking
Diagnostic errors are usually multifactorial in origin and typically involve system-related and individual factors. The systems-based piece includes environmental and organizational factors. Medical researchers conclude the majority of diagnostic errors arise from flaws in physician thinking, not technical mistakes.
Cognitive errors involve instances where knowledge, data gathering, data processing, or verification (such as by lab testing) are faulty. Improving diagnostics will require better accountability by institutions and individuals. To do the latter, experts say, physicians would do well to familiarize themselves with their diagnostic weaknesses.
Thinking about thinking is the science of cognitive psychology and addresses the cognitive aspects of clinical reasoning underlying diagnostic decision-making. It is an area of study in which few medical professionals are versed. “Except for a few of these guys who trained in psych or were voices in the wilderness that have been largely ignored,” most physicians are unaware of the cognitive psychology literature, Dr. Groopman says.
Common biases and errors in clinical reasoning are presented in Table 1 (right).4,5 These are largely individual mistakes for which physicians traditionally have been accountable.
Patterns and Heuristics
The following factors contribute to how shortcuts are used: the pressures of working in medicine, the degrees of uncertainty a physician may feel, and the fact that hospitalists rarely have all the information they need about a patient.
“That’s just the nature of medicine,” says Dr. Groopman. “These shortcuts are natural ways of thinking under those conditions. They succeed about 85% of the time; they fail up to 10-20% of the time. The first thing we need to educate ourselves about is that this is how our minds work as doctors.”
Dr. Groopman and those he interviewed for his book have a razor-sharp overview of clinical practice within hospitals throughout the U.S. and Canada, including academic centers, community centers, affluent areas, suburbs, inner cities, and Native American reservations. But except for Pat Croskerry, MD, PhD, in the department of emergency medicine at Dalhousie University’s Queen Elizabeth II Health Sciences Center in Halifax, Nova Scotia, none of the experts he interviewed had rigorous training in cognitive science.
Although how to think is a priority in physicians’ training, how to think about one’s thinking is not.
“We are not given a vocabulary during medical training, or later through CME courses, in this emerging science—and yet this science involves how our mind works successfully and when we make mistakes,” Dr. Groopman says.
The data back this assertion. In a study of 100 cases of diagnostic error, 90 involved injury, including 33 deaths; 74% were attributed to errors in cognitive reasoning (see Figure 1, right).1 Failure to consider reasonable alternatives after an initial diagnosis was the most common cause. Other common causes included faulty context generation, misjudging the salience of findings, faulty perception, and errors connected with the use of heuristics. In this study, faulty or inadequate knowledge was uncommon.
Underlying contributions to error fell into three categories: “no fault,” system-related, and cognitive. Only seven cases reflected no-fault errors alone. In the remaining 93 cases, 548 errors were identified as system-related or cognitive factors (5.9 per case). System-related factors contributed to the diagnostic error in 65% of the cases and cognitive factors in 74%. The most common system-related factors involved problems with policies and procedures, inefficient processes, teamwork, and communication. The most common cognitive problems involved faulty synthesis.
Dr. Groopman believes it is important for physicians to be more introspective about the thinking patterns they employ and learn the traps to which they are susceptible. He also feels it is imperative to develop curricula at different stages of medical training so this new knowledge can be used to reduce error rates. Because the names for these traps can vary, the development of a universal and comprehensive taxonomy for classifying diagnostic errors is also needed.
“It’s impossible to be perfect; we’re never going to be 100%,” Dr. Groopman says. “But I deeply believe that it is quite feasible to think about your thinking and to assess how your mind came to a conclusion about a diagnosis and treatment plan.”
When phy-sicians think about errors in cognitive reasoning, they often focus on the “don’t-miss diagnoses” or the uncommon variant missed by recall or anchoring errors.
“When I reflect on the errors I have made, they mostly fall into the categories that Dr. Groopman describes in his book,” Dr. Feinbloom says. “Interestingly, the errors that I see most often stem from the fear of making an error of omission.”
It is paradoxical, but in order to ensure that no possible diagnosis is missed, doctors often feel the need to rule out all possible diagnoses.
“While it makes us feel that we are doing the best for our patients, this approach leads to an inordinate amount of unnecessary testing and potentially harmful interventions,” says Dr. Feinbloom. “Understanding how cognitive errors occur should allow us to be judicious in our approach, with the confidence to hold back when the diagnosis is clear, and push harder when we know that something does not fit.”
Emotional Dimension
Although many diagnostic errors are attributable to mistakes in thinking, emotions, and feelings—which may not be easy to detect or admit—also contribute to decision-making.
As hypothesized by noted neurologist and author Antonio Damasio in Descartes’ Error: Emotion, Reason, and the Human Brain, some feelings—visceral signals he calls somatic markers—deter us from or attract us to certain images and decisions.6 Remaining cognizant of those feelings helps clarify how they may inform a medical decision—for good and bad.
The emotional dimension of decision-making cannot be disregarded, says Dr. Groopman. “We need to take our emotional temperature; there are patients we like more and patients we like less,” he says. “There are times when we are tremendously motivated to succeed with a very complicated and daunting patient in the hospital, and there are times when we retreat from that for whatever psychological reason. Sometimes it’s fear of failure, sometimes it’s stereotyping. Regardless, we need to have a level of self-awareness.”
The stressful atmosphere of hospital-based medicine contributes to a high level of anxiety. “Physicians use a telegraphic language full of sound bytes with each other that may contribute to the way heuristics are passed from one generation of doctors to the next,” Dr. Groopman says. “That language is enormously powerful in guiding our thinking and the kinds of shortcuts that we use.”
Pitfalls in Reasoning
Of all the bias errors in clinical reasoning, two of the most influential on physicians are anchoring and attribution. Bound-ed rationality—the failure to continue considering reasonable alternatives after an initial diagnosis is reached—is also a pitfall. The difference between the latter and anchoring is whether the clinician adjusts the diagnosis when new data emerge.
Anchoring errors may arise from seizing the first bits of data and allowing them to guide all future questioning. “It happens every day,” says Dr. Feinbloom. “The diagnosis kind of feels right. There is something about the speed with which it comes to mind, the familiarity with the diagnosis in question, [that] reinforces your confidence.”
Dr. Feinbloom teaches his young trainees to trust no one. “I mean that in a good-hearted way,” he says. “Never assume what you’re told is accurate. You have to review everything yourself, interview the patient again; skepticism is a powerful tool.”
With the woman who was ultimately diagnosed with Zollinger-Ellison syndrome, Dr. Li’s skepticism paid off—and the hospitalist team benefited from deconstructing its clinical thinking to see where it went awry.
“If someone had gotten the gastrin level earlier,” says Dr. Feinbloom, “they would have caught it, but it was not on anyone’s radar. When imaging was negative, the team assumed it wasn’t a tumor.”
Lessons Learned
There are lots of lessons here, says Dr. Feinbloom. “You could spin it any one of five different ways with heuristic lessons, but what jumped out at me was that if you don’t know it, you don’t know it, and you can’t diagnose it,’’ he says. “And that gives you a sense of confidence that you’ve covered everything.”
No one had a familiarity with the subtle manifestations of that diagnosis until Dr. Li stepped in. “One lesson is that if you think the patient is on the up and up, and you haven’t yet made a diagnosis,” says Dr. Feinbloom, “it doesn’t mean there’s no diagnosis to be made.”
Dr. Li gives this lesson to his students this way: You may not have seen diagnosis X, but has diagnosis X seen you?
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Graber ML, Franklin N, Gordon R. Diagnostic error in internal medicine. Arch Intern Med. 2005;165(13):1493-1499.
- Wachter RM. Is ambulatory patient safety just like hospital safety, only without the ‘‘stat’’? Ann Intern Med. 2006;145(7):547-549.
- Schiff GD, Kim S, Abrams R, et al. Diagnosing diagnosis errors: lessons from a multi-institutional collaborative project. Rockville, MD: Agency for Healthcare Research and Quality (AHRQ Publication No.050021-2.); 2005.
- Kempainen RR, Migeon MB, Wolf FM. Understanding our mistakes: a primer on errors in clinical reasoning. Med Teach. 2003;25(2):177-181.
- Redelmeier DA. Improving patient care. The cognitive psychology of missed diagnoses. Ann Intern Med. 2005;142(2):115-120.
- Damasio AR. Descartes’ Error: Emotion, Reason, and the Human Brain. New York: GP Putnam’s Sons; 1995.
This is the first of a two-part series examining medical errors. This article addresses thought processes hospitalists use that may lead to mistaken diagnoses. Part 2 will look at what healthcare corporations are doing to improve diagnoses and reduce errors.
When talking about tough diagnoses, academic hospitalist David Feinbloom, MD, recalls the story of a female patient seen by his hospitalist group whose diagnosis took some time to nail down.
This woman had been in and out of the hospital for several years with nonspecific abdominal pain and intermittent diarrhea. She had been seen by numerous doctors and tested extensively. Increasingly her doctors concluded that there was some psychiatric overlay—she was depressed or somatic.
“Patients like these are very common and often end up on the hospitalist service,” says Dr. Feinbloom, who works at Beth Israel Deaconess Medical Center in Boston.
But to Joseph Li, MD, director of the hospital medicine program at Beth Israel, this patient seemed normal. There was something about the symptoms she described that reminded him of a patient he had seen who had been diagnosed with a metastatic neuroendocrine tumor.
Although this patient’s past MRI had been negative, Dr. Li remembered that if you don’t perform the right MRI protocol, you’ll miss something. He asked the team to obtain a panel looking for specific markers and to repeat the MRI with the correct protocol. It was accepted as fact that there was no pathology to explain her symptoms but that she had had every test. He requested another gastrointestinal (GI) consult.
“It seemed so far out there, and then everything he said was completely correct,” says Dr. Feinbloom. “She had Zollinger-Ellison syndrome.”
Clues from Sherlock
In his book How Doctors Think, Jerome Groopman, MD, discusses Sir Arthur Conan Doyle, physician and creator of the brilliant detective Sherlock Holmes. When it comes to solving crimes, Holmes’ superior observation and logic, intellectual prowess, and pristine reasoning help him observe and interpret the most obscure and arcane clues. He is, in the end, a consummate diagnostician.
One of the first rules a great diagnostician must follow is to not get boxed into one way of thinking, says Dr. Groopman, the Dina and Raphael Recanati chair of medicine at the Harvard Medical School and chief of experimental medicine at the Beth Israel Deaconess Medical Center, Boston. That is one of the downsides of a too-easy attachment to using clinical practice guidelines, he says.
“Guidelines are valuable reference points, but in order to use a guideline effectively, you have to have the correct diagnosis,” he says. “Studies over decades with hospitalized patients show that the misdiagnosis rate is at least 15% and hasn’t changed.1 A great deal of effort needs to be put into improving our accuracy in making diagnoses.”
Compared with other kinds of medical errors, diagnostic errors have not gotten a great deal of attention. The hospital patient safety movement has been more focused on preventing medication errors, surgical errors, handoff communications, nosocomial infections, falls, and blood clots.2 There have been few studies pertaining exclusively to diagnostic errors—but the topic is gaining headway.3
Think about Thinking
Diagnostic errors are usually multifactorial in origin and typically involve system-related and individual factors. The systems-based piece includes environmental and organizational factors. Medical researchers conclude the majority of diagnostic errors arise from flaws in physician thinking, not technical mistakes.
Cognitive errors involve instances where knowledge, data gathering, data processing, or verification (such as by lab testing) are faulty. Improving diagnostics will require better accountability by institutions and individuals. To do the latter, experts say, physicians would do well to familiarize themselves with their diagnostic weaknesses.
Thinking about thinking is the science of cognitive psychology and addresses the cognitive aspects of clinical reasoning underlying diagnostic decision-making. It is an area of study in which few medical professionals are versed. “Except for a few of these guys who trained in psych or were voices in the wilderness that have been largely ignored,” most physicians are unaware of the cognitive psychology literature, Dr. Groopman says.
Common biases and errors in clinical reasoning are presented in Table 1 (right).4,5 These are largely individual mistakes for which physicians traditionally have been accountable.
Patterns and Heuristics
The following factors contribute to how shortcuts are used: the pressures of working in medicine, the degrees of uncertainty a physician may feel, and the fact that hospitalists rarely have all the information they need about a patient.
“That’s just the nature of medicine,” says Dr. Groopman. “These shortcuts are natural ways of thinking under those conditions. They succeed about 85% of the time; they fail up to 10-20% of the time. The first thing we need to educate ourselves about is that this is how our minds work as doctors.”
Dr. Groopman and those he interviewed for his book have a razor-sharp overview of clinical practice within hospitals throughout the U.S. and Canada, including academic centers, community centers, affluent areas, suburbs, inner cities, and Native American reservations. But except for Pat Croskerry, MD, PhD, in the department of emergency medicine at Dalhousie University’s Queen Elizabeth II Health Sciences Center in Halifax, Nova Scotia, none of the experts he interviewed had rigorous training in cognitive science.
Although how to think is a priority in physicians’ training, how to think about one’s thinking is not.
“We are not given a vocabulary during medical training, or later through CME courses, in this emerging science—and yet this science involves how our mind works successfully and when we make mistakes,” Dr. Groopman says.
The data back this assertion. In a study of 100 cases of diagnostic error, 90 involved injury, including 33 deaths; 74% were attributed to errors in cognitive reasoning (see Figure 1, right).1 Failure to consider reasonable alternatives after an initial diagnosis was the most common cause. Other common causes included faulty context generation, misjudging the salience of findings, faulty perception, and errors connected with the use of heuristics. In this study, faulty or inadequate knowledge was uncommon.
Underlying contributions to error fell into three categories: “no fault,” system-related, and cognitive. Only seven cases reflected no-fault errors alone. In the remaining 93 cases, 548 errors were identified as system-related or cognitive factors (5.9 per case). System-related factors contributed to the diagnostic error in 65% of the cases and cognitive factors in 74%. The most common system-related factors involved problems with policies and procedures, inefficient processes, teamwork, and communication. The most common cognitive problems involved faulty synthesis.
Dr. Groopman believes it is important for physicians to be more introspective about the thinking patterns they employ and learn the traps to which they are susceptible. He also feels it is imperative to develop curricula at different stages of medical training so this new knowledge can be used to reduce error rates. Because the names for these traps can vary, the development of a universal and comprehensive taxonomy for classifying diagnostic errors is also needed.
“It’s impossible to be perfect; we’re never going to be 100%,” Dr. Groopman says. “But I deeply believe that it is quite feasible to think about your thinking and to assess how your mind came to a conclusion about a diagnosis and treatment plan.”
When phy-sicians think about errors in cognitive reasoning, they often focus on the “don’t-miss diagnoses” or the uncommon variant missed by recall or anchoring errors.
“When I reflect on the errors I have made, they mostly fall into the categories that Dr. Groopman describes in his book,” Dr. Feinbloom says. “Interestingly, the errors that I see most often stem from the fear of making an error of omission.”
It is paradoxical, but in order to ensure that no possible diagnosis is missed, doctors often feel the need to rule out all possible diagnoses.
“While it makes us feel that we are doing the best for our patients, this approach leads to an inordinate amount of unnecessary testing and potentially harmful interventions,” says Dr. Feinbloom. “Understanding how cognitive errors occur should allow us to be judicious in our approach, with the confidence to hold back when the diagnosis is clear, and push harder when we know that something does not fit.”
Emotional Dimension
Although many diagnostic errors are attributable to mistakes in thinking, emotions, and feelings—which may not be easy to detect or admit—also contribute to decision-making.
As hypothesized by noted neurologist and author Antonio Damasio in Descartes’ Error: Emotion, Reason, and the Human Brain, some feelings—visceral signals he calls somatic markers—deter us from or attract us to certain images and decisions.6 Remaining cognizant of those feelings helps clarify how they may inform a medical decision—for good and bad.
The emotional dimension of decision-making cannot be disregarded, says Dr. Groopman. “We need to take our emotional temperature; there are patients we like more and patients we like less,” he says. “There are times when we are tremendously motivated to succeed with a very complicated and daunting patient in the hospital, and there are times when we retreat from that for whatever psychological reason. Sometimes it’s fear of failure, sometimes it’s stereotyping. Regardless, we need to have a level of self-awareness.”
The stressful atmosphere of hospital-based medicine contributes to a high level of anxiety. “Physicians use a telegraphic language full of sound bytes with each other that may contribute to the way heuristics are passed from one generation of doctors to the next,” Dr. Groopman says. “That language is enormously powerful in guiding our thinking and the kinds of shortcuts that we use.”
Pitfalls in Reasoning
Of all the bias errors in clinical reasoning, two of the most influential on physicians are anchoring and attribution. Bound-ed rationality—the failure to continue considering reasonable alternatives after an initial diagnosis is reached—is also a pitfall. The difference between the latter and anchoring is whether the clinician adjusts the diagnosis when new data emerge.
Anchoring errors may arise from seizing the first bits of data and allowing them to guide all future questioning. “It happens every day,” says Dr. Feinbloom. “The diagnosis kind of feels right. There is something about the speed with which it comes to mind, the familiarity with the diagnosis in question, [that] reinforces your confidence.”
Dr. Feinbloom teaches his young trainees to trust no one. “I mean that in a good-hearted way,” he says. “Never assume what you’re told is accurate. You have to review everything yourself, interview the patient again; skepticism is a powerful tool.”
With the woman who was ultimately diagnosed with Zollinger-Ellison syndrome, Dr. Li’s skepticism paid off—and the hospitalist team benefited from deconstructing its clinical thinking to see where it went awry.
“If someone had gotten the gastrin level earlier,” says Dr. Feinbloom, “they would have caught it, but it was not on anyone’s radar. When imaging was negative, the team assumed it wasn’t a tumor.”
Lessons Learned
There are lots of lessons here, says Dr. Feinbloom. “You could spin it any one of five different ways with heuristic lessons, but what jumped out at me was that if you don’t know it, you don’t know it, and you can’t diagnose it,’’ he says. “And that gives you a sense of confidence that you’ve covered everything.”
No one had a familiarity with the subtle manifestations of that diagnosis until Dr. Li stepped in. “One lesson is that if you think the patient is on the up and up, and you haven’t yet made a diagnosis,” says Dr. Feinbloom, “it doesn’t mean there’s no diagnosis to be made.”
Dr. Li gives this lesson to his students this way: You may not have seen diagnosis X, but has diagnosis X seen you?
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Graber ML, Franklin N, Gordon R. Diagnostic error in internal medicine. Arch Intern Med. 2005;165(13):1493-1499.
- Wachter RM. Is ambulatory patient safety just like hospital safety, only without the ‘‘stat’’? Ann Intern Med. 2006;145(7):547-549.
- Schiff GD, Kim S, Abrams R, et al. Diagnosing diagnosis errors: lessons from a multi-institutional collaborative project. Rockville, MD: Agency for Healthcare Research and Quality (AHRQ Publication No.050021-2.); 2005.
- Kempainen RR, Migeon MB, Wolf FM. Understanding our mistakes: a primer on errors in clinical reasoning. Med Teach. 2003;25(2):177-181.
- Redelmeier DA. Improving patient care. The cognitive psychology of missed diagnoses. Ann Intern Med. 2005;142(2):115-120.
- Damasio AR. Descartes’ Error: Emotion, Reason, and the Human Brain. New York: GP Putnam’s Sons; 1995.
What is the best medical therapy for the secondary prevention of stroke?
The Case
A 62-year-old obese woman with prior history of type 2 diabetes, hypertension, and a pack-a-day smoking habit presented to the emergency department (ED) for acute onset of right-side weakness and sensory loss noted on awakening from sleep.
She reports taking a baby aspirin daily to “prevent heart attacks” prior to her stroke. Her electrocardiogram demonstrates a left bundle branch block and frequent premature atrial contractions. She recovers with mild hemiparesis and is ready for discharge. What is the best medical therapy for secondary prevention of stroke?
Overview
Cerebrovascular accident (CVA) represents an important diagnosis for the hospitalist, with 700,000 people suffering a stroke in the U.S. each year.1 This translates to a stroke every 45 seconds. About 200,000 of these strokes are recurrent events.
Cardioembolism is the largest cause of ischemic strokes, representing 29% of all infarcts.2 Stasis from impaired contractile function, atrial fibrillation, or mechanical valves are significant risk factors. More rarely, a paradoxical embolus arising in the venous system may pass through a patent foramen ovale.
Large-artery atherosclerosis and lacunar infarcts each account for 16% of strokes. Risk factors for these forms of strokes are the same as those for atherosclerosis and include hypertension and diabetes. Rarer causes such as vasculitis, dissection, hypercoagulability, or hematological disorders account for 3% of strokes. Work-up for these should be driven by historical and atypical features such as young age, family history, or unusual distribution of ischemic zones. Despite appropriate work-up, the mechanism remains uncertain in 36% of strokes.
Regardless of the manifestation and residua of the index event, the hospitalist must initiate appropriate therapy to prevent a disabling CVA. While antithrombotic drugs are the mainstay of secondary prevention, it is a mistake to miss other opportunities for risk modification. Optimal management requires a tailored evaluation for etiology, identification of modifiable risk factors, and initiation of antiplatelet or anticoagulant therapy.
Cardioembolic Stroke
Treatment of stroke depends on the etiology of the original infarct. Evidence is strong that the optimal therapy for cardioembolic stroke is anticoagulation with warfarin.
The European Atrial Fibrillation Trial found that warfarin reduces the risk for second strokes in patients with atrial fibrillation by two-thirds and is superior to antiplatelet agents for preventing cardioembolic strokes.3 Warfarin increases the risk of extracranial bleeding, but not severely enough to negate the benefit of reducing stroke death and disability. The target international normalized ratio (INR) for non-valvular atrial fibrillation is generally two to three, although this may be higher for certain prosthetic valves.
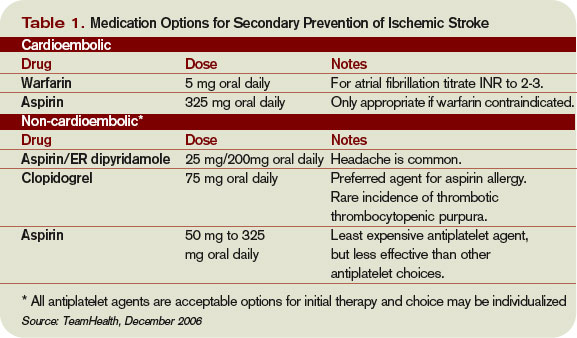
Noncardioembolic Stroke
For large-vessel atherosclerotic and lacunar cerebral ischemia, the oldest—and still effective—treatment for recurrent stroke is aspirin. The use of low-dose aspirin after transient ischemic attack (TIA) or stroke reduces second strokes or death by approximately 15%-18%.4-5 Larger doses do not appear to be more effective, although the rate of gastrointestinal complaints is greater with increased dosage. The use of either 325 mg or 1,200 mg of aspirin produced the same 15% reduction in second ischemic events. Similar efficacy has been seen in comparisons between 30 mg and 283 mg dosing.6
While a subset of patients may experience aspirin resistance, reliable assays in clinical practice are not commonly available to guide management. Current recommendations suggest that use of between 50 mg and 325 mg of aspirin is appropriate for secondary prevention.7
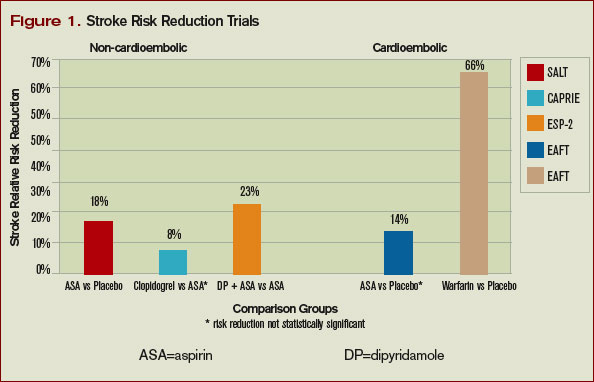
Clopidogrel is another antiplatelet agent that can be given daily at 75 mg as alternate therapy for secondary prevention of non-cardioembolic stroke. The Clopidogrel versus Aspirin in Patients at Risk of Ischemic Events trial comparing clopidogrel with aspirin in patients at risk of ischemic events demonstrated significant reduction in the annual rate of combined endpoint of stroke, myocardial infarction, and vascular death—from 5.83% with aspirin to 5.32% with clopidogrel.8 This study’s applicability to secondary prevention of stroke is limited by the fact that only 19% of the patients in this trial were included because of prior stroke, and the results were not significant for reduction of stroke as a lone endpoint. Clopidogrel is recommended as an acceptable agent for CVA secondary prevention and is preferred for patients with stroke and an aspirin allergy or with recent coronary stent.
The combination of a low-dose aspirin and extended-release dipyridamole has proved superior to aspirin monotherapy in multiple trials. Over two years, the European Stroke Prevention 2 trial found an 18% reduction with aspirin alone compared with 37% reduction with the combination therapy, and the European/Australasian Stroke Prevention in Reversible Ischaemia trial confirmed that the combination reduced the absolute rate of second ischemic events by 1% annually.9-10 Headache is a common side effect of dipyridamole and may limit use. Dypridamole/aspirin is recommended as another acceptable option for secondary prevention of non-cardioembolic stroke.
Evidence suggests that aspirin/dipyridamole and clopidogrel—although significantly more expensive—are more effective than aspirin monotherapy for preventing second cerebral ischemic events. Direct comparison between aspirin/dipyridamole and clopidogrel is ongoing in the Prevention Regimen for Effectively Avoiding Second Stroke trial, with results anticipated in 2008.
Things That Don’t Work
The Warfarin-Aspirin Recurrent Stroke Study trial demonstrated that warfarin was not better than aspirin for prevention of non-cardioembolic stroke, and the Warfarin–Aspirin Symptomatic Intracranial Disease trial found the same result for patients with intracranial stenosis.11-12 There is little evidence that warfarin should have a role in the treatment of most non-cardioembolic strokes. The MATCH trial failed to show benefit to adding aspirin to clopidogrel over clopidogrel monotherapy for secondary preventions of non-cardioembolic cerebral ischemia.13 Despite efficacy following coronary stenting, the combination of clopidogrel and aspirin can not be recommended for stroke prevention.

What To Do
Aggressive risk factor modification is key in the prevention of second ischemic events. One of the most promising therapies is the use of statins following a CVA. Maintaining low-density lipoprotein (LDL) at less than 100 mg/dL (or less than 70 mg/dL in the highest-risk patients) is recommended despite a relatively weak association between stroke and hyperlipidemia.
This stands in contrast to the strong relationship between elevated LDL and coronary disease. However, the Stroke Prevention by Aggressive Reduction in Cholesterol Levels trial utilized high-dose atorvastatin after acute CVA and was able to create an absolute risk reduction for second stroke of 2.2% over the next five years.14 It is possible that the findings of this trial may reflect actions of statin therapy on the endothelium independent of the lipid lowering effect.
Blood pressure commonly has a transient elevation following cerebral ischemia. This is managed permissively to preserve perfusion to the ischemic penumbra. Once the hyperacute period is over, reduction of blood pressure to less than 140/90 mm/Hg (130/80 mm/Hg for diabetics) is recommended.
Interventions to treat chronic hypertension have been demonstrated to reduce the rate of strokes by approximately 30% to 40% over four to five years.15-16 An optimal agent has not been determined, but therapy with angiotensin converting enzyme inhibitor (ACE-I) or angiotensin II receptor blocker (ARB), possibly in combination with a diuretic, have been effective. Close follow-up for titration to goal in the outpatient setting should be arranged. Diabetics should have optimization of glycemic control, and lifestyle counseling should occur regarding recognized risk factors for stroke such as smoking, inactivity, and alcohol abuse.
While antithrombotic therapy is the mainstay of what we think of in secondary prevention of stroke, treatment of these other modifiable risk factors have been shown to affect mortality and second strokes of a similar magnitude and should not be neglected.
How to Treat This Case
The patient described should undergo an MRI with diffusion (to define the area of ischemia) and targeted evaluation for etiology with cardiac monitoring, echocardiogram, and carotid ultrasound.
Assuming atrial fibrillation or intracardiac thrombus is ruled out, this likely represents atherosclerotic disease. MRI will help distinguish between large-vessel atherosclerotic etiology and lacunar infarct. If carotid stenosis of greater than 70% is found in the setting of large vessel atherosclerotic stroke, then she should be referred for carotid endarterectomy. At 50% to 69% stenosis, carotid endarterectomy would still be a consideration. Antithrombotic agent of choice for non-cardioembolic CVA is an anti-platelet agent. With a stroke occurring on a reasonable dose of aspirin, I would not recommend increasing the dose as there is little evidence that 325 mg is more effective than 81mg. The most appropriate step would be to change to an alternate anti-platelet agent such as combination dipyridamole/aspirin or clopidogrel.
In the absence of a direct comparison trial, either choice is acceptable. The evidence supporting dipyridamole/aspirin is stronger for secondary stroke prevention. Atorvastatin 80 mg daily is an evidence-based therapy after acute stroke and can be started immediately. Her hypertension should be managed permissively for the first few days after the acute event, but then an ACE-I or ARB—possibly in combination with a diuretic—would be appropriate. This patient’s goal blood pressure as a diabetic would be at least less than 130/80 mm/Hg.
Finally we would be remiss if we did not stress the importance of smoking cessation, exercise, and weight loss. TH
Dr. Cumbler is an assistant professor in the Section of Hospital Medicine at the University of Colorado, where he is a member of the Acute Stroke Service and serves on the Stroke Council.
References
- Rosamond W, Flegal K, Friday G, et al. Heart disease and stroke statistics-2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007 Feb 6;115(5):e69-e171.
- Petty GW, Brown RD, Whisnant JP, et al. Ischemic stroke subtypes: a population-based study of incidence and risk factors. Stroke. 1999;30:2513-2516.
- European Atrial Fibrillation Trial Study Group. Secondary prevention in non-rheumatic atrial fibrillation after transient ischaemic attack or minor stroke. Lancet. 1993;342:1255-1262.
- Swedish Aspirin Low-Dose Trial Collaborative Group. Swedish aspirin low-dose aspirin trial (SALT) of 775 mg aspirin as secondary prophylaxis after cerebrovascular ischaemic events. Lancet. 1991;338(8779):1345-1349.
- Farrell B, Godwin J, Richards S, et al. The United Kingdom Transient Ischaemic Attack (UK-TIA) aspirin trial: final results (abstract). J Neurol Neurosurg. Psychiatry 1991;54:1044-1054.
- Dutch TIA Trial Study Group. A comparison of two doses of aspirin (30 mg versus 283 mg a day) in patients after a transient ischemic attack or minor ischemic stroke. N Engl J Med. 1991 Oct 31;325(18):1261-1266.
- Sacco RL, Adams R, Albers G, et al. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack. Stroke. 2006 Feb;37(2):577-617.
- CAPRIE Steering Committee. A randomized, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events. Lancet 1996 Jan;348:1329-1339.
- Diener H, Cunha L, Forbes C, et al. European stroke prevention study 2: dipyridamole and acetylsalicylic acid in the secondary prevention of stroke. J Neurol Sci. 1996;143:1-13.
- ESPRIT Study Group. Aspirin plus dipyridamole versus aspirin alone after cerebral ischaemia of arterial origin (ESPRIT): randomised controlled trial. Lancet. 2006;367:1665-1673.
- Mohr JP, Thompson JLP, Lazar RM, et al. A comparison of warfarin and aspirin for the prevention of recurrent ischemic stroke. N Engl J Med. 2001 Nov 15; 345(20):1444-1451.
- Chimowitz MI, Lynn MJ, Howlett-Smith H, et al. Comparison of warfarin and aspirin for symptomatic intracranial arterial stenosis. N Engl J Med. 2005 Mar 31;352(13):1305-1316.
- Diener HC, Bogousslavsky J, Brass LM, et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo controlled trial. Lancet. 2004 Jul 24-30;36499431):331-337.
- Stroke Prevention by Aggressive Reduction in Cholesterol Levels Investigators. High-dose atorvastatin after stroke or transient ischemic attack. N Engl J Med. 2006;355(6):549-559.
- The PROGRESS Collaborative Group. Randomised trial of a perindopril-based blood-pressure-lowering regimen among 6,105 individuals with previous stroke or transient ischaemic attack. Lancet 2001;358(9287):1033-1041.
- The Heart Outcomes Prevention Evaluation Study Investigators. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. N Engl J Med. 2000 Jan 20;342:145-153.
The Case
A 62-year-old obese woman with prior history of type 2 diabetes, hypertension, and a pack-a-day smoking habit presented to the emergency department (ED) for acute onset of right-side weakness and sensory loss noted on awakening from sleep.
She reports taking a baby aspirin daily to “prevent heart attacks” prior to her stroke. Her electrocardiogram demonstrates a left bundle branch block and frequent premature atrial contractions. She recovers with mild hemiparesis and is ready for discharge. What is the best medical therapy for secondary prevention of stroke?
Overview
Cerebrovascular accident (CVA) represents an important diagnosis for the hospitalist, with 700,000 people suffering a stroke in the U.S. each year.1 This translates to a stroke every 45 seconds. About 200,000 of these strokes are recurrent events.
Cardioembolism is the largest cause of ischemic strokes, representing 29% of all infarcts.2 Stasis from impaired contractile function, atrial fibrillation, or mechanical valves are significant risk factors. More rarely, a paradoxical embolus arising in the venous system may pass through a patent foramen ovale.
Large-artery atherosclerosis and lacunar infarcts each account for 16% of strokes. Risk factors for these forms of strokes are the same as those for atherosclerosis and include hypertension and diabetes. Rarer causes such as vasculitis, dissection, hypercoagulability, or hematological disorders account for 3% of strokes. Work-up for these should be driven by historical and atypical features such as young age, family history, or unusual distribution of ischemic zones. Despite appropriate work-up, the mechanism remains uncertain in 36% of strokes.
Regardless of the manifestation and residua of the index event, the hospitalist must initiate appropriate therapy to prevent a disabling CVA. While antithrombotic drugs are the mainstay of secondary prevention, it is a mistake to miss other opportunities for risk modification. Optimal management requires a tailored evaluation for etiology, identification of modifiable risk factors, and initiation of antiplatelet or anticoagulant therapy.
Cardioembolic Stroke
Treatment of stroke depends on the etiology of the original infarct. Evidence is strong that the optimal therapy for cardioembolic stroke is anticoagulation with warfarin.
The European Atrial Fibrillation Trial found that warfarin reduces the risk for second strokes in patients with atrial fibrillation by two-thirds and is superior to antiplatelet agents for preventing cardioembolic strokes.3 Warfarin increases the risk of extracranial bleeding, but not severely enough to negate the benefit of reducing stroke death and disability. The target international normalized ratio (INR) for non-valvular atrial fibrillation is generally two to three, although this may be higher for certain prosthetic valves.
Noncardioembolic Stroke
For large-vessel atherosclerotic and lacunar cerebral ischemia, the oldest—and still effective—treatment for recurrent stroke is aspirin. The use of low-dose aspirin after transient ischemic attack (TIA) or stroke reduces second strokes or death by approximately 15%-18%.4-5 Larger doses do not appear to be more effective, although the rate of gastrointestinal complaints is greater with increased dosage. The use of either 325 mg or 1,200 mg of aspirin produced the same 15% reduction in second ischemic events. Similar efficacy has been seen in comparisons between 30 mg and 283 mg dosing.6
While a subset of patients may experience aspirin resistance, reliable assays in clinical practice are not commonly available to guide management. Current recommendations suggest that use of between 50 mg and 325 mg of aspirin is appropriate for secondary prevention.7
Clopidogrel is another antiplatelet agent that can be given daily at 75 mg as alternate therapy for secondary prevention of non-cardioembolic stroke. The Clopidogrel versus Aspirin in Patients at Risk of Ischemic Events trial comparing clopidogrel with aspirin in patients at risk of ischemic events demonstrated significant reduction in the annual rate of combined endpoint of stroke, myocardial infarction, and vascular death—from 5.83% with aspirin to 5.32% with clopidogrel.8 This study’s applicability to secondary prevention of stroke is limited by the fact that only 19% of the patients in this trial were included because of prior stroke, and the results were not significant for reduction of stroke as a lone endpoint. Clopidogrel is recommended as an acceptable agent for CVA secondary prevention and is preferred for patients with stroke and an aspirin allergy or with recent coronary stent.
The combination of a low-dose aspirin and extended-release dipyridamole has proved superior to aspirin monotherapy in multiple trials. Over two years, the European Stroke Prevention 2 trial found an 18% reduction with aspirin alone compared with 37% reduction with the combination therapy, and the European/Australasian Stroke Prevention in Reversible Ischaemia trial confirmed that the combination reduced the absolute rate of second ischemic events by 1% annually.9-10 Headache is a common side effect of dipyridamole and may limit use. Dypridamole/aspirin is recommended as another acceptable option for secondary prevention of non-cardioembolic stroke.
Evidence suggests that aspirin/dipyridamole and clopidogrel—although significantly more expensive—are more effective than aspirin monotherapy for preventing second cerebral ischemic events. Direct comparison between aspirin/dipyridamole and clopidogrel is ongoing in the Prevention Regimen for Effectively Avoiding Second Stroke trial, with results anticipated in 2008.
Things That Don’t Work
The Warfarin-Aspirin Recurrent Stroke Study trial demonstrated that warfarin was not better than aspirin for prevention of non-cardioembolic stroke, and the Warfarin–Aspirin Symptomatic Intracranial Disease trial found the same result for patients with intracranial stenosis.11-12 There is little evidence that warfarin should have a role in the treatment of most non-cardioembolic strokes. The MATCH trial failed to show benefit to adding aspirin to clopidogrel over clopidogrel monotherapy for secondary preventions of non-cardioembolic cerebral ischemia.13 Despite efficacy following coronary stenting, the combination of clopidogrel and aspirin can not be recommended for stroke prevention.
What To Do
Aggressive risk factor modification is key in the prevention of second ischemic events. One of the most promising therapies is the use of statins following a CVA. Maintaining low-density lipoprotein (LDL) at less than 100 mg/dL (or less than 70 mg/dL in the highest-risk patients) is recommended despite a relatively weak association between stroke and hyperlipidemia.
This stands in contrast to the strong relationship between elevated LDL and coronary disease. However, the Stroke Prevention by Aggressive Reduction in Cholesterol Levels trial utilized high-dose atorvastatin after acute CVA and was able to create an absolute risk reduction for second stroke of 2.2% over the next five years.14 It is possible that the findings of this trial may reflect actions of statin therapy on the endothelium independent of the lipid lowering effect.
Blood pressure commonly has a transient elevation following cerebral ischemia. This is managed permissively to preserve perfusion to the ischemic penumbra. Once the hyperacute period is over, reduction of blood pressure to less than 140/90 mm/Hg (130/80 mm/Hg for diabetics) is recommended.
Interventions to treat chronic hypertension have been demonstrated to reduce the rate of strokes by approximately 30% to 40% over four to five years.15-16 An optimal agent has not been determined, but therapy with angiotensin converting enzyme inhibitor (ACE-I) or angiotensin II receptor blocker (ARB), possibly in combination with a diuretic, have been effective. Close follow-up for titration to goal in the outpatient setting should be arranged. Diabetics should have optimization of glycemic control, and lifestyle counseling should occur regarding recognized risk factors for stroke such as smoking, inactivity, and alcohol abuse.
While antithrombotic therapy is the mainstay of what we think of in secondary prevention of stroke, treatment of these other modifiable risk factors have been shown to affect mortality and second strokes of a similar magnitude and should not be neglected.
How to Treat This Case
The patient described should undergo an MRI with diffusion (to define the area of ischemia) and targeted evaluation for etiology with cardiac monitoring, echocardiogram, and carotid ultrasound.
Assuming atrial fibrillation or intracardiac thrombus is ruled out, this likely represents atherosclerotic disease. MRI will help distinguish between large-vessel atherosclerotic etiology and lacunar infarct. If carotid stenosis of greater than 70% is found in the setting of large vessel atherosclerotic stroke, then she should be referred for carotid endarterectomy. At 50% to 69% stenosis, carotid endarterectomy would still be a consideration. Antithrombotic agent of choice for non-cardioembolic CVA is an anti-platelet agent. With a stroke occurring on a reasonable dose of aspirin, I would not recommend increasing the dose as there is little evidence that 325 mg is more effective than 81mg. The most appropriate step would be to change to an alternate anti-platelet agent such as combination dipyridamole/aspirin or clopidogrel.
In the absence of a direct comparison trial, either choice is acceptable. The evidence supporting dipyridamole/aspirin is stronger for secondary stroke prevention. Atorvastatin 80 mg daily is an evidence-based therapy after acute stroke and can be started immediately. Her hypertension should be managed permissively for the first few days after the acute event, but then an ACE-I or ARB—possibly in combination with a diuretic—would be appropriate. This patient’s goal blood pressure as a diabetic would be at least less than 130/80 mm/Hg.
Finally we would be remiss if we did not stress the importance of smoking cessation, exercise, and weight loss. TH
Dr. Cumbler is an assistant professor in the Section of Hospital Medicine at the University of Colorado, where he is a member of the Acute Stroke Service and serves on the Stroke Council.
References
- Rosamond W, Flegal K, Friday G, et al. Heart disease and stroke statistics-2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007 Feb 6;115(5):e69-e171.
- Petty GW, Brown RD, Whisnant JP, et al. Ischemic stroke subtypes: a population-based study of incidence and risk factors. Stroke. 1999;30:2513-2516.
- European Atrial Fibrillation Trial Study Group. Secondary prevention in non-rheumatic atrial fibrillation after transient ischaemic attack or minor stroke. Lancet. 1993;342:1255-1262.
- Swedish Aspirin Low-Dose Trial Collaborative Group. Swedish aspirin low-dose aspirin trial (SALT) of 775 mg aspirin as secondary prophylaxis after cerebrovascular ischaemic events. Lancet. 1991;338(8779):1345-1349.
- Farrell B, Godwin J, Richards S, et al. The United Kingdom Transient Ischaemic Attack (UK-TIA) aspirin trial: final results (abstract). J Neurol Neurosurg. Psychiatry 1991;54:1044-1054.
- Dutch TIA Trial Study Group. A comparison of two doses of aspirin (30 mg versus 283 mg a day) in patients after a transient ischemic attack or minor ischemic stroke. N Engl J Med. 1991 Oct 31;325(18):1261-1266.
- Sacco RL, Adams R, Albers G, et al. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack. Stroke. 2006 Feb;37(2):577-617.
- CAPRIE Steering Committee. A randomized, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events. Lancet 1996 Jan;348:1329-1339.
- Diener H, Cunha L, Forbes C, et al. European stroke prevention study 2: dipyridamole and acetylsalicylic acid in the secondary prevention of stroke. J Neurol Sci. 1996;143:1-13.
- ESPRIT Study Group. Aspirin plus dipyridamole versus aspirin alone after cerebral ischaemia of arterial origin (ESPRIT): randomised controlled trial. Lancet. 2006;367:1665-1673.
- Mohr JP, Thompson JLP, Lazar RM, et al. A comparison of warfarin and aspirin for the prevention of recurrent ischemic stroke. N Engl J Med. 2001 Nov 15; 345(20):1444-1451.
- Chimowitz MI, Lynn MJ, Howlett-Smith H, et al. Comparison of warfarin and aspirin for symptomatic intracranial arterial stenosis. N Engl J Med. 2005 Mar 31;352(13):1305-1316.
- Diener HC, Bogousslavsky J, Brass LM, et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo controlled trial. Lancet. 2004 Jul 24-30;36499431):331-337.
- Stroke Prevention by Aggressive Reduction in Cholesterol Levels Investigators. High-dose atorvastatin after stroke or transient ischemic attack. N Engl J Med. 2006;355(6):549-559.
- The PROGRESS Collaborative Group. Randomised trial of a perindopril-based blood-pressure-lowering regimen among 6,105 individuals with previous stroke or transient ischaemic attack. Lancet 2001;358(9287):1033-1041.
- The Heart Outcomes Prevention Evaluation Study Investigators. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. N Engl J Med. 2000 Jan 20;342:145-153.
The Case
A 62-year-old obese woman with prior history of type 2 diabetes, hypertension, and a pack-a-day smoking habit presented to the emergency department (ED) for acute onset of right-side weakness and sensory loss noted on awakening from sleep.
She reports taking a baby aspirin daily to “prevent heart attacks” prior to her stroke. Her electrocardiogram demonstrates a left bundle branch block and frequent premature atrial contractions. She recovers with mild hemiparesis and is ready for discharge. What is the best medical therapy for secondary prevention of stroke?
Overview
Cerebrovascular accident (CVA) represents an important diagnosis for the hospitalist, with 700,000 people suffering a stroke in the U.S. each year.1 This translates to a stroke every 45 seconds. About 200,000 of these strokes are recurrent events.
Cardioembolism is the largest cause of ischemic strokes, representing 29% of all infarcts.2 Stasis from impaired contractile function, atrial fibrillation, or mechanical valves are significant risk factors. More rarely, a paradoxical embolus arising in the venous system may pass through a patent foramen ovale.
Large-artery atherosclerosis and lacunar infarcts each account for 16% of strokes. Risk factors for these forms of strokes are the same as those for atherosclerosis and include hypertension and diabetes. Rarer causes such as vasculitis, dissection, hypercoagulability, or hematological disorders account for 3% of strokes. Work-up for these should be driven by historical and atypical features such as young age, family history, or unusual distribution of ischemic zones. Despite appropriate work-up, the mechanism remains uncertain in 36% of strokes.
Regardless of the manifestation and residua of the index event, the hospitalist must initiate appropriate therapy to prevent a disabling CVA. While antithrombotic drugs are the mainstay of secondary prevention, it is a mistake to miss other opportunities for risk modification. Optimal management requires a tailored evaluation for etiology, identification of modifiable risk factors, and initiation of antiplatelet or anticoagulant therapy.
Cardioembolic Stroke
Treatment of stroke depends on the etiology of the original infarct. Evidence is strong that the optimal therapy for cardioembolic stroke is anticoagulation with warfarin.
The European Atrial Fibrillation Trial found that warfarin reduces the risk for second strokes in patients with atrial fibrillation by two-thirds and is superior to antiplatelet agents for preventing cardioembolic strokes.3 Warfarin increases the risk of extracranial bleeding, but not severely enough to negate the benefit of reducing stroke death and disability. The target international normalized ratio (INR) for non-valvular atrial fibrillation is generally two to three, although this may be higher for certain prosthetic valves.
Noncardioembolic Stroke
For large-vessel atherosclerotic and lacunar cerebral ischemia, the oldest—and still effective—treatment for recurrent stroke is aspirin. The use of low-dose aspirin after transient ischemic attack (TIA) or stroke reduces second strokes or death by approximately 15%-18%.4-5 Larger doses do not appear to be more effective, although the rate of gastrointestinal complaints is greater with increased dosage. The use of either 325 mg or 1,200 mg of aspirin produced the same 15% reduction in second ischemic events. Similar efficacy has been seen in comparisons between 30 mg and 283 mg dosing.6
While a subset of patients may experience aspirin resistance, reliable assays in clinical practice are not commonly available to guide management. Current recommendations suggest that use of between 50 mg and 325 mg of aspirin is appropriate for secondary prevention.7
Clopidogrel is another antiplatelet agent that can be given daily at 75 mg as alternate therapy for secondary prevention of non-cardioembolic stroke. The Clopidogrel versus Aspirin in Patients at Risk of Ischemic Events trial comparing clopidogrel with aspirin in patients at risk of ischemic events demonstrated significant reduction in the annual rate of combined endpoint of stroke, myocardial infarction, and vascular death—from 5.83% with aspirin to 5.32% with clopidogrel.8 This study’s applicability to secondary prevention of stroke is limited by the fact that only 19% of the patients in this trial were included because of prior stroke, and the results were not significant for reduction of stroke as a lone endpoint. Clopidogrel is recommended as an acceptable agent for CVA secondary prevention and is preferred for patients with stroke and an aspirin allergy or with recent coronary stent.
The combination of a low-dose aspirin and extended-release dipyridamole has proved superior to aspirin monotherapy in multiple trials. Over two years, the European Stroke Prevention 2 trial found an 18% reduction with aspirin alone compared with 37% reduction with the combination therapy, and the European/Australasian Stroke Prevention in Reversible Ischaemia trial confirmed that the combination reduced the absolute rate of second ischemic events by 1% annually.9-10 Headache is a common side effect of dipyridamole and may limit use. Dypridamole/aspirin is recommended as another acceptable option for secondary prevention of non-cardioembolic stroke.
Evidence suggests that aspirin/dipyridamole and clopidogrel—although significantly more expensive—are more effective than aspirin monotherapy for preventing second cerebral ischemic events. Direct comparison between aspirin/dipyridamole and clopidogrel is ongoing in the Prevention Regimen for Effectively Avoiding Second Stroke trial, with results anticipated in 2008.
Things That Don’t Work
The Warfarin-Aspirin Recurrent Stroke Study trial demonstrated that warfarin was not better than aspirin for prevention of non-cardioembolic stroke, and the Warfarin–Aspirin Symptomatic Intracranial Disease trial found the same result for patients with intracranial stenosis.11-12 There is little evidence that warfarin should have a role in the treatment of most non-cardioembolic strokes. The MATCH trial failed to show benefit to adding aspirin to clopidogrel over clopidogrel monotherapy for secondary preventions of non-cardioembolic cerebral ischemia.13 Despite efficacy following coronary stenting, the combination of clopidogrel and aspirin can not be recommended for stroke prevention.
What To Do
Aggressive risk factor modification is key in the prevention of second ischemic events. One of the most promising therapies is the use of statins following a CVA. Maintaining low-density lipoprotein (LDL) at less than 100 mg/dL (or less than 70 mg/dL in the highest-risk patients) is recommended despite a relatively weak association between stroke and hyperlipidemia.
This stands in contrast to the strong relationship between elevated LDL and coronary disease. However, the Stroke Prevention by Aggressive Reduction in Cholesterol Levels trial utilized high-dose atorvastatin after acute CVA and was able to create an absolute risk reduction for second stroke of 2.2% over the next five years.14 It is possible that the findings of this trial may reflect actions of statin therapy on the endothelium independent of the lipid lowering effect.
Blood pressure commonly has a transient elevation following cerebral ischemia. This is managed permissively to preserve perfusion to the ischemic penumbra. Once the hyperacute period is over, reduction of blood pressure to less than 140/90 mm/Hg (130/80 mm/Hg for diabetics) is recommended.
Interventions to treat chronic hypertension have been demonstrated to reduce the rate of strokes by approximately 30% to 40% over four to five years.15-16 An optimal agent has not been determined, but therapy with angiotensin converting enzyme inhibitor (ACE-I) or angiotensin II receptor blocker (ARB), possibly in combination with a diuretic, have been effective. Close follow-up for titration to goal in the outpatient setting should be arranged. Diabetics should have optimization of glycemic control, and lifestyle counseling should occur regarding recognized risk factors for stroke such as smoking, inactivity, and alcohol abuse.
While antithrombotic therapy is the mainstay of what we think of in secondary prevention of stroke, treatment of these other modifiable risk factors have been shown to affect mortality and second strokes of a similar magnitude and should not be neglected.
How to Treat This Case
The patient described should undergo an MRI with diffusion (to define the area of ischemia) and targeted evaluation for etiology with cardiac monitoring, echocardiogram, and carotid ultrasound.
Assuming atrial fibrillation or intracardiac thrombus is ruled out, this likely represents atherosclerotic disease. MRI will help distinguish between large-vessel atherosclerotic etiology and lacunar infarct. If carotid stenosis of greater than 70% is found in the setting of large vessel atherosclerotic stroke, then she should be referred for carotid endarterectomy. At 50% to 69% stenosis, carotid endarterectomy would still be a consideration. Antithrombotic agent of choice for non-cardioembolic CVA is an anti-platelet agent. With a stroke occurring on a reasonable dose of aspirin, I would not recommend increasing the dose as there is little evidence that 325 mg is more effective than 81mg. The most appropriate step would be to change to an alternate anti-platelet agent such as combination dipyridamole/aspirin or clopidogrel.
In the absence of a direct comparison trial, either choice is acceptable. The evidence supporting dipyridamole/aspirin is stronger for secondary stroke prevention. Atorvastatin 80 mg daily is an evidence-based therapy after acute stroke and can be started immediately. Her hypertension should be managed permissively for the first few days after the acute event, but then an ACE-I or ARB—possibly in combination with a diuretic—would be appropriate. This patient’s goal blood pressure as a diabetic would be at least less than 130/80 mm/Hg.
Finally we would be remiss if we did not stress the importance of smoking cessation, exercise, and weight loss. TH
Dr. Cumbler is an assistant professor in the Section of Hospital Medicine at the University of Colorado, where he is a member of the Acute Stroke Service and serves on the Stroke Council.
References
- Rosamond W, Flegal K, Friday G, et al. Heart disease and stroke statistics-2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007 Feb 6;115(5):e69-e171.
- Petty GW, Brown RD, Whisnant JP, et al. Ischemic stroke subtypes: a population-based study of incidence and risk factors. Stroke. 1999;30:2513-2516.
- European Atrial Fibrillation Trial Study Group. Secondary prevention in non-rheumatic atrial fibrillation after transient ischaemic attack or minor stroke. Lancet. 1993;342:1255-1262.
- Swedish Aspirin Low-Dose Trial Collaborative Group. Swedish aspirin low-dose aspirin trial (SALT) of 775 mg aspirin as secondary prophylaxis after cerebrovascular ischaemic events. Lancet. 1991;338(8779):1345-1349.
- Farrell B, Godwin J, Richards S, et al. The United Kingdom Transient Ischaemic Attack (UK-TIA) aspirin trial: final results (abstract). J Neurol Neurosurg. Psychiatry 1991;54:1044-1054.
- Dutch TIA Trial Study Group. A comparison of two doses of aspirin (30 mg versus 283 mg a day) in patients after a transient ischemic attack or minor ischemic stroke. N Engl J Med. 1991 Oct 31;325(18):1261-1266.
- Sacco RL, Adams R, Albers G, et al. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack. Stroke. 2006 Feb;37(2):577-617.
- CAPRIE Steering Committee. A randomized, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events. Lancet 1996 Jan;348:1329-1339.
- Diener H, Cunha L, Forbes C, et al. European stroke prevention study 2: dipyridamole and acetylsalicylic acid in the secondary prevention of stroke. J Neurol Sci. 1996;143:1-13.
- ESPRIT Study Group. Aspirin plus dipyridamole versus aspirin alone after cerebral ischaemia of arterial origin (ESPRIT): randomised controlled trial. Lancet. 2006;367:1665-1673.
- Mohr JP, Thompson JLP, Lazar RM, et al. A comparison of warfarin and aspirin for the prevention of recurrent ischemic stroke. N Engl J Med. 2001 Nov 15; 345(20):1444-1451.
- Chimowitz MI, Lynn MJ, Howlett-Smith H, et al. Comparison of warfarin and aspirin for symptomatic intracranial arterial stenosis. N Engl J Med. 2005 Mar 31;352(13):1305-1316.
- Diener HC, Bogousslavsky J, Brass LM, et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo controlled trial. Lancet. 2004 Jul 24-30;36499431):331-337.
- Stroke Prevention by Aggressive Reduction in Cholesterol Levels Investigators. High-dose atorvastatin after stroke or transient ischemic attack. N Engl J Med. 2006;355(6):549-559.
- The PROGRESS Collaborative Group. Randomised trial of a perindopril-based blood-pressure-lowering regimen among 6,105 individuals with previous stroke or transient ischaemic attack. Lancet 2001;358(9287):1033-1041.
- The Heart Outcomes Prevention Evaluation Study Investigators. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. N Engl J Med. 2000 Jan 20;342:145-153.
Transfer Training
When attendings at Denver Health Medical Center (DHMC) were asked to be available to help supervise the teams of residents and interns with the hand-off process, Eugene Chu, MD, director of the hospital medicine program, quickly knew there was a problem.
“They didn’t really know what they were teaching,” says Dr. Chu. “They had an idea of how to do a hand-off, but they had never explicitly learned what a good hand-off was because it had never been described before. Some of our attendings fell back on what they did best—teach medicine. But that was not necessarily what the house staff wanted at that time of day.”
The house staff did want to learn to give safe, effective, and efficient hand-offs. “Giving a lecture on renal failure was not really the point of the hand-off,” says Dr. Chu.
Time for Training
“Sign outs serve a lot of purposes, not just information [transfer],” says Leora Horwitz, MD, an assistant professor in the division of general internal medicine at Yale School of Medicine, New Haven, Conn. “Signout is also a time for training. It is a time for socialization in terms of how we talk about patients and what is expected. And it is a time for catching errors and for rethinking plans and diagnoses because as you are describing something to someone, they might pick up on gaps or inconsistencies or things that should be done differently.”
Dr. Horwitz, who is also associate medical director of the Center for Outcomes Research and Evaluation at Yale-New Haven Hospital, has researched training for transfer of care over the past three years.1
“The most important thing is that hospitalists should not assume that residents have any skills [pertaining to transfer of care],” says Dr. Horwitz. “In medical schools, students are taught over and over how to present a patient for the first time. There’s a rigid order in which the information is supposed to flow, and there is a rigid list of categories of information that should be conveyed. People are taught that same order and that same flow and that same list of categories at all med schools. Consequently, as residents, everybody has the same sense of how to represent an initial history and physical. There is no such thing for hand-offs.”
Resident duty-hour limitations have increased the number of hand-offs, which creates greater risks for discontinuity of care and patient safety.2, 3 “Hand-offs occur two or three times a day and a patient presentation only occurs once—when the patient shows up,” says Dr. Horwitz. On top of that, when residents appear in their clinical duties, the attendings tend to forget residents don’t have the skills to execute a comprehensive and well-communicated hand-off. “The first thing to remember is that people need to be trained,” she says.
In a study in the Archives of Internal Medicine in 2006 (for which Dr. Horwitz is first author), the investigators asked internal medicine chief residents whether their program provides direct training in how to perform sign outs. Sign-out training varied considerably, and fewer than half the 202 programs that responded (62% of all U.S. residency programs) provided formal sign-out skill training: 40% of the programs taught sign-out skills through a lecture or workshop, 45% supervised oral sign outs, and 38% reviewed written sign outs.4 Residents in 27% of the programs received no training or supervision. Further, in more than one-third of training programs they found hand-offs were left to interns. “Residency programs need to recognize the problem and address it in some way,” Dr. Horwitz says.
Be Explicit, Create a Model
“Many residency programs have a standardized form that residents use to sign out to the cross-covering physician,” says Sunil Kripalani, MD, MSc, director of the Section of Hospital Medicine at Vanderbilt University in Nashville, Tenn. “However, there is often not much attention given to the actual process of transferring patient information to another physician.”
For example, residents may tack the form up to a wall or leave it on a computer, he says, because this may be more convenient than meeting for a verbal, face-to-face sign out. “It is important that residents receive training about how to best sign out patients, so it is viewed as a priority area,” he says.
The initial training should cover best practices for hand-offs, says Dr. Kripalani. “It may not be intuitive, especially to new residents, that poorly executed hand-offs can be perilous,” he says.
It is also important to teach trainees how to best convey that information. “Sometimes you’ll think more is better,” says Dr. Horwitz, “but that’s not the case; people turn off or get distracted. There is a tension between providing enough information to take care of the person overnight versus providing too much information.”
Modeling best behaviors is also an important part of training, says Jay Routson, MD, a teaching hospitalist and clinical assistant professor of medicine in the Idaho State University Department of Family Medicine in Pocatello, Idaho. Dr. Routson, trained in internal medicine, thinks opportunities to train residents and students in transfer of care are also a chance to model what you expect of them.
This is particularly important in Dr. Routson’s circumstances because of the nature of his university’s family medicine residency: It is conducted at a number of locations. At morning report on the first day of a block, residents who have been on the previous rotation are to transfer patient care to the incoming residents. But they may have already left for their new pediatrics or NICU assignments, for instance, not only elsewhere in Pocatello but perhaps in Boise or Logan.
Another problem in his program’s training for transfer of care, says Dr. Routson, is that less-experienced residents are not always aware of the important things to check. What one resident thinks is important to follow up on the next resident may put at the bottom of his or her list.
“I think that you have to model the importance you place on [hand-offs],” says Dr. Routson. “You have to set aside time during the day and make it a priority. Model the behavior when you’re checking out to a new attending, make sure the residents and interns know it’s a priority, especially early in the academic year.”
Supervision and Feedback
Supervised evaluation of performance and feedback are key aspects of training for transfer of care.
“Training residents means supervising them,” says Dr. Horwitz. “Are they getting the concepts? Are they incorporating the key points into everyday communication and actions?” Having more senior and experienced doctors present during sign out or at the very least prepare people for sign out is crucial, she says, because an issue such as anticipatory guidance/contingency planning is difficult for less-experienced residents.
“As a chief resident I made a point of periodically going around and observing sign outs,” she says. “Nobody ever watches sign out because it happens at the odd hours of the day; nobody gets feedback or evaluation. Ideally an attending should, at least now and again, be involved.”
Questions to ask include:
- Do the residents meet face to face in a dedicated time and place?
- Do they fill out a standardized template and updating it appropriately, especially with regard to medications?
- Do residents measure aspects of hand-offs to ensure they are being done?
Two-Way Street
Just as the DHMC team recognized that communication for hand-offs is a two-way street, the same is true for performing a discharge communication exchange. Are primary care providers considering best practices to train themselves in this integral aspect of patient care and safety?5, 6
“I don’t think the primary care community has gotten together and come up with a consensus of what they want to know and how much interaction they want,” Dr. Horwitz says. “There should be a standard for that.”
That is a first step to encourage greater training all around. She urges collaboration between SHM and a national organization, such as the American Academy on Family Practice, and hopes SHM will open that dialogue.
In that regard, some steps have been taken.7 Dr. Kripalani is a member of the SHM Hand-off and Communication Standards Task Force, which is developing national standards (The Hospitalist, August 2007, p. 17). There is a working list of nine best practices for hand-offs at shift changes or rotation ends, and the group plans to publish a final list in the upcoming year. The list is designed primarily for practicing hospitalists but will also be suitable for residents. The task force hopes other groups, such as internal medicine program directors and chief residents, will disseminate the best practices to trainees. National best practices are also likely to affect providers in the community.
“My suspicion is that a lot of community-based programs are interested in improving hand-offs, but each program may develop a different set of procedures,” says Dr. Kripalani. “One of the main reasons for developing national standards is so that both academic and community groups can refer to a list of evidence-based best practices.”
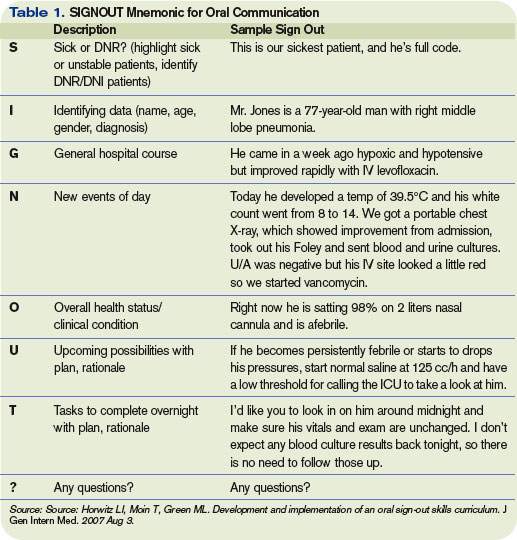
Evolution of Training
“Training for transfer of care and transfer of care are very different things, says Dr. Chu, “but they’re interrelated.” He and his colleague Gregory Misky, MD, a hospitalist and instructor with the University of Colorado Health Sciences Center (UCHSC), have been disseminating that training program throughout the UCHSC internal medicine residency program for the past three years.
In order to develop a structured, standard method for patient hand-offs, they took on teaching and supervising interns during their internal medicine ward rotations. Although much of the literature advocates the SBAR (situation, background, assessment, and recommendation) communication technique, the UCHSC team has developed a verbal structure specifically for hand-offs that differs from the SBAR model.8
Having learned many lessons their first year of training the trainers and the trainees, the Colorado hospitalists regrouped the next year. Because there were two interns coming on duty each evening, both taking cross cover, one attending could supervise only one of the interns. And, those hospitalists were getting called away to handle their clinical responsibilities.
“We felt it was important that attendings were available to guide the process safely,” says Dr. Chu. Therefore, because the evening hand-offs were conducted at 6 p.m. and a hospitalist was in house daily at that time, they began having the evening person, who was on each night until about 11, supervise the interns.
To improve the quality and consistency of the teaching, only four of the Division of Hospital Medicine’s eight attendings focused on supervising intern hand-offs. Also, in a series of focus-group meetings with attendings and house staff, they discussed supervision and identified several structures and standards for teaching hand-offs.
In addition to determining a consistent time and place for hand-off exchanges, they developed a consistent written template and a standard for verbal communication that provides an order of thinking and presenting, just as they use for presenting patient history and physical or daily patient progress updates. “The written template and the verbal are not necessarily the same thing,” says Dr. Chu. “We distinguished them as being two separate standards, just as they are with the written and verbal of morning rounds.”
With these protocols in place, attendings now had distinctions to watch for and a clear-cut means by which to supervise. In the third year of training at UCHSC, the hospitalist attendings provided training and feedback on the first night of call for the first four months beginning in July and in small-group sessions during the first week of the ward month.
The Reviews Are In
In response to a survey, the vast majority of UCHSC internal medicine residents said the new protocols were useful or extremely useful. Responses also revealed that training increased interns’ self-perceived hand-off skills and knowledge. The common denominator of a same time and place for hand-offs was judged the most useful element of the program; lectures were considered the least useful element.
Word got around of the program’s success. Eva Aagaard, MD, associate chair for education in the department of medicine, approached the originators to incorporate the program into the medical school’s interclinical curriculum, given to students between the third and fourth years as additional skills they would need in their sub-internships. Originally offered as an elective, demand for the course exceeded the class limit. Plans are under way to make this course mandatory.
“This past year, for the first time, we specifically taught our medical students hand-offs,” says Dr. Chu. He and his colleagues presented an abstract at SHM’s annual meeting in Dallas and are preparing a manuscript for publication.
Until now, all physicians have managed to do hand-offs without formal training. “Most residents figure out their own way of doing things after a while, but what we’re trying to do is not let it be a random evolution of learning,” says Dr. Chu. “It’s like learning to drive or ski with no lesson s: If you point your skis downhill, eventually you’ll learn how to ski, but you’ll have a lot of crashes. In hand-offs, that means communication failures, and a patient may suffer morbidity. We want to train and supervise [residents] so they learn in a progressive fashion and have fewer crashes.” TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Horwitz LI, Moin T, Green ML. Development and implementation of an oral sign-out skills curriculum. J Gen Intern Med. 2007 Aug 3.
- Kripalani S, LeFevre F, Phillips CO, et al. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297(8):831-841.
- Vidyarthi AR, Arora V, Schnipper JL, et al. Managing discontinuity in academic medical centers: strategies for a safe and effective resident sign-out. J Hosp Med. 2006;1(4):257-266.
- Horwitz LI, Krumholz HM, Green ML,. Transfers of patient care between house staff on internal medicine wards: a national survey. Arch Intern Med. 2006 Jun;166(11):1173-1177.
- Coleman EA, Berenson RA. Lost in transition: challenges and opportunities for improving the quality of transitional care. Ann Intern Med. 2004 Oct;141(7):533-536.
- Halasyamani L, Kripalani S, Coleman E, et al. Transition of care for hospitalized elderly patients—development of a discharge checklist for hospitalists. J Hosp Med. 2006 Nov;1(6):354-360.
- Pantilat SZ, Lindenauer PK, Katz PP, et al. Primary care physician attitudes regarding communication with hospitalists. Am J Med. 2001;111(9, Supplement 2):15-20.
- SBAR initiative to improve staff communication. Healthcare Benchmarks Qual Improv. 2005;12(4):40-41.
When attendings at Denver Health Medical Center (DHMC) were asked to be available to help supervise the teams of residents and interns with the hand-off process, Eugene Chu, MD, director of the hospital medicine program, quickly knew there was a problem.
“They didn’t really know what they were teaching,” says Dr. Chu. “They had an idea of how to do a hand-off, but they had never explicitly learned what a good hand-off was because it had never been described before. Some of our attendings fell back on what they did best—teach medicine. But that was not necessarily what the house staff wanted at that time of day.”
The house staff did want to learn to give safe, effective, and efficient hand-offs. “Giving a lecture on renal failure was not really the point of the hand-off,” says Dr. Chu.
Time for Training
“Sign outs serve a lot of purposes, not just information [transfer],” says Leora Horwitz, MD, an assistant professor in the division of general internal medicine at Yale School of Medicine, New Haven, Conn. “Signout is also a time for training. It is a time for socialization in terms of how we talk about patients and what is expected. And it is a time for catching errors and for rethinking plans and diagnoses because as you are describing something to someone, they might pick up on gaps or inconsistencies or things that should be done differently.”
Dr. Horwitz, who is also associate medical director of the Center for Outcomes Research and Evaluation at Yale-New Haven Hospital, has researched training for transfer of care over the past three years.1
“The most important thing is that hospitalists should not assume that residents have any skills [pertaining to transfer of care],” says Dr. Horwitz. “In medical schools, students are taught over and over how to present a patient for the first time. There’s a rigid order in which the information is supposed to flow, and there is a rigid list of categories of information that should be conveyed. People are taught that same order and that same flow and that same list of categories at all med schools. Consequently, as residents, everybody has the same sense of how to represent an initial history and physical. There is no such thing for hand-offs.”
Resident duty-hour limitations have increased the number of hand-offs, which creates greater risks for discontinuity of care and patient safety.2, 3 “Hand-offs occur two or three times a day and a patient presentation only occurs once—when the patient shows up,” says Dr. Horwitz. On top of that, when residents appear in their clinical duties, the attendings tend to forget residents don’t have the skills to execute a comprehensive and well-communicated hand-off. “The first thing to remember is that people need to be trained,” she says.
In a study in the Archives of Internal Medicine in 2006 (for which Dr. Horwitz is first author), the investigators asked internal medicine chief residents whether their program provides direct training in how to perform sign outs. Sign-out training varied considerably, and fewer than half the 202 programs that responded (62% of all U.S. residency programs) provided formal sign-out skill training: 40% of the programs taught sign-out skills through a lecture or workshop, 45% supervised oral sign outs, and 38% reviewed written sign outs.4 Residents in 27% of the programs received no training or supervision. Further, in more than one-third of training programs they found hand-offs were left to interns. “Residency programs need to recognize the problem and address it in some way,” Dr. Horwitz says.
Be Explicit, Create a Model
“Many residency programs have a standardized form that residents use to sign out to the cross-covering physician,” says Sunil Kripalani, MD, MSc, director of the Section of Hospital Medicine at Vanderbilt University in Nashville, Tenn. “However, there is often not much attention given to the actual process of transferring patient information to another physician.”
For example, residents may tack the form up to a wall or leave it on a computer, he says, because this may be more convenient than meeting for a verbal, face-to-face sign out. “It is important that residents receive training about how to best sign out patients, so it is viewed as a priority area,” he says.
The initial training should cover best practices for hand-offs, says Dr. Kripalani. “It may not be intuitive, especially to new residents, that poorly executed hand-offs can be perilous,” he says.
It is also important to teach trainees how to best convey that information. “Sometimes you’ll think more is better,” says Dr. Horwitz, “but that’s not the case; people turn off or get distracted. There is a tension between providing enough information to take care of the person overnight versus providing too much information.”
Modeling best behaviors is also an important part of training, says Jay Routson, MD, a teaching hospitalist and clinical assistant professor of medicine in the Idaho State University Department of Family Medicine in Pocatello, Idaho. Dr. Routson, trained in internal medicine, thinks opportunities to train residents and students in transfer of care are also a chance to model what you expect of them.
This is particularly important in Dr. Routson’s circumstances because of the nature of his university’s family medicine residency: It is conducted at a number of locations. At morning report on the first day of a block, residents who have been on the previous rotation are to transfer patient care to the incoming residents. But they may have already left for their new pediatrics or NICU assignments, for instance, not only elsewhere in Pocatello but perhaps in Boise or Logan.
Another problem in his program’s training for transfer of care, says Dr. Routson, is that less-experienced residents are not always aware of the important things to check. What one resident thinks is important to follow up on the next resident may put at the bottom of his or her list.
“I think that you have to model the importance you place on [hand-offs],” says Dr. Routson. “You have to set aside time during the day and make it a priority. Model the behavior when you’re checking out to a new attending, make sure the residents and interns know it’s a priority, especially early in the academic year.”
Supervision and Feedback
Supervised evaluation of performance and feedback are key aspects of training for transfer of care.
“Training residents means supervising them,” says Dr. Horwitz. “Are they getting the concepts? Are they incorporating the key points into everyday communication and actions?” Having more senior and experienced doctors present during sign out or at the very least prepare people for sign out is crucial, she says, because an issue such as anticipatory guidance/contingency planning is difficult for less-experienced residents.
“As a chief resident I made a point of periodically going around and observing sign outs,” she says. “Nobody ever watches sign out because it happens at the odd hours of the day; nobody gets feedback or evaluation. Ideally an attending should, at least now and again, be involved.”
Questions to ask include:
- Do the residents meet face to face in a dedicated time and place?
- Do they fill out a standardized template and updating it appropriately, especially with regard to medications?
- Do residents measure aspects of hand-offs to ensure they are being done?
Two-Way Street
Just as the DHMC team recognized that communication for hand-offs is a two-way street, the same is true for performing a discharge communication exchange. Are primary care providers considering best practices to train themselves in this integral aspect of patient care and safety?5, 6
“I don’t think the primary care community has gotten together and come up with a consensus of what they want to know and how much interaction they want,” Dr. Horwitz says. “There should be a standard for that.”
That is a first step to encourage greater training all around. She urges collaboration between SHM and a national organization, such as the American Academy on Family Practice, and hopes SHM will open that dialogue.
In that regard, some steps have been taken.7 Dr. Kripalani is a member of the SHM Hand-off and Communication Standards Task Force, which is developing national standards (The Hospitalist, August 2007, p. 17). There is a working list of nine best practices for hand-offs at shift changes or rotation ends, and the group plans to publish a final list in the upcoming year. The list is designed primarily for practicing hospitalists but will also be suitable for residents. The task force hopes other groups, such as internal medicine program directors and chief residents, will disseminate the best practices to trainees. National best practices are also likely to affect providers in the community.
“My suspicion is that a lot of community-based programs are interested in improving hand-offs, but each program may develop a different set of procedures,” says Dr. Kripalani. “One of the main reasons for developing national standards is so that both academic and community groups can refer to a list of evidence-based best practices.”
Evolution of Training
“Training for transfer of care and transfer of care are very different things, says Dr. Chu, “but they’re interrelated.” He and his colleague Gregory Misky, MD, a hospitalist and instructor with the University of Colorado Health Sciences Center (UCHSC), have been disseminating that training program throughout the UCHSC internal medicine residency program for the past three years.
In order to develop a structured, standard method for patient hand-offs, they took on teaching and supervising interns during their internal medicine ward rotations. Although much of the literature advocates the SBAR (situation, background, assessment, and recommendation) communication technique, the UCHSC team has developed a verbal structure specifically for hand-offs that differs from the SBAR model.8
Having learned many lessons their first year of training the trainers and the trainees, the Colorado hospitalists regrouped the next year. Because there were two interns coming on duty each evening, both taking cross cover, one attending could supervise only one of the interns. And, those hospitalists were getting called away to handle their clinical responsibilities.
“We felt it was important that attendings were available to guide the process safely,” says Dr. Chu. Therefore, because the evening hand-offs were conducted at 6 p.m. and a hospitalist was in house daily at that time, they began having the evening person, who was on each night until about 11, supervise the interns.
To improve the quality and consistency of the teaching, only four of the Division of Hospital Medicine’s eight attendings focused on supervising intern hand-offs. Also, in a series of focus-group meetings with attendings and house staff, they discussed supervision and identified several structures and standards for teaching hand-offs.
In addition to determining a consistent time and place for hand-off exchanges, they developed a consistent written template and a standard for verbal communication that provides an order of thinking and presenting, just as they use for presenting patient history and physical or daily patient progress updates. “The written template and the verbal are not necessarily the same thing,” says Dr. Chu. “We distinguished them as being two separate standards, just as they are with the written and verbal of morning rounds.”
With these protocols in place, attendings now had distinctions to watch for and a clear-cut means by which to supervise. In the third year of training at UCHSC, the hospitalist attendings provided training and feedback on the first night of call for the first four months beginning in July and in small-group sessions during the first week of the ward month.
The Reviews Are In
In response to a survey, the vast majority of UCHSC internal medicine residents said the new protocols were useful or extremely useful. Responses also revealed that training increased interns’ self-perceived hand-off skills and knowledge. The common denominator of a same time and place for hand-offs was judged the most useful element of the program; lectures were considered the least useful element.
Word got around of the program’s success. Eva Aagaard, MD, associate chair for education in the department of medicine, approached the originators to incorporate the program into the medical school’s interclinical curriculum, given to students between the third and fourth years as additional skills they would need in their sub-internships. Originally offered as an elective, demand for the course exceeded the class limit. Plans are under way to make this course mandatory.
“This past year, for the first time, we specifically taught our medical students hand-offs,” says Dr. Chu. He and his colleagues presented an abstract at SHM’s annual meeting in Dallas and are preparing a manuscript for publication.
Until now, all physicians have managed to do hand-offs without formal training. “Most residents figure out their own way of doing things after a while, but what we’re trying to do is not let it be a random evolution of learning,” says Dr. Chu. “It’s like learning to drive or ski with no lesson s: If you point your skis downhill, eventually you’ll learn how to ski, but you’ll have a lot of crashes. In hand-offs, that means communication failures, and a patient may suffer morbidity. We want to train and supervise [residents] so they learn in a progressive fashion and have fewer crashes.” TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Horwitz LI, Moin T, Green ML. Development and implementation of an oral sign-out skills curriculum. J Gen Intern Med. 2007 Aug 3.
- Kripalani S, LeFevre F, Phillips CO, et al. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297(8):831-841.
- Vidyarthi AR, Arora V, Schnipper JL, et al. Managing discontinuity in academic medical centers: strategies for a safe and effective resident sign-out. J Hosp Med. 2006;1(4):257-266.
- Horwitz LI, Krumholz HM, Green ML,. Transfers of patient care between house staff on internal medicine wards: a national survey. Arch Intern Med. 2006 Jun;166(11):1173-1177.
- Coleman EA, Berenson RA. Lost in transition: challenges and opportunities for improving the quality of transitional care. Ann Intern Med. 2004 Oct;141(7):533-536.
- Halasyamani L, Kripalani S, Coleman E, et al. Transition of care for hospitalized elderly patients—development of a discharge checklist for hospitalists. J Hosp Med. 2006 Nov;1(6):354-360.
- Pantilat SZ, Lindenauer PK, Katz PP, et al. Primary care physician attitudes regarding communication with hospitalists. Am J Med. 2001;111(9, Supplement 2):15-20.
- SBAR initiative to improve staff communication. Healthcare Benchmarks Qual Improv. 2005;12(4):40-41.
When attendings at Denver Health Medical Center (DHMC) were asked to be available to help supervise the teams of residents and interns with the hand-off process, Eugene Chu, MD, director of the hospital medicine program, quickly knew there was a problem.
“They didn’t really know what they were teaching,” says Dr. Chu. “They had an idea of how to do a hand-off, but they had never explicitly learned what a good hand-off was because it had never been described before. Some of our attendings fell back on what they did best—teach medicine. But that was not necessarily what the house staff wanted at that time of day.”
The house staff did want to learn to give safe, effective, and efficient hand-offs. “Giving a lecture on renal failure was not really the point of the hand-off,” says Dr. Chu.
Time for Training
“Sign outs serve a lot of purposes, not just information [transfer],” says Leora Horwitz, MD, an assistant professor in the division of general internal medicine at Yale School of Medicine, New Haven, Conn. “Signout is also a time for training. It is a time for socialization in terms of how we talk about patients and what is expected. And it is a time for catching errors and for rethinking plans and diagnoses because as you are describing something to someone, they might pick up on gaps or inconsistencies or things that should be done differently.”
Dr. Horwitz, who is also associate medical director of the Center for Outcomes Research and Evaluation at Yale-New Haven Hospital, has researched training for transfer of care over the past three years.1
“The most important thing is that hospitalists should not assume that residents have any skills [pertaining to transfer of care],” says Dr. Horwitz. “In medical schools, students are taught over and over how to present a patient for the first time. There’s a rigid order in which the information is supposed to flow, and there is a rigid list of categories of information that should be conveyed. People are taught that same order and that same flow and that same list of categories at all med schools. Consequently, as residents, everybody has the same sense of how to represent an initial history and physical. There is no such thing for hand-offs.”
Resident duty-hour limitations have increased the number of hand-offs, which creates greater risks for discontinuity of care and patient safety.2, 3 “Hand-offs occur two or three times a day and a patient presentation only occurs once—when the patient shows up,” says Dr. Horwitz. On top of that, when residents appear in their clinical duties, the attendings tend to forget residents don’t have the skills to execute a comprehensive and well-communicated hand-off. “The first thing to remember is that people need to be trained,” she says.
In a study in the Archives of Internal Medicine in 2006 (for which Dr. Horwitz is first author), the investigators asked internal medicine chief residents whether their program provides direct training in how to perform sign outs. Sign-out training varied considerably, and fewer than half the 202 programs that responded (62% of all U.S. residency programs) provided formal sign-out skill training: 40% of the programs taught sign-out skills through a lecture or workshop, 45% supervised oral sign outs, and 38% reviewed written sign outs.4 Residents in 27% of the programs received no training or supervision. Further, in more than one-third of training programs they found hand-offs were left to interns. “Residency programs need to recognize the problem and address it in some way,” Dr. Horwitz says.
Be Explicit, Create a Model
“Many residency programs have a standardized form that residents use to sign out to the cross-covering physician,” says Sunil Kripalani, MD, MSc, director of the Section of Hospital Medicine at Vanderbilt University in Nashville, Tenn. “However, there is often not much attention given to the actual process of transferring patient information to another physician.”
For example, residents may tack the form up to a wall or leave it on a computer, he says, because this may be more convenient than meeting for a verbal, face-to-face sign out. “It is important that residents receive training about how to best sign out patients, so it is viewed as a priority area,” he says.
The initial training should cover best practices for hand-offs, says Dr. Kripalani. “It may not be intuitive, especially to new residents, that poorly executed hand-offs can be perilous,” he says.
It is also important to teach trainees how to best convey that information. “Sometimes you’ll think more is better,” says Dr. Horwitz, “but that’s not the case; people turn off or get distracted. There is a tension between providing enough information to take care of the person overnight versus providing too much information.”
Modeling best behaviors is also an important part of training, says Jay Routson, MD, a teaching hospitalist and clinical assistant professor of medicine in the Idaho State University Department of Family Medicine in Pocatello, Idaho. Dr. Routson, trained in internal medicine, thinks opportunities to train residents and students in transfer of care are also a chance to model what you expect of them.
This is particularly important in Dr. Routson’s circumstances because of the nature of his university’s family medicine residency: It is conducted at a number of locations. At morning report on the first day of a block, residents who have been on the previous rotation are to transfer patient care to the incoming residents. But they may have already left for their new pediatrics or NICU assignments, for instance, not only elsewhere in Pocatello but perhaps in Boise or Logan.
Another problem in his program’s training for transfer of care, says Dr. Routson, is that less-experienced residents are not always aware of the important things to check. What one resident thinks is important to follow up on the next resident may put at the bottom of his or her list.
“I think that you have to model the importance you place on [hand-offs],” says Dr. Routson. “You have to set aside time during the day and make it a priority. Model the behavior when you’re checking out to a new attending, make sure the residents and interns know it’s a priority, especially early in the academic year.”
Supervision and Feedback
Supervised evaluation of performance and feedback are key aspects of training for transfer of care.
“Training residents means supervising them,” says Dr. Horwitz. “Are they getting the concepts? Are they incorporating the key points into everyday communication and actions?” Having more senior and experienced doctors present during sign out or at the very least prepare people for sign out is crucial, she says, because an issue such as anticipatory guidance/contingency planning is difficult for less-experienced residents.
“As a chief resident I made a point of periodically going around and observing sign outs,” she says. “Nobody ever watches sign out because it happens at the odd hours of the day; nobody gets feedback or evaluation. Ideally an attending should, at least now and again, be involved.”
Questions to ask include:
- Do the residents meet face to face in a dedicated time and place?
- Do they fill out a standardized template and updating it appropriately, especially with regard to medications?
- Do residents measure aspects of hand-offs to ensure they are being done?
Two-Way Street
Just as the DHMC team recognized that communication for hand-offs is a two-way street, the same is true for performing a discharge communication exchange. Are primary care providers considering best practices to train themselves in this integral aspect of patient care and safety?5, 6
“I don’t think the primary care community has gotten together and come up with a consensus of what they want to know and how much interaction they want,” Dr. Horwitz says. “There should be a standard for that.”
That is a first step to encourage greater training all around. She urges collaboration between SHM and a national organization, such as the American Academy on Family Practice, and hopes SHM will open that dialogue.
In that regard, some steps have been taken.7 Dr. Kripalani is a member of the SHM Hand-off and Communication Standards Task Force, which is developing national standards (The Hospitalist, August 2007, p. 17). There is a working list of nine best practices for hand-offs at shift changes or rotation ends, and the group plans to publish a final list in the upcoming year. The list is designed primarily for practicing hospitalists but will also be suitable for residents. The task force hopes other groups, such as internal medicine program directors and chief residents, will disseminate the best practices to trainees. National best practices are also likely to affect providers in the community.
“My suspicion is that a lot of community-based programs are interested in improving hand-offs, but each program may develop a different set of procedures,” says Dr. Kripalani. “One of the main reasons for developing national standards is so that both academic and community groups can refer to a list of evidence-based best practices.”
Evolution of Training
“Training for transfer of care and transfer of care are very different things, says Dr. Chu, “but they’re interrelated.” He and his colleague Gregory Misky, MD, a hospitalist and instructor with the University of Colorado Health Sciences Center (UCHSC), have been disseminating that training program throughout the UCHSC internal medicine residency program for the past three years.
In order to develop a structured, standard method for patient hand-offs, they took on teaching and supervising interns during their internal medicine ward rotations. Although much of the literature advocates the SBAR (situation, background, assessment, and recommendation) communication technique, the UCHSC team has developed a verbal structure specifically for hand-offs that differs from the SBAR model.8
Having learned many lessons their first year of training the trainers and the trainees, the Colorado hospitalists regrouped the next year. Because there were two interns coming on duty each evening, both taking cross cover, one attending could supervise only one of the interns. And, those hospitalists were getting called away to handle their clinical responsibilities.
“We felt it was important that attendings were available to guide the process safely,” says Dr. Chu. Therefore, because the evening hand-offs were conducted at 6 p.m. and a hospitalist was in house daily at that time, they began having the evening person, who was on each night until about 11, supervise the interns.
To improve the quality and consistency of the teaching, only four of the Division of Hospital Medicine’s eight attendings focused on supervising intern hand-offs. Also, in a series of focus-group meetings with attendings and house staff, they discussed supervision and identified several structures and standards for teaching hand-offs.
In addition to determining a consistent time and place for hand-off exchanges, they developed a consistent written template and a standard for verbal communication that provides an order of thinking and presenting, just as they use for presenting patient history and physical or daily patient progress updates. “The written template and the verbal are not necessarily the same thing,” says Dr. Chu. “We distinguished them as being two separate standards, just as they are with the written and verbal of morning rounds.”
With these protocols in place, attendings now had distinctions to watch for and a clear-cut means by which to supervise. In the third year of training at UCHSC, the hospitalist attendings provided training and feedback on the first night of call for the first four months beginning in July and in small-group sessions during the first week of the ward month.
The Reviews Are In
In response to a survey, the vast majority of UCHSC internal medicine residents said the new protocols were useful or extremely useful. Responses also revealed that training increased interns’ self-perceived hand-off skills and knowledge. The common denominator of a same time and place for hand-offs was judged the most useful element of the program; lectures were considered the least useful element.
Word got around of the program’s success. Eva Aagaard, MD, associate chair for education in the department of medicine, approached the originators to incorporate the program into the medical school’s interclinical curriculum, given to students between the third and fourth years as additional skills they would need in their sub-internships. Originally offered as an elective, demand for the course exceeded the class limit. Plans are under way to make this course mandatory.
“This past year, for the first time, we specifically taught our medical students hand-offs,” says Dr. Chu. He and his colleagues presented an abstract at SHM’s annual meeting in Dallas and are preparing a manuscript for publication.
Until now, all physicians have managed to do hand-offs without formal training. “Most residents figure out their own way of doing things after a while, but what we’re trying to do is not let it be a random evolution of learning,” says Dr. Chu. “It’s like learning to drive or ski with no lesson s: If you point your skis downhill, eventually you’ll learn how to ski, but you’ll have a lot of crashes. In hand-offs, that means communication failures, and a patient may suffer morbidity. We want to train and supervise [residents] so they learn in a progressive fashion and have fewer crashes.” TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Horwitz LI, Moin T, Green ML. Development and implementation of an oral sign-out skills curriculum. J Gen Intern Med. 2007 Aug 3.
- Kripalani S, LeFevre F, Phillips CO, et al. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297(8):831-841.
- Vidyarthi AR, Arora V, Schnipper JL, et al. Managing discontinuity in academic medical centers: strategies for a safe and effective resident sign-out. J Hosp Med. 2006;1(4):257-266.
- Horwitz LI, Krumholz HM, Green ML,. Transfers of patient care between house staff on internal medicine wards: a national survey. Arch Intern Med. 2006 Jun;166(11):1173-1177.
- Coleman EA, Berenson RA. Lost in transition: challenges and opportunities for improving the quality of transitional care. Ann Intern Med. 2004 Oct;141(7):533-536.
- Halasyamani L, Kripalani S, Coleman E, et al. Transition of care for hospitalized elderly patients—development of a discharge checklist for hospitalists. J Hosp Med. 2006 Nov;1(6):354-360.
- Pantilat SZ, Lindenauer PK, Katz PP, et al. Primary care physician attitudes regarding communication with hospitalists. Am J Med. 2001;111(9, Supplement 2):15-20.
- SBAR initiative to improve staff communication. Healthcare Benchmarks Qual Improv. 2005;12(4):40-41.
Fly Solo
Lone hospitalist. It sounds adventurous. It might mean having the chance to set the stage for a hospital medicine program—working exactly the way one wants to and enjoying the feeling of indispensability.
But it’s not for the faint of heart, as those who’d done it attest. There’s the potential for having no starting patient base, or being overwhelmed because there are few to no physicians to share coverage. Having the chance to educate the hospital and its staff about hospital medicine can be a blessing—and a curse.
An example of a lone hospitalist who has experienced the joys and pains of her position is Patricia M. Hopkins-Braddock, MD, an assistant professor of pediatrics at Albany Medical College in N.Y. She was hired as the only pediatric hospitalist in the pediatrics intensive care unit (PICU) at Albany Medical Center. This is her fourth year in that position. Having become the residency program director at her institution in January, she works every day plus one weekend a month, alternating weekly between a pediatrics floor and a long-term care facility and sedation service for children.
“I like the fact that I have turned into the go-to person for problems within the hospital continuum,” Dr. Hopkins-Braddock says. “I also have to say that that is probably one of the things I like least. I have that presence in the hospital and the understanding of the way the floor works. I also do pediatrics sedation. Somehow I become the solution for every problem. It’s good in its own sense, but it can also become very overwhelming.”
A Perfect World?
“If we could figure out a way for one person to function productively and efficiently by themselves, it would be wonderful,” says Cary Ward, MD, who works with hospitalist programs that are part of Catholic Health Initiatives, based in Denver, and is the chief medical officer at St. Elizabeth Regional Medicine Center in Lincoln, Neb. “There is a large group of hospitals that wants to have a hospitalist program, and those are the critical access hospitals.” At these hospitals, which never have more than 25 patients, several community physicians round at the hospital in the morning, finishing by 7 or 7:30 a.m., and return to their primary office bases. “These hospitals are often clamoring for someone to be in the hospital the majority of the day,” he says.
“You’ve heard the saying, ‘You’ve seen one hospitalist program, you’ve seen one hospitalist program,’ ” continues Dr. Ward. “I’ve been amazed at all the hybrid programs out there. At most small hospitalist groups, even those programs under the smallest census of 12 or 13 patients, hospitals still often bring in two doctors with alternate week rotations. “Many consider this the most feasible way to try to cover one hospital census at all times; however, some worry that this ‘feast or famine’ schedule may lead to burnout and this can be expensive for the hospital. To get only one physician to cover that kind of responsibility is a real challenge.”
And yet, some hospitals and hospitalists manage to do it. Of the 362 hospitalist groups that responded to SHM’s 2005-2006 survey “Bi-Annual Survey on the State of the Hospital Medicine Movement,” only nine groups (2.5%) consisted of one physician. Joseph A. Miller, MD, who staffs SHM’s Benchmarks Task Force and has been helping SHM build a national hospitalist database, estimates that of the 2,500 hospitalist groups in the U.S., 62 groups might have just one hospitalist.
Pluses and Minuses
Martin C. Johns, MD, a rural internal medicine and pediatrics hospitalist at Gifford Medical Center in Randolph, Vt., sees some definite advantages to being a lone hospitalist, a post he has held for the 1 1/2 years. “It allowed me the time to interact with all the other modalities and to establish with physician therapy, occupational therapy, care management, pharmacy, what was lacking in the previous model with a variety of docs covering,” Dr. Johns says. “I was trying to create standards that made sense for everyone. The establishment of my being the only hospitalist was determinant primarily on my ability to create those relationships and ensure that they were solid, and also to have the support of all the primary care doctors.”
Gifford’s administration was also supportive. “Because we are a critical access hospital, there are certain restrictions and requirements that we have to take into consideration with Medicare and Medicaid,” Dr. Johns says. “Being the sole hospitalist as we’re expanding allowed me to set the stage: what was lacking, what was missing, what we could improve on, what was already working quite well. [I incorporated] the help of the administration to fill in the gaps of what we needed.”
The primary nonclinical challenge for the lone hospitalist is finding patients to care for and doctors to share coverage. Christopher Farrar, MD, lead hospitalist at Anderson Hospital in Maryville, Ill., began the program there. His employer, the hospitalist company Inpatient Management Inc., based in St. Louis, Mo., manages 18 hospitalist programs in 12 states. “As I was ending my primary care role,” says Dr. Farrar, “this opportunity came available. I think that they weren’t expecting someone to jump in so quickly. They didn’t have the luxury of time to find another physician right away.”
There are now two physicians in the program there, and they are on the verge of getting a third. Dr. Farrar said he doesn’t think there are a lot of pluses to being the lone hospitalist. The most difficult part is avoiding burnout, he warns. Although there were plenty of patients and work for him when he first started at his institution, he wasn’t overwhelmed. But he was relieved when the company brought in a second physician with whom to share call. “I could have easily become overwhelmed quickly had it gone down that road,” he says.
Finding a patient base and physician call backup were not issues for J. Stewart Fulton, DO, medical director of the hospitalist program at Southern New Hampshire Medical Center in Nashua, when he began five years ago as the lone hospitalist. Foundation Medical Partners, a multispecialty group of 27 doctors directly affiliated with the hospital, recruited Dr. Fulton to start a hospitalist program. “I walked into an ideal situation,” he says. “I stepped into a group that had a patient base, that knew they needed hospital coverage, and were willing to support me as I grew to provide 24/7 coverage for myself.”

Culture Shock
In July 1998, Joseph Li, MD, director of the hospital medicine program at Beth Israel Deaconess Medical Center, Boston, was the chief medical resident at that institution when his chief of medicine approached him about starting a hospitalist program.
In the late 1990s there was no model of that kind in Boston. “He hired me as our first full-time hospitalist, and I was referred to as a hospitalist—but nobody really understood what that meant,” says Dr. Li. “Looking back now, I didn’t even really understand what that meant.”
Tin M. Oo, MD, medical director for the hospitalist program at St. Mary’s Health Center in Jefferson City, Mo., practiced for seven months as a lone hospitalist but was hardly a new physician. He has been practicing medicine for 34 years in the U.S. and four other countries: Burma (now Myanmar, his native country), Sri Lanka, Malaysia, and Brunei Darussalam. Since he emigrated to the U.S. 15 years ago, he has served as an epidemiologist with the state Department of Health in Minnesota, matriculated into a three-year internal medicine residency program in New York and practiced there, and was in private practice in Chattanooga, Tenn.
When Dr. Oo first came to St. Mary’s, he taught his co-workers, the patients, and their families. “The hospital [and nurses] didn’t have any experience with hospitalists so they didn’t know when to call me and when not to call me,” he says. Dr. Oo got his first hospitalist experience in Chattanooga, Tenn., when he worked with outpatients and some inpatients. His prior experience moonlighting as a hospitalist as well as an emergency physician has helped him greatly as a lone hospitalist. “It was a good thing that I wasn’t just a hospitalist; that I had been in private practice and worked in the ER and as a hospitalist. I knew what the private doctors were facing, and what was coming across from the ER.”
For those who have not yet practiced medicine, Dr. Oo would dissuade them from taking a position as a lone hospitalist. “You have to have a feel for what the ER physicians or what the family practice/ internists, and what the specialists do,” he says. “You also have to be in the hospitalist’s shoes, at least from time to time.”

Be Flexible
While all hospitalists need to be flexible, this may be particularly true for the lone hospitalist. Dr. Johns finds his dual internal medicine/pediatrics training serves him well. “I assist with patients, especially pediatrics, in the emergency department [ED], go up to [resuscitate the infant in] C sections, deal with all the pediatric issues and ER consultations during the day plus do all the general internal medicine care and adult care, which does make up the majority of what I do during the day,” he says. Two physician assistants have been brought on board to improve continuity on nights and weekends and decrease the workload of all physician providers.
Dr. Johns, whose title is associate medical director in charge of hospitalist services, finds the biggest challenge has been attaining and maintaining a commitment to quality on opposite shifts. Sharing coverage with several primary care physicians, he says, means there are differences in concepts of protocols for admissions, commitment to caring for the extra patients, and the physician’s comfort in his or her inpatient knowledge base.
Taking over after a previous night’s coverage, Dr. Johns is unsure which orders were carried out and which patients received what therapy, for instance. “The covering providers take care and make sure patients make it through to next day but often hesitate to alter the plan too much because they are not covering the following day as the inpatient provider.” A newly instated Thursday-through-Monday hospitalist service schedule has helped improve continuity of care and transfer of information through the weekend. But it is still not a perfect situation.
After 15 months as the lone hospitalist, Dr. Johns’ position has changed. He cares for patients during the day and during the opposite shift takes on administrative responsibilities, such as deciding on protocols and expanding services. That kind of juggling—without hospitalist colleagues—has required flexibility as well.

Plan and Set Boundaries
Educating the hospital taught Dr. Fulton a good deal as well, especially about his and their expectations. “The group that grasps the whole concept the quickest is the ancillary services (case management) and the nursing staff,” he says. He likens their receptivity to having a hospitalist to the workings of a pendulum: “There is nothing before this better way, and then they want more of it and they want it all the time. It really means needing to create boundaries”
Dr. Oo agrees that as a lone hospitalist it is important to set boundaries for your accountabilities. The administration of his hospital asked him whether he would take charge of rapid response calls. He declined, leaving that traditional role to the ED.
The year Dr. Fulton practiced as a lone hospitalist gave him a window of time to plan. “It really allowed me to hit the bumps in the road and figure things out so when I added partners, I was able to get them up to speed more quickly,” he says. “Hospitals continue to get busier and busier and that requires planning. I was tracking and trending the volume [of patients that] these 27 doctors were generating in the hospital so that I could anticipate how many doctors I needed. Hospitals continue to increase in volume. The intensity of medicine continues to increase. You always need to plan for one or two more docs than you think you need.”

Coverage
For many lone hospitalists, sharing schedule coverage is a dilemma. Dr. Li, an assistant professor of medicine at Harvard Medical School in Boston and a board member of SHM, spent one year as a lone hospitalist before another full-timer joined him. “Everybody understands that as sole physician you really can’t be expected to see patients 24/7/365,” says Dr. Li.
Dr. Li’s recommendation for any hospitalist group of any size—but particularly early on when the hospitalist is alone or in a small group—is to match volume with staffing. “With every program that I have seen or been involved with, early on there is always a massive shift of primary care providers who want to refer patients to you after the program is up and running, Dr. Li says.
Another recommendation Dr. Li has for the lone hospitalist is to identify how you will quickly get help in urgent circumstances. “There is a real benefit to the whole service for having more than one physician on any given day,” he says. It takes only one critically ill patient to cause an upheaval in the schedule.
Committee Work
As recent SHM data show, a large proportion of hospitalists serve on hospital committees. But during his year as a lone hospitalist, Dr. Li focused on taking care of patients, relying upon consultants, and getting through the day.
“I certainly had very little insight at that point of the hospitalist model in terms of communications and leading a team and being the leader of quality in the institution,” he says. “Those were the furthest things from my mind.”
Dr. Fulton participated on committees even though he was a lone hospitalist. “I was involved because I was willing to do the extra work and to use that opportunity to educate and establish who we were in the hospital,” he says. When he was joined by his first two partners, he protected them from committee work because that wasn’t their initial responsibility,” he says.
For lone hospitalists, “you either need to anticipate being on committees and protecting time for it, or you need to anticipate protecting yourself from the committees in order to provide your service,” says Dr. Fulton. “That’s sort of a slippery slope because if you lose the opportunity to become involved in committees, someone else will do it and then they’re making decisions for you that affect your practice of medicine in the hospital.”
Because Dr. Fulton would not sit in hourlong meetings, he took an indirect route—discussing issues with case managers on the floors in between patients or when they shared a patient.
Dr. Fulton advises the lone hospitalist to consider “who is boss” when he or she considers allocating time for committee involvement. Employment by a hospital versus a multispecialty group versus going out as a solo practitioner or working in a private group will determine whose agenda you have to fulfill. “If you are owned by the hospital, the hospital calls the shots; and you have to negotiate … where you put your efforts and your service. If they want you to be on committees, you need to negotiate less patient interaction. You can’t do both; you’ll begin to lose your mind.” TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
Lone hospitalist. It sounds adventurous. It might mean having the chance to set the stage for a hospital medicine program—working exactly the way one wants to and enjoying the feeling of indispensability.
But it’s not for the faint of heart, as those who’d done it attest. There’s the potential for having no starting patient base, or being overwhelmed because there are few to no physicians to share coverage. Having the chance to educate the hospital and its staff about hospital medicine can be a blessing—and a curse.
An example of a lone hospitalist who has experienced the joys and pains of her position is Patricia M. Hopkins-Braddock, MD, an assistant professor of pediatrics at Albany Medical College in N.Y. She was hired as the only pediatric hospitalist in the pediatrics intensive care unit (PICU) at Albany Medical Center. This is her fourth year in that position. Having become the residency program director at her institution in January, she works every day plus one weekend a month, alternating weekly between a pediatrics floor and a long-term care facility and sedation service for children.
“I like the fact that I have turned into the go-to person for problems within the hospital continuum,” Dr. Hopkins-Braddock says. “I also have to say that that is probably one of the things I like least. I have that presence in the hospital and the understanding of the way the floor works. I also do pediatrics sedation. Somehow I become the solution for every problem. It’s good in its own sense, but it can also become very overwhelming.”
A Perfect World?
“If we could figure out a way for one person to function productively and efficiently by themselves, it would be wonderful,” says Cary Ward, MD, who works with hospitalist programs that are part of Catholic Health Initiatives, based in Denver, and is the chief medical officer at St. Elizabeth Regional Medicine Center in Lincoln, Neb. “There is a large group of hospitals that wants to have a hospitalist program, and those are the critical access hospitals.” At these hospitals, which never have more than 25 patients, several community physicians round at the hospital in the morning, finishing by 7 or 7:30 a.m., and return to their primary office bases. “These hospitals are often clamoring for someone to be in the hospital the majority of the day,” he says.
“You’ve heard the saying, ‘You’ve seen one hospitalist program, you’ve seen one hospitalist program,’ ” continues Dr. Ward. “I’ve been amazed at all the hybrid programs out there. At most small hospitalist groups, even those programs under the smallest census of 12 or 13 patients, hospitals still often bring in two doctors with alternate week rotations. “Many consider this the most feasible way to try to cover one hospital census at all times; however, some worry that this ‘feast or famine’ schedule may lead to burnout and this can be expensive for the hospital. To get only one physician to cover that kind of responsibility is a real challenge.”
And yet, some hospitals and hospitalists manage to do it. Of the 362 hospitalist groups that responded to SHM’s 2005-2006 survey “Bi-Annual Survey on the State of the Hospital Medicine Movement,” only nine groups (2.5%) consisted of one physician. Joseph A. Miller, MD, who staffs SHM’s Benchmarks Task Force and has been helping SHM build a national hospitalist database, estimates that of the 2,500 hospitalist groups in the U.S., 62 groups might have just one hospitalist.
Pluses and Minuses
Martin C. Johns, MD, a rural internal medicine and pediatrics hospitalist at Gifford Medical Center in Randolph, Vt., sees some definite advantages to being a lone hospitalist, a post he has held for the 1 1/2 years. “It allowed me the time to interact with all the other modalities and to establish with physician therapy, occupational therapy, care management, pharmacy, what was lacking in the previous model with a variety of docs covering,” Dr. Johns says. “I was trying to create standards that made sense for everyone. The establishment of my being the only hospitalist was determinant primarily on my ability to create those relationships and ensure that they were solid, and also to have the support of all the primary care doctors.”
Gifford’s administration was also supportive. “Because we are a critical access hospital, there are certain restrictions and requirements that we have to take into consideration with Medicare and Medicaid,” Dr. Johns says. “Being the sole hospitalist as we’re expanding allowed me to set the stage: what was lacking, what was missing, what we could improve on, what was already working quite well. [I incorporated] the help of the administration to fill in the gaps of what we needed.”
The primary nonclinical challenge for the lone hospitalist is finding patients to care for and doctors to share coverage. Christopher Farrar, MD, lead hospitalist at Anderson Hospital in Maryville, Ill., began the program there. His employer, the hospitalist company Inpatient Management Inc., based in St. Louis, Mo., manages 18 hospitalist programs in 12 states. “As I was ending my primary care role,” says Dr. Farrar, “this opportunity came available. I think that they weren’t expecting someone to jump in so quickly. They didn’t have the luxury of time to find another physician right away.”
There are now two physicians in the program there, and they are on the verge of getting a third. Dr. Farrar said he doesn’t think there are a lot of pluses to being the lone hospitalist. The most difficult part is avoiding burnout, he warns. Although there were plenty of patients and work for him when he first started at his institution, he wasn’t overwhelmed. But he was relieved when the company brought in a second physician with whom to share call. “I could have easily become overwhelmed quickly had it gone down that road,” he says.
Finding a patient base and physician call backup were not issues for J. Stewart Fulton, DO, medical director of the hospitalist program at Southern New Hampshire Medical Center in Nashua, when he began five years ago as the lone hospitalist. Foundation Medical Partners, a multispecialty group of 27 doctors directly affiliated with the hospital, recruited Dr. Fulton to start a hospitalist program. “I walked into an ideal situation,” he says. “I stepped into a group that had a patient base, that knew they needed hospital coverage, and were willing to support me as I grew to provide 24/7 coverage for myself.”
Culture Shock
In July 1998, Joseph Li, MD, director of the hospital medicine program at Beth Israel Deaconess Medical Center, Boston, was the chief medical resident at that institution when his chief of medicine approached him about starting a hospitalist program.
In the late 1990s there was no model of that kind in Boston. “He hired me as our first full-time hospitalist, and I was referred to as a hospitalist—but nobody really understood what that meant,” says Dr. Li. “Looking back now, I didn’t even really understand what that meant.”
Tin M. Oo, MD, medical director for the hospitalist program at St. Mary’s Health Center in Jefferson City, Mo., practiced for seven months as a lone hospitalist but was hardly a new physician. He has been practicing medicine for 34 years in the U.S. and four other countries: Burma (now Myanmar, his native country), Sri Lanka, Malaysia, and Brunei Darussalam. Since he emigrated to the U.S. 15 years ago, he has served as an epidemiologist with the state Department of Health in Minnesota, matriculated into a three-year internal medicine residency program in New York and practiced there, and was in private practice in Chattanooga, Tenn.
When Dr. Oo first came to St. Mary’s, he taught his co-workers, the patients, and their families. “The hospital [and nurses] didn’t have any experience with hospitalists so they didn’t know when to call me and when not to call me,” he says. Dr. Oo got his first hospitalist experience in Chattanooga, Tenn., when he worked with outpatients and some inpatients. His prior experience moonlighting as a hospitalist as well as an emergency physician has helped him greatly as a lone hospitalist. “It was a good thing that I wasn’t just a hospitalist; that I had been in private practice and worked in the ER and as a hospitalist. I knew what the private doctors were facing, and what was coming across from the ER.”
For those who have not yet practiced medicine, Dr. Oo would dissuade them from taking a position as a lone hospitalist. “You have to have a feel for what the ER physicians or what the family practice/ internists, and what the specialists do,” he says. “You also have to be in the hospitalist’s shoes, at least from time to time.”
Be Flexible
While all hospitalists need to be flexible, this may be particularly true for the lone hospitalist. Dr. Johns finds his dual internal medicine/pediatrics training serves him well. “I assist with patients, especially pediatrics, in the emergency department [ED], go up to [resuscitate the infant in] C sections, deal with all the pediatric issues and ER consultations during the day plus do all the general internal medicine care and adult care, which does make up the majority of what I do during the day,” he says. Two physician assistants have been brought on board to improve continuity on nights and weekends and decrease the workload of all physician providers.
Dr. Johns, whose title is associate medical director in charge of hospitalist services, finds the biggest challenge has been attaining and maintaining a commitment to quality on opposite shifts. Sharing coverage with several primary care physicians, he says, means there are differences in concepts of protocols for admissions, commitment to caring for the extra patients, and the physician’s comfort in his or her inpatient knowledge base.
Taking over after a previous night’s coverage, Dr. Johns is unsure which orders were carried out and which patients received what therapy, for instance. “The covering providers take care and make sure patients make it through to next day but often hesitate to alter the plan too much because they are not covering the following day as the inpatient provider.” A newly instated Thursday-through-Monday hospitalist service schedule has helped improve continuity of care and transfer of information through the weekend. But it is still not a perfect situation.
After 15 months as the lone hospitalist, Dr. Johns’ position has changed. He cares for patients during the day and during the opposite shift takes on administrative responsibilities, such as deciding on protocols and expanding services. That kind of juggling—without hospitalist colleagues—has required flexibility as well.
Plan and Set Boundaries
Educating the hospital taught Dr. Fulton a good deal as well, especially about his and their expectations. “The group that grasps the whole concept the quickest is the ancillary services (case management) and the nursing staff,” he says. He likens their receptivity to having a hospitalist to the workings of a pendulum: “There is nothing before this better way, and then they want more of it and they want it all the time. It really means needing to create boundaries”
Dr. Oo agrees that as a lone hospitalist it is important to set boundaries for your accountabilities. The administration of his hospital asked him whether he would take charge of rapid response calls. He declined, leaving that traditional role to the ED.
The year Dr. Fulton practiced as a lone hospitalist gave him a window of time to plan. “It really allowed me to hit the bumps in the road and figure things out so when I added partners, I was able to get them up to speed more quickly,” he says. “Hospitals continue to get busier and busier and that requires planning. I was tracking and trending the volume [of patients that] these 27 doctors were generating in the hospital so that I could anticipate how many doctors I needed. Hospitals continue to increase in volume. The intensity of medicine continues to increase. You always need to plan for one or two more docs than you think you need.”
Coverage
For many lone hospitalists, sharing schedule coverage is a dilemma. Dr. Li, an assistant professor of medicine at Harvard Medical School in Boston and a board member of SHM, spent one year as a lone hospitalist before another full-timer joined him. “Everybody understands that as sole physician you really can’t be expected to see patients 24/7/365,” says Dr. Li.
Dr. Li’s recommendation for any hospitalist group of any size—but particularly early on when the hospitalist is alone or in a small group—is to match volume with staffing. “With every program that I have seen or been involved with, early on there is always a massive shift of primary care providers who want to refer patients to you after the program is up and running, Dr. Li says.
Another recommendation Dr. Li has for the lone hospitalist is to identify how you will quickly get help in urgent circumstances. “There is a real benefit to the whole service for having more than one physician on any given day,” he says. It takes only one critically ill patient to cause an upheaval in the schedule.
Committee Work
As recent SHM data show, a large proportion of hospitalists serve on hospital committees. But during his year as a lone hospitalist, Dr. Li focused on taking care of patients, relying upon consultants, and getting through the day.
“I certainly had very little insight at that point of the hospitalist model in terms of communications and leading a team and being the leader of quality in the institution,” he says. “Those were the furthest things from my mind.”
Dr. Fulton participated on committees even though he was a lone hospitalist. “I was involved because I was willing to do the extra work and to use that opportunity to educate and establish who we were in the hospital,” he says. When he was joined by his first two partners, he protected them from committee work because that wasn’t their initial responsibility,” he says.
For lone hospitalists, “you either need to anticipate being on committees and protecting time for it, or you need to anticipate protecting yourself from the committees in order to provide your service,” says Dr. Fulton. “That’s sort of a slippery slope because if you lose the opportunity to become involved in committees, someone else will do it and then they’re making decisions for you that affect your practice of medicine in the hospital.”
Because Dr. Fulton would not sit in hourlong meetings, he took an indirect route—discussing issues with case managers on the floors in between patients or when they shared a patient.
Dr. Fulton advises the lone hospitalist to consider “who is boss” when he or she considers allocating time for committee involvement. Employment by a hospital versus a multispecialty group versus going out as a solo practitioner or working in a private group will determine whose agenda you have to fulfill. “If you are owned by the hospital, the hospital calls the shots; and you have to negotiate … where you put your efforts and your service. If they want you to be on committees, you need to negotiate less patient interaction. You can’t do both; you’ll begin to lose your mind.” TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
Lone hospitalist. It sounds adventurous. It might mean having the chance to set the stage for a hospital medicine program—working exactly the way one wants to and enjoying the feeling of indispensability.
But it’s not for the faint of heart, as those who’d done it attest. There’s the potential for having no starting patient base, or being overwhelmed because there are few to no physicians to share coverage. Having the chance to educate the hospital and its staff about hospital medicine can be a blessing—and a curse.
An example of a lone hospitalist who has experienced the joys and pains of her position is Patricia M. Hopkins-Braddock, MD, an assistant professor of pediatrics at Albany Medical College in N.Y. She was hired as the only pediatric hospitalist in the pediatrics intensive care unit (PICU) at Albany Medical Center. This is her fourth year in that position. Having become the residency program director at her institution in January, she works every day plus one weekend a month, alternating weekly between a pediatrics floor and a long-term care facility and sedation service for children.
“I like the fact that I have turned into the go-to person for problems within the hospital continuum,” Dr. Hopkins-Braddock says. “I also have to say that that is probably one of the things I like least. I have that presence in the hospital and the understanding of the way the floor works. I also do pediatrics sedation. Somehow I become the solution for every problem. It’s good in its own sense, but it can also become very overwhelming.”
A Perfect World?
“If we could figure out a way for one person to function productively and efficiently by themselves, it would be wonderful,” says Cary Ward, MD, who works with hospitalist programs that are part of Catholic Health Initiatives, based in Denver, and is the chief medical officer at St. Elizabeth Regional Medicine Center in Lincoln, Neb. “There is a large group of hospitals that wants to have a hospitalist program, and those are the critical access hospitals.” At these hospitals, which never have more than 25 patients, several community physicians round at the hospital in the morning, finishing by 7 or 7:30 a.m., and return to their primary office bases. “These hospitals are often clamoring for someone to be in the hospital the majority of the day,” he says.
“You’ve heard the saying, ‘You’ve seen one hospitalist program, you’ve seen one hospitalist program,’ ” continues Dr. Ward. “I’ve been amazed at all the hybrid programs out there. At most small hospitalist groups, even those programs under the smallest census of 12 or 13 patients, hospitals still often bring in two doctors with alternate week rotations. “Many consider this the most feasible way to try to cover one hospital census at all times; however, some worry that this ‘feast or famine’ schedule may lead to burnout and this can be expensive for the hospital. To get only one physician to cover that kind of responsibility is a real challenge.”
And yet, some hospitals and hospitalists manage to do it. Of the 362 hospitalist groups that responded to SHM’s 2005-2006 survey “Bi-Annual Survey on the State of the Hospital Medicine Movement,” only nine groups (2.5%) consisted of one physician. Joseph A. Miller, MD, who staffs SHM’s Benchmarks Task Force and has been helping SHM build a national hospitalist database, estimates that of the 2,500 hospitalist groups in the U.S., 62 groups might have just one hospitalist.
Pluses and Minuses
Martin C. Johns, MD, a rural internal medicine and pediatrics hospitalist at Gifford Medical Center in Randolph, Vt., sees some definite advantages to being a lone hospitalist, a post he has held for the 1 1/2 years. “It allowed me the time to interact with all the other modalities and to establish with physician therapy, occupational therapy, care management, pharmacy, what was lacking in the previous model with a variety of docs covering,” Dr. Johns says. “I was trying to create standards that made sense for everyone. The establishment of my being the only hospitalist was determinant primarily on my ability to create those relationships and ensure that they were solid, and also to have the support of all the primary care doctors.”
Gifford’s administration was also supportive. “Because we are a critical access hospital, there are certain restrictions and requirements that we have to take into consideration with Medicare and Medicaid,” Dr. Johns says. “Being the sole hospitalist as we’re expanding allowed me to set the stage: what was lacking, what was missing, what we could improve on, what was already working quite well. [I incorporated] the help of the administration to fill in the gaps of what we needed.”
The primary nonclinical challenge for the lone hospitalist is finding patients to care for and doctors to share coverage. Christopher Farrar, MD, lead hospitalist at Anderson Hospital in Maryville, Ill., began the program there. His employer, the hospitalist company Inpatient Management Inc., based in St. Louis, Mo., manages 18 hospitalist programs in 12 states. “As I was ending my primary care role,” says Dr. Farrar, “this opportunity came available. I think that they weren’t expecting someone to jump in so quickly. They didn’t have the luxury of time to find another physician right away.”
There are now two physicians in the program there, and they are on the verge of getting a third. Dr. Farrar said he doesn’t think there are a lot of pluses to being the lone hospitalist. The most difficult part is avoiding burnout, he warns. Although there were plenty of patients and work for him when he first started at his institution, he wasn’t overwhelmed. But he was relieved when the company brought in a second physician with whom to share call. “I could have easily become overwhelmed quickly had it gone down that road,” he says.
Finding a patient base and physician call backup were not issues for J. Stewart Fulton, DO, medical director of the hospitalist program at Southern New Hampshire Medical Center in Nashua, when he began five years ago as the lone hospitalist. Foundation Medical Partners, a multispecialty group of 27 doctors directly affiliated with the hospital, recruited Dr. Fulton to start a hospitalist program. “I walked into an ideal situation,” he says. “I stepped into a group that had a patient base, that knew they needed hospital coverage, and were willing to support me as I grew to provide 24/7 coverage for myself.”
Culture Shock
In July 1998, Joseph Li, MD, director of the hospital medicine program at Beth Israel Deaconess Medical Center, Boston, was the chief medical resident at that institution when his chief of medicine approached him about starting a hospitalist program.
In the late 1990s there was no model of that kind in Boston. “He hired me as our first full-time hospitalist, and I was referred to as a hospitalist—but nobody really understood what that meant,” says Dr. Li. “Looking back now, I didn’t even really understand what that meant.”
Tin M. Oo, MD, medical director for the hospitalist program at St. Mary’s Health Center in Jefferson City, Mo., practiced for seven months as a lone hospitalist but was hardly a new physician. He has been practicing medicine for 34 years in the U.S. and four other countries: Burma (now Myanmar, his native country), Sri Lanka, Malaysia, and Brunei Darussalam. Since he emigrated to the U.S. 15 years ago, he has served as an epidemiologist with the state Department of Health in Minnesota, matriculated into a three-year internal medicine residency program in New York and practiced there, and was in private practice in Chattanooga, Tenn.
When Dr. Oo first came to St. Mary’s, he taught his co-workers, the patients, and their families. “The hospital [and nurses] didn’t have any experience with hospitalists so they didn’t know when to call me and when not to call me,” he says. Dr. Oo got his first hospitalist experience in Chattanooga, Tenn., when he worked with outpatients and some inpatients. His prior experience moonlighting as a hospitalist as well as an emergency physician has helped him greatly as a lone hospitalist. “It was a good thing that I wasn’t just a hospitalist; that I had been in private practice and worked in the ER and as a hospitalist. I knew what the private doctors were facing, and what was coming across from the ER.”
For those who have not yet practiced medicine, Dr. Oo would dissuade them from taking a position as a lone hospitalist. “You have to have a feel for what the ER physicians or what the family practice/ internists, and what the specialists do,” he says. “You also have to be in the hospitalist’s shoes, at least from time to time.”
Be Flexible
While all hospitalists need to be flexible, this may be particularly true for the lone hospitalist. Dr. Johns finds his dual internal medicine/pediatrics training serves him well. “I assist with patients, especially pediatrics, in the emergency department [ED], go up to [resuscitate the infant in] C sections, deal with all the pediatric issues and ER consultations during the day plus do all the general internal medicine care and adult care, which does make up the majority of what I do during the day,” he says. Two physician assistants have been brought on board to improve continuity on nights and weekends and decrease the workload of all physician providers.
Dr. Johns, whose title is associate medical director in charge of hospitalist services, finds the biggest challenge has been attaining and maintaining a commitment to quality on opposite shifts. Sharing coverage with several primary care physicians, he says, means there are differences in concepts of protocols for admissions, commitment to caring for the extra patients, and the physician’s comfort in his or her inpatient knowledge base.
Taking over after a previous night’s coverage, Dr. Johns is unsure which orders were carried out and which patients received what therapy, for instance. “The covering providers take care and make sure patients make it through to next day but often hesitate to alter the plan too much because they are not covering the following day as the inpatient provider.” A newly instated Thursday-through-Monday hospitalist service schedule has helped improve continuity of care and transfer of information through the weekend. But it is still not a perfect situation.
After 15 months as the lone hospitalist, Dr. Johns’ position has changed. He cares for patients during the day and during the opposite shift takes on administrative responsibilities, such as deciding on protocols and expanding services. That kind of juggling—without hospitalist colleagues—has required flexibility as well.
Plan and Set Boundaries
Educating the hospital taught Dr. Fulton a good deal as well, especially about his and their expectations. “The group that grasps the whole concept the quickest is the ancillary services (case management) and the nursing staff,” he says. He likens their receptivity to having a hospitalist to the workings of a pendulum: “There is nothing before this better way, and then they want more of it and they want it all the time. It really means needing to create boundaries”
Dr. Oo agrees that as a lone hospitalist it is important to set boundaries for your accountabilities. The administration of his hospital asked him whether he would take charge of rapid response calls. He declined, leaving that traditional role to the ED.
The year Dr. Fulton practiced as a lone hospitalist gave him a window of time to plan. “It really allowed me to hit the bumps in the road and figure things out so when I added partners, I was able to get them up to speed more quickly,” he says. “Hospitals continue to get busier and busier and that requires planning. I was tracking and trending the volume [of patients that] these 27 doctors were generating in the hospital so that I could anticipate how many doctors I needed. Hospitals continue to increase in volume. The intensity of medicine continues to increase. You always need to plan for one or two more docs than you think you need.”
Coverage
For many lone hospitalists, sharing schedule coverage is a dilemma. Dr. Li, an assistant professor of medicine at Harvard Medical School in Boston and a board member of SHM, spent one year as a lone hospitalist before another full-timer joined him. “Everybody understands that as sole physician you really can’t be expected to see patients 24/7/365,” says Dr. Li.
Dr. Li’s recommendation for any hospitalist group of any size—but particularly early on when the hospitalist is alone or in a small group—is to match volume with staffing. “With every program that I have seen or been involved with, early on there is always a massive shift of primary care providers who want to refer patients to you after the program is up and running, Dr. Li says.
Another recommendation Dr. Li has for the lone hospitalist is to identify how you will quickly get help in urgent circumstances. “There is a real benefit to the whole service for having more than one physician on any given day,” he says. It takes only one critically ill patient to cause an upheaval in the schedule.
Committee Work
As recent SHM data show, a large proportion of hospitalists serve on hospital committees. But during his year as a lone hospitalist, Dr. Li focused on taking care of patients, relying upon consultants, and getting through the day.
“I certainly had very little insight at that point of the hospitalist model in terms of communications and leading a team and being the leader of quality in the institution,” he says. “Those were the furthest things from my mind.”
Dr. Fulton participated on committees even though he was a lone hospitalist. “I was involved because I was willing to do the extra work and to use that opportunity to educate and establish who we were in the hospital,” he says. When he was joined by his first two partners, he protected them from committee work because that wasn’t their initial responsibility,” he says.
For lone hospitalists, “you either need to anticipate being on committees and protecting time for it, or you need to anticipate protecting yourself from the committees in order to provide your service,” says Dr. Fulton. “That’s sort of a slippery slope because if you lose the opportunity to become involved in committees, someone else will do it and then they’re making decisions for you that affect your practice of medicine in the hospital.”
Because Dr. Fulton would not sit in hourlong meetings, he took an indirect route—discussing issues with case managers on the floors in between patients or when they shared a patient.
Dr. Fulton advises the lone hospitalist to consider “who is boss” when he or she considers allocating time for committee involvement. Employment by a hospital versus a multispecialty group versus going out as a solo practitioner or working in a private group will determine whose agenda you have to fulfill. “If you are owned by the hospital, the hospital calls the shots; and you have to negotiate … where you put your efforts and your service. If they want you to be on committees, you need to negotiate less patient interaction. You can’t do both; you’ll begin to lose your mind.” TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
The Bad Hire
Hospital medicine groups depend on camaraderie and expertise to carry them through long days and heavy workloads. Group cohesiveness—often fragile—depends on recruiting and keeping hard-working doctors who pull their weight professionally and boost the group’s chemistry.
In a field with five job openings for every qualified candidate, and average annual turnover at 12%, hospital medicine groups can ill afford a bad hire. Whether that person is a practice killer, a cipher who blends into the wallpaper while collecting a paycheck, or a doctor marking time until a fellowship or something better comes along, the group leader must quickly limit a bad hire’s negative impact.
Recognizing that competition to hire hospitalists is fierce, it may seem that avoiding or axing a bad hire—the physician who either doesn’t mesh with your team, is a professional and/or personal train wreck, or has a blue-ribbon pedigree, but performs poorly—is a luxury hospitalist groups can’t afford.
But as Per Danielsson, MD, medical director of Seattle-based Swedish Medical Center’s adult hospitalist program has learned the hard way: “No doctor is better than the wrong doctor. I don’t sugarcoat the demands of our program with prospects. We’re a seasoned hospitalist program, we work hard, and, if we have a position vacant, we’ll work even harder for short periods of time until we find the right person.”
With a hospitalist group of 25 providers, Dr. Danielsson spends more time than he’d like recruiting and interviewing candidates, but he considers it time well spent. “The CV and interview are important, but I’ve devised a list of 12 personality traits that I consider important,” he says. “I share the list with candidates to see if we have a good fit.”
Chris Nussbaum, MD, CEO of Synergy Medical Group, based in Brandon, Fla., says: “They don’t make doctors the way they used to. I don’t see why some hospitalists think seeing 20 to 25 patients a day is such a big deal. I’ve had several tell me that 20 patients a day is no problem—and then they only last one day.” When that happens, Synergy cuts its losses, not allowing a bad hire to linger.
Dr. Nussbaum didn’t think twice about firing one new hire—a physician with an impressive resume who, while writing chart notes at a nursing station, watched a nurse have a seizure, gathered his notes and left the room. “He expected an endocrinologist standing nearby to help out, but it’s outrageous that any hospitalist wouldn’t respond appropriately,” he says. Such callous behavior would send shock waves through any group, and that physician was fired on the spot.
Another organizational disrupter, briefly employed by IPC-the Hospitalist Company (North Hollywood, Calif.) made inflammatory remarks about a hospital’s pre-eminent specialist and other referring physicians. He was fired. Several hospitalist leaders report hiring physicians with stellar pedigrees whose hands consistently strayed to nurses’ derrieres. Those doctors were quickly shown the door.
Robin Ryan, a career coach from Newcastle, Wash., who has prepared office-based physicians for professional moves to hospitalist careers, says the new career path can be confusing. When a physician and a hospitalist group have made a mistake, Ryan says most groups cut their losses by terminating someone who doesn’t fit. “Contracts often require a hefty severance fee, but it’s often the road that groups take,” she says.
Probing Personality
To weed out potential bad hires, employees long have used personality tests. Such tests also help job candidates clarify what matters most to them professionally. The SHM’s Career Satisfaction Task Force has developed a framework for hospitalists to do that. The self-test rests on four pillars of job satisfaction: reward/recognition, workload/schedule, autonomy/control, and community/environment (to view, go to www.hospitalmedicine.org and click “Career Satisfaction White Paper”).
Sylvia McKean, MD, medical director, the Brigham & Women’s Hospital/Faulkner Hospitalist Program in Boston and the task force’s co-chair, urges hospitalists to complete the self-test to maximize a potential job fit.
“All jobs have unpleasant side effects,” says Dr. McKean. “People get sick at bad times. There is high stress and sometimes high error rates. It’s important for a hospitalist to analyze what your needs are and to find an environment that best suits them.”
Dr. McKean also offers wisdom from the other side of desk, having interviewed candidates for coveted spots at Brigham & Women’s hospitalist program. “I’ve interviewed doctors who aren’t interested in hospitalist medicine but view our program as a stepping stone to the job they really want here,’’ she says. “We hired and fired someone who wanted her own way all the time. She left for another prestigious hospital. Then there are others who don’t want to teach, but choose a teaching hospital.”
Dr. McKean hopes SHM’s self-assessment tools will help job candidates focus on what they want from a hospital medicine group and avoid the “pebbles” that erode job satisfaction.
IPC, which employs 600 physicians in 100 practices in 24 markets, tried personality testing then discarded it. IPC hired a psychometric firm to devise a psychological profile of “best” and “worst” performing hospitalists. The testers created a test measuring seven key characteristics relating to temperament, intelligence, and clinical skills.
IPC’s CEO Adam Singer, MD, says: “We tested all candidates but found the test ineffective because nearly everyone, including me, got five or better.” He dropped the test, relying instead on extensive interviews. Dr. Singer reviews 2,500 to 3,000 physician resumes annually and spends significant resources on avoiding bad hires. All that hard work doesn’t avoid the occasional mistake.
“I’ve seen everything—the brilliant doctor who can’t function on a team, aloofness, temper tantrums, rudeness, and always pushing responsibility on someone else,” says Dr. Singer. “When something’s wrong, 90% of the time we terminate them ASAP. The other 10% we salvage by finding what’s stressing them, relieving the pressure, and mentoring them into proper behavior.”
Cynthia Stamer, a Dallas-based attorney at Glast, Phillips & Murray, P.C., works extensively with physicians and hospitals and sees young physicians straight from residency joining hospitalist programs “just looking for a job and not focused on whether or not there’s a good personality fit.” She urges job candidates and hirers to better probe the fit.
Stamer finds good hospitalists to be stress jockeys who thrive on the intensity of hospital work. “I think they’re born and not bred,” she says. “They tend to be bored or disruptive in office practices, and to enjoy a pattern of work hard, play hard. The ability to throw the ‘on’ switch and be intense for block scheduling, then be ‘off’ for a block suits them,” she says.
Not That Bad
In a field where an extra pair of hands can make the difference between taking night call or the freedom to take several days off for emergencies, a mediocre team member might seem better than none. Some hospitalist groups would rather pull a bigger load temporarily than tolerate a laggard; others stomach imperfection.
Spotting problems during the hiring process can turn a bad hire into a proper fit. For example, offering a permanent part-time position to someone with young children who can’t commit to full-time employment avoids potential problems. Or, asking enough probing questions might help you discover a physician has a year before a coveted fellowship begins; tailoring a one-year contract for that person optimizes fit. Eliminating managerial tasks for a pure clinician who eschews the leadership fast track works, too.
What to do with the mediocre performer rather than the egregious misfit? Perhaps she consistently arrives to work late, doesn’t complete her charts, and tries to avoid admissions or challenging assignments. A group leader may salvage the situation through mentoring and tying pay to performance. Dr. Singer says: “Underperformers usually don’t understand their impact on the group. We teach them healthcare economics and the flow of dollars. We train them to get the relationship between pay and performance, and hope for results.”
Stamer urges hospitalist leaders to build termination procedures into employment contracts, to document poor performance, and to give severance pay or buy out a contract with a bad hire. “People get testy around disengagement, but if you can take the heat out of the process, it’s better in the long run,” she concludes.
As hospitalist supply approaches demand, avoiding bad hires should be easier. For now, most groups prefer pulling together and working harder rather than abide an outlier. It comes with the territory. TH
Marlene Piturro is a frequent contributor to The Hospitalist.
Hospital medicine groups depend on camaraderie and expertise to carry them through long days and heavy workloads. Group cohesiveness—often fragile—depends on recruiting and keeping hard-working doctors who pull their weight professionally and boost the group’s chemistry.
In a field with five job openings for every qualified candidate, and average annual turnover at 12%, hospital medicine groups can ill afford a bad hire. Whether that person is a practice killer, a cipher who blends into the wallpaper while collecting a paycheck, or a doctor marking time until a fellowship or something better comes along, the group leader must quickly limit a bad hire’s negative impact.
Recognizing that competition to hire hospitalists is fierce, it may seem that avoiding or axing a bad hire—the physician who either doesn’t mesh with your team, is a professional and/or personal train wreck, or has a blue-ribbon pedigree, but performs poorly—is a luxury hospitalist groups can’t afford.
But as Per Danielsson, MD, medical director of Seattle-based Swedish Medical Center’s adult hospitalist program has learned the hard way: “No doctor is better than the wrong doctor. I don’t sugarcoat the demands of our program with prospects. We’re a seasoned hospitalist program, we work hard, and, if we have a position vacant, we’ll work even harder for short periods of time until we find the right person.”
With a hospitalist group of 25 providers, Dr. Danielsson spends more time than he’d like recruiting and interviewing candidates, but he considers it time well spent. “The CV and interview are important, but I’ve devised a list of 12 personality traits that I consider important,” he says. “I share the list with candidates to see if we have a good fit.”
Chris Nussbaum, MD, CEO of Synergy Medical Group, based in Brandon, Fla., says: “They don’t make doctors the way they used to. I don’t see why some hospitalists think seeing 20 to 25 patients a day is such a big deal. I’ve had several tell me that 20 patients a day is no problem—and then they only last one day.” When that happens, Synergy cuts its losses, not allowing a bad hire to linger.
Dr. Nussbaum didn’t think twice about firing one new hire—a physician with an impressive resume who, while writing chart notes at a nursing station, watched a nurse have a seizure, gathered his notes and left the room. “He expected an endocrinologist standing nearby to help out, but it’s outrageous that any hospitalist wouldn’t respond appropriately,” he says. Such callous behavior would send shock waves through any group, and that physician was fired on the spot.
Another organizational disrupter, briefly employed by IPC-the Hospitalist Company (North Hollywood, Calif.) made inflammatory remarks about a hospital’s pre-eminent specialist and other referring physicians. He was fired. Several hospitalist leaders report hiring physicians with stellar pedigrees whose hands consistently strayed to nurses’ derrieres. Those doctors were quickly shown the door.
Robin Ryan, a career coach from Newcastle, Wash., who has prepared office-based physicians for professional moves to hospitalist careers, says the new career path can be confusing. When a physician and a hospitalist group have made a mistake, Ryan says most groups cut their losses by terminating someone who doesn’t fit. “Contracts often require a hefty severance fee, but it’s often the road that groups take,” she says.
Probing Personality
To weed out potential bad hires, employees long have used personality tests. Such tests also help job candidates clarify what matters most to them professionally. The SHM’s Career Satisfaction Task Force has developed a framework for hospitalists to do that. The self-test rests on four pillars of job satisfaction: reward/recognition, workload/schedule, autonomy/control, and community/environment (to view, go to www.hospitalmedicine.org and click “Career Satisfaction White Paper”).
Sylvia McKean, MD, medical director, the Brigham & Women’s Hospital/Faulkner Hospitalist Program in Boston and the task force’s co-chair, urges hospitalists to complete the self-test to maximize a potential job fit.
“All jobs have unpleasant side effects,” says Dr. McKean. “People get sick at bad times. There is high stress and sometimes high error rates. It’s important for a hospitalist to analyze what your needs are and to find an environment that best suits them.”
Dr. McKean also offers wisdom from the other side of desk, having interviewed candidates for coveted spots at Brigham & Women’s hospitalist program. “I’ve interviewed doctors who aren’t interested in hospitalist medicine but view our program as a stepping stone to the job they really want here,’’ she says. “We hired and fired someone who wanted her own way all the time. She left for another prestigious hospital. Then there are others who don’t want to teach, but choose a teaching hospital.”
Dr. McKean hopes SHM’s self-assessment tools will help job candidates focus on what they want from a hospital medicine group and avoid the “pebbles” that erode job satisfaction.
IPC, which employs 600 physicians in 100 practices in 24 markets, tried personality testing then discarded it. IPC hired a psychometric firm to devise a psychological profile of “best” and “worst” performing hospitalists. The testers created a test measuring seven key characteristics relating to temperament, intelligence, and clinical skills.
IPC’s CEO Adam Singer, MD, says: “We tested all candidates but found the test ineffective because nearly everyone, including me, got five or better.” He dropped the test, relying instead on extensive interviews. Dr. Singer reviews 2,500 to 3,000 physician resumes annually and spends significant resources on avoiding bad hires. All that hard work doesn’t avoid the occasional mistake.
“I’ve seen everything—the brilliant doctor who can’t function on a team, aloofness, temper tantrums, rudeness, and always pushing responsibility on someone else,” says Dr. Singer. “When something’s wrong, 90% of the time we terminate them ASAP. The other 10% we salvage by finding what’s stressing them, relieving the pressure, and mentoring them into proper behavior.”
Cynthia Stamer, a Dallas-based attorney at Glast, Phillips & Murray, P.C., works extensively with physicians and hospitals and sees young physicians straight from residency joining hospitalist programs “just looking for a job and not focused on whether or not there’s a good personality fit.” She urges job candidates and hirers to better probe the fit.
Stamer finds good hospitalists to be stress jockeys who thrive on the intensity of hospital work. “I think they’re born and not bred,” she says. “They tend to be bored or disruptive in office practices, and to enjoy a pattern of work hard, play hard. The ability to throw the ‘on’ switch and be intense for block scheduling, then be ‘off’ for a block suits them,” she says.
Not That Bad
In a field where an extra pair of hands can make the difference between taking night call or the freedom to take several days off for emergencies, a mediocre team member might seem better than none. Some hospitalist groups would rather pull a bigger load temporarily than tolerate a laggard; others stomach imperfection.
Spotting problems during the hiring process can turn a bad hire into a proper fit. For example, offering a permanent part-time position to someone with young children who can’t commit to full-time employment avoids potential problems. Or, asking enough probing questions might help you discover a physician has a year before a coveted fellowship begins; tailoring a one-year contract for that person optimizes fit. Eliminating managerial tasks for a pure clinician who eschews the leadership fast track works, too.
What to do with the mediocre performer rather than the egregious misfit? Perhaps she consistently arrives to work late, doesn’t complete her charts, and tries to avoid admissions or challenging assignments. A group leader may salvage the situation through mentoring and tying pay to performance. Dr. Singer says: “Underperformers usually don’t understand their impact on the group. We teach them healthcare economics and the flow of dollars. We train them to get the relationship between pay and performance, and hope for results.”
Stamer urges hospitalist leaders to build termination procedures into employment contracts, to document poor performance, and to give severance pay or buy out a contract with a bad hire. “People get testy around disengagement, but if you can take the heat out of the process, it’s better in the long run,” she concludes.
As hospitalist supply approaches demand, avoiding bad hires should be easier. For now, most groups prefer pulling together and working harder rather than abide an outlier. It comes with the territory. TH
Marlene Piturro is a frequent contributor to The Hospitalist.
Hospital medicine groups depend on camaraderie and expertise to carry them through long days and heavy workloads. Group cohesiveness—often fragile—depends on recruiting and keeping hard-working doctors who pull their weight professionally and boost the group’s chemistry.
In a field with five job openings for every qualified candidate, and average annual turnover at 12%, hospital medicine groups can ill afford a bad hire. Whether that person is a practice killer, a cipher who blends into the wallpaper while collecting a paycheck, or a doctor marking time until a fellowship or something better comes along, the group leader must quickly limit a bad hire’s negative impact.
Recognizing that competition to hire hospitalists is fierce, it may seem that avoiding or axing a bad hire—the physician who either doesn’t mesh with your team, is a professional and/or personal train wreck, or has a blue-ribbon pedigree, but performs poorly—is a luxury hospitalist groups can’t afford.
But as Per Danielsson, MD, medical director of Seattle-based Swedish Medical Center’s adult hospitalist program has learned the hard way: “No doctor is better than the wrong doctor. I don’t sugarcoat the demands of our program with prospects. We’re a seasoned hospitalist program, we work hard, and, if we have a position vacant, we’ll work even harder for short periods of time until we find the right person.”
With a hospitalist group of 25 providers, Dr. Danielsson spends more time than he’d like recruiting and interviewing candidates, but he considers it time well spent. “The CV and interview are important, but I’ve devised a list of 12 personality traits that I consider important,” he says. “I share the list with candidates to see if we have a good fit.”
Chris Nussbaum, MD, CEO of Synergy Medical Group, based in Brandon, Fla., says: “They don’t make doctors the way they used to. I don’t see why some hospitalists think seeing 20 to 25 patients a day is such a big deal. I’ve had several tell me that 20 patients a day is no problem—and then they only last one day.” When that happens, Synergy cuts its losses, not allowing a bad hire to linger.
Dr. Nussbaum didn’t think twice about firing one new hire—a physician with an impressive resume who, while writing chart notes at a nursing station, watched a nurse have a seizure, gathered his notes and left the room. “He expected an endocrinologist standing nearby to help out, but it’s outrageous that any hospitalist wouldn’t respond appropriately,” he says. Such callous behavior would send shock waves through any group, and that physician was fired on the spot.
Another organizational disrupter, briefly employed by IPC-the Hospitalist Company (North Hollywood, Calif.) made inflammatory remarks about a hospital’s pre-eminent specialist and other referring physicians. He was fired. Several hospitalist leaders report hiring physicians with stellar pedigrees whose hands consistently strayed to nurses’ derrieres. Those doctors were quickly shown the door.
Robin Ryan, a career coach from Newcastle, Wash., who has prepared office-based physicians for professional moves to hospitalist careers, says the new career path can be confusing. When a physician and a hospitalist group have made a mistake, Ryan says most groups cut their losses by terminating someone who doesn’t fit. “Contracts often require a hefty severance fee, but it’s often the road that groups take,” she says.
Probing Personality
To weed out potential bad hires, employees long have used personality tests. Such tests also help job candidates clarify what matters most to them professionally. The SHM’s Career Satisfaction Task Force has developed a framework for hospitalists to do that. The self-test rests on four pillars of job satisfaction: reward/recognition, workload/schedule, autonomy/control, and community/environment (to view, go to www.hospitalmedicine.org and click “Career Satisfaction White Paper”).
Sylvia McKean, MD, medical director, the Brigham & Women’s Hospital/Faulkner Hospitalist Program in Boston and the task force’s co-chair, urges hospitalists to complete the self-test to maximize a potential job fit.
“All jobs have unpleasant side effects,” says Dr. McKean. “People get sick at bad times. There is high stress and sometimes high error rates. It’s important for a hospitalist to analyze what your needs are and to find an environment that best suits them.”
Dr. McKean also offers wisdom from the other side of desk, having interviewed candidates for coveted spots at Brigham & Women’s hospitalist program. “I’ve interviewed doctors who aren’t interested in hospitalist medicine but view our program as a stepping stone to the job they really want here,’’ she says. “We hired and fired someone who wanted her own way all the time. She left for another prestigious hospital. Then there are others who don’t want to teach, but choose a teaching hospital.”
Dr. McKean hopes SHM’s self-assessment tools will help job candidates focus on what they want from a hospital medicine group and avoid the “pebbles” that erode job satisfaction.
IPC, which employs 600 physicians in 100 practices in 24 markets, tried personality testing then discarded it. IPC hired a psychometric firm to devise a psychological profile of “best” and “worst” performing hospitalists. The testers created a test measuring seven key characteristics relating to temperament, intelligence, and clinical skills.
IPC’s CEO Adam Singer, MD, says: “We tested all candidates but found the test ineffective because nearly everyone, including me, got five or better.” He dropped the test, relying instead on extensive interviews. Dr. Singer reviews 2,500 to 3,000 physician resumes annually and spends significant resources on avoiding bad hires. All that hard work doesn’t avoid the occasional mistake.
“I’ve seen everything—the brilliant doctor who can’t function on a team, aloofness, temper tantrums, rudeness, and always pushing responsibility on someone else,” says Dr. Singer. “When something’s wrong, 90% of the time we terminate them ASAP. The other 10% we salvage by finding what’s stressing them, relieving the pressure, and mentoring them into proper behavior.”
Cynthia Stamer, a Dallas-based attorney at Glast, Phillips & Murray, P.C., works extensively with physicians and hospitals and sees young physicians straight from residency joining hospitalist programs “just looking for a job and not focused on whether or not there’s a good personality fit.” She urges job candidates and hirers to better probe the fit.
Stamer finds good hospitalists to be stress jockeys who thrive on the intensity of hospital work. “I think they’re born and not bred,” she says. “They tend to be bored or disruptive in office practices, and to enjoy a pattern of work hard, play hard. The ability to throw the ‘on’ switch and be intense for block scheduling, then be ‘off’ for a block suits them,” she says.
Not That Bad
In a field where an extra pair of hands can make the difference between taking night call or the freedom to take several days off for emergencies, a mediocre team member might seem better than none. Some hospitalist groups would rather pull a bigger load temporarily than tolerate a laggard; others stomach imperfection.
Spotting problems during the hiring process can turn a bad hire into a proper fit. For example, offering a permanent part-time position to someone with young children who can’t commit to full-time employment avoids potential problems. Or, asking enough probing questions might help you discover a physician has a year before a coveted fellowship begins; tailoring a one-year contract for that person optimizes fit. Eliminating managerial tasks for a pure clinician who eschews the leadership fast track works, too.
What to do with the mediocre performer rather than the egregious misfit? Perhaps she consistently arrives to work late, doesn’t complete her charts, and tries to avoid admissions or challenging assignments. A group leader may salvage the situation through mentoring and tying pay to performance. Dr. Singer says: “Underperformers usually don’t understand their impact on the group. We teach them healthcare economics and the flow of dollars. We train them to get the relationship between pay and performance, and hope for results.”
Stamer urges hospitalist leaders to build termination procedures into employment contracts, to document poor performance, and to give severance pay or buy out a contract with a bad hire. “People get testy around disengagement, but if you can take the heat out of the process, it’s better in the long run,” she concludes.
As hospitalist supply approaches demand, avoiding bad hires should be easier. For now, most groups prefer pulling together and working harder rather than abide an outlier. It comes with the territory. TH
Marlene Piturro is a frequent contributor to The Hospitalist.