User login
Nonsurgical OSA treatment ineffective in children with Down syndrome
CORONADO, CALIF. – Resolution of who were treated nonsurgically with either medication, observation, or supplemental oxygen was low, results from a small cohort study showed.

“This suggests that we should consider early treatment options, including multimodal approaches, for children with mild OSA and Down syndrome,” one of the study authors, Javier J.M. Howard, MPH, said at the Triological Society’s Combined Sections Meeting. “Prospective studies with longer follow-up are needed to better understand treatment outcomes in children with Down syndrome and mild OSA.”
An estimated 1%-6% of otherwise healthy children have obstructive sleep apnea, but the prevalence in children with Down syndrome is estimated to be between 30% and 70%, said Mr. Howard, a medical student at the University of Cincinnati. Additionally, those with Down syndrome tend to have more severe phenotypes, including significant hypoxemia and hypoventilation, compared with children without Down syndrome. “Nasal steroids, oral antileukotrienes, and supplemental oxygen have shown efficacy in the treatment of mild OSA in otherwise healthy children,” he said. “Observation is also employed in children with mild OSA, as a proportion of them will resolve spontaneously. The efficacy of these approaches in children with Down syndrome is unknown.”
In a study led by senior author Stacey L. Ishman, MD, MPH, researchers set out to examine the efficacy of single-medication therapy with either montelukast or intransal steroids versus observation versus oxygen on polysomnographic (PSG) outcomes in children with Down syndrome. They conducted a retrospective chart review of 24 children diagnosed with Down syndrome and mild OSA. The children were surgically naive and were treated between 2012 and 2017 with either supplemental oxygen, a single medication, or were observed. They had a follow-up PSG 3-12 months after initiation of treatment. The primary outcome was obstructive apnea hypopnea index (AHI), while secondary outcomes were oxygen saturation nadir, percent of total sleep time in rapid eye movement, and percentage of total sleep time with end-tidal carbon dioxide of greater than 50 mm Hg.
Of the 24 children, 58% were female, 67% were white, 13 were treated with observation, one was treated with oxygen, and 10 were treated with medication. Their baseline obstructive AHIs were 2.9, 3.5, and 3.3 events per hour, respectively. The follow-up PSGs revealed no statistically significant changes in obstructive AHI, oxygen saturation nadir, percentage of total sleep time in rapid eye movement, or percentage of total sleep time with end-tidal carbon dioxide greater than 50 mm Hg for any treatment group. OSA resolved in one patient in the observation group and in two patients in the medication group. At the same time, OSA worsened in two patients each in the medication and observation groups. Resolution of OSA was observed in 20% of patients in the medication group, compared with 7.1% of those in the observation or oxygen group (P = .82).
Mr. Howard acknowledged certain limitations of the study, including the potential for selection bias, its retrospective design, and its small sample size. “Resolution of mild OSA was low for all of our treatment groups after 3-12 months of treatment,” he said. “Resolution with medication was lower in our study, compared to published studies in otherwise healthy children.”
The researchers reported having no financial disclosures. The meeting was jointly sponsored by the Triological Society and the American College of Surgeons.
SOURCE: Howard J et al .Triological CSM, Abstracts.
CORONADO, CALIF. – Resolution of who were treated nonsurgically with either medication, observation, or supplemental oxygen was low, results from a small cohort study showed.
“This suggests that we should consider early treatment options, including multimodal approaches, for children with mild OSA and Down syndrome,” one of the study authors, Javier J.M. Howard, MPH, said at the Triological Society’s Combined Sections Meeting. “Prospective studies with longer follow-up are needed to better understand treatment outcomes in children with Down syndrome and mild OSA.”
An estimated 1%-6% of otherwise healthy children have obstructive sleep apnea, but the prevalence in children with Down syndrome is estimated to be between 30% and 70%, said Mr. Howard, a medical student at the University of Cincinnati. Additionally, those with Down syndrome tend to have more severe phenotypes, including significant hypoxemia and hypoventilation, compared with children without Down syndrome. “Nasal steroids, oral antileukotrienes, and supplemental oxygen have shown efficacy in the treatment of mild OSA in otherwise healthy children,” he said. “Observation is also employed in children with mild OSA, as a proportion of them will resolve spontaneously. The efficacy of these approaches in children with Down syndrome is unknown.”
In a study led by senior author Stacey L. Ishman, MD, MPH, researchers set out to examine the efficacy of single-medication therapy with either montelukast or intransal steroids versus observation versus oxygen on polysomnographic (PSG) outcomes in children with Down syndrome. They conducted a retrospective chart review of 24 children diagnosed with Down syndrome and mild OSA. The children were surgically naive and were treated between 2012 and 2017 with either supplemental oxygen, a single medication, or were observed. They had a follow-up PSG 3-12 months after initiation of treatment. The primary outcome was obstructive apnea hypopnea index (AHI), while secondary outcomes were oxygen saturation nadir, percent of total sleep time in rapid eye movement, and percentage of total sleep time with end-tidal carbon dioxide of greater than 50 mm Hg.
Of the 24 children, 58% were female, 67% were white, 13 were treated with observation, one was treated with oxygen, and 10 were treated with medication. Their baseline obstructive AHIs were 2.9, 3.5, and 3.3 events per hour, respectively. The follow-up PSGs revealed no statistically significant changes in obstructive AHI, oxygen saturation nadir, percentage of total sleep time in rapid eye movement, or percentage of total sleep time with end-tidal carbon dioxide greater than 50 mm Hg for any treatment group. OSA resolved in one patient in the observation group and in two patients in the medication group. At the same time, OSA worsened in two patients each in the medication and observation groups. Resolution of OSA was observed in 20% of patients in the medication group, compared with 7.1% of those in the observation or oxygen group (P = .82).
Mr. Howard acknowledged certain limitations of the study, including the potential for selection bias, its retrospective design, and its small sample size. “Resolution of mild OSA was low for all of our treatment groups after 3-12 months of treatment,” he said. “Resolution with medication was lower in our study, compared to published studies in otherwise healthy children.”
The researchers reported having no financial disclosures. The meeting was jointly sponsored by the Triological Society and the American College of Surgeons.
SOURCE: Howard J et al .Triological CSM, Abstracts.
CORONADO, CALIF. – Resolution of who were treated nonsurgically with either medication, observation, or supplemental oxygen was low, results from a small cohort study showed.
“This suggests that we should consider early treatment options, including multimodal approaches, for children with mild OSA and Down syndrome,” one of the study authors, Javier J.M. Howard, MPH, said at the Triological Society’s Combined Sections Meeting. “Prospective studies with longer follow-up are needed to better understand treatment outcomes in children with Down syndrome and mild OSA.”
An estimated 1%-6% of otherwise healthy children have obstructive sleep apnea, but the prevalence in children with Down syndrome is estimated to be between 30% and 70%, said Mr. Howard, a medical student at the University of Cincinnati. Additionally, those with Down syndrome tend to have more severe phenotypes, including significant hypoxemia and hypoventilation, compared with children without Down syndrome. “Nasal steroids, oral antileukotrienes, and supplemental oxygen have shown efficacy in the treatment of mild OSA in otherwise healthy children,” he said. “Observation is also employed in children with mild OSA, as a proportion of them will resolve spontaneously. The efficacy of these approaches in children with Down syndrome is unknown.”
In a study led by senior author Stacey L. Ishman, MD, MPH, researchers set out to examine the efficacy of single-medication therapy with either montelukast or intransal steroids versus observation versus oxygen on polysomnographic (PSG) outcomes in children with Down syndrome. They conducted a retrospective chart review of 24 children diagnosed with Down syndrome and mild OSA. The children were surgically naive and were treated between 2012 and 2017 with either supplemental oxygen, a single medication, or were observed. They had a follow-up PSG 3-12 months after initiation of treatment. The primary outcome was obstructive apnea hypopnea index (AHI), while secondary outcomes were oxygen saturation nadir, percent of total sleep time in rapid eye movement, and percentage of total sleep time with end-tidal carbon dioxide of greater than 50 mm Hg.
Of the 24 children, 58% were female, 67% were white, 13 were treated with observation, one was treated with oxygen, and 10 were treated with medication. Their baseline obstructive AHIs were 2.9, 3.5, and 3.3 events per hour, respectively. The follow-up PSGs revealed no statistically significant changes in obstructive AHI, oxygen saturation nadir, percentage of total sleep time in rapid eye movement, or percentage of total sleep time with end-tidal carbon dioxide greater than 50 mm Hg for any treatment group. OSA resolved in one patient in the observation group and in two patients in the medication group. At the same time, OSA worsened in two patients each in the medication and observation groups. Resolution of OSA was observed in 20% of patients in the medication group, compared with 7.1% of those in the observation or oxygen group (P = .82).
Mr. Howard acknowledged certain limitations of the study, including the potential for selection bias, its retrospective design, and its small sample size. “Resolution of mild OSA was low for all of our treatment groups after 3-12 months of treatment,” he said. “Resolution with medication was lower in our study, compared to published studies in otherwise healthy children.”
The researchers reported having no financial disclosures. The meeting was jointly sponsored by the Triological Society and the American College of Surgeons.
SOURCE: Howard J et al .Triological CSM, Abstracts.
REPORTING FROM TRIOLOGICAL CSM
Key clinical point: Resolution of mild OSA was low for all treatment groups after 3-12 months of treatment.
Major finding: Resolution of OSA was observed in 20% of patients in the medication group, compared with 7.1% of those in the observation or oxygen group (P = .82).
Study details: A retrospective chart review of 24 children diagnosed with Down syndrome and mild OSA.
Disclosures: The researchers reported having no financial disclosures.
Source: Howard J et al. Triological CSM, Abstracts.
New findings raise questions about the role of ANAs in SLE
Antinuclear antibodies (ANAs) have long been considered an important marker in rheumatologic conditions, particularly for the diagnosis and classification of patients with systemic lupus erythematosus, but recent findings are raising new questions about their role.
“We’ve measured ANAs for a long time – it’s a very important test in rheumatology,” David S. Pisetsky, MD, PhD, explained in an interview.
However, even though this test has been around for decades, “some interesting things have developed around it that have made a lot of people, including me, take a second look,” said Dr. Pisetsky, professor of medicine and immunology at Duke University, Durham, N.C.
He elaborated on those recent findings, which relate to the findings of ANA negativity in patients with an established diagnosis of systemic lupus erythematosus (SLE) and to variability among ANA test kit findings, during a presentation at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
“Screening of patients during clinical trials for new treatments of SLE suggest that a significant number of people with lupus – 20%-30%, in fact – are ANA negative despite disease activity at the time the test is done,” he said.
For example, unpublished (but recently submitted) data from a phase 2 trial looking at the efficacy and safety of an interleukin-6 monoclonal antibody for the treatment of SLE showed that 23.8% of baseline samples from 183 SLE patients with positive historical ANA and clinically active lupus prior to randomization were ANA negative.
A particular concern with respect to such findings is that ANA positivity is typically a criterion for entry into clinical trials of therapies for lupus and prescription of medications approved for active lupus, Dr. Pisetsky said.
“On the other hand, about 20% of otherwise healthy people – especially women – can be ANA positive, so it’s always been problematic as a screening test due to these false positives, but these new findings suggest that in lupus a real concern is false negatives,” he said. “It’s quite a surprise.”
The findings raise questions about whether ANA negativity in SLE reflects the natural history of the disease, an effect of treatments, or a problem with the assays.
It appears an important problem relates to test kit variability, he said.
“There are lots of different ANA test kits. Their performance characteristics are very different. The performance of ANA tests is much more variable than people realize,” he said, citing data from an analysis that he and his colleagues conducted using 103 samples from a cohort of patients with established SLE.
In that 2017 study, an ANA enzyme-linked immunosorbent assay showed an ANA-negativity rate of 11.7% with zero indeterminate tests, whereas three different test kits showed ANA-negativity rates of 22.3% (with 8.7% of samples reported as indeterminate), 9.7% (with another 9.7% indeterminate), and 4.9% (with another 1.9% indeterminate), respectively. Multiplex testing showed a 13.6% ANA-negativity rate and an indeterminate rate of 7.8% (Ann Rheum Dis. 2018;77:911-3).
Only one sample tested negative for ANA on all three test kits, and disagreement about ANA negativity occurred in one-third of the samples, he said.
Anti–double-stranded DNA assays
Recent findings also raise questions about the use of assays that specifically assess for anti–double-stranded DNA (anti-dsDNA) antibodies, which are highly associated with SLE and have been used as a biomarker for the disease, Dr. Pisetsky said.
For example, a comparison of two anti-dsDNA assays showed discordant results with respect to negativity for anti-dsDNA antibodies in 64 of 181 samples from SLE patients. One assay showed a 70.7% rate of anti-dsDNA negativity and the other showed a 37.6% rate.
The concern regarding test variability relates to the issue of ANA positivity and eligibility for study enrollment and certain treatments; test variability can affect the diagnosis of patients with SLE because ANA positivity is an important finding in routine clinical care, and for anti-dsDNA, test variability can affect assessment of disease activity, he explained.
Tests may differ in a number of ways, such as in their specificity, sensitivity, avidity, and range of epitopes detected. Unfortunately, not enough is known at this point to make specific recommendations regarding best test kits, and while there are alternative technologies that could be useful for ANA testing, none has been validated for particular use in the assessment of trial eligibility, Dr. Pisetsky said.
Nonetheless, awareness of the test variability is important, especially when it comes to assessing patients for trial eligibility and prescribing medications, he added. “For practical, real-world utilization, people need to know about this.”
Dr. Pisetsky reported receiving ANA-related research support from Pfizer, conducting collaborative research with Bio-Rad and EuroImmun, and serving as an adviser to ImmunArray.
Antinuclear antibodies (ANAs) have long been considered an important marker in rheumatologic conditions, particularly for the diagnosis and classification of patients with systemic lupus erythematosus, but recent findings are raising new questions about their role.
“We’ve measured ANAs for a long time – it’s a very important test in rheumatology,” David S. Pisetsky, MD, PhD, explained in an interview.
However, even though this test has been around for decades, “some interesting things have developed around it that have made a lot of people, including me, take a second look,” said Dr. Pisetsky, professor of medicine and immunology at Duke University, Durham, N.C.
He elaborated on those recent findings, which relate to the findings of ANA negativity in patients with an established diagnosis of systemic lupus erythematosus (SLE) and to variability among ANA test kit findings, during a presentation at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
“Screening of patients during clinical trials for new treatments of SLE suggest that a significant number of people with lupus – 20%-30%, in fact – are ANA negative despite disease activity at the time the test is done,” he said.
For example, unpublished (but recently submitted) data from a phase 2 trial looking at the efficacy and safety of an interleukin-6 monoclonal antibody for the treatment of SLE showed that 23.8% of baseline samples from 183 SLE patients with positive historical ANA and clinically active lupus prior to randomization were ANA negative.
A particular concern with respect to such findings is that ANA positivity is typically a criterion for entry into clinical trials of therapies for lupus and prescription of medications approved for active lupus, Dr. Pisetsky said.
“On the other hand, about 20% of otherwise healthy people – especially women – can be ANA positive, so it’s always been problematic as a screening test due to these false positives, but these new findings suggest that in lupus a real concern is false negatives,” he said. “It’s quite a surprise.”
The findings raise questions about whether ANA negativity in SLE reflects the natural history of the disease, an effect of treatments, or a problem with the assays.
It appears an important problem relates to test kit variability, he said.
“There are lots of different ANA test kits. Their performance characteristics are very different. The performance of ANA tests is much more variable than people realize,” he said, citing data from an analysis that he and his colleagues conducted using 103 samples from a cohort of patients with established SLE.
In that 2017 study, an ANA enzyme-linked immunosorbent assay showed an ANA-negativity rate of 11.7% with zero indeterminate tests, whereas three different test kits showed ANA-negativity rates of 22.3% (with 8.7% of samples reported as indeterminate), 9.7% (with another 9.7% indeterminate), and 4.9% (with another 1.9% indeterminate), respectively. Multiplex testing showed a 13.6% ANA-negativity rate and an indeterminate rate of 7.8% (Ann Rheum Dis. 2018;77:911-3).
Only one sample tested negative for ANA on all three test kits, and disagreement about ANA negativity occurred in one-third of the samples, he said.
Anti–double-stranded DNA assays
Recent findings also raise questions about the use of assays that specifically assess for anti–double-stranded DNA (anti-dsDNA) antibodies, which are highly associated with SLE and have been used as a biomarker for the disease, Dr. Pisetsky said.
For example, a comparison of two anti-dsDNA assays showed discordant results with respect to negativity for anti-dsDNA antibodies in 64 of 181 samples from SLE patients. One assay showed a 70.7% rate of anti-dsDNA negativity and the other showed a 37.6% rate.
The concern regarding test variability relates to the issue of ANA positivity and eligibility for study enrollment and certain treatments; test variability can affect the diagnosis of patients with SLE because ANA positivity is an important finding in routine clinical care, and for anti-dsDNA, test variability can affect assessment of disease activity, he explained.
Tests may differ in a number of ways, such as in their specificity, sensitivity, avidity, and range of epitopes detected. Unfortunately, not enough is known at this point to make specific recommendations regarding best test kits, and while there are alternative technologies that could be useful for ANA testing, none has been validated for particular use in the assessment of trial eligibility, Dr. Pisetsky said.
Nonetheless, awareness of the test variability is important, especially when it comes to assessing patients for trial eligibility and prescribing medications, he added. “For practical, real-world utilization, people need to know about this.”
Dr. Pisetsky reported receiving ANA-related research support from Pfizer, conducting collaborative research with Bio-Rad and EuroImmun, and serving as an adviser to ImmunArray.
Antinuclear antibodies (ANAs) have long been considered an important marker in rheumatologic conditions, particularly for the diagnosis and classification of patients with systemic lupus erythematosus, but recent findings are raising new questions about their role.
“We’ve measured ANAs for a long time – it’s a very important test in rheumatology,” David S. Pisetsky, MD, PhD, explained in an interview.
However, even though this test has been around for decades, “some interesting things have developed around it that have made a lot of people, including me, take a second look,” said Dr. Pisetsky, professor of medicine and immunology at Duke University, Durham, N.C.
He elaborated on those recent findings, which relate to the findings of ANA negativity in patients with an established diagnosis of systemic lupus erythematosus (SLE) and to variability among ANA test kit findings, during a presentation at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
“Screening of patients during clinical trials for new treatments of SLE suggest that a significant number of people with lupus – 20%-30%, in fact – are ANA negative despite disease activity at the time the test is done,” he said.
For example, unpublished (but recently submitted) data from a phase 2 trial looking at the efficacy and safety of an interleukin-6 monoclonal antibody for the treatment of SLE showed that 23.8% of baseline samples from 183 SLE patients with positive historical ANA and clinically active lupus prior to randomization were ANA negative.
A particular concern with respect to such findings is that ANA positivity is typically a criterion for entry into clinical trials of therapies for lupus and prescription of medications approved for active lupus, Dr. Pisetsky said.
“On the other hand, about 20% of otherwise healthy people – especially women – can be ANA positive, so it’s always been problematic as a screening test due to these false positives, but these new findings suggest that in lupus a real concern is false negatives,” he said. “It’s quite a surprise.”
The findings raise questions about whether ANA negativity in SLE reflects the natural history of the disease, an effect of treatments, or a problem with the assays.
It appears an important problem relates to test kit variability, he said.
“There are lots of different ANA test kits. Their performance characteristics are very different. The performance of ANA tests is much more variable than people realize,” he said, citing data from an analysis that he and his colleagues conducted using 103 samples from a cohort of patients with established SLE.
In that 2017 study, an ANA enzyme-linked immunosorbent assay showed an ANA-negativity rate of 11.7% with zero indeterminate tests, whereas three different test kits showed ANA-negativity rates of 22.3% (with 8.7% of samples reported as indeterminate), 9.7% (with another 9.7% indeterminate), and 4.9% (with another 1.9% indeterminate), respectively. Multiplex testing showed a 13.6% ANA-negativity rate and an indeterminate rate of 7.8% (Ann Rheum Dis. 2018;77:911-3).
Only one sample tested negative for ANA on all three test kits, and disagreement about ANA negativity occurred in one-third of the samples, he said.
Anti–double-stranded DNA assays
Recent findings also raise questions about the use of assays that specifically assess for anti–double-stranded DNA (anti-dsDNA) antibodies, which are highly associated with SLE and have been used as a biomarker for the disease, Dr. Pisetsky said.
For example, a comparison of two anti-dsDNA assays showed discordant results with respect to negativity for anti-dsDNA antibodies in 64 of 181 samples from SLE patients. One assay showed a 70.7% rate of anti-dsDNA negativity and the other showed a 37.6% rate.
The concern regarding test variability relates to the issue of ANA positivity and eligibility for study enrollment and certain treatments; test variability can affect the diagnosis of patients with SLE because ANA positivity is an important finding in routine clinical care, and for anti-dsDNA, test variability can affect assessment of disease activity, he explained.
Tests may differ in a number of ways, such as in their specificity, sensitivity, avidity, and range of epitopes detected. Unfortunately, not enough is known at this point to make specific recommendations regarding best test kits, and while there are alternative technologies that could be useful for ANA testing, none has been validated for particular use in the assessment of trial eligibility, Dr. Pisetsky said.
Nonetheless, awareness of the test variability is important, especially when it comes to assessing patients for trial eligibility and prescribing medications, he added. “For practical, real-world utilization, people need to know about this.”
Dr. Pisetsky reported receiving ANA-related research support from Pfizer, conducting collaborative research with Bio-Rad and EuroImmun, and serving as an adviser to ImmunArray.
EXPERT ANALYSIS FROM THE WINTER RHEUMATOLOGY SYMPOSIUM
Obstetric hospitalists can screen for postpartum depression
Postpartum depression (PPD) is the most common complication of pregnancy, and onset can occur at any time from pregnancy until up to 1 year post partum.1,2 The immediate postpartum period is a time during which care is shared among multiple providers for both mother and child, and the transition from inpatient to outpatient postpartum care can impede communication between those caring for the patient in each setting. In 2018, the American College of Obstetricians and Gynecologists published a committee opinion emphasizing the importance of the “fourth trimester” and calling for health care providers to assist women in navigating the transition from pre- to postpartum care.3 An important consideration of perinatal care is mental health care for the mother, including screening and care for postpartum depression; however, the optimal role for the obstetric hospitalist in providing such services has been unclear.

Estimates of the prevalence of PPD in new mothers in the United States varied by state from 8% to 20% in 2012, with an overall average of 12%.2 Left untreated, PPD may result in significant negative outcomes for women, their children, and families. The depressive symptoms of PPD may persist for months or years afterward,4 with one study finding elevated depressive symptoms in women up to 11 years post partum.5 Suicide is also a leading cause of pregnancy-related mortality associated with depressive symptoms.6-9 In addition, maternal postpartum depression symptoms have been associated with impaired mother-infant bonding at 6 months of age10 and decreased cognitive and fine motor development of children at 18 months.11
Importance of screening
Evidence from the literature shows that, without proper screening, approximately 50% of cases of PPD go undiagnosed, and that increasing the number of women being screened by perinatal providers is an important first step to improving outcomes.12-18 Current recommendations for the timing and frequency of screening for PPD vary among the published guidelines. ACOG recommends screening at least once during the perinatal period for depression and anxiety using a standardized, validated tool; an update of the ACOG committee opinion in 2018 also states: “It is recommended that all obstetrician-gynecologists and other obstetric care providers complete a full assessment of mood and emotional well-being (including screening for PPD and anxiety with a validated instrument) during the comprehensive postpartum visit for each patient.”19 The American Medical Association adopted new policies in 2017 promoting the implementation of a routine protocol for depression screening of perinatal women.20 The American Academy of Pediatrics recommends more frequent screening, with assessments at the 1-, 2-, 4-, and 6-month visits.21 Finally, the U.S. Preventive Services Task Force recommends screening for depression in the general population including pregnant and postpartum women.22
Multiple standardized, validated screening instruments are available for detecting possible symptoms of PPD, including the most widely used tools: the Edinburgh Postnatal Depression Scale (EPDS)19,23 and the Patient Health Questionnaire (PHQ-9).24 Two recent studies have shown that screening women for symptoms of PPD with a validated tool may reduce the duration or severity of depressive symptoms,25,26 further reinforcing the need to ensure that women experiencing symptoms of PPD are identified and treated early.
The inpatient hospitalization for labor, delivery, and birth of a child has not traditionally been viewed as an opportunity for PPD screening. While private practitioners and obstetric medical group practices typically have inquired about and documented the individual patient’s mental health history and risk factors for PPD, the obstetric hospitalist is most commonly meeting a patient in labor or in a postpartum encounter for the first time. As obstetric practices grow ever more consolidated, and as obstetric hospitalist care is implemented for a variety of reasons including, but not limited to, preventing burnout among private practitioners, serving as a safety net for all inpatient obstetric services, and increasing standardization in obstetric triage and obstetric emergency departments,
Barriers remain
Despite the need for early detection of PPD, screening practices remain inconsistent. A literature review of health care provider practices showed only one in four physicians reported using screening tools; obstetrician-gynecologists were most likely (36%) to use screening tools, followed by family practitioners (31%), with pediatricians the least likely (7%).27 This low rate is at least partially the result of perceived barriers to screening among health care providers, which contributes to underdiagnosis. A survey of more than 200 physicians who were members of ACOG showed that the top three barriers restricting screening practices were time constraints, inadequate training, and a lack of knowledge of the diagnostic criteria.28
Since 2017, Dignity Health has instituted routine screening of all inpatient postpartum patients at its 29 birth centers in Arizona, California, and Nevada. In this program, of which I am a physician participant, more than 30,000 women have been screened with the EPDS. In addition to providing screening, Dignity Health staff (physicians, certified nurse midwives, nurse practitioners, registered nurses, social workers, mental health therapists, lactation consultants, health educators, and others) have received in-person Perinatal Mental Health training. In this way, the entire care team coordinates inpatient screening and referral to outpatient care providers – thus bridging the gap in postpartum mental health care. For those patients who screen positive while an inpatient, a psychiatric telemedicine appointment is provided and, if necessary, short-course medications can be prescribed until the patient has outpatient follow-up and continuity of care. While we as obstetric hospitalists and community obstetrician-gynecologists recognize that inpatient postpartum screening may be limited in its sensitivity for capturing all women who will go on to develop PPD, there is definitely a benefit to having a discussion about PPD and maternal mental health early and often throughout the postpartum period. For many women suffering in silence, a 6-week postpartum outpatient visit is too late, especially given that approximately one-third of women are lost to postpartum follow-up.29,30

Addressing barriers
A growing number of states have enacted policies to address the challenge of peripartum behavioral health needs, and several states – Illinois, Massachusetts, New Jersey, and West Virginia – now mandate routine PPD screening by health care providers.31 However, few of these laws or policies contain specific guidance, such as the optimal timing for screening, instead leaving the details to providers.32 The proper identification and management of PPD cannot be achieved by state-level policy mandates alone, but must include clinician buy-in and participation.
Obstetricians play an essential role in the identification and treatment of PPD. Among nonpsychiatric specialists, obstetrician-gynecologists are the most likely providers to see and screen during the perinatal period.33 In addition, women prefer to receive help for PPD from either their obstetric practitioners or a mental-health specialists located at the obstetric clinic, and are more likely to receive mental-health services if they are provided at the same location as that of the obstetric provider.34,35 According to ACOG’s new guidance on the fourth trimester, obstetricians are encouraged to take responsibility for women’s care immediately after birth, and this care would include contact with all mothers within the first 3 weeks post partum, at follow-up visits as needed, and for a comprehensive postpartum visit at 12 weeks.3
Our specialty has and will continue to evolve, and obstetric hospitalists will play an ever more essential role in the care of women during their inpatient obstetric admission. Whether we are a patient’s primary inpatient obstetric provider or a practice extender for single or multigroup practice, we are in a unique role to screen, begin treatment for, and offer anticipatory guidance for maternal mental health and postpartum depression disorders. Obstetric hospitalists can be a bridge between inpatient and outpatient follow-up and catalysts for implementing universal inpatient PPD screening. Our role presents an opportunity to start the discussion early and often in the fourth trimester and to make a significant difference in addressing this critical unmet need in postnatal care.
Dr. van Dis is the medical director of the Ob Hospitalist Group in Burbank, Calif. She disclosed she received editorial assistance from Erik MacLaren, PhD, of Boston Strategic Partners Inc., with funding support from Sage Therapeutics Inc. E-mail obnews@mdedge.com.
References
1. Centers for Disease Control and Prevention. Postpartum Depression. 2017.
2. Morb Mortal Wkly Rep. 2017;66(6):153-8.
3. Obstet Gynecol. 2018;131(5):e140-e150.
4. Harv Rev Psychiatry. 2014;22(1):1-22.
5. JAMA Psychiatry. 2018;75(3):247-53.
6. J Womens Health (Larchmt). 2016;25(12):1219-24.
7. J Psychiatr Res. 2017;84:284-91.
8. Br J Psychiatry. 2003;183:279-81.
9. Obstet Gynecol Surv. 2005;60(3):183-90.
10. Arch Womens Ment Health. 2016;19(1):87-94.
11. Soc Psychiatry Psychiatr Epidemiol. 2013;48(8):1335-45.
12. J Reprod Med. 1999;44(4):351-8.
13. J Behav Health Serv Res. 2004;31(2):117-33.
14. J Clin Psychiatry. 2016;77(9):1189-200.
15. Am J Obstet Gynecol. 2000;182(5):1080-2.
16. J Fam Pract. 2001;50(2):117-22.
17. Obstet Gynecol. 1999;93(5 Pt 1):653-7.
18. J Womens Health (Larchmt). 2010;19(3):477-90.
19. Obstet Gynecol. 2018;132:e208-12.
20. “Physicians back programs to address maternal mortality, depression,” AMA, Nov. 15, 2017
21. Pediatrics. 2019 Jan 1;143(1):e20183260.
22. JAMA. 2016;315(4):380-7.
23. Br J Psychiatry. 1987;150:782-6.
24. Ann Fam Med. 2009;7(1):63-70.
25. Obstet Gynecol. 2016;127(5):917-25.
26. Pediatrics. 2017 Oct;140(4). pii: e20170110.
27. Womens Health Issues. 2015;25(6):703-10.
28. J Psychosom Obstet Gynaecol. 2011;32(1):27-34.
29. Matern Child Health J. 2016;20(Suppl 1):22-7.
30. National Committee for Quality Assurance. Prenatal and Postpartum Care (PPC). 2018.
31. Psychiatr Serv. 2015;66(3):324-8.
32. Postpartum Support International. Legislation. 2018.
33. American Academy of Pediatrics, American College of Obstetricians and Gynecologists, eds. Guidelines for Perinatal Care. 7th ed. (Elk Grove Village, IL: Washington, DC: American Academy of Pediatrics; American College of Obstetricians and Gynecologists; Oct 2012.)
34. Birth. 2009;36(1):60-9.
35. Gen Hosp Psychiatry. 2009;31(2):155-62.
Postpartum depression (PPD) is the most common complication of pregnancy, and onset can occur at any time from pregnancy until up to 1 year post partum.1,2 The immediate postpartum period is a time during which care is shared among multiple providers for both mother and child, and the transition from inpatient to outpatient postpartum care can impede communication between those caring for the patient in each setting. In 2018, the American College of Obstetricians and Gynecologists published a committee opinion emphasizing the importance of the “fourth trimester” and calling for health care providers to assist women in navigating the transition from pre- to postpartum care.3 An important consideration of perinatal care is mental health care for the mother, including screening and care for postpartum depression; however, the optimal role for the obstetric hospitalist in providing such services has been unclear.
Estimates of the prevalence of PPD in new mothers in the United States varied by state from 8% to 20% in 2012, with an overall average of 12%.2 Left untreated, PPD may result in significant negative outcomes for women, their children, and families. The depressive symptoms of PPD may persist for months or years afterward,4 with one study finding elevated depressive symptoms in women up to 11 years post partum.5 Suicide is also a leading cause of pregnancy-related mortality associated with depressive symptoms.6-9 In addition, maternal postpartum depression symptoms have been associated with impaired mother-infant bonding at 6 months of age10 and decreased cognitive and fine motor development of children at 18 months.11
Importance of screening
Evidence from the literature shows that, without proper screening, approximately 50% of cases of PPD go undiagnosed, and that increasing the number of women being screened by perinatal providers is an important first step to improving outcomes.12-18 Current recommendations for the timing and frequency of screening for PPD vary among the published guidelines. ACOG recommends screening at least once during the perinatal period for depression and anxiety using a standardized, validated tool; an update of the ACOG committee opinion in 2018 also states: “It is recommended that all obstetrician-gynecologists and other obstetric care providers complete a full assessment of mood and emotional well-being (including screening for PPD and anxiety with a validated instrument) during the comprehensive postpartum visit for each patient.”19 The American Medical Association adopted new policies in 2017 promoting the implementation of a routine protocol for depression screening of perinatal women.20 The American Academy of Pediatrics recommends more frequent screening, with assessments at the 1-, 2-, 4-, and 6-month visits.21 Finally, the U.S. Preventive Services Task Force recommends screening for depression in the general population including pregnant and postpartum women.22
Multiple standardized, validated screening instruments are available for detecting possible symptoms of PPD, including the most widely used tools: the Edinburgh Postnatal Depression Scale (EPDS)19,23 and the Patient Health Questionnaire (PHQ-9).24 Two recent studies have shown that screening women for symptoms of PPD with a validated tool may reduce the duration or severity of depressive symptoms,25,26 further reinforcing the need to ensure that women experiencing symptoms of PPD are identified and treated early.
The inpatient hospitalization for labor, delivery, and birth of a child has not traditionally been viewed as an opportunity for PPD screening. While private practitioners and obstetric medical group practices typically have inquired about and documented the individual patient’s mental health history and risk factors for PPD, the obstetric hospitalist is most commonly meeting a patient in labor or in a postpartum encounter for the first time. As obstetric practices grow ever more consolidated, and as obstetric hospitalist care is implemented for a variety of reasons including, but not limited to, preventing burnout among private practitioners, serving as a safety net for all inpatient obstetric services, and increasing standardization in obstetric triage and obstetric emergency departments,
Barriers remain
Despite the need for early detection of PPD, screening practices remain inconsistent. A literature review of health care provider practices showed only one in four physicians reported using screening tools; obstetrician-gynecologists were most likely (36%) to use screening tools, followed by family practitioners (31%), with pediatricians the least likely (7%).27 This low rate is at least partially the result of perceived barriers to screening among health care providers, which contributes to underdiagnosis. A survey of more than 200 physicians who were members of ACOG showed that the top three barriers restricting screening practices were time constraints, inadequate training, and a lack of knowledge of the diagnostic criteria.28
Since 2017, Dignity Health has instituted routine screening of all inpatient postpartum patients at its 29 birth centers in Arizona, California, and Nevada. In this program, of which I am a physician participant, more than 30,000 women have been screened with the EPDS. In addition to providing screening, Dignity Health staff (physicians, certified nurse midwives, nurse practitioners, registered nurses, social workers, mental health therapists, lactation consultants, health educators, and others) have received in-person Perinatal Mental Health training. In this way, the entire care team coordinates inpatient screening and referral to outpatient care providers – thus bridging the gap in postpartum mental health care. For those patients who screen positive while an inpatient, a psychiatric telemedicine appointment is provided and, if necessary, short-course medications can be prescribed until the patient has outpatient follow-up and continuity of care. While we as obstetric hospitalists and community obstetrician-gynecologists recognize that inpatient postpartum screening may be limited in its sensitivity for capturing all women who will go on to develop PPD, there is definitely a benefit to having a discussion about PPD and maternal mental health early and often throughout the postpartum period. For many women suffering in silence, a 6-week postpartum outpatient visit is too late, especially given that approximately one-third of women are lost to postpartum follow-up.29,30
Addressing barriers
A growing number of states have enacted policies to address the challenge of peripartum behavioral health needs, and several states – Illinois, Massachusetts, New Jersey, and West Virginia – now mandate routine PPD screening by health care providers.31 However, few of these laws or policies contain specific guidance, such as the optimal timing for screening, instead leaving the details to providers.32 The proper identification and management of PPD cannot be achieved by state-level policy mandates alone, but must include clinician buy-in and participation.
Obstetricians play an essential role in the identification and treatment of PPD. Among nonpsychiatric specialists, obstetrician-gynecologists are the most likely providers to see and screen during the perinatal period.33 In addition, women prefer to receive help for PPD from either their obstetric practitioners or a mental-health specialists located at the obstetric clinic, and are more likely to receive mental-health services if they are provided at the same location as that of the obstetric provider.34,35 According to ACOG’s new guidance on the fourth trimester, obstetricians are encouraged to take responsibility for women’s care immediately after birth, and this care would include contact with all mothers within the first 3 weeks post partum, at follow-up visits as needed, and for a comprehensive postpartum visit at 12 weeks.3
Our specialty has and will continue to evolve, and obstetric hospitalists will play an ever more essential role in the care of women during their inpatient obstetric admission. Whether we are a patient’s primary inpatient obstetric provider or a practice extender for single or multigroup practice, we are in a unique role to screen, begin treatment for, and offer anticipatory guidance for maternal mental health and postpartum depression disorders. Obstetric hospitalists can be a bridge between inpatient and outpatient follow-up and catalysts for implementing universal inpatient PPD screening. Our role presents an opportunity to start the discussion early and often in the fourth trimester and to make a significant difference in addressing this critical unmet need in postnatal care.
Dr. van Dis is the medical director of the Ob Hospitalist Group in Burbank, Calif. She disclosed she received editorial assistance from Erik MacLaren, PhD, of Boston Strategic Partners Inc., with funding support from Sage Therapeutics Inc. E-mail obnews@mdedge.com.
References
1. Centers for Disease Control and Prevention. Postpartum Depression. 2017.
2. Morb Mortal Wkly Rep. 2017;66(6):153-8.
3. Obstet Gynecol. 2018;131(5):e140-e150.
4. Harv Rev Psychiatry. 2014;22(1):1-22.
5. JAMA Psychiatry. 2018;75(3):247-53.
6. J Womens Health (Larchmt). 2016;25(12):1219-24.
7. J Psychiatr Res. 2017;84:284-91.
8. Br J Psychiatry. 2003;183:279-81.
9. Obstet Gynecol Surv. 2005;60(3):183-90.
10. Arch Womens Ment Health. 2016;19(1):87-94.
11. Soc Psychiatry Psychiatr Epidemiol. 2013;48(8):1335-45.
12. J Reprod Med. 1999;44(4):351-8.
13. J Behav Health Serv Res. 2004;31(2):117-33.
14. J Clin Psychiatry. 2016;77(9):1189-200.
15. Am J Obstet Gynecol. 2000;182(5):1080-2.
16. J Fam Pract. 2001;50(2):117-22.
17. Obstet Gynecol. 1999;93(5 Pt 1):653-7.
18. J Womens Health (Larchmt). 2010;19(3):477-90.
19. Obstet Gynecol. 2018;132:e208-12.
20. “Physicians back programs to address maternal mortality, depression,” AMA, Nov. 15, 2017
21. Pediatrics. 2019 Jan 1;143(1):e20183260.
22. JAMA. 2016;315(4):380-7.
23. Br J Psychiatry. 1987;150:782-6.
24. Ann Fam Med. 2009;7(1):63-70.
25. Obstet Gynecol. 2016;127(5):917-25.
26. Pediatrics. 2017 Oct;140(4). pii: e20170110.
27. Womens Health Issues. 2015;25(6):703-10.
28. J Psychosom Obstet Gynaecol. 2011;32(1):27-34.
29. Matern Child Health J. 2016;20(Suppl 1):22-7.
30. National Committee for Quality Assurance. Prenatal and Postpartum Care (PPC). 2018.
31. Psychiatr Serv. 2015;66(3):324-8.
32. Postpartum Support International. Legislation. 2018.
33. American Academy of Pediatrics, American College of Obstetricians and Gynecologists, eds. Guidelines for Perinatal Care. 7th ed. (Elk Grove Village, IL: Washington, DC: American Academy of Pediatrics; American College of Obstetricians and Gynecologists; Oct 2012.)
34. Birth. 2009;36(1):60-9.
35. Gen Hosp Psychiatry. 2009;31(2):155-62.
Postpartum depression (PPD) is the most common complication of pregnancy, and onset can occur at any time from pregnancy until up to 1 year post partum.1,2 The immediate postpartum period is a time during which care is shared among multiple providers for both mother and child, and the transition from inpatient to outpatient postpartum care can impede communication between those caring for the patient in each setting. In 2018, the American College of Obstetricians and Gynecologists published a committee opinion emphasizing the importance of the “fourth trimester” and calling for health care providers to assist women in navigating the transition from pre- to postpartum care.3 An important consideration of perinatal care is mental health care for the mother, including screening and care for postpartum depression; however, the optimal role for the obstetric hospitalist in providing such services has been unclear.
Estimates of the prevalence of PPD in new mothers in the United States varied by state from 8% to 20% in 2012, with an overall average of 12%.2 Left untreated, PPD may result in significant negative outcomes for women, their children, and families. The depressive symptoms of PPD may persist for months or years afterward,4 with one study finding elevated depressive symptoms in women up to 11 years post partum.5 Suicide is also a leading cause of pregnancy-related mortality associated with depressive symptoms.6-9 In addition, maternal postpartum depression symptoms have been associated with impaired mother-infant bonding at 6 months of age10 and decreased cognitive and fine motor development of children at 18 months.11
Importance of screening
Evidence from the literature shows that, without proper screening, approximately 50% of cases of PPD go undiagnosed, and that increasing the number of women being screened by perinatal providers is an important first step to improving outcomes.12-18 Current recommendations for the timing and frequency of screening for PPD vary among the published guidelines. ACOG recommends screening at least once during the perinatal period for depression and anxiety using a standardized, validated tool; an update of the ACOG committee opinion in 2018 also states: “It is recommended that all obstetrician-gynecologists and other obstetric care providers complete a full assessment of mood and emotional well-being (including screening for PPD and anxiety with a validated instrument) during the comprehensive postpartum visit for each patient.”19 The American Medical Association adopted new policies in 2017 promoting the implementation of a routine protocol for depression screening of perinatal women.20 The American Academy of Pediatrics recommends more frequent screening, with assessments at the 1-, 2-, 4-, and 6-month visits.21 Finally, the U.S. Preventive Services Task Force recommends screening for depression in the general population including pregnant and postpartum women.22
Multiple standardized, validated screening instruments are available for detecting possible symptoms of PPD, including the most widely used tools: the Edinburgh Postnatal Depression Scale (EPDS)19,23 and the Patient Health Questionnaire (PHQ-9).24 Two recent studies have shown that screening women for symptoms of PPD with a validated tool may reduce the duration or severity of depressive symptoms,25,26 further reinforcing the need to ensure that women experiencing symptoms of PPD are identified and treated early.
The inpatient hospitalization for labor, delivery, and birth of a child has not traditionally been viewed as an opportunity for PPD screening. While private practitioners and obstetric medical group practices typically have inquired about and documented the individual patient’s mental health history and risk factors for PPD, the obstetric hospitalist is most commonly meeting a patient in labor or in a postpartum encounter for the first time. As obstetric practices grow ever more consolidated, and as obstetric hospitalist care is implemented for a variety of reasons including, but not limited to, preventing burnout among private practitioners, serving as a safety net for all inpatient obstetric services, and increasing standardization in obstetric triage and obstetric emergency departments,
Barriers remain
Despite the need for early detection of PPD, screening practices remain inconsistent. A literature review of health care provider practices showed only one in four physicians reported using screening tools; obstetrician-gynecologists were most likely (36%) to use screening tools, followed by family practitioners (31%), with pediatricians the least likely (7%).27 This low rate is at least partially the result of perceived barriers to screening among health care providers, which contributes to underdiagnosis. A survey of more than 200 physicians who were members of ACOG showed that the top three barriers restricting screening practices were time constraints, inadequate training, and a lack of knowledge of the diagnostic criteria.28
Since 2017, Dignity Health has instituted routine screening of all inpatient postpartum patients at its 29 birth centers in Arizona, California, and Nevada. In this program, of which I am a physician participant, more than 30,000 women have been screened with the EPDS. In addition to providing screening, Dignity Health staff (physicians, certified nurse midwives, nurse practitioners, registered nurses, social workers, mental health therapists, lactation consultants, health educators, and others) have received in-person Perinatal Mental Health training. In this way, the entire care team coordinates inpatient screening and referral to outpatient care providers – thus bridging the gap in postpartum mental health care. For those patients who screen positive while an inpatient, a psychiatric telemedicine appointment is provided and, if necessary, short-course medications can be prescribed until the patient has outpatient follow-up and continuity of care. While we as obstetric hospitalists and community obstetrician-gynecologists recognize that inpatient postpartum screening may be limited in its sensitivity for capturing all women who will go on to develop PPD, there is definitely a benefit to having a discussion about PPD and maternal mental health early and often throughout the postpartum period. For many women suffering in silence, a 6-week postpartum outpatient visit is too late, especially given that approximately one-third of women are lost to postpartum follow-up.29,30
Addressing barriers
A growing number of states have enacted policies to address the challenge of peripartum behavioral health needs, and several states – Illinois, Massachusetts, New Jersey, and West Virginia – now mandate routine PPD screening by health care providers.31 However, few of these laws or policies contain specific guidance, such as the optimal timing for screening, instead leaving the details to providers.32 The proper identification and management of PPD cannot be achieved by state-level policy mandates alone, but must include clinician buy-in and participation.
Obstetricians play an essential role in the identification and treatment of PPD. Among nonpsychiatric specialists, obstetrician-gynecologists are the most likely providers to see and screen during the perinatal period.33 In addition, women prefer to receive help for PPD from either their obstetric practitioners or a mental-health specialists located at the obstetric clinic, and are more likely to receive mental-health services if they are provided at the same location as that of the obstetric provider.34,35 According to ACOG’s new guidance on the fourth trimester, obstetricians are encouraged to take responsibility for women’s care immediately after birth, and this care would include contact with all mothers within the first 3 weeks post partum, at follow-up visits as needed, and for a comprehensive postpartum visit at 12 weeks.3
Our specialty has and will continue to evolve, and obstetric hospitalists will play an ever more essential role in the care of women during their inpatient obstetric admission. Whether we are a patient’s primary inpatient obstetric provider or a practice extender for single or multigroup practice, we are in a unique role to screen, begin treatment for, and offer anticipatory guidance for maternal mental health and postpartum depression disorders. Obstetric hospitalists can be a bridge between inpatient and outpatient follow-up and catalysts for implementing universal inpatient PPD screening. Our role presents an opportunity to start the discussion early and often in the fourth trimester and to make a significant difference in addressing this critical unmet need in postnatal care.
Dr. van Dis is the medical director of the Ob Hospitalist Group in Burbank, Calif. She disclosed she received editorial assistance from Erik MacLaren, PhD, of Boston Strategic Partners Inc., with funding support from Sage Therapeutics Inc. E-mail obnews@mdedge.com.
References
1. Centers for Disease Control and Prevention. Postpartum Depression. 2017.
2. Morb Mortal Wkly Rep. 2017;66(6):153-8.
3. Obstet Gynecol. 2018;131(5):e140-e150.
4. Harv Rev Psychiatry. 2014;22(1):1-22.
5. JAMA Psychiatry. 2018;75(3):247-53.
6. J Womens Health (Larchmt). 2016;25(12):1219-24.
7. J Psychiatr Res. 2017;84:284-91.
8. Br J Psychiatry. 2003;183:279-81.
9. Obstet Gynecol Surv. 2005;60(3):183-90.
10. Arch Womens Ment Health. 2016;19(1):87-94.
11. Soc Psychiatry Psychiatr Epidemiol. 2013;48(8):1335-45.
12. J Reprod Med. 1999;44(4):351-8.
13. J Behav Health Serv Res. 2004;31(2):117-33.
14. J Clin Psychiatry. 2016;77(9):1189-200.
15. Am J Obstet Gynecol. 2000;182(5):1080-2.
16. J Fam Pract. 2001;50(2):117-22.
17. Obstet Gynecol. 1999;93(5 Pt 1):653-7.
18. J Womens Health (Larchmt). 2010;19(3):477-90.
19. Obstet Gynecol. 2018;132:e208-12.
20. “Physicians back programs to address maternal mortality, depression,” AMA, Nov. 15, 2017
21. Pediatrics. 2019 Jan 1;143(1):e20183260.
22. JAMA. 2016;315(4):380-7.
23. Br J Psychiatry. 1987;150:782-6.
24. Ann Fam Med. 2009;7(1):63-70.
25. Obstet Gynecol. 2016;127(5):917-25.
26. Pediatrics. 2017 Oct;140(4). pii: e20170110.
27. Womens Health Issues. 2015;25(6):703-10.
28. J Psychosom Obstet Gynaecol. 2011;32(1):27-34.
29. Matern Child Health J. 2016;20(Suppl 1):22-7.
30. National Committee for Quality Assurance. Prenatal and Postpartum Care (PPC). 2018.
31. Psychiatr Serv. 2015;66(3):324-8.
32. Postpartum Support International. Legislation. 2018.
33. American Academy of Pediatrics, American College of Obstetricians and Gynecologists, eds. Guidelines for Perinatal Care. 7th ed. (Elk Grove Village, IL: Washington, DC: American Academy of Pediatrics; American College of Obstetricians and Gynecologists; Oct 2012.)
34. Birth. 2009;36(1):60-9.
35. Gen Hosp Psychiatry. 2009;31(2):155-62.

Asthma, obesity, and the risk for severe sleep apnea in children
CORONADO, CALIF. –

“We have a good idea that obesity and asthma independently increase the risk of OSA, but a lot of the time in the pediatric population, these risk factors are found comorbid,” Ajay Narayanan at the Triological Society’s Combined Sections Meeting. “For this study we asked, how does the presence of asthma change the likelihood of having severe OSA in a cohort of obese patients? Knowing that both asthma and obesity independently increase the risk for OSA, we hypothesized that when they were comorbid, asthma would have a synergistic effect with obesity, causing severe OSA.”
Mr. Narayanan, a third-year student at the University of Texas Southwestern Medical Center, Dallas, and his colleagues performed a retrospective chart review of 367 children aged 9-17 years referred for a full-night polysomnography (PSG) for suspicion of having OSA. Demographic variables recorded included race, body mass index, rhinitis, gastroesophageal reflux disease, and tonsillar hypertrophy. Sleep variables recorded included apnea hypopnea index (AHI), sleep efficiency, rapid eye movement, and the peripheral capillary oxygen saturation (SpO2) nadir. The primary outcome was severe OSA defined as an AHI of 10 or greater on the PSG. They used logistic modeling to determine the association between asthma, obesity, and severe OSA.
The mean age of the study population was 14 years, 56% were male, and 43% were Hispanic. Of the 367 patients, 77 were neither obese nor asthmatic, 93 were nonobese but were asthmatic, 102 were obese but were nonasthmatic, and 95 were both obese and asthmatic. PSG results confirmed that obesity was associated with more signs of sleep apnea. For example, the nonobese, nonasthmatic group had a mean AHI of 11 events per hour, while the obese, nonasthmatic group had a mean AHI of 19 events per hour. “We observed a similar trend amongst our asthmatic population,” Mr. Narayanan said. “We observed an increase in the mean AHI amongst our asthmatic kids when we added obesity to the picture. Surprisingly, we found that asthma was associated with having fewer signs of sleep apnea.” Specifically, while the nonobese, nonasthmatic group had a mean AHI of 11 events per hour, those in the nonobese, asthmatic group had a mean of 5.6 events per hour (P = .005). “The finding was similar amongst our obese kids,” he said. “We saw a decrease in the mean AHI of our obese kids when we added asthma to the picture.”
On logistic regression analysis using obesity and asthma as independent variables, the researchers found that obesity increased the risk of severe OSA by 2.4-fold, but asthma decreased the odds of having severe OSA by about half (0.55). On multiple logistic regression controlling for commonly associated factors such as tonsillar hypertrophy, black race, and Hispanic ethnicity, obesity increased the risk of severe OSA by 2.2-fold, while asthma decreased the odds of having severe OSA by about half (0.51).
“In trying to explain this finding, we can turn to how these diseases are treated,” Mr. Narayanan said. “I say this because of the proven association between preexisting asthma and new onset OSA. Some of the reasons for this association include the tendency for airway collapsibility and systemwide inflammation seen in asthma, which then might contribute to the development of OSA. If we treat asthma symptoms early on, it might prevent the progression to sleep apnea down the line.”
Considering how prevalent comorbid asthma and OSA is, he continued, “we need to confirm that it is in fact well-controlled asthma that is associated with lowering the risk of severe OSA. Once we do this, we can ask the question: Can we use asthma pharmacotherapy to treat OSA? Some studies have shown that inhaled corticosteroids and montelukast (Singulair) may be effective treatment options for kids with OSA, but there’s definitely room for more research in this field, [such as determining] which patients would most benefit from this pharmacotherapy.” The researchers reported having no financial disclosures.
SOURCE: Narayanan A et al. Triological CSM, Abstracts.
CORONADO, CALIF. –
“We have a good idea that obesity and asthma independently increase the risk of OSA, but a lot of the time in the pediatric population, these risk factors are found comorbid,” Ajay Narayanan at the Triological Society’s Combined Sections Meeting. “For this study we asked, how does the presence of asthma change the likelihood of having severe OSA in a cohort of obese patients? Knowing that both asthma and obesity independently increase the risk for OSA, we hypothesized that when they were comorbid, asthma would have a synergistic effect with obesity, causing severe OSA.”
Mr. Narayanan, a third-year student at the University of Texas Southwestern Medical Center, Dallas, and his colleagues performed a retrospective chart review of 367 children aged 9-17 years referred for a full-night polysomnography (PSG) for suspicion of having OSA. Demographic variables recorded included race, body mass index, rhinitis, gastroesophageal reflux disease, and tonsillar hypertrophy. Sleep variables recorded included apnea hypopnea index (AHI), sleep efficiency, rapid eye movement, and the peripheral capillary oxygen saturation (SpO2) nadir. The primary outcome was severe OSA defined as an AHI of 10 or greater on the PSG. They used logistic modeling to determine the association between asthma, obesity, and severe OSA.
The mean age of the study population was 14 years, 56% were male, and 43% were Hispanic. Of the 367 patients, 77 were neither obese nor asthmatic, 93 were nonobese but were asthmatic, 102 were obese but were nonasthmatic, and 95 were both obese and asthmatic. PSG results confirmed that obesity was associated with more signs of sleep apnea. For example, the nonobese, nonasthmatic group had a mean AHI of 11 events per hour, while the obese, nonasthmatic group had a mean AHI of 19 events per hour. “We observed a similar trend amongst our asthmatic population,” Mr. Narayanan said. “We observed an increase in the mean AHI amongst our asthmatic kids when we added obesity to the picture. Surprisingly, we found that asthma was associated with having fewer signs of sleep apnea.” Specifically, while the nonobese, nonasthmatic group had a mean AHI of 11 events per hour, those in the nonobese, asthmatic group had a mean of 5.6 events per hour (P = .005). “The finding was similar amongst our obese kids,” he said. “We saw a decrease in the mean AHI of our obese kids when we added asthma to the picture.”
On logistic regression analysis using obesity and asthma as independent variables, the researchers found that obesity increased the risk of severe OSA by 2.4-fold, but asthma decreased the odds of having severe OSA by about half (0.55). On multiple logistic regression controlling for commonly associated factors such as tonsillar hypertrophy, black race, and Hispanic ethnicity, obesity increased the risk of severe OSA by 2.2-fold, while asthma decreased the odds of having severe OSA by about half (0.51).
“In trying to explain this finding, we can turn to how these diseases are treated,” Mr. Narayanan said. “I say this because of the proven association between preexisting asthma and new onset OSA. Some of the reasons for this association include the tendency for airway collapsibility and systemwide inflammation seen in asthma, which then might contribute to the development of OSA. If we treat asthma symptoms early on, it might prevent the progression to sleep apnea down the line.”
Considering how prevalent comorbid asthma and OSA is, he continued, “we need to confirm that it is in fact well-controlled asthma that is associated with lowering the risk of severe OSA. Once we do this, we can ask the question: Can we use asthma pharmacotherapy to treat OSA? Some studies have shown that inhaled corticosteroids and montelukast (Singulair) may be effective treatment options for kids with OSA, but there’s definitely room for more research in this field, [such as determining] which patients would most benefit from this pharmacotherapy.” The researchers reported having no financial disclosures.
SOURCE: Narayanan A et al. Triological CSM, Abstracts.
CORONADO, CALIF. –
“We have a good idea that obesity and asthma independently increase the risk of OSA, but a lot of the time in the pediatric population, these risk factors are found comorbid,” Ajay Narayanan at the Triological Society’s Combined Sections Meeting. “For this study we asked, how does the presence of asthma change the likelihood of having severe OSA in a cohort of obese patients? Knowing that both asthma and obesity independently increase the risk for OSA, we hypothesized that when they were comorbid, asthma would have a synergistic effect with obesity, causing severe OSA.”
Mr. Narayanan, a third-year student at the University of Texas Southwestern Medical Center, Dallas, and his colleagues performed a retrospective chart review of 367 children aged 9-17 years referred for a full-night polysomnography (PSG) for suspicion of having OSA. Demographic variables recorded included race, body mass index, rhinitis, gastroesophageal reflux disease, and tonsillar hypertrophy. Sleep variables recorded included apnea hypopnea index (AHI), sleep efficiency, rapid eye movement, and the peripheral capillary oxygen saturation (SpO2) nadir. The primary outcome was severe OSA defined as an AHI of 10 or greater on the PSG. They used logistic modeling to determine the association between asthma, obesity, and severe OSA.
The mean age of the study population was 14 years, 56% were male, and 43% were Hispanic. Of the 367 patients, 77 were neither obese nor asthmatic, 93 were nonobese but were asthmatic, 102 were obese but were nonasthmatic, and 95 were both obese and asthmatic. PSG results confirmed that obesity was associated with more signs of sleep apnea. For example, the nonobese, nonasthmatic group had a mean AHI of 11 events per hour, while the obese, nonasthmatic group had a mean AHI of 19 events per hour. “We observed a similar trend amongst our asthmatic population,” Mr. Narayanan said. “We observed an increase in the mean AHI amongst our asthmatic kids when we added obesity to the picture. Surprisingly, we found that asthma was associated with having fewer signs of sleep apnea.” Specifically, while the nonobese, nonasthmatic group had a mean AHI of 11 events per hour, those in the nonobese, asthmatic group had a mean of 5.6 events per hour (P = .005). “The finding was similar amongst our obese kids,” he said. “We saw a decrease in the mean AHI of our obese kids when we added asthma to the picture.”
On logistic regression analysis using obesity and asthma as independent variables, the researchers found that obesity increased the risk of severe OSA by 2.4-fold, but asthma decreased the odds of having severe OSA by about half (0.55). On multiple logistic regression controlling for commonly associated factors such as tonsillar hypertrophy, black race, and Hispanic ethnicity, obesity increased the risk of severe OSA by 2.2-fold, while asthma decreased the odds of having severe OSA by about half (0.51).
“In trying to explain this finding, we can turn to how these diseases are treated,” Mr. Narayanan said. “I say this because of the proven association between preexisting asthma and new onset OSA. Some of the reasons for this association include the tendency for airway collapsibility and systemwide inflammation seen in asthma, which then might contribute to the development of OSA. If we treat asthma symptoms early on, it might prevent the progression to sleep apnea down the line.”
Considering how prevalent comorbid asthma and OSA is, he continued, “we need to confirm that it is in fact well-controlled asthma that is associated with lowering the risk of severe OSA. Once we do this, we can ask the question: Can we use asthma pharmacotherapy to treat OSA? Some studies have shown that inhaled corticosteroids and montelukast (Singulair) may be effective treatment options for kids with OSA, but there’s definitely room for more research in this field, [such as determining] which patients would most benefit from this pharmacotherapy.” The researchers reported having no financial disclosures.
SOURCE: Narayanan A et al. Triological CSM, Abstracts.
REPORTING FROM THE TRIOLOGICAL CSM
Key clinical point: In children, having asthma could decrease the risk of having severe obstructive sleep apnea, regardless of their obesity status.
Major finding: On multiple logistic regression, obesity increased the risk of severe OSA by 2.2-fold, while asthma decreased the odds of having severe OSA by about half.
Study details: A retrospective review of 367 children referred for a full-night polysomnography for suspicion of having OSA.
Disclosures: The researchers reported having no financial disclosures.
Source: Narayanan A et al. Triological CSM, Abstracts.
ADHD: When and how do we choose to start medications?
- A 9-year-old boy has poor impulse control, throws things in class, and cannot sit still. Teachers ask: Is this ADHD and should we start a medication?
- A 9-year-old girl is an inattentive daydreamer with poor class performance and trouble turning in homework. Her parents and teachers ask: Is this ADHD and should we start a medication?
- A 17-year-old boy who is a high achiever is taking the upcoming SATs and does poorly on timed tests because of poor focus and is now wondering: Do I have ADHD and would a medication help me perform better?
- A 17-year-old boy had poor grades for much of his early school years, but his parents always thought he was just a “lazy kid” although he insists he is trying his best. His parents now ask: Is this ADHD and has it been all along?
The above cases may sound familiar to you. They are an oversimplification of the patients who may come to you with two questions: Do I or someone I care about have ADHD and should they have medication for it? What may matter even more is how they are doing with that inattentiveness and how much it impacts their lives.
Sigmund Freud was known to think about goals for treatment as “liebe und arbeit” translated into “to love and to work.” As in, can someone live, love, and work or are their psychiatric symptoms impairing those functionalities? For a child, to live, work, and play (well with others) is most apt here. It is often more helpful to think in terms of childhood daily life when choosing to begin a medication or not. With inattention, a child can range from having a parent hoping for performance enhancement to having a severe impairment in their day-to-day functioning in a classroom. In the above case examples, each child or adolescent has varying impairments in performance – one is a high academic performer with very few issues outside of testing and another is a young child who can’t even sit still in a classroom to learn. Who should be prescribed a stimulant? Any or all of the above? It’s not as easy an answer as you may suspect, and there may not be one “right” answer either.
We know that stimulants can help a great deal of patients. They have the highest effect size for ADHD in that about 80% of children can benefit from stimulant treatment for ADHD. Specifically, “a high response rate of 70%-85% has been noted with methylphenidate and amphetamine formulations. The response rate is lower for atomoxetine [60%-65%] and guanfacine [30%-40%]” (Venkat B, Hechtman L. Considerations in selecting pharmacological treatments for attention deficit hyperactivity disorder. Clinical Pharmacist. 2016 Feb 11). In thinking about when to prescribe, we want to balance offering nonpharmacologic means to address symptoms of inattention (like mindfulness, exercise, and school supports such as individualized learning plans where applicable). We also do not want to withhold helpful treatments such as stimulants or other nonstimulant medications or trend toward overprescribing potentially habit-forming and imperfect medications.
It is important to make that distinction between impairment and the desire for medications to “enhance” life and optimize performance rather than treating symptoms of a disorder. It is most helpful to gain skills to navigate those challenges simultaneously to ultimately help our patients live, learn, love, and play to the best of their abilities.
Where to begin
When I was in training, I had difficulty teasing out the various ADHD stimulant formations. There were and are so many Ritalin preparations! Mostly there is a variation in shorter-acting to longer-acting effects. If the diagnosis is highly suspected and uncomplicated ADHD, I usually choose to start with Concerta 18 mg daily (a long-acting methylphenidate) for children aged over 6 years. Many times I don’t see the need to titrate that upwards much further toward the maximum clinically used dose of 54 mg daily (despite guidelines saying otherwise up to 72 mg daily, which I have found unnecessary usually and poorly tolerated). Concerta has an immediate effect (20%) and then slowly peaks until 12 p.m. (80%) and then is out of system by about 3 p.m. (for a total of 7 hours duration of action). There also are shorter-acting preparations (Ritalin, Methylin) which are “on/off” in 4 hours and use of these is more consistent with an antiquated way of prescribing, often up to twice daily and three times daily dosing schedules with the risk of the harder to tolerate “drop-off” effects with stimulants. And, if there is not an effect, I often reconsider the diagnosis and any co-occurring anxiety disorder, stressful life events, or depression or other illness with the knowledge that these medications so often are effective.
Anxiety + ADHD
If there is prominent anxiety, anxiety disorder, or tics, I often consider Strattera 10-20 mg daily up to around 40 mg. I tend to dose this lower than as written for tolerability and in a “dose low and go slow” approach with kids, which often results in better experiences with the medication. This medication also is recommended to be dosed by weight; this should be taken into account as well. Atomoxetine is a selective serotonin and norepinephrine reuptake inhibitor which is likely similar to Cymbalta (duloxetine). It may have a lower effect size of around less than 60% but this also is around the reported effect sizes for selective serotonin reuptake inhibitors (SSRIs) for depression. If a patient has both ADHD and an anxiety disorder, I often consider an SSRI alternatively first to manage attention issues associated with anxiety and then would add on a stimulant if attention issues persist once anxiety is better treated.
Second/third line ADHD treatments
As a second-line approach to long-acting Ritalin and if there is not a response to it, I would consider extended-release Adderall preparations such as Vyvanse, which is an amphetamine preparation supposedly less abusable than Adderall (one can’t snort it), but I also caution that it releases dopamine, peaks faster, and does not reduce to zero stimulant in 24 hours because of a variable half-life.

In this way, I always have imagined that these amphetamines may be more theoretically concerning than Ritalin/methylphenidate because they increase dopamine dumping into the synapse (which is a different and extra mechanism than just reuptake). For a third line, I may consider guanfacine depending on weight daily, which is an Food and Drug Administration–approved, nonstimulant alpha-2 agonist, which also acts longer than clonidine and may be better for hyperactivity symptoms. I may begin with doses as low as 0.25-0.5 mg in the evening for concerns with sedation or groggy aftereffects in the morning.
Throughout all treatment with medication, I emphasize the importance of assertively managing ADHD symptoms which may be in the form of “behavioral treatment,” like cognitive behavioral therapy, organizational coaching available at some educational centers, or even finding ways to train one’s focus with athletics or practices such as yoga and mindfulness. In addition to this combined approach to treatment, stimulants are not perfect medications. All stimulants have a “drop-off effect” and were made to work during a school day lasting from 8 a.m. to 3 p.m. Some patients and families complain about the drop-off effect and may want to “dose” around a medication more frequently, in the late afternoon and in the evening, which can lead to poor appetite at dinner and insomnia.
My answers to the cases above would be that all the patients could have ADHD, but they also may have anxiety or stress-related disorders, depression, worries about performance, or poor skills to manage inattention. They may not yet have received school supports, coaching, or found ways to manage these symptoms either. Because stimulants can improve and enhance performance but also have their own drawbacks and risks not covered here, it’s important to consider each case as a whole with thoughtfulness about a child’s unique ability to “live and work” in this world.
Dr. Pawlowski is an adult, adolescent, and child psychiatrist at the University of Vermont Medical Center and an assistant professor of psychiatry at UVM, both in Burlington. She reported no relevant financial disclosures. Email her at pdnews@mdedge.com.
- A 9-year-old boy has poor impulse control, throws things in class, and cannot sit still. Teachers ask: Is this ADHD and should we start a medication?
- A 9-year-old girl is an inattentive daydreamer with poor class performance and trouble turning in homework. Her parents and teachers ask: Is this ADHD and should we start a medication?
- A 17-year-old boy who is a high achiever is taking the upcoming SATs and does poorly on timed tests because of poor focus and is now wondering: Do I have ADHD and would a medication help me perform better?
- A 17-year-old boy had poor grades for much of his early school years, but his parents always thought he was just a “lazy kid” although he insists he is trying his best. His parents now ask: Is this ADHD and has it been all along?
The above cases may sound familiar to you. They are an oversimplification of the patients who may come to you with two questions: Do I or someone I care about have ADHD and should they have medication for it? What may matter even more is how they are doing with that inattentiveness and how much it impacts their lives.
Sigmund Freud was known to think about goals for treatment as “liebe und arbeit” translated into “to love and to work.” As in, can someone live, love, and work or are their psychiatric symptoms impairing those functionalities? For a child, to live, work, and play (well with others) is most apt here. It is often more helpful to think in terms of childhood daily life when choosing to begin a medication or not. With inattention, a child can range from having a parent hoping for performance enhancement to having a severe impairment in their day-to-day functioning in a classroom. In the above case examples, each child or adolescent has varying impairments in performance – one is a high academic performer with very few issues outside of testing and another is a young child who can’t even sit still in a classroom to learn. Who should be prescribed a stimulant? Any or all of the above? It’s not as easy an answer as you may suspect, and there may not be one “right” answer either.
We know that stimulants can help a great deal of patients. They have the highest effect size for ADHD in that about 80% of children can benefit from stimulant treatment for ADHD. Specifically, “a high response rate of 70%-85% has been noted with methylphenidate and amphetamine formulations. The response rate is lower for atomoxetine [60%-65%] and guanfacine [30%-40%]” (Venkat B, Hechtman L. Considerations in selecting pharmacological treatments for attention deficit hyperactivity disorder. Clinical Pharmacist. 2016 Feb 11). In thinking about when to prescribe, we want to balance offering nonpharmacologic means to address symptoms of inattention (like mindfulness, exercise, and school supports such as individualized learning plans where applicable). We also do not want to withhold helpful treatments such as stimulants or other nonstimulant medications or trend toward overprescribing potentially habit-forming and imperfect medications.
It is important to make that distinction between impairment and the desire for medications to “enhance” life and optimize performance rather than treating symptoms of a disorder. It is most helpful to gain skills to navigate those challenges simultaneously to ultimately help our patients live, learn, love, and play to the best of their abilities.
Where to begin
When I was in training, I had difficulty teasing out the various ADHD stimulant formations. There were and are so many Ritalin preparations! Mostly there is a variation in shorter-acting to longer-acting effects. If the diagnosis is highly suspected and uncomplicated ADHD, I usually choose to start with Concerta 18 mg daily (a long-acting methylphenidate) for children aged over 6 years. Many times I don’t see the need to titrate that upwards much further toward the maximum clinically used dose of 54 mg daily (despite guidelines saying otherwise up to 72 mg daily, which I have found unnecessary usually and poorly tolerated). Concerta has an immediate effect (20%) and then slowly peaks until 12 p.m. (80%) and then is out of system by about 3 p.m. (for a total of 7 hours duration of action). There also are shorter-acting preparations (Ritalin, Methylin) which are “on/off” in 4 hours and use of these is more consistent with an antiquated way of prescribing, often up to twice daily and three times daily dosing schedules with the risk of the harder to tolerate “drop-off” effects with stimulants. And, if there is not an effect, I often reconsider the diagnosis and any co-occurring anxiety disorder, stressful life events, or depression or other illness with the knowledge that these medications so often are effective.
Anxiety + ADHD
If there is prominent anxiety, anxiety disorder, or tics, I often consider Strattera 10-20 mg daily up to around 40 mg. I tend to dose this lower than as written for tolerability and in a “dose low and go slow” approach with kids, which often results in better experiences with the medication. This medication also is recommended to be dosed by weight; this should be taken into account as well. Atomoxetine is a selective serotonin and norepinephrine reuptake inhibitor which is likely similar to Cymbalta (duloxetine). It may have a lower effect size of around less than 60% but this also is around the reported effect sizes for selective serotonin reuptake inhibitors (SSRIs) for depression. If a patient has both ADHD and an anxiety disorder, I often consider an SSRI alternatively first to manage attention issues associated with anxiety and then would add on a stimulant if attention issues persist once anxiety is better treated.
Second/third line ADHD treatments
As a second-line approach to long-acting Ritalin and if there is not a response to it, I would consider extended-release Adderall preparations such as Vyvanse, which is an amphetamine preparation supposedly less abusable than Adderall (one can’t snort it), but I also caution that it releases dopamine, peaks faster, and does not reduce to zero stimulant in 24 hours because of a variable half-life.
In this way, I always have imagined that these amphetamines may be more theoretically concerning than Ritalin/methylphenidate because they increase dopamine dumping into the synapse (which is a different and extra mechanism than just reuptake). For a third line, I may consider guanfacine depending on weight daily, which is an Food and Drug Administration–approved, nonstimulant alpha-2 agonist, which also acts longer than clonidine and may be better for hyperactivity symptoms. I may begin with doses as low as 0.25-0.5 mg in the evening for concerns with sedation or groggy aftereffects in the morning.
Throughout all treatment with medication, I emphasize the importance of assertively managing ADHD symptoms which may be in the form of “behavioral treatment,” like cognitive behavioral therapy, organizational coaching available at some educational centers, or even finding ways to train one’s focus with athletics or practices such as yoga and mindfulness. In addition to this combined approach to treatment, stimulants are not perfect medications. All stimulants have a “drop-off effect” and were made to work during a school day lasting from 8 a.m. to 3 p.m. Some patients and families complain about the drop-off effect and may want to “dose” around a medication more frequently, in the late afternoon and in the evening, which can lead to poor appetite at dinner and insomnia.
My answers to the cases above would be that all the patients could have ADHD, but they also may have anxiety or stress-related disorders, depression, worries about performance, or poor skills to manage inattention. They may not yet have received school supports, coaching, or found ways to manage these symptoms either. Because stimulants can improve and enhance performance but also have their own drawbacks and risks not covered here, it’s important to consider each case as a whole with thoughtfulness about a child’s unique ability to “live and work” in this world.
Dr. Pawlowski is an adult, adolescent, and child psychiatrist at the University of Vermont Medical Center and an assistant professor of psychiatry at UVM, both in Burlington. She reported no relevant financial disclosures. Email her at pdnews@mdedge.com.
- A 9-year-old boy has poor impulse control, throws things in class, and cannot sit still. Teachers ask: Is this ADHD and should we start a medication?
- A 9-year-old girl is an inattentive daydreamer with poor class performance and trouble turning in homework. Her parents and teachers ask: Is this ADHD and should we start a medication?
- A 17-year-old boy who is a high achiever is taking the upcoming SATs and does poorly on timed tests because of poor focus and is now wondering: Do I have ADHD and would a medication help me perform better?
- A 17-year-old boy had poor grades for much of his early school years, but his parents always thought he was just a “lazy kid” although he insists he is trying his best. His parents now ask: Is this ADHD and has it been all along?
The above cases may sound familiar to you. They are an oversimplification of the patients who may come to you with two questions: Do I or someone I care about have ADHD and should they have medication for it? What may matter even more is how they are doing with that inattentiveness and how much it impacts their lives.
Sigmund Freud was known to think about goals for treatment as “liebe und arbeit” translated into “to love and to work.” As in, can someone live, love, and work or are their psychiatric symptoms impairing those functionalities? For a child, to live, work, and play (well with others) is most apt here. It is often more helpful to think in terms of childhood daily life when choosing to begin a medication or not. With inattention, a child can range from having a parent hoping for performance enhancement to having a severe impairment in their day-to-day functioning in a classroom. In the above case examples, each child or adolescent has varying impairments in performance – one is a high academic performer with very few issues outside of testing and another is a young child who can’t even sit still in a classroom to learn. Who should be prescribed a stimulant? Any or all of the above? It’s not as easy an answer as you may suspect, and there may not be one “right” answer either.
We know that stimulants can help a great deal of patients. They have the highest effect size for ADHD in that about 80% of children can benefit from stimulant treatment for ADHD. Specifically, “a high response rate of 70%-85% has been noted with methylphenidate and amphetamine formulations. The response rate is lower for atomoxetine [60%-65%] and guanfacine [30%-40%]” (Venkat B, Hechtman L. Considerations in selecting pharmacological treatments for attention deficit hyperactivity disorder. Clinical Pharmacist. 2016 Feb 11). In thinking about when to prescribe, we want to balance offering nonpharmacologic means to address symptoms of inattention (like mindfulness, exercise, and school supports such as individualized learning plans where applicable). We also do not want to withhold helpful treatments such as stimulants or other nonstimulant medications or trend toward overprescribing potentially habit-forming and imperfect medications.
It is important to make that distinction between impairment and the desire for medications to “enhance” life and optimize performance rather than treating symptoms of a disorder. It is most helpful to gain skills to navigate those challenges simultaneously to ultimately help our patients live, learn, love, and play to the best of their abilities.
Where to begin
When I was in training, I had difficulty teasing out the various ADHD stimulant formations. There were and are so many Ritalin preparations! Mostly there is a variation in shorter-acting to longer-acting effects. If the diagnosis is highly suspected and uncomplicated ADHD, I usually choose to start with Concerta 18 mg daily (a long-acting methylphenidate) for children aged over 6 years. Many times I don’t see the need to titrate that upwards much further toward the maximum clinically used dose of 54 mg daily (despite guidelines saying otherwise up to 72 mg daily, which I have found unnecessary usually and poorly tolerated). Concerta has an immediate effect (20%) and then slowly peaks until 12 p.m. (80%) and then is out of system by about 3 p.m. (for a total of 7 hours duration of action). There also are shorter-acting preparations (Ritalin, Methylin) which are “on/off” in 4 hours and use of these is more consistent with an antiquated way of prescribing, often up to twice daily and three times daily dosing schedules with the risk of the harder to tolerate “drop-off” effects with stimulants. And, if there is not an effect, I often reconsider the diagnosis and any co-occurring anxiety disorder, stressful life events, or depression or other illness with the knowledge that these medications so often are effective.
Anxiety + ADHD
If there is prominent anxiety, anxiety disorder, or tics, I often consider Strattera 10-20 mg daily up to around 40 mg. I tend to dose this lower than as written for tolerability and in a “dose low and go slow” approach with kids, which often results in better experiences with the medication. This medication also is recommended to be dosed by weight; this should be taken into account as well. Atomoxetine is a selective serotonin and norepinephrine reuptake inhibitor which is likely similar to Cymbalta (duloxetine). It may have a lower effect size of around less than 60% but this also is around the reported effect sizes for selective serotonin reuptake inhibitors (SSRIs) for depression. If a patient has both ADHD and an anxiety disorder, I often consider an SSRI alternatively first to manage attention issues associated with anxiety and then would add on a stimulant if attention issues persist once anxiety is better treated.
Second/third line ADHD treatments
As a second-line approach to long-acting Ritalin and if there is not a response to it, I would consider extended-release Adderall preparations such as Vyvanse, which is an amphetamine preparation supposedly less abusable than Adderall (one can’t snort it), but I also caution that it releases dopamine, peaks faster, and does not reduce to zero stimulant in 24 hours because of a variable half-life.
In this way, I always have imagined that these amphetamines may be more theoretically concerning than Ritalin/methylphenidate because they increase dopamine dumping into the synapse (which is a different and extra mechanism than just reuptake). For a third line, I may consider guanfacine depending on weight daily, which is an Food and Drug Administration–approved, nonstimulant alpha-2 agonist, which also acts longer than clonidine and may be better for hyperactivity symptoms. I may begin with doses as low as 0.25-0.5 mg in the evening for concerns with sedation or groggy aftereffects in the morning.
Throughout all treatment with medication, I emphasize the importance of assertively managing ADHD symptoms which may be in the form of “behavioral treatment,” like cognitive behavioral therapy, organizational coaching available at some educational centers, or even finding ways to train one’s focus with athletics or practices such as yoga and mindfulness. In addition to this combined approach to treatment, stimulants are not perfect medications. All stimulants have a “drop-off effect” and were made to work during a school day lasting from 8 a.m. to 3 p.m. Some patients and families complain about the drop-off effect and may want to “dose” around a medication more frequently, in the late afternoon and in the evening, which can lead to poor appetite at dinner and insomnia.
My answers to the cases above would be that all the patients could have ADHD, but they also may have anxiety or stress-related disorders, depression, worries about performance, or poor skills to manage inattention. They may not yet have received school supports, coaching, or found ways to manage these symptoms either. Because stimulants can improve and enhance performance but also have their own drawbacks and risks not covered here, it’s important to consider each case as a whole with thoughtfulness about a child’s unique ability to “live and work” in this world.
Dr. Pawlowski is an adult, adolescent, and child psychiatrist at the University of Vermont Medical Center and an assistant professor of psychiatry at UVM, both in Burlington. She reported no relevant financial disclosures. Email her at pdnews@mdedge.com.
‘Simple’ way to cut PAD risk, misguided ED visits for atrial fib, and more
This week in MDedge Cardiocast: Elevated CAC in highly active men doesn’t raise risk of death, Life’s Simple 7 scores can be used to modify PAD risk, medical guidance often leads atrial fibrillation patients to needlessly seek emergency department care, and thinking of pregnancy as a stress test can help predict women’s future cardiovascular risk.
Amazon AlexaApple Podcasts
Google Podcasts
TuneIn
This week in MDedge Cardiocast: Elevated CAC in highly active men doesn’t raise risk of death, Life’s Simple 7 scores can be used to modify PAD risk, medical guidance often leads atrial fibrillation patients to needlessly seek emergency department care, and thinking of pregnancy as a stress test can help predict women’s future cardiovascular risk.
Amazon AlexaApple Podcasts
Google Podcasts
TuneIn
This week in MDedge Cardiocast: Elevated CAC in highly active men doesn’t raise risk of death, Life’s Simple 7 scores can be used to modify PAD risk, medical guidance often leads atrial fibrillation patients to needlessly seek emergency department care, and thinking of pregnancy as a stress test can help predict women’s future cardiovascular risk.
Amazon AlexaApple Podcasts
Google Podcasts
TuneIn

Cilostazol plus aspirin or clopidogrel reduces the risk of recurrent stroke
HONOLULU – The combination also entails a similar risk of major bleeding, compared with aspirin and clopidogrel alone, according to results from the Cilostazol Stroke Prevention Study for Antiplatelet Combination (CSPS.com).

Dual-antiplatelet therapy with aspirin and clopidogrel reduced the rate of recurrent stroke in previous studies. The benefit of this drug combination is relatively short-lived, however, and long-term concomitant use of aspirin and clopidogrel entails a risk of major bleeding. Other data have indicated that cilostazol, which is approved by the Food and Drug Administration to alleviate intermittent claudication in patients with peripheral vascular disease, prevents stroke recurrence without increasing the incidence of serious bleeding, compared with aspirin, said Kazunori Toyoda, MD, PhD, who presented the results of the CSPS.com trial at the International Stroke Conference sponsored by the American Heart Association.
Dr. Toyoda of the National Cerebral and Cardiovascular Center in Osaka, Japan, and his colleagues randomized 1,879 high-risk patients at 8-180 days after the onset of noncardioembolic ischemic stroke identified on MRI to receive 81 or 100 mg aspirin or 50 or 75 mg clopidogrel alone, or a combination of cilostazol 100 mg twice daily with aspirin or clopidogrel. They conducted their open-label, parallel-group trial at 292 sites in Japan from December 2013 through March 2017.
To be considered at high risk, participants had to meet one or more of the following criteria: 50% or greater stenosis of a major intracranial artery, 50% or greater stenosis of an extracranial artery, and two or more vascular risk factors. The trial’s primary efficacy outcome was the first recurrence of ischemic stroke. Safety outcomes included severe or life-threatening bleeding.
The investigators ended the trial early because of a delay in recruiting patients. They enrolled 1,884 and randomized 1,879 of an anticipated 4,000 patients. At randomization, 41% in the dual-therapy group received aspirin and 59% clopidogrel, and in the monotherapy group, 40% received aspirin and 60% clopidogrel. Baseline characteristics were similar between the treatment groups. The population’s mean age was 70. Approximately 30% of patients were women.
During a median follow-up period of 17 months, ischemic stroke recurred in 29 of 932 patients receiving dual therapy including cilostazol for an annual rate of 2.2% and in 64 of 947 patients receiving monotherapy for an annual rate of 4.5% (hazard ratio, 0.49; 95% confidence interval, 0.31-0.76; P = .001). Severe or life-threatening bleeding occurred in 8 patients (0.6% per year) receiving dual therapy and 13 patients (0.9% per year) receiving monotherapy (HR, 0.66; 95% CI, 0.27-1.60; P = .354).
The study was funded by Otsuka Pharmaceutical, which manufactures cilostazol. Dr. Toyoda reported receiving support from Bayer Yakuhin, Daiichi Sankyo, Bristol-Myers Squibb, and Nippon Boehringer Ingelheim.
SOURCE: Toyoda K et al. ISC 2019, Abstract LB3.
HONOLULU – The combination also entails a similar risk of major bleeding, compared with aspirin and clopidogrel alone, according to results from the Cilostazol Stroke Prevention Study for Antiplatelet Combination (CSPS.com).
Dual-antiplatelet therapy with aspirin and clopidogrel reduced the rate of recurrent stroke in previous studies. The benefit of this drug combination is relatively short-lived, however, and long-term concomitant use of aspirin and clopidogrel entails a risk of major bleeding. Other data have indicated that cilostazol, which is approved by the Food and Drug Administration to alleviate intermittent claudication in patients with peripheral vascular disease, prevents stroke recurrence without increasing the incidence of serious bleeding, compared with aspirin, said Kazunori Toyoda, MD, PhD, who presented the results of the CSPS.com trial at the International Stroke Conference sponsored by the American Heart Association.
Dr. Toyoda of the National Cerebral and Cardiovascular Center in Osaka, Japan, and his colleagues randomized 1,879 high-risk patients at 8-180 days after the onset of noncardioembolic ischemic stroke identified on MRI to receive 81 or 100 mg aspirin or 50 or 75 mg clopidogrel alone, or a combination of cilostazol 100 mg twice daily with aspirin or clopidogrel. They conducted their open-label, parallel-group trial at 292 sites in Japan from December 2013 through March 2017.
To be considered at high risk, participants had to meet one or more of the following criteria: 50% or greater stenosis of a major intracranial artery, 50% or greater stenosis of an extracranial artery, and two or more vascular risk factors. The trial’s primary efficacy outcome was the first recurrence of ischemic stroke. Safety outcomes included severe or life-threatening bleeding.
The investigators ended the trial early because of a delay in recruiting patients. They enrolled 1,884 and randomized 1,879 of an anticipated 4,000 patients. At randomization, 41% in the dual-therapy group received aspirin and 59% clopidogrel, and in the monotherapy group, 40% received aspirin and 60% clopidogrel. Baseline characteristics were similar between the treatment groups. The population’s mean age was 70. Approximately 30% of patients were women.
During a median follow-up period of 17 months, ischemic stroke recurred in 29 of 932 patients receiving dual therapy including cilostazol for an annual rate of 2.2% and in 64 of 947 patients receiving monotherapy for an annual rate of 4.5% (hazard ratio, 0.49; 95% confidence interval, 0.31-0.76; P = .001). Severe or life-threatening bleeding occurred in 8 patients (0.6% per year) receiving dual therapy and 13 patients (0.9% per year) receiving monotherapy (HR, 0.66; 95% CI, 0.27-1.60; P = .354).
The study was funded by Otsuka Pharmaceutical, which manufactures cilostazol. Dr. Toyoda reported receiving support from Bayer Yakuhin, Daiichi Sankyo, Bristol-Myers Squibb, and Nippon Boehringer Ingelheim.
SOURCE: Toyoda K et al. ISC 2019, Abstract LB3.
HONOLULU – The combination also entails a similar risk of major bleeding, compared with aspirin and clopidogrel alone, according to results from the Cilostazol Stroke Prevention Study for Antiplatelet Combination (CSPS.com).
Dual-antiplatelet therapy with aspirin and clopidogrel reduced the rate of recurrent stroke in previous studies. The benefit of this drug combination is relatively short-lived, however, and long-term concomitant use of aspirin and clopidogrel entails a risk of major bleeding. Other data have indicated that cilostazol, which is approved by the Food and Drug Administration to alleviate intermittent claudication in patients with peripheral vascular disease, prevents stroke recurrence without increasing the incidence of serious bleeding, compared with aspirin, said Kazunori Toyoda, MD, PhD, who presented the results of the CSPS.com trial at the International Stroke Conference sponsored by the American Heart Association.
Dr. Toyoda of the National Cerebral and Cardiovascular Center in Osaka, Japan, and his colleagues randomized 1,879 high-risk patients at 8-180 days after the onset of noncardioembolic ischemic stroke identified on MRI to receive 81 or 100 mg aspirin or 50 or 75 mg clopidogrel alone, or a combination of cilostazol 100 mg twice daily with aspirin or clopidogrel. They conducted their open-label, parallel-group trial at 292 sites in Japan from December 2013 through March 2017.
To be considered at high risk, participants had to meet one or more of the following criteria: 50% or greater stenosis of a major intracranial artery, 50% or greater stenosis of an extracranial artery, and two or more vascular risk factors. The trial’s primary efficacy outcome was the first recurrence of ischemic stroke. Safety outcomes included severe or life-threatening bleeding.
The investigators ended the trial early because of a delay in recruiting patients. They enrolled 1,884 and randomized 1,879 of an anticipated 4,000 patients. At randomization, 41% in the dual-therapy group received aspirin and 59% clopidogrel, and in the monotherapy group, 40% received aspirin and 60% clopidogrel. Baseline characteristics were similar between the treatment groups. The population’s mean age was 70. Approximately 30% of patients were women.
During a median follow-up period of 17 months, ischemic stroke recurred in 29 of 932 patients receiving dual therapy including cilostazol for an annual rate of 2.2% and in 64 of 947 patients receiving monotherapy for an annual rate of 4.5% (hazard ratio, 0.49; 95% confidence interval, 0.31-0.76; P = .001). Severe or life-threatening bleeding occurred in 8 patients (0.6% per year) receiving dual therapy and 13 patients (0.9% per year) receiving monotherapy (HR, 0.66; 95% CI, 0.27-1.60; P = .354).
The study was funded by Otsuka Pharmaceutical, which manufactures cilostazol. Dr. Toyoda reported receiving support from Bayer Yakuhin, Daiichi Sankyo, Bristol-Myers Squibb, and Nippon Boehringer Ingelheim.
SOURCE: Toyoda K et al. ISC 2019, Abstract LB3.
REPORTING FROM ISC
Key clinical point: Treating patients at high risk of recurrent stroke with cilostazol and aspirin or clopidogrel reduced the risk of recurrent stroke more than either aspirin or clopidogrel alone and was just as safe.
Major finding: Dual therapy with cilostazol and aspirin or clopidogrel reduced the risk of recurrent stroke by approximately half, compared with aspirin or clopidogrel alone.
Study details: A multicenter, randomized, open-label, parallel-group trial including 1,879 patients at high risk of recurrent stroke.
Disclosures: Otsuka Pharmaceutical funded the study. The presenter reported receiving support from Bayer Yakuhin, Daiichi Sankyo, Bristol-Myers Squibb, and Nippon Boehringer Ingelheim.
Source: Toyoda K et al. ISC 2019, Abstract LB3.
A patient with severe adenomyosis requests uterine-sparing surgery
CASE
A 28-year-old patient presents for evaluation and management of her chronic pelvic pain, dysmenorrhea, and menorrhagia. She previously tried ibuprofen with no pain relief. She also tried oral and long-acting reversible contraceptives but continued to be symptomatic. She underwent pelvic sonography, which demonstrated a large globular uterus with myometrial thickening and myometrial cysts with increased hypervascularity. Subsequent magnetic resonance imaging indicated a thickened junctional zone. Feeling she had exhausted medical manegement options with no significant improvement, she desired surgical treatment, but wanted to retain her future fertility. As a newlywed, she and her husband were planning on building a family so she desired to retain her uterus for potential future pregnancy.
How would you address this patient’s disruptive symptoms, while affirming her long-term plans by choosing the proper intervention?
Adenomyosis is characterized by endometrial-like glands and stroma deep within the myometrium of the uterus and generally is classified as diffuse or focal. This common, benign gynecologic condition is known to cause enlargement of the uterus secondary to stimulation of ectopic endometrial-like cells.1-3 Although the true incidence of adenomyosis is unknown because of the difficulty of making the diagnosis, prevalence has been variously reported at 6% to 70% among reproductive-aged women.4,5
In this review, we first examine the clinical presentation and diagnosis of adenomyosis. We then discuss clinical indications for, and surgical techniques of, adenomyomectomy, including our preferred uterine-sparing approach for focal disease or when the patient wants to preserve fertility: video laparoscopic resection with or without robotic assistance, aided by minilaparotomy when indicated.
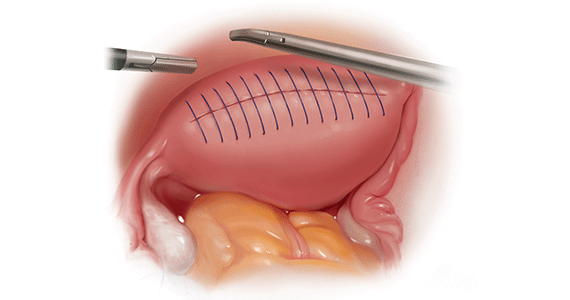
Treatment evolved in a century and a half
Adenomyosis was first described more than 150 years ago; historically, hysterectomy was the mainstay of treatment.2,6 Conservative surgical treatment for adenomyosis has been reported since the early 1950s.6-8 Surgical treatment initially became more widespread following the introduction of wedge resection, which allowed for partial excision of adenomyotic nodules.9
More recent developments in diagnostic technologies and capabilities have allowed for the emergence of additional uterine-sparing and minimally invasive surgical treatment options for adenomyosis.3,10 Although the use of laparoscopic approaches is limited because a high level of technical skill is required to undertake these procedures, such approaches are becoming increasingly important as more and more patients seek fertility conservation.11-13
How does adenomyosis present?
Adenomyosis symptoms commonly consist of abnormal uterine bleeding and dysmenorrhea, affecting approximately 40% to 60% and 15% to 30% of patients with the condition, respectively.14 These symptoms are considered nonspecific because they are also associated with other uterine abnormalities.15 Although menorrhagia is not associated with extent of disease, dysmenorrhea is associated with both the number and depth of adenomyotic foci.14
Other symptoms reported with adenomyosis include chronic pelvic pain, dyspareunia, as well as infertility. Note, however, that a large percentage of patients are asymptomatic.16,17
On physical examination, patients commonly exhibit a diffusely enlarged, globular uterus. This finding is secondary to uniform hyperplasia and hypertrophy of the myometrium, caused by stimulation of ectopic endometrial cells.2 A subset of patients experience significant uterine tenderness.18 Other common findings associated with adenomyosis include uterine abnormalities, such as leiomyomata, endometriosis, and endometrial polyps.
Continue to: Two-pronged route to diagnosis and a differential...
Two-pronged route to diagnosis and a differential
Histology
Adenomyosis is definitively diagnosed based on histologic findings of endometrial-like tissue within the myometrium. Historically, histologic analysis was performed on specimens following hysterectomy but, more recently, has utilized specimens obtained from hysteroscopic and laparoscopic myometrial biopsies.19 Importantly, although hysteroscopic and laparoscopic biopsies are taken under direct visualization, there are no pathognomonic signs for adenomyosis; a diagnosis can therefore be missed if adenomyosis is not present at biopsied sites.1 The sensitivity of random biopsy at laparoscopy has been found to be as low as 2% to as high as 56%.20
Imaging
Imaging can be helpful in clinical decision making and to guide the differential diagnosis. Transvaginal ultrasonography (TVUS) is often the first mode of imaging used for the investigation of abnormal uterine bleeding or pelvic pain. Diagnosis by TVUS is difficult because the modality is operator dependent and standard diagnostic criteria are lacking.5
The most commonly reported ultrasonographic features of adenomyosis are21,22:
- a globally enlarged uterus
- asymmetry
- myometrial thickening with heterogeneity
- poorly defined foci of hyperechoic regions, surrounded by hypoechoic areas that correspond to smooth-muscle hyperplasia
- myometrial cysts.
Doppler ultrasound examination in patients with adenomyosis reveals increased flow to the myometrium without evidence of large blood vessels.
3-dimensional (3-D) ultrasonography. Integration of 3-D ultrasonography has allowed for identification of the thicker junctional zone that suggests adenomyosis. In a systematic review of the accuracy of TVUS, investigators reported a pooled sensitivity and specificity for 2-dimensional ultrasonography of 83.8% and 63.9%, respectively, and a pooled sensitivity and specificity for 3-dimensional ultrasonography of 88.9% and 56.0%, respectively.22
Magnetic resonance imaging (MRI) is also used in the evaluation of adenomyosis. Although MRI is considered a more accurate diagnostic modality because it is not operator dependent, expense often prohibits its use in the work-up of abnormal uterine bleeding and chronic pelvic pain.2,23
The most commonly reported MRI findings in adenomyosis include a globular or asymmetric uterus, heterogeneity of myometrial signal intensity, and thickening of the junctional zone24 (FIGURE 1). In a systematic review, researchers reported a pooled sensitivity and specificity of 77% and 89%, respectively, for the diagnosis of adenomyosis using MRI.25
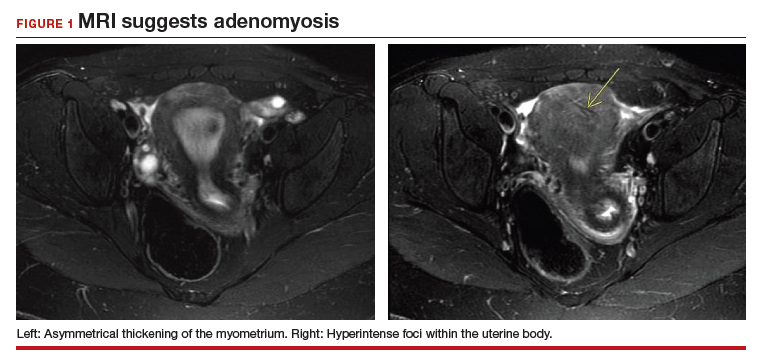
Approaches to treatment
Medical management
No medical therapies or guidelines specific to the treatment of adenomyosis exist.9 Often, nonsteroidal anti-inflammatory drugs (NSAIDs) are employed to combat cramping and pain associated with increased prostaglandin levels.26 A systematic review found that NSAIDs are significantly better at treating dysmenorrhea than placebo alone.26
Moreover, adenomyosis is an estrogen-dependent disease; consequently, many medical treatments are targeted at suppressing the hypothalamic–pituitary–ovarian axis and inducing endometrial atrophy. Medications commonly used (off-label) for this effect include combined or progestin-only oral contraceptive pills, gonadotropin-releasing hormone (GnRH) agonists, levonorgestrel-releasing intrauterine devices, danazol, and aromatase inhibitors.
Use of a GnRH agonist, such as leuprolide, is limited to a short course (<6 months) because menopausal-like symptoms, such as hot flashes, vaginal atrophy, and loss of bone-mineral density, can develop.16 Symptoms of adenomyosis often return upon cessation of hormonal treatment.1
Novel therapies are under investigation, including GnRH antagonists, selective progesterone-receptor modulators, and antiplatelet therapy.27
Although there are few data showing the effectiveness of medical therapy on adenomyosis-specific outcomes, medications are particularly useful in patients who are poor surgical candidates or who may prefer not to undergo surgery. Furthermore, medical therapy has considerable use in conjunction with surgical intervention; a prospective observational study showed that women who underwent GnRH agonist treatment following surgery had significantly greater improvement of their dysmenorrhea and menorrhagia, compared with those who underwent surgery only.28 In addition, preoperative administration of a GnRH agonist or danazol several months prior to surgery has been shown to reduce uterine vascularity and, thus, blood loss at surgery.29,30
- Adenomyosis is common and benign, but remains underdiagnosed because of a nonspecific clinical presentation and lack of standardized diagnostic criteria.
- Adenomyosis can cause significant associated morbidity: dysmenorrhea, heavy menstrual bleeding, chronic pelvic pain, and infertility.
- High clinical suspicion warrants evaluation by imaging.
- Medical management is largely aimed at ameliorating symptoms.
- A patient who does not respond to medical treatment or does not desire pregnancy has a variety of surgical options; the extent of disease and the patient’s wish for uterine preservation guide the selection of surgical technique.
- Hysterectomy is the definitive treatment but, in patients who want to avoid radical resection, techniques developed for laparotomy are available, to allow conservative resection using laparoscopy.
- Ideally, surgery is performed using a combined laparoscopy and minilaparotomy approach, after appropriate imaging.
Continue to: Surgery
Surgery
The objective of surgical management is to ameliorate symptoms in a conservative manner, by excision or cytoreduction of adenomyotic lesions, while preserving, even improving, fertility.3,11,31 The choice of procedure depends, ultimately, on the location and extent of disease, the patient’s desire for uterine preservation and fertility, and surgical skill.3
Historically, hysterectomy was used to treat adenomyosis; for patients declining fertility preservation, hysterectomy remains the definitive treatment. Since the early 1950s, several techniques for laparotomic reduction have been developed. Surgeries that achieve partial reduction include:
Wedge resection of the uterine wall entails removal of the seromuscular layer at the identified location of adenomyotic tissue, with subsequent repair of the remaining muscular and serosal layers surrounding the wound.3,32 Because adenomyotic tissue can remain on either side of the incision in wedge resection, clinical improvement in symptoms of dysmenorrhea and menorrhagia are modest, and recurrence is possible.7
Modified reduction surgery. Modifications of reduction surgery include slicing adenomyotic tissue using microsurgery and partial excision.33
Transverse-H incision of the uterine wall involves a transverse incision on the uterine fundus, separating serosa and myometrium, followed by removal of diseased tissue using an electrosurgical scalpel or scissors. Tensionless suturing is used to close the myometrial layers in 1 or 2 layers to establish hemostasis and close the defect; serosal flaps are closed with subserosal interrupted sutures.34 Data show that, following surgery with this technique, 21.4% to 38.7% of patients who attempt conception achieve clinical pregnancy.7
Complete, conservative resection in cases of diffuse and focal adenomyosis is possible using the triple-flap method, in which total resection is achieved by removing diseased myometrium until healthy, soft tissue—with normal texture, color, and vascularity—is reached.2 Repair with this technique reduces the risk of uterine rupture by reconstructing the uterine wall using a muscle flap prepared by metroplasty.7 In a study of 64 women who underwent triple-flap resection, a clinical pregnancy rate of 74% and a live birth rate of 52% were reported.7
Minimally invasive approaches. Although several techniques have been developed for focal excision of adenomyosis by laparotomy,7 the trend has been toward minimally invasive surgery, which reduces estimated blood loss, decreases length of stay, and reduces adhesion formation—all without a statistically significant difference in long-term clinical outcomes, compared to other techniques.35-39 Furthermore, enhanced visualization of pelvic organs provided by laparoscopy is vital in the case of adenomyosis.3,31
How our group approaches surgical management. A challenge in laparoscopic surgery of adenomyosis is extraction of an extensive amount of diseased tissue. In 1994, our group described the use of simultaneous operative laparoscopy and minilaparotomy technique as an effective and safe alternative to laparotomy in the treatment of myomectomy6; the surgical principles of that approach are applied to adenomyomectomy. The technique involves treatment of pelvic pathology with laparoscopy, removal of tissue through the minilaparotomy incision, and repair of the uterine wall defect in layers.
How adenomyosis originates is not fully understood. Several theories have been proposed, however (including, more prominently, the first 2 below):
Invasion theory. The endometrial basalis layer invaginates and invades the myometrium1,2 (FIGURE); the etiology of invagination remains unknown.
Reaction theory. Myometrial weakness or dysfunction, brought on by trauma from previous uterine surgery or pregnancy, could predispose uterine musculature to deep invasion.3
Metaplasia theory. Adenomyosis is a result of metaplasia of pluripotent Müllerian rests.
Müllerian remnant theory. Related to the Müllerian metaplasia theory, adenomyosis is formed de novo from 1) adult stem cells located in the endometrial basalis that is involved in the cyclic regeneration of the endometrium4-6 or 2) adult stem cells displaced from bone marrow.7,8
Once adenomyosis is established, it is thought to progress by epithelial–mesenchymal transition,2 a process by which epithelial cells become highly motile mesenchymal cells that are capable of migration and invasion, due to loss of cell–cell adhesion properties.9
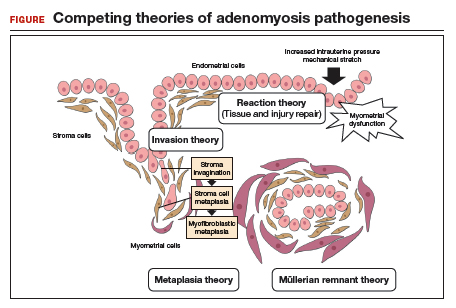
References
- Struble J, Reid S, Bedaiwy MA. Adenomyosis: a clinical review of a challenging gynecologic condition. J Minim Invasive Gynecol.2016; 23:164-185.
- García-Solares J, Donnez J, Donnez O, et al. Pathogenesis of uterine adenomyosis: invagination or metaplasia? Fertil Steril.2018;109:371-379.
- Ferenczy A. Pathophysiology of adenomyosis. Hum Reprod Update. 1998;4:312-322.
- Gargett CE. Uterine stem cells: what is the evidence? Hum Reprod Update. 2007;13:87-101.
- Chan RW, Schwab KE, Gargett CE. Clonogenicity of human endometrial epithelial and stromal cells. Biol Reprod. 2004;70:1738-1750.
- Schwab KE, Chan RWS, Gargett CE. Putative stem cell activity of human endometrial epithelial and stromal cells during the menstrual cycle. Fertil Steril. 2005;84(Suppl 2):1124-1130.
- Sasson IE, Taylor HS. Stem cells and the pathogenesis of endometriosis. Ann N Y Acad Sci. 2008;1127:106-115.
- Du H, Taylor HS. Stem cells and female reproduction. Reprod Sci. 2009;16:126-139.
- Acloque H, Adams MS, Fishwick K, et al. Epithelial-mesenchymal transitions: the importance of changing cell state in development and disease. J Clin Invest. 2009;119:1438-1449.
Continue to: In 57 women who underwent…
In 57 women who underwent this procedure, the mean operative time was 127 minutes; average estimated blood loss was 267 mL.40 Overall, laparoscopy with minilaparotomy was found to be a less technically difficult technique for laparoscopic myomectomy; allowed better closure of the uterine defect; and might have required less time to perform.3
We therefore advocate video laparoscopic wedge resection with or without robotic assistance, aided by minilaparotomy when necessary for safe removal of larger adenomyomas, as the preferred uterine-sparing surgical approach for focal adenomyosis or when the patient wants to preserve fertility (FIGURE 2). We think that this technique allows focal adenomyosis to be treated by wedge resection of the diseased myometrium, with subsequent closure of the remaining myometrial defect using a barbed V-Loc (Medtronic, Minneapolis, Minnesota) delayed absorbable suture in layers (FIGURE 3). Minilaparotomy can be utilized when indicated to aid removal of the resected myometrial specimen.
In our extensive experience, we have found that this technique provides significant relief of symptoms and improvements in fertility outcomes while minimizing surgical morbidity.
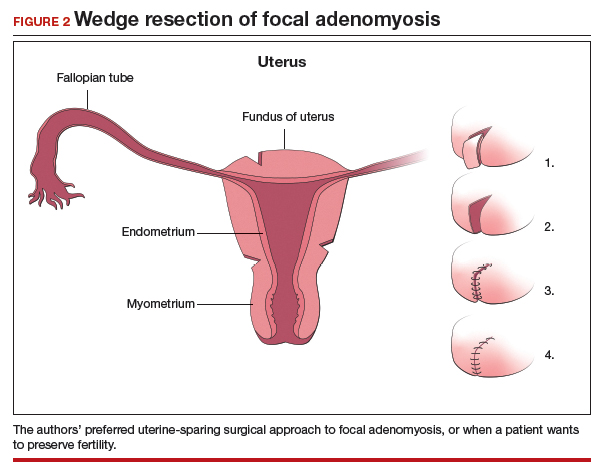
CASE Resolved
The patient underwent successful wedge resection of her adenomyosis by laparoscopy. She experienced nearly complete resolution of her symptoms of dysmenorrhea, menorrhagia, and pelvic pain. She retained good uterine integrity. Three years later, she and her husband became parents when she delivered their first child by cesarean delivery at full term. After she completed childbearing, she ultimately opted for minimally invasive hysterectomy.

The authors would like to acknowledge Mailinh Vu, MD, Fellow at Camran Nezhat Institute, for reviewing and editing this article.
- Garcia L, Isaacson K. Adenomyosis: review of the literature. J Minim Invasive Gynecol. 2011;18:428-437.
- Nezhat C, Nezhat F, Nezhat C, eds. Nezhat's Video-Assisted and Robotic-Assisted Laparoscopy and Hysteroscopy. 4th ed. Cambridge, UK: Cambridge University Press; 2013.
- Osada H. Uterine adenomyosis and adenomyoma: the surgical approach. Fertil Steril. 2018;109:406-417.
- Azziz R. Adenomyosis: current perspectives. Obstet Gynecol Clin North Am. 1989;16:221-235.
- Struble J, Reid S, Bedaiwy MA. Adenomyosis: A clinical review of a challenging gynecologic condition. J Minim Invasive Gynecol. 2016;23:164-185.
- Rokitansky C. Ueber Uterusdrsen-Neubildung in Uterus- und Ovarial-Sarcomen. Gesellschaft der Ärzte in Wien. 1860;16:1-4.
- Osada H. Uterine adenomyosis and adenomyoma: the surgical approach. Fertil Steril. 2018;109:406-417.
- Van Praagh I. Conservative surgical treatment for adenomyosis uteri in young women: local excision and metroplasty. Can Med Assoc J. 1965;93:1174-1175.
- Donnez J, Donnez O, Dolmans MM. Introduction: Uterine adenomyosis, another enigmatic disease of our time. Fertil Steril. 2018;109:369-370.
- Nishida M, Takano K, Arai Y, et al. Conservative surgical management for diffuse uterine adenomyosis. Fertil Steril. 2010;94:715-719.
- Abbott JA. Adenomyosis and abnormal uterine bleeding (AUB-A)--Pathogenesis, diagnosis, and management. Best Pract Res Clin Obstet Gynaecol. 2017;40:68-81.
- Matalliotakis IM, Katsikis IK, Panidis DK. Adenomyosis: what is the impact on fertility? Curr Opin Obstet Gynecol. 2005;17:261-264.
- Devlieger R, D'Hooghe T, Timmerman D. Uterine adenomyosis in the infertility clinic. Hum Reprod Update. 2003;9:139-147.
- Levgur M, Abadi MA, Tucker A. Adenomyosis: symptoms, histology, and pregnancy terminations. Obstet Gynecol. 2000;95:688-691.
- Weiss G, Maseelall P, Schott LL, et al. Adenomyosis a variant, not a disease? Evidence from hysterectomized menopausal women in the Study of Women's Health Across the Nation (SWAN). Fertil Steril. 2009;91:201-206.
- Huang F, Kung FT, Chang SY, et al. Effects of short-course buserelin therapy on adenomyosis. A report of two cases. J Reprod Med. 1999;44:741-744.
- Benson RC, Sneeden VD. Adenomyosis: a reappraisal of symptomatology. Am J Obstet Gynecol. 1958;76:1044-1061.
- Shrestha A, Sedai LB. Understanding clinical features of adenomyosis: a case control study. Nepal Med Coll J. 2012;14:176-179.
- Fernández C, Ricci P, Fernández E. Adenomyosis visualized during hysteroscopy. J Minim Invasive Gynecol. 2007;14:555-556.
- Brosens JJ, Barker FG. The role of myometrial needle biopsies in the diagnosis of adenomyosis. Fertil Steril. 1995;63:1347-1349.
- Van den Bosch T, Van Schoubroeck D. Ultrasound diagnosis of endometriosis and adenomyosis: state of the art. Best Pract Res Clin Obstet Gynaecol. 2018;51:16-24.
- Andres MP, Borrelli GM, Ribeiro J, et al. Transvaginal ultrasound for the diagnosis of adenomyosis: systematic review and meta-analysis. J Minim Invasive Gynecol. 2018;25:257-264.
- Bazot M, Cortez A, Darai E, et al. Ultrasonography compared with magnetic resonance imaging for the diagnosis of adenomyosis: correlation with histopathology. Hum Reprod. 2001;16:2427-2433.
- Bragheto AM, Caserta N, Bahamondes L, et al. Effectiveness of the levonorgestrel-releasing intrauterine system in the treatment of adenomyosis diagnosed and monitored by magnetic resonance imaging. Contraception. 2007;76:195-199.
- Champaneria R, Abedin P, Daniels J, et al. Ultrasound scan and magnetic resonance imaging for the diagnosis of adenomyosis: systematic review comparing test accuracy. Acta Obstet Gynecol Scand. 2010; 89:1374-1384.
- Marjoribanks J, Proctor M, Farquhar C, et al. Nonsteroidal anti-inflammatory drugs for dysmenorrhoea. Cochrane Database Syst Rev. 2010;(1):CD001751.
- Vannuccini S, Luisi S, Tosti C, et al. Role of medical therapy in the management of uterine adenomyosis. Fertil Steril. 2018;109:398-405.
- Wang PH, Liu WM, Fuh JL, et al. Comparison of surgery alone and combined surgical-medical treatment in the management of symptomatic uterine adenomyoma. Fertil Steril. 2009;92:876-885.
- Wood C, Maher P, Woods R. Laparoscopic surgical techniques for endometriosis and adenomyosis. Diagn Ther Endosc. 2000;6:153-168.
- Wang CJ, Yuen LT, Chang SD, et al. Use of laparoscopic cytoreductive surgery to treat infertile women with localized adenomyosis. Fertil Steril. 2006;86:462.e5-e8.
- Nezhat C, Hajhosseini B, King LP. Robotic-assisted laparoscopic treatment of bowel, bladder, and ureteral endometriosis. JSLS. 2011;15:387-392.
- Sun A, Luo M, Wang W, et al. Characteristics and efficacy of modified adenomyomectomy in the treatment of uterine adenomyoma. Chin Med J. 2011;124:1322-1326.
- Fedele L, Bianchi S, Zanotti F, et al. Surgery: Fertility after conservative surgery for adenomyomas. Hum Reprod. 1993;8:1708-1710.
- Fujishita A, Masuzaki H, Khan KN, et al. Modified reduction surgery for adenomyosis. A preliminary report of the transverse H incision technique. Gynecol Obstet Invest. 2004;57:132-138.
- Operative Laparoscopy Study Group. Postoperative adhesion development after operative laparoscopy: evaluation at early second-look procedures. Fertil Steril. 1991;55:700-704.
- Luciano AA, Maier DB, Koch EI, et al. A comparative study of postoperative adhesions following laser surgery by laparoscopy versus laparotomy in the rabbit model. Obstet Gynecol. 1989;74:220-224.
- Lundorff P, Hahlin M, Källfelt B, et al. Adhesion formation after laparoscopic surgery in tubal pregnancy: a randomized trial versus laparotomy. Fertil Steril. 1991;55:911-915.
- Kwack JY, Kwon YS. Laparoscopic surgery for focal adenomyosis. JSLS. 2017;21. pii:e2017.00014.
- Podratz K. Degrees of Freedom: Advances in Gynecological and Obstetrical Surgery. Remembering Milestones and Achievements in Surgery: Inspiring Quality for a Hundred Years 1913-2012. Chicago, IL: American College of Surgeons; 2012.
- Nezhat C, Nezhat F, Bess O, et al. Laparoscopically assisted myomectomy: a report of a new technique in 57 cases. Int J Fertil Menopausal Stud. 1994;39:39-44.
CASE
A 28-year-old patient presents for evaluation and management of her chronic pelvic pain, dysmenorrhea, and menorrhagia. She previously tried ibuprofen with no pain relief. She also tried oral and long-acting reversible contraceptives but continued to be symptomatic. She underwent pelvic sonography, which demonstrated a large globular uterus with myometrial thickening and myometrial cysts with increased hypervascularity. Subsequent magnetic resonance imaging indicated a thickened junctional zone. Feeling she had exhausted medical manegement options with no significant improvement, she desired surgical treatment, but wanted to retain her future fertility. As a newlywed, she and her husband were planning on building a family so she desired to retain her uterus for potential future pregnancy.
How would you address this patient’s disruptive symptoms, while affirming her long-term plans by choosing the proper intervention?
Adenomyosis is characterized by endometrial-like glands and stroma deep within the myometrium of the uterus and generally is classified as diffuse or focal. This common, benign gynecologic condition is known to cause enlargement of the uterus secondary to stimulation of ectopic endometrial-like cells.1-3 Although the true incidence of adenomyosis is unknown because of the difficulty of making the diagnosis, prevalence has been variously reported at 6% to 70% among reproductive-aged women.4,5
In this review, we first examine the clinical presentation and diagnosis of adenomyosis. We then discuss clinical indications for, and surgical techniques of, adenomyomectomy, including our preferred uterine-sparing approach for focal disease or when the patient wants to preserve fertility: video laparoscopic resection with or without robotic assistance, aided by minilaparotomy when indicated.
Treatment evolved in a century and a half
Adenomyosis was first described more than 150 years ago; historically, hysterectomy was the mainstay of treatment.2,6 Conservative surgical treatment for adenomyosis has been reported since the early 1950s.6-8 Surgical treatment initially became more widespread following the introduction of wedge resection, which allowed for partial excision of adenomyotic nodules.9
More recent developments in diagnostic technologies and capabilities have allowed for the emergence of additional uterine-sparing and minimally invasive surgical treatment options for adenomyosis.3,10 Although the use of laparoscopic approaches is limited because a high level of technical skill is required to undertake these procedures, such approaches are becoming increasingly important as more and more patients seek fertility conservation.11-13
How does adenomyosis present?
Adenomyosis symptoms commonly consist of abnormal uterine bleeding and dysmenorrhea, affecting approximately 40% to 60% and 15% to 30% of patients with the condition, respectively.14 These symptoms are considered nonspecific because they are also associated with other uterine abnormalities.15 Although menorrhagia is not associated with extent of disease, dysmenorrhea is associated with both the number and depth of adenomyotic foci.14
Other symptoms reported with adenomyosis include chronic pelvic pain, dyspareunia, as well as infertility. Note, however, that a large percentage of patients are asymptomatic.16,17
On physical examination, patients commonly exhibit a diffusely enlarged, globular uterus. This finding is secondary to uniform hyperplasia and hypertrophy of the myometrium, caused by stimulation of ectopic endometrial cells.2 A subset of patients experience significant uterine tenderness.18 Other common findings associated with adenomyosis include uterine abnormalities, such as leiomyomata, endometriosis, and endometrial polyps.
Continue to: Two-pronged route to diagnosis and a differential...
Two-pronged route to diagnosis and a differential
Histology
Adenomyosis is definitively diagnosed based on histologic findings of endometrial-like tissue within the myometrium. Historically, histologic analysis was performed on specimens following hysterectomy but, more recently, has utilized specimens obtained from hysteroscopic and laparoscopic myometrial biopsies.19 Importantly, although hysteroscopic and laparoscopic biopsies are taken under direct visualization, there are no pathognomonic signs for adenomyosis; a diagnosis can therefore be missed if adenomyosis is not present at biopsied sites.1 The sensitivity of random biopsy at laparoscopy has been found to be as low as 2% to as high as 56%.20
Imaging
Imaging can be helpful in clinical decision making and to guide the differential diagnosis. Transvaginal ultrasonography (TVUS) is often the first mode of imaging used for the investigation of abnormal uterine bleeding or pelvic pain. Diagnosis by TVUS is difficult because the modality is operator dependent and standard diagnostic criteria are lacking.5
The most commonly reported ultrasonographic features of adenomyosis are21,22:
- a globally enlarged uterus
- asymmetry
- myometrial thickening with heterogeneity
- poorly defined foci of hyperechoic regions, surrounded by hypoechoic areas that correspond to smooth-muscle hyperplasia
- myometrial cysts.
Doppler ultrasound examination in patients with adenomyosis reveals increased flow to the myometrium without evidence of large blood vessels.
3-dimensional (3-D) ultrasonography. Integration of 3-D ultrasonography has allowed for identification of the thicker junctional zone that suggests adenomyosis. In a systematic review of the accuracy of TVUS, investigators reported a pooled sensitivity and specificity for 2-dimensional ultrasonography of 83.8% and 63.9%, respectively, and a pooled sensitivity and specificity for 3-dimensional ultrasonography of 88.9% and 56.0%, respectively.22
Magnetic resonance imaging (MRI) is also used in the evaluation of adenomyosis. Although MRI is considered a more accurate diagnostic modality because it is not operator dependent, expense often prohibits its use in the work-up of abnormal uterine bleeding and chronic pelvic pain.2,23
The most commonly reported MRI findings in adenomyosis include a globular or asymmetric uterus, heterogeneity of myometrial signal intensity, and thickening of the junctional zone24 (FIGURE 1). In a systematic review, researchers reported a pooled sensitivity and specificity of 77% and 89%, respectively, for the diagnosis of adenomyosis using MRI.25
Approaches to treatment
Medical management
No medical therapies or guidelines specific to the treatment of adenomyosis exist.9 Often, nonsteroidal anti-inflammatory drugs (NSAIDs) are employed to combat cramping and pain associated with increased prostaglandin levels.26 A systematic review found that NSAIDs are significantly better at treating dysmenorrhea than placebo alone.26
Moreover, adenomyosis is an estrogen-dependent disease; consequently, many medical treatments are targeted at suppressing the hypothalamic–pituitary–ovarian axis and inducing endometrial atrophy. Medications commonly used (off-label) for this effect include combined or progestin-only oral contraceptive pills, gonadotropin-releasing hormone (GnRH) agonists, levonorgestrel-releasing intrauterine devices, danazol, and aromatase inhibitors.
Use of a GnRH agonist, such as leuprolide, is limited to a short course (<6 months) because menopausal-like symptoms, such as hot flashes, vaginal atrophy, and loss of bone-mineral density, can develop.16 Symptoms of adenomyosis often return upon cessation of hormonal treatment.1
Novel therapies are under investigation, including GnRH antagonists, selective progesterone-receptor modulators, and antiplatelet therapy.27
Although there are few data showing the effectiveness of medical therapy on adenomyosis-specific outcomes, medications are particularly useful in patients who are poor surgical candidates or who may prefer not to undergo surgery. Furthermore, medical therapy has considerable use in conjunction with surgical intervention; a prospective observational study showed that women who underwent GnRH agonist treatment following surgery had significantly greater improvement of their dysmenorrhea and menorrhagia, compared with those who underwent surgery only.28 In addition, preoperative administration of a GnRH agonist or danazol several months prior to surgery has been shown to reduce uterine vascularity and, thus, blood loss at surgery.29,30
- Adenomyosis is common and benign, but remains underdiagnosed because of a nonspecific clinical presentation and lack of standardized diagnostic criteria.
- Adenomyosis can cause significant associated morbidity: dysmenorrhea, heavy menstrual bleeding, chronic pelvic pain, and infertility.
- High clinical suspicion warrants evaluation by imaging.
- Medical management is largely aimed at ameliorating symptoms.
- A patient who does not respond to medical treatment or does not desire pregnancy has a variety of surgical options; the extent of disease and the patient’s wish for uterine preservation guide the selection of surgical technique.
- Hysterectomy is the definitive treatment but, in patients who want to avoid radical resection, techniques developed for laparotomy are available, to allow conservative resection using laparoscopy.
- Ideally, surgery is performed using a combined laparoscopy and minilaparotomy approach, after appropriate imaging.
Continue to: Surgery
Surgery
The objective of surgical management is to ameliorate symptoms in a conservative manner, by excision or cytoreduction of adenomyotic lesions, while preserving, even improving, fertility.3,11,31 The choice of procedure depends, ultimately, on the location and extent of disease, the patient’s desire for uterine preservation and fertility, and surgical skill.3
Historically, hysterectomy was used to treat adenomyosis; for patients declining fertility preservation, hysterectomy remains the definitive treatment. Since the early 1950s, several techniques for laparotomic reduction have been developed. Surgeries that achieve partial reduction include:
Wedge resection of the uterine wall entails removal of the seromuscular layer at the identified location of adenomyotic tissue, with subsequent repair of the remaining muscular and serosal layers surrounding the wound.3,32 Because adenomyotic tissue can remain on either side of the incision in wedge resection, clinical improvement in symptoms of dysmenorrhea and menorrhagia are modest, and recurrence is possible.7
Modified reduction surgery. Modifications of reduction surgery include slicing adenomyotic tissue using microsurgery and partial excision.33
Transverse-H incision of the uterine wall involves a transverse incision on the uterine fundus, separating serosa and myometrium, followed by removal of diseased tissue using an electrosurgical scalpel or scissors. Tensionless suturing is used to close the myometrial layers in 1 or 2 layers to establish hemostasis and close the defect; serosal flaps are closed with subserosal interrupted sutures.34 Data show that, following surgery with this technique, 21.4% to 38.7% of patients who attempt conception achieve clinical pregnancy.7
Complete, conservative resection in cases of diffuse and focal adenomyosis is possible using the triple-flap method, in which total resection is achieved by removing diseased myometrium until healthy, soft tissue—with normal texture, color, and vascularity—is reached.2 Repair with this technique reduces the risk of uterine rupture by reconstructing the uterine wall using a muscle flap prepared by metroplasty.7 In a study of 64 women who underwent triple-flap resection, a clinical pregnancy rate of 74% and a live birth rate of 52% were reported.7
Minimally invasive approaches. Although several techniques have been developed for focal excision of adenomyosis by laparotomy,7 the trend has been toward minimally invasive surgery, which reduces estimated blood loss, decreases length of stay, and reduces adhesion formation—all without a statistically significant difference in long-term clinical outcomes, compared to other techniques.35-39 Furthermore, enhanced visualization of pelvic organs provided by laparoscopy is vital in the case of adenomyosis.3,31
How our group approaches surgical management. A challenge in laparoscopic surgery of adenomyosis is extraction of an extensive amount of diseased tissue. In 1994, our group described the use of simultaneous operative laparoscopy and minilaparotomy technique as an effective and safe alternative to laparotomy in the treatment of myomectomy6; the surgical principles of that approach are applied to adenomyomectomy. The technique involves treatment of pelvic pathology with laparoscopy, removal of tissue through the minilaparotomy incision, and repair of the uterine wall defect in layers.
How adenomyosis originates is not fully understood. Several theories have been proposed, however (including, more prominently, the first 2 below):
Invasion theory. The endometrial basalis layer invaginates and invades the myometrium1,2 (FIGURE); the etiology of invagination remains unknown.
Reaction theory. Myometrial weakness or dysfunction, brought on by trauma from previous uterine surgery or pregnancy, could predispose uterine musculature to deep invasion.3
Metaplasia theory. Adenomyosis is a result of metaplasia of pluripotent Müllerian rests.
Müllerian remnant theory. Related to the Müllerian metaplasia theory, adenomyosis is formed de novo from 1) adult stem cells located in the endometrial basalis that is involved in the cyclic regeneration of the endometrium4-6 or 2) adult stem cells displaced from bone marrow.7,8
Once adenomyosis is established, it is thought to progress by epithelial–mesenchymal transition,2 a process by which epithelial cells become highly motile mesenchymal cells that are capable of migration and invasion, due to loss of cell–cell adhesion properties.9
References
- Struble J, Reid S, Bedaiwy MA. Adenomyosis: a clinical review of a challenging gynecologic condition. J Minim Invasive Gynecol.2016; 23:164-185.
- García-Solares J, Donnez J, Donnez O, et al. Pathogenesis of uterine adenomyosis: invagination or metaplasia? Fertil Steril.2018;109:371-379.
- Ferenczy A. Pathophysiology of adenomyosis. Hum Reprod Update. 1998;4:312-322.
- Gargett CE. Uterine stem cells: what is the evidence? Hum Reprod Update. 2007;13:87-101.
- Chan RW, Schwab KE, Gargett CE. Clonogenicity of human endometrial epithelial and stromal cells. Biol Reprod. 2004;70:1738-1750.
- Schwab KE, Chan RWS, Gargett CE. Putative stem cell activity of human endometrial epithelial and stromal cells during the menstrual cycle. Fertil Steril. 2005;84(Suppl 2):1124-1130.
- Sasson IE, Taylor HS. Stem cells and the pathogenesis of endometriosis. Ann N Y Acad Sci. 2008;1127:106-115.
- Du H, Taylor HS. Stem cells and female reproduction. Reprod Sci. 2009;16:126-139.
- Acloque H, Adams MS, Fishwick K, et al. Epithelial-mesenchymal transitions: the importance of changing cell state in development and disease. J Clin Invest. 2009;119:1438-1449.
Continue to: In 57 women who underwent…
In 57 women who underwent this procedure, the mean operative time was 127 minutes; average estimated blood loss was 267 mL.40 Overall, laparoscopy with minilaparotomy was found to be a less technically difficult technique for laparoscopic myomectomy; allowed better closure of the uterine defect; and might have required less time to perform.3
We therefore advocate video laparoscopic wedge resection with or without robotic assistance, aided by minilaparotomy when necessary for safe removal of larger adenomyomas, as the preferred uterine-sparing surgical approach for focal adenomyosis or when the patient wants to preserve fertility (FIGURE 2). We think that this technique allows focal adenomyosis to be treated by wedge resection of the diseased myometrium, with subsequent closure of the remaining myometrial defect using a barbed V-Loc (Medtronic, Minneapolis, Minnesota) delayed absorbable suture in layers (FIGURE 3). Minilaparotomy can be utilized when indicated to aid removal of the resected myometrial specimen.
In our extensive experience, we have found that this technique provides significant relief of symptoms and improvements in fertility outcomes while minimizing surgical morbidity.
CASE Resolved
The patient underwent successful wedge resection of her adenomyosis by laparoscopy. She experienced nearly complete resolution of her symptoms of dysmenorrhea, menorrhagia, and pelvic pain. She retained good uterine integrity. Three years later, she and her husband became parents when she delivered their first child by cesarean delivery at full term. After she completed childbearing, she ultimately opted for minimally invasive hysterectomy.
The authors would like to acknowledge Mailinh Vu, MD, Fellow at Camran Nezhat Institute, for reviewing and editing this article.
CASE
A 28-year-old patient presents for evaluation and management of her chronic pelvic pain, dysmenorrhea, and menorrhagia. She previously tried ibuprofen with no pain relief. She also tried oral and long-acting reversible contraceptives but continued to be symptomatic. She underwent pelvic sonography, which demonstrated a large globular uterus with myometrial thickening and myometrial cysts with increased hypervascularity. Subsequent magnetic resonance imaging indicated a thickened junctional zone. Feeling she had exhausted medical manegement options with no significant improvement, she desired surgical treatment, but wanted to retain her future fertility. As a newlywed, she and her husband were planning on building a family so she desired to retain her uterus for potential future pregnancy.
How would you address this patient’s disruptive symptoms, while affirming her long-term plans by choosing the proper intervention?
Adenomyosis is characterized by endometrial-like glands and stroma deep within the myometrium of the uterus and generally is classified as diffuse or focal. This common, benign gynecologic condition is known to cause enlargement of the uterus secondary to stimulation of ectopic endometrial-like cells.1-3 Although the true incidence of adenomyosis is unknown because of the difficulty of making the diagnosis, prevalence has been variously reported at 6% to 70% among reproductive-aged women.4,5
In this review, we first examine the clinical presentation and diagnosis of adenomyosis. We then discuss clinical indications for, and surgical techniques of, adenomyomectomy, including our preferred uterine-sparing approach for focal disease or when the patient wants to preserve fertility: video laparoscopic resection with or without robotic assistance, aided by minilaparotomy when indicated.
Treatment evolved in a century and a half
Adenomyosis was first described more than 150 years ago; historically, hysterectomy was the mainstay of treatment.2,6 Conservative surgical treatment for adenomyosis has been reported since the early 1950s.6-8 Surgical treatment initially became more widespread following the introduction of wedge resection, which allowed for partial excision of adenomyotic nodules.9
More recent developments in diagnostic technologies and capabilities have allowed for the emergence of additional uterine-sparing and minimally invasive surgical treatment options for adenomyosis.3,10 Although the use of laparoscopic approaches is limited because a high level of technical skill is required to undertake these procedures, such approaches are becoming increasingly important as more and more patients seek fertility conservation.11-13
How does adenomyosis present?
Adenomyosis symptoms commonly consist of abnormal uterine bleeding and dysmenorrhea, affecting approximately 40% to 60% and 15% to 30% of patients with the condition, respectively.14 These symptoms are considered nonspecific because they are also associated with other uterine abnormalities.15 Although menorrhagia is not associated with extent of disease, dysmenorrhea is associated with both the number and depth of adenomyotic foci.14
Other symptoms reported with adenomyosis include chronic pelvic pain, dyspareunia, as well as infertility. Note, however, that a large percentage of patients are asymptomatic.16,17
On physical examination, patients commonly exhibit a diffusely enlarged, globular uterus. This finding is secondary to uniform hyperplasia and hypertrophy of the myometrium, caused by stimulation of ectopic endometrial cells.2 A subset of patients experience significant uterine tenderness.18 Other common findings associated with adenomyosis include uterine abnormalities, such as leiomyomata, endometriosis, and endometrial polyps.
Continue to: Two-pronged route to diagnosis and a differential...
Two-pronged route to diagnosis and a differential
Histology
Adenomyosis is definitively diagnosed based on histologic findings of endometrial-like tissue within the myometrium. Historically, histologic analysis was performed on specimens following hysterectomy but, more recently, has utilized specimens obtained from hysteroscopic and laparoscopic myometrial biopsies.19 Importantly, although hysteroscopic and laparoscopic biopsies are taken under direct visualization, there are no pathognomonic signs for adenomyosis; a diagnosis can therefore be missed if adenomyosis is not present at biopsied sites.1 The sensitivity of random biopsy at laparoscopy has been found to be as low as 2% to as high as 56%.20
Imaging
Imaging can be helpful in clinical decision making and to guide the differential diagnosis. Transvaginal ultrasonography (TVUS) is often the first mode of imaging used for the investigation of abnormal uterine bleeding or pelvic pain. Diagnosis by TVUS is difficult because the modality is operator dependent and standard diagnostic criteria are lacking.5
The most commonly reported ultrasonographic features of adenomyosis are21,22:
- a globally enlarged uterus
- asymmetry
- myometrial thickening with heterogeneity
- poorly defined foci of hyperechoic regions, surrounded by hypoechoic areas that correspond to smooth-muscle hyperplasia
- myometrial cysts.
Doppler ultrasound examination in patients with adenomyosis reveals increased flow to the myometrium without evidence of large blood vessels.
3-dimensional (3-D) ultrasonography. Integration of 3-D ultrasonography has allowed for identification of the thicker junctional zone that suggests adenomyosis. In a systematic review of the accuracy of TVUS, investigators reported a pooled sensitivity and specificity for 2-dimensional ultrasonography of 83.8% and 63.9%, respectively, and a pooled sensitivity and specificity for 3-dimensional ultrasonography of 88.9% and 56.0%, respectively.22
Magnetic resonance imaging (MRI) is also used in the evaluation of adenomyosis. Although MRI is considered a more accurate diagnostic modality because it is not operator dependent, expense often prohibits its use in the work-up of abnormal uterine bleeding and chronic pelvic pain.2,23
The most commonly reported MRI findings in adenomyosis include a globular or asymmetric uterus, heterogeneity of myometrial signal intensity, and thickening of the junctional zone24 (FIGURE 1). In a systematic review, researchers reported a pooled sensitivity and specificity of 77% and 89%, respectively, for the diagnosis of adenomyosis using MRI.25
Approaches to treatment
Medical management
No medical therapies or guidelines specific to the treatment of adenomyosis exist.9 Often, nonsteroidal anti-inflammatory drugs (NSAIDs) are employed to combat cramping and pain associated with increased prostaglandin levels.26 A systematic review found that NSAIDs are significantly better at treating dysmenorrhea than placebo alone.26
Moreover, adenomyosis is an estrogen-dependent disease; consequently, many medical treatments are targeted at suppressing the hypothalamic–pituitary–ovarian axis and inducing endometrial atrophy. Medications commonly used (off-label) for this effect include combined or progestin-only oral contraceptive pills, gonadotropin-releasing hormone (GnRH) agonists, levonorgestrel-releasing intrauterine devices, danazol, and aromatase inhibitors.
Use of a GnRH agonist, such as leuprolide, is limited to a short course (<6 months) because menopausal-like symptoms, such as hot flashes, vaginal atrophy, and loss of bone-mineral density, can develop.16 Symptoms of adenomyosis often return upon cessation of hormonal treatment.1
Novel therapies are under investigation, including GnRH antagonists, selective progesterone-receptor modulators, and antiplatelet therapy.27
Although there are few data showing the effectiveness of medical therapy on adenomyosis-specific outcomes, medications are particularly useful in patients who are poor surgical candidates or who may prefer not to undergo surgery. Furthermore, medical therapy has considerable use in conjunction with surgical intervention; a prospective observational study showed that women who underwent GnRH agonist treatment following surgery had significantly greater improvement of their dysmenorrhea and menorrhagia, compared with those who underwent surgery only.28 In addition, preoperative administration of a GnRH agonist or danazol several months prior to surgery has been shown to reduce uterine vascularity and, thus, blood loss at surgery.29,30
- Adenomyosis is common and benign, but remains underdiagnosed because of a nonspecific clinical presentation and lack of standardized diagnostic criteria.
- Adenomyosis can cause significant associated morbidity: dysmenorrhea, heavy menstrual bleeding, chronic pelvic pain, and infertility.
- High clinical suspicion warrants evaluation by imaging.
- Medical management is largely aimed at ameliorating symptoms.
- A patient who does not respond to medical treatment or does not desire pregnancy has a variety of surgical options; the extent of disease and the patient’s wish for uterine preservation guide the selection of surgical technique.
- Hysterectomy is the definitive treatment but, in patients who want to avoid radical resection, techniques developed for laparotomy are available, to allow conservative resection using laparoscopy.
- Ideally, surgery is performed using a combined laparoscopy and minilaparotomy approach, after appropriate imaging.
Continue to: Surgery
Surgery
The objective of surgical management is to ameliorate symptoms in a conservative manner, by excision or cytoreduction of adenomyotic lesions, while preserving, even improving, fertility.3,11,31 The choice of procedure depends, ultimately, on the location and extent of disease, the patient’s desire for uterine preservation and fertility, and surgical skill.3
Historically, hysterectomy was used to treat adenomyosis; for patients declining fertility preservation, hysterectomy remains the definitive treatment. Since the early 1950s, several techniques for laparotomic reduction have been developed. Surgeries that achieve partial reduction include:
Wedge resection of the uterine wall entails removal of the seromuscular layer at the identified location of adenomyotic tissue, with subsequent repair of the remaining muscular and serosal layers surrounding the wound.3,32 Because adenomyotic tissue can remain on either side of the incision in wedge resection, clinical improvement in symptoms of dysmenorrhea and menorrhagia are modest, and recurrence is possible.7
Modified reduction surgery. Modifications of reduction surgery include slicing adenomyotic tissue using microsurgery and partial excision.33
Transverse-H incision of the uterine wall involves a transverse incision on the uterine fundus, separating serosa and myometrium, followed by removal of diseased tissue using an electrosurgical scalpel or scissors. Tensionless suturing is used to close the myometrial layers in 1 or 2 layers to establish hemostasis and close the defect; serosal flaps are closed with subserosal interrupted sutures.34 Data show that, following surgery with this technique, 21.4% to 38.7% of patients who attempt conception achieve clinical pregnancy.7
Complete, conservative resection in cases of diffuse and focal adenomyosis is possible using the triple-flap method, in which total resection is achieved by removing diseased myometrium until healthy, soft tissue—with normal texture, color, and vascularity—is reached.2 Repair with this technique reduces the risk of uterine rupture by reconstructing the uterine wall using a muscle flap prepared by metroplasty.7 In a study of 64 women who underwent triple-flap resection, a clinical pregnancy rate of 74% and a live birth rate of 52% were reported.7
Minimally invasive approaches. Although several techniques have been developed for focal excision of adenomyosis by laparotomy,7 the trend has been toward minimally invasive surgery, which reduces estimated blood loss, decreases length of stay, and reduces adhesion formation—all without a statistically significant difference in long-term clinical outcomes, compared to other techniques.35-39 Furthermore, enhanced visualization of pelvic organs provided by laparoscopy is vital in the case of adenomyosis.3,31
How our group approaches surgical management. A challenge in laparoscopic surgery of adenomyosis is extraction of an extensive amount of diseased tissue. In 1994, our group described the use of simultaneous operative laparoscopy and minilaparotomy technique as an effective and safe alternative to laparotomy in the treatment of myomectomy6; the surgical principles of that approach are applied to adenomyomectomy. The technique involves treatment of pelvic pathology with laparoscopy, removal of tissue through the minilaparotomy incision, and repair of the uterine wall defect in layers.
How adenomyosis originates is not fully understood. Several theories have been proposed, however (including, more prominently, the first 2 below):
Invasion theory. The endometrial basalis layer invaginates and invades the myometrium1,2 (FIGURE); the etiology of invagination remains unknown.
Reaction theory. Myometrial weakness or dysfunction, brought on by trauma from previous uterine surgery or pregnancy, could predispose uterine musculature to deep invasion.3
Metaplasia theory. Adenomyosis is a result of metaplasia of pluripotent Müllerian rests.
Müllerian remnant theory. Related to the Müllerian metaplasia theory, adenomyosis is formed de novo from 1) adult stem cells located in the endometrial basalis that is involved in the cyclic regeneration of the endometrium4-6 or 2) adult stem cells displaced from bone marrow.7,8
Once adenomyosis is established, it is thought to progress by epithelial–mesenchymal transition,2 a process by which epithelial cells become highly motile mesenchymal cells that are capable of migration and invasion, due to loss of cell–cell adhesion properties.9
References
- Struble J, Reid S, Bedaiwy MA. Adenomyosis: a clinical review of a challenging gynecologic condition. J Minim Invasive Gynecol.2016; 23:164-185.
- García-Solares J, Donnez J, Donnez O, et al. Pathogenesis of uterine adenomyosis: invagination or metaplasia? Fertil Steril.2018;109:371-379.
- Ferenczy A. Pathophysiology of adenomyosis. Hum Reprod Update. 1998;4:312-322.
- Gargett CE. Uterine stem cells: what is the evidence? Hum Reprod Update. 2007;13:87-101.
- Chan RW, Schwab KE, Gargett CE. Clonogenicity of human endometrial epithelial and stromal cells. Biol Reprod. 2004;70:1738-1750.
- Schwab KE, Chan RWS, Gargett CE. Putative stem cell activity of human endometrial epithelial and stromal cells during the menstrual cycle. Fertil Steril. 2005;84(Suppl 2):1124-1130.
- Sasson IE, Taylor HS. Stem cells and the pathogenesis of endometriosis. Ann N Y Acad Sci. 2008;1127:106-115.
- Du H, Taylor HS. Stem cells and female reproduction. Reprod Sci. 2009;16:126-139.
- Acloque H, Adams MS, Fishwick K, et al. Epithelial-mesenchymal transitions: the importance of changing cell state in development and disease. J Clin Invest. 2009;119:1438-1449.
Continue to: In 57 women who underwent…
In 57 women who underwent this procedure, the mean operative time was 127 minutes; average estimated blood loss was 267 mL.40 Overall, laparoscopy with minilaparotomy was found to be a less technically difficult technique for laparoscopic myomectomy; allowed better closure of the uterine defect; and might have required less time to perform.3
We therefore advocate video laparoscopic wedge resection with or without robotic assistance, aided by minilaparotomy when necessary for safe removal of larger adenomyomas, as the preferred uterine-sparing surgical approach for focal adenomyosis or when the patient wants to preserve fertility (FIGURE 2). We think that this technique allows focal adenomyosis to be treated by wedge resection of the diseased myometrium, with subsequent closure of the remaining myometrial defect using a barbed V-Loc (Medtronic, Minneapolis, Minnesota) delayed absorbable suture in layers (FIGURE 3). Minilaparotomy can be utilized when indicated to aid removal of the resected myometrial specimen.
In our extensive experience, we have found that this technique provides significant relief of symptoms and improvements in fertility outcomes while minimizing surgical morbidity.
CASE Resolved
The patient underwent successful wedge resection of her adenomyosis by laparoscopy. She experienced nearly complete resolution of her symptoms of dysmenorrhea, menorrhagia, and pelvic pain. She retained good uterine integrity. Three years later, she and her husband became parents when she delivered their first child by cesarean delivery at full term. After she completed childbearing, she ultimately opted for minimally invasive hysterectomy.
The authors would like to acknowledge Mailinh Vu, MD, Fellow at Camran Nezhat Institute, for reviewing and editing this article.
- Garcia L, Isaacson K. Adenomyosis: review of the literature. J Minim Invasive Gynecol. 2011;18:428-437.
- Nezhat C, Nezhat F, Nezhat C, eds. Nezhat's Video-Assisted and Robotic-Assisted Laparoscopy and Hysteroscopy. 4th ed. Cambridge, UK: Cambridge University Press; 2013.
- Osada H. Uterine adenomyosis and adenomyoma: the surgical approach. Fertil Steril. 2018;109:406-417.
- Azziz R. Adenomyosis: current perspectives. Obstet Gynecol Clin North Am. 1989;16:221-235.
- Struble J, Reid S, Bedaiwy MA. Adenomyosis: A clinical review of a challenging gynecologic condition. J Minim Invasive Gynecol. 2016;23:164-185.
- Rokitansky C. Ueber Uterusdrsen-Neubildung in Uterus- und Ovarial-Sarcomen. Gesellschaft der Ärzte in Wien. 1860;16:1-4.
- Osada H. Uterine adenomyosis and adenomyoma: the surgical approach. Fertil Steril. 2018;109:406-417.
- Van Praagh I. Conservative surgical treatment for adenomyosis uteri in young women: local excision and metroplasty. Can Med Assoc J. 1965;93:1174-1175.
- Donnez J, Donnez O, Dolmans MM. Introduction: Uterine adenomyosis, another enigmatic disease of our time. Fertil Steril. 2018;109:369-370.
- Nishida M, Takano K, Arai Y, et al. Conservative surgical management for diffuse uterine adenomyosis. Fertil Steril. 2010;94:715-719.
- Abbott JA. Adenomyosis and abnormal uterine bleeding (AUB-A)--Pathogenesis, diagnosis, and management. Best Pract Res Clin Obstet Gynaecol. 2017;40:68-81.
- Matalliotakis IM, Katsikis IK, Panidis DK. Adenomyosis: what is the impact on fertility? Curr Opin Obstet Gynecol. 2005;17:261-264.
- Devlieger R, D'Hooghe T, Timmerman D. Uterine adenomyosis in the infertility clinic. Hum Reprod Update. 2003;9:139-147.
- Levgur M, Abadi MA, Tucker A. Adenomyosis: symptoms, histology, and pregnancy terminations. Obstet Gynecol. 2000;95:688-691.
- Weiss G, Maseelall P, Schott LL, et al. Adenomyosis a variant, not a disease? Evidence from hysterectomized menopausal women in the Study of Women's Health Across the Nation (SWAN). Fertil Steril. 2009;91:201-206.
- Huang F, Kung FT, Chang SY, et al. Effects of short-course buserelin therapy on adenomyosis. A report of two cases. J Reprod Med. 1999;44:741-744.
- Benson RC, Sneeden VD. Adenomyosis: a reappraisal of symptomatology. Am J Obstet Gynecol. 1958;76:1044-1061.
- Shrestha A, Sedai LB. Understanding clinical features of adenomyosis: a case control study. Nepal Med Coll J. 2012;14:176-179.
- Fernández C, Ricci P, Fernández E. Adenomyosis visualized during hysteroscopy. J Minim Invasive Gynecol. 2007;14:555-556.
- Brosens JJ, Barker FG. The role of myometrial needle biopsies in the diagnosis of adenomyosis. Fertil Steril. 1995;63:1347-1349.
- Van den Bosch T, Van Schoubroeck D. Ultrasound diagnosis of endometriosis and adenomyosis: state of the art. Best Pract Res Clin Obstet Gynaecol. 2018;51:16-24.
- Andres MP, Borrelli GM, Ribeiro J, et al. Transvaginal ultrasound for the diagnosis of adenomyosis: systematic review and meta-analysis. J Minim Invasive Gynecol. 2018;25:257-264.
- Bazot M, Cortez A, Darai E, et al. Ultrasonography compared with magnetic resonance imaging for the diagnosis of adenomyosis: correlation with histopathology. Hum Reprod. 2001;16:2427-2433.
- Bragheto AM, Caserta N, Bahamondes L, et al. Effectiveness of the levonorgestrel-releasing intrauterine system in the treatment of adenomyosis diagnosed and monitored by magnetic resonance imaging. Contraception. 2007;76:195-199.
- Champaneria R, Abedin P, Daniels J, et al. Ultrasound scan and magnetic resonance imaging for the diagnosis of adenomyosis: systematic review comparing test accuracy. Acta Obstet Gynecol Scand. 2010; 89:1374-1384.
- Marjoribanks J, Proctor M, Farquhar C, et al. Nonsteroidal anti-inflammatory drugs for dysmenorrhoea. Cochrane Database Syst Rev. 2010;(1):CD001751.
- Vannuccini S, Luisi S, Tosti C, et al. Role of medical therapy in the management of uterine adenomyosis. Fertil Steril. 2018;109:398-405.
- Wang PH, Liu WM, Fuh JL, et al. Comparison of surgery alone and combined surgical-medical treatment in the management of symptomatic uterine adenomyoma. Fertil Steril. 2009;92:876-885.
- Wood C, Maher P, Woods R. Laparoscopic surgical techniques for endometriosis and adenomyosis. Diagn Ther Endosc. 2000;6:153-168.
- Wang CJ, Yuen LT, Chang SD, et al. Use of laparoscopic cytoreductive surgery to treat infertile women with localized adenomyosis. Fertil Steril. 2006;86:462.e5-e8.
- Nezhat C, Hajhosseini B, King LP. Robotic-assisted laparoscopic treatment of bowel, bladder, and ureteral endometriosis. JSLS. 2011;15:387-392.
- Sun A, Luo M, Wang W, et al. Characteristics and efficacy of modified adenomyomectomy in the treatment of uterine adenomyoma. Chin Med J. 2011;124:1322-1326.
- Fedele L, Bianchi S, Zanotti F, et al. Surgery: Fertility after conservative surgery for adenomyomas. Hum Reprod. 1993;8:1708-1710.
- Fujishita A, Masuzaki H, Khan KN, et al. Modified reduction surgery for adenomyosis. A preliminary report of the transverse H incision technique. Gynecol Obstet Invest. 2004;57:132-138.
- Operative Laparoscopy Study Group. Postoperative adhesion development after operative laparoscopy: evaluation at early second-look procedures. Fertil Steril. 1991;55:700-704.
- Luciano AA, Maier DB, Koch EI, et al. A comparative study of postoperative adhesions following laser surgery by laparoscopy versus laparotomy in the rabbit model. Obstet Gynecol. 1989;74:220-224.
- Lundorff P, Hahlin M, Källfelt B, et al. Adhesion formation after laparoscopic surgery in tubal pregnancy: a randomized trial versus laparotomy. Fertil Steril. 1991;55:911-915.
- Kwack JY, Kwon YS. Laparoscopic surgery for focal adenomyosis. JSLS. 2017;21. pii:e2017.00014.
- Podratz K. Degrees of Freedom: Advances in Gynecological and Obstetrical Surgery. Remembering Milestones and Achievements in Surgery: Inspiring Quality for a Hundred Years 1913-2012. Chicago, IL: American College of Surgeons; 2012.
- Nezhat C, Nezhat F, Bess O, et al. Laparoscopically assisted myomectomy: a report of a new technique in 57 cases. Int J Fertil Menopausal Stud. 1994;39:39-44.
- Garcia L, Isaacson K. Adenomyosis: review of the literature. J Minim Invasive Gynecol. 2011;18:428-437.
- Nezhat C, Nezhat F, Nezhat C, eds. Nezhat's Video-Assisted and Robotic-Assisted Laparoscopy and Hysteroscopy. 4th ed. Cambridge, UK: Cambridge University Press; 2013.
- Osada H. Uterine adenomyosis and adenomyoma: the surgical approach. Fertil Steril. 2018;109:406-417.
- Azziz R. Adenomyosis: current perspectives. Obstet Gynecol Clin North Am. 1989;16:221-235.
- Struble J, Reid S, Bedaiwy MA. Adenomyosis: A clinical review of a challenging gynecologic condition. J Minim Invasive Gynecol. 2016;23:164-185.
- Rokitansky C. Ueber Uterusdrsen-Neubildung in Uterus- und Ovarial-Sarcomen. Gesellschaft der Ärzte in Wien. 1860;16:1-4.
- Osada H. Uterine adenomyosis and adenomyoma: the surgical approach. Fertil Steril. 2018;109:406-417.
- Van Praagh I. Conservative surgical treatment for adenomyosis uteri in young women: local excision and metroplasty. Can Med Assoc J. 1965;93:1174-1175.
- Donnez J, Donnez O, Dolmans MM. Introduction: Uterine adenomyosis, another enigmatic disease of our time. Fertil Steril. 2018;109:369-370.
- Nishida M, Takano K, Arai Y, et al. Conservative surgical management for diffuse uterine adenomyosis. Fertil Steril. 2010;94:715-719.
- Abbott JA. Adenomyosis and abnormal uterine bleeding (AUB-A)--Pathogenesis, diagnosis, and management. Best Pract Res Clin Obstet Gynaecol. 2017;40:68-81.
- Matalliotakis IM, Katsikis IK, Panidis DK. Adenomyosis: what is the impact on fertility? Curr Opin Obstet Gynecol. 2005;17:261-264.
- Devlieger R, D'Hooghe T, Timmerman D. Uterine adenomyosis in the infertility clinic. Hum Reprod Update. 2003;9:139-147.
- Levgur M, Abadi MA, Tucker A. Adenomyosis: symptoms, histology, and pregnancy terminations. Obstet Gynecol. 2000;95:688-691.
- Weiss G, Maseelall P, Schott LL, et al. Adenomyosis a variant, not a disease? Evidence from hysterectomized menopausal women in the Study of Women's Health Across the Nation (SWAN). Fertil Steril. 2009;91:201-206.
- Huang F, Kung FT, Chang SY, et al. Effects of short-course buserelin therapy on adenomyosis. A report of two cases. J Reprod Med. 1999;44:741-744.
- Benson RC, Sneeden VD. Adenomyosis: a reappraisal of symptomatology. Am J Obstet Gynecol. 1958;76:1044-1061.
- Shrestha A, Sedai LB. Understanding clinical features of adenomyosis: a case control study. Nepal Med Coll J. 2012;14:176-179.
- Fernández C, Ricci P, Fernández E. Adenomyosis visualized during hysteroscopy. J Minim Invasive Gynecol. 2007;14:555-556.
- Brosens JJ, Barker FG. The role of myometrial needle biopsies in the diagnosis of adenomyosis. Fertil Steril. 1995;63:1347-1349.
- Van den Bosch T, Van Schoubroeck D. Ultrasound diagnosis of endometriosis and adenomyosis: state of the art. Best Pract Res Clin Obstet Gynaecol. 2018;51:16-24.
- Andres MP, Borrelli GM, Ribeiro J, et al. Transvaginal ultrasound for the diagnosis of adenomyosis: systematic review and meta-analysis. J Minim Invasive Gynecol. 2018;25:257-264.
- Bazot M, Cortez A, Darai E, et al. Ultrasonography compared with magnetic resonance imaging for the diagnosis of adenomyosis: correlation with histopathology. Hum Reprod. 2001;16:2427-2433.
- Bragheto AM, Caserta N, Bahamondes L, et al. Effectiveness of the levonorgestrel-releasing intrauterine system in the treatment of adenomyosis diagnosed and monitored by magnetic resonance imaging. Contraception. 2007;76:195-199.
- Champaneria R, Abedin P, Daniels J, et al. Ultrasound scan and magnetic resonance imaging for the diagnosis of adenomyosis: systematic review comparing test accuracy. Acta Obstet Gynecol Scand. 2010; 89:1374-1384.
- Marjoribanks J, Proctor M, Farquhar C, et al. Nonsteroidal anti-inflammatory drugs for dysmenorrhoea. Cochrane Database Syst Rev. 2010;(1):CD001751.
- Vannuccini S, Luisi S, Tosti C, et al. Role of medical therapy in the management of uterine adenomyosis. Fertil Steril. 2018;109:398-405.
- Wang PH, Liu WM, Fuh JL, et al. Comparison of surgery alone and combined surgical-medical treatment in the management of symptomatic uterine adenomyoma. Fertil Steril. 2009;92:876-885.
- Wood C, Maher P, Woods R. Laparoscopic surgical techniques for endometriosis and adenomyosis. Diagn Ther Endosc. 2000;6:153-168.
- Wang CJ, Yuen LT, Chang SD, et al. Use of laparoscopic cytoreductive surgery to treat infertile women with localized adenomyosis. Fertil Steril. 2006;86:462.e5-e8.
- Nezhat C, Hajhosseini B, King LP. Robotic-assisted laparoscopic treatment of bowel, bladder, and ureteral endometriosis. JSLS. 2011;15:387-392.
- Sun A, Luo M, Wang W, et al. Characteristics and efficacy of modified adenomyomectomy in the treatment of uterine adenomyoma. Chin Med J. 2011;124:1322-1326.
- Fedele L, Bianchi S, Zanotti F, et al. Surgery: Fertility after conservative surgery for adenomyomas. Hum Reprod. 1993;8:1708-1710.
- Fujishita A, Masuzaki H, Khan KN, et al. Modified reduction surgery for adenomyosis. A preliminary report of the transverse H incision technique. Gynecol Obstet Invest. 2004;57:132-138.
- Operative Laparoscopy Study Group. Postoperative adhesion development after operative laparoscopy: evaluation at early second-look procedures. Fertil Steril. 1991;55:700-704.
- Luciano AA, Maier DB, Koch EI, et al. A comparative study of postoperative adhesions following laser surgery by laparoscopy versus laparotomy in the rabbit model. Obstet Gynecol. 1989;74:220-224.
- Lundorff P, Hahlin M, Källfelt B, et al. Adhesion formation after laparoscopic surgery in tubal pregnancy: a randomized trial versus laparotomy. Fertil Steril. 1991;55:911-915.
- Kwack JY, Kwon YS. Laparoscopic surgery for focal adenomyosis. JSLS. 2017;21. pii:e2017.00014.
- Podratz K. Degrees of Freedom: Advances in Gynecological and Obstetrical Surgery. Remembering Milestones and Achievements in Surgery: Inspiring Quality for a Hundred Years 1913-2012. Chicago, IL: American College of Surgeons; 2012.
- Nezhat C, Nezhat F, Bess O, et al. Laparoscopically assisted myomectomy: a report of a new technique in 57 cases. Int J Fertil Menopausal Stud. 1994;39:39-44.
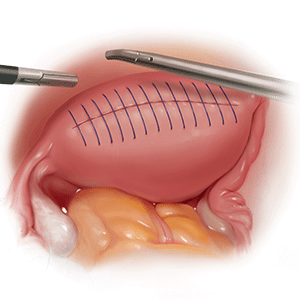
Intensive insulin added no benefit for hyperglycemia after ischemic stroke
HONOLULU – In patients who were hyperglycemic following an acute ischemic stroke, intensive insulin control using a continuous insulin drip and an aggressive blood glucose target of 80-130 mg/dL provided no incremental benefit in clinical outcome, compared with a more standard approach of serial, subcutaneous insulin injections and a moderate blood glucose target in a multicenter, U.S. trial with more than 1,100 patients.

The results also highlighted the potential downside to aggressive insulin treatment, with an associated 2.6% incidence of severe hypoglycemia, defined as blood glucose falling below 40 mg/dL, Karen C. Johnston, MD, said at the International Stroke Conference sponsored by the American Heart Association.
“Our data suggest that subcutaneously administered insulin with a target blood glucose level of less than 180 mg/dL is the preferred treatment” because it produces similar efficacy without causing any episodes of severe hypoglycemia, concluded Dr. Johnston, professor and chair of neurology at the University of Virginia in Charlottesville. “There should be no further debate” over the potential superiority of a glucose target substantially below 180 mg/dL, she added in an interview.
Continuing to use a glucose target of less than 180 mg/dL and treating patients with subcutaneous insulin injections every 6 hours to achieve this will mean substantially less resource use and precludes the need for keeping patients in intensive care beds as is needed with an insulin drip, Dr. Johnston noted. A treatment target of less than 180 mg/dL is also consistent with the most recent American Heart Association stroke treatment guidelines, which listed a blood glucose target of 140-180 mg/dL as a class IIa recommendation (Stroke. 2018 March;49[3]:e66-99).
The SHINE (Stroke Hyperglycemia Insulin Network Effort) trial enrolled 1,151 adults diagnosed with an acute ischemic stroke at 63 U.S. centers during 2012-2018, excluding patients with type 1 diabetes. Patients had to enter the study within 12 hours of their last known well time, and with an elevated blood glucose level, above 110 mg/dL in patients with type 2 diabetes or at or above 150 mg/dL in other patients. The median glucose level of enrolled patients was about 188 mg/dL. Enrolled patients averaged 66 years old, and about 80% had type 2 diabetes. The median time from last known well to randomization was just over 7 hours. Almost two-thirds of the patients received thrombolytic treatment, and about 13% underwent thrombectomy.
During up to 72 hours of treatment following enrollment the patients in the standard-treatment arm showed a fairly steady average blood glucose level of 179 mg/dL; patients in the intensive arm showed a steady average of 118 mg/dL.
The study’s primary end point was the percentage of patients with a favorable outcome 90 days after enrollment based on their modified Rankin scale score at that time, with the scores that qualified for this end point varying depending on stroke severity at baseline. The percentage of patients achieving this was 20.5% among the intensive patients and 21.6% among those who received standard insulin treatment, a difference that was not statistically significant.
The findings left open the question of how to better manage acute ischemic stroke patients who present with hyperglycemia.
“Hyperglycemic stroke patients have worse outcomes than stroke patients without hyperglycemia. More aggressively treating the hyperglycemia did not help these patients, We need to figure out what will help them,” Dr. Johnson said.
SOURCE: Johnston KC et al. ISC 2019, Abstract LB1.
SHINE was a well-designed trial that was run with a high degree of rigor, and its results advance the field. The results left no doubt that the result was neutral, that , while resulting in an excess of severe hypoglycemia episodes.

Using a less intensive insulin regimen that does not require a continuous drip is easier. The question of how aggressive treatment needs to be when managing glucose in acute ischemic stroke patients is something that U.S. clinicians who care for stroke patients argue about virtually daily. At my center, Cedars-Sinai in Los Angeles, we have recently used an approach that blended standard insulin treatment with more aggressive treatment. The SHINE results may not be practice changing, but they will be argument changing. The new results will make a difference. We will now stop arguing. We now know what we need to do.
Patrick D. Lyden, MD , is professor and chair of neurology at Cedars-Sinai Medical Center in Los Angeles. He had no relevant disclosures. He made these comments in an interview.
SHINE was a well-designed trial that was run with a high degree of rigor, and its results advance the field. The results left no doubt that the result was neutral, that , while resulting in an excess of severe hypoglycemia episodes.
Using a less intensive insulin regimen that does not require a continuous drip is easier. The question of how aggressive treatment needs to be when managing glucose in acute ischemic stroke patients is something that U.S. clinicians who care for stroke patients argue about virtually daily. At my center, Cedars-Sinai in Los Angeles, we have recently used an approach that blended standard insulin treatment with more aggressive treatment. The SHINE results may not be practice changing, but they will be argument changing. The new results will make a difference. We will now stop arguing. We now know what we need to do.
Patrick D. Lyden, MD , is professor and chair of neurology at Cedars-Sinai Medical Center in Los Angeles. He had no relevant disclosures. He made these comments in an interview.
SHINE was a well-designed trial that was run with a high degree of rigor, and its results advance the field. The results left no doubt that the result was neutral, that , while resulting in an excess of severe hypoglycemia episodes.
Using a less intensive insulin regimen that does not require a continuous drip is easier. The question of how aggressive treatment needs to be when managing glucose in acute ischemic stroke patients is something that U.S. clinicians who care for stroke patients argue about virtually daily. At my center, Cedars-Sinai in Los Angeles, we have recently used an approach that blended standard insulin treatment with more aggressive treatment. The SHINE results may not be practice changing, but they will be argument changing. The new results will make a difference. We will now stop arguing. We now know what we need to do.
Patrick D. Lyden, MD , is professor and chair of neurology at Cedars-Sinai Medical Center in Los Angeles. He had no relevant disclosures. He made these comments in an interview.
HONOLULU – In patients who were hyperglycemic following an acute ischemic stroke, intensive insulin control using a continuous insulin drip and an aggressive blood glucose target of 80-130 mg/dL provided no incremental benefit in clinical outcome, compared with a more standard approach of serial, subcutaneous insulin injections and a moderate blood glucose target in a multicenter, U.S. trial with more than 1,100 patients.
The results also highlighted the potential downside to aggressive insulin treatment, with an associated 2.6% incidence of severe hypoglycemia, defined as blood glucose falling below 40 mg/dL, Karen C. Johnston, MD, said at the International Stroke Conference sponsored by the American Heart Association.
“Our data suggest that subcutaneously administered insulin with a target blood glucose level of less than 180 mg/dL is the preferred treatment” because it produces similar efficacy without causing any episodes of severe hypoglycemia, concluded Dr. Johnston, professor and chair of neurology at the University of Virginia in Charlottesville. “There should be no further debate” over the potential superiority of a glucose target substantially below 180 mg/dL, she added in an interview.
Continuing to use a glucose target of less than 180 mg/dL and treating patients with subcutaneous insulin injections every 6 hours to achieve this will mean substantially less resource use and precludes the need for keeping patients in intensive care beds as is needed with an insulin drip, Dr. Johnston noted. A treatment target of less than 180 mg/dL is also consistent with the most recent American Heart Association stroke treatment guidelines, which listed a blood glucose target of 140-180 mg/dL as a class IIa recommendation (Stroke. 2018 March;49[3]:e66-99).
The SHINE (Stroke Hyperglycemia Insulin Network Effort) trial enrolled 1,151 adults diagnosed with an acute ischemic stroke at 63 U.S. centers during 2012-2018, excluding patients with type 1 diabetes. Patients had to enter the study within 12 hours of their last known well time, and with an elevated blood glucose level, above 110 mg/dL in patients with type 2 diabetes or at or above 150 mg/dL in other patients. The median glucose level of enrolled patients was about 188 mg/dL. Enrolled patients averaged 66 years old, and about 80% had type 2 diabetes. The median time from last known well to randomization was just over 7 hours. Almost two-thirds of the patients received thrombolytic treatment, and about 13% underwent thrombectomy.
During up to 72 hours of treatment following enrollment the patients in the standard-treatment arm showed a fairly steady average blood glucose level of 179 mg/dL; patients in the intensive arm showed a steady average of 118 mg/dL.
The study’s primary end point was the percentage of patients with a favorable outcome 90 days after enrollment based on their modified Rankin scale score at that time, with the scores that qualified for this end point varying depending on stroke severity at baseline. The percentage of patients achieving this was 20.5% among the intensive patients and 21.6% among those who received standard insulin treatment, a difference that was not statistically significant.
The findings left open the question of how to better manage acute ischemic stroke patients who present with hyperglycemia.
“Hyperglycemic stroke patients have worse outcomes than stroke patients without hyperglycemia. More aggressively treating the hyperglycemia did not help these patients, We need to figure out what will help them,” Dr. Johnson said.
SOURCE: Johnston KC et al. ISC 2019, Abstract LB1.
HONOLULU – In patients who were hyperglycemic following an acute ischemic stroke, intensive insulin control using a continuous insulin drip and an aggressive blood glucose target of 80-130 mg/dL provided no incremental benefit in clinical outcome, compared with a more standard approach of serial, subcutaneous insulin injections and a moderate blood glucose target in a multicenter, U.S. trial with more than 1,100 patients.
The results also highlighted the potential downside to aggressive insulin treatment, with an associated 2.6% incidence of severe hypoglycemia, defined as blood glucose falling below 40 mg/dL, Karen C. Johnston, MD, said at the International Stroke Conference sponsored by the American Heart Association.
“Our data suggest that subcutaneously administered insulin with a target blood glucose level of less than 180 mg/dL is the preferred treatment” because it produces similar efficacy without causing any episodes of severe hypoglycemia, concluded Dr. Johnston, professor and chair of neurology at the University of Virginia in Charlottesville. “There should be no further debate” over the potential superiority of a glucose target substantially below 180 mg/dL, she added in an interview.
Continuing to use a glucose target of less than 180 mg/dL and treating patients with subcutaneous insulin injections every 6 hours to achieve this will mean substantially less resource use and precludes the need for keeping patients in intensive care beds as is needed with an insulin drip, Dr. Johnston noted. A treatment target of less than 180 mg/dL is also consistent with the most recent American Heart Association stroke treatment guidelines, which listed a blood glucose target of 140-180 mg/dL as a class IIa recommendation (Stroke. 2018 March;49[3]:e66-99).
The SHINE (Stroke Hyperglycemia Insulin Network Effort) trial enrolled 1,151 adults diagnosed with an acute ischemic stroke at 63 U.S. centers during 2012-2018, excluding patients with type 1 diabetes. Patients had to enter the study within 12 hours of their last known well time, and with an elevated blood glucose level, above 110 mg/dL in patients with type 2 diabetes or at or above 150 mg/dL in other patients. The median glucose level of enrolled patients was about 188 mg/dL. Enrolled patients averaged 66 years old, and about 80% had type 2 diabetes. The median time from last known well to randomization was just over 7 hours. Almost two-thirds of the patients received thrombolytic treatment, and about 13% underwent thrombectomy.
During up to 72 hours of treatment following enrollment the patients in the standard-treatment arm showed a fairly steady average blood glucose level of 179 mg/dL; patients in the intensive arm showed a steady average of 118 mg/dL.
The study’s primary end point was the percentage of patients with a favorable outcome 90 days after enrollment based on their modified Rankin scale score at that time, with the scores that qualified for this end point varying depending on stroke severity at baseline. The percentage of patients achieving this was 20.5% among the intensive patients and 21.6% among those who received standard insulin treatment, a difference that was not statistically significant.
The findings left open the question of how to better manage acute ischemic stroke patients who present with hyperglycemia.
“Hyperglycemic stroke patients have worse outcomes than stroke patients without hyperglycemia. More aggressively treating the hyperglycemia did not help these patients, We need to figure out what will help them,” Dr. Johnson said.
SOURCE: Johnston KC et al. ISC 2019, Abstract LB1.
REPORTING FROM ISC 2019
Key clinical point: Aggressive insulin management of hyperglycemia following an ischemic stroke gave no clinical benefit, compared with a standard approach.
Major finding: After 90 days, favorable outcomes occurred in 21% of patients on aggressive insulin treatment and 22% on standard treatment.
Study details: SHINE, a multicenter, randomized trial with 1,151 acute ischemic stroke patients.
Disclosures: SHINE received no commercial funding. Dr. Johnston had no disclosures.
Source: Johnston KC et al. ISC 2019, Abstract LB1.
New cryoablating catheter shows promising AF efficacy, safety
BOSTON – An ultra-low-temperature ablation catheter was safe and effective in the first 48 atrial fibrillation (AF) patients to undergo treatment with the device.

The ultra-low-temperature catheter, cooled by liquid nitrogen to –196° C, showed excellent safety and a high success rate, in the modest number of patients who have been followed for 6 or 12 months, Tom De Potter, MD, said at the annual International AF Symposium. The catheter is capable of delivering both focal and linear lesions, said Dr. De Potter, a cardiac electrophysiologist at the Cardiovascular Center of OLV Hospital in Aalst, Belgium.
He reported results on the first 48 AF patients treated with the catheter at either his center or at St. Antonius Hospital in Nieuwegein, the Netherlands, in the CryoCure2 (Investigation of the Adagio Cryoablation System in Patients With Atrial Fibrillation) study. The investigators included safety findings only from the first 13 patients treated, but they assessed both safety and efficacy for the following 35 patients.
The safety review showed one patient with a groin-puncture injury, and two patients with phrenic nerve palsy, but no cases of phrenic nerve palsy in the most recent 41 patients who were treated with an updated version of the catheter that included a cryomapping feature. None of the 48 patients had a stroke, transient ischemic attack, esophageal injury, tamponade, or MI.
The 35 patients reviewed for efficacy included 10 patients with paroxysmal AF and 25 with persistent AF. All five of the paroxysmal AF patients followed for at least 6 months, and all four of those patients followed for 12 months, showed no AF recurrences. One of the persistent AF patients never achieved cardioversion at the time of the ablation procedure. All 17 other persistent AF patients followed for at least 6 months remained in sinus rhythm at 6 months. Among the eight of these patients followed for at least 12 months after treatment, one patient had AF recurrence, so the current 12-month rate of freedom from recurrence is seven of nine patients (including the one who never achieved cardioversion), or 78%.
The average procedure time to perform pulmonary vein isolation (PVI) only was 106 minutes, and procedure time was 116 minutes in the patients who underwent PVI plus additional ablation procedures. Average ablation time was 12 minutes among those just having PVI, and 14 minutes in those who underwent PVI plus other ablations. The cryoablation catheter comes with 20 electrodes that allow it to also record electrograms.
The attraction of the ultra-low-temperature cryoablation catheter used in the study is it “can achieve complete PVI considerably faster” than other ablation methods while also achieving “unsurpassed efficacy,” Dr. De Potter said in a written statement. In addition, “the new, adjustable diagnostic capacity simplifies the procedure and makes it much less operator dependent,” he added.
BOSTON – An ultra-low-temperature ablation catheter was safe and effective in the first 48 atrial fibrillation (AF) patients to undergo treatment with the device.
The ultra-low-temperature catheter, cooled by liquid nitrogen to –196° C, showed excellent safety and a high success rate, in the modest number of patients who have been followed for 6 or 12 months, Tom De Potter, MD, said at the annual International AF Symposium. The catheter is capable of delivering both focal and linear lesions, said Dr. De Potter, a cardiac electrophysiologist at the Cardiovascular Center of OLV Hospital in Aalst, Belgium.
He reported results on the first 48 AF patients treated with the catheter at either his center or at St. Antonius Hospital in Nieuwegein, the Netherlands, in the CryoCure2 (Investigation of the Adagio Cryoablation System in Patients With Atrial Fibrillation) study. The investigators included safety findings only from the first 13 patients treated, but they assessed both safety and efficacy for the following 35 patients.
The safety review showed one patient with a groin-puncture injury, and two patients with phrenic nerve palsy, but no cases of phrenic nerve palsy in the most recent 41 patients who were treated with an updated version of the catheter that included a cryomapping feature. None of the 48 patients had a stroke, transient ischemic attack, esophageal injury, tamponade, or MI.
The 35 patients reviewed for efficacy included 10 patients with paroxysmal AF and 25 with persistent AF. All five of the paroxysmal AF patients followed for at least 6 months, and all four of those patients followed for 12 months, showed no AF recurrences. One of the persistent AF patients never achieved cardioversion at the time of the ablation procedure. All 17 other persistent AF patients followed for at least 6 months remained in sinus rhythm at 6 months. Among the eight of these patients followed for at least 12 months after treatment, one patient had AF recurrence, so the current 12-month rate of freedom from recurrence is seven of nine patients (including the one who never achieved cardioversion), or 78%.
The average procedure time to perform pulmonary vein isolation (PVI) only was 106 minutes, and procedure time was 116 minutes in the patients who underwent PVI plus additional ablation procedures. Average ablation time was 12 minutes among those just having PVI, and 14 minutes in those who underwent PVI plus other ablations. The cryoablation catheter comes with 20 electrodes that allow it to also record electrograms.
The attraction of the ultra-low-temperature cryoablation catheter used in the study is it “can achieve complete PVI considerably faster” than other ablation methods while also achieving “unsurpassed efficacy,” Dr. De Potter said in a written statement. In addition, “the new, adjustable diagnostic capacity simplifies the procedure and makes it much less operator dependent,” he added.
BOSTON – An ultra-low-temperature ablation catheter was safe and effective in the first 48 atrial fibrillation (AF) patients to undergo treatment with the device.
The ultra-low-temperature catheter, cooled by liquid nitrogen to –196° C, showed excellent safety and a high success rate, in the modest number of patients who have been followed for 6 or 12 months, Tom De Potter, MD, said at the annual International AF Symposium. The catheter is capable of delivering both focal and linear lesions, said Dr. De Potter, a cardiac electrophysiologist at the Cardiovascular Center of OLV Hospital in Aalst, Belgium.
He reported results on the first 48 AF patients treated with the catheter at either his center or at St. Antonius Hospital in Nieuwegein, the Netherlands, in the CryoCure2 (Investigation of the Adagio Cryoablation System in Patients With Atrial Fibrillation) study. The investigators included safety findings only from the first 13 patients treated, but they assessed both safety and efficacy for the following 35 patients.
The safety review showed one patient with a groin-puncture injury, and two patients with phrenic nerve palsy, but no cases of phrenic nerve palsy in the most recent 41 patients who were treated with an updated version of the catheter that included a cryomapping feature. None of the 48 patients had a stroke, transient ischemic attack, esophageal injury, tamponade, or MI.
The 35 patients reviewed for efficacy included 10 patients with paroxysmal AF and 25 with persistent AF. All five of the paroxysmal AF patients followed for at least 6 months, and all four of those patients followed for 12 months, showed no AF recurrences. One of the persistent AF patients never achieved cardioversion at the time of the ablation procedure. All 17 other persistent AF patients followed for at least 6 months remained in sinus rhythm at 6 months. Among the eight of these patients followed for at least 12 months after treatment, one patient had AF recurrence, so the current 12-month rate of freedom from recurrence is seven of nine patients (including the one who never achieved cardioversion), or 78%.
The average procedure time to perform pulmonary vein isolation (PVI) only was 106 minutes, and procedure time was 116 minutes in the patients who underwent PVI plus additional ablation procedures. Average ablation time was 12 minutes among those just having PVI, and 14 minutes in those who underwent PVI plus other ablations. The cryoablation catheter comes with 20 electrodes that allow it to also record electrograms.
The attraction of the ultra-low-temperature cryoablation catheter used in the study is it “can achieve complete PVI considerably faster” than other ablation methods while also achieving “unsurpassed efficacy,” Dr. De Potter said in a written statement. In addition, “the new, adjustable diagnostic capacity simplifies the procedure and makes it much less operator dependent,” he added.
REPORTING FROM THE AF SYMPOSIUM 2019
Key clinical point:
Major finding: A year after cryoablation, seven of nine treated patients with persistent atrial fibrillation remained recurrence free.
Study details: CryoCure2, a single arm, multicenter, European study with 48 patients.
Disclosures: The CryoCure2 study is sponsored by Adagio Medical, the company developing the cryoablation catheter. Dr. De Potter has received travel support from Adagio, and he has received research funding from Boston Scientific and Johnson & Johnson.