User login
Moment of truth approaches for low-risk TAVR
SNOWMASS, COLO. – There are now more transcatheter aortic valve replacements performed each year than surgical ones in the United States, a disparity that may grow vastly larger.
That’s if the results of the two pivotal randomized trials comparing transcatheter aortic valve replacement (TAVR) and surgical aortic valve replacement (SAVR) in low-surgical-risk patients scheduled for presentation at the annual scientific session of the American College of Cardiology in March turn out to show TAVR outcomes are equivalent or superior to SAVR.
And that just might be the scenario, provided the eye-popping results already reported from another, much smaller study – the Low Risk TAVR study, a 200-patient, prospective, nonrandomized, observational study – are at all reflective of what’s to come when the pivotal PARTNER 3 and EVOLUT R trials are released at the ACC meeting in New Orleans, Michael J. Mack, MD, said at the Annual Cardiovascular Conference at Snowmass sponsored by the American College of Cardiology.
“The TAVR train has left the station on the way to low risk, and I don’t really see it coming back,” said Dr. Mack, medical director for cardiothoracic surgery at Baylor Scott & White Health in Dallas.
He wasn’t part of the Low Risk TAVR study, in which 200 low-surgical-risk patients with symptomatic severe aortic stenosis underwent TAVR with contemporary devices at 11 centers and were matched to 719 historical control SAVR patients at the same centers. But he called the study results “pretty spectacular”: zero 30-day all cause mortality in the TAVR group versus 1.7% with SAVR, no in-hospital strokes with TAVR versus a 0.6% rate with SAVR, and similar permanent pacemaker implantation rates of 5.0% with TAVR and 4.5% with SAVR.
Also, the TAVR group had a mere 3.0% rate of new-onset atrial fibrillation, a 2-day hospital length of stay, and a 0.5% incidence of greater-than-mild paravalvular leak at 30 days (J Am Coll Cardiol. 2018 Oct 30;72[18]:2095-105).
The two major trials due to report 1-year outcomes at the ACC meeting in March are similarly designed. The PARTNER 3 trial includes 1,000 low-surgical-risk patients with a mean age of 73 years and a predicted 30-day surgical mortality risk of 1.9%. Seventy-one percent of them were New York Heart Association (NYHA) Class II at enrollment. Participants were randomized to TAVR with the Edwards Lifesciences Sapien 3 valve or to SAVR, with the primary outcome being a composite of all-cause mortality, stroke, and rehospitalization 1 year post procedure. The EVOLUT R trial is similar, except the TAVR valve is the Medtronic CoreValve.
Both trials will continue to follow patients annually for 10 years in order to address the still-open issue of TAVR and SAVR valve durability. Also, the Food and Drug Administration has mandated that 4D CT imaging substudies be conducted in 800 of the combined 2,000 participants in the two trials in order to provide new insight into the issue of subclinical valve leaflet thrombosis, which was detected in 14% of participants in the Low Risk TAVR study 30 days post procedure.
“The clinical impact and need for anticoagulant therapy are currently unknown. However, clot anywhere else in the body doesn’t do good things, so it’s hard to imagine it’s helping here. Pretending it doesn’t exist isn’t going to make the problem go away,” Dr. Mack said.
The 4D CT imaging substudy results are expected to be presented later this year at the Transcatheter Cardiovascular Therapeutics conference in San Francisco.
In 2017, 51,064 TAVR procedures for symptomatic severe aortic stenosis were done in the United States, compared with 41,490 SAVRs. The past several years have seen a decreasing proportion of TAVRs being done in high-surgical-risk patients and a growing proportion in intermediate-risk patients.
Even if PARTNER 3 and EVOLUT R prove to be resoundingly positive for TAVR in low-risk patients, however, SAVR is not going to vanish, according to Dr. Mack. He cited four factors working against universal adoption of TAVR: the uncertainty surrounding valve durability, which will take years to resolve; the issue of TAVR valve leaflet thrombosis and the for-now theoretic possibility that all TAVR patients might need to receive postprocedure oral anticoagulation; the high rate of new permanent pacemaker implantation associated with TAVR, which Dr. Mack called the procedure’s Achilles heel; and the total absence of high-quality data on TAVR in patients with bicuspid aortic stenosis.
Even though TAVR for diseased bicuspid valves is not off-label therapy – the FDA’s indication for TAVR is for native valve aortic stenosis – patients with bicuspid valves weren’t included in any of the randomized trials, he explained.
Younger patients are likely to stick with SAVR for the foreseeable future, regardless of the outcomes of PARTNER 3 and EVOLUT R, according to the surgeon, because of the unresolved issue of valve durability, as well as TAVR’s greater associated need for a permanent pacemaker, both significant considerations in individuals with a life expectancy of another 20-30 years.
There are now roughly 600 TAVR centers and 1,150 SAVR centers nationally. One of the hot topics in the field stems from the fact that half of these TAVR centers do only one TAVR per week or less. That’s concerning in light of a recent New York State study showing a clear association between operator volume and outcomes.
“The more you do, the better your outcomes are, similar to many other procedures in medicine,” Dr. Mack commented.
On the other hand, it’s unlikely that patients who present to one of the roughly 550 SAVR-only centers are truly getting informed consent as to their options, he added.
TAVR timeline for 2019
March
PARTNER 3 and EVOLUT R primary outcomes to be presented at the American College of Cardiology annual scientific session.
Centers for Medicare & Medicaid Services to issue proposal for a revised National Coverage Determination for TAVR reimbursement.
June
Following a public comment period, CMS will release final revised criteria for TAVR reimbursement.
September
Results of the PARTNER 3 and EVOLUT R 4D CT imaging substudies will probably be presented late in the month at the annual Transcatheter Cardiovascular Therapeutics conference in San Francisco.
Late 2019
If PARTNER 3 and EVOLUT R trials are positive, FDA approval of the TAVR valves in low-surgical-risk patients is expected.
Dr. Mack is coprincipal investigator of PARTNER 3, which was sponsored by Edwards Lifesciences, and of Abbott Vascular’s COAPT trial. He’s also on the executive committee of the INTREPID trial, sponsored by Medtronic.
SNOWMASS, COLO. – There are now more transcatheter aortic valve replacements performed each year than surgical ones in the United States, a disparity that may grow vastly larger.
That’s if the results of the two pivotal randomized trials comparing transcatheter aortic valve replacement (TAVR) and surgical aortic valve replacement (SAVR) in low-surgical-risk patients scheduled for presentation at the annual scientific session of the American College of Cardiology in March turn out to show TAVR outcomes are equivalent or superior to SAVR.
And that just might be the scenario, provided the eye-popping results already reported from another, much smaller study – the Low Risk TAVR study, a 200-patient, prospective, nonrandomized, observational study – are at all reflective of what’s to come when the pivotal PARTNER 3 and EVOLUT R trials are released at the ACC meeting in New Orleans, Michael J. Mack, MD, said at the Annual Cardiovascular Conference at Snowmass sponsored by the American College of Cardiology.
“The TAVR train has left the station on the way to low risk, and I don’t really see it coming back,” said Dr. Mack, medical director for cardiothoracic surgery at Baylor Scott & White Health in Dallas.
He wasn’t part of the Low Risk TAVR study, in which 200 low-surgical-risk patients with symptomatic severe aortic stenosis underwent TAVR with contemporary devices at 11 centers and were matched to 719 historical control SAVR patients at the same centers. But he called the study results “pretty spectacular”: zero 30-day all cause mortality in the TAVR group versus 1.7% with SAVR, no in-hospital strokes with TAVR versus a 0.6% rate with SAVR, and similar permanent pacemaker implantation rates of 5.0% with TAVR and 4.5% with SAVR.
Also, the TAVR group had a mere 3.0% rate of new-onset atrial fibrillation, a 2-day hospital length of stay, and a 0.5% incidence of greater-than-mild paravalvular leak at 30 days (J Am Coll Cardiol. 2018 Oct 30;72[18]:2095-105).
The two major trials due to report 1-year outcomes at the ACC meeting in March are similarly designed. The PARTNER 3 trial includes 1,000 low-surgical-risk patients with a mean age of 73 years and a predicted 30-day surgical mortality risk of 1.9%. Seventy-one percent of them were New York Heart Association (NYHA) Class II at enrollment. Participants were randomized to TAVR with the Edwards Lifesciences Sapien 3 valve or to SAVR, with the primary outcome being a composite of all-cause mortality, stroke, and rehospitalization 1 year post procedure. The EVOLUT R trial is similar, except the TAVR valve is the Medtronic CoreValve.
Both trials will continue to follow patients annually for 10 years in order to address the still-open issue of TAVR and SAVR valve durability. Also, the Food and Drug Administration has mandated that 4D CT imaging substudies be conducted in 800 of the combined 2,000 participants in the two trials in order to provide new insight into the issue of subclinical valve leaflet thrombosis, which was detected in 14% of participants in the Low Risk TAVR study 30 days post procedure.
“The clinical impact and need for anticoagulant therapy are currently unknown. However, clot anywhere else in the body doesn’t do good things, so it’s hard to imagine it’s helping here. Pretending it doesn’t exist isn’t going to make the problem go away,” Dr. Mack said.
The 4D CT imaging substudy results are expected to be presented later this year at the Transcatheter Cardiovascular Therapeutics conference in San Francisco.
In 2017, 51,064 TAVR procedures for symptomatic severe aortic stenosis were done in the United States, compared with 41,490 SAVRs. The past several years have seen a decreasing proportion of TAVRs being done in high-surgical-risk patients and a growing proportion in intermediate-risk patients.
Even if PARTNER 3 and EVOLUT R prove to be resoundingly positive for TAVR in low-risk patients, however, SAVR is not going to vanish, according to Dr. Mack. He cited four factors working against universal adoption of TAVR: the uncertainty surrounding valve durability, which will take years to resolve; the issue of TAVR valve leaflet thrombosis and the for-now theoretic possibility that all TAVR patients might need to receive postprocedure oral anticoagulation; the high rate of new permanent pacemaker implantation associated with TAVR, which Dr. Mack called the procedure’s Achilles heel; and the total absence of high-quality data on TAVR in patients with bicuspid aortic stenosis.
Even though TAVR for diseased bicuspid valves is not off-label therapy – the FDA’s indication for TAVR is for native valve aortic stenosis – patients with bicuspid valves weren’t included in any of the randomized trials, he explained.
Younger patients are likely to stick with SAVR for the foreseeable future, regardless of the outcomes of PARTNER 3 and EVOLUT R, according to the surgeon, because of the unresolved issue of valve durability, as well as TAVR’s greater associated need for a permanent pacemaker, both significant considerations in individuals with a life expectancy of another 20-30 years.
There are now roughly 600 TAVR centers and 1,150 SAVR centers nationally. One of the hot topics in the field stems from the fact that half of these TAVR centers do only one TAVR per week or less. That’s concerning in light of a recent New York State study showing a clear association between operator volume and outcomes.
“The more you do, the better your outcomes are, similar to many other procedures in medicine,” Dr. Mack commented.
On the other hand, it’s unlikely that patients who present to one of the roughly 550 SAVR-only centers are truly getting informed consent as to their options, he added.
TAVR timeline for 2019
March
PARTNER 3 and EVOLUT R primary outcomes to be presented at the American College of Cardiology annual scientific session.
Centers for Medicare & Medicaid Services to issue proposal for a revised National Coverage Determination for TAVR reimbursement.
June
Following a public comment period, CMS will release final revised criteria for TAVR reimbursement.
September
Results of the PARTNER 3 and EVOLUT R 4D CT imaging substudies will probably be presented late in the month at the annual Transcatheter Cardiovascular Therapeutics conference in San Francisco.
Late 2019
If PARTNER 3 and EVOLUT R trials are positive, FDA approval of the TAVR valves in low-surgical-risk patients is expected.
Dr. Mack is coprincipal investigator of PARTNER 3, which was sponsored by Edwards Lifesciences, and of Abbott Vascular’s COAPT trial. He’s also on the executive committee of the INTREPID trial, sponsored by Medtronic.
SNOWMASS, COLO. – There are now more transcatheter aortic valve replacements performed each year than surgical ones in the United States, a disparity that may grow vastly larger.
That’s if the results of the two pivotal randomized trials comparing transcatheter aortic valve replacement (TAVR) and surgical aortic valve replacement (SAVR) in low-surgical-risk patients scheduled for presentation at the annual scientific session of the American College of Cardiology in March turn out to show TAVR outcomes are equivalent or superior to SAVR.
And that just might be the scenario, provided the eye-popping results already reported from another, much smaller study – the Low Risk TAVR study, a 200-patient, prospective, nonrandomized, observational study – are at all reflective of what’s to come when the pivotal PARTNER 3 and EVOLUT R trials are released at the ACC meeting in New Orleans, Michael J. Mack, MD, said at the Annual Cardiovascular Conference at Snowmass sponsored by the American College of Cardiology.
“The TAVR train has left the station on the way to low risk, and I don’t really see it coming back,” said Dr. Mack, medical director for cardiothoracic surgery at Baylor Scott & White Health in Dallas.
He wasn’t part of the Low Risk TAVR study, in which 200 low-surgical-risk patients with symptomatic severe aortic stenosis underwent TAVR with contemporary devices at 11 centers and were matched to 719 historical control SAVR patients at the same centers. But he called the study results “pretty spectacular”: zero 30-day all cause mortality in the TAVR group versus 1.7% with SAVR, no in-hospital strokes with TAVR versus a 0.6% rate with SAVR, and similar permanent pacemaker implantation rates of 5.0% with TAVR and 4.5% with SAVR.
Also, the TAVR group had a mere 3.0% rate of new-onset atrial fibrillation, a 2-day hospital length of stay, and a 0.5% incidence of greater-than-mild paravalvular leak at 30 days (J Am Coll Cardiol. 2018 Oct 30;72[18]:2095-105).
The two major trials due to report 1-year outcomes at the ACC meeting in March are similarly designed. The PARTNER 3 trial includes 1,000 low-surgical-risk patients with a mean age of 73 years and a predicted 30-day surgical mortality risk of 1.9%. Seventy-one percent of them were New York Heart Association (NYHA) Class II at enrollment. Participants were randomized to TAVR with the Edwards Lifesciences Sapien 3 valve or to SAVR, with the primary outcome being a composite of all-cause mortality, stroke, and rehospitalization 1 year post procedure. The EVOLUT R trial is similar, except the TAVR valve is the Medtronic CoreValve.
Both trials will continue to follow patients annually for 10 years in order to address the still-open issue of TAVR and SAVR valve durability. Also, the Food and Drug Administration has mandated that 4D CT imaging substudies be conducted in 800 of the combined 2,000 participants in the two trials in order to provide new insight into the issue of subclinical valve leaflet thrombosis, which was detected in 14% of participants in the Low Risk TAVR study 30 days post procedure.
“The clinical impact and need for anticoagulant therapy are currently unknown. However, clot anywhere else in the body doesn’t do good things, so it’s hard to imagine it’s helping here. Pretending it doesn’t exist isn’t going to make the problem go away,” Dr. Mack said.
The 4D CT imaging substudy results are expected to be presented later this year at the Transcatheter Cardiovascular Therapeutics conference in San Francisco.
In 2017, 51,064 TAVR procedures for symptomatic severe aortic stenosis were done in the United States, compared with 41,490 SAVRs. The past several years have seen a decreasing proportion of TAVRs being done in high-surgical-risk patients and a growing proportion in intermediate-risk patients.
Even if PARTNER 3 and EVOLUT R prove to be resoundingly positive for TAVR in low-risk patients, however, SAVR is not going to vanish, according to Dr. Mack. He cited four factors working against universal adoption of TAVR: the uncertainty surrounding valve durability, which will take years to resolve; the issue of TAVR valve leaflet thrombosis and the for-now theoretic possibility that all TAVR patients might need to receive postprocedure oral anticoagulation; the high rate of new permanent pacemaker implantation associated with TAVR, which Dr. Mack called the procedure’s Achilles heel; and the total absence of high-quality data on TAVR in patients with bicuspid aortic stenosis.
Even though TAVR for diseased bicuspid valves is not off-label therapy – the FDA’s indication for TAVR is for native valve aortic stenosis – patients with bicuspid valves weren’t included in any of the randomized trials, he explained.
Younger patients are likely to stick with SAVR for the foreseeable future, regardless of the outcomes of PARTNER 3 and EVOLUT R, according to the surgeon, because of the unresolved issue of valve durability, as well as TAVR’s greater associated need for a permanent pacemaker, both significant considerations in individuals with a life expectancy of another 20-30 years.
There are now roughly 600 TAVR centers and 1,150 SAVR centers nationally. One of the hot topics in the field stems from the fact that half of these TAVR centers do only one TAVR per week or less. That’s concerning in light of a recent New York State study showing a clear association between operator volume and outcomes.
“The more you do, the better your outcomes are, similar to many other procedures in medicine,” Dr. Mack commented.
On the other hand, it’s unlikely that patients who present to one of the roughly 550 SAVR-only centers are truly getting informed consent as to their options, he added.
TAVR timeline for 2019
March
PARTNER 3 and EVOLUT R primary outcomes to be presented at the American College of Cardiology annual scientific session.
Centers for Medicare & Medicaid Services to issue proposal for a revised National Coverage Determination for TAVR reimbursement.
June
Following a public comment period, CMS will release final revised criteria for TAVR reimbursement.
September
Results of the PARTNER 3 and EVOLUT R 4D CT imaging substudies will probably be presented late in the month at the annual Transcatheter Cardiovascular Therapeutics conference in San Francisco.
Late 2019
If PARTNER 3 and EVOLUT R trials are positive, FDA approval of the TAVR valves in low-surgical-risk patients is expected.
Dr. Mack is coprincipal investigator of PARTNER 3, which was sponsored by Edwards Lifesciences, and of Abbott Vascular’s COAPT trial. He’s also on the executive committee of the INTREPID trial, sponsored by Medtronic.
EXPERT ANALYSIS FROM ACC SNOWMASS 2019
Novel plasma biomarkers may predict preclinical Alzheimer’s disease
, researchers reported in Science Advances.

“To our knowledge, this is the first time that a multianalyte plasma biomarker panel for an Alzheimer’s disease–related phenotype has been found and independently replicated by a nontargeted mass spectrometry approach,” said Nicholas J. Ashton, PhD, of King’s College London and the University of Gothenburg in Sweden, and his research colleagues.
Blood-based measures that predict amyloid-beta burden in preclinical Alzheimer’s disease have the potential to help investigators conduct clinical trials and aid in diagnostic management. However, this novel approach needs to be validated and translated “to a simpler automated platform suitable for wider utility,” the investigators noted. In addition, it is unclear whether their classifier can track changes in amyloid-beta or differentiate between other diseases with amyloid-beta pathology.
Advances in mass spectrometry technology have renewed interest in the analysis of plasma proteins in patients with various diseases. To assess whether proteomic discovery in plasma can help predict amyloid-beta burden in preclinical Alzheimer’s disease, Dr. Ashton and his colleagues studied 238 cognitively unimpaired individuals from the Australian Imaging, Biomarker and Lifestyle Flagship Study of Ageing (AIBL) and the Kerr Anglican Retirement Village Initiative in Ageing Health (KARVIAH). The participants had undergone PET to determine their amyloid-beta status. In the AIBL cohort (n = 144), 100 participants were amyloid-beta negative, and 44 were amyloid-beta positive. In the KARVIAH cohort (n = 94), 59 participants were amyloid-beta negative, and 35 were amyloid-beta positive. There were significantly more APOE4 carriers in the amyloid-beta–positive groups than in the amyloid-beta–negative groups. In addition, the amyloid-beta–positive groups tended to be older.
A support vector machine analysis created classifiers predicting amyloid-beta positivity in the AIBL cohort using demographics, proteins, or both. The researchers then tested each classifier in the KARVIAH dataset to identify which model best predicted amyloid-beta positivity. The optimal model included 10 protein features (prothrombin, adhesion G protein–coupled receptor, amyloid-beta A4 protein, NGN2, DNAH10, REST, NfL, RPS6KA3, GPSM2, FHAD1) and two demographic features (APOE4 count and age).
The classifier achieved a testing area under the receiver operator characteristic curve of 0.891 in the KARVIAH cohort to predict amyloid-beta positivity in cognitively unimpaired individuals with a sensitivity of 0.78 and specificity of 0.77.
The 10 protein features “represent a diverse array of pathways,” and the highest ranked feature was the serine protease prothrombin, which is a precursor to thrombin, the authors noted. “Multiple lines of evidence support that cerebrovascular disease may play a role in AD and that amyloid-beta may be involved in thrombosis, fibrinolysis, and inflammation via its interaction with the coagulation cascade,” the researchers wrote.
Two of the biomarkers – amyloid-beta A4 protein and NfL – have been examined in prior research and had a greater effect size in a secondary analysis that included participants with mild cognitive impairment and Alzheimer’s disease. This finding confirms “their connection with the more established disease state,” Dr. Ashton and colleagues said. In the secondary analysis, the optimal classifier included one demographic factor (APOE4 count) and nine protein features, eight of which also were used in the cognitively unimpaired classifier.
The study was funded in part by the National Institute for Health Research Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King’s College London, and many authors reported additional research support from various institutions. One author is an employee of Johnson & Johnson and a named inventor on unrelated biomarker intellectual property owned by Proteome Science and King’s College London.
SOURCE: Ashton NJ et al. Sci Adv. 2019 Feb 6. doi: 10.1126/sciadv.aau7220.
, researchers reported in Science Advances.
“To our knowledge, this is the first time that a multianalyte plasma biomarker panel for an Alzheimer’s disease–related phenotype has been found and independently replicated by a nontargeted mass spectrometry approach,” said Nicholas J. Ashton, PhD, of King’s College London and the University of Gothenburg in Sweden, and his research colleagues.
Blood-based measures that predict amyloid-beta burden in preclinical Alzheimer’s disease have the potential to help investigators conduct clinical trials and aid in diagnostic management. However, this novel approach needs to be validated and translated “to a simpler automated platform suitable for wider utility,” the investigators noted. In addition, it is unclear whether their classifier can track changes in amyloid-beta or differentiate between other diseases with amyloid-beta pathology.
Advances in mass spectrometry technology have renewed interest in the analysis of plasma proteins in patients with various diseases. To assess whether proteomic discovery in plasma can help predict amyloid-beta burden in preclinical Alzheimer’s disease, Dr. Ashton and his colleagues studied 238 cognitively unimpaired individuals from the Australian Imaging, Biomarker and Lifestyle Flagship Study of Ageing (AIBL) and the Kerr Anglican Retirement Village Initiative in Ageing Health (KARVIAH). The participants had undergone PET to determine their amyloid-beta status. In the AIBL cohort (n = 144), 100 participants were amyloid-beta negative, and 44 were amyloid-beta positive. In the KARVIAH cohort (n = 94), 59 participants were amyloid-beta negative, and 35 were amyloid-beta positive. There were significantly more APOE4 carriers in the amyloid-beta–positive groups than in the amyloid-beta–negative groups. In addition, the amyloid-beta–positive groups tended to be older.
A support vector machine analysis created classifiers predicting amyloid-beta positivity in the AIBL cohort using demographics, proteins, or both. The researchers then tested each classifier in the KARVIAH dataset to identify which model best predicted amyloid-beta positivity. The optimal model included 10 protein features (prothrombin, adhesion G protein–coupled receptor, amyloid-beta A4 protein, NGN2, DNAH10, REST, NfL, RPS6KA3, GPSM2, FHAD1) and two demographic features (APOE4 count and age).
The classifier achieved a testing area under the receiver operator characteristic curve of 0.891 in the KARVIAH cohort to predict amyloid-beta positivity in cognitively unimpaired individuals with a sensitivity of 0.78 and specificity of 0.77.
The 10 protein features “represent a diverse array of pathways,” and the highest ranked feature was the serine protease prothrombin, which is a precursor to thrombin, the authors noted. “Multiple lines of evidence support that cerebrovascular disease may play a role in AD and that amyloid-beta may be involved in thrombosis, fibrinolysis, and inflammation via its interaction with the coagulation cascade,” the researchers wrote.
Two of the biomarkers – amyloid-beta A4 protein and NfL – have been examined in prior research and had a greater effect size in a secondary analysis that included participants with mild cognitive impairment and Alzheimer’s disease. This finding confirms “their connection with the more established disease state,” Dr. Ashton and colleagues said. In the secondary analysis, the optimal classifier included one demographic factor (APOE4 count) and nine protein features, eight of which also were used in the cognitively unimpaired classifier.
The study was funded in part by the National Institute for Health Research Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King’s College London, and many authors reported additional research support from various institutions. One author is an employee of Johnson & Johnson and a named inventor on unrelated biomarker intellectual property owned by Proteome Science and King’s College London.
SOURCE: Ashton NJ et al. Sci Adv. 2019 Feb 6. doi: 10.1126/sciadv.aau7220.
, researchers reported in Science Advances.
“To our knowledge, this is the first time that a multianalyte plasma biomarker panel for an Alzheimer’s disease–related phenotype has been found and independently replicated by a nontargeted mass spectrometry approach,” said Nicholas J. Ashton, PhD, of King’s College London and the University of Gothenburg in Sweden, and his research colleagues.
Blood-based measures that predict amyloid-beta burden in preclinical Alzheimer’s disease have the potential to help investigators conduct clinical trials and aid in diagnostic management. However, this novel approach needs to be validated and translated “to a simpler automated platform suitable for wider utility,” the investigators noted. In addition, it is unclear whether their classifier can track changes in amyloid-beta or differentiate between other diseases with amyloid-beta pathology.
Advances in mass spectrometry technology have renewed interest in the analysis of plasma proteins in patients with various diseases. To assess whether proteomic discovery in plasma can help predict amyloid-beta burden in preclinical Alzheimer’s disease, Dr. Ashton and his colleagues studied 238 cognitively unimpaired individuals from the Australian Imaging, Biomarker and Lifestyle Flagship Study of Ageing (AIBL) and the Kerr Anglican Retirement Village Initiative in Ageing Health (KARVIAH). The participants had undergone PET to determine their amyloid-beta status. In the AIBL cohort (n = 144), 100 participants were amyloid-beta negative, and 44 were amyloid-beta positive. In the KARVIAH cohort (n = 94), 59 participants were amyloid-beta negative, and 35 were amyloid-beta positive. There were significantly more APOE4 carriers in the amyloid-beta–positive groups than in the amyloid-beta–negative groups. In addition, the amyloid-beta–positive groups tended to be older.
A support vector machine analysis created classifiers predicting amyloid-beta positivity in the AIBL cohort using demographics, proteins, or both. The researchers then tested each classifier in the KARVIAH dataset to identify which model best predicted amyloid-beta positivity. The optimal model included 10 protein features (prothrombin, adhesion G protein–coupled receptor, amyloid-beta A4 protein, NGN2, DNAH10, REST, NfL, RPS6KA3, GPSM2, FHAD1) and two demographic features (APOE4 count and age).
The classifier achieved a testing area under the receiver operator characteristic curve of 0.891 in the KARVIAH cohort to predict amyloid-beta positivity in cognitively unimpaired individuals with a sensitivity of 0.78 and specificity of 0.77.
The 10 protein features “represent a diverse array of pathways,” and the highest ranked feature was the serine protease prothrombin, which is a precursor to thrombin, the authors noted. “Multiple lines of evidence support that cerebrovascular disease may play a role in AD and that amyloid-beta may be involved in thrombosis, fibrinolysis, and inflammation via its interaction with the coagulation cascade,” the researchers wrote.
Two of the biomarkers – amyloid-beta A4 protein and NfL – have been examined in prior research and had a greater effect size in a secondary analysis that included participants with mild cognitive impairment and Alzheimer’s disease. This finding confirms “their connection with the more established disease state,” Dr. Ashton and colleagues said. In the secondary analysis, the optimal classifier included one demographic factor (APOE4 count) and nine protein features, eight of which also were used in the cognitively unimpaired classifier.
The study was funded in part by the National Institute for Health Research Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King’s College London, and many authors reported additional research support from various institutions. One author is an employee of Johnson & Johnson and a named inventor on unrelated biomarker intellectual property owned by Proteome Science and King’s College London.
SOURCE: Ashton NJ et al. Sci Adv. 2019 Feb 6. doi: 10.1126/sciadv.aau7220.
FROM SCIENCE ADVANCES
Key clinical point: Blood-based measures that predict amyloid-beta burden in preclinical Alzheimer’s disease have the potential to help investigators conduct clinical trials and aid in diagnostic management.
Major finding: A classifier developed using plasma proteomic analysis achieved an area under the receiver operator characteristic curve of 0.891.
Study details: An analysis of data from 238 cognitively unimpaired individuals from the Australian Imaging, Biomarker and Lifestyle Flagship Study of Ageing (AIBL) and the Kerr Anglican Retirement Village Initiative in Ageing Health (KARVIAH).
Disclosures: The study was funded in part by the National Institute for Health Research Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King’s College London, and many authors reported additional research support from various institutions. One author is an employee of Johnson & Johnson and a named inventor on unrelated biomarker intellectual property owned by Proteome Science and King’s College London.
Source: Ashton NJ et al. Sci Adv. 2019 Feb 6. doi: 10.1126/sciadv.aau7220.
Functional MRI detects consciousness after brain damage
Functional MRI can measure patterns of connectivity to determine levels of consciousness in nonresponsive patients with brain injury, according to results from a multicenter, cross-sectional, observational study.
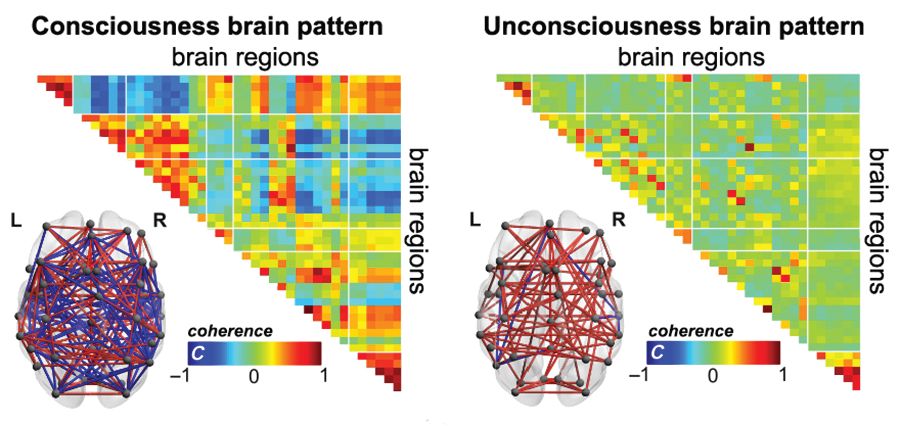
Blood oxygen level–dependent (BOLD) fMRI showed that brain-wide coordination patterns of high complexity became increasingly common moving from unresponsive patients to those with minimal consciousness to healthy individuals, reported lead author Athena Demertzi, PhD, of GIGA Research Institute at the University of Liège in Belgium, and her colleagues.
“Finding reliable markers indicating the presence or absence of consciousness represents an outstanding open problem for science,” the investigators wrote in Science Advances.
In medicine, an fMRI-based measure of consciousness could supplement behavioral assessments of awareness and guide therapeutic strategies; more broadly, image-based markers could help elucidate the nature of consciousness itself.
“We postulate that consciousness has specific characteristics that are based on the temporal dynamics of ongoing brain activity and its coordination over distant cortical regions,” the investigators wrote. “Our hypothesis stems from the common stance of various contemporary theories which propose that consciousness relates to a dynamic process of self-sustained, coordinated brain-scale activity assisting the tuning to a constantly evolving environment, rather than in static descriptions of brain function.”
There is a need for a reliable way of distinguishing consciousness from unconscious states, the investigators said. “Given that nonresponsiveness can be associated with a variety of brain lesions, varying levels of vigilance, and covert cognition, we highlight the need to determine a common set of features capable of accounting for the capacity to sustain conscious experience.”
To search for patterns of brain signal coordination that correlate with consciousness, four independent research centers performed BOLD fMRI scans of participants at rest or under anesthesia with propofol. Of 159 total participants, 47 were healthy individuals and 112 were patients in a vegetative state/with unresponsive wakefulness syndrome (UWS) or in a minimally conscious state (MCS), based on standardized behavioral assessments. The main data analysis, which included 125 participants, assessed BOLD fMRI signal coordination between six brain networks known to have roles in cognitive and functional processes.
The researchers’ analysis revealed four distinct and recurring brain-wide coordination patterns ranging on a scale from highest activity (pattern 1) to lowest activity (pattern 4). Pattern 1, which exhibited most long-distance edges, spatial complexity, efficiency, and community structure, became increasingly common when moving from UWS patients to MCS patients to healthy control individuals (UWS < MCS < HC, rho = 0.7, Spearman rank correlation between rate and group, P less than 1 x 10-16).
In contrast, pattern 4, characterized by low interareal coordination, showed an inverse trend; it became less common when moving from vegetative patients to healthy individuals (UWS > MCS > HC, Spearman rank correlation between rate and group, rho = –0.6, P less than 1 x 10-11). Although patterns 2 and 3 occurred with equal frequency across all groups, the investigators noted that switching between patterns was most common and predictably sequential in healthy individuals, versus patients with UWS, who were least likely to switch patterns. A total of 23 patients who were scanned under propofol anesthesia were equally likely to exhibit pattern 4, regardless of health status, suggesting that pattern 4 depends upon fixed anatomical pathways. Results were not affected by scanning site or other patient characteristics, such as age, gender, etiology, or chronicity.
“We conclude that these patterns of transient brain signal coordination are characteristic of conscious and unconscious brain states,” the investigators wrote, “warranting future research concerning their relationship to ongoing conscious content, and the possibility of modifying their prevalence by external perturbations, both in healthy and pathological individuals, as well as across species.”
The study was funded by a James S. McDonnell Foundation Collaborative Activity Award, INSERM, the Belgian National Funds for Scientific Research, the Canada Excellence Research Chairs program, and others. The authors declared having no conflicts of interest.
SOURCE: Demertzi A et al. Sci Adv. 2019 Feb 6. doi: 10.1126/sciadv.aat7603.
Functional MRI can measure patterns of connectivity to determine levels of consciousness in nonresponsive patients with brain injury, according to results from a multicenter, cross-sectional, observational study.
Blood oxygen level–dependent (BOLD) fMRI showed that brain-wide coordination patterns of high complexity became increasingly common moving from unresponsive patients to those with minimal consciousness to healthy individuals, reported lead author Athena Demertzi, PhD, of GIGA Research Institute at the University of Liège in Belgium, and her colleagues.
“Finding reliable markers indicating the presence or absence of consciousness represents an outstanding open problem for science,” the investigators wrote in Science Advances.
In medicine, an fMRI-based measure of consciousness could supplement behavioral assessments of awareness and guide therapeutic strategies; more broadly, image-based markers could help elucidate the nature of consciousness itself.
“We postulate that consciousness has specific characteristics that are based on the temporal dynamics of ongoing brain activity and its coordination over distant cortical regions,” the investigators wrote. “Our hypothesis stems from the common stance of various contemporary theories which propose that consciousness relates to a dynamic process of self-sustained, coordinated brain-scale activity assisting the tuning to a constantly evolving environment, rather than in static descriptions of brain function.”
There is a need for a reliable way of distinguishing consciousness from unconscious states, the investigators said. “Given that nonresponsiveness can be associated with a variety of brain lesions, varying levels of vigilance, and covert cognition, we highlight the need to determine a common set of features capable of accounting for the capacity to sustain conscious experience.”
To search for patterns of brain signal coordination that correlate with consciousness, four independent research centers performed BOLD fMRI scans of participants at rest or under anesthesia with propofol. Of 159 total participants, 47 were healthy individuals and 112 were patients in a vegetative state/with unresponsive wakefulness syndrome (UWS) or in a minimally conscious state (MCS), based on standardized behavioral assessments. The main data analysis, which included 125 participants, assessed BOLD fMRI signal coordination between six brain networks known to have roles in cognitive and functional processes.
The researchers’ analysis revealed four distinct and recurring brain-wide coordination patterns ranging on a scale from highest activity (pattern 1) to lowest activity (pattern 4). Pattern 1, which exhibited most long-distance edges, spatial complexity, efficiency, and community structure, became increasingly common when moving from UWS patients to MCS patients to healthy control individuals (UWS < MCS < HC, rho = 0.7, Spearman rank correlation between rate and group, P less than 1 x 10-16).
In contrast, pattern 4, characterized by low interareal coordination, showed an inverse trend; it became less common when moving from vegetative patients to healthy individuals (UWS > MCS > HC, Spearman rank correlation between rate and group, rho = –0.6, P less than 1 x 10-11). Although patterns 2 and 3 occurred with equal frequency across all groups, the investigators noted that switching between patterns was most common and predictably sequential in healthy individuals, versus patients with UWS, who were least likely to switch patterns. A total of 23 patients who were scanned under propofol anesthesia were equally likely to exhibit pattern 4, regardless of health status, suggesting that pattern 4 depends upon fixed anatomical pathways. Results were not affected by scanning site or other patient characteristics, such as age, gender, etiology, or chronicity.
“We conclude that these patterns of transient brain signal coordination are characteristic of conscious and unconscious brain states,” the investigators wrote, “warranting future research concerning their relationship to ongoing conscious content, and the possibility of modifying their prevalence by external perturbations, both in healthy and pathological individuals, as well as across species.”
The study was funded by a James S. McDonnell Foundation Collaborative Activity Award, INSERM, the Belgian National Funds for Scientific Research, the Canada Excellence Research Chairs program, and others. The authors declared having no conflicts of interest.
SOURCE: Demertzi A et al. Sci Adv. 2019 Feb 6. doi: 10.1126/sciadv.aat7603.
Functional MRI can measure patterns of connectivity to determine levels of consciousness in nonresponsive patients with brain injury, according to results from a multicenter, cross-sectional, observational study.
Blood oxygen level–dependent (BOLD) fMRI showed that brain-wide coordination patterns of high complexity became increasingly common moving from unresponsive patients to those with minimal consciousness to healthy individuals, reported lead author Athena Demertzi, PhD, of GIGA Research Institute at the University of Liège in Belgium, and her colleagues.
“Finding reliable markers indicating the presence or absence of consciousness represents an outstanding open problem for science,” the investigators wrote in Science Advances.
In medicine, an fMRI-based measure of consciousness could supplement behavioral assessments of awareness and guide therapeutic strategies; more broadly, image-based markers could help elucidate the nature of consciousness itself.
“We postulate that consciousness has specific characteristics that are based on the temporal dynamics of ongoing brain activity and its coordination over distant cortical regions,” the investigators wrote. “Our hypothesis stems from the common stance of various contemporary theories which propose that consciousness relates to a dynamic process of self-sustained, coordinated brain-scale activity assisting the tuning to a constantly evolving environment, rather than in static descriptions of brain function.”
There is a need for a reliable way of distinguishing consciousness from unconscious states, the investigators said. “Given that nonresponsiveness can be associated with a variety of brain lesions, varying levels of vigilance, and covert cognition, we highlight the need to determine a common set of features capable of accounting for the capacity to sustain conscious experience.”
To search for patterns of brain signal coordination that correlate with consciousness, four independent research centers performed BOLD fMRI scans of participants at rest or under anesthesia with propofol. Of 159 total participants, 47 were healthy individuals and 112 were patients in a vegetative state/with unresponsive wakefulness syndrome (UWS) or in a minimally conscious state (MCS), based on standardized behavioral assessments. The main data analysis, which included 125 participants, assessed BOLD fMRI signal coordination between six brain networks known to have roles in cognitive and functional processes.
The researchers’ analysis revealed four distinct and recurring brain-wide coordination patterns ranging on a scale from highest activity (pattern 1) to lowest activity (pattern 4). Pattern 1, which exhibited most long-distance edges, spatial complexity, efficiency, and community structure, became increasingly common when moving from UWS patients to MCS patients to healthy control individuals (UWS < MCS < HC, rho = 0.7, Spearman rank correlation between rate and group, P less than 1 x 10-16).
In contrast, pattern 4, characterized by low interareal coordination, showed an inverse trend; it became less common when moving from vegetative patients to healthy individuals (UWS > MCS > HC, Spearman rank correlation between rate and group, rho = –0.6, P less than 1 x 10-11). Although patterns 2 and 3 occurred with equal frequency across all groups, the investigators noted that switching between patterns was most common and predictably sequential in healthy individuals, versus patients with UWS, who were least likely to switch patterns. A total of 23 patients who were scanned under propofol anesthesia were equally likely to exhibit pattern 4, regardless of health status, suggesting that pattern 4 depends upon fixed anatomical pathways. Results were not affected by scanning site or other patient characteristics, such as age, gender, etiology, or chronicity.
“We conclude that these patterns of transient brain signal coordination are characteristic of conscious and unconscious brain states,” the investigators wrote, “warranting future research concerning their relationship to ongoing conscious content, and the possibility of modifying their prevalence by external perturbations, both in healthy and pathological individuals, as well as across species.”
The study was funded by a James S. McDonnell Foundation Collaborative Activity Award, INSERM, the Belgian National Funds for Scientific Research, the Canada Excellence Research Chairs program, and others. The authors declared having no conflicts of interest.
SOURCE: Demertzi A et al. Sci Adv. 2019 Feb 6. doi: 10.1126/sciadv.aat7603.
FROM SCIENCE ADVANCES
Key clinical point:
Major finding: A brain-wide coordination pattern of high complexity became increasingly common when moving from patients with unresponsive wakefulness syndrome (UWS) to patients in a minimally conscious state (MCS) to healthy control individuals.
Study details: A study involving blood oxygen level–dependent (BOLD) fMRI scans at rest or under anesthesia in 159 participants at four independent research facilities.
Disclosures: The study was funded by a James S. McDonnell Foundation Collaborative Activity Award, INSERM, the Belgian National Funds for Scientific Research, the Canada Excellence Research Chairs program, and others. The authors declared having no conflicts of interest.
Source: Demertzi A et al. Sci Adv. 2019 Feb 6. doi: 10.1126/sciadv.aat7603.
American football and CTE: Is a racial divide inevitable?
Evidence that American football can lead to chronic traumatic encephalopathy (CTE), continues to grow. As a result, some parents are opting to sign their sons up for other sports.

In the 2017-2018 school year, 6.6% fewer high school athletes participated in tackle football than did 8 years before according to the National Federation of State High School Associations.
Many black parents encourage their sons to play football as a way to protect them gang activity. In addition, the sport can be their sole option for securing a college education for their children, an article in the Atlantic said. A recent survey of 50,000 8th-, 10th-, and 12th-grade students found that tackle football is predominantly the domain of black youth.
“This divergence paints a troubling picture of how economic opportunity – or a lack thereof – governs which boys are incentivized to put their body and brain at risk to play. Depending on where families live, and what other options are available to them, they see either a game that is too violent to consider or one that is necessary and important, if risky. Millions of Americans still watch football; NFL ratings were up this season,” Alana Semuels wrote in the article. “That a distinct portion of families won’t let their children play creates a disturbing future for the country’s most popular game.”
“Without a reversal in economic fortunes for poor communities across the country, football could one day become a sport played almost exclusively by black athletes, while still enjoyed by everyone. Black athletes – who already make up the majority of players in the most dangerous on-field positions – would continue to suffer from long-term brain damage, their life cut short by dementia and the scourge of CTE,” she wrote.
Meanwhile, numerous outlets reported that Super Bowl LIII garnered the lowest ratings since 2008.
Psychiatric hospital set to close
In both Kansas and Missouri, a shortage in mental health care has become evident, according to an article in the Kansas City Star. And now the Two Rivers Behavioral Health System, a private psychiatric hospital in southeast Kansas City, Mo., is closing its doors. The result will be a loss of 129 jobs and 105 fewer mental health beds in the city.
Patients currently in the facility will be relocated, and their care will continue. But for those who come after, care will now be tougher to find.
Two Rivers, owned by Pennsylvania-based Universal Health Services, treats children and adults. It had 2,347 discharges in 2017 and almost $28 million in revenue but had a net loss of about $3.4 million. The facility has been under scrutiny in the past two decades over its treatment of patients, with accusations about the bolstering of false memories concerning involvements in satanic cults and the treatment of a convicted sex offender who assaulted another patient. The most recent state inspection showed that Two Rivers had failed to provide a safe environment for six patients who were considered suicide risks. The patients had unsupervised access to the nurses’ station, as well as access to pens that could have been used for stabbing and a charging cord that could have been used for strangulation.
In an interview with the Star, Mark Stringer, director of the Missouri Department of Mental Health, said private psychiatric hospitals like Two Rivers are finding it harder to keep functioning, partly because of nursing shortages. Private facilities are not subsidized like state mental hospitals and are unable to secure staff from other facilities.
“There is a general worry about the availability of psychiatric services for people in crisis; there’s just no doubt about that,” Mr. Stringer said. “The loss of beds certainly hurts.”
New center offers ‘kind patient care’
In Nashville, Tenn., a new mental illness crisis treatment center is open. The center offers a 24/7 option for those with mental health issues who have run afoul of the law. Instead of incarceration, they can receive treatment, the Tennessean reported.
Estimates are that more than 1 million residents of Tennessee aged 18 years and older have a mental health or substance use disorder. About 25% of those residents having a serious mental health illness.
The new facility includes a crisis walk-in center and a unit where those in the throes of a mental health crisis can seek care. A goal is to get people suffering from an urgent mental illness crisis connected to help faster, especially when they come into contact with police.
“It’s very important to come to a place that’s going to get you help,” Bonnie Kelly said in the article. Ms. Kelly, who reportedly has bipolar disorder, has been arrested several times for disorderly conduct tied to her condition. “It means everything. It is good, kind patient care, rather than just getting you out of the way.”
Aside from benefiting those in need of mental health care, the center will ease the strain on Nashville police, who currently spend more than 5,000 hours each year responding to mental health–related calls. The officers must remain with the person until transfer to a jail or mental health facility is done.
“As a city, we are recognizing that there is a need, and we are investing in that,” East Precinct Commander David Imhof said in the article. “We are helping a population that has had no voice in the past.” Right now, fewer than 60% of patients discharged from state mental health facilities receive any sort of coverage. The result can be cycles of release, arrest, and incarceration.
Agency aims to protect patients
The Oregon Health Authority has stepped in to prevent numerous state-funded mental health facilities run by the same contractor from booting out patients with severe mental health problems.
The contractor is Kepro, a Pennsylvania-based company. Since December, the health authority has reversed decisions to release 17 patients, according to an article in the Oregonian. The harder line follows revelations by the newspaper of serious harm to patients who had been released before they were capable of caring for themselves.
Kepro was hired by the health authority and paid $27 million to evaluate the medical needs of mental health patients in Oregon. As part of the evaluation, 215 of 250 patients were deemed unqualified to remain in care.
One was Ruane Oliverio, who has schizophrenia, who was kicked out of a locked facility in Portland last June. Clinicians had warned against her release, insisting that her mental state remained too vulnerable. After being hospitalized multiple times, she was sent to the Oregon State Hospital, the highest and most expensive level of care. She was one of those targeted for release. This decision was reversed, and she continues to receive care.
Coalition seeks mental health care for refugees
A new coalition called Matters Involving Neuro-Disorders, or MIND, is trying to help refugees with mental health conditions. The effort is a response to several mental health-related deaths of refugees during 2014-2016, a video produced by the San Diego Union-Tribune said.
“Refugees are brought to this country to help them rebuild their lives,” said Justin Mudekereza, executive director of New Neighbor Relief, a nonprofit organization dedicated to helping refugees adjust to their new lives in the United States. “They have gone through a lot in their countries, then from there, they went to refugee camps, where they spend 15-20 years or more before they got a chance to come to this country.”
Sheila S. Mitra-Sarkar, PhD, of the Institute of Public Urban Affairs at San Diego State University, described the need for a “comprehensive solution” to help refugees adapt to their new society, learn English, find housing and employment, and thrive.
“When I see a patient or someone who seems to have a psychological issue ... I look at everything that goes around them,” said John C. Kuek, PhD, of La Maestra Community Health Centers in San Diego. “I’m looking at the housing issue, the employment issue, and translational issue – meaning they have some family back home and they have a live family here to care for.”
Evidence that American football can lead to chronic traumatic encephalopathy (CTE), continues to grow. As a result, some parents are opting to sign their sons up for other sports.
In the 2017-2018 school year, 6.6% fewer high school athletes participated in tackle football than did 8 years before according to the National Federation of State High School Associations.
Many black parents encourage their sons to play football as a way to protect them gang activity. In addition, the sport can be their sole option for securing a college education for their children, an article in the Atlantic said. A recent survey of 50,000 8th-, 10th-, and 12th-grade students found that tackle football is predominantly the domain of black youth.
“This divergence paints a troubling picture of how economic opportunity – or a lack thereof – governs which boys are incentivized to put their body and brain at risk to play. Depending on where families live, and what other options are available to them, they see either a game that is too violent to consider or one that is necessary and important, if risky. Millions of Americans still watch football; NFL ratings were up this season,” Alana Semuels wrote in the article. “That a distinct portion of families won’t let their children play creates a disturbing future for the country’s most popular game.”
“Without a reversal in economic fortunes for poor communities across the country, football could one day become a sport played almost exclusively by black athletes, while still enjoyed by everyone. Black athletes – who already make up the majority of players in the most dangerous on-field positions – would continue to suffer from long-term brain damage, their life cut short by dementia and the scourge of CTE,” she wrote.
Meanwhile, numerous outlets reported that Super Bowl LIII garnered the lowest ratings since 2008.
Psychiatric hospital set to close
In both Kansas and Missouri, a shortage in mental health care has become evident, according to an article in the Kansas City Star. And now the Two Rivers Behavioral Health System, a private psychiatric hospital in southeast Kansas City, Mo., is closing its doors. The result will be a loss of 129 jobs and 105 fewer mental health beds in the city.
Patients currently in the facility will be relocated, and their care will continue. But for those who come after, care will now be tougher to find.
Two Rivers, owned by Pennsylvania-based Universal Health Services, treats children and adults. It had 2,347 discharges in 2017 and almost $28 million in revenue but had a net loss of about $3.4 million. The facility has been under scrutiny in the past two decades over its treatment of patients, with accusations about the bolstering of false memories concerning involvements in satanic cults and the treatment of a convicted sex offender who assaulted another patient. The most recent state inspection showed that Two Rivers had failed to provide a safe environment for six patients who were considered suicide risks. The patients had unsupervised access to the nurses’ station, as well as access to pens that could have been used for stabbing and a charging cord that could have been used for strangulation.
In an interview with the Star, Mark Stringer, director of the Missouri Department of Mental Health, said private psychiatric hospitals like Two Rivers are finding it harder to keep functioning, partly because of nursing shortages. Private facilities are not subsidized like state mental hospitals and are unable to secure staff from other facilities.
“There is a general worry about the availability of psychiatric services for people in crisis; there’s just no doubt about that,” Mr. Stringer said. “The loss of beds certainly hurts.”
New center offers ‘kind patient care’
In Nashville, Tenn., a new mental illness crisis treatment center is open. The center offers a 24/7 option for those with mental health issues who have run afoul of the law. Instead of incarceration, they can receive treatment, the Tennessean reported.
Estimates are that more than 1 million residents of Tennessee aged 18 years and older have a mental health or substance use disorder. About 25% of those residents having a serious mental health illness.
The new facility includes a crisis walk-in center and a unit where those in the throes of a mental health crisis can seek care. A goal is to get people suffering from an urgent mental illness crisis connected to help faster, especially when they come into contact with police.
“It’s very important to come to a place that’s going to get you help,” Bonnie Kelly said in the article. Ms. Kelly, who reportedly has bipolar disorder, has been arrested several times for disorderly conduct tied to her condition. “It means everything. It is good, kind patient care, rather than just getting you out of the way.”
Aside from benefiting those in need of mental health care, the center will ease the strain on Nashville police, who currently spend more than 5,000 hours each year responding to mental health–related calls. The officers must remain with the person until transfer to a jail or mental health facility is done.
“As a city, we are recognizing that there is a need, and we are investing in that,” East Precinct Commander David Imhof said in the article. “We are helping a population that has had no voice in the past.” Right now, fewer than 60% of patients discharged from state mental health facilities receive any sort of coverage. The result can be cycles of release, arrest, and incarceration.
Agency aims to protect patients
The Oregon Health Authority has stepped in to prevent numerous state-funded mental health facilities run by the same contractor from booting out patients with severe mental health problems.
The contractor is Kepro, a Pennsylvania-based company. Since December, the health authority has reversed decisions to release 17 patients, according to an article in the Oregonian. The harder line follows revelations by the newspaper of serious harm to patients who had been released before they were capable of caring for themselves.
Kepro was hired by the health authority and paid $27 million to evaluate the medical needs of mental health patients in Oregon. As part of the evaluation, 215 of 250 patients were deemed unqualified to remain in care.
One was Ruane Oliverio, who has schizophrenia, who was kicked out of a locked facility in Portland last June. Clinicians had warned against her release, insisting that her mental state remained too vulnerable. After being hospitalized multiple times, she was sent to the Oregon State Hospital, the highest and most expensive level of care. She was one of those targeted for release. This decision was reversed, and she continues to receive care.
Coalition seeks mental health care for refugees
A new coalition called Matters Involving Neuro-Disorders, or MIND, is trying to help refugees with mental health conditions. The effort is a response to several mental health-related deaths of refugees during 2014-2016, a video produced by the San Diego Union-Tribune said.
“Refugees are brought to this country to help them rebuild their lives,” said Justin Mudekereza, executive director of New Neighbor Relief, a nonprofit organization dedicated to helping refugees adjust to their new lives in the United States. “They have gone through a lot in their countries, then from there, they went to refugee camps, where they spend 15-20 years or more before they got a chance to come to this country.”
Sheila S. Mitra-Sarkar, PhD, of the Institute of Public Urban Affairs at San Diego State University, described the need for a “comprehensive solution” to help refugees adapt to their new society, learn English, find housing and employment, and thrive.
“When I see a patient or someone who seems to have a psychological issue ... I look at everything that goes around them,” said John C. Kuek, PhD, of La Maestra Community Health Centers in San Diego. “I’m looking at the housing issue, the employment issue, and translational issue – meaning they have some family back home and they have a live family here to care for.”
Evidence that American football can lead to chronic traumatic encephalopathy (CTE), continues to grow. As a result, some parents are opting to sign their sons up for other sports.
In the 2017-2018 school year, 6.6% fewer high school athletes participated in tackle football than did 8 years before according to the National Federation of State High School Associations.
Many black parents encourage their sons to play football as a way to protect them gang activity. In addition, the sport can be their sole option for securing a college education for their children, an article in the Atlantic said. A recent survey of 50,000 8th-, 10th-, and 12th-grade students found that tackle football is predominantly the domain of black youth.
“This divergence paints a troubling picture of how economic opportunity – or a lack thereof – governs which boys are incentivized to put their body and brain at risk to play. Depending on where families live, and what other options are available to them, they see either a game that is too violent to consider or one that is necessary and important, if risky. Millions of Americans still watch football; NFL ratings were up this season,” Alana Semuels wrote in the article. “That a distinct portion of families won’t let their children play creates a disturbing future for the country’s most popular game.”
“Without a reversal in economic fortunes for poor communities across the country, football could one day become a sport played almost exclusively by black athletes, while still enjoyed by everyone. Black athletes – who already make up the majority of players in the most dangerous on-field positions – would continue to suffer from long-term brain damage, their life cut short by dementia and the scourge of CTE,” she wrote.
Meanwhile, numerous outlets reported that Super Bowl LIII garnered the lowest ratings since 2008.
Psychiatric hospital set to close
In both Kansas and Missouri, a shortage in mental health care has become evident, according to an article in the Kansas City Star. And now the Two Rivers Behavioral Health System, a private psychiatric hospital in southeast Kansas City, Mo., is closing its doors. The result will be a loss of 129 jobs and 105 fewer mental health beds in the city.
Patients currently in the facility will be relocated, and their care will continue. But for those who come after, care will now be tougher to find.
Two Rivers, owned by Pennsylvania-based Universal Health Services, treats children and adults. It had 2,347 discharges in 2017 and almost $28 million in revenue but had a net loss of about $3.4 million. The facility has been under scrutiny in the past two decades over its treatment of patients, with accusations about the bolstering of false memories concerning involvements in satanic cults and the treatment of a convicted sex offender who assaulted another patient. The most recent state inspection showed that Two Rivers had failed to provide a safe environment for six patients who were considered suicide risks. The patients had unsupervised access to the nurses’ station, as well as access to pens that could have been used for stabbing and a charging cord that could have been used for strangulation.
In an interview with the Star, Mark Stringer, director of the Missouri Department of Mental Health, said private psychiatric hospitals like Two Rivers are finding it harder to keep functioning, partly because of nursing shortages. Private facilities are not subsidized like state mental hospitals and are unable to secure staff from other facilities.
“There is a general worry about the availability of psychiatric services for people in crisis; there’s just no doubt about that,” Mr. Stringer said. “The loss of beds certainly hurts.”
New center offers ‘kind patient care’
In Nashville, Tenn., a new mental illness crisis treatment center is open. The center offers a 24/7 option for those with mental health issues who have run afoul of the law. Instead of incarceration, they can receive treatment, the Tennessean reported.
Estimates are that more than 1 million residents of Tennessee aged 18 years and older have a mental health or substance use disorder. About 25% of those residents having a serious mental health illness.
The new facility includes a crisis walk-in center and a unit where those in the throes of a mental health crisis can seek care. A goal is to get people suffering from an urgent mental illness crisis connected to help faster, especially when they come into contact with police.
“It’s very important to come to a place that’s going to get you help,” Bonnie Kelly said in the article. Ms. Kelly, who reportedly has bipolar disorder, has been arrested several times for disorderly conduct tied to her condition. “It means everything. It is good, kind patient care, rather than just getting you out of the way.”
Aside from benefiting those in need of mental health care, the center will ease the strain on Nashville police, who currently spend more than 5,000 hours each year responding to mental health–related calls. The officers must remain with the person until transfer to a jail or mental health facility is done.
“As a city, we are recognizing that there is a need, and we are investing in that,” East Precinct Commander David Imhof said in the article. “We are helping a population that has had no voice in the past.” Right now, fewer than 60% of patients discharged from state mental health facilities receive any sort of coverage. The result can be cycles of release, arrest, and incarceration.
Agency aims to protect patients
The Oregon Health Authority has stepped in to prevent numerous state-funded mental health facilities run by the same contractor from booting out patients with severe mental health problems.
The contractor is Kepro, a Pennsylvania-based company. Since December, the health authority has reversed decisions to release 17 patients, according to an article in the Oregonian. The harder line follows revelations by the newspaper of serious harm to patients who had been released before they were capable of caring for themselves.
Kepro was hired by the health authority and paid $27 million to evaluate the medical needs of mental health patients in Oregon. As part of the evaluation, 215 of 250 patients were deemed unqualified to remain in care.
One was Ruane Oliverio, who has schizophrenia, who was kicked out of a locked facility in Portland last June. Clinicians had warned against her release, insisting that her mental state remained too vulnerable. After being hospitalized multiple times, she was sent to the Oregon State Hospital, the highest and most expensive level of care. She was one of those targeted for release. This decision was reversed, and she continues to receive care.
Coalition seeks mental health care for refugees
A new coalition called Matters Involving Neuro-Disorders, or MIND, is trying to help refugees with mental health conditions. The effort is a response to several mental health-related deaths of refugees during 2014-2016, a video produced by the San Diego Union-Tribune said.
“Refugees are brought to this country to help them rebuild their lives,” said Justin Mudekereza, executive director of New Neighbor Relief, a nonprofit organization dedicated to helping refugees adjust to their new lives in the United States. “They have gone through a lot in their countries, then from there, they went to refugee camps, where they spend 15-20 years or more before they got a chance to come to this country.”
Sheila S. Mitra-Sarkar, PhD, of the Institute of Public Urban Affairs at San Diego State University, described the need for a “comprehensive solution” to help refugees adapt to their new society, learn English, find housing and employment, and thrive.
“When I see a patient or someone who seems to have a psychological issue ... I look at everything that goes around them,” said John C. Kuek, PhD, of La Maestra Community Health Centers in San Diego. “I’m looking at the housing issue, the employment issue, and translational issue – meaning they have some family back home and they have a live family here to care for.”
Public insurance income limits and hospitalizations for low-income children
Vulnerable populations at greater risk
Background: Medicaid and the Children’s Health Insurance Program (CHIP) provide health care to over 30 million children in the United States.1,2 As a result, low-income children have had increased access to health care, of all forms, which has increased the utilization of primary care and decreased unnecessary ED visits and hospitalizations. However, this comes at a high cost, both at the state and national level. Medicaid currently subsidizes more than 50% of every state’s public insurance program, spending about $100 billion/year in health care payments for children.3 Given this hefty price tag, there have been myriad strategies proposed to help decrease these costs. One such strategy, includes decreasing enrollment in public insurance through decreasing income eligibility thresholds. As a result, many children from low-income families would lose their public insurance and be eligible for commercial insurance only. Consequently, this would place an undue financial burden on these families and the health care systems that care for them. Furthermore, it is anticipated that poor health care outcomes would increase in these vulnerable populations.
Study design: Retrospective cohort study using 2014 State Inpatient Databases.
Setting: Pediatric hospitalizations (aged less than 18 years) from 14 states during 2014 with public insurance listed as the primary payer. This encompassed about 30% of family households in the United States in 2014.
Synopsis: Simulations were done at three different thresholds of the federal poverty level (FPL), including less than 100%, less than 200% and less than 300%. Of the families included, 43% lived below 300%, 27% below 200% and 11% below 100% of the FPL. Of note, public insurance FPL eligibility limits tended to be lower in states with a greater percentage of the population being below 300% of the FPL. The results, of these reductions, were as follows:
- If reduced to less than 300% of the FPL, about 155,000 hospitalizations became ineligible for reimbursement. The median per-hospitalization estimated costs ranged from approximately $6,000 to approximately $10,000, accumulating $1.2 billion in estimated costs.
- If reduced to less than 200% of the FPL, about 440,000 hospitalizations became ineligible for reimbursement. The median per-hospitalization estimated costs ranged from approximately $2,000 to approximately $10,000, accumulating $3.1 billion in estimated costs.
- If reduced to less than 100% of the FPL, about 650,000 hospitalizations became ineligible for reimbursement. The median per-hospitalization estimated costs ranged from approximately $2,000 to approximately $10,000, accumulating $4.4 billion in estimated costs.
If these reductions occurred, healthy newborns would be disproportionately affected by them, which is important to note because newborn hospitalization is one of the fastest-rising costs in pediatric care. In fact, it can range from approximately $700 to approximately $2,000 per hospitalization, which may represent a huge financial strain for families that are unable to secure commercial insurance. Furthermore, with the average hospitalization of non-newborns ranging from $3,000 to $10,000, it is likely that this cost would constitute a fairly large percentage of a low income family’s annual income, which may represent an untenable financial burden.
Thus, if these families are unable to obtain commercial insurance and/or pay these debts, the financial burden will shift to the institutions that care for these vulnerable populations.
Bottom line: If public insurance eligibility thresholds were decreased, a large number of pediatric hospitalizations would become ineligible for coverage, which would shift the costs to families and institutions that are already financially strained and likely result in poor health care outcomes for some of our most vulnerable pediatric patients.
Citation: Bettenhausen JL et al. The effect of lowering public insurance income limits on hospitalizations for low-income children. Pediatrics. 2018 Aug. doi: 10.1542/peds.2017-3486.
Dr. Darden is a pediatric hospitalist at Phoenix Children’s Hospital and clinical assistant professor, University of Arizona, Phoenix.
References
1. The Henry J. Kaiser Family Foundation. Total Medicaid Spending. 2016. Available at: http://kff.org/medicaid/state-indicator/total-medicaid-spending/.
2. Medicaid and CHIP Payment and Access Commission. Trends in Medicaid Spending. 2016. Available at https://www.macpac.gov/wp-content/uploads/2016/06/Trends-in-Medicaid-Spending.pdf.
3. Medicaid and CHIP Payment and Access Commission. Medicaid’s share of state budgets. 2017. Available at: https://www.macpac.gov/subtopic/medicaids-share-of-state-budgets/.
Vulnerable populations at greater risk
Vulnerable populations at greater risk
Background: Medicaid and the Children’s Health Insurance Program (CHIP) provide health care to over 30 million children in the United States.1,2 As a result, low-income children have had increased access to health care, of all forms, which has increased the utilization of primary care and decreased unnecessary ED visits and hospitalizations. However, this comes at a high cost, both at the state and national level. Medicaid currently subsidizes more than 50% of every state’s public insurance program, spending about $100 billion/year in health care payments for children.3 Given this hefty price tag, there have been myriad strategies proposed to help decrease these costs. One such strategy, includes decreasing enrollment in public insurance through decreasing income eligibility thresholds. As a result, many children from low-income families would lose their public insurance and be eligible for commercial insurance only. Consequently, this would place an undue financial burden on these families and the health care systems that care for them. Furthermore, it is anticipated that poor health care outcomes would increase in these vulnerable populations.
Study design: Retrospective cohort study using 2014 State Inpatient Databases.
Setting: Pediatric hospitalizations (aged less than 18 years) from 14 states during 2014 with public insurance listed as the primary payer. This encompassed about 30% of family households in the United States in 2014.
Synopsis: Simulations were done at three different thresholds of the federal poverty level (FPL), including less than 100%, less than 200% and less than 300%. Of the families included, 43% lived below 300%, 27% below 200% and 11% below 100% of the FPL. Of note, public insurance FPL eligibility limits tended to be lower in states with a greater percentage of the population being below 300% of the FPL. The results, of these reductions, were as follows:
- If reduced to less than 300% of the FPL, about 155,000 hospitalizations became ineligible for reimbursement. The median per-hospitalization estimated costs ranged from approximately $6,000 to approximately $10,000, accumulating $1.2 billion in estimated costs.
- If reduced to less than 200% of the FPL, about 440,000 hospitalizations became ineligible for reimbursement. The median per-hospitalization estimated costs ranged from approximately $2,000 to approximately $10,000, accumulating $3.1 billion in estimated costs.
- If reduced to less than 100% of the FPL, about 650,000 hospitalizations became ineligible for reimbursement. The median per-hospitalization estimated costs ranged from approximately $2,000 to approximately $10,000, accumulating $4.4 billion in estimated costs.
If these reductions occurred, healthy newborns would be disproportionately affected by them, which is important to note because newborn hospitalization is one of the fastest-rising costs in pediatric care. In fact, it can range from approximately $700 to approximately $2,000 per hospitalization, which may represent a huge financial strain for families that are unable to secure commercial insurance. Furthermore, with the average hospitalization of non-newborns ranging from $3,000 to $10,000, it is likely that this cost would constitute a fairly large percentage of a low income family’s annual income, which may represent an untenable financial burden.
Thus, if these families are unable to obtain commercial insurance and/or pay these debts, the financial burden will shift to the institutions that care for these vulnerable populations.
Bottom line: If public insurance eligibility thresholds were decreased, a large number of pediatric hospitalizations would become ineligible for coverage, which would shift the costs to families and institutions that are already financially strained and likely result in poor health care outcomes for some of our most vulnerable pediatric patients.
Citation: Bettenhausen JL et al. The effect of lowering public insurance income limits on hospitalizations for low-income children. Pediatrics. 2018 Aug. doi: 10.1542/peds.2017-3486.
Dr. Darden is a pediatric hospitalist at Phoenix Children’s Hospital and clinical assistant professor, University of Arizona, Phoenix.
References
1. The Henry J. Kaiser Family Foundation. Total Medicaid Spending. 2016. Available at: http://kff.org/medicaid/state-indicator/total-medicaid-spending/.
2. Medicaid and CHIP Payment and Access Commission. Trends in Medicaid Spending. 2016. Available at https://www.macpac.gov/wp-content/uploads/2016/06/Trends-in-Medicaid-Spending.pdf.
3. Medicaid and CHIP Payment and Access Commission. Medicaid’s share of state budgets. 2017. Available at: https://www.macpac.gov/subtopic/medicaids-share-of-state-budgets/.
Background: Medicaid and the Children’s Health Insurance Program (CHIP) provide health care to over 30 million children in the United States.1,2 As a result, low-income children have had increased access to health care, of all forms, which has increased the utilization of primary care and decreased unnecessary ED visits and hospitalizations. However, this comes at a high cost, both at the state and national level. Medicaid currently subsidizes more than 50% of every state’s public insurance program, spending about $100 billion/year in health care payments for children.3 Given this hefty price tag, there have been myriad strategies proposed to help decrease these costs. One such strategy, includes decreasing enrollment in public insurance through decreasing income eligibility thresholds. As a result, many children from low-income families would lose their public insurance and be eligible for commercial insurance only. Consequently, this would place an undue financial burden on these families and the health care systems that care for them. Furthermore, it is anticipated that poor health care outcomes would increase in these vulnerable populations.
Study design: Retrospective cohort study using 2014 State Inpatient Databases.
Setting: Pediatric hospitalizations (aged less than 18 years) from 14 states during 2014 with public insurance listed as the primary payer. This encompassed about 30% of family households in the United States in 2014.
Synopsis: Simulations were done at three different thresholds of the federal poverty level (FPL), including less than 100%, less than 200% and less than 300%. Of the families included, 43% lived below 300%, 27% below 200% and 11% below 100% of the FPL. Of note, public insurance FPL eligibility limits tended to be lower in states with a greater percentage of the population being below 300% of the FPL. The results, of these reductions, were as follows:
- If reduced to less than 300% of the FPL, about 155,000 hospitalizations became ineligible for reimbursement. The median per-hospitalization estimated costs ranged from approximately $6,000 to approximately $10,000, accumulating $1.2 billion in estimated costs.
- If reduced to less than 200% of the FPL, about 440,000 hospitalizations became ineligible for reimbursement. The median per-hospitalization estimated costs ranged from approximately $2,000 to approximately $10,000, accumulating $3.1 billion in estimated costs.
- If reduced to less than 100% of the FPL, about 650,000 hospitalizations became ineligible for reimbursement. The median per-hospitalization estimated costs ranged from approximately $2,000 to approximately $10,000, accumulating $4.4 billion in estimated costs.
If these reductions occurred, healthy newborns would be disproportionately affected by them, which is important to note because newborn hospitalization is one of the fastest-rising costs in pediatric care. In fact, it can range from approximately $700 to approximately $2,000 per hospitalization, which may represent a huge financial strain for families that are unable to secure commercial insurance. Furthermore, with the average hospitalization of non-newborns ranging from $3,000 to $10,000, it is likely that this cost would constitute a fairly large percentage of a low income family’s annual income, which may represent an untenable financial burden.
Thus, if these families are unable to obtain commercial insurance and/or pay these debts, the financial burden will shift to the institutions that care for these vulnerable populations.
Bottom line: If public insurance eligibility thresholds were decreased, a large number of pediatric hospitalizations would become ineligible for coverage, which would shift the costs to families and institutions that are already financially strained and likely result in poor health care outcomes for some of our most vulnerable pediatric patients.
Citation: Bettenhausen JL et al. The effect of lowering public insurance income limits on hospitalizations for low-income children. Pediatrics. 2018 Aug. doi: 10.1542/peds.2017-3486.
Dr. Darden is a pediatric hospitalist at Phoenix Children’s Hospital and clinical assistant professor, University of Arizona, Phoenix.
References
1. The Henry J. Kaiser Family Foundation. Total Medicaid Spending. 2016. Available at: http://kff.org/medicaid/state-indicator/total-medicaid-spending/.
2. Medicaid and CHIP Payment and Access Commission. Trends in Medicaid Spending. 2016. Available at https://www.macpac.gov/wp-content/uploads/2016/06/Trends-in-Medicaid-Spending.pdf.
3. Medicaid and CHIP Payment and Access Commission. Medicaid’s share of state budgets. 2017. Available at: https://www.macpac.gov/subtopic/medicaids-share-of-state-budgets/.
Product Update: Bijuva; Liletta; Aegea Vapor System; Natural Cycles
TREATMENT FOR VASOMOTOR SYMPTOMS

BIJUVA™ has been US Food and Drug Administration (FDA)–approved as the first oral treatment for moderate-to-severe vasomotor symptoms due to menopause in women with a uterus. BIJUVA offers a combination of bioidentical estradiol to reduce moderate-to-severe hot flashes and bioidentical progesterone to reduce the risk for endometrial hyperplasia.
TherapeuticsMD says that BIJUVA will be available Spring 2019 and is a proven treatment option for women who are experiencing bothersome symptoms of menopause, with clinical trial data demonstrating a statistically significant reduction in both the frequency and severity of moderate-to-severe vasomotor symptoms. The manufacturer also says that BIJUVA is developed to be identical in molecular structure to the hormones already produced by the body and is designed to help women restore what is lost during menopause.
BIJUVA estradiol and progesterone combination (1 mg/100 mg) will be available in capsule form.
FOR MORE INFORMATION, VISIT:https://bijuva.com/discover/
LILETTA USE EXTENDED

The FDA has approved LILETTA® (levonorgestrel-releasing intrauterine system) 52 mg for 5-year use. This approval is based on efficacy and safety data from ACCESS IUS, the largest ongoing intrauterine device (IUD) Phase 3 clinical trial in the United States. Previously, LILETTA was indicated for use up to 4 years.
LILETTA continues to be greater than 99% effective in preventing pregnancy in a broad range of women, regardless of age, race, body mass index, or parity, according to Allergan and Medicines360. The extended duration and proven efficacy across a diverse population enables more women in the United States to obtain effective birth control, as the IUD is now available for a low cost at public health clinics.
FOR MORE INFORMATION, VISIT: https://www.liletta.com
Continue to: ENDOMETRIAL ABLATION TECHNOLOGY
ENDOMETRIAL ABLATION TECHNOLOGY

AEGEA Medical introduces the AEGEA Vapor SystemTM, an innovative solution for endometrial ablation to treat menorrhagia.
The system uses Adaptive Vapor Ablation and is the first endometrial ablation system specifically designed for use in the doctor’s office, allowing minimal anesthesia/analgesia and rapid recovery, says AEGEA Medical.
AEGEA Medical describes the AEGEA Vapor System as a fully automated safety monitoring and vapor delivery system that uses a slender, flexible Vapor Probe with SmartSealTM technology and the Integrity ProTM safety feature, for an added level of confidence. The 4-minute procedure time includes 2 minutes of vapor treatment and can be performed in patients with a wider range of uterine anatomies than indicated for use with currently available treatments, says AEGEA Medical.
FOR MORE INFORMATION, VISIT: http://aegeamedical.com/
NATURAL CYCLES

The FDA has cleared Natural Cycles as the first digital method of birth control in the United States. Delivered in the form of an app, Natural Cycles is a fertility awareness–based contraceptive that uses a sophisticated algorithm to accurately and conveniently determine a woman’s daily fertility based on basal body temperature.
That data builds into a personalized fertility indicator that informs her when she needs to use protection to minimize the chance of conception. The app also can be used to help plan a pregnancy when the time is right, according to Natural Cycles.
A clinical study showed that the efficacy of a contraceptive mobile application is higher than usually reported for traditional fertility awareness–based methods. The application may contribute to reducing the unmet need for contraception, says Natural Cycles.
FOR MORE INFORMATION, VISIT: https://www.naturalcycles.com/en/hcp
TREATMENT FOR VASOMOTOR SYMPTOMS
BIJUVA™ has been US Food and Drug Administration (FDA)–approved as the first oral treatment for moderate-to-severe vasomotor symptoms due to menopause in women with a uterus. BIJUVA offers a combination of bioidentical estradiol to reduce moderate-to-severe hot flashes and bioidentical progesterone to reduce the risk for endometrial hyperplasia.
TherapeuticsMD says that BIJUVA will be available Spring 2019 and is a proven treatment option for women who are experiencing bothersome symptoms of menopause, with clinical trial data demonstrating a statistically significant reduction in both the frequency and severity of moderate-to-severe vasomotor symptoms. The manufacturer also says that BIJUVA is developed to be identical in molecular structure to the hormones already produced by the body and is designed to help women restore what is lost during menopause.
BIJUVA estradiol and progesterone combination (1 mg/100 mg) will be available in capsule form.
FOR MORE INFORMATION, VISIT:https://bijuva.com/discover/
LILETTA USE EXTENDED
The FDA has approved LILETTA® (levonorgestrel-releasing intrauterine system) 52 mg for 5-year use. This approval is based on efficacy and safety data from ACCESS IUS, the largest ongoing intrauterine device (IUD) Phase 3 clinical trial in the United States. Previously, LILETTA was indicated for use up to 4 years.
LILETTA continues to be greater than 99% effective in preventing pregnancy in a broad range of women, regardless of age, race, body mass index, or parity, according to Allergan and Medicines360. The extended duration and proven efficacy across a diverse population enables more women in the United States to obtain effective birth control, as the IUD is now available for a low cost at public health clinics.
FOR MORE INFORMATION, VISIT: https://www.liletta.com
Continue to: ENDOMETRIAL ABLATION TECHNOLOGY
ENDOMETRIAL ABLATION TECHNOLOGY
AEGEA Medical introduces the AEGEA Vapor SystemTM, an innovative solution for endometrial ablation to treat menorrhagia.
The system uses Adaptive Vapor Ablation and is the first endometrial ablation system specifically designed for use in the doctor’s office, allowing minimal anesthesia/analgesia and rapid recovery, says AEGEA Medical.
AEGEA Medical describes the AEGEA Vapor System as a fully automated safety monitoring and vapor delivery system that uses a slender, flexible Vapor Probe with SmartSealTM technology and the Integrity ProTM safety feature, for an added level of confidence. The 4-minute procedure time includes 2 minutes of vapor treatment and can be performed in patients with a wider range of uterine anatomies than indicated for use with currently available treatments, says AEGEA Medical.
FOR MORE INFORMATION, VISIT: http://aegeamedical.com/
NATURAL CYCLES
The FDA has cleared Natural Cycles as the first digital method of birth control in the United States. Delivered in the form of an app, Natural Cycles is a fertility awareness–based contraceptive that uses a sophisticated algorithm to accurately and conveniently determine a woman’s daily fertility based on basal body temperature.
That data builds into a personalized fertility indicator that informs her when she needs to use protection to minimize the chance of conception. The app also can be used to help plan a pregnancy when the time is right, according to Natural Cycles.
A clinical study showed that the efficacy of a contraceptive mobile application is higher than usually reported for traditional fertility awareness–based methods. The application may contribute to reducing the unmet need for contraception, says Natural Cycles.
FOR MORE INFORMATION, VISIT: https://www.naturalcycles.com/en/hcp
TREATMENT FOR VASOMOTOR SYMPTOMS
BIJUVA™ has been US Food and Drug Administration (FDA)–approved as the first oral treatment for moderate-to-severe vasomotor symptoms due to menopause in women with a uterus. BIJUVA offers a combination of bioidentical estradiol to reduce moderate-to-severe hot flashes and bioidentical progesterone to reduce the risk for endometrial hyperplasia.
TherapeuticsMD says that BIJUVA will be available Spring 2019 and is a proven treatment option for women who are experiencing bothersome symptoms of menopause, with clinical trial data demonstrating a statistically significant reduction in both the frequency and severity of moderate-to-severe vasomotor symptoms. The manufacturer also says that BIJUVA is developed to be identical in molecular structure to the hormones already produced by the body and is designed to help women restore what is lost during menopause.
BIJUVA estradiol and progesterone combination (1 mg/100 mg) will be available in capsule form.
FOR MORE INFORMATION, VISIT:https://bijuva.com/discover/
LILETTA USE EXTENDED
The FDA has approved LILETTA® (levonorgestrel-releasing intrauterine system) 52 mg for 5-year use. This approval is based on efficacy and safety data from ACCESS IUS, the largest ongoing intrauterine device (IUD) Phase 3 clinical trial in the United States. Previously, LILETTA was indicated for use up to 4 years.
LILETTA continues to be greater than 99% effective in preventing pregnancy in a broad range of women, regardless of age, race, body mass index, or parity, according to Allergan and Medicines360. The extended duration and proven efficacy across a diverse population enables more women in the United States to obtain effective birth control, as the IUD is now available for a low cost at public health clinics.
FOR MORE INFORMATION, VISIT: https://www.liletta.com
Continue to: ENDOMETRIAL ABLATION TECHNOLOGY
ENDOMETRIAL ABLATION TECHNOLOGY
AEGEA Medical introduces the AEGEA Vapor SystemTM, an innovative solution for endometrial ablation to treat menorrhagia.
The system uses Adaptive Vapor Ablation and is the first endometrial ablation system specifically designed for use in the doctor’s office, allowing minimal anesthesia/analgesia and rapid recovery, says AEGEA Medical.
AEGEA Medical describes the AEGEA Vapor System as a fully automated safety monitoring and vapor delivery system that uses a slender, flexible Vapor Probe with SmartSealTM technology and the Integrity ProTM safety feature, for an added level of confidence. The 4-minute procedure time includes 2 minutes of vapor treatment and can be performed in patients with a wider range of uterine anatomies than indicated for use with currently available treatments, says AEGEA Medical.
FOR MORE INFORMATION, VISIT: http://aegeamedical.com/
NATURAL CYCLES
The FDA has cleared Natural Cycles as the first digital method of birth control in the United States. Delivered in the form of an app, Natural Cycles is a fertility awareness–based contraceptive that uses a sophisticated algorithm to accurately and conveniently determine a woman’s daily fertility based on basal body temperature.
That data builds into a personalized fertility indicator that informs her when she needs to use protection to minimize the chance of conception. The app also can be used to help plan a pregnancy when the time is right, according to Natural Cycles.
A clinical study showed that the efficacy of a contraceptive mobile application is higher than usually reported for traditional fertility awareness–based methods. The application may contribute to reducing the unmet need for contraception, says Natural Cycles.
FOR MORE INFORMATION, VISIT: https://www.naturalcycles.com/en/hcp
Michigan Medicine launches effort to make wellness a cultural norm
CORONADO, CALIF. – Officials at staff, and learners.

“If you look long and hard at your hospitals, health centers, and medical schools, you would find incidences of depression, near-miss suicide, opioid addiction, substance abuse addictions, and suicide,” Carol R. Bradford, MD, said at the Triological Society’s Combined Sections Meeting. “Another component of this is that we all struggle with our work or learning communities where people don’t take care of each other. People don’t treat each other with respect and civility. Promoting a healthy and civil work environment are essential components of a supportive environment.”
According to Dr. Bradford, executive vice dean for academic affairs at the University of Michigan, Ann Arbor, the complexities and stress of the health care environment compromises the well-being of its workforce with a myriad of time-consuming tasks, including navigating electronic records and ever-populating email inboxes. “We are all connected to devices 24/7, and it has become more and more difficult to maintain a healthy work-life balance,” Dr. Bradford said. “The more accepted term now is integration, because it’s almost impossible to achieve balance. Burnout and other physical and health problems are the result of all of these challenges.”
In late 2017, she and her colleagues used two different validated survey questionnaires to assess the health of Michigan Medicine faculty physicians. They found that about 40% of faculty members in both clinical and basic science departments met criteria for burnout. The top 10 stressors based on the survey were email, clerical activity, time worked outside of regular hours, workload time pressure, work expectations, insufficient time for meaningful activities, in-basket messages, lack of decisional transparency, inadequate compensation, and too many work hours. The top 10 coping strategies were finding meaning in work, using all vacation time, paying attention to healthy/balanced eating, engaging in exercise, seek personal/professional balance, protecting time away from work, protecting sleep time, using a social support network, nurturing spiritual aspects, and engaging in recreation or hobbies.
Results of the survey prompted development of a task force to examine wellness and civility at Michigan Medicine, and to devise strategies and tactics to conquer these challenges. “The goal is to help all human beings who are suffering in our work environment,” said Dr. Bradford, who is also chief academic officer for Michigan Medicine. “What we learned initially is that there is a bit of an overlap. Some lack of wellness is due to a lack of civility, but there are wellness issues and civility issues that are independent of one another.”
Members of the task force formulated several recommendations, the first being to create a Michigan Medicine Wellness Office. Dr. Bradford is currently negotiating with a finalist to serve as its faculty director. She characterized the office as a “hub and spoke” model that will partner with existing entities, including human resources, the office of medical student education, the program in biological sciences, graduate medical education, the office of health equality and inclusion, the office of clinical affairs, and the office of counseling and workplace resilience. “The idea is to create a strategic wellness plan,” said Dr. Bradford, who is also a professor of otolaryngology–head and neck surgery. “One key strategy is to endorse the health and well-being of our faculty, staff, and learners as a core value and cultural norm of Michigan Medicine. In other words, the leadership has to make health and well-being a priority and a value.”
Another goal of the office is to improve the overall workplace environment and experience of Michigan Medicine’s faculty, staff, and learners. “You’re not going to have a well workplace if people are not treating each other with respect,” she said at the meeting, jointly sponsored by the Triological Society and the American College of Surgeons. “One of the many challenges is that there is great stigma in our profession for those who are suffering from mental health challenges such as stress, anxiety, depression, and perhaps substance abuse. We need to reduce the stigma, because it’s very dangerous if people who are struggling are unwilling to seek help. We don’t ask people that we supervise or work with how they’re doing, so we have adopted an optional wellness check-in that is incorporated into mid-year and annual evaluations for faculty, staff, and learners to enable leaders to address any challenges that may arise.” In addition, a group of residents is piloting the use of meditation and mindfulness applications such as MoodGym and Headspace to see if they affect resident wellness.
Ultimately, Dr. Bradford and her associates plan to use a standardized benchmark instrument to measure well-being, and include the measure in the institutional performance dashboard. “Administrative burden is a growing problem,” she said. “We’re going to address this for health care professionals, particularly as it relates to the electronic medical record. Our primary care colleagues sometimes spend as many hours outside of clinic documenting as they do in clinic. We want to develop and implement strategies to lessen or remove this burden in order to improve provider efficiency and satisfaction.”
In the course of helping to develop the wellness initiative, Dr. Bradford said that she learned the importance of addressing moral distress in the workplace. “We sort of lose our humanity if we don’t show emotion when tragedies happen. There is really good literature around terminal event debriefings, so if somebody dies unexpectedly in the operating room or in the CT scanner, rather than just walking away and pretending nothing happened, we’re supposed to pause and gather, and reflect on the sadness of the loss. Because if we don’t grieve our losses we become more like machines than human beings. It’s important to provide emotional support for all individuals involved.”
She reported having no relevant financial disclosures.
CORONADO, CALIF. – Officials at staff, and learners.
“If you look long and hard at your hospitals, health centers, and medical schools, you would find incidences of depression, near-miss suicide, opioid addiction, substance abuse addictions, and suicide,” Carol R. Bradford, MD, said at the Triological Society’s Combined Sections Meeting. “Another component of this is that we all struggle with our work or learning communities where people don’t take care of each other. People don’t treat each other with respect and civility. Promoting a healthy and civil work environment are essential components of a supportive environment.”
According to Dr. Bradford, executive vice dean for academic affairs at the University of Michigan, Ann Arbor, the complexities and stress of the health care environment compromises the well-being of its workforce with a myriad of time-consuming tasks, including navigating electronic records and ever-populating email inboxes. “We are all connected to devices 24/7, and it has become more and more difficult to maintain a healthy work-life balance,” Dr. Bradford said. “The more accepted term now is integration, because it’s almost impossible to achieve balance. Burnout and other physical and health problems are the result of all of these challenges.”
In late 2017, she and her colleagues used two different validated survey questionnaires to assess the health of Michigan Medicine faculty physicians. They found that about 40% of faculty members in both clinical and basic science departments met criteria for burnout. The top 10 stressors based on the survey were email, clerical activity, time worked outside of regular hours, workload time pressure, work expectations, insufficient time for meaningful activities, in-basket messages, lack of decisional transparency, inadequate compensation, and too many work hours. The top 10 coping strategies were finding meaning in work, using all vacation time, paying attention to healthy/balanced eating, engaging in exercise, seek personal/professional balance, protecting time away from work, protecting sleep time, using a social support network, nurturing spiritual aspects, and engaging in recreation or hobbies.
Results of the survey prompted development of a task force to examine wellness and civility at Michigan Medicine, and to devise strategies and tactics to conquer these challenges. “The goal is to help all human beings who are suffering in our work environment,” said Dr. Bradford, who is also chief academic officer for Michigan Medicine. “What we learned initially is that there is a bit of an overlap. Some lack of wellness is due to a lack of civility, but there are wellness issues and civility issues that are independent of one another.”
Members of the task force formulated several recommendations, the first being to create a Michigan Medicine Wellness Office. Dr. Bradford is currently negotiating with a finalist to serve as its faculty director. She characterized the office as a “hub and spoke” model that will partner with existing entities, including human resources, the office of medical student education, the program in biological sciences, graduate medical education, the office of health equality and inclusion, the office of clinical affairs, and the office of counseling and workplace resilience. “The idea is to create a strategic wellness plan,” said Dr. Bradford, who is also a professor of otolaryngology–head and neck surgery. “One key strategy is to endorse the health and well-being of our faculty, staff, and learners as a core value and cultural norm of Michigan Medicine. In other words, the leadership has to make health and well-being a priority and a value.”
Another goal of the office is to improve the overall workplace environment and experience of Michigan Medicine’s faculty, staff, and learners. “You’re not going to have a well workplace if people are not treating each other with respect,” she said at the meeting, jointly sponsored by the Triological Society and the American College of Surgeons. “One of the many challenges is that there is great stigma in our profession for those who are suffering from mental health challenges such as stress, anxiety, depression, and perhaps substance abuse. We need to reduce the stigma, because it’s very dangerous if people who are struggling are unwilling to seek help. We don’t ask people that we supervise or work with how they’re doing, so we have adopted an optional wellness check-in that is incorporated into mid-year and annual evaluations for faculty, staff, and learners to enable leaders to address any challenges that may arise.” In addition, a group of residents is piloting the use of meditation and mindfulness applications such as MoodGym and Headspace to see if they affect resident wellness.
Ultimately, Dr. Bradford and her associates plan to use a standardized benchmark instrument to measure well-being, and include the measure in the institutional performance dashboard. “Administrative burden is a growing problem,” she said. “We’re going to address this for health care professionals, particularly as it relates to the electronic medical record. Our primary care colleagues sometimes spend as many hours outside of clinic documenting as they do in clinic. We want to develop and implement strategies to lessen or remove this burden in order to improve provider efficiency and satisfaction.”
In the course of helping to develop the wellness initiative, Dr. Bradford said that she learned the importance of addressing moral distress in the workplace. “We sort of lose our humanity if we don’t show emotion when tragedies happen. There is really good literature around terminal event debriefings, so if somebody dies unexpectedly in the operating room or in the CT scanner, rather than just walking away and pretending nothing happened, we’re supposed to pause and gather, and reflect on the sadness of the loss. Because if we don’t grieve our losses we become more like machines than human beings. It’s important to provide emotional support for all individuals involved.”
She reported having no relevant financial disclosures.
CORONADO, CALIF. – Officials at staff, and learners.
“If you look long and hard at your hospitals, health centers, and medical schools, you would find incidences of depression, near-miss suicide, opioid addiction, substance abuse addictions, and suicide,” Carol R. Bradford, MD, said at the Triological Society’s Combined Sections Meeting. “Another component of this is that we all struggle with our work or learning communities where people don’t take care of each other. People don’t treat each other with respect and civility. Promoting a healthy and civil work environment are essential components of a supportive environment.”
According to Dr. Bradford, executive vice dean for academic affairs at the University of Michigan, Ann Arbor, the complexities and stress of the health care environment compromises the well-being of its workforce with a myriad of time-consuming tasks, including navigating electronic records and ever-populating email inboxes. “We are all connected to devices 24/7, and it has become more and more difficult to maintain a healthy work-life balance,” Dr. Bradford said. “The more accepted term now is integration, because it’s almost impossible to achieve balance. Burnout and other physical and health problems are the result of all of these challenges.”
In late 2017, she and her colleagues used two different validated survey questionnaires to assess the health of Michigan Medicine faculty physicians. They found that about 40% of faculty members in both clinical and basic science departments met criteria for burnout. The top 10 stressors based on the survey were email, clerical activity, time worked outside of regular hours, workload time pressure, work expectations, insufficient time for meaningful activities, in-basket messages, lack of decisional transparency, inadequate compensation, and too many work hours. The top 10 coping strategies were finding meaning in work, using all vacation time, paying attention to healthy/balanced eating, engaging in exercise, seek personal/professional balance, protecting time away from work, protecting sleep time, using a social support network, nurturing spiritual aspects, and engaging in recreation or hobbies.
Results of the survey prompted development of a task force to examine wellness and civility at Michigan Medicine, and to devise strategies and tactics to conquer these challenges. “The goal is to help all human beings who are suffering in our work environment,” said Dr. Bradford, who is also chief academic officer for Michigan Medicine. “What we learned initially is that there is a bit of an overlap. Some lack of wellness is due to a lack of civility, but there are wellness issues and civility issues that are independent of one another.”
Members of the task force formulated several recommendations, the first being to create a Michigan Medicine Wellness Office. Dr. Bradford is currently negotiating with a finalist to serve as its faculty director. She characterized the office as a “hub and spoke” model that will partner with existing entities, including human resources, the office of medical student education, the program in biological sciences, graduate medical education, the office of health equality and inclusion, the office of clinical affairs, and the office of counseling and workplace resilience. “The idea is to create a strategic wellness plan,” said Dr. Bradford, who is also a professor of otolaryngology–head and neck surgery. “One key strategy is to endorse the health and well-being of our faculty, staff, and learners as a core value and cultural norm of Michigan Medicine. In other words, the leadership has to make health and well-being a priority and a value.”
Another goal of the office is to improve the overall workplace environment and experience of Michigan Medicine’s faculty, staff, and learners. “You’re not going to have a well workplace if people are not treating each other with respect,” she said at the meeting, jointly sponsored by the Triological Society and the American College of Surgeons. “One of the many challenges is that there is great stigma in our profession for those who are suffering from mental health challenges such as stress, anxiety, depression, and perhaps substance abuse. We need to reduce the stigma, because it’s very dangerous if people who are struggling are unwilling to seek help. We don’t ask people that we supervise or work with how they’re doing, so we have adopted an optional wellness check-in that is incorporated into mid-year and annual evaluations for faculty, staff, and learners to enable leaders to address any challenges that may arise.” In addition, a group of residents is piloting the use of meditation and mindfulness applications such as MoodGym and Headspace to see if they affect resident wellness.
Ultimately, Dr. Bradford and her associates plan to use a standardized benchmark instrument to measure well-being, and include the measure in the institutional performance dashboard. “Administrative burden is a growing problem,” she said. “We’re going to address this for health care professionals, particularly as it relates to the electronic medical record. Our primary care colleagues sometimes spend as many hours outside of clinic documenting as they do in clinic. We want to develop and implement strategies to lessen or remove this burden in order to improve provider efficiency and satisfaction.”
In the course of helping to develop the wellness initiative, Dr. Bradford said that she learned the importance of addressing moral distress in the workplace. “We sort of lose our humanity if we don’t show emotion when tragedies happen. There is really good literature around terminal event debriefings, so if somebody dies unexpectedly in the operating room or in the CT scanner, rather than just walking away and pretending nothing happened, we’re supposed to pause and gather, and reflect on the sadness of the loss. Because if we don’t grieve our losses we become more like machines than human beings. It’s important to provide emotional support for all individuals involved.”
She reported having no relevant financial disclosures.
EXPERT ANALYSIS FROM THE TRIOLOGICAL CSM
HHS effort aims to end new HIV cases within 10 years
WASHINGTON – Leaders from five federal agencies came together to announce the framework for a bold new national initiative that aims to eliminate new cases of HIV infection in the United States within 10 years. The announcement came the day after President Trump’s State of the Union address, which highlighted the new effort.

“HIV has cost America too much for too long,” said Adm. Brett Giroir, MD, assistant secretary for health at the Department of Health & Human Services, in a press briefing. In addition to the 700,000 U.S. lives the disease has claimed since 1981, “We are at high risk of another 400,000 becoming infected over the next decade,” with about 40,000 new infections still occurring every year, he said.
Dr. Giroir will lead a coordinated effort among HHS, the Centers for Disease Control, the National Institutes of Health, the Health Resources and Services Administration, and the Indian Health Service. The goals are to reduce new cases of HIV by 50% within 5 years, and by 90% within 10 years.
These 48 counties, together with Washington and San Juan, Puerto Rico, accounted for more than half of the new HIV diagnoses in 2016 and 2017, said Dr. Giroir.
“This is a laser-focused program targeting counties where infection is the highest,” said CDC Director Robert R. Redfield, MD. “We propose to deploy personnel, resources, and strategies” in these targeted areas to maximize not just diagnosis and treatment but also to reach those at risk for HIV to enroll them in preexposure prophylaxis (PrEP) regimens, he said.
In addition to the targeted counties, seven states in the rural South as well as Native American and Alaskan Native populations also will receive intensified education, diagnostic, and treatment services. The targeted states are Alabama, Arkansas, Kentucky, Mississippi, Missouri, Oklahoma, and South Carolina.
George Sigounas, PhD, administrator or the Health Resources and Services Administration, said that existing community health centers will be especially important in reaching rural underserved and marginalized populations. Currently, he said, HRSA supports 12,000 service delivery sites across the country that are already delivering care to 27 million individuals. “These sites will play a major expanded role in providing PrEP to those who are at the greatest risk of contracting HIV,” said Dr. Sigounas.
Among the currently existing resources that will be leveraged are services provided by the Ryan White HIV/AIDS program, which already provides HIV primary medical care and support services through a network of grants to states and local government and community organizations. About half of the people currently diagnosed with HIV in the United States receive services through this program now.
The NIH maintains a geographically distributed network of Centers for AIDS Research that also will be folded into the new initiative.
In his remarks, Anthony S. Fauci, MD, director of the NIH’s National Center for Allergy and Infectious Diseases, pointed out that, “Treatment and detection are wrapped together, because treated individuals can’t transmit HIV” if they are adherent to antiretroviral medication use and achieve an undetectable viral load, he said. “If you get everyone who’s infected on antiretrovirals and give those who need it PrEP, you can theoretically end the epidemic as we know it – and that is our goal.”
Dr. Fauci went on to say that implementation science will play a key role in achieving a targeted and coordinated approach. “We will work closely with our colleagues to make sure the implementation is done well. We have lessons learned; we will do better and better,” he said.
The nuts and bolts of the program include a four-pronged strategy to diagnose individuals as early as possible after infection, to initiate prompt, effective, and sustained treatment, to protect those at risk for HIV by proven means including PrEP, and to provide rapid response when new HIV clusters are identified. A reimagining of current and future personnel into an “HIV health force” will put teams on the ground in each jurisdiction to carry out the initiative.
Though the goal is to provide PrEP to every at-risk individual, Dr. Fauci said that current modeling shows that if PrEP reaches 50%-60% in the at-risk population, new infections can be reduced by 90%. He added, “PrEP works. The efficacy is well over 90%.”
Funding details were not released at the press briefing; Dr. Giroir said that figures will be released by the Office of Management and Budget as part of the 2020 budget cycle. He confirmed, however, that new funds will be allocated for the effort, rather than a mere reshuffling of existing fund and resources.
Several of the leaders acknowledged the problem of stigma and marginalization that many individuals living with or at risk for HIV face, since men who have sex with men, transgender people, sex workers, and those with opioid use disorder all fall into this category.
“Every American deserves to be treated with respect and dignity. We will vigorously enforce all laws on the books about discrimination,” said Rear Adm. Michael Weahkee, MD, principal deputy director of the Indian Health Service. This is especially important in Native American communities “where everybody knows everybody,” he said, and it’s vitally important to include individual and community education in the efforts.
Dr. Redfield concurred, adding that “Dr. Fauci and I have been engaged in HIV since 1981. We have witnessed firsthand the negative impact that stigma can have on our capacity to practice public health. The transgender population, in particular, needs to be reached out to. We need to be able to address in a comprehensive way how to destigmatize the HIV population.”
WASHINGTON – Leaders from five federal agencies came together to announce the framework for a bold new national initiative that aims to eliminate new cases of HIV infection in the United States within 10 years. The announcement came the day after President Trump’s State of the Union address, which highlighted the new effort.
“HIV has cost America too much for too long,” said Adm. Brett Giroir, MD, assistant secretary for health at the Department of Health & Human Services, in a press briefing. In addition to the 700,000 U.S. lives the disease has claimed since 1981, “We are at high risk of another 400,000 becoming infected over the next decade,” with about 40,000 new infections still occurring every year, he said.
Dr. Giroir will lead a coordinated effort among HHS, the Centers for Disease Control, the National Institutes of Health, the Health Resources and Services Administration, and the Indian Health Service. The goals are to reduce new cases of HIV by 50% within 5 years, and by 90% within 10 years.
These 48 counties, together with Washington and San Juan, Puerto Rico, accounted for more than half of the new HIV diagnoses in 2016 and 2017, said Dr. Giroir.
“This is a laser-focused program targeting counties where infection is the highest,” said CDC Director Robert R. Redfield, MD. “We propose to deploy personnel, resources, and strategies” in these targeted areas to maximize not just diagnosis and treatment but also to reach those at risk for HIV to enroll them in preexposure prophylaxis (PrEP) regimens, he said.
In addition to the targeted counties, seven states in the rural South as well as Native American and Alaskan Native populations also will receive intensified education, diagnostic, and treatment services. The targeted states are Alabama, Arkansas, Kentucky, Mississippi, Missouri, Oklahoma, and South Carolina.
George Sigounas, PhD, administrator or the Health Resources and Services Administration, said that existing community health centers will be especially important in reaching rural underserved and marginalized populations. Currently, he said, HRSA supports 12,000 service delivery sites across the country that are already delivering care to 27 million individuals. “These sites will play a major expanded role in providing PrEP to those who are at the greatest risk of contracting HIV,” said Dr. Sigounas.
Among the currently existing resources that will be leveraged are services provided by the Ryan White HIV/AIDS program, which already provides HIV primary medical care and support services through a network of grants to states and local government and community organizations. About half of the people currently diagnosed with HIV in the United States receive services through this program now.
The NIH maintains a geographically distributed network of Centers for AIDS Research that also will be folded into the new initiative.
In his remarks, Anthony S. Fauci, MD, director of the NIH’s National Center for Allergy and Infectious Diseases, pointed out that, “Treatment and detection are wrapped together, because treated individuals can’t transmit HIV” if they are adherent to antiretroviral medication use and achieve an undetectable viral load, he said. “If you get everyone who’s infected on antiretrovirals and give those who need it PrEP, you can theoretically end the epidemic as we know it – and that is our goal.”
Dr. Fauci went on to say that implementation science will play a key role in achieving a targeted and coordinated approach. “We will work closely with our colleagues to make sure the implementation is done well. We have lessons learned; we will do better and better,” he said.
The nuts and bolts of the program include a four-pronged strategy to diagnose individuals as early as possible after infection, to initiate prompt, effective, and sustained treatment, to protect those at risk for HIV by proven means including PrEP, and to provide rapid response when new HIV clusters are identified. A reimagining of current and future personnel into an “HIV health force” will put teams on the ground in each jurisdiction to carry out the initiative.
Though the goal is to provide PrEP to every at-risk individual, Dr. Fauci said that current modeling shows that if PrEP reaches 50%-60% in the at-risk population, new infections can be reduced by 90%. He added, “PrEP works. The efficacy is well over 90%.”
Funding details were not released at the press briefing; Dr. Giroir said that figures will be released by the Office of Management and Budget as part of the 2020 budget cycle. He confirmed, however, that new funds will be allocated for the effort, rather than a mere reshuffling of existing fund and resources.
Several of the leaders acknowledged the problem of stigma and marginalization that many individuals living with or at risk for HIV face, since men who have sex with men, transgender people, sex workers, and those with opioid use disorder all fall into this category.
“Every American deserves to be treated with respect and dignity. We will vigorously enforce all laws on the books about discrimination,” said Rear Adm. Michael Weahkee, MD, principal deputy director of the Indian Health Service. This is especially important in Native American communities “where everybody knows everybody,” he said, and it’s vitally important to include individual and community education in the efforts.
Dr. Redfield concurred, adding that “Dr. Fauci and I have been engaged in HIV since 1981. We have witnessed firsthand the negative impact that stigma can have on our capacity to practice public health. The transgender population, in particular, needs to be reached out to. We need to be able to address in a comprehensive way how to destigmatize the HIV population.”
WASHINGTON – Leaders from five federal agencies came together to announce the framework for a bold new national initiative that aims to eliminate new cases of HIV infection in the United States within 10 years. The announcement came the day after President Trump’s State of the Union address, which highlighted the new effort.
“HIV has cost America too much for too long,” said Adm. Brett Giroir, MD, assistant secretary for health at the Department of Health & Human Services, in a press briefing. In addition to the 700,000 U.S. lives the disease has claimed since 1981, “We are at high risk of another 400,000 becoming infected over the next decade,” with about 40,000 new infections still occurring every year, he said.
Dr. Giroir will lead a coordinated effort among HHS, the Centers for Disease Control, the National Institutes of Health, the Health Resources and Services Administration, and the Indian Health Service. The goals are to reduce new cases of HIV by 50% within 5 years, and by 90% within 10 years.
These 48 counties, together with Washington and San Juan, Puerto Rico, accounted for more than half of the new HIV diagnoses in 2016 and 2017, said Dr. Giroir.
“This is a laser-focused program targeting counties where infection is the highest,” said CDC Director Robert R. Redfield, MD. “We propose to deploy personnel, resources, and strategies” in these targeted areas to maximize not just diagnosis and treatment but also to reach those at risk for HIV to enroll them in preexposure prophylaxis (PrEP) regimens, he said.
In addition to the targeted counties, seven states in the rural South as well as Native American and Alaskan Native populations also will receive intensified education, diagnostic, and treatment services. The targeted states are Alabama, Arkansas, Kentucky, Mississippi, Missouri, Oklahoma, and South Carolina.
George Sigounas, PhD, administrator or the Health Resources and Services Administration, said that existing community health centers will be especially important in reaching rural underserved and marginalized populations. Currently, he said, HRSA supports 12,000 service delivery sites across the country that are already delivering care to 27 million individuals. “These sites will play a major expanded role in providing PrEP to those who are at the greatest risk of contracting HIV,” said Dr. Sigounas.
Among the currently existing resources that will be leveraged are services provided by the Ryan White HIV/AIDS program, which already provides HIV primary medical care and support services through a network of grants to states and local government and community organizations. About half of the people currently diagnosed with HIV in the United States receive services through this program now.
The NIH maintains a geographically distributed network of Centers for AIDS Research that also will be folded into the new initiative.
In his remarks, Anthony S. Fauci, MD, director of the NIH’s National Center for Allergy and Infectious Diseases, pointed out that, “Treatment and detection are wrapped together, because treated individuals can’t transmit HIV” if they are adherent to antiretroviral medication use and achieve an undetectable viral load, he said. “If you get everyone who’s infected on antiretrovirals and give those who need it PrEP, you can theoretically end the epidemic as we know it – and that is our goal.”
Dr. Fauci went on to say that implementation science will play a key role in achieving a targeted and coordinated approach. “We will work closely with our colleagues to make sure the implementation is done well. We have lessons learned; we will do better and better,” he said.
The nuts and bolts of the program include a four-pronged strategy to diagnose individuals as early as possible after infection, to initiate prompt, effective, and sustained treatment, to protect those at risk for HIV by proven means including PrEP, and to provide rapid response when new HIV clusters are identified. A reimagining of current and future personnel into an “HIV health force” will put teams on the ground in each jurisdiction to carry out the initiative.
Though the goal is to provide PrEP to every at-risk individual, Dr. Fauci said that current modeling shows that if PrEP reaches 50%-60% in the at-risk population, new infections can be reduced by 90%. He added, “PrEP works. The efficacy is well over 90%.”
Funding details were not released at the press briefing; Dr. Giroir said that figures will be released by the Office of Management and Budget as part of the 2020 budget cycle. He confirmed, however, that new funds will be allocated for the effort, rather than a mere reshuffling of existing fund and resources.
Several of the leaders acknowledged the problem of stigma and marginalization that many individuals living with or at risk for HIV face, since men who have sex with men, transgender people, sex workers, and those with opioid use disorder all fall into this category.
“Every American deserves to be treated with respect and dignity. We will vigorously enforce all laws on the books about discrimination,” said Rear Adm. Michael Weahkee, MD, principal deputy director of the Indian Health Service. This is especially important in Native American communities “where everybody knows everybody,” he said, and it’s vitally important to include individual and community education in the efforts.
Dr. Redfield concurred, adding that “Dr. Fauci and I have been engaged in HIV since 1981. We have witnessed firsthand the negative impact that stigma can have on our capacity to practice public health. The transgender population, in particular, needs to be reached out to. We need to be able to address in a comprehensive way how to destigmatize the HIV population.”
FROM A HEALTH AND HUMAN SERVICES BRIEFING
Surgeon: Sacral colpopexy can be smart strategy in POP repairs
LAS VEGAS – While research suggests that vaginal mesh grafts are inappropriate for many prolapse repairs, an obstetrician-gynecologist told colleagues that they’re still a valid tool in the repair procedure known as sacral colpopexy, in which mesh is attached via an abdominal route.
Beri M. Ridgeway, MD, of Cleveland Clinic, spoke about the role of mesh grafts and prolapse repairs at the Pelvic Anatomy and Gynecologic Surgery Symposium.
As Dr. Ridgeway noted, vaginal mesh grafts are controversial because of concerns about their safety. Although many women had favorable outcomes, an unacceptable proportion have experienced complications.
In 2011, the Food and Drug Administration warned that urogynecologic surgical mesh had been linked to 2,874 reports of injuries, deaths, and malfunctions, mostly in pelvic organ prolapse (POP) repairs, over 3 years. The other injuries were in stress urinary incontinence repairs. The report focuses on transvaginal mesh for prolapse and not sacral colpopexy or synthetic midurethral slings, which are considered to have a more favorable risk profile.
The FDA declared that “serious adverse events are NOT rare ... and transvaginally placed mesh in POP repair does NOT conclusively improve clinical outcomes over traditional non-mesh repair.” Subsequently, most companies stopped marketing mesh for transvaginal repair of POP.
Since 2011, research has offered new perspective on the use of mesh in specific POP situations.
“We know that mesh does have some slight improvement in medium-term outcome for subjective and objective symptoms,” Dr. Ridgeway said at the meeting, which was jointly provided by Global Academy for Medical Education and the University of Cincinnati. “This all comes at a price. There’s more blood loss, and you can actually have prolapse in other compartments and de novo SUI.”
She pointed out that these outcomes were noted in a 2013 Cochrane Review. It found improvements in subjective and objective results after treatment with polypropylene mesh vs. native tissue for anterior compartment POP repairs. But the review found multiple disadvantages for mesh vs. native tissue in operating time, blood loss, and reoperations (Cochrane Database Syst Rev. 2013 Apr 30;[4]:CD004014).
In 2016, an updated Cochrane Review declared that “current evidence does not support the use of mesh repair compared with native tissue repair for anterior compartment prolapse owing to increased morbidity.” The review also cautioned that while new light-weight transvaginal meshes are available, they haven’t been fully studied. “Clinicians and women should be cautious when utilizing these products, as their safety and efficacy have not been established,” according to the review (Cochrane Database of Syst Rev. 2016[11];CD004014).
In a follow-up interview, Dr. Ridgeway said “the data are scarce, so it is hard to have an opinion on this.”
She focused much of her presentation on sacral colpopexy. .
“Compared to native tissue prolapse repair using a vaginal approach, sacral colpopexy does have an increased risk profile but likely is associated with better durability,” she said in the interview. “The long-term outcomes following sacral colpopexy are favorable and the risk profile is acceptably low.”
She prefers the approach for recurrent prolapse and post-hysterectomy prolapse, especially in patients with a shorter vagina. She also offers this procedure for younger patients with significant prolapse and those women who are very active or perform repetitive heavy lifting.
In the interview, she offered these tips about the procedure:
- “Identify pertinent anatomy and set yourself up for success. Restore anatomy, retract the colon if necessary, use angled laparoscopes to optimize visualization, and don’t place the vagina on significant tension.”
- “In cases with unusual anatomy, one must recheck anatomic landmarks because it is critical to avoid the middle sacral artery and left common iliac vein, which is often located close to the midline.”
- “The vagina should be well supported but not on tension. One must communicate with assistants to elevate the vagina but not push it too much. I often demonstrate to the assistant how I like it to be.”
- “In regard to closing the peritoneum over the mesh, I like to make sure this dissection is sufficient at the beginning of the case so this part is not a struggle.”
Dr. Ridgeway discloses consulting for Coloplast and serving as an independent contractor (Legal) for Ethicon.
Global Academy and this news organization are owned by the same company.
LAS VEGAS – While research suggests that vaginal mesh grafts are inappropriate for many prolapse repairs, an obstetrician-gynecologist told colleagues that they’re still a valid tool in the repair procedure known as sacral colpopexy, in which mesh is attached via an abdominal route.
Beri M. Ridgeway, MD, of Cleveland Clinic, spoke about the role of mesh grafts and prolapse repairs at the Pelvic Anatomy and Gynecologic Surgery Symposium.
As Dr. Ridgeway noted, vaginal mesh grafts are controversial because of concerns about their safety. Although many women had favorable outcomes, an unacceptable proportion have experienced complications.
In 2011, the Food and Drug Administration warned that urogynecologic surgical mesh had been linked to 2,874 reports of injuries, deaths, and malfunctions, mostly in pelvic organ prolapse (POP) repairs, over 3 years. The other injuries were in stress urinary incontinence repairs. The report focuses on transvaginal mesh for prolapse and not sacral colpopexy or synthetic midurethral slings, which are considered to have a more favorable risk profile.
The FDA declared that “serious adverse events are NOT rare ... and transvaginally placed mesh in POP repair does NOT conclusively improve clinical outcomes over traditional non-mesh repair.” Subsequently, most companies stopped marketing mesh for transvaginal repair of POP.
Since 2011, research has offered new perspective on the use of mesh in specific POP situations.
“We know that mesh does have some slight improvement in medium-term outcome for subjective and objective symptoms,” Dr. Ridgeway said at the meeting, which was jointly provided by Global Academy for Medical Education and the University of Cincinnati. “This all comes at a price. There’s more blood loss, and you can actually have prolapse in other compartments and de novo SUI.”
She pointed out that these outcomes were noted in a 2013 Cochrane Review. It found improvements in subjective and objective results after treatment with polypropylene mesh vs. native tissue for anterior compartment POP repairs. But the review found multiple disadvantages for mesh vs. native tissue in operating time, blood loss, and reoperations (Cochrane Database Syst Rev. 2013 Apr 30;[4]:CD004014).
In 2016, an updated Cochrane Review declared that “current evidence does not support the use of mesh repair compared with native tissue repair for anterior compartment prolapse owing to increased morbidity.” The review also cautioned that while new light-weight transvaginal meshes are available, they haven’t been fully studied. “Clinicians and women should be cautious when utilizing these products, as their safety and efficacy have not been established,” according to the review (Cochrane Database of Syst Rev. 2016[11];CD004014).
In a follow-up interview, Dr. Ridgeway said “the data are scarce, so it is hard to have an opinion on this.”
She focused much of her presentation on sacral colpopexy. .
“Compared to native tissue prolapse repair using a vaginal approach, sacral colpopexy does have an increased risk profile but likely is associated with better durability,” she said in the interview. “The long-term outcomes following sacral colpopexy are favorable and the risk profile is acceptably low.”
She prefers the approach for recurrent prolapse and post-hysterectomy prolapse, especially in patients with a shorter vagina. She also offers this procedure for younger patients with significant prolapse and those women who are very active or perform repetitive heavy lifting.
In the interview, she offered these tips about the procedure:
- “Identify pertinent anatomy and set yourself up for success. Restore anatomy, retract the colon if necessary, use angled laparoscopes to optimize visualization, and don’t place the vagina on significant tension.”
- “In cases with unusual anatomy, one must recheck anatomic landmarks because it is critical to avoid the middle sacral artery and left common iliac vein, which is often located close to the midline.”
- “The vagina should be well supported but not on tension. One must communicate with assistants to elevate the vagina but not push it too much. I often demonstrate to the assistant how I like it to be.”
- “In regard to closing the peritoneum over the mesh, I like to make sure this dissection is sufficient at the beginning of the case so this part is not a struggle.”
Dr. Ridgeway discloses consulting for Coloplast and serving as an independent contractor (Legal) for Ethicon.
Global Academy and this news organization are owned by the same company.
LAS VEGAS – While research suggests that vaginal mesh grafts are inappropriate for many prolapse repairs, an obstetrician-gynecologist told colleagues that they’re still a valid tool in the repair procedure known as sacral colpopexy, in which mesh is attached via an abdominal route.
Beri M. Ridgeway, MD, of Cleveland Clinic, spoke about the role of mesh grafts and prolapse repairs at the Pelvic Anatomy and Gynecologic Surgery Symposium.
As Dr. Ridgeway noted, vaginal mesh grafts are controversial because of concerns about their safety. Although many women had favorable outcomes, an unacceptable proportion have experienced complications.
In 2011, the Food and Drug Administration warned that urogynecologic surgical mesh had been linked to 2,874 reports of injuries, deaths, and malfunctions, mostly in pelvic organ prolapse (POP) repairs, over 3 years. The other injuries were in stress urinary incontinence repairs. The report focuses on transvaginal mesh for prolapse and not sacral colpopexy or synthetic midurethral slings, which are considered to have a more favorable risk profile.
The FDA declared that “serious adverse events are NOT rare ... and transvaginally placed mesh in POP repair does NOT conclusively improve clinical outcomes over traditional non-mesh repair.” Subsequently, most companies stopped marketing mesh for transvaginal repair of POP.
Since 2011, research has offered new perspective on the use of mesh in specific POP situations.
“We know that mesh does have some slight improvement in medium-term outcome for subjective and objective symptoms,” Dr. Ridgeway said at the meeting, which was jointly provided by Global Academy for Medical Education and the University of Cincinnati. “This all comes at a price. There’s more blood loss, and you can actually have prolapse in other compartments and de novo SUI.”
She pointed out that these outcomes were noted in a 2013 Cochrane Review. It found improvements in subjective and objective results after treatment with polypropylene mesh vs. native tissue for anterior compartment POP repairs. But the review found multiple disadvantages for mesh vs. native tissue in operating time, blood loss, and reoperations (Cochrane Database Syst Rev. 2013 Apr 30;[4]:CD004014).
In 2016, an updated Cochrane Review declared that “current evidence does not support the use of mesh repair compared with native tissue repair for anterior compartment prolapse owing to increased morbidity.” The review also cautioned that while new light-weight transvaginal meshes are available, they haven’t been fully studied. “Clinicians and women should be cautious when utilizing these products, as their safety and efficacy have not been established,” according to the review (Cochrane Database of Syst Rev. 2016[11];CD004014).
In a follow-up interview, Dr. Ridgeway said “the data are scarce, so it is hard to have an opinion on this.”
She focused much of her presentation on sacral colpopexy. .
“Compared to native tissue prolapse repair using a vaginal approach, sacral colpopexy does have an increased risk profile but likely is associated with better durability,” she said in the interview. “The long-term outcomes following sacral colpopexy are favorable and the risk profile is acceptably low.”
She prefers the approach for recurrent prolapse and post-hysterectomy prolapse, especially in patients with a shorter vagina. She also offers this procedure for younger patients with significant prolapse and those women who are very active or perform repetitive heavy lifting.
In the interview, she offered these tips about the procedure:
- “Identify pertinent anatomy and set yourself up for success. Restore anatomy, retract the colon if necessary, use angled laparoscopes to optimize visualization, and don’t place the vagina on significant tension.”
- “In cases with unusual anatomy, one must recheck anatomic landmarks because it is critical to avoid the middle sacral artery and left common iliac vein, which is often located close to the midline.”
- “The vagina should be well supported but not on tension. One must communicate with assistants to elevate the vagina but not push it too much. I often demonstrate to the assistant how I like it to be.”
- “In regard to closing the peritoneum over the mesh, I like to make sure this dissection is sufficient at the beginning of the case so this part is not a struggle.”
Dr. Ridgeway discloses consulting for Coloplast and serving as an independent contractor (Legal) for Ethicon.
Global Academy and this news organization are owned by the same company.
EXPERT ANALYSIS FROM PAGS
Despite concerns, synthetic slings are still ‘standard of care’ in SUI
LAS VEGAS – A few weeks before she was scheduled to speak at the annual Pelvic Anatomy and Gynecologic Surgery Symposium, Beri M. Ridgeway, MD, received an anonymous note about her upcoming presentation. “Someone wanted me to think very carefully about what I’d be talking about during my presentation on synthetics,” she recalled.

The note reflects the deep controversy over the use of transvaginal synthetic mesh products, which have been linked to a long list of serious adverse effects. “There are women who have been harmed, and I take care of a lot of those,” said Dr. Ridgeway, who’s based at Cleveland Clinic. One key distinction is that there is a very different risk profile between transvaginal synthetic mesh prolapse kits and polypropylene midurethral slings. While it’s important to be thoughtful about the use of mesh in synthetic midurethral (MU) slings, she said, they remain well supported as an effective treatment for stress urinary incontinence (SUI).
Even so, she said, the news about the risks of mesh “weighs on our patients’ minds” and spawns fear among physicians. Meanwhile, she said, “there is quite a bit of flux” in the marketplace as companies withdraw products because of their perception of risk.
Even amid the controversy, she said, it’s important to remember how crucial it is to treat women in need. “SUI is a very common problem, and women suffer significantly. With our aging population, the prevalence will increase even more,” she said. “It is critical that we screen patients for SUI and have the ability to offer treatment. Having different treatment options benefit women significantly.”
Dr. Ridgeway offered these pearls about the use of synthetic MU slings and alternative approaches to treating SUI.
It’s helpful to find a single strategy and embrace it.
“For ob.gyn. specialists who treat primary, uncomplicated SUI, I recommend surgeons become comfortable with an approach and focus on becoming high-volume surgeons in that approach,” Dr. Ridgeway said. “It is also good to partner with a female pelvic medicine & reconstructive surgery specialist who can back one up for more complicated cases, complications, or recurrent SUI. These specialists should be able to offer a full array of procedures to treat SUI and tailor the treatment to the individual patient, especially in more complex cases.”
Synthetic MU slings are the “definitive standard of care.”
More than 17 years of research suggest the efficacy of the slings is durable, she said, especially when the goal is to resolve symptoms in patients with pure SUI symptoms. she said, pointing to more than 500 articles and more than 40 randomized controlled trials.
According to her, synthetic slings have similar efficacy to traditional slings but require less time in the operating room and produce less voiding dysfunction and de novo urgency. “The revision rate of synthetic MU slings is very low,” she added. “In large studies, the revision rate at 10 years is 3%-4%.”
It’s important to keep patient consent in mind, she said. “Patients should know and understand the specific risks of any procedure, including MU slings, so that they can share in decision making.”
Transobdurator (TOT) slings offer benefits.
There’s less risk of bladder and vascular injury from the TOT procedure, which is easy to learn and teach, Dr. Ridgeway said. Research suggests the tension-free vaginal tape (TVT) approach is more likely to cause voiding dysfunction, she added.
But TOT is probably less effective in patients with SUI linked to intrinsic sphincter deficiency and in longer-term follow-up, she said. And there are cases of male sex partners injuring their penises during contact with TOT slings during intercourse.
Single-incision slings are up-and-coming options.
These slings offer promising results in short-term studies, but long-term results aren’t available yet. They may be a good option for cases of mild and occult SUI, she said.
Alternative treatments for SUI have limitations.
These include urethral bulking agents, which mainly lead to improvement rather than cure. Autologous fascial pubovaginal slings are another option, especially if patients don’t want a mesh-based treatment or have recurrent SUI following a synthetic mesh complication. However, she noted that research points to morbidity and de novo urinary urgency, she said.
The Pelvic Anatomy & Gynecologic Surgery Symposium was jointly provided by Global Academy for Medical Education and the University of Cincinnati. Global Academy and this news organization are owned by the same company.
Dr. Ridgeway disclosed consulting for Coloplast and having served as an independent contractor (legal) for Ethicon.
LAS VEGAS – A few weeks before she was scheduled to speak at the annual Pelvic Anatomy and Gynecologic Surgery Symposium, Beri M. Ridgeway, MD, received an anonymous note about her upcoming presentation. “Someone wanted me to think very carefully about what I’d be talking about during my presentation on synthetics,” she recalled.
The note reflects the deep controversy over the use of transvaginal synthetic mesh products, which have been linked to a long list of serious adverse effects. “There are women who have been harmed, and I take care of a lot of those,” said Dr. Ridgeway, who’s based at Cleveland Clinic. One key distinction is that there is a very different risk profile between transvaginal synthetic mesh prolapse kits and polypropylene midurethral slings. While it’s important to be thoughtful about the use of mesh in synthetic midurethral (MU) slings, she said, they remain well supported as an effective treatment for stress urinary incontinence (SUI).
Even so, she said, the news about the risks of mesh “weighs on our patients’ minds” and spawns fear among physicians. Meanwhile, she said, “there is quite a bit of flux” in the marketplace as companies withdraw products because of their perception of risk.
Even amid the controversy, she said, it’s important to remember how crucial it is to treat women in need. “SUI is a very common problem, and women suffer significantly. With our aging population, the prevalence will increase even more,” she said. “It is critical that we screen patients for SUI and have the ability to offer treatment. Having different treatment options benefit women significantly.”
Dr. Ridgeway offered these pearls about the use of synthetic MU slings and alternative approaches to treating SUI.
It’s helpful to find a single strategy and embrace it.
“For ob.gyn. specialists who treat primary, uncomplicated SUI, I recommend surgeons become comfortable with an approach and focus on becoming high-volume surgeons in that approach,” Dr. Ridgeway said. “It is also good to partner with a female pelvic medicine & reconstructive surgery specialist who can back one up for more complicated cases, complications, or recurrent SUI. These specialists should be able to offer a full array of procedures to treat SUI and tailor the treatment to the individual patient, especially in more complex cases.”
Synthetic MU slings are the “definitive standard of care.”
More than 17 years of research suggest the efficacy of the slings is durable, she said, especially when the goal is to resolve symptoms in patients with pure SUI symptoms. she said, pointing to more than 500 articles and more than 40 randomized controlled trials.
According to her, synthetic slings have similar efficacy to traditional slings but require less time in the operating room and produce less voiding dysfunction and de novo urgency. “The revision rate of synthetic MU slings is very low,” she added. “In large studies, the revision rate at 10 years is 3%-4%.”
It’s important to keep patient consent in mind, she said. “Patients should know and understand the specific risks of any procedure, including MU slings, so that they can share in decision making.”
Transobdurator (TOT) slings offer benefits.
There’s less risk of bladder and vascular injury from the TOT procedure, which is easy to learn and teach, Dr. Ridgeway said. Research suggests the tension-free vaginal tape (TVT) approach is more likely to cause voiding dysfunction, she added.
But TOT is probably less effective in patients with SUI linked to intrinsic sphincter deficiency and in longer-term follow-up, she said. And there are cases of male sex partners injuring their penises during contact with TOT slings during intercourse.
Single-incision slings are up-and-coming options.
These slings offer promising results in short-term studies, but long-term results aren’t available yet. They may be a good option for cases of mild and occult SUI, she said.
Alternative treatments for SUI have limitations.
These include urethral bulking agents, which mainly lead to improvement rather than cure. Autologous fascial pubovaginal slings are another option, especially if patients don’t want a mesh-based treatment or have recurrent SUI following a synthetic mesh complication. However, she noted that research points to morbidity and de novo urinary urgency, she said.
The Pelvic Anatomy & Gynecologic Surgery Symposium was jointly provided by Global Academy for Medical Education and the University of Cincinnati. Global Academy and this news organization are owned by the same company.
Dr. Ridgeway disclosed consulting for Coloplast and having served as an independent contractor (legal) for Ethicon.
LAS VEGAS – A few weeks before she was scheduled to speak at the annual Pelvic Anatomy and Gynecologic Surgery Symposium, Beri M. Ridgeway, MD, received an anonymous note about her upcoming presentation. “Someone wanted me to think very carefully about what I’d be talking about during my presentation on synthetics,” she recalled.
The note reflects the deep controversy over the use of transvaginal synthetic mesh products, which have been linked to a long list of serious adverse effects. “There are women who have been harmed, and I take care of a lot of those,” said Dr. Ridgeway, who’s based at Cleveland Clinic. One key distinction is that there is a very different risk profile between transvaginal synthetic mesh prolapse kits and polypropylene midurethral slings. While it’s important to be thoughtful about the use of mesh in synthetic midurethral (MU) slings, she said, they remain well supported as an effective treatment for stress urinary incontinence (SUI).
Even so, she said, the news about the risks of mesh “weighs on our patients’ minds” and spawns fear among physicians. Meanwhile, she said, “there is quite a bit of flux” in the marketplace as companies withdraw products because of their perception of risk.
Even amid the controversy, she said, it’s important to remember how crucial it is to treat women in need. “SUI is a very common problem, and women suffer significantly. With our aging population, the prevalence will increase even more,” she said. “It is critical that we screen patients for SUI and have the ability to offer treatment. Having different treatment options benefit women significantly.”
Dr. Ridgeway offered these pearls about the use of synthetic MU slings and alternative approaches to treating SUI.
It’s helpful to find a single strategy and embrace it.
“For ob.gyn. specialists who treat primary, uncomplicated SUI, I recommend surgeons become comfortable with an approach and focus on becoming high-volume surgeons in that approach,” Dr. Ridgeway said. “It is also good to partner with a female pelvic medicine & reconstructive surgery specialist who can back one up for more complicated cases, complications, or recurrent SUI. These specialists should be able to offer a full array of procedures to treat SUI and tailor the treatment to the individual patient, especially in more complex cases.”
Synthetic MU slings are the “definitive standard of care.”
More than 17 years of research suggest the efficacy of the slings is durable, she said, especially when the goal is to resolve symptoms in patients with pure SUI symptoms. she said, pointing to more than 500 articles and more than 40 randomized controlled trials.
According to her, synthetic slings have similar efficacy to traditional slings but require less time in the operating room and produce less voiding dysfunction and de novo urgency. “The revision rate of synthetic MU slings is very low,” she added. “In large studies, the revision rate at 10 years is 3%-4%.”
It’s important to keep patient consent in mind, she said. “Patients should know and understand the specific risks of any procedure, including MU slings, so that they can share in decision making.”
Transobdurator (TOT) slings offer benefits.
There’s less risk of bladder and vascular injury from the TOT procedure, which is easy to learn and teach, Dr. Ridgeway said. Research suggests the tension-free vaginal tape (TVT) approach is more likely to cause voiding dysfunction, she added.
But TOT is probably less effective in patients with SUI linked to intrinsic sphincter deficiency and in longer-term follow-up, she said. And there are cases of male sex partners injuring their penises during contact with TOT slings during intercourse.
Single-incision slings are up-and-coming options.
These slings offer promising results in short-term studies, but long-term results aren’t available yet. They may be a good option for cases of mild and occult SUI, she said.
Alternative treatments for SUI have limitations.
These include urethral bulking agents, which mainly lead to improvement rather than cure. Autologous fascial pubovaginal slings are another option, especially if patients don’t want a mesh-based treatment or have recurrent SUI following a synthetic mesh complication. However, she noted that research points to morbidity and de novo urinary urgency, she said.
The Pelvic Anatomy & Gynecologic Surgery Symposium was jointly provided by Global Academy for Medical Education and the University of Cincinnati. Global Academy and this news organization are owned by the same company.
Dr. Ridgeway disclosed consulting for Coloplast and having served as an independent contractor (legal) for Ethicon.
EXPERT ANALYSIS FROM PAGS