User login
AFib patients do best on a DOAC started 7-10 days post stroke
LOS ANGELES – When a patient with atrial fibrillation (AFib) has a cardioembolic stroke, the best blood thinner to start may be a direct-acting oral anticoagulant (DOAC), possibly beginning 7-10 days after the index stroke, according to an analysis of 90-day, observational outcomes data from nearly 1,300 patients.

The analysis also suggested that the use of “bridging” anticoagulant treatment by injection before a patient with atrial fibrillation (AFib) starts a daily oral anticoagulant regimen following a cardioembolic stroke is not a good idea. Patients who received bridging anticoagulation had a nearly threefold higher rate of symptomatic intracranial hemorrhage than did patients who did not, and their bridging treatment failed to protect them from recurrent ischemic events, Shadi Yaghi, MD, said at the International Stroke Conference, sponsored by the American Heart Association. The bridging regimens delivered either heparin or low-molecular-weight heparin.
Based on the findings, “it seems reasonable to avoid bridging unless absolutely necessary, to initiate a DOAC unless it’s contraindicated, and to start the DOAC on day 7-10 following the stroke in most patients,” said Dr. Yaghi, a vascular neurologist and director of stroke research at NYU Langone Health in New York.
“It’s been hard to develop a broad guideline on when to start oral anticoagulation” after a cardioembolic stroke in AFib patients. The best time “depends on a lot of variables and how the patient responded to acute treatment,” commented Alexis Simpkins, MD, a vascular and stroke neurologist at the University of Florida in Gainesville. “You want to start treatment before the patient has another stroke, but not so soon that the treatment causes symptomatic hemorrhagic transformation.”
Dr. Yaghi’s suggestion, based on his findings, to start treatment for most patients with a DOAC 7-10 days after their index stroke “shows consistency” with the prevailing guideline recommendation from the AHA/American Stroke Association to start oral anticoagulation in this patient population 4-14 days after the index stroke (Stroke. 2018 March;49[3]:e46-e99), she noted.
A recent article reviewed the uncertainty about the best time to start oral anticoagulation in AFib patients after a cardioembolic stroke and the subtle differences that distinguish various international medical groups that, like the ASA, have made recommendations (Lancet Neurol. 2019 Jan 1;18[1]:117-26). According to this review, a major limitation of these various recommendations has been the lack of actual evidence collected from AFib patients who began receiving a DOAC shortly after a cardioembolic stroke, although the article added that several studies in progress are collecting these data.
The study reported by Dr. Yaghi pooled data collected from 2,084 recent AFib patients with a cardioembolic stroke treated at any of eight comprehensive U.S. stroke centers. They excluded patients who died from causes unrelated to the primary endpoint, those who did not receive an anticoagulant or had incomplete data, and patients lost to follow-up, leaving 1,289 evaluable patients. During their 90-day follow-up, 10% of the patients had an ischemic event, a symptomatic intracranial hemorrhage, or an extracranial hemorrhage.
The study’s primary analysis showed no statistically significant difference in the incidence of recurrent ischemic events, symptomatic intracranial hemorrhage, or both based on when oral anticoagulant treatment began: 0-3 days, 4-14 days, or more than 14 days after the index stroke.
The investigators then subdivided patients into the subgroup that started treatment with a DOAC and the subgroup that started treatment with warfarin and also further subdivided the 4-14 day time window for starting treatment. Results of this analysis showed that patients who received a DOAC and began this treatment 7-10 days after their stroke had a 50% cut in their 90-day events compared with other patients, a difference that fell just short of statistical significance at P = .07. All the other combinations of oral anticoagulant and time of treatment initiation analyzed showed neutral effects that never came near statistical significance.
Secondary data analyses also showed that both patients with a history of a stroke prior to their index stroke and patients with ipsilateral atherosclerosis came close to having a statistically significant increased rate of a subsequent ischemic event during 90-day follow-up. Furthermore, women, patients with a history of hyperlipidemia, and patients who developed hemorrhagic transformation of their index stroke all had significantly increased rates of developing a symptomatic intracranial hemorrhage during 90-day follow-up. When the endpoint was limited to recurrent ischemic events only, patients who received a DOAC were 50% less likely to have an event than were patients treated with warfarin, a statistically significant difference.
Although starting a DOAC 7-10 days after the index stroke seems reasonable based on this analysis, the question needs a prospective, randomized study to create an appropriate evidence base, Dr. Yaghi said.
Dr. Yaghi disclosed a financial relationship with Medtronic. Dr. Simpkins had no disclosures.
SOURCE: Yaghi S et al. Stroke. 2020 Feb;51(suppl 1):A119.
LOS ANGELES – When a patient with atrial fibrillation (AFib) has a cardioembolic stroke, the best blood thinner to start may be a direct-acting oral anticoagulant (DOAC), possibly beginning 7-10 days after the index stroke, according to an analysis of 90-day, observational outcomes data from nearly 1,300 patients.
The analysis also suggested that the use of “bridging” anticoagulant treatment by injection before a patient with atrial fibrillation (AFib) starts a daily oral anticoagulant regimen following a cardioembolic stroke is not a good idea. Patients who received bridging anticoagulation had a nearly threefold higher rate of symptomatic intracranial hemorrhage than did patients who did not, and their bridging treatment failed to protect them from recurrent ischemic events, Shadi Yaghi, MD, said at the International Stroke Conference, sponsored by the American Heart Association. The bridging regimens delivered either heparin or low-molecular-weight heparin.
Based on the findings, “it seems reasonable to avoid bridging unless absolutely necessary, to initiate a DOAC unless it’s contraindicated, and to start the DOAC on day 7-10 following the stroke in most patients,” said Dr. Yaghi, a vascular neurologist and director of stroke research at NYU Langone Health in New York.
“It’s been hard to develop a broad guideline on when to start oral anticoagulation” after a cardioembolic stroke in AFib patients. The best time “depends on a lot of variables and how the patient responded to acute treatment,” commented Alexis Simpkins, MD, a vascular and stroke neurologist at the University of Florida in Gainesville. “You want to start treatment before the patient has another stroke, but not so soon that the treatment causes symptomatic hemorrhagic transformation.”
Dr. Yaghi’s suggestion, based on his findings, to start treatment for most patients with a DOAC 7-10 days after their index stroke “shows consistency” with the prevailing guideline recommendation from the AHA/American Stroke Association to start oral anticoagulation in this patient population 4-14 days after the index stroke (Stroke. 2018 March;49[3]:e46-e99), she noted.
A recent article reviewed the uncertainty about the best time to start oral anticoagulation in AFib patients after a cardioembolic stroke and the subtle differences that distinguish various international medical groups that, like the ASA, have made recommendations (Lancet Neurol. 2019 Jan 1;18[1]:117-26). According to this review, a major limitation of these various recommendations has been the lack of actual evidence collected from AFib patients who began receiving a DOAC shortly after a cardioembolic stroke, although the article added that several studies in progress are collecting these data.
The study reported by Dr. Yaghi pooled data collected from 2,084 recent AFib patients with a cardioembolic stroke treated at any of eight comprehensive U.S. stroke centers. They excluded patients who died from causes unrelated to the primary endpoint, those who did not receive an anticoagulant or had incomplete data, and patients lost to follow-up, leaving 1,289 evaluable patients. During their 90-day follow-up, 10% of the patients had an ischemic event, a symptomatic intracranial hemorrhage, or an extracranial hemorrhage.
The study’s primary analysis showed no statistically significant difference in the incidence of recurrent ischemic events, symptomatic intracranial hemorrhage, or both based on when oral anticoagulant treatment began: 0-3 days, 4-14 days, or more than 14 days after the index stroke.
The investigators then subdivided patients into the subgroup that started treatment with a DOAC and the subgroup that started treatment with warfarin and also further subdivided the 4-14 day time window for starting treatment. Results of this analysis showed that patients who received a DOAC and began this treatment 7-10 days after their stroke had a 50% cut in their 90-day events compared with other patients, a difference that fell just short of statistical significance at P = .07. All the other combinations of oral anticoagulant and time of treatment initiation analyzed showed neutral effects that never came near statistical significance.
Secondary data analyses also showed that both patients with a history of a stroke prior to their index stroke and patients with ipsilateral atherosclerosis came close to having a statistically significant increased rate of a subsequent ischemic event during 90-day follow-up. Furthermore, women, patients with a history of hyperlipidemia, and patients who developed hemorrhagic transformation of their index stroke all had significantly increased rates of developing a symptomatic intracranial hemorrhage during 90-day follow-up. When the endpoint was limited to recurrent ischemic events only, patients who received a DOAC were 50% less likely to have an event than were patients treated with warfarin, a statistically significant difference.
Although starting a DOAC 7-10 days after the index stroke seems reasonable based on this analysis, the question needs a prospective, randomized study to create an appropriate evidence base, Dr. Yaghi said.
Dr. Yaghi disclosed a financial relationship with Medtronic. Dr. Simpkins had no disclosures.
SOURCE: Yaghi S et al. Stroke. 2020 Feb;51(suppl 1):A119.
LOS ANGELES – When a patient with atrial fibrillation (AFib) has a cardioembolic stroke, the best blood thinner to start may be a direct-acting oral anticoagulant (DOAC), possibly beginning 7-10 days after the index stroke, according to an analysis of 90-day, observational outcomes data from nearly 1,300 patients.
The analysis also suggested that the use of “bridging” anticoagulant treatment by injection before a patient with atrial fibrillation (AFib) starts a daily oral anticoagulant regimen following a cardioembolic stroke is not a good idea. Patients who received bridging anticoagulation had a nearly threefold higher rate of symptomatic intracranial hemorrhage than did patients who did not, and their bridging treatment failed to protect them from recurrent ischemic events, Shadi Yaghi, MD, said at the International Stroke Conference, sponsored by the American Heart Association. The bridging regimens delivered either heparin or low-molecular-weight heparin.
Based on the findings, “it seems reasonable to avoid bridging unless absolutely necessary, to initiate a DOAC unless it’s contraindicated, and to start the DOAC on day 7-10 following the stroke in most patients,” said Dr. Yaghi, a vascular neurologist and director of stroke research at NYU Langone Health in New York.
“It’s been hard to develop a broad guideline on when to start oral anticoagulation” after a cardioembolic stroke in AFib patients. The best time “depends on a lot of variables and how the patient responded to acute treatment,” commented Alexis Simpkins, MD, a vascular and stroke neurologist at the University of Florida in Gainesville. “You want to start treatment before the patient has another stroke, but not so soon that the treatment causes symptomatic hemorrhagic transformation.”
Dr. Yaghi’s suggestion, based on his findings, to start treatment for most patients with a DOAC 7-10 days after their index stroke “shows consistency” with the prevailing guideline recommendation from the AHA/American Stroke Association to start oral anticoagulation in this patient population 4-14 days after the index stroke (Stroke. 2018 March;49[3]:e46-e99), she noted.
A recent article reviewed the uncertainty about the best time to start oral anticoagulation in AFib patients after a cardioembolic stroke and the subtle differences that distinguish various international medical groups that, like the ASA, have made recommendations (Lancet Neurol. 2019 Jan 1;18[1]:117-26). According to this review, a major limitation of these various recommendations has been the lack of actual evidence collected from AFib patients who began receiving a DOAC shortly after a cardioembolic stroke, although the article added that several studies in progress are collecting these data.
The study reported by Dr. Yaghi pooled data collected from 2,084 recent AFib patients with a cardioembolic stroke treated at any of eight comprehensive U.S. stroke centers. They excluded patients who died from causes unrelated to the primary endpoint, those who did not receive an anticoagulant or had incomplete data, and patients lost to follow-up, leaving 1,289 evaluable patients. During their 90-day follow-up, 10% of the patients had an ischemic event, a symptomatic intracranial hemorrhage, or an extracranial hemorrhage.
The study’s primary analysis showed no statistically significant difference in the incidence of recurrent ischemic events, symptomatic intracranial hemorrhage, or both based on when oral anticoagulant treatment began: 0-3 days, 4-14 days, or more than 14 days after the index stroke.
The investigators then subdivided patients into the subgroup that started treatment with a DOAC and the subgroup that started treatment with warfarin and also further subdivided the 4-14 day time window for starting treatment. Results of this analysis showed that patients who received a DOAC and began this treatment 7-10 days after their stroke had a 50% cut in their 90-day events compared with other patients, a difference that fell just short of statistical significance at P = .07. All the other combinations of oral anticoagulant and time of treatment initiation analyzed showed neutral effects that never came near statistical significance.
Secondary data analyses also showed that both patients with a history of a stroke prior to their index stroke and patients with ipsilateral atherosclerosis came close to having a statistically significant increased rate of a subsequent ischemic event during 90-day follow-up. Furthermore, women, patients with a history of hyperlipidemia, and patients who developed hemorrhagic transformation of their index stroke all had significantly increased rates of developing a symptomatic intracranial hemorrhage during 90-day follow-up. When the endpoint was limited to recurrent ischemic events only, patients who received a DOAC were 50% less likely to have an event than were patients treated with warfarin, a statistically significant difference.
Although starting a DOAC 7-10 days after the index stroke seems reasonable based on this analysis, the question needs a prospective, randomized study to create an appropriate evidence base, Dr. Yaghi said.
Dr. Yaghi disclosed a financial relationship with Medtronic. Dr. Simpkins had no disclosures.
SOURCE: Yaghi S et al. Stroke. 2020 Feb;51(suppl 1):A119.
REPORTING FROM ISC 2020
CLTX-CAR T cells exhibit preclinical activity and move on to a clinical trial
Chlorotoxin (CLTX)-directed chimeric antigen receptor (CAR) T cells demonstrated activity against glioblastoma in a preclinical study and will soon be tested in a clinical trial.
“We sought to develop a CAR T cell using chlorotoxin peptide as the tumor-targeting domain,” wrote Dongrui Wang, a PhD candidate at City of Hope National Medical Center in Duarte, Calif., and colleagues. Their report is in Science Translational Medicine.
“CLTX has been established to bind broadly and specifically to glioblastoma and other neuroectodermal tumors while showing minimal cross-reactivity with nonmalignant cells,” the researchers noted.
The team evaluated CLTX binding capacity in 23 tumor samples from 15 glioblastoma patients, in patient-derived glioblastoma cell lines, and in orthotopic mouse xenograft models. These experiments showed that CLTX could bind to a high percentage of patient tumors as well as to most glioblastoma cells within a tumor.
In the design phase, the researchers engineered a peptide-bearing CAR, which overcame previous barriers of other glioblastoma-directed CARs, including antigen escape and tumor heterogeneity.
The team evaluated the antitumor activity of CLTX-CAR T cells in two orthotopic mouse xenograft models. Intracranial administration of CLTX-CAR T cells controlled tumor growth and extended survival in both models. All mice originally bearing PBT106-TS tumors became tumor-free and remained so for more than 170 days. However, only a subset of mice bearing PBT003-4-TS tumors experienced similar long-term tumor-free survival.
The researchers assessed potential off-target effects of CLTX-CAR T cells in normal human cells. The team observed limited binding of CLTX-CAR T cells to embryonic kidney cells, peripheral blood mononuclear cells, and neural progenitor cells, suggesting minimal off-target activity.
Further toxicity experiments demonstrated that, even at high doses, CLTX-CAR T cells were tolerated in mouse models, suggesting high potency for tumor cells and low risk of systemic toxicity.
Additional preclinical experiments elucidated mechanisms of CLTX-CAR T-cell function, namely the essential role of matrix metalloproteinase 2 expression for cell activation.
The researchers acknowledged that a key limitation of this study was the use of glioblastoma xenograft models, which may not fully represent tumor activity in glioblastoma patients.
Nevertheless, the researchers concluded that “CLTX-CAR T cells present a strategic combination of selective yet ubiquitous tumor targeting and are a candidate for clinical development as anti-glioblastoma immunotherapy.”
In fact, City of Hope is now screening patients for a clinical trial of CLTX-CAR T cells for the treatment of recurrent or progressive glioblastoma (NCT04214392).
The preclinical research was funded by the Ben and Catherine Ivy Foundation and the National Institutes of Health. Two authors disclosed financial affiliations with Mustang Bio.
SOURCE: Wang D et al. Sci Transl Med. 2020 Mar 4. doi: 10.1126/scitranslmed.aaw2672.
Chlorotoxin (CLTX)-directed chimeric antigen receptor (CAR) T cells demonstrated activity against glioblastoma in a preclinical study and will soon be tested in a clinical trial.
“We sought to develop a CAR T cell using chlorotoxin peptide as the tumor-targeting domain,” wrote Dongrui Wang, a PhD candidate at City of Hope National Medical Center in Duarte, Calif., and colleagues. Their report is in Science Translational Medicine.
“CLTX has been established to bind broadly and specifically to glioblastoma and other neuroectodermal tumors while showing minimal cross-reactivity with nonmalignant cells,” the researchers noted.
The team evaluated CLTX binding capacity in 23 tumor samples from 15 glioblastoma patients, in patient-derived glioblastoma cell lines, and in orthotopic mouse xenograft models. These experiments showed that CLTX could bind to a high percentage of patient tumors as well as to most glioblastoma cells within a tumor.
In the design phase, the researchers engineered a peptide-bearing CAR, which overcame previous barriers of other glioblastoma-directed CARs, including antigen escape and tumor heterogeneity.
The team evaluated the antitumor activity of CLTX-CAR T cells in two orthotopic mouse xenograft models. Intracranial administration of CLTX-CAR T cells controlled tumor growth and extended survival in both models. All mice originally bearing PBT106-TS tumors became tumor-free and remained so for more than 170 days. However, only a subset of mice bearing PBT003-4-TS tumors experienced similar long-term tumor-free survival.
The researchers assessed potential off-target effects of CLTX-CAR T cells in normal human cells. The team observed limited binding of CLTX-CAR T cells to embryonic kidney cells, peripheral blood mononuclear cells, and neural progenitor cells, suggesting minimal off-target activity.
Further toxicity experiments demonstrated that, even at high doses, CLTX-CAR T cells were tolerated in mouse models, suggesting high potency for tumor cells and low risk of systemic toxicity.
Additional preclinical experiments elucidated mechanisms of CLTX-CAR T-cell function, namely the essential role of matrix metalloproteinase 2 expression for cell activation.
The researchers acknowledged that a key limitation of this study was the use of glioblastoma xenograft models, which may not fully represent tumor activity in glioblastoma patients.
Nevertheless, the researchers concluded that “CLTX-CAR T cells present a strategic combination of selective yet ubiquitous tumor targeting and are a candidate for clinical development as anti-glioblastoma immunotherapy.”
In fact, City of Hope is now screening patients for a clinical trial of CLTX-CAR T cells for the treatment of recurrent or progressive glioblastoma (NCT04214392).
The preclinical research was funded by the Ben and Catherine Ivy Foundation and the National Institutes of Health. Two authors disclosed financial affiliations with Mustang Bio.
SOURCE: Wang D et al. Sci Transl Med. 2020 Mar 4. doi: 10.1126/scitranslmed.aaw2672.
Chlorotoxin (CLTX)-directed chimeric antigen receptor (CAR) T cells demonstrated activity against glioblastoma in a preclinical study and will soon be tested in a clinical trial.
“We sought to develop a CAR T cell using chlorotoxin peptide as the tumor-targeting domain,” wrote Dongrui Wang, a PhD candidate at City of Hope National Medical Center in Duarte, Calif., and colleagues. Their report is in Science Translational Medicine.
“CLTX has been established to bind broadly and specifically to glioblastoma and other neuroectodermal tumors while showing minimal cross-reactivity with nonmalignant cells,” the researchers noted.
The team evaluated CLTX binding capacity in 23 tumor samples from 15 glioblastoma patients, in patient-derived glioblastoma cell lines, and in orthotopic mouse xenograft models. These experiments showed that CLTX could bind to a high percentage of patient tumors as well as to most glioblastoma cells within a tumor.
In the design phase, the researchers engineered a peptide-bearing CAR, which overcame previous barriers of other glioblastoma-directed CARs, including antigen escape and tumor heterogeneity.
The team evaluated the antitumor activity of CLTX-CAR T cells in two orthotopic mouse xenograft models. Intracranial administration of CLTX-CAR T cells controlled tumor growth and extended survival in both models. All mice originally bearing PBT106-TS tumors became tumor-free and remained so for more than 170 days. However, only a subset of mice bearing PBT003-4-TS tumors experienced similar long-term tumor-free survival.
The researchers assessed potential off-target effects of CLTX-CAR T cells in normal human cells. The team observed limited binding of CLTX-CAR T cells to embryonic kidney cells, peripheral blood mononuclear cells, and neural progenitor cells, suggesting minimal off-target activity.
Further toxicity experiments demonstrated that, even at high doses, CLTX-CAR T cells were tolerated in mouse models, suggesting high potency for tumor cells and low risk of systemic toxicity.
Additional preclinical experiments elucidated mechanisms of CLTX-CAR T-cell function, namely the essential role of matrix metalloproteinase 2 expression for cell activation.
The researchers acknowledged that a key limitation of this study was the use of glioblastoma xenograft models, which may not fully represent tumor activity in glioblastoma patients.
Nevertheless, the researchers concluded that “CLTX-CAR T cells present a strategic combination of selective yet ubiquitous tumor targeting and are a candidate for clinical development as anti-glioblastoma immunotherapy.”
In fact, City of Hope is now screening patients for a clinical trial of CLTX-CAR T cells for the treatment of recurrent or progressive glioblastoma (NCT04214392).
The preclinical research was funded by the Ben and Catherine Ivy Foundation and the National Institutes of Health. Two authors disclosed financial affiliations with Mustang Bio.
SOURCE: Wang D et al. Sci Transl Med. 2020 Mar 4. doi: 10.1126/scitranslmed.aaw2672.
FROM SCIENCE TRANSLATIONAL MEDICINE
COVID-19’s hairy conspiracy, and a Kardashian Kolonoscopy
Coronavirus conspiracy gets hairy
It was inevitable, of course. The government’s response to COVID-19 and the novel coronavirus has become an issue, and the increased scrutiny has now turned up a conspiracy.
This particular plot, recently uncovered by the Twitterverse and reported by Newsweek, is being perpetuated by the CDC against the American patriots who make up the bearded wings of the Men-ocratic and Republi-man parties.
Our story begins on Nov. 2, 2017, when the National Institute for Occupational Safety and Health posted “To Beard or not to Beard? That’s a good Question!” on its science blog, which was aimed at “workers who wear tight-fitting respirators.” Like the N95 face mask. More than 2 years before the coronavirus was “discovered” in China. Hmmm, interesting.
The NIOSH post claimed that beards, sideburns, and some mustaches “will interfere with respirators that rely on a tight facepiece seal to achieve maximum protection.” The agency further alleged that “research tells us that the presence of facial hair under the sealing surface causes 20 to 1,000 times more leakage, compared to clean-shaven individuals.” As if research ever proved anything.
The post’s pièce de résistance, however, was an infograph illustrating 36 types of facial hairstyles and whether they worked with a face mask/respirator. Did you know that beard styles such as the chin curtain, French fork, Garibaldi, and Hulihee get a thumbs down? Did you know there are beard styles called the chin curtain, French fork, Garibaldi, and Hulihee? [What? No ZZ Top beard?]
Most mustaches are okay, though, and therein lies the proof of a conspiracy. Among the approved mustache styles is the toothbrush. You’ll find it on the bottom row of the graph, third from the left. Notice anything?
It’s a Hitler mustache! The CDC put its seal of approval on a Hitler mustache!
Thus, by the transfollicular property of the High Castle corollary to the Boys from Brazil theorem, a government conspiracy must exist.
The coronavirus will now proceed to take over the world. Have a nice day.
Keeping up with the Kolonoscopies

Imagine owing your life to the Kardashians. It’s a bit tough to swallow, but a man from Ohio owes Kim and her Krew a life debt.
Gary Paine was just passing the time, watching some daytime “Keeping Up With the Kardashians” television in the doctor’s waiting room while his wife was getting a colonoscopy. We’ve all been there – we in the Bureau of LOTME have watched more waiting-room “Judge Judy” than we care to admit.
And just like us, Gary said he was getting bored while watching the Kardashians’ TV travails. Although he felt relatively healthy, he decided to distract himself the best way he knew how: making his own colonoscopy appointment. Anything’s better than getting sucked into an 8-hour Kardashian marathon, right?
During Gary’s Kim K–inspired colonoscopy, it was discovered that he had an irregularity in his heart. Eventually, doctors found two severely blocked arteries. Paine underwent immediate, lifesaving quadruple-bypass surgery.
He now urges people to be aware that checkups are essential, whether you’re showing symptoms of poor health or not.
Which leads us to wonder: Do Kris Jenner and her clan know they’re now officially more painful than a colonoscopy appointment?
(Crosswalks) Don’t stop me now

There’s always that one guy. You’re stuck in a long line behind a big slow tractor trailer going 10 under the speed limit, and there’s a flashy BMW practically living inside your trunk. A brief passing zone approaches, but there’s no point ... oh, of course they swerve around and cut you off, what did they even gain from doing that?
Point is, people who drive expensive cars have a bit of a reputation for being less than courteous behind the wheel, and thanks to a study published in the Journal of Transport & Health, there’s some science to back that up.
A group of four presumably well-paid volunteers were sent out to crosswalks and crossed in front of cars to see how many would yield. Results were less than encouraging: Only 28% of 461 cars yielded. The only factor that significantly predicted whether or not a car would yield was how expensive it was; for every $1,000 increase in the value of the car, the driver was 3% less likely to stop.
It’s not looking good for owners of expensive cars, especially when even the study authors suggest that these drivers were displaying increased entitlement and narcissism through their lack of yielding behavior.
Our suggestion? Clearly rich people are sick and need intensive psychotherapy, and the offending vehicles should be removed and redistributed to the rest of us. We wouldn’t mind a nice slightly used Corvette, in red preferably. Nope, no ulterior motive here.
Coronavirus conspiracy gets hairy
It was inevitable, of course. The government’s response to COVID-19 and the novel coronavirus has become an issue, and the increased scrutiny has now turned up a conspiracy.
This particular plot, recently uncovered by the Twitterverse and reported by Newsweek, is being perpetuated by the CDC against the American patriots who make up the bearded wings of the Men-ocratic and Republi-man parties.
Our story begins on Nov. 2, 2017, when the National Institute for Occupational Safety and Health posted “To Beard or not to Beard? That’s a good Question!” on its science blog, which was aimed at “workers who wear tight-fitting respirators.” Like the N95 face mask. More than 2 years before the coronavirus was “discovered” in China. Hmmm, interesting.
The NIOSH post claimed that beards, sideburns, and some mustaches “will interfere with respirators that rely on a tight facepiece seal to achieve maximum protection.” The agency further alleged that “research tells us that the presence of facial hair under the sealing surface causes 20 to 1,000 times more leakage, compared to clean-shaven individuals.” As if research ever proved anything.
The post’s pièce de résistance, however, was an infograph illustrating 36 types of facial hairstyles and whether they worked with a face mask/respirator. Did you know that beard styles such as the chin curtain, French fork, Garibaldi, and Hulihee get a thumbs down? Did you know there are beard styles called the chin curtain, French fork, Garibaldi, and Hulihee? [What? No ZZ Top beard?]
Most mustaches are okay, though, and therein lies the proof of a conspiracy. Among the approved mustache styles is the toothbrush. You’ll find it on the bottom row of the graph, third from the left. Notice anything?
It’s a Hitler mustache! The CDC put its seal of approval on a Hitler mustache!
Thus, by the transfollicular property of the High Castle corollary to the Boys from Brazil theorem, a government conspiracy must exist.
The coronavirus will now proceed to take over the world. Have a nice day.
Keeping up with the Kolonoscopies
Imagine owing your life to the Kardashians. It’s a bit tough to swallow, but a man from Ohio owes Kim and her Krew a life debt.
Gary Paine was just passing the time, watching some daytime “Keeping Up With the Kardashians” television in the doctor’s waiting room while his wife was getting a colonoscopy. We’ve all been there – we in the Bureau of LOTME have watched more waiting-room “Judge Judy” than we care to admit.
And just like us, Gary said he was getting bored while watching the Kardashians’ TV travails. Although he felt relatively healthy, he decided to distract himself the best way he knew how: making his own colonoscopy appointment. Anything’s better than getting sucked into an 8-hour Kardashian marathon, right?
During Gary’s Kim K–inspired colonoscopy, it was discovered that he had an irregularity in his heart. Eventually, doctors found two severely blocked arteries. Paine underwent immediate, lifesaving quadruple-bypass surgery.
He now urges people to be aware that checkups are essential, whether you’re showing symptoms of poor health or not.
Which leads us to wonder: Do Kris Jenner and her clan know they’re now officially more painful than a colonoscopy appointment?
(Crosswalks) Don’t stop me now
There’s always that one guy. You’re stuck in a long line behind a big slow tractor trailer going 10 under the speed limit, and there’s a flashy BMW practically living inside your trunk. A brief passing zone approaches, but there’s no point ... oh, of course they swerve around and cut you off, what did they even gain from doing that?
Point is, people who drive expensive cars have a bit of a reputation for being less than courteous behind the wheel, and thanks to a study published in the Journal of Transport & Health, there’s some science to back that up.
A group of four presumably well-paid volunteers were sent out to crosswalks and crossed in front of cars to see how many would yield. Results were less than encouraging: Only 28% of 461 cars yielded. The only factor that significantly predicted whether or not a car would yield was how expensive it was; for every $1,000 increase in the value of the car, the driver was 3% less likely to stop.
It’s not looking good for owners of expensive cars, especially when even the study authors suggest that these drivers were displaying increased entitlement and narcissism through their lack of yielding behavior.
Our suggestion? Clearly rich people are sick and need intensive psychotherapy, and the offending vehicles should be removed and redistributed to the rest of us. We wouldn’t mind a nice slightly used Corvette, in red preferably. Nope, no ulterior motive here.
Coronavirus conspiracy gets hairy
It was inevitable, of course. The government’s response to COVID-19 and the novel coronavirus has become an issue, and the increased scrutiny has now turned up a conspiracy.
This particular plot, recently uncovered by the Twitterverse and reported by Newsweek, is being perpetuated by the CDC against the American patriots who make up the bearded wings of the Men-ocratic and Republi-man parties.
Our story begins on Nov. 2, 2017, when the National Institute for Occupational Safety and Health posted “To Beard or not to Beard? That’s a good Question!” on its science blog, which was aimed at “workers who wear tight-fitting respirators.” Like the N95 face mask. More than 2 years before the coronavirus was “discovered” in China. Hmmm, interesting.
The NIOSH post claimed that beards, sideburns, and some mustaches “will interfere with respirators that rely on a tight facepiece seal to achieve maximum protection.” The agency further alleged that “research tells us that the presence of facial hair under the sealing surface causes 20 to 1,000 times more leakage, compared to clean-shaven individuals.” As if research ever proved anything.
The post’s pièce de résistance, however, was an infograph illustrating 36 types of facial hairstyles and whether they worked with a face mask/respirator. Did you know that beard styles such as the chin curtain, French fork, Garibaldi, and Hulihee get a thumbs down? Did you know there are beard styles called the chin curtain, French fork, Garibaldi, and Hulihee? [What? No ZZ Top beard?]
Most mustaches are okay, though, and therein lies the proof of a conspiracy. Among the approved mustache styles is the toothbrush. You’ll find it on the bottom row of the graph, third from the left. Notice anything?
It’s a Hitler mustache! The CDC put its seal of approval on a Hitler mustache!
Thus, by the transfollicular property of the High Castle corollary to the Boys from Brazil theorem, a government conspiracy must exist.
The coronavirus will now proceed to take over the world. Have a nice day.
Keeping up with the Kolonoscopies
Imagine owing your life to the Kardashians. It’s a bit tough to swallow, but a man from Ohio owes Kim and her Krew a life debt.
Gary Paine was just passing the time, watching some daytime “Keeping Up With the Kardashians” television in the doctor’s waiting room while his wife was getting a colonoscopy. We’ve all been there – we in the Bureau of LOTME have watched more waiting-room “Judge Judy” than we care to admit.
And just like us, Gary said he was getting bored while watching the Kardashians’ TV travails. Although he felt relatively healthy, he decided to distract himself the best way he knew how: making his own colonoscopy appointment. Anything’s better than getting sucked into an 8-hour Kardashian marathon, right?
During Gary’s Kim K–inspired colonoscopy, it was discovered that he had an irregularity in his heart. Eventually, doctors found two severely blocked arteries. Paine underwent immediate, lifesaving quadruple-bypass surgery.
He now urges people to be aware that checkups are essential, whether you’re showing symptoms of poor health or not.
Which leads us to wonder: Do Kris Jenner and her clan know they’re now officially more painful than a colonoscopy appointment?
(Crosswalks) Don’t stop me now
There’s always that one guy. You’re stuck in a long line behind a big slow tractor trailer going 10 under the speed limit, and there’s a flashy BMW practically living inside your trunk. A brief passing zone approaches, but there’s no point ... oh, of course they swerve around and cut you off, what did they even gain from doing that?
Point is, people who drive expensive cars have a bit of a reputation for being less than courteous behind the wheel, and thanks to a study published in the Journal of Transport & Health, there’s some science to back that up.
A group of four presumably well-paid volunteers were sent out to crosswalks and crossed in front of cars to see how many would yield. Results were less than encouraging: Only 28% of 461 cars yielded. The only factor that significantly predicted whether or not a car would yield was how expensive it was; for every $1,000 increase in the value of the car, the driver was 3% less likely to stop.
It’s not looking good for owners of expensive cars, especially when even the study authors suggest that these drivers were displaying increased entitlement and narcissism through their lack of yielding behavior.
Our suggestion? Clearly rich people are sick and need intensive psychotherapy, and the offending vehicles should be removed and redistributed to the rest of us. We wouldn’t mind a nice slightly used Corvette, in red preferably. Nope, no ulterior motive here.
Are computers and AI prompting us to think less?
The collection of vast amounts of data and the use of more sophisticated algorithms seem beneficial in all fields. However, I have deep concerns about the “other side of the coin” when it comes to artificial intelligence (AI) as discussed in “An FP’s guide to AI-enabled clinical decision support” (J Fam Pract. 2019;68:486-492).
Years ago, when I worked in urgent care, one of my colleagues would log in to her favorite Web site to search for the appropriate diagnosis for almost all of her patients. Surely this physician was able to memorize and regurgitate enough information to get through medical school and pass the boards, but was she able to think, in the sense of using/applying the information she stored away? My answer is, “No!”
Certainly, having a computer helps one to get through medical school. However, while we use terms such as “AI,” I would argue that none of these machines do more than duplicate the algorithmic functioning of the brain. Which leads me to the other side of the coin: Are computers, of which we ask questions and expect legitimate answers in return, helping us to think? Or are they leading us to think less?
In other words, are we inadvertently “dumbing down” as physicians (and as a species)? And do we want a physician who seems less capable of actually processing the sum total of a patient’s complaints, symptoms, and findings in trying to understand the patient’s problem?
While we cannot go back and disconnect from computers, we can make sure that we do not become totally dependent on them. We need to acknowledge this possible blind spot in the evolution of technology (particularly AI)—the potential to reinforce “not thinking”—especially within the medical school environment. There needs to be an awareness of, and a conscious effort to counter, an overreliance on computers thinking for us.
As individual physicians, we owe it to our patients and ourselves, each and every working day, to use our brains to apply our education, training, and accumulated data to help diagnose and treat our patients effectively.
Barry Marged, DO, ABD, MA
Mansfield, OH
The collection of vast amounts of data and the use of more sophisticated algorithms seem beneficial in all fields. However, I have deep concerns about the “other side of the coin” when it comes to artificial intelligence (AI) as discussed in “An FP’s guide to AI-enabled clinical decision support” (J Fam Pract. 2019;68:486-492).
Years ago, when I worked in urgent care, one of my colleagues would log in to her favorite Web site to search for the appropriate diagnosis for almost all of her patients. Surely this physician was able to memorize and regurgitate enough information to get through medical school and pass the boards, but was she able to think, in the sense of using/applying the information she stored away? My answer is, “No!”
Certainly, having a computer helps one to get through medical school. However, while we use terms such as “AI,” I would argue that none of these machines do more than duplicate the algorithmic functioning of the brain. Which leads me to the other side of the coin: Are computers, of which we ask questions and expect legitimate answers in return, helping us to think? Or are they leading us to think less?
In other words, are we inadvertently “dumbing down” as physicians (and as a species)? And do we want a physician who seems less capable of actually processing the sum total of a patient’s complaints, symptoms, and findings in trying to understand the patient’s problem?
While we cannot go back and disconnect from computers, we can make sure that we do not become totally dependent on them. We need to acknowledge this possible blind spot in the evolution of technology (particularly AI)—the potential to reinforce “not thinking”—especially within the medical school environment. There needs to be an awareness of, and a conscious effort to counter, an overreliance on computers thinking for us.
As individual physicians, we owe it to our patients and ourselves, each and every working day, to use our brains to apply our education, training, and accumulated data to help diagnose and treat our patients effectively.
Barry Marged, DO, ABD, MA
Mansfield, OH
The collection of vast amounts of data and the use of more sophisticated algorithms seem beneficial in all fields. However, I have deep concerns about the “other side of the coin” when it comes to artificial intelligence (AI) as discussed in “An FP’s guide to AI-enabled clinical decision support” (J Fam Pract. 2019;68:486-492).
Years ago, when I worked in urgent care, one of my colleagues would log in to her favorite Web site to search for the appropriate diagnosis for almost all of her patients. Surely this physician was able to memorize and regurgitate enough information to get through medical school and pass the boards, but was she able to think, in the sense of using/applying the information she stored away? My answer is, “No!”
Certainly, having a computer helps one to get through medical school. However, while we use terms such as “AI,” I would argue that none of these machines do more than duplicate the algorithmic functioning of the brain. Which leads me to the other side of the coin: Are computers, of which we ask questions and expect legitimate answers in return, helping us to think? Or are they leading us to think less?
In other words, are we inadvertently “dumbing down” as physicians (and as a species)? And do we want a physician who seems less capable of actually processing the sum total of a patient’s complaints, symptoms, and findings in trying to understand the patient’s problem?
While we cannot go back and disconnect from computers, we can make sure that we do not become totally dependent on them. We need to acknowledge this possible blind spot in the evolution of technology (particularly AI)—the potential to reinforce “not thinking”—especially within the medical school environment. There needs to be an awareness of, and a conscious effort to counter, an overreliance on computers thinking for us.
As individual physicians, we owe it to our patients and ourselves, each and every working day, to use our brains to apply our education, training, and accumulated data to help diagnose and treat our patients effectively.
Barry Marged, DO, ABD, MA
Mansfield, OH
A rarely discussed aspect of the opioid crisis
Your article, “A patient-centered approach to tapering opioids” (J Fam Pract. 2019;68:548-556) by Davis et al is the most thoughtful article I have seen on opioids. The patient-centered ap-proach takes this article to a place that is rarely discussed in the opioid crisis.
If we could really understand and treat chronic psychic and physical pain better, we might begin to have a real impact on this crisis. I completely agree that evidence-based intensive trauma treatment is generally unavailable in the United States. I have been working with women in a residential chemical dependency treatment program for the past 15 years and more than 90% of them were sexually abused. Trauma can lead to all forms of addiction, and trauma induced hyperalgesia is not the same as nociceptive pain.
We have so many unaddressed mental health issues in our country and your article emphasized the importance of understanding people and their mental health issues rather than taking a formulaic approach and replacing one opioid with another. It is clear to me that we will not win this battle with medication-assisted treatment alone.
Richard Usatine, MD
San Antonio, TX
Associate Editor, The Journal of Family Practice
Your article, “A patient-centered approach to tapering opioids” (J Fam Pract. 2019;68:548-556) by Davis et al is the most thoughtful article I have seen on opioids. The patient-centered ap-proach takes this article to a place that is rarely discussed in the opioid crisis.
If we could really understand and treat chronic psychic and physical pain better, we might begin to have a real impact on this crisis. I completely agree that evidence-based intensive trauma treatment is generally unavailable in the United States. I have been working with women in a residential chemical dependency treatment program for the past 15 years and more than 90% of them were sexually abused. Trauma can lead to all forms of addiction, and trauma induced hyperalgesia is not the same as nociceptive pain.
We have so many unaddressed mental health issues in our country and your article emphasized the importance of understanding people and their mental health issues rather than taking a formulaic approach and replacing one opioid with another. It is clear to me that we will not win this battle with medication-assisted treatment alone.
Richard Usatine, MD
San Antonio, TX
Associate Editor, The Journal of Family Practice
Your article, “A patient-centered approach to tapering opioids” (J Fam Pract. 2019;68:548-556) by Davis et al is the most thoughtful article I have seen on opioids. The patient-centered ap-proach takes this article to a place that is rarely discussed in the opioid crisis.
If we could really understand and treat chronic psychic and physical pain better, we might begin to have a real impact on this crisis. I completely agree that evidence-based intensive trauma treatment is generally unavailable in the United States. I have been working with women in a residential chemical dependency treatment program for the past 15 years and more than 90% of them were sexually abused. Trauma can lead to all forms of addiction, and trauma induced hyperalgesia is not the same as nociceptive pain.
We have so many unaddressed mental health issues in our country and your article emphasized the importance of understanding people and their mental health issues rather than taking a formulaic approach and replacing one opioid with another. It is clear to me that we will not win this battle with medication-assisted treatment alone.
Richard Usatine, MD
San Antonio, TX
Associate Editor, The Journal of Family Practice
MACE benefits with dapagliflozin improve with disease duration
Treatment with the sodium-glucose transporter 2 inhibitor dapagliflozin reduced the risk for cardiovascular disease or hospitalization for heart failure (CVD/HHF) in patients with diabetes, regardless of the duration of the disease, but had a greater protective benefit against major adverse cardiovascular events (MACE) and renal events in patients with longer disease duration, according to new findings from a post hoc analysis of the DECLARE-TIMI 58 trial.
The positive effect of dapagliflozin in patients with MACE – which includes myocardial infarction (MI), CVD, and ischemic stroke – may have been driven by lower rates of MI and ischemic stroke with the drug, compared with placebo, in patients with longer disease duration, wrote Harpreet S. Bajaj, MD, and colleagues. Their report is in Diabetes, Obesity and Metabolism (2020 Feb 23. doi: 10.1111/dom.14011).
It has been previously reported that the risk for complications in diabetes increases with increasing duration of the disease. Recent studies with SGLT-2 inhibitors have shown that the drugs improve cardiovascular and renal outcomes in diabetes, and they are recommended by the American Diabetes Association as second-line therapy in patients with atherosclerotic cardiovascular disease, chronic kidney disease, or heart failure. The European Society of Cardiology and the European Association for the Study of Diabetes recommend that patients with diabetes patients who have three or more risk factors, or those with a disease duration of more than 20 years, should be deemed very high risk and be considered for early treatment with SGLT2 inhibitors.
“The MACE benefit observed with dapagliflozin in this study in patients with diabetes duration of [more than] 20 years, clearly supports that notion,” the authors wrote.
In DECLARE-TIMI 58, 17,160 patients with type 2 diabetes received dapagliflozin or placebo and were followed for a median of 4.2 years. Of those patients, 22.4% had a disease duration of fewer than 5 years; 27.6%, a duration of 5-10 years; 23.0%, 10-15 years; 14.2%, 10-15 years; and 12.9%, more than 20 years. The median duration of disease was 11 years.
Patients in all the age groups had similar reductions in CVD/HHF, compared with placebo, with hazard ratios of 0.79 (disease duration of 5 or fewer years), 0.86, 0.92, 0.81, and 0.75 (duration of 20 years), respectively (interaction trend P = .760).
Treatment with dapagliflozin reduced the incidence of MACE, but the benefit was more apparent in patients with longer-term disease: HR, 1.08; 1.02; 0.94; 0.92; and 0.67, respectively (interaction trend P = .004). Similar trends were seen with MI (interaction trend P = .019) and ischemic stroke (interaction trend P = .015).
The researchers also reported improved benefits in renal-specific outcome with increasing disease duration, with HRs ranging from 0.79 in patients with diabetes duration of fewer than 5 years, to 0.42 in those with a duration of more than 20 years (interaction trend P = .084).
Limitations of the study include the fact that the information about diabetes duration relied on patient reports, and that the original trial was not powered for all subgroup interactions. This authors emphasized that this was a post hoc analysis and as such, should be considered hypothesis generating.
All but two of the authors reported relationships with Astra Zeneca, which funded the study, and other drug companies.
SOURCE: Bajaj HS et al. Diabetes Obes Metab. 2020 Feb 23. doi: 10.1111/dom.14011.
Treatment with the sodium-glucose transporter 2 inhibitor dapagliflozin reduced the risk for cardiovascular disease or hospitalization for heart failure (CVD/HHF) in patients with diabetes, regardless of the duration of the disease, but had a greater protective benefit against major adverse cardiovascular events (MACE) and renal events in patients with longer disease duration, according to new findings from a post hoc analysis of the DECLARE-TIMI 58 trial.
The positive effect of dapagliflozin in patients with MACE – which includes myocardial infarction (MI), CVD, and ischemic stroke – may have been driven by lower rates of MI and ischemic stroke with the drug, compared with placebo, in patients with longer disease duration, wrote Harpreet S. Bajaj, MD, and colleagues. Their report is in Diabetes, Obesity and Metabolism (2020 Feb 23. doi: 10.1111/dom.14011).
It has been previously reported that the risk for complications in diabetes increases with increasing duration of the disease. Recent studies with SGLT-2 inhibitors have shown that the drugs improve cardiovascular and renal outcomes in diabetes, and they are recommended by the American Diabetes Association as second-line therapy in patients with atherosclerotic cardiovascular disease, chronic kidney disease, or heart failure. The European Society of Cardiology and the European Association for the Study of Diabetes recommend that patients with diabetes patients who have three or more risk factors, or those with a disease duration of more than 20 years, should be deemed very high risk and be considered for early treatment with SGLT2 inhibitors.
“The MACE benefit observed with dapagliflozin in this study in patients with diabetes duration of [more than] 20 years, clearly supports that notion,” the authors wrote.
In DECLARE-TIMI 58, 17,160 patients with type 2 diabetes received dapagliflozin or placebo and were followed for a median of 4.2 years. Of those patients, 22.4% had a disease duration of fewer than 5 years; 27.6%, a duration of 5-10 years; 23.0%, 10-15 years; 14.2%, 10-15 years; and 12.9%, more than 20 years. The median duration of disease was 11 years.
Patients in all the age groups had similar reductions in CVD/HHF, compared with placebo, with hazard ratios of 0.79 (disease duration of 5 or fewer years), 0.86, 0.92, 0.81, and 0.75 (duration of 20 years), respectively (interaction trend P = .760).
Treatment with dapagliflozin reduced the incidence of MACE, but the benefit was more apparent in patients with longer-term disease: HR, 1.08; 1.02; 0.94; 0.92; and 0.67, respectively (interaction trend P = .004). Similar trends were seen with MI (interaction trend P = .019) and ischemic stroke (interaction trend P = .015).
The researchers also reported improved benefits in renal-specific outcome with increasing disease duration, with HRs ranging from 0.79 in patients with diabetes duration of fewer than 5 years, to 0.42 in those with a duration of more than 20 years (interaction trend P = .084).
Limitations of the study include the fact that the information about diabetes duration relied on patient reports, and that the original trial was not powered for all subgroup interactions. This authors emphasized that this was a post hoc analysis and as such, should be considered hypothesis generating.
All but two of the authors reported relationships with Astra Zeneca, which funded the study, and other drug companies.
SOURCE: Bajaj HS et al. Diabetes Obes Metab. 2020 Feb 23. doi: 10.1111/dom.14011.
Treatment with the sodium-glucose transporter 2 inhibitor dapagliflozin reduced the risk for cardiovascular disease or hospitalization for heart failure (CVD/HHF) in patients with diabetes, regardless of the duration of the disease, but had a greater protective benefit against major adverse cardiovascular events (MACE) and renal events in patients with longer disease duration, according to new findings from a post hoc analysis of the DECLARE-TIMI 58 trial.
The positive effect of dapagliflozin in patients with MACE – which includes myocardial infarction (MI), CVD, and ischemic stroke – may have been driven by lower rates of MI and ischemic stroke with the drug, compared with placebo, in patients with longer disease duration, wrote Harpreet S. Bajaj, MD, and colleagues. Their report is in Diabetes, Obesity and Metabolism (2020 Feb 23. doi: 10.1111/dom.14011).
It has been previously reported that the risk for complications in diabetes increases with increasing duration of the disease. Recent studies with SGLT-2 inhibitors have shown that the drugs improve cardiovascular and renal outcomes in diabetes, and they are recommended by the American Diabetes Association as second-line therapy in patients with atherosclerotic cardiovascular disease, chronic kidney disease, or heart failure. The European Society of Cardiology and the European Association for the Study of Diabetes recommend that patients with diabetes patients who have three or more risk factors, or those with a disease duration of more than 20 years, should be deemed very high risk and be considered for early treatment with SGLT2 inhibitors.
“The MACE benefit observed with dapagliflozin in this study in patients with diabetes duration of [more than] 20 years, clearly supports that notion,” the authors wrote.
In DECLARE-TIMI 58, 17,160 patients with type 2 diabetes received dapagliflozin or placebo and were followed for a median of 4.2 years. Of those patients, 22.4% had a disease duration of fewer than 5 years; 27.6%, a duration of 5-10 years; 23.0%, 10-15 years; 14.2%, 10-15 years; and 12.9%, more than 20 years. The median duration of disease was 11 years.
Patients in all the age groups had similar reductions in CVD/HHF, compared with placebo, with hazard ratios of 0.79 (disease duration of 5 or fewer years), 0.86, 0.92, 0.81, and 0.75 (duration of 20 years), respectively (interaction trend P = .760).
Treatment with dapagliflozin reduced the incidence of MACE, but the benefit was more apparent in patients with longer-term disease: HR, 1.08; 1.02; 0.94; 0.92; and 0.67, respectively (interaction trend P = .004). Similar trends were seen with MI (interaction trend P = .019) and ischemic stroke (interaction trend P = .015).
The researchers also reported improved benefits in renal-specific outcome with increasing disease duration, with HRs ranging from 0.79 in patients with diabetes duration of fewer than 5 years, to 0.42 in those with a duration of more than 20 years (interaction trend P = .084).
Limitations of the study include the fact that the information about diabetes duration relied on patient reports, and that the original trial was not powered for all subgroup interactions. This authors emphasized that this was a post hoc analysis and as such, should be considered hypothesis generating.
All but two of the authors reported relationships with Astra Zeneca, which funded the study, and other drug companies.
SOURCE: Bajaj HS et al. Diabetes Obes Metab. 2020 Feb 23. doi: 10.1111/dom.14011.
FROM DIABETES, OBESITY AND METABOLISM
Preoperative chemoradiotherapy failed to boost overall survival in pancreatic cancer
, according to findings from a phase 3 trial.
On the other hand, preoperative chemoradiotherapy improved disease-free survival, locoregional failure-free interval, and other secondary endpoints, according to study author Eva Versteijne, MD, of the University of Amsterdam, and colleagues. Their findings were published in the Journal of Clinical Oncology.
The randomized, phase 3 study included 246 patients with borderline or resectable pancreatic ductal adenocarcinoma without distant metastases. Patients were randomized to receive preoperative chemoradiotherapy (n = 119) or immediate surgery (n = 127).
Patients in the preoperative chemoradiotherapy arm received three courses of gemcitabine at 1,000 mg/m2, combined with 15 fractions of radiotherapy at 2.4 Gy during the second course. Explorative laparotomy with subsequent resection followed, in addition to four 4-week cycles of adjuvant gemcitabine at 1,000 mg/m2. Following resection in the immediate surgery arm, patients received six 4-week cycles of adjuvant gemcitabine at the same dose.
The primary outcome was median overall survival in the intention-to-treat population. The median overall survival was 16.0 months in the preoperative chemoradiotherapy arm and 14.3 months in the immediate surgery arm (hazard ratio, 0.78; P = .096).
Secondary outcomes included disease-free survival, resection rate, R0 resection rate, and locoregional failure-free interval, among others.
The resection rate was 61% in the preoperative chemoradiotherapy arm and 72% in the immediate surgery arm (odds ratio, 0.58; P = .058). The R0 resection rates were 71% and 40%, respectively (OR, 3.61; P less than .001).
The median disease-free survival was 8.1 months in the preoperative chemoradiotherapy arm and 7.7 months in the immediate surgery arm (HR, 0.73; P = .032). The median locoregional failure-free interval was not reached and 13.4 months, respectively (HR, 0.56; P = .0034). The rate of serious adverse events was 52% and 41%, respectively (OR, 1.57; P = .096).
“Preoperative chemoradiotherapy was associated with significantly better [disease-free survival] and [locoregional failure-free interval] as well as with significantly lower rates of pathologic lymph nodes, perineural invasion, and venous invasion,” the researchers noted.
They acknowledged that some findings, particularly the median overall survival in patients assigned to immediate surgery, require further investigation, as these data suggest the trial may have been underpowered.
“The consistent benefits for most secondary endpoints and the better compliance with preoperative chemoradiotherapy compared with postoperative adjuvant chemotherapy suggest superiority of the neoadjuvant approach,” the researchers concluded.
The study was funded by the Dutch Cancer Society. The authors disclosed financial affiliations with Bristol-Myers Squibb, Eisai, Ipsen, Merck Serono, and several other companies.
SOURCE: Versteijne E et al. J Clin Oncol. 2020 Feb 27. doi: 10.1200/JCO.19.02274.
, according to findings from a phase 3 trial.
On the other hand, preoperative chemoradiotherapy improved disease-free survival, locoregional failure-free interval, and other secondary endpoints, according to study author Eva Versteijne, MD, of the University of Amsterdam, and colleagues. Their findings were published in the Journal of Clinical Oncology.
The randomized, phase 3 study included 246 patients with borderline or resectable pancreatic ductal adenocarcinoma without distant metastases. Patients were randomized to receive preoperative chemoradiotherapy (n = 119) or immediate surgery (n = 127).
Patients in the preoperative chemoradiotherapy arm received three courses of gemcitabine at 1,000 mg/m2, combined with 15 fractions of radiotherapy at 2.4 Gy during the second course. Explorative laparotomy with subsequent resection followed, in addition to four 4-week cycles of adjuvant gemcitabine at 1,000 mg/m2. Following resection in the immediate surgery arm, patients received six 4-week cycles of adjuvant gemcitabine at the same dose.
The primary outcome was median overall survival in the intention-to-treat population. The median overall survival was 16.0 months in the preoperative chemoradiotherapy arm and 14.3 months in the immediate surgery arm (hazard ratio, 0.78; P = .096).
Secondary outcomes included disease-free survival, resection rate, R0 resection rate, and locoregional failure-free interval, among others.
The resection rate was 61% in the preoperative chemoradiotherapy arm and 72% in the immediate surgery arm (odds ratio, 0.58; P = .058). The R0 resection rates were 71% and 40%, respectively (OR, 3.61; P less than .001).
The median disease-free survival was 8.1 months in the preoperative chemoradiotherapy arm and 7.7 months in the immediate surgery arm (HR, 0.73; P = .032). The median locoregional failure-free interval was not reached and 13.4 months, respectively (HR, 0.56; P = .0034). The rate of serious adverse events was 52% and 41%, respectively (OR, 1.57; P = .096).
“Preoperative chemoradiotherapy was associated with significantly better [disease-free survival] and [locoregional failure-free interval] as well as with significantly lower rates of pathologic lymph nodes, perineural invasion, and venous invasion,” the researchers noted.
They acknowledged that some findings, particularly the median overall survival in patients assigned to immediate surgery, require further investigation, as these data suggest the trial may have been underpowered.
“The consistent benefits for most secondary endpoints and the better compliance with preoperative chemoradiotherapy compared with postoperative adjuvant chemotherapy suggest superiority of the neoadjuvant approach,” the researchers concluded.
The study was funded by the Dutch Cancer Society. The authors disclosed financial affiliations with Bristol-Myers Squibb, Eisai, Ipsen, Merck Serono, and several other companies.
SOURCE: Versteijne E et al. J Clin Oncol. 2020 Feb 27. doi: 10.1200/JCO.19.02274.
, according to findings from a phase 3 trial.
On the other hand, preoperative chemoradiotherapy improved disease-free survival, locoregional failure-free interval, and other secondary endpoints, according to study author Eva Versteijne, MD, of the University of Amsterdam, and colleagues. Their findings were published in the Journal of Clinical Oncology.
The randomized, phase 3 study included 246 patients with borderline or resectable pancreatic ductal adenocarcinoma without distant metastases. Patients were randomized to receive preoperative chemoradiotherapy (n = 119) or immediate surgery (n = 127).
Patients in the preoperative chemoradiotherapy arm received three courses of gemcitabine at 1,000 mg/m2, combined with 15 fractions of radiotherapy at 2.4 Gy during the second course. Explorative laparotomy with subsequent resection followed, in addition to four 4-week cycles of adjuvant gemcitabine at 1,000 mg/m2. Following resection in the immediate surgery arm, patients received six 4-week cycles of adjuvant gemcitabine at the same dose.
The primary outcome was median overall survival in the intention-to-treat population. The median overall survival was 16.0 months in the preoperative chemoradiotherapy arm and 14.3 months in the immediate surgery arm (hazard ratio, 0.78; P = .096).
Secondary outcomes included disease-free survival, resection rate, R0 resection rate, and locoregional failure-free interval, among others.
The resection rate was 61% in the preoperative chemoradiotherapy arm and 72% in the immediate surgery arm (odds ratio, 0.58; P = .058). The R0 resection rates were 71% and 40%, respectively (OR, 3.61; P less than .001).
The median disease-free survival was 8.1 months in the preoperative chemoradiotherapy arm and 7.7 months in the immediate surgery arm (HR, 0.73; P = .032). The median locoregional failure-free interval was not reached and 13.4 months, respectively (HR, 0.56; P = .0034). The rate of serious adverse events was 52% and 41%, respectively (OR, 1.57; P = .096).
“Preoperative chemoradiotherapy was associated with significantly better [disease-free survival] and [locoregional failure-free interval] as well as with significantly lower rates of pathologic lymph nodes, perineural invasion, and venous invasion,” the researchers noted.
They acknowledged that some findings, particularly the median overall survival in patients assigned to immediate surgery, require further investigation, as these data suggest the trial may have been underpowered.
“The consistent benefits for most secondary endpoints and the better compliance with preoperative chemoradiotherapy compared with postoperative adjuvant chemotherapy suggest superiority of the neoadjuvant approach,” the researchers concluded.
The study was funded by the Dutch Cancer Society. The authors disclosed financial affiliations with Bristol-Myers Squibb, Eisai, Ipsen, Merck Serono, and several other companies.
SOURCE: Versteijne E et al. J Clin Oncol. 2020 Feb 27. doi: 10.1200/JCO.19.02274.
FROM JOURNAL OF CLINICAL ONCOLOGY
In a public health crisis, obstetric collaboration is mission-critical
With the novel coronavirus (COVID-19) monopolizing the news cycle, fear and misinformation are at an all-time high. Public health officials and physicians are accelerating education outreach to the public to address misinformation, and identify and care for patients who may have been exposed to the virus.

In times of public health crises, pregnant women have unique and pressing concerns about their personal health and the health of their unborn children. While not often mentioned in major news coverage, obstetricians play a critical role during health crises because of their uniquely personal role with patients during all stages of pregnancy, providing this vulnerable population with the most up-to-date information and following the latest guidelines for recommended care.
Unfortunately, COVID-19 is breaking unfamiliar new ground. We know that pregnant women are at higher risk for viral infection – annually, influenza is a grim reminder that pregnant women are more immunocompromised than the general public – but we do not yet have data to confirm or refute that pregnant women have a higher susceptibility to COVID-19 than the rest of the adult population. We also do not know enough about COVID-19 transmission, including whether the virus can cross the transplacental barrier to affect a fetus, or whether it can be transmitted through breast milk.
As private practice community obstetricians work to protect their patients during this public health crisis, Ob hospitalists can play an important role in supporting them in the provision of patient care.
First, Ob hospitalists are highly-trained specialists who can help ensure that pregnant patients who seek care at the hospital – either with viral symptoms or with separate pregnancy-related concerns – are protected during triage until the treating community obstetrician can take the reins.
When a pregnant woman presents at a hospital, in most cases she will bypass the ED and instead be sent directly to the labor and delivery (L&D) unit. During a viral outbreak, there are two major concerns with this approach. For one thing, it means an immunocompromised woman is being sent through the hospital to get to L&D, and along the path, is exposed to every airborne pathogen in the facility (and, if she is already infected, exposes others along the way). In addition, in hospitals without an Ob hospitalist on site, the patient generally is not immediately triaged by a physician, physician’s assistant, or nurse practitioner upon arrival because those clinicians are not consistently on site in L&D.
In times of viral pandemics, new approaches are warranted. For hospitals with contracted L&D management with hospitalists, hospitalists work closely with department heads to implement protocols loosely based on the Emergency Severity Index (ESI) model established by the Agency for Healthcare Research and Quality. Just as the ESI algorithm guides clinical stratification of patients, in times of reported viral outbreaks, L&D should consider triage of all pregnant women at higher levels of acuity, regardless of presentation status. In particular, if they show clinical symptoms, they should be masked, accompanied to the L&D unit by protected personnel, separated from other patients in areas of forced proximity such as hallways and elevators, and triaged in a secure single-patient room with a closed door (ideally at negative pressure relative to the surrounding areas).
If the patient has traveled to an area of outbreak, reports exposure to travelers who have visited high-risk areas, has had contact with individuals who tested positive for COVID-19, or exhibits any clinical symptoms of COVID-19 (fever, dry cough, fatigue, etc.), her care management should adhere to standing hospital emergency protocols. Following consultation with the assigned community obstetrician, the Ob hospitalist and hospital staff should contact their local/state health departments immediately for all cases of patients who show symptoms to determine if the patient meets requirements for a person under investigation (PUI) for COVID-19. The state/local health department will work with clinicians to collect, store, and ship clinical specimens appropriately. Very ill patients may need to be treated in an intensive care setting where respiratory status can be closely monitored.
At Ob Hospitalist Group, our body of evidence from our large national footprint has informed the development of standard sets of protocols for delivery complications such as preeclampsia and postpartum hemorrhage, as well as a cesarean section reduction toolkit to combat medically unnecessary cesarean sections. OB hospitalists therefore can assist with refining COVID-19 protocols specifically for the L&D setting, using evidence-based data to tailor protocols to address public health emergencies as they evolve.
The second way that Ob hospitalists can support their colleagues is by covering L&D 24/7 so that community obstetricians can focus on other pressing medical needs. From our experience with other outbreaks such as severe acute respiratory syndrome (SARS) and influenza, we anticipate that obstetricians in private practice likely will have their hands full juggling a regular patient load, fielding calls from concerned patients, and caring for infected or ill patients who are being treated in an outpatient setting. Adding to that plate the need to rush to the hospital to clinically assess a patient for COVID-19 or for a delivery only compounds stress and exhaustion. At Ob Hospitalist Group, our hospitalist programs provide coverage and support to community obstetricians until they can arrive at the hospital or when the woman has no assigned obstetrician, reducing the pressure on community obstetricians to rush through their schedules.
Diagnostic and pharmaceutical companies are collaborating with public health officials to expedite diagnostic testing staff, hospital treatment capacity, vaccines, and even early therapies that may help to minimize severity. But right now, as clinicians work to protect their vulnerable patients, a close collaboration between community obstetricians and Ob hospitalists will help to keep patients and health care personnel safe and healthy – a goal that should apply not only to public health crises, but to the provision of maternal care every day.
Dr. Simon is chief medical officer at Ob Hospitalist Group (OBHG), is a board-certified ob.gyn., and former head of the department of obstetrics and gynecology for a U.S. hospital. He has no relevant conflicts of interest or financial disclosures. Email him at obnews@mdedge.com.
With the novel coronavirus (COVID-19) monopolizing the news cycle, fear and misinformation are at an all-time high. Public health officials and physicians are accelerating education outreach to the public to address misinformation, and identify and care for patients who may have been exposed to the virus.
In times of public health crises, pregnant women have unique and pressing concerns about their personal health and the health of their unborn children. While not often mentioned in major news coverage, obstetricians play a critical role during health crises because of their uniquely personal role with patients during all stages of pregnancy, providing this vulnerable population with the most up-to-date information and following the latest guidelines for recommended care.
Unfortunately, COVID-19 is breaking unfamiliar new ground. We know that pregnant women are at higher risk for viral infection – annually, influenza is a grim reminder that pregnant women are more immunocompromised than the general public – but we do not yet have data to confirm or refute that pregnant women have a higher susceptibility to COVID-19 than the rest of the adult population. We also do not know enough about COVID-19 transmission, including whether the virus can cross the transplacental barrier to affect a fetus, or whether it can be transmitted through breast milk.
As private practice community obstetricians work to protect their patients during this public health crisis, Ob hospitalists can play an important role in supporting them in the provision of patient care.
First, Ob hospitalists are highly-trained specialists who can help ensure that pregnant patients who seek care at the hospital – either with viral symptoms or with separate pregnancy-related concerns – are protected during triage until the treating community obstetrician can take the reins.
When a pregnant woman presents at a hospital, in most cases she will bypass the ED and instead be sent directly to the labor and delivery (L&D) unit. During a viral outbreak, there are two major concerns with this approach. For one thing, it means an immunocompromised woman is being sent through the hospital to get to L&D, and along the path, is exposed to every airborne pathogen in the facility (and, if she is already infected, exposes others along the way). In addition, in hospitals without an Ob hospitalist on site, the patient generally is not immediately triaged by a physician, physician’s assistant, or nurse practitioner upon arrival because those clinicians are not consistently on site in L&D.
In times of viral pandemics, new approaches are warranted. For hospitals with contracted L&D management with hospitalists, hospitalists work closely with department heads to implement protocols loosely based on the Emergency Severity Index (ESI) model established by the Agency for Healthcare Research and Quality. Just as the ESI algorithm guides clinical stratification of patients, in times of reported viral outbreaks, L&D should consider triage of all pregnant women at higher levels of acuity, regardless of presentation status. In particular, if they show clinical symptoms, they should be masked, accompanied to the L&D unit by protected personnel, separated from other patients in areas of forced proximity such as hallways and elevators, and triaged in a secure single-patient room with a closed door (ideally at negative pressure relative to the surrounding areas).
If the patient has traveled to an area of outbreak, reports exposure to travelers who have visited high-risk areas, has had contact with individuals who tested positive for COVID-19, or exhibits any clinical symptoms of COVID-19 (fever, dry cough, fatigue, etc.), her care management should adhere to standing hospital emergency protocols. Following consultation with the assigned community obstetrician, the Ob hospitalist and hospital staff should contact their local/state health departments immediately for all cases of patients who show symptoms to determine if the patient meets requirements for a person under investigation (PUI) for COVID-19. The state/local health department will work with clinicians to collect, store, and ship clinical specimens appropriately. Very ill patients may need to be treated in an intensive care setting where respiratory status can be closely monitored.
At Ob Hospitalist Group, our body of evidence from our large national footprint has informed the development of standard sets of protocols for delivery complications such as preeclampsia and postpartum hemorrhage, as well as a cesarean section reduction toolkit to combat medically unnecessary cesarean sections. OB hospitalists therefore can assist with refining COVID-19 protocols specifically for the L&D setting, using evidence-based data to tailor protocols to address public health emergencies as they evolve.
The second way that Ob hospitalists can support their colleagues is by covering L&D 24/7 so that community obstetricians can focus on other pressing medical needs. From our experience with other outbreaks such as severe acute respiratory syndrome (SARS) and influenza, we anticipate that obstetricians in private practice likely will have their hands full juggling a regular patient load, fielding calls from concerned patients, and caring for infected or ill patients who are being treated in an outpatient setting. Adding to that plate the need to rush to the hospital to clinically assess a patient for COVID-19 or for a delivery only compounds stress and exhaustion. At Ob Hospitalist Group, our hospitalist programs provide coverage and support to community obstetricians until they can arrive at the hospital or when the woman has no assigned obstetrician, reducing the pressure on community obstetricians to rush through their schedules.
Diagnostic and pharmaceutical companies are collaborating with public health officials to expedite diagnostic testing staff, hospital treatment capacity, vaccines, and even early therapies that may help to minimize severity. But right now, as clinicians work to protect their vulnerable patients, a close collaboration between community obstetricians and Ob hospitalists will help to keep patients and health care personnel safe and healthy – a goal that should apply not only to public health crises, but to the provision of maternal care every day.
Dr. Simon is chief medical officer at Ob Hospitalist Group (OBHG), is a board-certified ob.gyn., and former head of the department of obstetrics and gynecology for a U.S. hospital. He has no relevant conflicts of interest or financial disclosures. Email him at obnews@mdedge.com.
With the novel coronavirus (COVID-19) monopolizing the news cycle, fear and misinformation are at an all-time high. Public health officials and physicians are accelerating education outreach to the public to address misinformation, and identify and care for patients who may have been exposed to the virus.
In times of public health crises, pregnant women have unique and pressing concerns about their personal health and the health of their unborn children. While not often mentioned in major news coverage, obstetricians play a critical role during health crises because of their uniquely personal role with patients during all stages of pregnancy, providing this vulnerable population with the most up-to-date information and following the latest guidelines for recommended care.
Unfortunately, COVID-19 is breaking unfamiliar new ground. We know that pregnant women are at higher risk for viral infection – annually, influenza is a grim reminder that pregnant women are more immunocompromised than the general public – but we do not yet have data to confirm or refute that pregnant women have a higher susceptibility to COVID-19 than the rest of the adult population. We also do not know enough about COVID-19 transmission, including whether the virus can cross the transplacental barrier to affect a fetus, or whether it can be transmitted through breast milk.
As private practice community obstetricians work to protect their patients during this public health crisis, Ob hospitalists can play an important role in supporting them in the provision of patient care.
First, Ob hospitalists are highly-trained specialists who can help ensure that pregnant patients who seek care at the hospital – either with viral symptoms or with separate pregnancy-related concerns – are protected during triage until the treating community obstetrician can take the reins.
When a pregnant woman presents at a hospital, in most cases she will bypass the ED and instead be sent directly to the labor and delivery (L&D) unit. During a viral outbreak, there are two major concerns with this approach. For one thing, it means an immunocompromised woman is being sent through the hospital to get to L&D, and along the path, is exposed to every airborne pathogen in the facility (and, if she is already infected, exposes others along the way). In addition, in hospitals without an Ob hospitalist on site, the patient generally is not immediately triaged by a physician, physician’s assistant, or nurse practitioner upon arrival because those clinicians are not consistently on site in L&D.
In times of viral pandemics, new approaches are warranted. For hospitals with contracted L&D management with hospitalists, hospitalists work closely with department heads to implement protocols loosely based on the Emergency Severity Index (ESI) model established by the Agency for Healthcare Research and Quality. Just as the ESI algorithm guides clinical stratification of patients, in times of reported viral outbreaks, L&D should consider triage of all pregnant women at higher levels of acuity, regardless of presentation status. In particular, if they show clinical symptoms, they should be masked, accompanied to the L&D unit by protected personnel, separated from other patients in areas of forced proximity such as hallways and elevators, and triaged in a secure single-patient room with a closed door (ideally at negative pressure relative to the surrounding areas).
If the patient has traveled to an area of outbreak, reports exposure to travelers who have visited high-risk areas, has had contact with individuals who tested positive for COVID-19, or exhibits any clinical symptoms of COVID-19 (fever, dry cough, fatigue, etc.), her care management should adhere to standing hospital emergency protocols. Following consultation with the assigned community obstetrician, the Ob hospitalist and hospital staff should contact their local/state health departments immediately for all cases of patients who show symptoms to determine if the patient meets requirements for a person under investigation (PUI) for COVID-19. The state/local health department will work with clinicians to collect, store, and ship clinical specimens appropriately. Very ill patients may need to be treated in an intensive care setting where respiratory status can be closely monitored.
At Ob Hospitalist Group, our body of evidence from our large national footprint has informed the development of standard sets of protocols for delivery complications such as preeclampsia and postpartum hemorrhage, as well as a cesarean section reduction toolkit to combat medically unnecessary cesarean sections. OB hospitalists therefore can assist with refining COVID-19 protocols specifically for the L&D setting, using evidence-based data to tailor protocols to address public health emergencies as they evolve.
The second way that Ob hospitalists can support their colleagues is by covering L&D 24/7 so that community obstetricians can focus on other pressing medical needs. From our experience with other outbreaks such as severe acute respiratory syndrome (SARS) and influenza, we anticipate that obstetricians in private practice likely will have their hands full juggling a regular patient load, fielding calls from concerned patients, and caring for infected or ill patients who are being treated in an outpatient setting. Adding to that plate the need to rush to the hospital to clinically assess a patient for COVID-19 or for a delivery only compounds stress and exhaustion. At Ob Hospitalist Group, our hospitalist programs provide coverage and support to community obstetricians until they can arrive at the hospital or when the woman has no assigned obstetrician, reducing the pressure on community obstetricians to rush through their schedules.
Diagnostic and pharmaceutical companies are collaborating with public health officials to expedite diagnostic testing staff, hospital treatment capacity, vaccines, and even early therapies that may help to minimize severity. But right now, as clinicians work to protect their vulnerable patients, a close collaboration between community obstetricians and Ob hospitalists will help to keep patients and health care personnel safe and healthy – a goal that should apply not only to public health crises, but to the provision of maternal care every day.
Dr. Simon is chief medical officer at Ob Hospitalist Group (OBHG), is a board-certified ob.gyn., and former head of the department of obstetrics and gynecology for a U.S. hospital. He has no relevant conflicts of interest or financial disclosures. Email him at obnews@mdedge.com.
DAPT may benefit symptomatic carotid endarterectomy patients
LOS ANGELES –

The only patients who benefited from postsurgical treatment with dual antiplatelet therapy (DAPT) were those who were symptomatic (had a stroke or transient ischemic attack) prior to their carotid endarterectomy surgery, a minority of the more than 17,000 matched U.S. patients who underwent carotid endarterectomy during 2003-2018 and were part of this analysis, Nathan Belkin, MD, said at the International Stroke Conference, sponsored by the American Heart Association.
Among patients with symptoms prior to their carotid endarterectomy, DAPT at the time of hospital discharge was associated with a 2-year follow-up rate of stroke, transient ischemic attack (TIA), or death of about 8%, compared with a rate of about 11% among similar patients discharged on aspirin only, a statistically significant difference. In contrast, among patients who were asymptomatic prior to their carotid endarterectomy, discharge treatment with aspirin only was associated with a 2-year event rate similar to the rate among patients discharged on DAPT.
Based in part on this finding, Dr. Belkin and associates at the University of Pennsylvania, Philadelphia, now start symptomatic patients scheduled for carotid endarterectomy on DAPT with aspirin plus clopidogrel (Plavix) about 2 weeks before surgery, and then continue the combined regimen long term after surgery. A prospective, randomized study is needed to fully resolve the optimal use of DAPT in patients with significant carotid artery disease scheduled for carotid endarterectomy, but until then, “we’re individualizing DAPT” to patients at high risk because of a prior stroke or TIA who also have no evidence of an elevated bleeding risk, said Dr. Belkin, a vascular surgeon.
“We hypothesize that patients with systemic carotid disease have a systemic disease process and more activated platelets,” which suggests a potential benefit from DAPT, he explained. But the data that Dr. Belkin reported also indicated that recent U.S. use of DAPT in patients undergoing carotid endarterectomy has moved beyond this subgroup. The U.S. national data set that Dr. Belkin used for the analysis, the Vascular Quality Initiative registry maintained by the Society for Vascular Surgery, included 87,074 patients who underwent carotid endarterectomy during 2003-2018. During the entire 16-year period, 30% of patients overall received a prescription for DAPT at hospital discharge, but this level went steadily up during those years. In 2003, the rate of DAPT prescriptions at discharge was below 10% of patients but then rose incrementally over the following years and by 2018 had increased to about 44% despite a prevalence of symptomatic carotid disease closer to about a third of patients.
“It’s surprising that so many patients received DAPT for carotid disease” in recent years, commented Mai N. Nguyen-Huynh, MD, a vascular neurologist with Kaiser Permanente Northern California in Oakland. “It’s been thought that DAPT, and especially clopidogrel, was more beneficial for patients with intracranial atherosclerotic disease, but not so much for patients with carotid disease,” she said in an interview. “We don’t always see systemic atherosclerotic disease in patients with carotid artery disease. It’s not standard practice to look for systemic atherosclerotic disease in patients with carotid disease,” unless something in the patient’s presentation suggests wider vascular-disease progression.
The primary analysis that Dr. Belkin and associates ran removed about 16% of the patients who underwent carotid endarterectomy from the database: those who received no antiplatelet drug, those who received only clopidogrel, and those who went home from surgery on an anticoagulant. Among the remaining 72,122 patients, 35% received DAPT at discharge and 65% received aspirin only. The patients averaged 70 years old, 61% were men, 37% had a history of stroke or TIA, and their overall 2-year incidence of stroke, TIA, or death was 7.3%. To adjust for many baseline differences between the patients discharged on DAPT and those who got only aspirin, the researchers used propensity-score sorting to identify 17,398 matched patients from the two treatment subgroups, 24% of the total population. Comparison of these DAPT and aspirin-only subgroups showed no difference in the overall, 2-year rate of stroke, TIA, or death.
However, when the analysis divided the patients into asymptomatic and symptomatic subgroups, those discharged on DAPT showed a statistically significant lower rate of stroke, TIA, or death during 2 years of follow-up. The same symptomatic subgroup also showed a statistically significant lower rate of total mortality during 5 years of follow-up when treated with DAPT compared with aspirin only, again an absolute, between-group difference of about 3 percentage points that was statistically significant, a difference not seen in the asymptomatic patients. The type of treatment that symptomatic patients received had no relationship to their 2-year incidence of stroke or TIA.
To confirm these findings, Dr. Belkin and coworkers ran a multivariate logistic regression analysis on the data collected from all 72,122 patients who underwent carotid endarterectomy and subsequently received either DAPT or aspirin only. The only statistically significant association between treatment and outcome was among the symptomatic patients who received DAPT, who had a significant reduction in their 5-year mortality, compared with symptomatic patients who received only aspirin at hospital discharge.
Ideally, a comparison of DAPT and aspirin-only treatment should also assess the incidence and severity of bleeding events associated with these treatments, but bleeding data were not available in the database, Dr. Belkin said.
Dr. Belkin and Dr. Nguyen-Huynh had no relevant disclosures.
SOURCE: Belkin N et al. Stroke. 2020 Feb;51(suppl 1): Abstract 67.
LOS ANGELES –
The only patients who benefited from postsurgical treatment with dual antiplatelet therapy (DAPT) were those who were symptomatic (had a stroke or transient ischemic attack) prior to their carotid endarterectomy surgery, a minority of the more than 17,000 matched U.S. patients who underwent carotid endarterectomy during 2003-2018 and were part of this analysis, Nathan Belkin, MD, said at the International Stroke Conference, sponsored by the American Heart Association.
Among patients with symptoms prior to their carotid endarterectomy, DAPT at the time of hospital discharge was associated with a 2-year follow-up rate of stroke, transient ischemic attack (TIA), or death of about 8%, compared with a rate of about 11% among similar patients discharged on aspirin only, a statistically significant difference. In contrast, among patients who were asymptomatic prior to their carotid endarterectomy, discharge treatment with aspirin only was associated with a 2-year event rate similar to the rate among patients discharged on DAPT.
Based in part on this finding, Dr. Belkin and associates at the University of Pennsylvania, Philadelphia, now start symptomatic patients scheduled for carotid endarterectomy on DAPT with aspirin plus clopidogrel (Plavix) about 2 weeks before surgery, and then continue the combined regimen long term after surgery. A prospective, randomized study is needed to fully resolve the optimal use of DAPT in patients with significant carotid artery disease scheduled for carotid endarterectomy, but until then, “we’re individualizing DAPT” to patients at high risk because of a prior stroke or TIA who also have no evidence of an elevated bleeding risk, said Dr. Belkin, a vascular surgeon.
“We hypothesize that patients with systemic carotid disease have a systemic disease process and more activated platelets,” which suggests a potential benefit from DAPT, he explained. But the data that Dr. Belkin reported also indicated that recent U.S. use of DAPT in patients undergoing carotid endarterectomy has moved beyond this subgroup. The U.S. national data set that Dr. Belkin used for the analysis, the Vascular Quality Initiative registry maintained by the Society for Vascular Surgery, included 87,074 patients who underwent carotid endarterectomy during 2003-2018. During the entire 16-year period, 30% of patients overall received a prescription for DAPT at hospital discharge, but this level went steadily up during those years. In 2003, the rate of DAPT prescriptions at discharge was below 10% of patients but then rose incrementally over the following years and by 2018 had increased to about 44% despite a prevalence of symptomatic carotid disease closer to about a third of patients.
“It’s surprising that so many patients received DAPT for carotid disease” in recent years, commented Mai N. Nguyen-Huynh, MD, a vascular neurologist with Kaiser Permanente Northern California in Oakland. “It’s been thought that DAPT, and especially clopidogrel, was more beneficial for patients with intracranial atherosclerotic disease, but not so much for patients with carotid disease,” she said in an interview. “We don’t always see systemic atherosclerotic disease in patients with carotid artery disease. It’s not standard practice to look for systemic atherosclerotic disease in patients with carotid disease,” unless something in the patient’s presentation suggests wider vascular-disease progression.
The primary analysis that Dr. Belkin and associates ran removed about 16% of the patients who underwent carotid endarterectomy from the database: those who received no antiplatelet drug, those who received only clopidogrel, and those who went home from surgery on an anticoagulant. Among the remaining 72,122 patients, 35% received DAPT at discharge and 65% received aspirin only. The patients averaged 70 years old, 61% were men, 37% had a history of stroke or TIA, and their overall 2-year incidence of stroke, TIA, or death was 7.3%. To adjust for many baseline differences between the patients discharged on DAPT and those who got only aspirin, the researchers used propensity-score sorting to identify 17,398 matched patients from the two treatment subgroups, 24% of the total population. Comparison of these DAPT and aspirin-only subgroups showed no difference in the overall, 2-year rate of stroke, TIA, or death.
However, when the analysis divided the patients into asymptomatic and symptomatic subgroups, those discharged on DAPT showed a statistically significant lower rate of stroke, TIA, or death during 2 years of follow-up. The same symptomatic subgroup also showed a statistically significant lower rate of total mortality during 5 years of follow-up when treated with DAPT compared with aspirin only, again an absolute, between-group difference of about 3 percentage points that was statistically significant, a difference not seen in the asymptomatic patients. The type of treatment that symptomatic patients received had no relationship to their 2-year incidence of stroke or TIA.
To confirm these findings, Dr. Belkin and coworkers ran a multivariate logistic regression analysis on the data collected from all 72,122 patients who underwent carotid endarterectomy and subsequently received either DAPT or aspirin only. The only statistically significant association between treatment and outcome was among the symptomatic patients who received DAPT, who had a significant reduction in their 5-year mortality, compared with symptomatic patients who received only aspirin at hospital discharge.
Ideally, a comparison of DAPT and aspirin-only treatment should also assess the incidence and severity of bleeding events associated with these treatments, but bleeding data were not available in the database, Dr. Belkin said.
Dr. Belkin and Dr. Nguyen-Huynh had no relevant disclosures.
SOURCE: Belkin N et al. Stroke. 2020 Feb;51(suppl 1): Abstract 67.
LOS ANGELES –
The only patients who benefited from postsurgical treatment with dual antiplatelet therapy (DAPT) were those who were symptomatic (had a stroke or transient ischemic attack) prior to their carotid endarterectomy surgery, a minority of the more than 17,000 matched U.S. patients who underwent carotid endarterectomy during 2003-2018 and were part of this analysis, Nathan Belkin, MD, said at the International Stroke Conference, sponsored by the American Heart Association.
Among patients with symptoms prior to their carotid endarterectomy, DAPT at the time of hospital discharge was associated with a 2-year follow-up rate of stroke, transient ischemic attack (TIA), or death of about 8%, compared with a rate of about 11% among similar patients discharged on aspirin only, a statistically significant difference. In contrast, among patients who were asymptomatic prior to their carotid endarterectomy, discharge treatment with aspirin only was associated with a 2-year event rate similar to the rate among patients discharged on DAPT.
Based in part on this finding, Dr. Belkin and associates at the University of Pennsylvania, Philadelphia, now start symptomatic patients scheduled for carotid endarterectomy on DAPT with aspirin plus clopidogrel (Plavix) about 2 weeks before surgery, and then continue the combined regimen long term after surgery. A prospective, randomized study is needed to fully resolve the optimal use of DAPT in patients with significant carotid artery disease scheduled for carotid endarterectomy, but until then, “we’re individualizing DAPT” to patients at high risk because of a prior stroke or TIA who also have no evidence of an elevated bleeding risk, said Dr. Belkin, a vascular surgeon.
“We hypothesize that patients with systemic carotid disease have a systemic disease process and more activated platelets,” which suggests a potential benefit from DAPT, he explained. But the data that Dr. Belkin reported also indicated that recent U.S. use of DAPT in patients undergoing carotid endarterectomy has moved beyond this subgroup. The U.S. national data set that Dr. Belkin used for the analysis, the Vascular Quality Initiative registry maintained by the Society for Vascular Surgery, included 87,074 patients who underwent carotid endarterectomy during 2003-2018. During the entire 16-year period, 30% of patients overall received a prescription for DAPT at hospital discharge, but this level went steadily up during those years. In 2003, the rate of DAPT prescriptions at discharge was below 10% of patients but then rose incrementally over the following years and by 2018 had increased to about 44% despite a prevalence of symptomatic carotid disease closer to about a third of patients.
“It’s surprising that so many patients received DAPT for carotid disease” in recent years, commented Mai N. Nguyen-Huynh, MD, a vascular neurologist with Kaiser Permanente Northern California in Oakland. “It’s been thought that DAPT, and especially clopidogrel, was more beneficial for patients with intracranial atherosclerotic disease, but not so much for patients with carotid disease,” she said in an interview. “We don’t always see systemic atherosclerotic disease in patients with carotid artery disease. It’s not standard practice to look for systemic atherosclerotic disease in patients with carotid disease,” unless something in the patient’s presentation suggests wider vascular-disease progression.
The primary analysis that Dr. Belkin and associates ran removed about 16% of the patients who underwent carotid endarterectomy from the database: those who received no antiplatelet drug, those who received only clopidogrel, and those who went home from surgery on an anticoagulant. Among the remaining 72,122 patients, 35% received DAPT at discharge and 65% received aspirin only. The patients averaged 70 years old, 61% were men, 37% had a history of stroke or TIA, and their overall 2-year incidence of stroke, TIA, or death was 7.3%. To adjust for many baseline differences between the patients discharged on DAPT and those who got only aspirin, the researchers used propensity-score sorting to identify 17,398 matched patients from the two treatment subgroups, 24% of the total population. Comparison of these DAPT and aspirin-only subgroups showed no difference in the overall, 2-year rate of stroke, TIA, or death.
However, when the analysis divided the patients into asymptomatic and symptomatic subgroups, those discharged on DAPT showed a statistically significant lower rate of stroke, TIA, or death during 2 years of follow-up. The same symptomatic subgroup also showed a statistically significant lower rate of total mortality during 5 years of follow-up when treated with DAPT compared with aspirin only, again an absolute, between-group difference of about 3 percentage points that was statistically significant, a difference not seen in the asymptomatic patients. The type of treatment that symptomatic patients received had no relationship to their 2-year incidence of stroke or TIA.
To confirm these findings, Dr. Belkin and coworkers ran a multivariate logistic regression analysis on the data collected from all 72,122 patients who underwent carotid endarterectomy and subsequently received either DAPT or aspirin only. The only statistically significant association between treatment and outcome was among the symptomatic patients who received DAPT, who had a significant reduction in their 5-year mortality, compared with symptomatic patients who received only aspirin at hospital discharge.
Ideally, a comparison of DAPT and aspirin-only treatment should also assess the incidence and severity of bleeding events associated with these treatments, but bleeding data were not available in the database, Dr. Belkin said.
Dr. Belkin and Dr. Nguyen-Huynh had no relevant disclosures.
SOURCE: Belkin N et al. Stroke. 2020 Feb;51(suppl 1): Abstract 67.
REPORTING FROM ISC 2020
Firm Abdominal Papule
The Diagnosis: Cutaneous Metastatic Gastric Carcinoma
Cutaneous metastasis of primary gastric carcinoma is a rare occurrence, with the more common metastatic sites being the lymph nodes, liver, and peritoneal cavity. The incidence of visceral neoplasm metastasis to the skin ranges from 0.7% to 9% and is less than 1% for upper digestive tract carcinomas.1 Cutaneous metastases make up 2% of all tumors of the skin and commonly are located near the site of the primary tumor.2 The most common cutaneous metastasis sites for gastric carcinoma include the neck, chest, and head.3 One of the more typical sites of cutaneous metastasis from gastric cancer is the umbilicus (ie, Sister Mary Joseph nodule). Cutaneous metastases from gastric carcinoma commonly present as asymptomatic hyperpigmented nodules.1,3
In our patient, histopathologic sections showed diffuse infiltration of the dermis by atypical polygonal/round cells arranged in cords and small aggregates. Some of the neoplastic cells had signet ring morphology (Figure). Tumor cells demonstrated positive immunostaining for CDX2, villin, CAM 5.2, and epithelial membrane antigen; they were negative for S-100, MART-1 (melanoma-associated antigen recognized by T cells 1), leukocyte common antigen, gross cystic disease fluid protein 15, estrogen and progesterone receptor, and HER2/neu (human epidermal growth factor receptor 2).
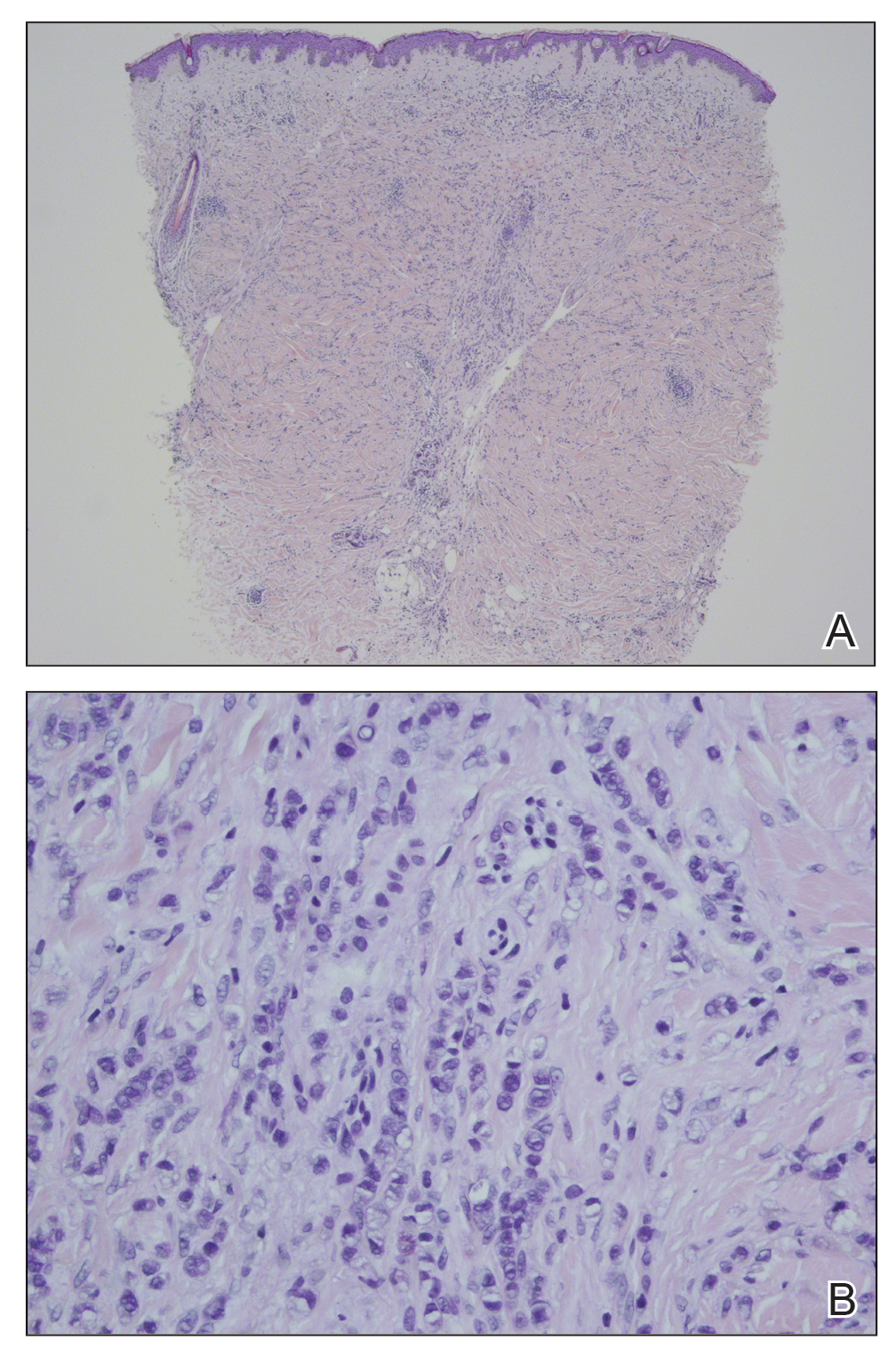
Our patient's presentation was rare in that she developed an asymptomatic erythematous papule on the skin of the abdomen. However, her history of stage IIIB gastric adenocarcinoma in conjunction with the clinical picture and microscopic findings were most consistent with metastatic carcinoma of gastrointestinal origin. The histologic hallmarks of cutaneous metastatic gastric carcinoma include aggregates of neoplastic cells arranged in cords, sometimes forming glands, embedded in a fibrous stroma. Tumor cells may demonstrate signet ring morphology. These unique histologic findings, as well as positive immunostaining for CDX2, villin, CAM 5.2, and epithelial membrane antigen, rule out other potential diagnoses for an asymptomatic solitary papule.
Dermatofibrosarcoma protuberans presents as an asymptomatic, slow-growing, indurated papule or plaque that develops into a red or brownish nodule. Histologically, dermatofibrosarcoma protuberans is characterized by spindled cells, few mitotic figures, infiltration of the subcutaneous tissue in a honeycomblike pattern, and obliteration of the adnexal structures.4
Cutaneous B-cell lymphoma (CBCL) can present as single or multiple red papules or nodules located on the trunk, face, or extremities. Histologically, CBCL would show a nodular or diffuse infiltrate throughout the dermis, frequently with accentuation in the deep reticular dermis, sparing of the epidermis, and the presence of a grenz zone. The infiltrate in CBCL consists of CD20+, CD19+, and CD79a+ B cells. Identification of a monoclonal B-cell population either by immunohistochemistry or polymerase chain reaction would further support a diagnosis of CBCL.4 These specific histologic findings and the immunohistochemical staining pattern helped rule out CBCL as the diagnosis in our patient.
Amelanotic melanomas present as flesh-colored to light pink papules, making them especially challenging to diagnose clinically. Asymmetrical, poorly circumscribed nests of atypical melanocytes as well as single melanocytes within the epidermis and dermis are seen histologically; mitotic figures are common. Immunohistochemical staining for melanoma includes S-100, human melanoma black 45, MART-1/Melan-A, tyrosinase, and microphthalmia-associated transcription factor 1.4
Neurothekeomas can present as asymptomatic, solitary, flesh-colored papules located on the head, neck, and upper trunk. Histologically, neurothekeomas have a distinct appearance consisting of a well-defined mass composed of variable-sized lobules of spindled and epithelioid cells dispersed in a myxoid stroma within the reticular dermis.4 These specific histologic findings helped rule out neurothekeoma in our patient.
Following the diagnosis of cutaneous metastatic gastric carcinoma in our patient, positron emission tomography and computed tomography of the chest, abdomen, and pelvis were unremarkable for distant disease. Subsequently, the patient underwent surgical excision of the papule with clear margins, followed by a short course of radiation therapy. She currently is under close monitoring but remains in remission with no new cutaneous manifestations of the gastric carcinoma.
- Erdemir A, Atilganoglu U, Onsun N, et al. Cutaneous metastases from gastric adenocarcinoma. Indian J Dermatol. 2011;56:236-237.
- Junqueira AL, Corbett AM, Oliveira Filho Jd, et al. Cutaneous metastasis from gastrointestinal adenocarcinoma of unknown primary origin. An Bras Dermatol. 2015;90:564-566.
- Cesaretti M, Malerba M, Basso V, et al. Cutaneous metastasis from primary gastric cancer: a case report and review of the literature. Cutis. 2014;93:E9-E13.
- Bolognia J, Jorizzo JL, Schaffer JV. Dermatology. Philadelphia, PA: Elsevier Saunders; 2012.
The Diagnosis: Cutaneous Metastatic Gastric Carcinoma
Cutaneous metastasis of primary gastric carcinoma is a rare occurrence, with the more common metastatic sites being the lymph nodes, liver, and peritoneal cavity. The incidence of visceral neoplasm metastasis to the skin ranges from 0.7% to 9% and is less than 1% for upper digestive tract carcinomas.1 Cutaneous metastases make up 2% of all tumors of the skin and commonly are located near the site of the primary tumor.2 The most common cutaneous metastasis sites for gastric carcinoma include the neck, chest, and head.3 One of the more typical sites of cutaneous metastasis from gastric cancer is the umbilicus (ie, Sister Mary Joseph nodule). Cutaneous metastases from gastric carcinoma commonly present as asymptomatic hyperpigmented nodules.1,3
In our patient, histopathologic sections showed diffuse infiltration of the dermis by atypical polygonal/round cells arranged in cords and small aggregates. Some of the neoplastic cells had signet ring morphology (Figure). Tumor cells demonstrated positive immunostaining for CDX2, villin, CAM 5.2, and epithelial membrane antigen; they were negative for S-100, MART-1 (melanoma-associated antigen recognized by T cells 1), leukocyte common antigen, gross cystic disease fluid protein 15, estrogen and progesterone receptor, and HER2/neu (human epidermal growth factor receptor 2).
Our patient's presentation was rare in that she developed an asymptomatic erythematous papule on the skin of the abdomen. However, her history of stage IIIB gastric adenocarcinoma in conjunction with the clinical picture and microscopic findings were most consistent with metastatic carcinoma of gastrointestinal origin. The histologic hallmarks of cutaneous metastatic gastric carcinoma include aggregates of neoplastic cells arranged in cords, sometimes forming glands, embedded in a fibrous stroma. Tumor cells may demonstrate signet ring morphology. These unique histologic findings, as well as positive immunostaining for CDX2, villin, CAM 5.2, and epithelial membrane antigen, rule out other potential diagnoses for an asymptomatic solitary papule.
Dermatofibrosarcoma protuberans presents as an asymptomatic, slow-growing, indurated papule or plaque that develops into a red or brownish nodule. Histologically, dermatofibrosarcoma protuberans is characterized by spindled cells, few mitotic figures, infiltration of the subcutaneous tissue in a honeycomblike pattern, and obliteration of the adnexal structures.4
Cutaneous B-cell lymphoma (CBCL) can present as single or multiple red papules or nodules located on the trunk, face, or extremities. Histologically, CBCL would show a nodular or diffuse infiltrate throughout the dermis, frequently with accentuation in the deep reticular dermis, sparing of the epidermis, and the presence of a grenz zone. The infiltrate in CBCL consists of CD20+, CD19+, and CD79a+ B cells. Identification of a monoclonal B-cell population either by immunohistochemistry or polymerase chain reaction would further support a diagnosis of CBCL.4 These specific histologic findings and the immunohistochemical staining pattern helped rule out CBCL as the diagnosis in our patient.
Amelanotic melanomas present as flesh-colored to light pink papules, making them especially challenging to diagnose clinically. Asymmetrical, poorly circumscribed nests of atypical melanocytes as well as single melanocytes within the epidermis and dermis are seen histologically; mitotic figures are common. Immunohistochemical staining for melanoma includes S-100, human melanoma black 45, MART-1/Melan-A, tyrosinase, and microphthalmia-associated transcription factor 1.4
Neurothekeomas can present as asymptomatic, solitary, flesh-colored papules located on the head, neck, and upper trunk. Histologically, neurothekeomas have a distinct appearance consisting of a well-defined mass composed of variable-sized lobules of spindled and epithelioid cells dispersed in a myxoid stroma within the reticular dermis.4 These specific histologic findings helped rule out neurothekeoma in our patient.
Following the diagnosis of cutaneous metastatic gastric carcinoma in our patient, positron emission tomography and computed tomography of the chest, abdomen, and pelvis were unremarkable for distant disease. Subsequently, the patient underwent surgical excision of the papule with clear margins, followed by a short course of radiation therapy. She currently is under close monitoring but remains in remission with no new cutaneous manifestations of the gastric carcinoma.
The Diagnosis: Cutaneous Metastatic Gastric Carcinoma
Cutaneous metastasis of primary gastric carcinoma is a rare occurrence, with the more common metastatic sites being the lymph nodes, liver, and peritoneal cavity. The incidence of visceral neoplasm metastasis to the skin ranges from 0.7% to 9% and is less than 1% for upper digestive tract carcinomas.1 Cutaneous metastases make up 2% of all tumors of the skin and commonly are located near the site of the primary tumor.2 The most common cutaneous metastasis sites for gastric carcinoma include the neck, chest, and head.3 One of the more typical sites of cutaneous metastasis from gastric cancer is the umbilicus (ie, Sister Mary Joseph nodule). Cutaneous metastases from gastric carcinoma commonly present as asymptomatic hyperpigmented nodules.1,3
In our patient, histopathologic sections showed diffuse infiltration of the dermis by atypical polygonal/round cells arranged in cords and small aggregates. Some of the neoplastic cells had signet ring morphology (Figure). Tumor cells demonstrated positive immunostaining for CDX2, villin, CAM 5.2, and epithelial membrane antigen; they were negative for S-100, MART-1 (melanoma-associated antigen recognized by T cells 1), leukocyte common antigen, gross cystic disease fluid protein 15, estrogen and progesterone receptor, and HER2/neu (human epidermal growth factor receptor 2).
Our patient's presentation was rare in that she developed an asymptomatic erythematous papule on the skin of the abdomen. However, her history of stage IIIB gastric adenocarcinoma in conjunction with the clinical picture and microscopic findings were most consistent with metastatic carcinoma of gastrointestinal origin. The histologic hallmarks of cutaneous metastatic gastric carcinoma include aggregates of neoplastic cells arranged in cords, sometimes forming glands, embedded in a fibrous stroma. Tumor cells may demonstrate signet ring morphology. These unique histologic findings, as well as positive immunostaining for CDX2, villin, CAM 5.2, and epithelial membrane antigen, rule out other potential diagnoses for an asymptomatic solitary papule.
Dermatofibrosarcoma protuberans presents as an asymptomatic, slow-growing, indurated papule or plaque that develops into a red or brownish nodule. Histologically, dermatofibrosarcoma protuberans is characterized by spindled cells, few mitotic figures, infiltration of the subcutaneous tissue in a honeycomblike pattern, and obliteration of the adnexal structures.4
Cutaneous B-cell lymphoma (CBCL) can present as single or multiple red papules or nodules located on the trunk, face, or extremities. Histologically, CBCL would show a nodular or diffuse infiltrate throughout the dermis, frequently with accentuation in the deep reticular dermis, sparing of the epidermis, and the presence of a grenz zone. The infiltrate in CBCL consists of CD20+, CD19+, and CD79a+ B cells. Identification of a monoclonal B-cell population either by immunohistochemistry or polymerase chain reaction would further support a diagnosis of CBCL.4 These specific histologic findings and the immunohistochemical staining pattern helped rule out CBCL as the diagnosis in our patient.
Amelanotic melanomas present as flesh-colored to light pink papules, making them especially challenging to diagnose clinically. Asymmetrical, poorly circumscribed nests of atypical melanocytes as well as single melanocytes within the epidermis and dermis are seen histologically; mitotic figures are common. Immunohistochemical staining for melanoma includes S-100, human melanoma black 45, MART-1/Melan-A, tyrosinase, and microphthalmia-associated transcription factor 1.4
Neurothekeomas can present as asymptomatic, solitary, flesh-colored papules located on the head, neck, and upper trunk. Histologically, neurothekeomas have a distinct appearance consisting of a well-defined mass composed of variable-sized lobules of spindled and epithelioid cells dispersed in a myxoid stroma within the reticular dermis.4 These specific histologic findings helped rule out neurothekeoma in our patient.
Following the diagnosis of cutaneous metastatic gastric carcinoma in our patient, positron emission tomography and computed tomography of the chest, abdomen, and pelvis were unremarkable for distant disease. Subsequently, the patient underwent surgical excision of the papule with clear margins, followed by a short course of radiation therapy. She currently is under close monitoring but remains in remission with no new cutaneous manifestations of the gastric carcinoma.
- Erdemir A, Atilganoglu U, Onsun N, et al. Cutaneous metastases from gastric adenocarcinoma. Indian J Dermatol. 2011;56:236-237.
- Junqueira AL, Corbett AM, Oliveira Filho Jd, et al. Cutaneous metastasis from gastrointestinal adenocarcinoma of unknown primary origin. An Bras Dermatol. 2015;90:564-566.
- Cesaretti M, Malerba M, Basso V, et al. Cutaneous metastasis from primary gastric cancer: a case report and review of the literature. Cutis. 2014;93:E9-E13.
- Bolognia J, Jorizzo JL, Schaffer JV. Dermatology. Philadelphia, PA: Elsevier Saunders; 2012.
- Erdemir A, Atilganoglu U, Onsun N, et al. Cutaneous metastases from gastric adenocarcinoma. Indian J Dermatol. 2011;56:236-237.
- Junqueira AL, Corbett AM, Oliveira Filho Jd, et al. Cutaneous metastasis from gastrointestinal adenocarcinoma of unknown primary origin. An Bras Dermatol. 2015;90:564-566.
- Cesaretti M, Malerba M, Basso V, et al. Cutaneous metastasis from primary gastric cancer: a case report and review of the literature. Cutis. 2014;93:E9-E13.
- Bolognia J, Jorizzo JL, Schaffer JV. Dermatology. Philadelphia, PA: Elsevier Saunders; 2012.
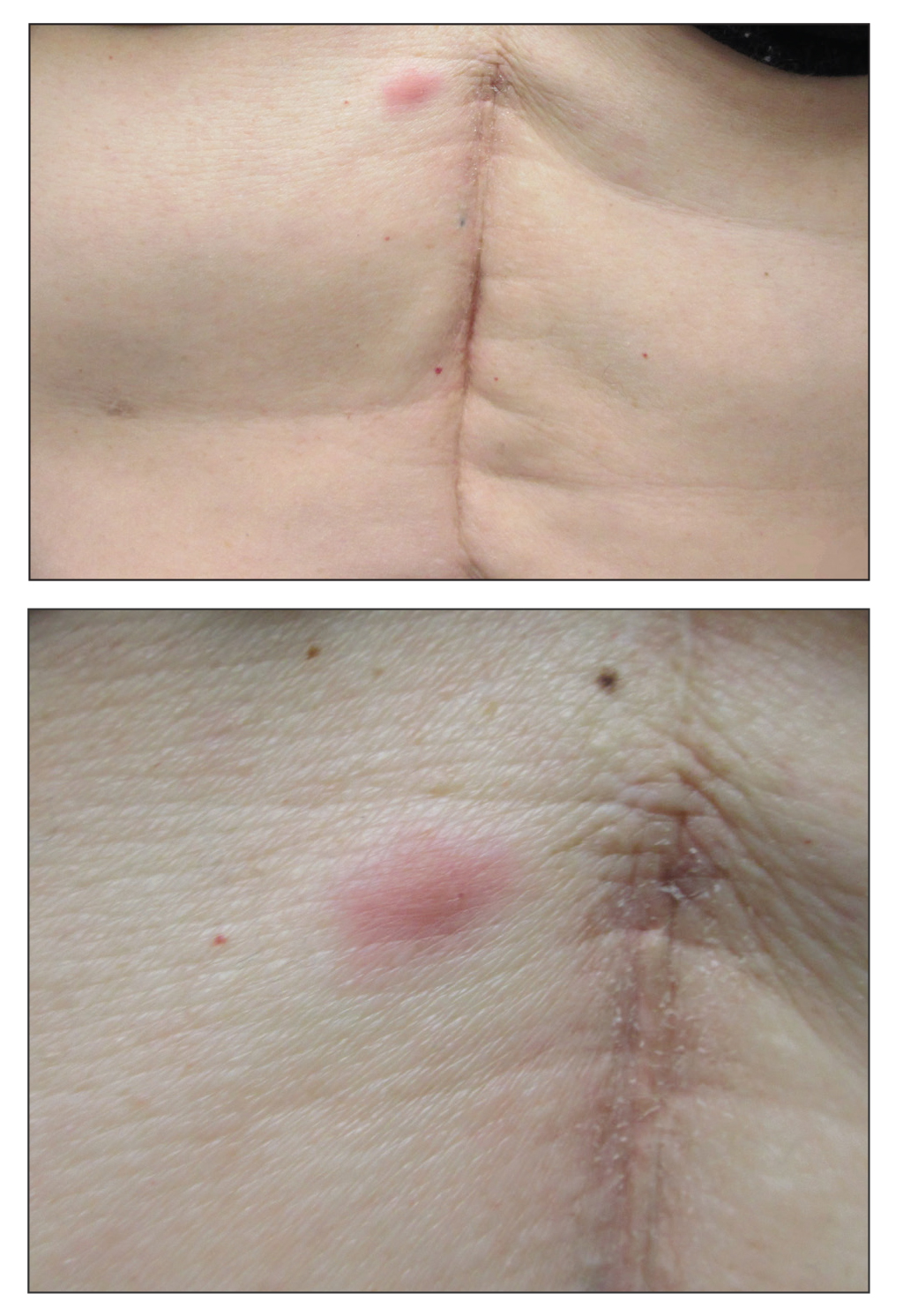
A 53-year-old woman with a history of melanoma on the right thigh, stage II Hodgkin lymphoma, and stage IIIB gastric adenocarcinoma treated with a distal gastrectomy presented with an asymptomatic but persistent skin lesion on the abdomen of 2 months' duration. The lesion arose spontaneously 6 months prior and had increased in size during that time. Physical examination revealed a 6-mm, solitary, firm, erythematous papule on the skin of the right upper quadrant of the abdomen. The patient was otherwise healthy, and a review of systems did not reveal any abnormalities. A punch biopsy was submitted for histopathologic review.
