User login
Behavioral intervention improves physical activity in patients with diabetes
A behavioral intervention that involves regular counseling sessions could help patients with type 2 diabetes increase their levels of physical activity and decrease their amount of sedentary time, according to findings from a prospective, randomized trial of 300 physically inactive patients with type 2 diabetes.
“The primary strength of this study is the application of an intervention targeting both physical activity and sedentary time across all settings (e.g., leisure, transportation, household, and occupation), based on theoretical grounds and using several behavior-change techniques,” wrote Stefano Balducci, MD, of Sapienza University in Rome and his colleagues. The findings were published in JAMA.
Half the participants were randomized to an intervention that involved one individual theoretical counseling session with a diabetologist and eight biweekly theoretical and practical counseling sessions with an exercise specialist each year for 3 years. The other half received standard care in the form of recommendations from their general physician about increasing physical activity and decreasing sedentary time. Both groups also received the same general treatment regimen according to guidelines.
The findings showed significant increases in volume of physical activity, light-intensity physical activity, and moderate to vigorous physical activity in the intervention group during the first 4 months of the trial. Those increases also were greater than the increases seen in the usual care group. Patients in the intervention group also showed greater decreases in sedentary time, compared with those in the control group during the same time.
After 4 months, the increases in physical activity in the intervention group plateaued but remained stable until 2 years. After that, the levels of activity declined but still remained significantly higher than at baseline. The level of sedentary time also increased after 2 years but was still lower than at baseline.
By the end of the study, the intervention group accumulated 13.8 metabolic equivalent hours/week of physical activity volume, compared with 10.5 hours in the control group; 18.9 minutes/day of moderate to vigorous intensity physical activity, compared with 12.5 minutes in the control group; and 4.6 hours/day of light-intensity physical activity, compared with 3.8 hours in the control group. In regard to sedentary time, the intervention group accumulated 10.9 hours/day, compared with 11.7 hours in the control group. All differences were statistically significant.
“The present findings support the need for interventions targeting all domains of behavior to obtain substantial lifestyle changes, not limited to moderate- to vigorous-intensity physical activity, which has little effect on sedentary time,” Dr. Balducci and his coauthors wrote. “This concept is consistent with a 2018 report showing that physical activity, sedentary time, and cardiorespiratory fitness are all important for cardiometabolic health.”
For the secondary outcomes of cardiorespiratory fitness and lower-body strength, the authors saw significant improvements in the intervention group, whereas the control group showed a worsening in those outcomes. The intervention group also showed significant improvements in fasting plasma glucose level, systolic blood pressure, total coronary heart disease 10-year risk score, and fatal coronary heart disease 10-year risk score. They also had significantly greater improvements than did the control group in total stroke risk score, hemoglobin A1c, fasting plasma glucose levels, and coronary heart disease risk.
In all, there were 41 adverse events in the intervention group, compared with 59 in the control group, outside of the sessions. During the sessions, participants in the intervention group experienced mild hypoglycemia (8 episodes), tachycardia/arrhythmia (3), and musculoskeletal injury or discomfort (19).
One of the limitations highlighted by the authors was that the benefits of their strategy could vary in other cohorts because of differences in climatic, socioeconomic, or cultural settings.
The study was supported by the Metabolic Fitness Association. Three authors declared grants and personal fees from pharmaceutical companies, and one author was an employee of Technogym. No other conflicts of interest were declared.
SOURCE: Balducci S et al. JAMA. 2019;321:880-90.
A behavioral intervention that involves regular counseling sessions could help patients with type 2 diabetes increase their levels of physical activity and decrease their amount of sedentary time, according to findings from a prospective, randomized trial of 300 physically inactive patients with type 2 diabetes.
“The primary strength of this study is the application of an intervention targeting both physical activity and sedentary time across all settings (e.g., leisure, transportation, household, and occupation), based on theoretical grounds and using several behavior-change techniques,” wrote Stefano Balducci, MD, of Sapienza University in Rome and his colleagues. The findings were published in JAMA.
Half the participants were randomized to an intervention that involved one individual theoretical counseling session with a diabetologist and eight biweekly theoretical and practical counseling sessions with an exercise specialist each year for 3 years. The other half received standard care in the form of recommendations from their general physician about increasing physical activity and decreasing sedentary time. Both groups also received the same general treatment regimen according to guidelines.
The findings showed significant increases in volume of physical activity, light-intensity physical activity, and moderate to vigorous physical activity in the intervention group during the first 4 months of the trial. Those increases also were greater than the increases seen in the usual care group. Patients in the intervention group also showed greater decreases in sedentary time, compared with those in the control group during the same time.
After 4 months, the increases in physical activity in the intervention group plateaued but remained stable until 2 years. After that, the levels of activity declined but still remained significantly higher than at baseline. The level of sedentary time also increased after 2 years but was still lower than at baseline.
By the end of the study, the intervention group accumulated 13.8 metabolic equivalent hours/week of physical activity volume, compared with 10.5 hours in the control group; 18.9 minutes/day of moderate to vigorous intensity physical activity, compared with 12.5 minutes in the control group; and 4.6 hours/day of light-intensity physical activity, compared with 3.8 hours in the control group. In regard to sedentary time, the intervention group accumulated 10.9 hours/day, compared with 11.7 hours in the control group. All differences were statistically significant.
“The present findings support the need for interventions targeting all domains of behavior to obtain substantial lifestyle changes, not limited to moderate- to vigorous-intensity physical activity, which has little effect on sedentary time,” Dr. Balducci and his coauthors wrote. “This concept is consistent with a 2018 report showing that physical activity, sedentary time, and cardiorespiratory fitness are all important for cardiometabolic health.”
For the secondary outcomes of cardiorespiratory fitness and lower-body strength, the authors saw significant improvements in the intervention group, whereas the control group showed a worsening in those outcomes. The intervention group also showed significant improvements in fasting plasma glucose level, systolic blood pressure, total coronary heart disease 10-year risk score, and fatal coronary heart disease 10-year risk score. They also had significantly greater improvements than did the control group in total stroke risk score, hemoglobin A1c, fasting plasma glucose levels, and coronary heart disease risk.
In all, there were 41 adverse events in the intervention group, compared with 59 in the control group, outside of the sessions. During the sessions, participants in the intervention group experienced mild hypoglycemia (8 episodes), tachycardia/arrhythmia (3), and musculoskeletal injury or discomfort (19).
One of the limitations highlighted by the authors was that the benefits of their strategy could vary in other cohorts because of differences in climatic, socioeconomic, or cultural settings.
The study was supported by the Metabolic Fitness Association. Three authors declared grants and personal fees from pharmaceutical companies, and one author was an employee of Technogym. No other conflicts of interest were declared.
SOURCE: Balducci S et al. JAMA. 2019;321:880-90.
A behavioral intervention that involves regular counseling sessions could help patients with type 2 diabetes increase their levels of physical activity and decrease their amount of sedentary time, according to findings from a prospective, randomized trial of 300 physically inactive patients with type 2 diabetes.
“The primary strength of this study is the application of an intervention targeting both physical activity and sedentary time across all settings (e.g., leisure, transportation, household, and occupation), based on theoretical grounds and using several behavior-change techniques,” wrote Stefano Balducci, MD, of Sapienza University in Rome and his colleagues. The findings were published in JAMA.
Half the participants were randomized to an intervention that involved one individual theoretical counseling session with a diabetologist and eight biweekly theoretical and practical counseling sessions with an exercise specialist each year for 3 years. The other half received standard care in the form of recommendations from their general physician about increasing physical activity and decreasing sedentary time. Both groups also received the same general treatment regimen according to guidelines.
The findings showed significant increases in volume of physical activity, light-intensity physical activity, and moderate to vigorous physical activity in the intervention group during the first 4 months of the trial. Those increases also were greater than the increases seen in the usual care group. Patients in the intervention group also showed greater decreases in sedentary time, compared with those in the control group during the same time.
After 4 months, the increases in physical activity in the intervention group plateaued but remained stable until 2 years. After that, the levels of activity declined but still remained significantly higher than at baseline. The level of sedentary time also increased after 2 years but was still lower than at baseline.
By the end of the study, the intervention group accumulated 13.8 metabolic equivalent hours/week of physical activity volume, compared with 10.5 hours in the control group; 18.9 minutes/day of moderate to vigorous intensity physical activity, compared with 12.5 minutes in the control group; and 4.6 hours/day of light-intensity physical activity, compared with 3.8 hours in the control group. In regard to sedentary time, the intervention group accumulated 10.9 hours/day, compared with 11.7 hours in the control group. All differences were statistically significant.
“The present findings support the need for interventions targeting all domains of behavior to obtain substantial lifestyle changes, not limited to moderate- to vigorous-intensity physical activity, which has little effect on sedentary time,” Dr. Balducci and his coauthors wrote. “This concept is consistent with a 2018 report showing that physical activity, sedentary time, and cardiorespiratory fitness are all important for cardiometabolic health.”
For the secondary outcomes of cardiorespiratory fitness and lower-body strength, the authors saw significant improvements in the intervention group, whereas the control group showed a worsening in those outcomes. The intervention group also showed significant improvements in fasting plasma glucose level, systolic blood pressure, total coronary heart disease 10-year risk score, and fatal coronary heart disease 10-year risk score. They also had significantly greater improvements than did the control group in total stroke risk score, hemoglobin A1c, fasting plasma glucose levels, and coronary heart disease risk.
In all, there were 41 adverse events in the intervention group, compared with 59 in the control group, outside of the sessions. During the sessions, participants in the intervention group experienced mild hypoglycemia (8 episodes), tachycardia/arrhythmia (3), and musculoskeletal injury or discomfort (19).
One of the limitations highlighted by the authors was that the benefits of their strategy could vary in other cohorts because of differences in climatic, socioeconomic, or cultural settings.
The study was supported by the Metabolic Fitness Association. Three authors declared grants and personal fees from pharmaceutical companies, and one author was an employee of Technogym. No other conflicts of interest were declared.
SOURCE: Balducci S et al. JAMA. 2019;321:880-90.
FROM JAMA
Teledermatology can increase efficiency
WASHINGTON – , according to a retrospective study presented at the annual meeting of the American Academy of Dermatology
Investigators previously have found that teledermatology systems, used by dermatologists to triage and manage patients, do improve patient access. Analyses of the clinical efficiency of these systems have demonstrated mixed results, however, and few such studies have been conducted in large, closed health care settings such as VA and county hospitals.
To investigate these open questions, Adam Zakaria, a third-year medical student at the University of California, San Francisco, and colleagues created a direct efficiency measure to analyze the teledermatology system at Zuckerberg San Francisco General Hospital and Trauma Center (ZSFG), which was established in January 2015. ZSFG is a public safety net hospital that serves approximately 150,000 patients annually, according to Mr. Zakaria.
Before the teledermatology system was implemented, each patient seeking to consult a ZSFG dermatologist needed a referral from a primary care provider. Appointments were given on a first-come, first-served basis, “with little consideration for the acuity or the severity of the patient’s complaint,” Mr. Zakaria said at the meeting. Since the teledermatology system has been put in place, referring providers have submitted brief clinical histories and relevant photographs to the system. Once per week, a UCSF dermatology provider and three to four UCSF dermatology residents meet to review cases and decide whether patients can be treated by their primary care providers with recommendations from teledermatology, or whether they need to be seen in person at the dermatology clinic for further evaluation.
The investigators compared data for two patient cohorts: Patients scheduled for in-person clinic visits between June 2014 and December 2014 (the preteledermatology sample), and the second cohort, patients who were triaged through the teledermatology system between June 2017 and December 2017 and who only received a clinic appointment if they could not be managed by their referring provider with teledermatology recommendations (the postteledermatology sample). Data came from chart review, administrative record review, and records from the specialty care and diagnostics department at ZSFG.
Patient wait times for the live clinic and total patient cases handled per month were chosen as measures of accessibility. The measures of efficiency were the number of cases handled per dermatologist hour and the percentage of referrals managed without a live visit. Mr. Zakaria and colleagues performed two-tailed t-tests for each measure.
The analysis included 11,586 patients. Approximately 50% of the sample identified as nonwhite, approximately one-third of patients had a native language other than English, and more than three-quarters of patients had a form of public health insurance.
After the hospital implemented teledermatology, patient wait times decreased significantly (84.6 days vs. 6.7 days; P less than .001), total cases handled per month increased significantly (754 vs. 902; P = .008). In the postteledermatology period, 61.8% of teledermatology consults were handled without a live visit.
After the implementation of teledermatology, the number of cases handled per dermatologist hour increased from 2.27 to 2.63, which was statistically significant (P = .01). The total time that dermatologists spent reviewing teledermatology cases or seeing patients in the live dermatology clinic increased from 332 hours per month to 342 hours per month, an increase that was not statistically significant, however. When the researchers compared provider hours and resident hours, they again found no statistically significant difference.
The results indicate that “the benefits of teledermatology did carry over when applied in a large, closed health care setting,” said Mr. Zakaria. “Two future areas of investigation include evaluating the impact of teledermatology on the quality of resident education and assessing the costs and benefits that teledermatology imposes upon referring primary care providers.” Mr. Zakaria and his colleagues also are analyzing the costs of teledermatology.
SOURCE: Zakaria A et al. AAD 19, Abstract 10087.
WASHINGTON – , according to a retrospective study presented at the annual meeting of the American Academy of Dermatology
Investigators previously have found that teledermatology systems, used by dermatologists to triage and manage patients, do improve patient access. Analyses of the clinical efficiency of these systems have demonstrated mixed results, however, and few such studies have been conducted in large, closed health care settings such as VA and county hospitals.
To investigate these open questions, Adam Zakaria, a third-year medical student at the University of California, San Francisco, and colleagues created a direct efficiency measure to analyze the teledermatology system at Zuckerberg San Francisco General Hospital and Trauma Center (ZSFG), which was established in January 2015. ZSFG is a public safety net hospital that serves approximately 150,000 patients annually, according to Mr. Zakaria.
Before the teledermatology system was implemented, each patient seeking to consult a ZSFG dermatologist needed a referral from a primary care provider. Appointments were given on a first-come, first-served basis, “with little consideration for the acuity or the severity of the patient’s complaint,” Mr. Zakaria said at the meeting. Since the teledermatology system has been put in place, referring providers have submitted brief clinical histories and relevant photographs to the system. Once per week, a UCSF dermatology provider and three to four UCSF dermatology residents meet to review cases and decide whether patients can be treated by their primary care providers with recommendations from teledermatology, or whether they need to be seen in person at the dermatology clinic for further evaluation.
The investigators compared data for two patient cohorts: Patients scheduled for in-person clinic visits between June 2014 and December 2014 (the preteledermatology sample), and the second cohort, patients who were triaged through the teledermatology system between June 2017 and December 2017 and who only received a clinic appointment if they could not be managed by their referring provider with teledermatology recommendations (the postteledermatology sample). Data came from chart review, administrative record review, and records from the specialty care and diagnostics department at ZSFG.
Patient wait times for the live clinic and total patient cases handled per month were chosen as measures of accessibility. The measures of efficiency were the number of cases handled per dermatologist hour and the percentage of referrals managed without a live visit. Mr. Zakaria and colleagues performed two-tailed t-tests for each measure.
The analysis included 11,586 patients. Approximately 50% of the sample identified as nonwhite, approximately one-third of patients had a native language other than English, and more than three-quarters of patients had a form of public health insurance.
After the hospital implemented teledermatology, patient wait times decreased significantly (84.6 days vs. 6.7 days; P less than .001), total cases handled per month increased significantly (754 vs. 902; P = .008). In the postteledermatology period, 61.8% of teledermatology consults were handled without a live visit.
After the implementation of teledermatology, the number of cases handled per dermatologist hour increased from 2.27 to 2.63, which was statistically significant (P = .01). The total time that dermatologists spent reviewing teledermatology cases or seeing patients in the live dermatology clinic increased from 332 hours per month to 342 hours per month, an increase that was not statistically significant, however. When the researchers compared provider hours and resident hours, they again found no statistically significant difference.
The results indicate that “the benefits of teledermatology did carry over when applied in a large, closed health care setting,” said Mr. Zakaria. “Two future areas of investigation include evaluating the impact of teledermatology on the quality of resident education and assessing the costs and benefits that teledermatology imposes upon referring primary care providers.” Mr. Zakaria and his colleagues also are analyzing the costs of teledermatology.
SOURCE: Zakaria A et al. AAD 19, Abstract 10087.
WASHINGTON – , according to a retrospective study presented at the annual meeting of the American Academy of Dermatology
Investigators previously have found that teledermatology systems, used by dermatologists to triage and manage patients, do improve patient access. Analyses of the clinical efficiency of these systems have demonstrated mixed results, however, and few such studies have been conducted in large, closed health care settings such as VA and county hospitals.
To investigate these open questions, Adam Zakaria, a third-year medical student at the University of California, San Francisco, and colleagues created a direct efficiency measure to analyze the teledermatology system at Zuckerberg San Francisco General Hospital and Trauma Center (ZSFG), which was established in January 2015. ZSFG is a public safety net hospital that serves approximately 150,000 patients annually, according to Mr. Zakaria.
Before the teledermatology system was implemented, each patient seeking to consult a ZSFG dermatologist needed a referral from a primary care provider. Appointments were given on a first-come, first-served basis, “with little consideration for the acuity or the severity of the patient’s complaint,” Mr. Zakaria said at the meeting. Since the teledermatology system has been put in place, referring providers have submitted brief clinical histories and relevant photographs to the system. Once per week, a UCSF dermatology provider and three to four UCSF dermatology residents meet to review cases and decide whether patients can be treated by their primary care providers with recommendations from teledermatology, or whether they need to be seen in person at the dermatology clinic for further evaluation.
The investigators compared data for two patient cohorts: Patients scheduled for in-person clinic visits between June 2014 and December 2014 (the preteledermatology sample), and the second cohort, patients who were triaged through the teledermatology system between June 2017 and December 2017 and who only received a clinic appointment if they could not be managed by their referring provider with teledermatology recommendations (the postteledermatology sample). Data came from chart review, administrative record review, and records from the specialty care and diagnostics department at ZSFG.
Patient wait times for the live clinic and total patient cases handled per month were chosen as measures of accessibility. The measures of efficiency were the number of cases handled per dermatologist hour and the percentage of referrals managed without a live visit. Mr. Zakaria and colleagues performed two-tailed t-tests for each measure.
The analysis included 11,586 patients. Approximately 50% of the sample identified as nonwhite, approximately one-third of patients had a native language other than English, and more than three-quarters of patients had a form of public health insurance.
After the hospital implemented teledermatology, patient wait times decreased significantly (84.6 days vs. 6.7 days; P less than .001), total cases handled per month increased significantly (754 vs. 902; P = .008). In the postteledermatology period, 61.8% of teledermatology consults were handled without a live visit.
After the implementation of teledermatology, the number of cases handled per dermatologist hour increased from 2.27 to 2.63, which was statistically significant (P = .01). The total time that dermatologists spent reviewing teledermatology cases or seeing patients in the live dermatology clinic increased from 332 hours per month to 342 hours per month, an increase that was not statistically significant, however. When the researchers compared provider hours and resident hours, they again found no statistically significant difference.
The results indicate that “the benefits of teledermatology did carry over when applied in a large, closed health care setting,” said Mr. Zakaria. “Two future areas of investigation include evaluating the impact of teledermatology on the quality of resident education and assessing the costs and benefits that teledermatology imposes upon referring primary care providers.” Mr. Zakaria and his colleagues also are analyzing the costs of teledermatology.
SOURCE: Zakaria A et al. AAD 19, Abstract 10087.
REPORTING FROM AAD 19
Report: Cutting sodium consumption recommended
according to a report outlining the first-ever Dietary Reference Intakes (DRIs) recommendation intended to address chronic disease risk.

For individuals aged 14 years and older consuming sodium above that level, cutting back could reduce their risk for hypertension and other chronic diseases, according to the report from the National Academies of Sciences, Engineering, and Medicine.
That cutoff, referred to as a Chronic Disease Risk Reduction Intake (CDRR), represents an expansion of the DRIs model beyond the Recommended Dietary Allowance (RDA) and other measures of adequacy, and the Tolerable Upper Intake Level (UL), which is the maximum intake unlikely to result in adverse health effects, a report author said in a press conference.
“CDRR is a level now that will join all the rest of the alphabet soup and be a part of how we describe recommended dietary intakes,” said Virginia A. Stallings, MD, chair of the committee that reviewed the sodium and potassium DRIs. Most U.S. adults are already consuming sodium above the recommended CDRR, said Dr. Stallings, who is a professor of pediatrics at the University of Pennsylvania, Philadelphia, and the director of the Nutrition Center at Children’s Hospital of Philadelphia.
The recommendation to reduce sodium intakes to below 2,300 mg/day applies to both hypertensive and normotensive individuals, and it could be particularly beneficial in older adults, non-Hispanic blacks, and other groups at higher risk of cardiovascular disease, Dr. Stallings and her coauthors of the new report wrote. The DRIs established in 2005 for both sodium and potassium are also updated based on new methodology in this report
Lower sodium CDRRs were set for younger individuals. Children aged 1-3 years should cut back if sodium intake is above 1,200 mg/day, while the levels for children aged 4-8 years and 9-13 years were set at 1,500 and 1,800 mg/day, respectively, according to the report.
By contrast, authors of this report were unable to establish a CDRR level for potassium based on current evidence. However, that doesn’t rule out the possibility that changing potassium intake could be beneficial, they suggested, adding that the effects of potassium need to be further explored.
Sodium and potassium play important roles in maintaining physiologic homeostasis, and they have also been implicated in risk of cardiovascular disease, mainly through their effects on blood pressure, and other chronic diseases.
“The unique nature of potassium and sodium – that is, the coexistence of their essentiality with a relationship to adverse health effects, including chronic disease risk – necessitated a new approach to the review of intake recommendations for these nutrients within the [DRI] context,” the report reads. The report also affirms, and in some cases revises, levels of sodium and potassium assumed to be adequate in healthy individuals that had been established in 2005. The sodium Adequate Intake (AI) levels for individuals aged 14-50 years is unchanged at 1,500 mg daily, but that for individuals aged 51 years and older has been increased to the 1,500-mg level.
“As we examined the evidence and looked specifically at those age cuts, there was no evidence that older people needed less sodium,” Dr. Stallings said in the press conference.
Potassium AIs were decreased for most age groups. For adults, the new recommended potassium AIs are 3,400 mg/day in men and 2,600 mg/day in women, whereas the AI for potassium was 4,700 mg/day for all adults in the 2005 recommendations.
In 2005, much of the evidence used to establish the potassium AI values was based on research studies that included potassium supplementation, rather than simply potassium intake in the usual diet. “In our process, we did not use supplementation studies, but we used the intake of apparently healthy people,” Dr. Stallings said in the press conference.
Less than half of U.S. and Canadian adults have potassium intakes that meet or exceed the potassium AI, with intakes lowest among non-Hispanic blacks, Dr. Stallings said in the press conference.
Dietary potassium intake is related to fruit and vegetable consumption, which rarely meets the recommended servings per day, Dr. Stallings and her colleagues wrote in a preface to the National Academies report. Milk, white potatoes, and fruit are higher sources of dietary potassium, she said, while coffee is the leading source of potassium for Americans aged 51 years and older.
By contrast, most sodium in the modern diet comes from commercially prepared foods and beverages, instead of consumers adding salt at the time of cooking or eating, Dr. Stallings wrote.
“For the desired public health benefit of reduced sodium intake to be achieved, more attention must be paid by industry to reducing sodium in the food supply and by consumers who have the needed sodium content information and an understanding of how to make health-inspired food choices,” they wrote in the report.
The American Heart Association’s CEO, Nancy Brown, expressed her support for the new recommendation for sodium intake. The recommendation “aligns with what the American Heart Association and other prominent public health organizations have been saying for years: We must eat less salt,” she said.
“Our excessive sodium intake isn’t entirely driven by the salt shaker; it’s largely controlled by the food industry. More than 70 percent of sodium consumed is added to food before it reaches our plates. It is added in restaurants and during the manufacturing of processed and prepackaged foods,” she claimed. “We hope this report encourages the Food and Drug Administration to quickly release its voluntary sodium reduction targets for the food industry. School leaders should also take note and reject the recent U.S. Department of Agriculture decision to weaken sodium standards in school meals and continue their commitment to serve students healthier foods.”
The DRIs report on sodium and potassium was supported by contracts between the National Academy of Sciences and the Centers for Disease Control, Food and Drug Administration, Health Canada, National Institutes of Health, Public Health Agency of Canada, and the Department of Agriculture. Partial support also came from the National Academy of Sciences W. K. Kellogg Foundation Fund and the National Academy of Medicine.
SOURCE: National Academies of Sciences, Engineering, and Medicine. 2019. Dietary Reference Intakes for sodium and potassium. Washington: The National Academies Press. doi: 10.17226/25353.
according to a report outlining the first-ever Dietary Reference Intakes (DRIs) recommendation intended to address chronic disease risk.
For individuals aged 14 years and older consuming sodium above that level, cutting back could reduce their risk for hypertension and other chronic diseases, according to the report from the National Academies of Sciences, Engineering, and Medicine.
That cutoff, referred to as a Chronic Disease Risk Reduction Intake (CDRR), represents an expansion of the DRIs model beyond the Recommended Dietary Allowance (RDA) and other measures of adequacy, and the Tolerable Upper Intake Level (UL), which is the maximum intake unlikely to result in adverse health effects, a report author said in a press conference.
“CDRR is a level now that will join all the rest of the alphabet soup and be a part of how we describe recommended dietary intakes,” said Virginia A. Stallings, MD, chair of the committee that reviewed the sodium and potassium DRIs. Most U.S. adults are already consuming sodium above the recommended CDRR, said Dr. Stallings, who is a professor of pediatrics at the University of Pennsylvania, Philadelphia, and the director of the Nutrition Center at Children’s Hospital of Philadelphia.
The recommendation to reduce sodium intakes to below 2,300 mg/day applies to both hypertensive and normotensive individuals, and it could be particularly beneficial in older adults, non-Hispanic blacks, and other groups at higher risk of cardiovascular disease, Dr. Stallings and her coauthors of the new report wrote. The DRIs established in 2005 for both sodium and potassium are also updated based on new methodology in this report
Lower sodium CDRRs were set for younger individuals. Children aged 1-3 years should cut back if sodium intake is above 1,200 mg/day, while the levels for children aged 4-8 years and 9-13 years were set at 1,500 and 1,800 mg/day, respectively, according to the report.
By contrast, authors of this report were unable to establish a CDRR level for potassium based on current evidence. However, that doesn’t rule out the possibility that changing potassium intake could be beneficial, they suggested, adding that the effects of potassium need to be further explored.
Sodium and potassium play important roles in maintaining physiologic homeostasis, and they have also been implicated in risk of cardiovascular disease, mainly through their effects on blood pressure, and other chronic diseases.
“The unique nature of potassium and sodium – that is, the coexistence of their essentiality with a relationship to adverse health effects, including chronic disease risk – necessitated a new approach to the review of intake recommendations for these nutrients within the [DRI] context,” the report reads. The report also affirms, and in some cases revises, levels of sodium and potassium assumed to be adequate in healthy individuals that had been established in 2005. The sodium Adequate Intake (AI) levels for individuals aged 14-50 years is unchanged at 1,500 mg daily, but that for individuals aged 51 years and older has been increased to the 1,500-mg level.
“As we examined the evidence and looked specifically at those age cuts, there was no evidence that older people needed less sodium,” Dr. Stallings said in the press conference.
Potassium AIs were decreased for most age groups. For adults, the new recommended potassium AIs are 3,400 mg/day in men and 2,600 mg/day in women, whereas the AI for potassium was 4,700 mg/day for all adults in the 2005 recommendations.
In 2005, much of the evidence used to establish the potassium AI values was based on research studies that included potassium supplementation, rather than simply potassium intake in the usual diet. “In our process, we did not use supplementation studies, but we used the intake of apparently healthy people,” Dr. Stallings said in the press conference.
Less than half of U.S. and Canadian adults have potassium intakes that meet or exceed the potassium AI, with intakes lowest among non-Hispanic blacks, Dr. Stallings said in the press conference.
Dietary potassium intake is related to fruit and vegetable consumption, which rarely meets the recommended servings per day, Dr. Stallings and her colleagues wrote in a preface to the National Academies report. Milk, white potatoes, and fruit are higher sources of dietary potassium, she said, while coffee is the leading source of potassium for Americans aged 51 years and older.
By contrast, most sodium in the modern diet comes from commercially prepared foods and beverages, instead of consumers adding salt at the time of cooking or eating, Dr. Stallings wrote.
“For the desired public health benefit of reduced sodium intake to be achieved, more attention must be paid by industry to reducing sodium in the food supply and by consumers who have the needed sodium content information and an understanding of how to make health-inspired food choices,” they wrote in the report.
The American Heart Association’s CEO, Nancy Brown, expressed her support for the new recommendation for sodium intake. The recommendation “aligns with what the American Heart Association and other prominent public health organizations have been saying for years: We must eat less salt,” she said.
“Our excessive sodium intake isn’t entirely driven by the salt shaker; it’s largely controlled by the food industry. More than 70 percent of sodium consumed is added to food before it reaches our plates. It is added in restaurants and during the manufacturing of processed and prepackaged foods,” she claimed. “We hope this report encourages the Food and Drug Administration to quickly release its voluntary sodium reduction targets for the food industry. School leaders should also take note and reject the recent U.S. Department of Agriculture decision to weaken sodium standards in school meals and continue their commitment to serve students healthier foods.”
The DRIs report on sodium and potassium was supported by contracts between the National Academy of Sciences and the Centers for Disease Control, Food and Drug Administration, Health Canada, National Institutes of Health, Public Health Agency of Canada, and the Department of Agriculture. Partial support also came from the National Academy of Sciences W. K. Kellogg Foundation Fund and the National Academy of Medicine.
SOURCE: National Academies of Sciences, Engineering, and Medicine. 2019. Dietary Reference Intakes for sodium and potassium. Washington: The National Academies Press. doi: 10.17226/25353.
according to a report outlining the first-ever Dietary Reference Intakes (DRIs) recommendation intended to address chronic disease risk.
For individuals aged 14 years and older consuming sodium above that level, cutting back could reduce their risk for hypertension and other chronic diseases, according to the report from the National Academies of Sciences, Engineering, and Medicine.
That cutoff, referred to as a Chronic Disease Risk Reduction Intake (CDRR), represents an expansion of the DRIs model beyond the Recommended Dietary Allowance (RDA) and other measures of adequacy, and the Tolerable Upper Intake Level (UL), which is the maximum intake unlikely to result in adverse health effects, a report author said in a press conference.
“CDRR is a level now that will join all the rest of the alphabet soup and be a part of how we describe recommended dietary intakes,” said Virginia A. Stallings, MD, chair of the committee that reviewed the sodium and potassium DRIs. Most U.S. adults are already consuming sodium above the recommended CDRR, said Dr. Stallings, who is a professor of pediatrics at the University of Pennsylvania, Philadelphia, and the director of the Nutrition Center at Children’s Hospital of Philadelphia.
The recommendation to reduce sodium intakes to below 2,300 mg/day applies to both hypertensive and normotensive individuals, and it could be particularly beneficial in older adults, non-Hispanic blacks, and other groups at higher risk of cardiovascular disease, Dr. Stallings and her coauthors of the new report wrote. The DRIs established in 2005 for both sodium and potassium are also updated based on new methodology in this report
Lower sodium CDRRs were set for younger individuals. Children aged 1-3 years should cut back if sodium intake is above 1,200 mg/day, while the levels for children aged 4-8 years and 9-13 years were set at 1,500 and 1,800 mg/day, respectively, according to the report.
By contrast, authors of this report were unable to establish a CDRR level for potassium based on current evidence. However, that doesn’t rule out the possibility that changing potassium intake could be beneficial, they suggested, adding that the effects of potassium need to be further explored.
Sodium and potassium play important roles in maintaining physiologic homeostasis, and they have also been implicated in risk of cardiovascular disease, mainly through their effects on blood pressure, and other chronic diseases.
“The unique nature of potassium and sodium – that is, the coexistence of their essentiality with a relationship to adverse health effects, including chronic disease risk – necessitated a new approach to the review of intake recommendations for these nutrients within the [DRI] context,” the report reads. The report also affirms, and in some cases revises, levels of sodium and potassium assumed to be adequate in healthy individuals that had been established in 2005. The sodium Adequate Intake (AI) levels for individuals aged 14-50 years is unchanged at 1,500 mg daily, but that for individuals aged 51 years and older has been increased to the 1,500-mg level.
“As we examined the evidence and looked specifically at those age cuts, there was no evidence that older people needed less sodium,” Dr. Stallings said in the press conference.
Potassium AIs were decreased for most age groups. For adults, the new recommended potassium AIs are 3,400 mg/day in men and 2,600 mg/day in women, whereas the AI for potassium was 4,700 mg/day for all adults in the 2005 recommendations.
In 2005, much of the evidence used to establish the potassium AI values was based on research studies that included potassium supplementation, rather than simply potassium intake in the usual diet. “In our process, we did not use supplementation studies, but we used the intake of apparently healthy people,” Dr. Stallings said in the press conference.
Less than half of U.S. and Canadian adults have potassium intakes that meet or exceed the potassium AI, with intakes lowest among non-Hispanic blacks, Dr. Stallings said in the press conference.
Dietary potassium intake is related to fruit and vegetable consumption, which rarely meets the recommended servings per day, Dr. Stallings and her colleagues wrote in a preface to the National Academies report. Milk, white potatoes, and fruit are higher sources of dietary potassium, she said, while coffee is the leading source of potassium for Americans aged 51 years and older.
By contrast, most sodium in the modern diet comes from commercially prepared foods and beverages, instead of consumers adding salt at the time of cooking or eating, Dr. Stallings wrote.
“For the desired public health benefit of reduced sodium intake to be achieved, more attention must be paid by industry to reducing sodium in the food supply and by consumers who have the needed sodium content information and an understanding of how to make health-inspired food choices,” they wrote in the report.
The American Heart Association’s CEO, Nancy Brown, expressed her support for the new recommendation for sodium intake. The recommendation “aligns with what the American Heart Association and other prominent public health organizations have been saying for years: We must eat less salt,” she said.
“Our excessive sodium intake isn’t entirely driven by the salt shaker; it’s largely controlled by the food industry. More than 70 percent of sodium consumed is added to food before it reaches our plates. It is added in restaurants and during the manufacturing of processed and prepackaged foods,” she claimed. “We hope this report encourages the Food and Drug Administration to quickly release its voluntary sodium reduction targets for the food industry. School leaders should also take note and reject the recent U.S. Department of Agriculture decision to weaken sodium standards in school meals and continue their commitment to serve students healthier foods.”
The DRIs report on sodium and potassium was supported by contracts between the National Academy of Sciences and the Centers for Disease Control, Food and Drug Administration, Health Canada, National Institutes of Health, Public Health Agency of Canada, and the Department of Agriculture. Partial support also came from the National Academy of Sciences W. K. Kellogg Foundation Fund and the National Academy of Medicine.
SOURCE: National Academies of Sciences, Engineering, and Medicine. 2019. Dietary Reference Intakes for sodium and potassium. Washington: The National Academies Press. doi: 10.17226/25353.
Food allergies and atopic dermatitis: What is the evidence?
WASHINGTON – The and brings up an interesting discussion, Peter Lio, MD, said in a video interview at the annual meeting of the American Academy of Dermatology.
Patients are often convinced that food is the main driver of their AD, or parents believe it is a trigger in their children with AD, according to Dr. Lio of the departments of dermatology and pediatrics at Northwestern University, Chicago.

There is an increased risk of true food allergy in patients with AD, which “seems to get worse with increasing severity of the disease,” he pointed out. However, he added, many patients believe that food allergy is what is driving their eczema, “and that’s the part we don’t really think bears out” in clinical trials.
In the interview, Dr. Lio reviewed some of the clinical trial data and discussed other issues, including foods that seem to have an inflammatory effect in the body, the concepts of “transcutaneous sensitization” in children with AD and the “leaky gut,” and why he tends to recommend probiotics for patients with AD.
Dr. Lio spoke on diet and AD during a session titled “Dietary Triggers and Modifications of Common Dermatologic Conditions – An Evidence Based Approach,” at the meeting, He had no relevant disclosures.
WASHINGTON – The and brings up an interesting discussion, Peter Lio, MD, said in a video interview at the annual meeting of the American Academy of Dermatology.
Patients are often convinced that food is the main driver of their AD, or parents believe it is a trigger in their children with AD, according to Dr. Lio of the departments of dermatology and pediatrics at Northwestern University, Chicago.
There is an increased risk of true food allergy in patients with AD, which “seems to get worse with increasing severity of the disease,” he pointed out. However, he added, many patients believe that food allergy is what is driving their eczema, “and that’s the part we don’t really think bears out” in clinical trials.
In the interview, Dr. Lio reviewed some of the clinical trial data and discussed other issues, including foods that seem to have an inflammatory effect in the body, the concepts of “transcutaneous sensitization” in children with AD and the “leaky gut,” and why he tends to recommend probiotics for patients with AD.
Dr. Lio spoke on diet and AD during a session titled “Dietary Triggers and Modifications of Common Dermatologic Conditions – An Evidence Based Approach,” at the meeting, He had no relevant disclosures.
WASHINGTON – The and brings up an interesting discussion, Peter Lio, MD, said in a video interview at the annual meeting of the American Academy of Dermatology.
Patients are often convinced that food is the main driver of their AD, or parents believe it is a trigger in their children with AD, according to Dr. Lio of the departments of dermatology and pediatrics at Northwestern University, Chicago.
There is an increased risk of true food allergy in patients with AD, which “seems to get worse with increasing severity of the disease,” he pointed out. However, he added, many patients believe that food allergy is what is driving their eczema, “and that’s the part we don’t really think bears out” in clinical trials.
In the interview, Dr. Lio reviewed some of the clinical trial data and discussed other issues, including foods that seem to have an inflammatory effect in the body, the concepts of “transcutaneous sensitization” in children with AD and the “leaky gut,” and why he tends to recommend probiotics for patients with AD.
Dr. Lio spoke on diet and AD during a session titled “Dietary Triggers and Modifications of Common Dermatologic Conditions – An Evidence Based Approach,” at the meeting, He had no relevant disclosures.
REPORTING FROM AAD 2019
Groups of physicians produce more accurate diagnoses than individuals
Groups of physicians and trainees diagnose clinical cases with more accuracy than individuals, according to a study of solo and aggregate diagnoses collected through an online medical teaching platform.
“These findings suggest that using the concept of collective intelligence to pool many physicians’ diagnoses could be a scalable approach to improve diagnostic accuracy,” wrote lead author Michael L. Barnett, MD, of Harvard University in Boston and his coauthors, adding that “groups of all sizes outperformed individual subspecialists on cases in their own subspecialty.” The study was published online in JAMA Network Open.
This cross-sectional study examined 1,572 cases solved within the Human Diagnosis Project (Human Dx) system, an online platform for authoring and diagnosing teaching cases. The system presents real-life cases from clinical practices and asks respondents to generate ranked differential diagnoses. Cases are tagged for specialties based on both intended diagnoses and the top diagnoses chosen by respondents. All cases used in this study were authored between May 7, 2014, and October 5, 2016, and had 10 or more respondents.
Of the 2,069 attending physicians and fellows, residents, and medical students (users) who solved cases within the Human Dx system, 1,452 (70.2%) were trained in internal medicine, 1,228 (59.4%) were residents or fellows, 431 (20.8%) were attending physicians, and 410 (19.8%) were medical students. To create a collective differential, Dr. Barnett and his colleagues aggregated the responses of up to nine participants via a weighted combination of each clinician’s top three diagnoses, which they dubbed “collective intelligence.”
The diagnostic accuracy for groups of nine was 85.6% (95% confidence interval, 83.9%-87.4%), compared with individual users at 62.5% (95% CI, 60.1%-64.9%), a difference of 23% (95% CI, 14.9%-31.2%; P less than .001). Groups of five saw a 17.8% difference in accuracy versus an individual (95% CI, 14.0%-21.6%; P less than .001), compared with 12.5% for groups of two (95% CI, 9.3%-15.8%; P less than .001). Taken together, these seem to underline an association between larger groups and increased accuracy.
Individual specialists solved cases in their particular areas with a diagnostic accuracy of 66.3% (95% CI, 59.1%-73.5%), compared with nonmatched specialty accuracy of 63.9% (95% CI, 56.6%-71.2%). Groups, however, outperformed specialists across the board: 77.7% accuracy for a group of 2 (95% CI, 70.1%-84.6%; P less than .001) and 85.5% accuracy for a group of 9 (95% CI, 75.1%-95.9%; P less than .001).
The coauthors shared the limitations of their study, including the possibility that the users who contributed these cases to Human Dx may not be representative of the medical community as a whole. They also noted that, while their 431 attending physicians constituted the “largest number ... to date in a study of collective intelligence,” trainees still made up almost 80% of users. In addition, they acknowledged that Human Dx was not designed to generate collective diagnoses nor assess collective intelligence; another platform created with that ability in mind may have returned different results. Finally, they were unable to assess how exactly greater accuracy would have been linked to changes in treatment, calling it “an important question for future work.”
The authors disclosed several conflicts of interest. One doctor reported receiving personal fees from Greylock McKinnon Associates; another reported receiving personal fees from the Human Diagnosis Project and serving as their nonprofit director during the study. A third doctor reported consulting for a company that makes patient-safety monitoring systems and receiving compensation from a not-for-profit incubator, along with having equity in three medical data and software companies.
SOURCE: Barnett ML et al. JAMA Netw Open. 2019 Mar 1. doi: 10.1001/jamanetworkopen.2019.0096.
Although this study from Barnett et al. is not the silver bullet for misdiagnosis, better understanding why physicians make mistakes is a necessary and valuable undertaking, according to Stephan D. Fihn, MD, of the University of Washington, Seattle.
In the past, the “correct” diagnostic approach included making a list of potential diagnoses and systematically ruling them out one by one, a process conveyed via clinicopathologic conferences in teaching hospitals. These, Dr. Fihn recalled, lasted until medical educators recognized them as “more ... theatrical events than meaningful teaching exercises” and understood that master clinicians did not actually think in the manner this approach modeled. Since then, the maturation of cognitive psychology and “a growing literature” have made diagnostic error seem like a common, sometimes unavoidable element of being human.
What can be done? Computers have always been a possibility, but “none have achieved the breadth of content and accuracy necessary to be adopted to any great extent,” Dr. Fihn wrote. Another option is crowdsourcing, as described in this study from Barnett and colleagues. Their approach has its pitfalls: A 62.5% level of diagnostic accuracy from individuals is not very high, which suggests either difficult cases or a preponderance of inexperienced clinicians who may benefit from collective intelligence even more. Regardless, he stated, “clinicians need to be cognizant of their own inherent limitations and acknowledge fallibility”; being humble and willing to seek advice “remain important, albeit imperfect, antidotes to misdiagnosis.”
These comments are adapted from an accompanying editorial (JAMA Netw Open. 2019 Mar 1. doi: 10.1001/jamanetworkopen.2019.1071 ). No conflicts of interest were reported.
Although this study from Barnett et al. is not the silver bullet for misdiagnosis, better understanding why physicians make mistakes is a necessary and valuable undertaking, according to Stephan D. Fihn, MD, of the University of Washington, Seattle.
In the past, the “correct” diagnostic approach included making a list of potential diagnoses and systematically ruling them out one by one, a process conveyed via clinicopathologic conferences in teaching hospitals. These, Dr. Fihn recalled, lasted until medical educators recognized them as “more ... theatrical events than meaningful teaching exercises” and understood that master clinicians did not actually think in the manner this approach modeled. Since then, the maturation of cognitive psychology and “a growing literature” have made diagnostic error seem like a common, sometimes unavoidable element of being human.
What can be done? Computers have always been a possibility, but “none have achieved the breadth of content and accuracy necessary to be adopted to any great extent,” Dr. Fihn wrote. Another option is crowdsourcing, as described in this study from Barnett and colleagues. Their approach has its pitfalls: A 62.5% level of diagnostic accuracy from individuals is not very high, which suggests either difficult cases or a preponderance of inexperienced clinicians who may benefit from collective intelligence even more. Regardless, he stated, “clinicians need to be cognizant of their own inherent limitations and acknowledge fallibility”; being humble and willing to seek advice “remain important, albeit imperfect, antidotes to misdiagnosis.”
These comments are adapted from an accompanying editorial (JAMA Netw Open. 2019 Mar 1. doi: 10.1001/jamanetworkopen.2019.1071 ). No conflicts of interest were reported.
Although this study from Barnett et al. is not the silver bullet for misdiagnosis, better understanding why physicians make mistakes is a necessary and valuable undertaking, according to Stephan D. Fihn, MD, of the University of Washington, Seattle.
In the past, the “correct” diagnostic approach included making a list of potential diagnoses and systematically ruling them out one by one, a process conveyed via clinicopathologic conferences in teaching hospitals. These, Dr. Fihn recalled, lasted until medical educators recognized them as “more ... theatrical events than meaningful teaching exercises” and understood that master clinicians did not actually think in the manner this approach modeled. Since then, the maturation of cognitive psychology and “a growing literature” have made diagnostic error seem like a common, sometimes unavoidable element of being human.
What can be done? Computers have always been a possibility, but “none have achieved the breadth of content and accuracy necessary to be adopted to any great extent,” Dr. Fihn wrote. Another option is crowdsourcing, as described in this study from Barnett and colleagues. Their approach has its pitfalls: A 62.5% level of diagnostic accuracy from individuals is not very high, which suggests either difficult cases or a preponderance of inexperienced clinicians who may benefit from collective intelligence even more. Regardless, he stated, “clinicians need to be cognizant of their own inherent limitations and acknowledge fallibility”; being humble and willing to seek advice “remain important, albeit imperfect, antidotes to misdiagnosis.”
These comments are adapted from an accompanying editorial (JAMA Netw Open. 2019 Mar 1. doi: 10.1001/jamanetworkopen.2019.1071 ). No conflicts of interest were reported.
Groups of physicians and trainees diagnose clinical cases with more accuracy than individuals, according to a study of solo and aggregate diagnoses collected through an online medical teaching platform.
“These findings suggest that using the concept of collective intelligence to pool many physicians’ diagnoses could be a scalable approach to improve diagnostic accuracy,” wrote lead author Michael L. Barnett, MD, of Harvard University in Boston and his coauthors, adding that “groups of all sizes outperformed individual subspecialists on cases in their own subspecialty.” The study was published online in JAMA Network Open.
This cross-sectional study examined 1,572 cases solved within the Human Diagnosis Project (Human Dx) system, an online platform for authoring and diagnosing teaching cases. The system presents real-life cases from clinical practices and asks respondents to generate ranked differential diagnoses. Cases are tagged for specialties based on both intended diagnoses and the top diagnoses chosen by respondents. All cases used in this study were authored between May 7, 2014, and October 5, 2016, and had 10 or more respondents.
Of the 2,069 attending physicians and fellows, residents, and medical students (users) who solved cases within the Human Dx system, 1,452 (70.2%) were trained in internal medicine, 1,228 (59.4%) were residents or fellows, 431 (20.8%) were attending physicians, and 410 (19.8%) were medical students. To create a collective differential, Dr. Barnett and his colleagues aggregated the responses of up to nine participants via a weighted combination of each clinician’s top three diagnoses, which they dubbed “collective intelligence.”
The diagnostic accuracy for groups of nine was 85.6% (95% confidence interval, 83.9%-87.4%), compared with individual users at 62.5% (95% CI, 60.1%-64.9%), a difference of 23% (95% CI, 14.9%-31.2%; P less than .001). Groups of five saw a 17.8% difference in accuracy versus an individual (95% CI, 14.0%-21.6%; P less than .001), compared with 12.5% for groups of two (95% CI, 9.3%-15.8%; P less than .001). Taken together, these seem to underline an association between larger groups and increased accuracy.
Individual specialists solved cases in their particular areas with a diagnostic accuracy of 66.3% (95% CI, 59.1%-73.5%), compared with nonmatched specialty accuracy of 63.9% (95% CI, 56.6%-71.2%). Groups, however, outperformed specialists across the board: 77.7% accuracy for a group of 2 (95% CI, 70.1%-84.6%; P less than .001) and 85.5% accuracy for a group of 9 (95% CI, 75.1%-95.9%; P less than .001).
The coauthors shared the limitations of their study, including the possibility that the users who contributed these cases to Human Dx may not be representative of the medical community as a whole. They also noted that, while their 431 attending physicians constituted the “largest number ... to date in a study of collective intelligence,” trainees still made up almost 80% of users. In addition, they acknowledged that Human Dx was not designed to generate collective diagnoses nor assess collective intelligence; another platform created with that ability in mind may have returned different results. Finally, they were unable to assess how exactly greater accuracy would have been linked to changes in treatment, calling it “an important question for future work.”
The authors disclosed several conflicts of interest. One doctor reported receiving personal fees from Greylock McKinnon Associates; another reported receiving personal fees from the Human Diagnosis Project and serving as their nonprofit director during the study. A third doctor reported consulting for a company that makes patient-safety monitoring systems and receiving compensation from a not-for-profit incubator, along with having equity in three medical data and software companies.
SOURCE: Barnett ML et al. JAMA Netw Open. 2019 Mar 1. doi: 10.1001/jamanetworkopen.2019.0096.
Groups of physicians and trainees diagnose clinical cases with more accuracy than individuals, according to a study of solo and aggregate diagnoses collected through an online medical teaching platform.
“These findings suggest that using the concept of collective intelligence to pool many physicians’ diagnoses could be a scalable approach to improve diagnostic accuracy,” wrote lead author Michael L. Barnett, MD, of Harvard University in Boston and his coauthors, adding that “groups of all sizes outperformed individual subspecialists on cases in their own subspecialty.” The study was published online in JAMA Network Open.
This cross-sectional study examined 1,572 cases solved within the Human Diagnosis Project (Human Dx) system, an online platform for authoring and diagnosing teaching cases. The system presents real-life cases from clinical practices and asks respondents to generate ranked differential diagnoses. Cases are tagged for specialties based on both intended diagnoses and the top diagnoses chosen by respondents. All cases used in this study were authored between May 7, 2014, and October 5, 2016, and had 10 or more respondents.
Of the 2,069 attending physicians and fellows, residents, and medical students (users) who solved cases within the Human Dx system, 1,452 (70.2%) were trained in internal medicine, 1,228 (59.4%) were residents or fellows, 431 (20.8%) were attending physicians, and 410 (19.8%) were medical students. To create a collective differential, Dr. Barnett and his colleagues aggregated the responses of up to nine participants via a weighted combination of each clinician’s top three diagnoses, which they dubbed “collective intelligence.”
The diagnostic accuracy for groups of nine was 85.6% (95% confidence interval, 83.9%-87.4%), compared with individual users at 62.5% (95% CI, 60.1%-64.9%), a difference of 23% (95% CI, 14.9%-31.2%; P less than .001). Groups of five saw a 17.8% difference in accuracy versus an individual (95% CI, 14.0%-21.6%; P less than .001), compared with 12.5% for groups of two (95% CI, 9.3%-15.8%; P less than .001). Taken together, these seem to underline an association between larger groups and increased accuracy.
Individual specialists solved cases in their particular areas with a diagnostic accuracy of 66.3% (95% CI, 59.1%-73.5%), compared with nonmatched specialty accuracy of 63.9% (95% CI, 56.6%-71.2%). Groups, however, outperformed specialists across the board: 77.7% accuracy for a group of 2 (95% CI, 70.1%-84.6%; P less than .001) and 85.5% accuracy for a group of 9 (95% CI, 75.1%-95.9%; P less than .001).
The coauthors shared the limitations of their study, including the possibility that the users who contributed these cases to Human Dx may not be representative of the medical community as a whole. They also noted that, while their 431 attending physicians constituted the “largest number ... to date in a study of collective intelligence,” trainees still made up almost 80% of users. In addition, they acknowledged that Human Dx was not designed to generate collective diagnoses nor assess collective intelligence; another platform created with that ability in mind may have returned different results. Finally, they were unable to assess how exactly greater accuracy would have been linked to changes in treatment, calling it “an important question for future work.”
The authors disclosed several conflicts of interest. One doctor reported receiving personal fees from Greylock McKinnon Associates; another reported receiving personal fees from the Human Diagnosis Project and serving as their nonprofit director during the study. A third doctor reported consulting for a company that makes patient-safety monitoring systems and receiving compensation from a not-for-profit incubator, along with having equity in three medical data and software companies.
SOURCE: Barnett ML et al. JAMA Netw Open. 2019 Mar 1. doi: 10.1001/jamanetworkopen.2019.0096.
FROM JAMA NETWORK OPEN
Erythematous Edematous Plaques on the Dorsal Aspects of the Hands
The Diagnosis: Phytophotodermatitis
Initially, there was concern for autoimmune or connective tissue disease because of the edematous plaques localized over sun-exposed regions of the hands with marked sparing of the knuckles. Lupus erythematosus (LE), mixed connective tissue disease, CREST (calcinosis, Raynaud phenomenon, esophageal motility disorders, sclerodactyly, telangiectasia) syndrome, dermatomyositis (DM), and erythromelalgia all were considered. Common disorders such as contact dermatitis and phytophotodermatitis remained in the differential diagnosis, though the patient adamantly denied any recent exposures. As part of the initial workup, laboratory studies including a complete blood cell count, comprehensive metabolic panel, serum lactate dehydrogenase, serum creatinine kinase, erythrocyte sedimentation rate, and an antinuclear antibody panel were performed. Additionally, a punch biopsy at the border of the lesion was performed.
Lupus erythematosus was considered given the patient’s age and sex and the photoexposed location of the plaques. The photosensitive rash of LE classically affects the dorsal aspects of the hands while sparing the interphalangeal joints.1,2 However, the patient had no nail fold findings consistent with systemic LE with no evidence of erythema or dilated tortuous vessels.3 Furthermore, there were no other cutaneous symptoms, and there was a negative review of systems, including malar/discoid rash, oral ulcers, photosensitivity, history of hematologic abnormalities, and end organ damage.4,5 A negative antinuclear antibody serologic panel combined with a negative review of systems made the diagnosis of LE less likely.
Given the presenting clinical appearance, DM also was considered. Dermatomyositis traditionally displays ragged cuticular dystrophy with nail fold telangiectasia, mechanic hands, and involvement of the dorsal aspects of the hands with violaceous accentuation of the knuckles.6 The patient reported pruritus, which is common among DM patients; however, the nail folds were unaffected.7 Finally, she demonstrated sparing rather than involvement of the knuckles, which would be an unlikely presentation for DM.6
CREST syndrome, systemic sclerosis, and syndromes with overlapping features such as mixed connective tissue disease also were considered. The cutaneous features of CREST syndrome are characterized by initial edema of the digits with a subsequent taut and shiny indurated phase. Flexion contractures, ulceration, tapering of the digits, and loss of cutaneous fat pads can progressively occur.8,9 Raynaud phenomenon is a common early finding in CREST syndrome or systemic sclerosis, and patients may develop ice pick digital infarcts and calcinosis in progressed disease.8 Common nail fold findings include periungual telangiectasia with dropout areas.10,11 The marked edema and white discoloration of the knuckles in this patient could be mistaken for Raynaud phenomenon; however, she lacked pain or cold sensitivity and her discoloration was static.12 Without sclerodermoid changes, nail fold findings, matted telangiectasia, taut skin, or systemic findings, a diagnosis of CREST syndrome, scleroderma, or other mixed connective tissue disease would be unlikely.8
Erythromelalgia is a clinical syndrome characterized by burning pain, erythema, and increased skin temperature that intermittently affects both the arms and legs. This rare disorder can be further classified into type 1 (associated with thrombocytopenia), type 2 (primary or idiopathic), and type 3 (associated with other medical cause excluding thrombocytopenia).1,13 The patient endorsed some discomfort from the lesions but denied any subjective feeling of burning pain or increased skin temperature. Additionally, she had no family history of inheritable skin disorders and no personal history of polycythemia. Consequently, erythromelalgia remained less likely on the differential diagnosis.
The histology of the acral skin revealed mild focal spongiosis with no increase in dermal mucin on colloidal iron or mucopolysaccharide stains (Figure). After receiving the biopsy results and additional questioning of the patient, it was discovered that 2 days prior to her initial presentation she had juiced numerous limes by hand and subsequently spent a long period of time outside with sunlight exposure. Upon discovery of this additional historical information, the diagnosis of phytophotodermatitis was made.
Phytophotodermatitis is an erythematous inflammatory reaction that occurs on the skin after exposure to a plant-derived photosensitizer followed by UVA light radiation.14 This phenomenon was first described by the ancient Egyptians as a treatment for vitiligo.1 The most common plant families that can cause this nonimmune cutaneous reaction include Apiaceae eg, hogweed, celery, dill, fennel) and Rutaceae (eg, citrus plants, rue).14 The psoralens or furocoumarins found in these plants bind loosely to DNA at their ground state but covalently bond to pyrimidine bases during photoexcitation with UVA, resulting in DNA damage and subsequent local inflammation.14 Given the patient’s clinical examination, pathology findings, and history, phytophotodermatitis secondary to lime juice exposure was confirmed. Two weeks after applying clobetasol ointment twice daily, the patient’s hands had returned to baseline with complete resolution of the erythematous lesions.
Although lime phytophotodermatitis is a routine diagnosis, this clinical case stands as an important reminder to demonstrate how common diseases can masquerade as more exotic cutaneous disorders. There often is a clinical desire to seek out more complicated diagnoses, particularly during residency training; however, this case reinforces the invaluable importance of collecting a thorough patient history, as it can ultimately minimize excessive testing and in some cases prevent unnecessary therapy.
- Bolognia JL, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. China:Elsevier Saunders; 2012.
- Uva L, Miguel D, Pinheiro C, et al. Cutaneous manifestations of systemiclupus erythematosus. Autoimmune Dis. 2012;2012:834291.
- Furtado R, Pucinelli M, Cristo V, et al. Scleroderma-like nailfold capillaroscopicabnormalities are associated with anti-U1-RNP antibodies and Raynaud’s phenomenon in SLE patients. Lupus. 2002;11:35-41.
- Wenzel J, Zahn S, Tuting T. Pathogenesis of cutaneous lupus erythematosus:common and different features in distinct subsets. Lupus. 2010;19:1020-1028.
- Avilés Izquierdo JA, Cano Martínez N, Lázaro Ochaita P. Epidemiologicalcharacteristics of patients with cutaneous lupus erythematosus.Actas Dermosifiliogr. 2014;105:69-73.
- Marvi U, Chung L, Fiorentino DF. Clinical presentation and evaluation of dermatomyositis. Indian J Dermatol. 2012;57:375-381.
- Shirani Z, Kucenic MJ, Carroll CL, et al. Pruritus in adult dermatomyositis. Clin Exp Dermatol. 2004;29:273-276.
- Krieg T, Takehara K. Skin disease: a cardinal feature of systemic sclerosis. Rheumatology (Oxford). 2009;48(suppl 3):14-18.
- Mizutani H, Mizutani T, Okada H, et al. Round fingerpad sign: an early sign of scleroderma. J Am Acad Dermatol. 1991;24:67-69.
- Baran R, Dawber RP, Haneke E, et al, eds. A Text Atlas of Nail Disorders Techniques in Investigation and Diagnosis. 3rd ed. Boca Raton, FL: CRC Press; 2005.
- Ghali FE, Stein LD, Fine J, et al. Gingival telangiectases: an underappreciated physical sign of juvenile dermatomyositis. Arch Dermatol. 1999;135:1370-1374.
- Grader-Beck T, Wigley FM. Raynaud’s phenomenon in mixed connective tissue disease. Rheum Dis Clin North Am. 2005;31:465-481.
- Davis MD, Weenig RH, Genebriera J, et al. Histopathologic findings in primary erythromelalgia are nonspecific: special studies show a decrease in small nerve fiber density. J Am Acad Dermatol. 2006;55:519-522.
- Sasseville D. Clinical patterns of phytophotodermatitis. Dermatol Clin. 2009;27:299-308.
The Diagnosis: Phytophotodermatitis
Initially, there was concern for autoimmune or connective tissue disease because of the edematous plaques localized over sun-exposed regions of the hands with marked sparing of the knuckles. Lupus erythematosus (LE), mixed connective tissue disease, CREST (calcinosis, Raynaud phenomenon, esophageal motility disorders, sclerodactyly, telangiectasia) syndrome, dermatomyositis (DM), and erythromelalgia all were considered. Common disorders such as contact dermatitis and phytophotodermatitis remained in the differential diagnosis, though the patient adamantly denied any recent exposures. As part of the initial workup, laboratory studies including a complete blood cell count, comprehensive metabolic panel, serum lactate dehydrogenase, serum creatinine kinase, erythrocyte sedimentation rate, and an antinuclear antibody panel were performed. Additionally, a punch biopsy at the border of the lesion was performed.
Lupus erythematosus was considered given the patient’s age and sex and the photoexposed location of the plaques. The photosensitive rash of LE classically affects the dorsal aspects of the hands while sparing the interphalangeal joints.1,2 However, the patient had no nail fold findings consistent with systemic LE with no evidence of erythema or dilated tortuous vessels.3 Furthermore, there were no other cutaneous symptoms, and there was a negative review of systems, including malar/discoid rash, oral ulcers, photosensitivity, history of hematologic abnormalities, and end organ damage.4,5 A negative antinuclear antibody serologic panel combined with a negative review of systems made the diagnosis of LE less likely.
Given the presenting clinical appearance, DM also was considered. Dermatomyositis traditionally displays ragged cuticular dystrophy with nail fold telangiectasia, mechanic hands, and involvement of the dorsal aspects of the hands with violaceous accentuation of the knuckles.6 The patient reported pruritus, which is common among DM patients; however, the nail folds were unaffected.7 Finally, she demonstrated sparing rather than involvement of the knuckles, which would be an unlikely presentation for DM.6
CREST syndrome, systemic sclerosis, and syndromes with overlapping features such as mixed connective tissue disease also were considered. The cutaneous features of CREST syndrome are characterized by initial edema of the digits with a subsequent taut and shiny indurated phase. Flexion contractures, ulceration, tapering of the digits, and loss of cutaneous fat pads can progressively occur.8,9 Raynaud phenomenon is a common early finding in CREST syndrome or systemic sclerosis, and patients may develop ice pick digital infarcts and calcinosis in progressed disease.8 Common nail fold findings include periungual telangiectasia with dropout areas.10,11 The marked edema and white discoloration of the knuckles in this patient could be mistaken for Raynaud phenomenon; however, she lacked pain or cold sensitivity and her discoloration was static.12 Without sclerodermoid changes, nail fold findings, matted telangiectasia, taut skin, or systemic findings, a diagnosis of CREST syndrome, scleroderma, or other mixed connective tissue disease would be unlikely.8
Erythromelalgia is a clinical syndrome characterized by burning pain, erythema, and increased skin temperature that intermittently affects both the arms and legs. This rare disorder can be further classified into type 1 (associated with thrombocytopenia), type 2 (primary or idiopathic), and type 3 (associated with other medical cause excluding thrombocytopenia).1,13 The patient endorsed some discomfort from the lesions but denied any subjective feeling of burning pain or increased skin temperature. Additionally, she had no family history of inheritable skin disorders and no personal history of polycythemia. Consequently, erythromelalgia remained less likely on the differential diagnosis.
The histology of the acral skin revealed mild focal spongiosis with no increase in dermal mucin on colloidal iron or mucopolysaccharide stains (Figure). After receiving the biopsy results and additional questioning of the patient, it was discovered that 2 days prior to her initial presentation she had juiced numerous limes by hand and subsequently spent a long period of time outside with sunlight exposure. Upon discovery of this additional historical information, the diagnosis of phytophotodermatitis was made.
Phytophotodermatitis is an erythematous inflammatory reaction that occurs on the skin after exposure to a plant-derived photosensitizer followed by UVA light radiation.14 This phenomenon was first described by the ancient Egyptians as a treatment for vitiligo.1 The most common plant families that can cause this nonimmune cutaneous reaction include Apiaceae eg, hogweed, celery, dill, fennel) and Rutaceae (eg, citrus plants, rue).14 The psoralens or furocoumarins found in these plants bind loosely to DNA at their ground state but covalently bond to pyrimidine bases during photoexcitation with UVA, resulting in DNA damage and subsequent local inflammation.14 Given the patient’s clinical examination, pathology findings, and history, phytophotodermatitis secondary to lime juice exposure was confirmed. Two weeks after applying clobetasol ointment twice daily, the patient’s hands had returned to baseline with complete resolution of the erythematous lesions.
Although lime phytophotodermatitis is a routine diagnosis, this clinical case stands as an important reminder to demonstrate how common diseases can masquerade as more exotic cutaneous disorders. There often is a clinical desire to seek out more complicated diagnoses, particularly during residency training; however, this case reinforces the invaluable importance of collecting a thorough patient history, as it can ultimately minimize excessive testing and in some cases prevent unnecessary therapy.
The Diagnosis: Phytophotodermatitis
Initially, there was concern for autoimmune or connective tissue disease because of the edematous plaques localized over sun-exposed regions of the hands with marked sparing of the knuckles. Lupus erythematosus (LE), mixed connective tissue disease, CREST (calcinosis, Raynaud phenomenon, esophageal motility disorders, sclerodactyly, telangiectasia) syndrome, dermatomyositis (DM), and erythromelalgia all were considered. Common disorders such as contact dermatitis and phytophotodermatitis remained in the differential diagnosis, though the patient adamantly denied any recent exposures. As part of the initial workup, laboratory studies including a complete blood cell count, comprehensive metabolic panel, serum lactate dehydrogenase, serum creatinine kinase, erythrocyte sedimentation rate, and an antinuclear antibody panel were performed. Additionally, a punch biopsy at the border of the lesion was performed.
Lupus erythematosus was considered given the patient’s age and sex and the photoexposed location of the plaques. The photosensitive rash of LE classically affects the dorsal aspects of the hands while sparing the interphalangeal joints.1,2 However, the patient had no nail fold findings consistent with systemic LE with no evidence of erythema or dilated tortuous vessels.3 Furthermore, there were no other cutaneous symptoms, and there was a negative review of systems, including malar/discoid rash, oral ulcers, photosensitivity, history of hematologic abnormalities, and end organ damage.4,5 A negative antinuclear antibody serologic panel combined with a negative review of systems made the diagnosis of LE less likely.
Given the presenting clinical appearance, DM also was considered. Dermatomyositis traditionally displays ragged cuticular dystrophy with nail fold telangiectasia, mechanic hands, and involvement of the dorsal aspects of the hands with violaceous accentuation of the knuckles.6 The patient reported pruritus, which is common among DM patients; however, the nail folds were unaffected.7 Finally, she demonstrated sparing rather than involvement of the knuckles, which would be an unlikely presentation for DM.6
CREST syndrome, systemic sclerosis, and syndromes with overlapping features such as mixed connective tissue disease also were considered. The cutaneous features of CREST syndrome are characterized by initial edema of the digits with a subsequent taut and shiny indurated phase. Flexion contractures, ulceration, tapering of the digits, and loss of cutaneous fat pads can progressively occur.8,9 Raynaud phenomenon is a common early finding in CREST syndrome or systemic sclerosis, and patients may develop ice pick digital infarcts and calcinosis in progressed disease.8 Common nail fold findings include periungual telangiectasia with dropout areas.10,11 The marked edema and white discoloration of the knuckles in this patient could be mistaken for Raynaud phenomenon; however, she lacked pain or cold sensitivity and her discoloration was static.12 Without sclerodermoid changes, nail fold findings, matted telangiectasia, taut skin, or systemic findings, a diagnosis of CREST syndrome, scleroderma, or other mixed connective tissue disease would be unlikely.8
Erythromelalgia is a clinical syndrome characterized by burning pain, erythema, and increased skin temperature that intermittently affects both the arms and legs. This rare disorder can be further classified into type 1 (associated with thrombocytopenia), type 2 (primary or idiopathic), and type 3 (associated with other medical cause excluding thrombocytopenia).1,13 The patient endorsed some discomfort from the lesions but denied any subjective feeling of burning pain or increased skin temperature. Additionally, she had no family history of inheritable skin disorders and no personal history of polycythemia. Consequently, erythromelalgia remained less likely on the differential diagnosis.
The histology of the acral skin revealed mild focal spongiosis with no increase in dermal mucin on colloidal iron or mucopolysaccharide stains (Figure). After receiving the biopsy results and additional questioning of the patient, it was discovered that 2 days prior to her initial presentation she had juiced numerous limes by hand and subsequently spent a long period of time outside with sunlight exposure. Upon discovery of this additional historical information, the diagnosis of phytophotodermatitis was made.
Phytophotodermatitis is an erythematous inflammatory reaction that occurs on the skin after exposure to a plant-derived photosensitizer followed by UVA light radiation.14 This phenomenon was first described by the ancient Egyptians as a treatment for vitiligo.1 The most common plant families that can cause this nonimmune cutaneous reaction include Apiaceae eg, hogweed, celery, dill, fennel) and Rutaceae (eg, citrus plants, rue).14 The psoralens or furocoumarins found in these plants bind loosely to DNA at their ground state but covalently bond to pyrimidine bases during photoexcitation with UVA, resulting in DNA damage and subsequent local inflammation.14 Given the patient’s clinical examination, pathology findings, and history, phytophotodermatitis secondary to lime juice exposure was confirmed. Two weeks after applying clobetasol ointment twice daily, the patient’s hands had returned to baseline with complete resolution of the erythematous lesions.
Although lime phytophotodermatitis is a routine diagnosis, this clinical case stands as an important reminder to demonstrate how common diseases can masquerade as more exotic cutaneous disorders. There often is a clinical desire to seek out more complicated diagnoses, particularly during residency training; however, this case reinforces the invaluable importance of collecting a thorough patient history, as it can ultimately minimize excessive testing and in some cases prevent unnecessary therapy.
- Bolognia JL, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. China:Elsevier Saunders; 2012.
- Uva L, Miguel D, Pinheiro C, et al. Cutaneous manifestations of systemiclupus erythematosus. Autoimmune Dis. 2012;2012:834291.
- Furtado R, Pucinelli M, Cristo V, et al. Scleroderma-like nailfold capillaroscopicabnormalities are associated with anti-U1-RNP antibodies and Raynaud’s phenomenon in SLE patients. Lupus. 2002;11:35-41.
- Wenzel J, Zahn S, Tuting T. Pathogenesis of cutaneous lupus erythematosus:common and different features in distinct subsets. Lupus. 2010;19:1020-1028.
- Avilés Izquierdo JA, Cano Martínez N, Lázaro Ochaita P. Epidemiologicalcharacteristics of patients with cutaneous lupus erythematosus.Actas Dermosifiliogr. 2014;105:69-73.
- Marvi U, Chung L, Fiorentino DF. Clinical presentation and evaluation of dermatomyositis. Indian J Dermatol. 2012;57:375-381.
- Shirani Z, Kucenic MJ, Carroll CL, et al. Pruritus in adult dermatomyositis. Clin Exp Dermatol. 2004;29:273-276.
- Krieg T, Takehara K. Skin disease: a cardinal feature of systemic sclerosis. Rheumatology (Oxford). 2009;48(suppl 3):14-18.
- Mizutani H, Mizutani T, Okada H, et al. Round fingerpad sign: an early sign of scleroderma. J Am Acad Dermatol. 1991;24:67-69.
- Baran R, Dawber RP, Haneke E, et al, eds. A Text Atlas of Nail Disorders Techniques in Investigation and Diagnosis. 3rd ed. Boca Raton, FL: CRC Press; 2005.
- Ghali FE, Stein LD, Fine J, et al. Gingival telangiectases: an underappreciated physical sign of juvenile dermatomyositis. Arch Dermatol. 1999;135:1370-1374.
- Grader-Beck T, Wigley FM. Raynaud’s phenomenon in mixed connective tissue disease. Rheum Dis Clin North Am. 2005;31:465-481.
- Davis MD, Weenig RH, Genebriera J, et al. Histopathologic findings in primary erythromelalgia are nonspecific: special studies show a decrease in small nerve fiber density. J Am Acad Dermatol. 2006;55:519-522.
- Sasseville D. Clinical patterns of phytophotodermatitis. Dermatol Clin. 2009;27:299-308.
- Bolognia JL, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. China:Elsevier Saunders; 2012.
- Uva L, Miguel D, Pinheiro C, et al. Cutaneous manifestations of systemiclupus erythematosus. Autoimmune Dis. 2012;2012:834291.
- Furtado R, Pucinelli M, Cristo V, et al. Scleroderma-like nailfold capillaroscopicabnormalities are associated with anti-U1-RNP antibodies and Raynaud’s phenomenon in SLE patients. Lupus. 2002;11:35-41.
- Wenzel J, Zahn S, Tuting T. Pathogenesis of cutaneous lupus erythematosus:common and different features in distinct subsets. Lupus. 2010;19:1020-1028.
- Avilés Izquierdo JA, Cano Martínez N, Lázaro Ochaita P. Epidemiologicalcharacteristics of patients with cutaneous lupus erythematosus.Actas Dermosifiliogr. 2014;105:69-73.
- Marvi U, Chung L, Fiorentino DF. Clinical presentation and evaluation of dermatomyositis. Indian J Dermatol. 2012;57:375-381.
- Shirani Z, Kucenic MJ, Carroll CL, et al. Pruritus in adult dermatomyositis. Clin Exp Dermatol. 2004;29:273-276.
- Krieg T, Takehara K. Skin disease: a cardinal feature of systemic sclerosis. Rheumatology (Oxford). 2009;48(suppl 3):14-18.
- Mizutani H, Mizutani T, Okada H, et al. Round fingerpad sign: an early sign of scleroderma. J Am Acad Dermatol. 1991;24:67-69.
- Baran R, Dawber RP, Haneke E, et al, eds. A Text Atlas of Nail Disorders Techniques in Investigation and Diagnosis. 3rd ed. Boca Raton, FL: CRC Press; 2005.
- Ghali FE, Stein LD, Fine J, et al. Gingival telangiectases: an underappreciated physical sign of juvenile dermatomyositis. Arch Dermatol. 1999;135:1370-1374.
- Grader-Beck T, Wigley FM. Raynaud’s phenomenon in mixed connective tissue disease. Rheum Dis Clin North Am. 2005;31:465-481.
- Davis MD, Weenig RH, Genebriera J, et al. Histopathologic findings in primary erythromelalgia are nonspecific: special studies show a decrease in small nerve fiber density. J Am Acad Dermatol. 2006;55:519-522.
- Sasseville D. Clinical patterns of phytophotodermatitis. Dermatol Clin. 2009;27:299-308.

A 48-year-old woman presented with erythematous swelling of the dorsal aspects of the bilateral hands followed by desquamation and pruritus of 2 weeks’ duration. She denied any recent contact with plants, chemicals, or topical products or use of over-the-counter medications. A 6-day course of prednisone provided by her primary care physician relieved the swelling and pruritus; however, the erythema persisted. Physical examination revealed clearly demarcated, erythematous to violaceous, edematous plaques with peripheral scaling that involved all digits. There was notable sparing of the proximal interphalangeal joints and volar aspects of the hands extending proximally to the metacarpophalangeal joints.

Take stronger steps to prevent staph infections and sepsis
according to data from a Vital Signs report issued by the Centers for Disease Control and Prevention. The data include both methicillin-resistant S. aureus (MRSA) and methicillin-susceptible S. aureus (MSSA).
![]()
Although MRSA infections in health care settings declined by approximately 17% during 2005-2012, rates plateaued during 2012-2017, Anne Schuchat, MD, principal deputy director of the CDC, said in a teleconference March 5 to present the findings. The report emphasizes the potential for serious illness and death with any staph infection and the need for ongoing vigilance on the part of clinicians, she said.
In addition, community-onset MSSA infections increased by 3.9%/year during 2012-2017. Data from previous studies suggest that this increase may be connected to the opioid epidemic, said Dr. Schuchat.
“People who inject drugs are 16% more likely to develop a staph infection” than are those who don’t inject drugs, she said.
Community-onset MRSA declined by 6.9% during 2001-2016, attributed to declines in health care–associated infections, according to Vital Signs author Athena P. Kourtis, MD, of the CDC’s National Center for Emerging and Zoonotic Infectious Diseases, and her colleagues. Rates of hospital-associated MSSA infection remained essentially unchanged (P = .11). The overall unadjusted in-hospital mortality among patients with S. aureus bloodstream infections over the study period was 18%.
The data for the report were collected from electronic health records at more than 400 acute care hospitals, as well as population-based surveillance data from the CDC’s Emerging Infections Program.
Most people carry staph on their skin with no ill effects, but the bacteria become dangerous when they enter the bloodstream, Dr. Schuchat emphasized. “We hope the new data today will refocus the nation’s efforts to protect patients from staph infections,” she said.
Dr. Schuchat advised clinicians and hospital administrators to review their data and step up their safety protocols to prevent staph infections. Precautions include wearing gowns and gloves, following proper hand washing protocols, cautious use of antibiotics, and treating infections rapidly when they occur, she said. Dr. Schuchat noted that lack of adherence to these recommendations may have declined in recent years if clinicians and hospital administrators were wondering whether their protocols have an effect and have value. However, “this is a very serious infection, and we think it is very much worth preventing,” she emphasized.
Other strategies to prevent staph infections in health care settings include reviewing infection data regularly, exploring new approaches to prevent infections, and educating patients about when they may be at increased risk for infection, such as when invasive devices are in place or during surgical procedures. Also, clinicians should be aware of the increased risk for patients who inject drugs, Dr. Schuchat said.
Dr. Schuchat commended the Department of Veterans Affairs Medical Centers (VAMC), which overall reduced their rate of staph infections by 43% during the period from 2005 through 2017 in contrast to the national trend. These findings also appeared in the MMWR on March 5. The VAMC implemented additional interventions and increased their adherence to CDC recommendations during this period, she noted.
The Vital Signs data were published March 5 in the CDC’s Morbidity and Mortality Weekly Report; read the full report here.
The CDC researchers had no financial conflicts to disclose.
SOURCE: Kourtis AP et al. MMWR. 2019 Mar 5; 68:1-6.
according to data from a Vital Signs report issued by the Centers for Disease Control and Prevention. The data include both methicillin-resistant S. aureus (MRSA) and methicillin-susceptible S. aureus (MSSA).
![]()
Although MRSA infections in health care settings declined by approximately 17% during 2005-2012, rates plateaued during 2012-2017, Anne Schuchat, MD, principal deputy director of the CDC, said in a teleconference March 5 to present the findings. The report emphasizes the potential for serious illness and death with any staph infection and the need for ongoing vigilance on the part of clinicians, she said.
In addition, community-onset MSSA infections increased by 3.9%/year during 2012-2017. Data from previous studies suggest that this increase may be connected to the opioid epidemic, said Dr. Schuchat.
“People who inject drugs are 16% more likely to develop a staph infection” than are those who don’t inject drugs, she said.
Community-onset MRSA declined by 6.9% during 2001-2016, attributed to declines in health care–associated infections, according to Vital Signs author Athena P. Kourtis, MD, of the CDC’s National Center for Emerging and Zoonotic Infectious Diseases, and her colleagues. Rates of hospital-associated MSSA infection remained essentially unchanged (P = .11). The overall unadjusted in-hospital mortality among patients with S. aureus bloodstream infections over the study period was 18%.
The data for the report were collected from electronic health records at more than 400 acute care hospitals, as well as population-based surveillance data from the CDC’s Emerging Infections Program.
Most people carry staph on their skin with no ill effects, but the bacteria become dangerous when they enter the bloodstream, Dr. Schuchat emphasized. “We hope the new data today will refocus the nation’s efforts to protect patients from staph infections,” she said.
Dr. Schuchat advised clinicians and hospital administrators to review their data and step up their safety protocols to prevent staph infections. Precautions include wearing gowns and gloves, following proper hand washing protocols, cautious use of antibiotics, and treating infections rapidly when they occur, she said. Dr. Schuchat noted that lack of adherence to these recommendations may have declined in recent years if clinicians and hospital administrators were wondering whether their protocols have an effect and have value. However, “this is a very serious infection, and we think it is very much worth preventing,” she emphasized.
Other strategies to prevent staph infections in health care settings include reviewing infection data regularly, exploring new approaches to prevent infections, and educating patients about when they may be at increased risk for infection, such as when invasive devices are in place or during surgical procedures. Also, clinicians should be aware of the increased risk for patients who inject drugs, Dr. Schuchat said.
Dr. Schuchat commended the Department of Veterans Affairs Medical Centers (VAMC), which overall reduced their rate of staph infections by 43% during the period from 2005 through 2017 in contrast to the national trend. These findings also appeared in the MMWR on March 5. The VAMC implemented additional interventions and increased their adherence to CDC recommendations during this period, she noted.
The Vital Signs data were published March 5 in the CDC’s Morbidity and Mortality Weekly Report; read the full report here.
The CDC researchers had no financial conflicts to disclose.
SOURCE: Kourtis AP et al. MMWR. 2019 Mar 5; 68:1-6.
according to data from a Vital Signs report issued by the Centers for Disease Control and Prevention. The data include both methicillin-resistant S. aureus (MRSA) and methicillin-susceptible S. aureus (MSSA).
![]()
Although MRSA infections in health care settings declined by approximately 17% during 2005-2012, rates plateaued during 2012-2017, Anne Schuchat, MD, principal deputy director of the CDC, said in a teleconference March 5 to present the findings. The report emphasizes the potential for serious illness and death with any staph infection and the need for ongoing vigilance on the part of clinicians, she said.
In addition, community-onset MSSA infections increased by 3.9%/year during 2012-2017. Data from previous studies suggest that this increase may be connected to the opioid epidemic, said Dr. Schuchat.
“People who inject drugs are 16% more likely to develop a staph infection” than are those who don’t inject drugs, she said.
Community-onset MRSA declined by 6.9% during 2001-2016, attributed to declines in health care–associated infections, according to Vital Signs author Athena P. Kourtis, MD, of the CDC’s National Center for Emerging and Zoonotic Infectious Diseases, and her colleagues. Rates of hospital-associated MSSA infection remained essentially unchanged (P = .11). The overall unadjusted in-hospital mortality among patients with S. aureus bloodstream infections over the study period was 18%.
The data for the report were collected from electronic health records at more than 400 acute care hospitals, as well as population-based surveillance data from the CDC’s Emerging Infections Program.
Most people carry staph on their skin with no ill effects, but the bacteria become dangerous when they enter the bloodstream, Dr. Schuchat emphasized. “We hope the new data today will refocus the nation’s efforts to protect patients from staph infections,” she said.
Dr. Schuchat advised clinicians and hospital administrators to review their data and step up their safety protocols to prevent staph infections. Precautions include wearing gowns and gloves, following proper hand washing protocols, cautious use of antibiotics, and treating infections rapidly when they occur, she said. Dr. Schuchat noted that lack of adherence to these recommendations may have declined in recent years if clinicians and hospital administrators were wondering whether their protocols have an effect and have value. However, “this is a very serious infection, and we think it is very much worth preventing,” she emphasized.
Other strategies to prevent staph infections in health care settings include reviewing infection data regularly, exploring new approaches to prevent infections, and educating patients about when they may be at increased risk for infection, such as when invasive devices are in place or during surgical procedures. Also, clinicians should be aware of the increased risk for patients who inject drugs, Dr. Schuchat said.
Dr. Schuchat commended the Department of Veterans Affairs Medical Centers (VAMC), which overall reduced their rate of staph infections by 43% during the period from 2005 through 2017 in contrast to the national trend. These findings also appeared in the MMWR on March 5. The VAMC implemented additional interventions and increased their adherence to CDC recommendations during this period, she noted.
The Vital Signs data were published March 5 in the CDC’s Morbidity and Mortality Weekly Report; read the full report here.
The CDC researchers had no financial conflicts to disclose.
SOURCE: Kourtis AP et al. MMWR. 2019 Mar 5; 68:1-6.
FROM THE MORBIDITY AND MORTALITY WEEKLY REPORT
Don’t overlook this step in combatting the rise in STIs
Resources
1. Kuehn BM. A proactive approach needed to combat rising STIs. JAMA. 2019;321:330-332.
2. Screening Recommendations and Considerations Referenced in Treatment Guidelines and Original Sources. Centers for Disease Control and Prevention. https://www.cdc.gov/std/tg2015/screening-recommendations.htm. Updated June 4, 2015. Accessed February 27, 2019.
3. STD Clinical Consultation Network. National STD Curriculum. https://www.std.uw.edu/page/site/clinical-consultation. Accessed February 27, 2019.
4. National STD Curriculum. https://www.std.uw.edu/. Accessed February 27, 2019.
5. Sexually Transmitted Disease Surveillance 2017. Syphilis. Centers for Disease Control and Prevention. https://www.cdc.gov/std/stats17/syphilis.htm. Reviewed July 24, 2018. Accessed February 27, 2019.
Resources
1. Kuehn BM. A proactive approach needed to combat rising STIs. JAMA. 2019;321:330-332.
2. Screening Recommendations and Considerations Referenced in Treatment Guidelines and Original Sources. Centers for Disease Control and Prevention. https://www.cdc.gov/std/tg2015/screening-recommendations.htm. Updated June 4, 2015. Accessed February 27, 2019.
3. STD Clinical Consultation Network. National STD Curriculum. https://www.std.uw.edu/page/site/clinical-consultation. Accessed February 27, 2019.
4. National STD Curriculum. https://www.std.uw.edu/. Accessed February 27, 2019.
5. Sexually Transmitted Disease Surveillance 2017. Syphilis. Centers for Disease Control and Prevention. https://www.cdc.gov/std/stats17/syphilis.htm. Reviewed July 24, 2018. Accessed February 27, 2019.
Resources
1. Kuehn BM. A proactive approach needed to combat rising STIs. JAMA. 2019;321:330-332.
2. Screening Recommendations and Considerations Referenced in Treatment Guidelines and Original Sources. Centers for Disease Control and Prevention. https://www.cdc.gov/std/tg2015/screening-recommendations.htm. Updated June 4, 2015. Accessed February 27, 2019.
3. STD Clinical Consultation Network. National STD Curriculum. https://www.std.uw.edu/page/site/clinical-consultation. Accessed February 27, 2019.
4. National STD Curriculum. https://www.std.uw.edu/. Accessed February 27, 2019.
5. Sexually Transmitted Disease Surveillance 2017. Syphilis. Centers for Disease Control and Prevention. https://www.cdc.gov/std/stats17/syphilis.htm. Reviewed July 24, 2018. Accessed February 27, 2019.

Drug pricing does not inspire Americans’ trust
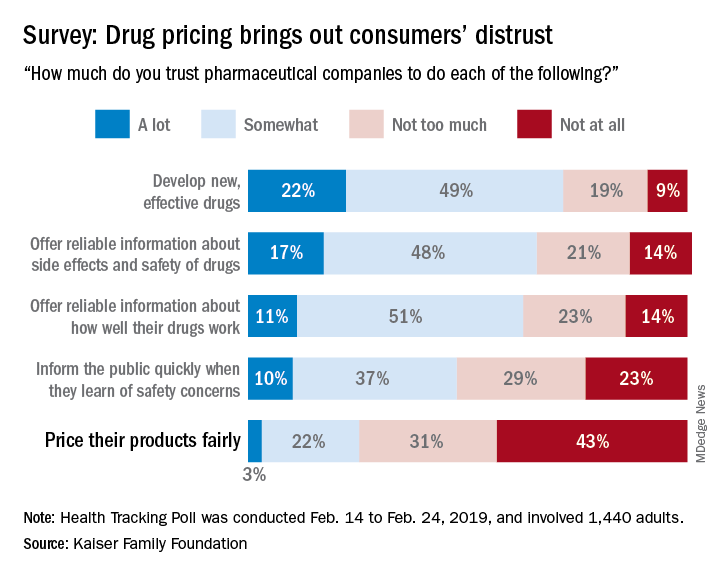
Only 25% of the respondents said that they currently trust drug companies “a lot” (3%) or “somewhat” (22%) when it comes to pricing their products fairly, which “is a significant decrease from 41% who said they trusted pharmaceutical companies to price their products fairly back in 2008,” Kaiser said in a recent Health Tracking Poll.
Safety issues were also a bit of a sore point in the current survey: Less than half of the 1,440 adults responding said that they trusted pharmaceutical companies a lot (10%) or somewhat (37%) regarding informing the public quickly when a safety concern is discovered.
Trust was more forthcoming when people were asked about the development of new, effective drugs – 71% expressed a favorable opinion – and companies’ offering “reliable information about side effects and safety of drugs,” which received a favorable response from 65% of those surveyed during Feb. 14 to Feb. 24, 2019.
A majority of respondents (61%) also thought that pharmaceutical companies could be trusted to “offer reliable information about how well their drugs work,” the report’s authors noted.
The lack of trust expressed regarding drug pricing also may explain why most consumers (80%) said that drug company profits were a major contributor to the cost of prescription drugs. The cost of research and development, at 69%, was the next most commonly mentioned factor, followed by profits made by pharmacy benefit managers at 63%, according to the report.
Only 25% of the respondents said that they currently trust drug companies “a lot” (3%) or “somewhat” (22%) when it comes to pricing their products fairly, which “is a significant decrease from 41% who said they trusted pharmaceutical companies to price their products fairly back in 2008,” Kaiser said in a recent Health Tracking Poll.
Safety issues were also a bit of a sore point in the current survey: Less than half of the 1,440 adults responding said that they trusted pharmaceutical companies a lot (10%) or somewhat (37%) regarding informing the public quickly when a safety concern is discovered.
Trust was more forthcoming when people were asked about the development of new, effective drugs – 71% expressed a favorable opinion – and companies’ offering “reliable information about side effects and safety of drugs,” which received a favorable response from 65% of those surveyed during Feb. 14 to Feb. 24, 2019.
A majority of respondents (61%) also thought that pharmaceutical companies could be trusted to “offer reliable information about how well their drugs work,” the report’s authors noted.
The lack of trust expressed regarding drug pricing also may explain why most consumers (80%) said that drug company profits were a major contributor to the cost of prescription drugs. The cost of research and development, at 69%, was the next most commonly mentioned factor, followed by profits made by pharmacy benefit managers at 63%, according to the report.
Only 25% of the respondents said that they currently trust drug companies “a lot” (3%) or “somewhat” (22%) when it comes to pricing their products fairly, which “is a significant decrease from 41% who said they trusted pharmaceutical companies to price their products fairly back in 2008,” Kaiser said in a recent Health Tracking Poll.
Safety issues were also a bit of a sore point in the current survey: Less than half of the 1,440 adults responding said that they trusted pharmaceutical companies a lot (10%) or somewhat (37%) regarding informing the public quickly when a safety concern is discovered.
Trust was more forthcoming when people were asked about the development of new, effective drugs – 71% expressed a favorable opinion – and companies’ offering “reliable information about side effects and safety of drugs,” which received a favorable response from 65% of those surveyed during Feb. 14 to Feb. 24, 2019.
A majority of respondents (61%) also thought that pharmaceutical companies could be trusted to “offer reliable information about how well their drugs work,” the report’s authors noted.
The lack of trust expressed regarding drug pricing also may explain why most consumers (80%) said that drug company profits were a major contributor to the cost of prescription drugs. The cost of research and development, at 69%, was the next most commonly mentioned factor, followed by profits made by pharmacy benefit managers at 63%, according to the report.
Try behavioral interventions for chronic insomnia
“The greatest medicine of all is teaching people how not to need it.” – Hippocrates
For many years, over-the-counter and prescription medications indicated for sleep problems/disorders have been available to patients. But the side effects associated with some of these medications are many. In light of the numerous nonpharmacologic interventions that are available to patients, they should be offered first when appropriate.

One of the top nonpharmacologic interventions is cognitive-behavioral therapy for insomnia, or CBT-I, which the American Academy of Sleep Medicine’s clinical guidelines say should be used as initial treatment if possible.1 Elements of CBT-I include cognitive therapy, which is aimed at reducing dysfunctional beliefs about sleep. Common distortions expressed by patients include: “I cannot sleep without medications” and “I must get 8 hours of sleep to feel refreshed and function well the next day.” It helps in dealing with anxiety and catastrophic thinking to establish realistic expectations and treatment related to insomnia.
CBT-I can be delivered in the form of monotherapy or in a combined manner. The individual components include psychoeducation, behavioral strategies, cognitive therapy, and relaxation training. CBT-I combines cognitive therapy with behavioral interventions. Behavioral elements include stimulus control therapy and sleep restriction therapy. Relaxation therapy might or might not be included. Sleep hygiene education usually is a part of it.2
Two other kinds of CBT that can be effective options are telephone-based CBT-I and Internet-based CBT-I.3,4 Meanwhile, among the disadvantages of CBT for insomnia are longer duration of therapy and lack of skilled clinicians.5
Many other kinds of behavioral interventions are available to patients with problems related to sleep, including stimulus control therapy, relaxation therapy, exercise therapy, and sleep restriction therapy.
Stimulus control therapy
This is a strategy aimed at strengthening the association of bed and bedroom to sleep, establishing a consistent sleep-wake rhythm, and reducing the activities that might interfere with sleep. This behavioral therapy is based on the idea that arousal occurs as a conditioned response to the stimulus of sleep environment, and it is among the most effective behavioral treatments.6,7 Strategies include the following:
1. Lie down with the intention of sleeping when sleepy.
2. Do not watch television, read, eat or worry while in bed. Use bed only for sleep and sex.
3. Get out of bed if unable to fall asleep within 10-15 minutes and go to another room. Return to bed only when sleepy. Do not watch the clock. Repeat this step as many times as necessary throughout the night.
4. Set an alarm clock to wake up at a fixed time each morning, including weekends, regardless of how much sleep you got during the night.
5. Do not take a nap during the day.
The goal of these strategies is to extinguish negative associations between bed and undesirable outcomes, such as wakefulness and frustration. One study showed that stimulus control participants, unlike control group participants, experienced significant improvement at follow-up for total sleep time, sleep efficiency, and sleep quality.8
Relaxation therapy
This encompasses different techniques that produce a relaxation response and reduce somatic arousal. It can be implemented before each sleep period. Progressive muscle relaxation, autogenic training, and biofeedback help reduce somatic arousal. Attention-focused procedures, such as imagery training and meditation, tend to lower presleep cognitive arousal (for example, intrusive thoughts, racing minds).9 Slow paced breathing prior to onset of sleep enhances vagal activity, which results in improved sleep parameters.10 One study showed improved quality of sleep and cognitive functions in the elderly by self-relaxation training.11
Exercise training
Participating in physical exercise can be useful in the treatment of insomnia.12 One randomized, controlled trial found that exercising regularly for at least 150 minutes per week was optimal.13 Another study found that, among overweight and obese men with insomnia, aerobic exercise over a 6-month period reduced difficulty in initiating and improving sleep.14
Sleep restriction therapy
The goal of this therapy is to increase the homeostatic drive to sleep. This is carried out by limiting the amount of time spent in bed to the same amount of time that the person reports sleeping. Naps are not allowed. Patients improve with increased drive to sleep in successive nights. In patients with bipolar disorder, however, sleep restriction should be used with caution as it can trigger manic episodes.15
Always ask about sleep
Clinicians should always ask patients about sleep during visits. Sleep duration and sleep quality should be assessed. Insomnia, which is an independent condition, may or may not coexist with other conditions. It is important to determine whether another sleep disorder, or a physical (such as pain, heart, or lung disease), neurological (such as Parkinson’s disease or cerebrovascular disease), or psychiatric disorder (such as depressive illness, anxiety disorder, or substance misuse) is the primary diagnosis. Treatment of insomnia can improve comorbidities.16

In addition, it is important to teach patients about basic sleep hygiene, which includes abiding by a consistent bedtime, and avoiding coffee, alcohol, and nicotine. Eliminating a bedroom clock, not exercising in the late afternoon/early evening, and consuming light bedtime snacks are other measures that can be taken. Avoiding the prolonged use of light-emitting screens before bedtime is another positive step.17
In conclusion, cognitive and behavioral methods are just as effective as prescription medications for short-term treatment of chronic insomnia and should be considered as first line before considering medications. The beneficial effects of CBT-I, in contrast to those produced by medication, might last well beyond the termination of active treatment.
References
1. J Clin Sleep Med. 2008 Oct 15;4(5):487-504.
2. J Clin Psychol. 2010;66(11):1148-60.
3. Sleep. 2013 Mar 1;36(3):353-62.
4. Sleep Med Rev. 2016 Dec;30:1-10.
5. BMC Family Prac. 2012;13:40.
6. Sleep. 2006 Nov;29(11):1398-414.
7. Behavioral Treatments for Sleep Disorders. 1991. doi: 10.1016/13978-0-12-381522-4.00002-X.
8. Behav Modif 1998 Jan;22(1):3-28.
9. Am Fam Physician. 1999 Jun;59(11):3029-38.
10. Psychophysiology. 2015 Mar;52(3):388-96.
11. J Clin Nursing. 2013 April 10. doi: 10.1111/jocn.12096.
12. J Physiother. 2012;58(3):157-63.
13. J Sleep Res. 2015 Oct;24(5):526-34.
14 Sleep Med. 2016 Sep;25:113-121.
15. Am J Psychiatry. 2013 Jul;170(7):716-20.
16. JAMA Intern Med. 2015 Sep;175(9):1461-72.
17. Proc Natl Acad Sci USA. 2015;112(4):1232-7.
Dr. Lamba is a psychiatrist and medical director at Bayridge Hospital in Lynn, Mass. Dr. Rana is assistant professor of pediatrics at Boston University.
“The greatest medicine of all is teaching people how not to need it.” – Hippocrates
For many years, over-the-counter and prescription medications indicated for sleep problems/disorders have been available to patients. But the side effects associated with some of these medications are many. In light of the numerous nonpharmacologic interventions that are available to patients, they should be offered first when appropriate.
One of the top nonpharmacologic interventions is cognitive-behavioral therapy for insomnia, or CBT-I, which the American Academy of Sleep Medicine’s clinical guidelines say should be used as initial treatment if possible.1 Elements of CBT-I include cognitive therapy, which is aimed at reducing dysfunctional beliefs about sleep. Common distortions expressed by patients include: “I cannot sleep without medications” and “I must get 8 hours of sleep to feel refreshed and function well the next day.” It helps in dealing with anxiety and catastrophic thinking to establish realistic expectations and treatment related to insomnia.
CBT-I can be delivered in the form of monotherapy or in a combined manner. The individual components include psychoeducation, behavioral strategies, cognitive therapy, and relaxation training. CBT-I combines cognitive therapy with behavioral interventions. Behavioral elements include stimulus control therapy and sleep restriction therapy. Relaxation therapy might or might not be included. Sleep hygiene education usually is a part of it.2
Two other kinds of CBT that can be effective options are telephone-based CBT-I and Internet-based CBT-I.3,4 Meanwhile, among the disadvantages of CBT for insomnia are longer duration of therapy and lack of skilled clinicians.5
Many other kinds of behavioral interventions are available to patients with problems related to sleep, including stimulus control therapy, relaxation therapy, exercise therapy, and sleep restriction therapy.
Stimulus control therapy
This is a strategy aimed at strengthening the association of bed and bedroom to sleep, establishing a consistent sleep-wake rhythm, and reducing the activities that might interfere with sleep. This behavioral therapy is based on the idea that arousal occurs as a conditioned response to the stimulus of sleep environment, and it is among the most effective behavioral treatments.6,7 Strategies include the following:
1. Lie down with the intention of sleeping when sleepy.
2. Do not watch television, read, eat or worry while in bed. Use bed only for sleep and sex.
3. Get out of bed if unable to fall asleep within 10-15 minutes and go to another room. Return to bed only when sleepy. Do not watch the clock. Repeat this step as many times as necessary throughout the night.
4. Set an alarm clock to wake up at a fixed time each morning, including weekends, regardless of how much sleep you got during the night.
5. Do not take a nap during the day.
The goal of these strategies is to extinguish negative associations between bed and undesirable outcomes, such as wakefulness and frustration. One study showed that stimulus control participants, unlike control group participants, experienced significant improvement at follow-up for total sleep time, sleep efficiency, and sleep quality.8
Relaxation therapy
This encompasses different techniques that produce a relaxation response and reduce somatic arousal. It can be implemented before each sleep period. Progressive muscle relaxation, autogenic training, and biofeedback help reduce somatic arousal. Attention-focused procedures, such as imagery training and meditation, tend to lower presleep cognitive arousal (for example, intrusive thoughts, racing minds).9 Slow paced breathing prior to onset of sleep enhances vagal activity, which results in improved sleep parameters.10 One study showed improved quality of sleep and cognitive functions in the elderly by self-relaxation training.11
Exercise training
Participating in physical exercise can be useful in the treatment of insomnia.12 One randomized, controlled trial found that exercising regularly for at least 150 minutes per week was optimal.13 Another study found that, among overweight and obese men with insomnia, aerobic exercise over a 6-month period reduced difficulty in initiating and improving sleep.14
Sleep restriction therapy
The goal of this therapy is to increase the homeostatic drive to sleep. This is carried out by limiting the amount of time spent in bed to the same amount of time that the person reports sleeping. Naps are not allowed. Patients improve with increased drive to sleep in successive nights. In patients with bipolar disorder, however, sleep restriction should be used with caution as it can trigger manic episodes.15
Always ask about sleep
Clinicians should always ask patients about sleep during visits. Sleep duration and sleep quality should be assessed. Insomnia, which is an independent condition, may or may not coexist with other conditions. It is important to determine whether another sleep disorder, or a physical (such as pain, heart, or lung disease), neurological (such as Parkinson’s disease or cerebrovascular disease), or psychiatric disorder (such as depressive illness, anxiety disorder, or substance misuse) is the primary diagnosis. Treatment of insomnia can improve comorbidities.16
In addition, it is important to teach patients about basic sleep hygiene, which includes abiding by a consistent bedtime, and avoiding coffee, alcohol, and nicotine. Eliminating a bedroom clock, not exercising in the late afternoon/early evening, and consuming light bedtime snacks are other measures that can be taken. Avoiding the prolonged use of light-emitting screens before bedtime is another positive step.17
In conclusion, cognitive and behavioral methods are just as effective as prescription medications for short-term treatment of chronic insomnia and should be considered as first line before considering medications. The beneficial effects of CBT-I, in contrast to those produced by medication, might last well beyond the termination of active treatment.
References
1. J Clin Sleep Med. 2008 Oct 15;4(5):487-504.
2. J Clin Psychol. 2010;66(11):1148-60.
3. Sleep. 2013 Mar 1;36(3):353-62.
4. Sleep Med Rev. 2016 Dec;30:1-10.
5. BMC Family Prac. 2012;13:40.
6. Sleep. 2006 Nov;29(11):1398-414.
7. Behavioral Treatments for Sleep Disorders. 1991. doi: 10.1016/13978-0-12-381522-4.00002-X.
8. Behav Modif 1998 Jan;22(1):3-28.
9. Am Fam Physician. 1999 Jun;59(11):3029-38.
10. Psychophysiology. 2015 Mar;52(3):388-96.
11. J Clin Nursing. 2013 April 10. doi: 10.1111/jocn.12096.
12. J Physiother. 2012;58(3):157-63.
13. J Sleep Res. 2015 Oct;24(5):526-34.
14 Sleep Med. 2016 Sep;25:113-121.
15. Am J Psychiatry. 2013 Jul;170(7):716-20.
16. JAMA Intern Med. 2015 Sep;175(9):1461-72.
17. Proc Natl Acad Sci USA. 2015;112(4):1232-7.
Dr. Lamba is a psychiatrist and medical director at Bayridge Hospital in Lynn, Mass. Dr. Rana is assistant professor of pediatrics at Boston University.
“The greatest medicine of all is teaching people how not to need it.” – Hippocrates
For many years, over-the-counter and prescription medications indicated for sleep problems/disorders have been available to patients. But the side effects associated with some of these medications are many. In light of the numerous nonpharmacologic interventions that are available to patients, they should be offered first when appropriate.
One of the top nonpharmacologic interventions is cognitive-behavioral therapy for insomnia, or CBT-I, which the American Academy of Sleep Medicine’s clinical guidelines say should be used as initial treatment if possible.1 Elements of CBT-I include cognitive therapy, which is aimed at reducing dysfunctional beliefs about sleep. Common distortions expressed by patients include: “I cannot sleep without medications” and “I must get 8 hours of sleep to feel refreshed and function well the next day.” It helps in dealing with anxiety and catastrophic thinking to establish realistic expectations and treatment related to insomnia.
CBT-I can be delivered in the form of monotherapy or in a combined manner. The individual components include psychoeducation, behavioral strategies, cognitive therapy, and relaxation training. CBT-I combines cognitive therapy with behavioral interventions. Behavioral elements include stimulus control therapy and sleep restriction therapy. Relaxation therapy might or might not be included. Sleep hygiene education usually is a part of it.2
Two other kinds of CBT that can be effective options are telephone-based CBT-I and Internet-based CBT-I.3,4 Meanwhile, among the disadvantages of CBT for insomnia are longer duration of therapy and lack of skilled clinicians.5
Many other kinds of behavioral interventions are available to patients with problems related to sleep, including stimulus control therapy, relaxation therapy, exercise therapy, and sleep restriction therapy.
Stimulus control therapy
This is a strategy aimed at strengthening the association of bed and bedroom to sleep, establishing a consistent sleep-wake rhythm, and reducing the activities that might interfere with sleep. This behavioral therapy is based on the idea that arousal occurs as a conditioned response to the stimulus of sleep environment, and it is among the most effective behavioral treatments.6,7 Strategies include the following:
1. Lie down with the intention of sleeping when sleepy.
2. Do not watch television, read, eat or worry while in bed. Use bed only for sleep and sex.
3. Get out of bed if unable to fall asleep within 10-15 minutes and go to another room. Return to bed only when sleepy. Do not watch the clock. Repeat this step as many times as necessary throughout the night.
4. Set an alarm clock to wake up at a fixed time each morning, including weekends, regardless of how much sleep you got during the night.
5. Do not take a nap during the day.
The goal of these strategies is to extinguish negative associations between bed and undesirable outcomes, such as wakefulness and frustration. One study showed that stimulus control participants, unlike control group participants, experienced significant improvement at follow-up for total sleep time, sleep efficiency, and sleep quality.8
Relaxation therapy
This encompasses different techniques that produce a relaxation response and reduce somatic arousal. It can be implemented before each sleep period. Progressive muscle relaxation, autogenic training, and biofeedback help reduce somatic arousal. Attention-focused procedures, such as imagery training and meditation, tend to lower presleep cognitive arousal (for example, intrusive thoughts, racing minds).9 Slow paced breathing prior to onset of sleep enhances vagal activity, which results in improved sleep parameters.10 One study showed improved quality of sleep and cognitive functions in the elderly by self-relaxation training.11
Exercise training
Participating in physical exercise can be useful in the treatment of insomnia.12 One randomized, controlled trial found that exercising regularly for at least 150 minutes per week was optimal.13 Another study found that, among overweight and obese men with insomnia, aerobic exercise over a 6-month period reduced difficulty in initiating and improving sleep.14
Sleep restriction therapy
The goal of this therapy is to increase the homeostatic drive to sleep. This is carried out by limiting the amount of time spent in bed to the same amount of time that the person reports sleeping. Naps are not allowed. Patients improve with increased drive to sleep in successive nights. In patients with bipolar disorder, however, sleep restriction should be used with caution as it can trigger manic episodes.15
Always ask about sleep
Clinicians should always ask patients about sleep during visits. Sleep duration and sleep quality should be assessed. Insomnia, which is an independent condition, may or may not coexist with other conditions. It is important to determine whether another sleep disorder, or a physical (such as pain, heart, or lung disease), neurological (such as Parkinson’s disease or cerebrovascular disease), or psychiatric disorder (such as depressive illness, anxiety disorder, or substance misuse) is the primary diagnosis. Treatment of insomnia can improve comorbidities.16
In addition, it is important to teach patients about basic sleep hygiene, which includes abiding by a consistent bedtime, and avoiding coffee, alcohol, and nicotine. Eliminating a bedroom clock, not exercising in the late afternoon/early evening, and consuming light bedtime snacks are other measures that can be taken. Avoiding the prolonged use of light-emitting screens before bedtime is another positive step.17
In conclusion, cognitive and behavioral methods are just as effective as prescription medications for short-term treatment of chronic insomnia and should be considered as first line before considering medications. The beneficial effects of CBT-I, in contrast to those produced by medication, might last well beyond the termination of active treatment.
References
1. J Clin Sleep Med. 2008 Oct 15;4(5):487-504.
2. J Clin Psychol. 2010;66(11):1148-60.
3. Sleep. 2013 Mar 1;36(3):353-62.
4. Sleep Med Rev. 2016 Dec;30:1-10.
5. BMC Family Prac. 2012;13:40.
6. Sleep. 2006 Nov;29(11):1398-414.
7. Behavioral Treatments for Sleep Disorders. 1991. doi: 10.1016/13978-0-12-381522-4.00002-X.
8. Behav Modif 1998 Jan;22(1):3-28.
9. Am Fam Physician. 1999 Jun;59(11):3029-38.
10. Psychophysiology. 2015 Mar;52(3):388-96.
11. J Clin Nursing. 2013 April 10. doi: 10.1111/jocn.12096.
12. J Physiother. 2012;58(3):157-63.
13. J Sleep Res. 2015 Oct;24(5):526-34.
14 Sleep Med. 2016 Sep;25:113-121.
15. Am J Psychiatry. 2013 Jul;170(7):716-20.
16. JAMA Intern Med. 2015 Sep;175(9):1461-72.
17. Proc Natl Acad Sci USA. 2015;112(4):1232-7.
Dr. Lamba is a psychiatrist and medical director at Bayridge Hospital in Lynn, Mass. Dr. Rana is assistant professor of pediatrics at Boston University.