User login
As deep sleep decreases, Alzheimer’s pathology – particularly tau – increases
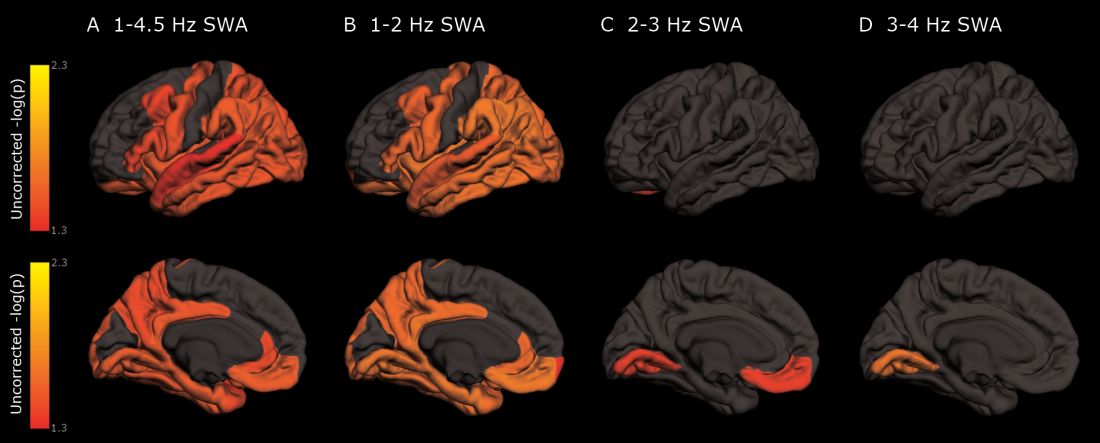
The protein was evident in areas associated with memory consolidation, typically affected in Alzheimer’s disease: the entorhinal, parahippocampal, inferior parietal, insula, isthmus cingulate, lingual, supramarginal, and orbitofrontal regions.
Because the findings were observed in a population of cognitively normal and minimally impaired subjects, they suggest a role for sleep studies in assessing the risk for cognitive decline and Alzheimer’s disease, and in monitoring patients with the disease, reported Brendan P. Lucey, MD, and his colleagues. The report is in Science and Translational Medicine (Sci Transl Med. 2019 Jan 9;11:eaau6550).
“With the rising incidence of Alzheimer’s disease in an aging population, our findings have potential application in both clinical trials and patient screening for Alzheimer’s disease to noninvasively monitor for progression of Alzheimer’s disease pathology,” wrote Dr. Lucey, director of the Sleep Medicine Center and assistant professor of neurology at Washington University in St. Louis. “For instance, periodically measuring non-REM slow wave activity, in conjunction with other biomarkers, may have utility for monitoring Alzheimer’s disease risk or response to an Alzheimer’s disease treatment.”
Dr. Lucey and his colleagues examined sleep architecture and tau and amyloid deposition in 119 subjects enrolled in longitudinal aging studies. For 6 nights, subjects slept with a single-channel EEG monitor on. They also underwent cognitive testing and genotyping for Alzheimer’s disease risk factors.
Subjects were a mean of 74 years old. Almost 80% had normal cognition as measured by the Clinical Dementia Rating Scale (CDR); the remainder had very mild cognitive impairment (CDR 0.5)
Among those with positive biomarker findings, sleep architecture was altered in several ways: lower REM latency, lower wake after sleep onset, prolonged sleep-onset latency, and longer self-reported total sleep time. The differences were evident in those with normal cognition, but even more pronounced in those with mild cognitive impairment. Despite the longer sleep times, however, sleep efficiency was decreased.
Decreased non-REM slow wave activity was associated with increased tau deposition. The protein was largely concentrated in areas of typical Alzheimer’s disease pathology (entorhinal, parahippocampal, orbital frontal, precuneus, inferior parietal, and inferior temporal regions). There were no significant associations between non-REM slow wave activity and amyloid deposits.
Other sleep parameters, however, were associated with amyloid, including REM latency and sleep latency, “suggesting that as amyloid-beta deposition increased, the time to fall asleep and enter REM sleep decreased,” the investigators said.
Those with tau pathology also slept longer, reporting more daytime naps. “This suggests that participants with greater tau pathology experienced daytime sleepiness despite increased total sleep time.”
“These results, coupled with the non-REM slow wave activity findings, suggest that the quality of sleep decreases with increasing tau despite increased sleep time.” Questions about napping should probably be included in dementia screening discussions, they said.
The study was largely funded by the National Institutes of Health. Dr. Lucey had no financial conflicts.
SOURCE: Lucey BP et al. Sci Transl Med 2019 Jan 9;11:eaau6550.
The protein was evident in areas associated with memory consolidation, typically affected in Alzheimer’s disease: the entorhinal, parahippocampal, inferior parietal, insula, isthmus cingulate, lingual, supramarginal, and orbitofrontal regions.
Because the findings were observed in a population of cognitively normal and minimally impaired subjects, they suggest a role for sleep studies in assessing the risk for cognitive decline and Alzheimer’s disease, and in monitoring patients with the disease, reported Brendan P. Lucey, MD, and his colleagues. The report is in Science and Translational Medicine (Sci Transl Med. 2019 Jan 9;11:eaau6550).
“With the rising incidence of Alzheimer’s disease in an aging population, our findings have potential application in both clinical trials and patient screening for Alzheimer’s disease to noninvasively monitor for progression of Alzheimer’s disease pathology,” wrote Dr. Lucey, director of the Sleep Medicine Center and assistant professor of neurology at Washington University in St. Louis. “For instance, periodically measuring non-REM slow wave activity, in conjunction with other biomarkers, may have utility for monitoring Alzheimer’s disease risk or response to an Alzheimer’s disease treatment.”
Dr. Lucey and his colleagues examined sleep architecture and tau and amyloid deposition in 119 subjects enrolled in longitudinal aging studies. For 6 nights, subjects slept with a single-channel EEG monitor on. They also underwent cognitive testing and genotyping for Alzheimer’s disease risk factors.
Subjects were a mean of 74 years old. Almost 80% had normal cognition as measured by the Clinical Dementia Rating Scale (CDR); the remainder had very mild cognitive impairment (CDR 0.5)
Among those with positive biomarker findings, sleep architecture was altered in several ways: lower REM latency, lower wake after sleep onset, prolonged sleep-onset latency, and longer self-reported total sleep time. The differences were evident in those with normal cognition, but even more pronounced in those with mild cognitive impairment. Despite the longer sleep times, however, sleep efficiency was decreased.
Decreased non-REM slow wave activity was associated with increased tau deposition. The protein was largely concentrated in areas of typical Alzheimer’s disease pathology (entorhinal, parahippocampal, orbital frontal, precuneus, inferior parietal, and inferior temporal regions). There were no significant associations between non-REM slow wave activity and amyloid deposits.
Other sleep parameters, however, were associated with amyloid, including REM latency and sleep latency, “suggesting that as amyloid-beta deposition increased, the time to fall asleep and enter REM sleep decreased,” the investigators said.
Those with tau pathology also slept longer, reporting more daytime naps. “This suggests that participants with greater tau pathology experienced daytime sleepiness despite increased total sleep time.”
“These results, coupled with the non-REM slow wave activity findings, suggest that the quality of sleep decreases with increasing tau despite increased sleep time.” Questions about napping should probably be included in dementia screening discussions, they said.
The study was largely funded by the National Institutes of Health. Dr. Lucey had no financial conflicts.
SOURCE: Lucey BP et al. Sci Transl Med 2019 Jan 9;11:eaau6550.
The protein was evident in areas associated with memory consolidation, typically affected in Alzheimer’s disease: the entorhinal, parahippocampal, inferior parietal, insula, isthmus cingulate, lingual, supramarginal, and orbitofrontal regions.
Because the findings were observed in a population of cognitively normal and minimally impaired subjects, they suggest a role for sleep studies in assessing the risk for cognitive decline and Alzheimer’s disease, and in monitoring patients with the disease, reported Brendan P. Lucey, MD, and his colleagues. The report is in Science and Translational Medicine (Sci Transl Med. 2019 Jan 9;11:eaau6550).
“With the rising incidence of Alzheimer’s disease in an aging population, our findings have potential application in both clinical trials and patient screening for Alzheimer’s disease to noninvasively monitor for progression of Alzheimer’s disease pathology,” wrote Dr. Lucey, director of the Sleep Medicine Center and assistant professor of neurology at Washington University in St. Louis. “For instance, periodically measuring non-REM slow wave activity, in conjunction with other biomarkers, may have utility for monitoring Alzheimer’s disease risk or response to an Alzheimer’s disease treatment.”
Dr. Lucey and his colleagues examined sleep architecture and tau and amyloid deposition in 119 subjects enrolled in longitudinal aging studies. For 6 nights, subjects slept with a single-channel EEG monitor on. They also underwent cognitive testing and genotyping for Alzheimer’s disease risk factors.
Subjects were a mean of 74 years old. Almost 80% had normal cognition as measured by the Clinical Dementia Rating Scale (CDR); the remainder had very mild cognitive impairment (CDR 0.5)
Among those with positive biomarker findings, sleep architecture was altered in several ways: lower REM latency, lower wake after sleep onset, prolonged sleep-onset latency, and longer self-reported total sleep time. The differences were evident in those with normal cognition, but even more pronounced in those with mild cognitive impairment. Despite the longer sleep times, however, sleep efficiency was decreased.
Decreased non-REM slow wave activity was associated with increased tau deposition. The protein was largely concentrated in areas of typical Alzheimer’s disease pathology (entorhinal, parahippocampal, orbital frontal, precuneus, inferior parietal, and inferior temporal regions). There were no significant associations between non-REM slow wave activity and amyloid deposits.
Other sleep parameters, however, were associated with amyloid, including REM latency and sleep latency, “suggesting that as amyloid-beta deposition increased, the time to fall asleep and enter REM sleep decreased,” the investigators said.
Those with tau pathology also slept longer, reporting more daytime naps. “This suggests that participants with greater tau pathology experienced daytime sleepiness despite increased total sleep time.”
“These results, coupled with the non-REM slow wave activity findings, suggest that the quality of sleep decreases with increasing tau despite increased sleep time.” Questions about napping should probably be included in dementia screening discussions, they said.
The study was largely funded by the National Institutes of Health. Dr. Lucey had no financial conflicts.
SOURCE: Lucey BP et al. Sci Transl Med 2019 Jan 9;11:eaau6550.
FROM SCIENCE TRANSLATIONAL MEDICINE
Key clinical point: Cognitively normal subjects with tau deposition experience altered sleep patterns.
Major finding: Decreased time in non-REM deep sleep was associated with increased tau pathology in Alzheimer’s-affected brain regions and in cerebrospinal fluid.
Study details: The prospective longitudinal study comprised 119 subjects.
Disclosures: The authors reported no relevant financial disclosures.
Source: Lucey BP et al. Sci Transl Med. 2019 Jan 9;11:eaau6550.
January 2019 Highlights

Autologous Hematopoietic Stem Cells May Treat Aggressive MS Effectively
The therapy may halt disease activity and promote sustained functional improvement.
BERLIN—Autologous hematopoietic stem cell transplantation (HSCT) could prevent disease activity and promote functional recovery in patients with aggressive multiple sclerosis (MS), according to a retrospective case series presented at ECTRIMS 2018.
A review article suggested that the likelihood of achieving no evidence of disease activity (NEDA) after two years of treatment ranges between 10% and 60%
Like other highly effective therapies, HSCT has been considered to entail significant safety risks. When the European Society for Blood and Marrow Transplantation (EBMT) reviewed their data, however, they identified one death related to HSCT between 2012 and 2016. The estimated risk of death from HSCT is thus approximately 0.2%. “Mortality associated with transplantation has decreased so much that it is almost into the range of other standard disease-modifying therapies,” said Joyutpal Das, MBBS, a neuroscientist at Royal Hallamshire Hospital in Sheffield, United Kingdom.
EBMT recommended that neurologists consider HSCT for patients with highly active radiologic and clinical disease who have failed to respond to standard disease-modifying therapy. The treatment can be considered as first-line therapy for patients with exceptionally active disease who have become disabled, they added.
A Retrospective Case Series
To examine the efficacy of HSCT in this patient population, Dr. Das and colleagues conducted a retrospective case series of 20 patients with MS from five centers in various countries. The patients’ treating physicians decided that HSCT should be their first-line therapy. Dr. Das and colleagues used NEDA-3 (which includes relapses, disability progression, and MRI activity) as their primary outcome. Each patient underwent brain MRI during the first six months of treatment and at six- to 12-month intervals thereafter.
The case series included equal numbers of men and women. All patients had frequent relapses, incomplete recovery, and multiple gadolinium enhancing lesions on serial MRI scans. The lesions often affected the brainstem, cerebellum, and spine. Patients’ median age of diagnosis and median age of treatment were 28. The time between the first onset of symptoms and treatment was nine months, and that between diagnosis and treatment was five months. Patients’ median pretreatment Expanded Disability Status Scale (EDSS) score was 6.5. Median follow-up duration was 2.5 years.
EDSS Score Improved
Three patients had new lesions during the first six months of treatment, but no patients had new lesions on subsequent MRI scans. “It has been suggested … that if you want to use NEDA to measure efficacy, the patient should have rebaseline imaging after the initiation of treatment,” said Dr. Das. “If we use our six-month scan as rebaseline imaging, then we have no further disease activity on MRI scan.”
After treatment initiation, the median EDSS score decreased from 6.5 to 2. Patients’ median improvement on EDSS score was 2.5 points, which was statistically significant. Seven patients had an EDSS score improvement of 3 points or greater. EDSS score improved for all but one patient. The results suggest that HSCT induced rapid and sustained remission, said Dr. Das.
The investigators observed typical transplant-related toxicity in the population, and no patient died. One woman conceived and gave birth to a healthy baby, and one man fathered a healthy baby.
—Erik Greb
Suggested Reading
Sormani MP, Muraro PA, Saccardi R, Mancardi G. NEDA status in highly active MS can be more easily obtained with autologous hematopoietic stem cell transplantation than other drugs. Mult Scler. 2017;23(2):201-204.
The therapy may halt disease activity and promote sustained functional improvement.
The therapy may halt disease activity and promote sustained functional improvement.
BERLIN—Autologous hematopoietic stem cell transplantation (HSCT) could prevent disease activity and promote functional recovery in patients with aggressive multiple sclerosis (MS), according to a retrospective case series presented at ECTRIMS 2018.
A review article suggested that the likelihood of achieving no evidence of disease activity (NEDA) after two years of treatment ranges between 10% and 60%
Like other highly effective therapies, HSCT has been considered to entail significant safety risks. When the European Society for Blood and Marrow Transplantation (EBMT) reviewed their data, however, they identified one death related to HSCT between 2012 and 2016. The estimated risk of death from HSCT is thus approximately 0.2%. “Mortality associated with transplantation has decreased so much that it is almost into the range of other standard disease-modifying therapies,” said Joyutpal Das, MBBS, a neuroscientist at Royal Hallamshire Hospital in Sheffield, United Kingdom.
EBMT recommended that neurologists consider HSCT for patients with highly active radiologic and clinical disease who have failed to respond to standard disease-modifying therapy. The treatment can be considered as first-line therapy for patients with exceptionally active disease who have become disabled, they added.
A Retrospective Case Series
To examine the efficacy of HSCT in this patient population, Dr. Das and colleagues conducted a retrospective case series of 20 patients with MS from five centers in various countries. The patients’ treating physicians decided that HSCT should be their first-line therapy. Dr. Das and colleagues used NEDA-3 (which includes relapses, disability progression, and MRI activity) as their primary outcome. Each patient underwent brain MRI during the first six months of treatment and at six- to 12-month intervals thereafter.
The case series included equal numbers of men and women. All patients had frequent relapses, incomplete recovery, and multiple gadolinium enhancing lesions on serial MRI scans. The lesions often affected the brainstem, cerebellum, and spine. Patients’ median age of diagnosis and median age of treatment were 28. The time between the first onset of symptoms and treatment was nine months, and that between diagnosis and treatment was five months. Patients’ median pretreatment Expanded Disability Status Scale (EDSS) score was 6.5. Median follow-up duration was 2.5 years.
EDSS Score Improved
Three patients had new lesions during the first six months of treatment, but no patients had new lesions on subsequent MRI scans. “It has been suggested … that if you want to use NEDA to measure efficacy, the patient should have rebaseline imaging after the initiation of treatment,” said Dr. Das. “If we use our six-month scan as rebaseline imaging, then we have no further disease activity on MRI scan.”
After treatment initiation, the median EDSS score decreased from 6.5 to 2. Patients’ median improvement on EDSS score was 2.5 points, which was statistically significant. Seven patients had an EDSS score improvement of 3 points or greater. EDSS score improved for all but one patient. The results suggest that HSCT induced rapid and sustained remission, said Dr. Das.
The investigators observed typical transplant-related toxicity in the population, and no patient died. One woman conceived and gave birth to a healthy baby, and one man fathered a healthy baby.
—Erik Greb
Suggested Reading
Sormani MP, Muraro PA, Saccardi R, Mancardi G. NEDA status in highly active MS can be more easily obtained with autologous hematopoietic stem cell transplantation than other drugs. Mult Scler. 2017;23(2):201-204.
BERLIN—Autologous hematopoietic stem cell transplantation (HSCT) could prevent disease activity and promote functional recovery in patients with aggressive multiple sclerosis (MS), according to a retrospective case series presented at ECTRIMS 2018.
A review article suggested that the likelihood of achieving no evidence of disease activity (NEDA) after two years of treatment ranges between 10% and 60%
Like other highly effective therapies, HSCT has been considered to entail significant safety risks. When the European Society for Blood and Marrow Transplantation (EBMT) reviewed their data, however, they identified one death related to HSCT between 2012 and 2016. The estimated risk of death from HSCT is thus approximately 0.2%. “Mortality associated with transplantation has decreased so much that it is almost into the range of other standard disease-modifying therapies,” said Joyutpal Das, MBBS, a neuroscientist at Royal Hallamshire Hospital in Sheffield, United Kingdom.
EBMT recommended that neurologists consider HSCT for patients with highly active radiologic and clinical disease who have failed to respond to standard disease-modifying therapy. The treatment can be considered as first-line therapy for patients with exceptionally active disease who have become disabled, they added.
A Retrospective Case Series
To examine the efficacy of HSCT in this patient population, Dr. Das and colleagues conducted a retrospective case series of 20 patients with MS from five centers in various countries. The patients’ treating physicians decided that HSCT should be their first-line therapy. Dr. Das and colleagues used NEDA-3 (which includes relapses, disability progression, and MRI activity) as their primary outcome. Each patient underwent brain MRI during the first six months of treatment and at six- to 12-month intervals thereafter.
The case series included equal numbers of men and women. All patients had frequent relapses, incomplete recovery, and multiple gadolinium enhancing lesions on serial MRI scans. The lesions often affected the brainstem, cerebellum, and spine. Patients’ median age of diagnosis and median age of treatment were 28. The time between the first onset of symptoms and treatment was nine months, and that between diagnosis and treatment was five months. Patients’ median pretreatment Expanded Disability Status Scale (EDSS) score was 6.5. Median follow-up duration was 2.5 years.
EDSS Score Improved
Three patients had new lesions during the first six months of treatment, but no patients had new lesions on subsequent MRI scans. “It has been suggested … that if you want to use NEDA to measure efficacy, the patient should have rebaseline imaging after the initiation of treatment,” said Dr. Das. “If we use our six-month scan as rebaseline imaging, then we have no further disease activity on MRI scan.”
After treatment initiation, the median EDSS score decreased from 6.5 to 2. Patients’ median improvement on EDSS score was 2.5 points, which was statistically significant. Seven patients had an EDSS score improvement of 3 points or greater. EDSS score improved for all but one patient. The results suggest that HSCT induced rapid and sustained remission, said Dr. Das.
The investigators observed typical transplant-related toxicity in the population, and no patient died. One woman conceived and gave birth to a healthy baby, and one man fathered a healthy baby.
—Erik Greb
Suggested Reading
Sormani MP, Muraro PA, Saccardi R, Mancardi G. NEDA status in highly active MS can be more easily obtained with autologous hematopoietic stem cell transplantation than other drugs. Mult Scler. 2017;23(2):201-204.
Interferon Beta May Not Affect Pregnancy Outcomes in MS
The rates of live births and congenital anomalies are similar between exposed and nonexposed patients.
BERLIN—European registry data do not support the hypothesis that exposure to interferon beta before conception or during pregnancy adversely affects pregnancy outcome or infant outcome, according to an analysis presented at ECTRIMS 2018.
In women, diagnosis of multiple sclerosis (MS) and treatment initiation often occur during childbearing years, but neurologists have not reached consensus about treatment before or during pregnancy. The European Interferon Beta Pregnancy Registry was created to gather evidence about the effect of this treatment on maternal and fetal outcomes. A separate population-based cohort study examined health care registry data from Finland and Sweden (ie, Nordic registries) for the same purpose.
An Analysis of Prospective Data
Kerstin Hellwig, MD, Senior Consultant Neurologist and researcher at St. Joseph and St. Elizabeth Hospital and Ruhr University in Bochum, Germany, and colleagues examined these databases to evaluate the prevalence of pregnancy and infant outcomes in women with MS who had been exposed to interferon beta. The investigators analyzed 948 pregnancy reports with recorded pregnancy outcomes from the European Interferon Beta Pregnancy Registry. They also examined 875 pregnancy events in the Nordic registries among patients exposed to interferon beta and other treatments and 1,831 events among untreated patients.
Treatment Did Not Affect Birth Weight
Approximately 82% of pregnancies in the European registry had an outcome of live birth without congenital anomalies. The prevalence of spontaneous abortions and live births with congenital anomalies were similar to those reported in the general population.
About 98% of pregnancies in the exposed cohort of the Nordic registries had an outcome of live birth without congenital anomalies. This result is similar to the corresponding 97% rate in the nonexposed cohort. The prevalence of spontaneous abortions and congenital anomalies also were similar between the exposed and nonexposed cohorts of the Nordic registries.
Birth weights ranged from 580 g to 5,160 g in the Nordic registries. The proportion of babies with low or very low birth weight was 5.0% in the interferon-exposed cohort, 4.7% among babies exposed to interferon and other treatments, and 5.8% among nonexposed babies. Mean birth weight was 3,421.2 g in the interferon-exposed cohort, 3,434.3 g in the cohort exposed to interferon and other treatments, and 3,389.3 g in the nonexposed cohort. These weights were consistent with results from the prospective German pregnancy registry, according to the authors. Birth weights were not recorded systematically in the European registry.
“The European Interferon Beta Pregnancy Registry showed no evidence that interferon beta exposure before conception or during pregnancy adversely affected pregnancy or infant outcomes,” said Dr. Hellwig and colleagues. “This is consistent with data collected from the Nordic registers.”
This study was supported by Merck in
—Erik Greb
Suggested Reading
Alroughani R, Altintas A, Al Jumah M, et al. Pregnancy and the use of disease-modifying therapies in patients with multiple sclerosis: benefits versus risks. Mult Scler Int. 2016;2016:1034912.
Friend S, Richman S, Bloomgren G, et al. Evaluation of pregnancy outcomes from the Tysabri (natalizumab) pregnancy exposure registry: a global, observational, follow-up study. BMC Neurol. 2016;16(1):150.
The rates of live births and congenital anomalies are similar between exposed and nonexposed patients.
The rates of live births and congenital anomalies are similar between exposed and nonexposed patients.
BERLIN—European registry data do not support the hypothesis that exposure to interferon beta before conception or during pregnancy adversely affects pregnancy outcome or infant outcome, according to an analysis presented at ECTRIMS 2018.
In women, diagnosis of multiple sclerosis (MS) and treatment initiation often occur during childbearing years, but neurologists have not reached consensus about treatment before or during pregnancy. The European Interferon Beta Pregnancy Registry was created to gather evidence about the effect of this treatment on maternal and fetal outcomes. A separate population-based cohort study examined health care registry data from Finland and Sweden (ie, Nordic registries) for the same purpose.
An Analysis of Prospective Data
Kerstin Hellwig, MD, Senior Consultant Neurologist and researcher at St. Joseph and St. Elizabeth Hospital and Ruhr University in Bochum, Germany, and colleagues examined these databases to evaluate the prevalence of pregnancy and infant outcomes in women with MS who had been exposed to interferon beta. The investigators analyzed 948 pregnancy reports with recorded pregnancy outcomes from the European Interferon Beta Pregnancy Registry. They also examined 875 pregnancy events in the Nordic registries among patients exposed to interferon beta and other treatments and 1,831 events among untreated patients.
Treatment Did Not Affect Birth Weight
Approximately 82% of pregnancies in the European registry had an outcome of live birth without congenital anomalies. The prevalence of spontaneous abortions and live births with congenital anomalies were similar to those reported in the general population.
About 98% of pregnancies in the exposed cohort of the Nordic registries had an outcome of live birth without congenital anomalies. This result is similar to the corresponding 97% rate in the nonexposed cohort. The prevalence of spontaneous abortions and congenital anomalies also were similar between the exposed and nonexposed cohorts of the Nordic registries.
Birth weights ranged from 580 g to 5,160 g in the Nordic registries. The proportion of babies with low or very low birth weight was 5.0% in the interferon-exposed cohort, 4.7% among babies exposed to interferon and other treatments, and 5.8% among nonexposed babies. Mean birth weight was 3,421.2 g in the interferon-exposed cohort, 3,434.3 g in the cohort exposed to interferon and other treatments, and 3,389.3 g in the nonexposed cohort. These weights were consistent with results from the prospective German pregnancy registry, according to the authors. Birth weights were not recorded systematically in the European registry.
“The European Interferon Beta Pregnancy Registry showed no evidence that interferon beta exposure before conception or during pregnancy adversely affected pregnancy or infant outcomes,” said Dr. Hellwig and colleagues. “This is consistent with data collected from the Nordic registers.”
This study was supported by Merck in
—Erik Greb
Suggested Reading
Alroughani R, Altintas A, Al Jumah M, et al. Pregnancy and the use of disease-modifying therapies in patients with multiple sclerosis: benefits versus risks. Mult Scler Int. 2016;2016:1034912.
Friend S, Richman S, Bloomgren G, et al. Evaluation of pregnancy outcomes from the Tysabri (natalizumab) pregnancy exposure registry: a global, observational, follow-up study. BMC Neurol. 2016;16(1):150.
BERLIN—European registry data do not support the hypothesis that exposure to interferon beta before conception or during pregnancy adversely affects pregnancy outcome or infant outcome, according to an analysis presented at ECTRIMS 2018.
In women, diagnosis of multiple sclerosis (MS) and treatment initiation often occur during childbearing years, but neurologists have not reached consensus about treatment before or during pregnancy. The European Interferon Beta Pregnancy Registry was created to gather evidence about the effect of this treatment on maternal and fetal outcomes. A separate population-based cohort study examined health care registry data from Finland and Sweden (ie, Nordic registries) for the same purpose.
An Analysis of Prospective Data
Kerstin Hellwig, MD, Senior Consultant Neurologist and researcher at St. Joseph and St. Elizabeth Hospital and Ruhr University in Bochum, Germany, and colleagues examined these databases to evaluate the prevalence of pregnancy and infant outcomes in women with MS who had been exposed to interferon beta. The investigators analyzed 948 pregnancy reports with recorded pregnancy outcomes from the European Interferon Beta Pregnancy Registry. They also examined 875 pregnancy events in the Nordic registries among patients exposed to interferon beta and other treatments and 1,831 events among untreated patients.
Treatment Did Not Affect Birth Weight
Approximately 82% of pregnancies in the European registry had an outcome of live birth without congenital anomalies. The prevalence of spontaneous abortions and live births with congenital anomalies were similar to those reported in the general population.
About 98% of pregnancies in the exposed cohort of the Nordic registries had an outcome of live birth without congenital anomalies. This result is similar to the corresponding 97% rate in the nonexposed cohort. The prevalence of spontaneous abortions and congenital anomalies also were similar between the exposed and nonexposed cohorts of the Nordic registries.
Birth weights ranged from 580 g to 5,160 g in the Nordic registries. The proportion of babies with low or very low birth weight was 5.0% in the interferon-exposed cohort, 4.7% among babies exposed to interferon and other treatments, and 5.8% among nonexposed babies. Mean birth weight was 3,421.2 g in the interferon-exposed cohort, 3,434.3 g in the cohort exposed to interferon and other treatments, and 3,389.3 g in the nonexposed cohort. These weights were consistent with results from the prospective German pregnancy registry, according to the authors. Birth weights were not recorded systematically in the European registry.
“The European Interferon Beta Pregnancy Registry showed no evidence that interferon beta exposure before conception or during pregnancy adversely affected pregnancy or infant outcomes,” said Dr. Hellwig and colleagues. “This is consistent with data collected from the Nordic registers.”
This study was supported by Merck in
—Erik Greb
Suggested Reading
Alroughani R, Altintas A, Al Jumah M, et al. Pregnancy and the use of disease-modifying therapies in patients with multiple sclerosis: benefits versus risks. Mult Scler Int. 2016;2016:1034912.
Friend S, Richman S, Bloomgren G, et al. Evaluation of pregnancy outcomes from the Tysabri (natalizumab) pregnancy exposure registry: a global, observational, follow-up study. BMC Neurol. 2016;16(1):150.
Alcohol use, psychological distress associated with possible RBD
(RBD), according to a population-based cohort study published in Neurology. In addition, the results also replicate previous findings of an association between possible RBD and smoking, low education, and male sex.

The risk factors for RBD have been studied comparatively little. “While much is still unknown about RBD, it can be caused by medications or it may be an early sign of another neurologic condition like Parkinson’s disease, dementia with Lewy bodies, or multiple system atrophy,” according to Ronald B. Postuma, MD, an associate professor at McGill University, Montreal. “Identifying lifestyle and personal risk factors linked to this sleep disorder may lead to finding ways to reduce the chances of developing it.”
To assess sociodemographic, socioeconomic, and clinical correlates of possible RBD, Dr. Postuma and his colleagues examined baseline data collected between 2012 and 2015 in the Canadian Longitudinal Study on Aging (CLSA), which included 30,097 participants. To screen for possible RBD, the CLSA researchers asked patients, “Have you ever been told, or suspected yourself, that you seem to ‘act out your dreams’ while asleep [e.g., punching, flailing your arms in the air, making running movements, etc.]?” Participants answered additional questions to rule out RBD mimics. Patients with symptom onset before age 20 years, positive apnea screen, or a diagnosis of dementia, Alzheimer’s disease, parkinsonism, or Parkinson’s disease were excluded from analysis.
In all, 3,271 participants screened positive for possible RBD. After the investigators excluded participants with potential mimics, 958 patients (about 3.2% of the total population) remained in the analysis. Approximately 59% of patients with possible RBD were male, compared with 42% of controls. Patients with possible RBD were more likely to be married, in a common-law relationship, or widowed.
Participants with possible RBD had slightly less education (estimated mean, 13.2 years vs. 13.6 years) and lower income, compared with controls. Participants with possible RBD retired at a slightly younger age (57.5 years vs. 58.6 years) and were more likely to have retired because of health concerns (28.9% vs. 22.0%), compared with controls.
In addition, patients with possible RBD were more likely to drink more and to be moderate to heavy drinkers than controls; they were also more likely to be current or past smokers. Antidepressant use was more frequent and psychological distress was greater among participants with possible RBD.
When the investigators performed a multivariable logistic regression analysis, the associations between possible RBD and male sex and relationship status remained. Lower educational level, but not income level, also remained associated with possible RBD. Furthermore, retirement age and having reported retirement because of health concerns remained significantly associated with possible RBD, as did the amount of alcohol consumed weekly and moderate to heavy drinking. Sensitivity analyses did not change the results significantly.
One of the study’s limitations is its reliance on self-report to identify participants with possible RBD, the authors wrote. The prevalence of possible RBD in the study was 3.2%, but research using polysomnography has found a prevalence of about 1%. Thus, the majority of cases in this study may have other disorders such as restless legs syndrome or periodic limb movements. Furthermore, many participants who enact their dreams (such as unmarried people) are likely unaware of it. Finally, the researchers did not measure several variables of interest, such as consumption of caffeinated products.
“The main advantages of our current study are the large sample size; the systematic population-based sampling; the capacity to adjust for diverse potential confounding variables, including mental illness; and the ability to screen out RBD mimics,” the authors concluded.
SOURCE: Postuma RB et al. Neurology. 2018 Dec 26. doi: 10.1212/WNL.0000000000006849.
(RBD), according to a population-based cohort study published in Neurology. In addition, the results also replicate previous findings of an association between possible RBD and smoking, low education, and male sex.
The risk factors for RBD have been studied comparatively little. “While much is still unknown about RBD, it can be caused by medications or it may be an early sign of another neurologic condition like Parkinson’s disease, dementia with Lewy bodies, or multiple system atrophy,” according to Ronald B. Postuma, MD, an associate professor at McGill University, Montreal. “Identifying lifestyle and personal risk factors linked to this sleep disorder may lead to finding ways to reduce the chances of developing it.”
To assess sociodemographic, socioeconomic, and clinical correlates of possible RBD, Dr. Postuma and his colleagues examined baseline data collected between 2012 and 2015 in the Canadian Longitudinal Study on Aging (CLSA), which included 30,097 participants. To screen for possible RBD, the CLSA researchers asked patients, “Have you ever been told, or suspected yourself, that you seem to ‘act out your dreams’ while asleep [e.g., punching, flailing your arms in the air, making running movements, etc.]?” Participants answered additional questions to rule out RBD mimics. Patients with symptom onset before age 20 years, positive apnea screen, or a diagnosis of dementia, Alzheimer’s disease, parkinsonism, or Parkinson’s disease were excluded from analysis.
In all, 3,271 participants screened positive for possible RBD. After the investigators excluded participants with potential mimics, 958 patients (about 3.2% of the total population) remained in the analysis. Approximately 59% of patients with possible RBD were male, compared with 42% of controls. Patients with possible RBD were more likely to be married, in a common-law relationship, or widowed.
Participants with possible RBD had slightly less education (estimated mean, 13.2 years vs. 13.6 years) and lower income, compared with controls. Participants with possible RBD retired at a slightly younger age (57.5 years vs. 58.6 years) and were more likely to have retired because of health concerns (28.9% vs. 22.0%), compared with controls.
In addition, patients with possible RBD were more likely to drink more and to be moderate to heavy drinkers than controls; they were also more likely to be current or past smokers. Antidepressant use was more frequent and psychological distress was greater among participants with possible RBD.
When the investigators performed a multivariable logistic regression analysis, the associations between possible RBD and male sex and relationship status remained. Lower educational level, but not income level, also remained associated with possible RBD. Furthermore, retirement age and having reported retirement because of health concerns remained significantly associated with possible RBD, as did the amount of alcohol consumed weekly and moderate to heavy drinking. Sensitivity analyses did not change the results significantly.
One of the study’s limitations is its reliance on self-report to identify participants with possible RBD, the authors wrote. The prevalence of possible RBD in the study was 3.2%, but research using polysomnography has found a prevalence of about 1%. Thus, the majority of cases in this study may have other disorders such as restless legs syndrome or periodic limb movements. Furthermore, many participants who enact their dreams (such as unmarried people) are likely unaware of it. Finally, the researchers did not measure several variables of interest, such as consumption of caffeinated products.
“The main advantages of our current study are the large sample size; the systematic population-based sampling; the capacity to adjust for diverse potential confounding variables, including mental illness; and the ability to screen out RBD mimics,” the authors concluded.
SOURCE: Postuma RB et al. Neurology. 2018 Dec 26. doi: 10.1212/WNL.0000000000006849.
(RBD), according to a population-based cohort study published in Neurology. In addition, the results also replicate previous findings of an association between possible RBD and smoking, low education, and male sex.
The risk factors for RBD have been studied comparatively little. “While much is still unknown about RBD, it can be caused by medications or it may be an early sign of another neurologic condition like Parkinson’s disease, dementia with Lewy bodies, or multiple system atrophy,” according to Ronald B. Postuma, MD, an associate professor at McGill University, Montreal. “Identifying lifestyle and personal risk factors linked to this sleep disorder may lead to finding ways to reduce the chances of developing it.”
To assess sociodemographic, socioeconomic, and clinical correlates of possible RBD, Dr. Postuma and his colleagues examined baseline data collected between 2012 and 2015 in the Canadian Longitudinal Study on Aging (CLSA), which included 30,097 participants. To screen for possible RBD, the CLSA researchers asked patients, “Have you ever been told, or suspected yourself, that you seem to ‘act out your dreams’ while asleep [e.g., punching, flailing your arms in the air, making running movements, etc.]?” Participants answered additional questions to rule out RBD mimics. Patients with symptom onset before age 20 years, positive apnea screen, or a diagnosis of dementia, Alzheimer’s disease, parkinsonism, or Parkinson’s disease were excluded from analysis.
In all, 3,271 participants screened positive for possible RBD. After the investigators excluded participants with potential mimics, 958 patients (about 3.2% of the total population) remained in the analysis. Approximately 59% of patients with possible RBD were male, compared with 42% of controls. Patients with possible RBD were more likely to be married, in a common-law relationship, or widowed.
Participants with possible RBD had slightly less education (estimated mean, 13.2 years vs. 13.6 years) and lower income, compared with controls. Participants with possible RBD retired at a slightly younger age (57.5 years vs. 58.6 years) and were more likely to have retired because of health concerns (28.9% vs. 22.0%), compared with controls.
In addition, patients with possible RBD were more likely to drink more and to be moderate to heavy drinkers than controls; they were also more likely to be current or past smokers. Antidepressant use was more frequent and psychological distress was greater among participants with possible RBD.
When the investigators performed a multivariable logistic regression analysis, the associations between possible RBD and male sex and relationship status remained. Lower educational level, but not income level, also remained associated with possible RBD. Furthermore, retirement age and having reported retirement because of health concerns remained significantly associated with possible RBD, as did the amount of alcohol consumed weekly and moderate to heavy drinking. Sensitivity analyses did not change the results significantly.
One of the study’s limitations is its reliance on self-report to identify participants with possible RBD, the authors wrote. The prevalence of possible RBD in the study was 3.2%, but research using polysomnography has found a prevalence of about 1%. Thus, the majority of cases in this study may have other disorders such as restless legs syndrome or periodic limb movements. Furthermore, many participants who enact their dreams (such as unmarried people) are likely unaware of it. Finally, the researchers did not measure several variables of interest, such as consumption of caffeinated products.
“The main advantages of our current study are the large sample size; the systematic population-based sampling; the capacity to adjust for diverse potential confounding variables, including mental illness; and the ability to screen out RBD mimics,” the authors concluded.
SOURCE: Postuma RB et al. Neurology. 2018 Dec 26. doi: 10.1212/WNL.0000000000006849.
FROM NEUROLOGY
Key clinical point: Alcohol use and psychological distress are associated with possible REM sleep behavior disorder.
Major finding: A self-report questionnaire yielded a 3.2% prevalence of possible REM sleep behavior disorder.
Study details: A prospective, population-based cohort study of 30,097 participants.
Disclosures: The Canadian government provided funding for the research.
Source: Postuma RB et al. Neurology. 2018 Dec 26. doi: 10.1212/WNL.0000000000006849.
ACOG updates guidance on chronic hypertension in pregnancy, gestational hypertension
Ob.gyns. will need to focus more on individualized care as they use the two new practice bulletins, one on chronic hypertension in pregnancy and one on gestational hypertension and preeclampsia, released by the American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins–Obstetrics.

The bulletins will replace the 2013 ACOG hypertension in pregnancy task force report and are published in the January issue of Obstetrics & Gynecology.
“The task force was a tour de force in creating a comprehensive view of hypertensive diseases of pregnancy, including research,” Christian M. Pettker, MD, who helped develop both practice bulletins, stated in a press release. “The updated guidance provides clearer recommendations for the management of gestational hypertension with severe-range blood pressure, an emphasis on and instructions for timely treatment of acutely elevated blood pressures, and more defined recommendations for the management of pain in postoperative patients with hypertension.”
“Ob.gyns. will need to focus more on individualized care and may find it’s best to err on the side of caution because the appropriate treatment of hypertensive diseases in pregnancy may be the most important focus of our attempts to improve maternal mortality and morbidity in the United States,” he said.*
Gestational hypertension or preeclampsia
For women with gestational hypertension or preeclampsia at 37 weeks of gestation or later without severe features, the guidelines recommend delivery rather than expectant management.
Those patients with severe features of gestational hypertension or preeclampsia or eclampsia should receive magnesium sulfate to prevent or treat seizures.
Patients should receive low-dose aspirin (81 mg/day) for preeclampsia prophylaxis between 12 weeks and 28 weeks of gestation if they have high-risk factors of preeclampsia such as multifetal gestation, a previous pregnancy with preeclampsia, renal disease, autoimmune disease, type 1 or type 2 diabetes mellitus, chronic hypertension, or a previous pregnancy with preeclampsia; or more than one moderate risk factor such as a family history of preeclampsia, maternal age greater than 35 years, first pregnancy, body mass index greater than 30, personal history factors, or sociodemographic characteristics.
NSAIDs should continue to be used in preference to opioid analgesics.
The guidance also discusses mode of delivery, antihypertensive drugs and thresholds for treatment, management of acute complications for preeclampsia with HELLP (hemolysis, elevated liver enzymes, low platelet count) syndrome, the optimal treatment for eclampsia, and postpartum hypertension and headache.
Chronic hypertension
Pregnant women with chronic hypertension also should receive low-dose aspirin between 12 weeks and 28 weeks of gestation. Antihypertensive therapy should be initiated for women with persistent chronic hypertension at systolic pressure of 160 mm Hg or higher and/or diastolic pressure of 110 mm Hg or higher. Consider treating patients at lower blood pressure (BP) thresholds depending on comorbidities or underlying impaired renal function.
ACOG has recommended treating pregnant patients as chronically hypertensive according to recently changed criteria from the American College of Cardiology and the American Heart Association, which call for classifying blood pressure into the following categories:
- Normal. Systolic BP less than 120 mm Hg; diastolic BP less than 80 mm Hg.
- Elevated. Systolic BP greater than or equal to 120-129 mm Hg; diastolic BP greater than 80 mm Hg.
- Stage 1 hypertension. Systolic BP, 130-139 mm Hg; diastolic BP, 80-89 mm Hg.
- Stage 2 hypertension. Systolic BP greater than or equal to 140 mm Hg; diastolic BP greater than or equal to 90 mm Hg.
“The new blood pressure ranges for nonpregnant women have a lower threshold for hypertension diagnosis compared to ACOG’s criteria,” Dr. Pettker said. “This will likely cause a general increase in patients classified as chronic hypertensive and will require shared decision making by the ob.gyn. and the patient regarding appropriate management in pregnancy.”
The guideline also discusses chronic hypertension with superimposed preeclampsia; tests for baseline evaluation of chronic hypertension in pregnancy; common oral antihypertensive agents to use in pregnancy and those to use for urgent blood pressure control in pregnancy; control of acute-onset severe-range hypertension; and postpartum considerations in patients with chronic hypertension.
SOURCE: Gestational hypertension and preeclampsia. ACOG Practice Bulletin No. 202. Obstet Gynecol. 2019;133:e1-25; Chronic hypertension in pregnancy. ACOG Practice Bulletin No. 203. Obstet Gynecol. 2019;133:e26-50.
This article was updated 1/11/19 and 11/19/19.
Ob.gyns. will need to focus more on individualized care as they use the two new practice bulletins, one on chronic hypertension in pregnancy and one on gestational hypertension and preeclampsia, released by the American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins–Obstetrics.
The bulletins will replace the 2013 ACOG hypertension in pregnancy task force report and are published in the January issue of Obstetrics & Gynecology.
“The task force was a tour de force in creating a comprehensive view of hypertensive diseases of pregnancy, including research,” Christian M. Pettker, MD, who helped develop both practice bulletins, stated in a press release. “The updated guidance provides clearer recommendations for the management of gestational hypertension with severe-range blood pressure, an emphasis on and instructions for timely treatment of acutely elevated blood pressures, and more defined recommendations for the management of pain in postoperative patients with hypertension.”
“Ob.gyns. will need to focus more on individualized care and may find it’s best to err on the side of caution because the appropriate treatment of hypertensive diseases in pregnancy may be the most important focus of our attempts to improve maternal mortality and morbidity in the United States,” he said.*
Gestational hypertension or preeclampsia
For women with gestational hypertension or preeclampsia at 37 weeks of gestation or later without severe features, the guidelines recommend delivery rather than expectant management.
Those patients with severe features of gestational hypertension or preeclampsia or eclampsia should receive magnesium sulfate to prevent or treat seizures.
Patients should receive low-dose aspirin (81 mg/day) for preeclampsia prophylaxis between 12 weeks and 28 weeks of gestation if they have high-risk factors of preeclampsia such as multifetal gestation, a previous pregnancy with preeclampsia, renal disease, autoimmune disease, type 1 or type 2 diabetes mellitus, chronic hypertension, or a previous pregnancy with preeclampsia; or more than one moderate risk factor such as a family history of preeclampsia, maternal age greater than 35 years, first pregnancy, body mass index greater than 30, personal history factors, or sociodemographic characteristics.
NSAIDs should continue to be used in preference to opioid analgesics.
The guidance also discusses mode of delivery, antihypertensive drugs and thresholds for treatment, management of acute complications for preeclampsia with HELLP (hemolysis, elevated liver enzymes, low platelet count) syndrome, the optimal treatment for eclampsia, and postpartum hypertension and headache.
Chronic hypertension
Pregnant women with chronic hypertension also should receive low-dose aspirin between 12 weeks and 28 weeks of gestation. Antihypertensive therapy should be initiated for women with persistent chronic hypertension at systolic pressure of 160 mm Hg or higher and/or diastolic pressure of 110 mm Hg or higher. Consider treating patients at lower blood pressure (BP) thresholds depending on comorbidities or underlying impaired renal function.
ACOG has recommended treating pregnant patients as chronically hypertensive according to recently changed criteria from the American College of Cardiology and the American Heart Association, which call for classifying blood pressure into the following categories:
- Normal. Systolic BP less than 120 mm Hg; diastolic BP less than 80 mm Hg.
- Elevated. Systolic BP greater than or equal to 120-129 mm Hg; diastolic BP greater than 80 mm Hg.
- Stage 1 hypertension. Systolic BP, 130-139 mm Hg; diastolic BP, 80-89 mm Hg.
- Stage 2 hypertension. Systolic BP greater than or equal to 140 mm Hg; diastolic BP greater than or equal to 90 mm Hg.
“The new blood pressure ranges for nonpregnant women have a lower threshold for hypertension diagnosis compared to ACOG’s criteria,” Dr. Pettker said. “This will likely cause a general increase in patients classified as chronic hypertensive and will require shared decision making by the ob.gyn. and the patient regarding appropriate management in pregnancy.”
The guideline also discusses chronic hypertension with superimposed preeclampsia; tests for baseline evaluation of chronic hypertension in pregnancy; common oral antihypertensive agents to use in pregnancy and those to use for urgent blood pressure control in pregnancy; control of acute-onset severe-range hypertension; and postpartum considerations in patients with chronic hypertension.
SOURCE: Gestational hypertension and preeclampsia. ACOG Practice Bulletin No. 202. Obstet Gynecol. 2019;133:e1-25; Chronic hypertension in pregnancy. ACOG Practice Bulletin No. 203. Obstet Gynecol. 2019;133:e26-50.
This article was updated 1/11/19 and 11/19/19.
Ob.gyns. will need to focus more on individualized care as they use the two new practice bulletins, one on chronic hypertension in pregnancy and one on gestational hypertension and preeclampsia, released by the American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins–Obstetrics.
The bulletins will replace the 2013 ACOG hypertension in pregnancy task force report and are published in the January issue of Obstetrics & Gynecology.
“The task force was a tour de force in creating a comprehensive view of hypertensive diseases of pregnancy, including research,” Christian M. Pettker, MD, who helped develop both practice bulletins, stated in a press release. “The updated guidance provides clearer recommendations for the management of gestational hypertension with severe-range blood pressure, an emphasis on and instructions for timely treatment of acutely elevated blood pressures, and more defined recommendations for the management of pain in postoperative patients with hypertension.”
“Ob.gyns. will need to focus more on individualized care and may find it’s best to err on the side of caution because the appropriate treatment of hypertensive diseases in pregnancy may be the most important focus of our attempts to improve maternal mortality and morbidity in the United States,” he said.*
Gestational hypertension or preeclampsia
For women with gestational hypertension or preeclampsia at 37 weeks of gestation or later without severe features, the guidelines recommend delivery rather than expectant management.
Those patients with severe features of gestational hypertension or preeclampsia or eclampsia should receive magnesium sulfate to prevent or treat seizures.
Patients should receive low-dose aspirin (81 mg/day) for preeclampsia prophylaxis between 12 weeks and 28 weeks of gestation if they have high-risk factors of preeclampsia such as multifetal gestation, a previous pregnancy with preeclampsia, renal disease, autoimmune disease, type 1 or type 2 diabetes mellitus, chronic hypertension, or a previous pregnancy with preeclampsia; or more than one moderate risk factor such as a family history of preeclampsia, maternal age greater than 35 years, first pregnancy, body mass index greater than 30, personal history factors, or sociodemographic characteristics.
NSAIDs should continue to be used in preference to opioid analgesics.
The guidance also discusses mode of delivery, antihypertensive drugs and thresholds for treatment, management of acute complications for preeclampsia with HELLP (hemolysis, elevated liver enzymes, low platelet count) syndrome, the optimal treatment for eclampsia, and postpartum hypertension and headache.
Chronic hypertension
Pregnant women with chronic hypertension also should receive low-dose aspirin between 12 weeks and 28 weeks of gestation. Antihypertensive therapy should be initiated for women with persistent chronic hypertension at systolic pressure of 160 mm Hg or higher and/or diastolic pressure of 110 mm Hg or higher. Consider treating patients at lower blood pressure (BP) thresholds depending on comorbidities or underlying impaired renal function.
ACOG has recommended treating pregnant patients as chronically hypertensive according to recently changed criteria from the American College of Cardiology and the American Heart Association, which call for classifying blood pressure into the following categories:
- Normal. Systolic BP less than 120 mm Hg; diastolic BP less than 80 mm Hg.
- Elevated. Systolic BP greater than or equal to 120-129 mm Hg; diastolic BP greater than 80 mm Hg.
- Stage 1 hypertension. Systolic BP, 130-139 mm Hg; diastolic BP, 80-89 mm Hg.
- Stage 2 hypertension. Systolic BP greater than or equal to 140 mm Hg; diastolic BP greater than or equal to 90 mm Hg.
“The new blood pressure ranges for nonpregnant women have a lower threshold for hypertension diagnosis compared to ACOG’s criteria,” Dr. Pettker said. “This will likely cause a general increase in patients classified as chronic hypertensive and will require shared decision making by the ob.gyn. and the patient regarding appropriate management in pregnancy.”
The guideline also discusses chronic hypertension with superimposed preeclampsia; tests for baseline evaluation of chronic hypertension in pregnancy; common oral antihypertensive agents to use in pregnancy and those to use for urgent blood pressure control in pregnancy; control of acute-onset severe-range hypertension; and postpartum considerations in patients with chronic hypertension.
SOURCE: Gestational hypertension and preeclampsia. ACOG Practice Bulletin No. 202. Obstet Gynecol. 2019;133:e1-25; Chronic hypertension in pregnancy. ACOG Practice Bulletin No. 203. Obstet Gynecol. 2019;133:e26-50.
This article was updated 1/11/19 and 11/19/19.
FROM OBSTETRICS & GYNECOLOGY
Heberden’s nodes linked to knee OA progression
according to a review of 575 participants in a substudy of the Osteoarthritis Initiative cohort.
After assessing Heberden’s nodes (HNs) – bony enlargements of the last finger joint – and knee MRI findings at baseline and 24 months, the investigators found that HNs were associated with periarticular bone area expansion in the knee. The investigators reported their findings in Arthritis & Rheumatology.

Comparing the 395 subjects with HNs with the 180 without, there was more periarticular bone area expansion among HN patients at 2 years in the knee joint (adjusted odds ratio, 1.39; 95% confidence interval, 1.06-1.83), especially in the medial femur (aOR, 1.49; 95% CI, 1.05-2.13), lateral femur (aOR, 2.51; 95% CI, 1.58-3.97), femoral notch (aOR, 1.37; 95% CI, 1.02-1.84), and lateral trochlea (aOR, 1.44; 95% CI, 1.08-1.9). The comparisons were adjusted for age, sex, body mass index, and bone remodeling agent use.
“The presence of Heberden’s nodes in a physical examination is associated with a distinct pattern of worsening of osteoarthritis-related structural damage in the knee joint,” lead investigator Arya Haj-Mirzaian, MD, a radiologist and postdoctoral fellow at Johns Hopkins University, Baltimore, said in a press release.
However, HNs were also associated with less worsening of knee osteophytes, especially at the femoral end of the knee joint (aOR, 0.54; 95% CI, 0.31-0.95); the finding seemed to contradict the overall picture of worsening knee osteoarthritis with HNs.
“Although osteophytes are thought to be a late secondary sequel or compensatory repair mechanism in OA and indicator of advanced knee OA, less worsening in osteophytes’ score ... may propose that less ossification is involved in the pathophysiology of knee OA in the presence of HNs,” the investigators wrote. It’s a subject for future research.
Patients with HNs were older, more often female, and had a lower frequency for other knee OA risk factors, such as excessive body mass index and knee injury. Patients with gout were excluded.
There was no external funding, and the investigators reported no disclosures.
SOURCE: Haj-Mirzaian A et al. Arthritis Rheumatol. 2019 Jan 9. doi: 10.1002/art.40811.
according to a review of 575 participants in a substudy of the Osteoarthritis Initiative cohort.
After assessing Heberden’s nodes (HNs) – bony enlargements of the last finger joint – and knee MRI findings at baseline and 24 months, the investigators found that HNs were associated with periarticular bone area expansion in the knee. The investigators reported their findings in Arthritis & Rheumatology.
Comparing the 395 subjects with HNs with the 180 without, there was more periarticular bone area expansion among HN patients at 2 years in the knee joint (adjusted odds ratio, 1.39; 95% confidence interval, 1.06-1.83), especially in the medial femur (aOR, 1.49; 95% CI, 1.05-2.13), lateral femur (aOR, 2.51; 95% CI, 1.58-3.97), femoral notch (aOR, 1.37; 95% CI, 1.02-1.84), and lateral trochlea (aOR, 1.44; 95% CI, 1.08-1.9). The comparisons were adjusted for age, sex, body mass index, and bone remodeling agent use.
“The presence of Heberden’s nodes in a physical examination is associated with a distinct pattern of worsening of osteoarthritis-related structural damage in the knee joint,” lead investigator Arya Haj-Mirzaian, MD, a radiologist and postdoctoral fellow at Johns Hopkins University, Baltimore, said in a press release.
However, HNs were also associated with less worsening of knee osteophytes, especially at the femoral end of the knee joint (aOR, 0.54; 95% CI, 0.31-0.95); the finding seemed to contradict the overall picture of worsening knee osteoarthritis with HNs.
“Although osteophytes are thought to be a late secondary sequel or compensatory repair mechanism in OA and indicator of advanced knee OA, less worsening in osteophytes’ score ... may propose that less ossification is involved in the pathophysiology of knee OA in the presence of HNs,” the investigators wrote. It’s a subject for future research.
Patients with HNs were older, more often female, and had a lower frequency for other knee OA risk factors, such as excessive body mass index and knee injury. Patients with gout were excluded.
There was no external funding, and the investigators reported no disclosures.
SOURCE: Haj-Mirzaian A et al. Arthritis Rheumatol. 2019 Jan 9. doi: 10.1002/art.40811.
according to a review of 575 participants in a substudy of the Osteoarthritis Initiative cohort.
After assessing Heberden’s nodes (HNs) – bony enlargements of the last finger joint – and knee MRI findings at baseline and 24 months, the investigators found that HNs were associated with periarticular bone area expansion in the knee. The investigators reported their findings in Arthritis & Rheumatology.
Comparing the 395 subjects with HNs with the 180 without, there was more periarticular bone area expansion among HN patients at 2 years in the knee joint (adjusted odds ratio, 1.39; 95% confidence interval, 1.06-1.83), especially in the medial femur (aOR, 1.49; 95% CI, 1.05-2.13), lateral femur (aOR, 2.51; 95% CI, 1.58-3.97), femoral notch (aOR, 1.37; 95% CI, 1.02-1.84), and lateral trochlea (aOR, 1.44; 95% CI, 1.08-1.9). The comparisons were adjusted for age, sex, body mass index, and bone remodeling agent use.
“The presence of Heberden’s nodes in a physical examination is associated with a distinct pattern of worsening of osteoarthritis-related structural damage in the knee joint,” lead investigator Arya Haj-Mirzaian, MD, a radiologist and postdoctoral fellow at Johns Hopkins University, Baltimore, said in a press release.
However, HNs were also associated with less worsening of knee osteophytes, especially at the femoral end of the knee joint (aOR, 0.54; 95% CI, 0.31-0.95); the finding seemed to contradict the overall picture of worsening knee osteoarthritis with HNs.
“Although osteophytes are thought to be a late secondary sequel or compensatory repair mechanism in OA and indicator of advanced knee OA, less worsening in osteophytes’ score ... may propose that less ossification is involved in the pathophysiology of knee OA in the presence of HNs,” the investigators wrote. It’s a subject for future research.
Patients with HNs were older, more often female, and had a lower frequency for other knee OA risk factors, such as excessive body mass index and knee injury. Patients with gout were excluded.
There was no external funding, and the investigators reported no disclosures.
SOURCE: Haj-Mirzaian A et al. Arthritis Rheumatol. 2019 Jan 9. doi: 10.1002/art.40811.
FROM ARTHRITIS & RHEUMATOLOGY
Key clinical point: Heberden’s nodes may be an indicator of knee OA progression.
Major finding: There was more periarticular bone area expansion among patients with Heberden’s nodes at 2 years in the knee joint (adjusted odds ratio, 1.39; 95% confidence interval, 1.06-1.83).
Study details: A substudy of 575 participants in the Osteoarthritis Initiative cohort
Disclosures: There was no external funding, and the investigators reported no disclosures.
Source: Haj-Mirzaian A et al. Arthritis Rheumatol. 2019 Jan 9. doi: 10.1002/art.40811.
Remote Canadian province has unusual prevalence of hereditary bleeding disorders
Isolated communities in the Canadian province of Newfoundland and Labrador have an “unusual prevalence” of certain hereditary bleeding disorders, a fact attributable to the province’s unique topography and settlement patterns, according to a new study.

The prevalence of hemophilia A in Newfoundland and Labrador (NL) is 2.89 times higher than in the rest of Canada. Deficiencies in Factors V, XI, and XIII are 4.54, 5.44, and 9.22 times more prevalent in NL than mainland Canada, respectively. The study also found more cases than expected of the extremely rare hereditary bleeding disorder, Glanzmann thrombasthenia (n = 4). One case of Bernard-Soulier syndrome was also seen, the investigators reported in Transfusion and Apheresis Science.
“This comparatively high prevalence provides a potential pool of patients for genotype/phenotype research,” wrote Mary-Frances Scully, MD, a hematologist at Memorial University, St. John’s, Nfld., and her associates.
In addition to founding populations of indigenous Innu, Inuit, and Mi’kmaq populations, present-day residents of Canada’s easternmost province trace their lineages to about 28,000 settlers who came from southwest England and southeast Ireland for the area’s rich fisheries, explained Dr. Scully and her coauthors. The overall population density of NL is still very low, at about 1.38 individuals per square kilometer, less than half that of Canada overall and far less than the United States’ 36 per square kilometer.
Overall, the investigators reviewed records for 180 patients with hereditary bleeding disorders who were receiving specialty care in St. John’s. Most (n = 127) had hemophilia A; of these patients, those who had mutation testing primarily had the Val 2016A1 mutation. This was particularly true for patients with mild hemophilia A. More than 73% (83/111 patients) carried this mutation, demonstrating a founder effect, wrote Dr. Scully and her coauthors. The next most common hereditary bleeding disorder was Factor XI deficiency, seen in 29 patients.
Additionally, of the seven patients with Factor XIII deficiency, five were homozygous for the c.691-1 G greater than A mutation.
More males in NL than in global comparator data had Factor V deficiency and Glanzmann thrombasthenia, though Dr. Scully and her colleagues acknowledged that the numbers were low overall.
Coagulation tests performed at the time of diagnosis and before treatment initiation were used, when available, to ascertain the severity of the bleeding disorder. Patients were included whether they were heterozygous or homozygous for hereditary bleeding disorders, so long as their baseline coagulation factor levels were below predetermined cutoff levels.
Comparing the prevalence of all the hereditary bleeding disorders identified in the NL population against mainland Canada and that of four other reference countries – Iran, Ireland, the United Kingdom, and the United States – the increased prevalence rates in NL were highly statistically significant (P less than .0001) for all but the single case of Bernard-Soulier syndrome.
Hemophilia B was the only hereditary bleeding disorder seen less frequently in the NL population than in Canada or the other reference populations.
“These results show that NL’s unique geography and population distribution led to a genetic drift that increased the prevalence of some rare factor deficiencies,” wrote Dr. Scully and her colleagues.
The investigators plan to continue investigating and reporting genotype and phenotype correlations among their patient population; they also invite broader international collaboration into the prevalence of rare hereditary bleeding disorders in isolated populations.
The authors reported having no conflicts of interest and no outside sources of funding.
SOURCE: Scully M-F et al. Transfus Apher Sci. 2018 Dec;57(6):713-6.
Isolated communities in the Canadian province of Newfoundland and Labrador have an “unusual prevalence” of certain hereditary bleeding disorders, a fact attributable to the province’s unique topography and settlement patterns, according to a new study.
The prevalence of hemophilia A in Newfoundland and Labrador (NL) is 2.89 times higher than in the rest of Canada. Deficiencies in Factors V, XI, and XIII are 4.54, 5.44, and 9.22 times more prevalent in NL than mainland Canada, respectively. The study also found more cases than expected of the extremely rare hereditary bleeding disorder, Glanzmann thrombasthenia (n = 4). One case of Bernard-Soulier syndrome was also seen, the investigators reported in Transfusion and Apheresis Science.
“This comparatively high prevalence provides a potential pool of patients for genotype/phenotype research,” wrote Mary-Frances Scully, MD, a hematologist at Memorial University, St. John’s, Nfld., and her associates.
In addition to founding populations of indigenous Innu, Inuit, and Mi’kmaq populations, present-day residents of Canada’s easternmost province trace their lineages to about 28,000 settlers who came from southwest England and southeast Ireland for the area’s rich fisheries, explained Dr. Scully and her coauthors. The overall population density of NL is still very low, at about 1.38 individuals per square kilometer, less than half that of Canada overall and far less than the United States’ 36 per square kilometer.
Overall, the investigators reviewed records for 180 patients with hereditary bleeding disorders who were receiving specialty care in St. John’s. Most (n = 127) had hemophilia A; of these patients, those who had mutation testing primarily had the Val 2016A1 mutation. This was particularly true for patients with mild hemophilia A. More than 73% (83/111 patients) carried this mutation, demonstrating a founder effect, wrote Dr. Scully and her coauthors. The next most common hereditary bleeding disorder was Factor XI deficiency, seen in 29 patients.
Additionally, of the seven patients with Factor XIII deficiency, five were homozygous for the c.691-1 G greater than A mutation.
More males in NL than in global comparator data had Factor V deficiency and Glanzmann thrombasthenia, though Dr. Scully and her colleagues acknowledged that the numbers were low overall.
Coagulation tests performed at the time of diagnosis and before treatment initiation were used, when available, to ascertain the severity of the bleeding disorder. Patients were included whether they were heterozygous or homozygous for hereditary bleeding disorders, so long as their baseline coagulation factor levels were below predetermined cutoff levels.
Comparing the prevalence of all the hereditary bleeding disorders identified in the NL population against mainland Canada and that of four other reference countries – Iran, Ireland, the United Kingdom, and the United States – the increased prevalence rates in NL were highly statistically significant (P less than .0001) for all but the single case of Bernard-Soulier syndrome.
Hemophilia B was the only hereditary bleeding disorder seen less frequently in the NL population than in Canada or the other reference populations.
“These results show that NL’s unique geography and population distribution led to a genetic drift that increased the prevalence of some rare factor deficiencies,” wrote Dr. Scully and her colleagues.
The investigators plan to continue investigating and reporting genotype and phenotype correlations among their patient population; they also invite broader international collaboration into the prevalence of rare hereditary bleeding disorders in isolated populations.
The authors reported having no conflicts of interest and no outside sources of funding.
SOURCE: Scully M-F et al. Transfus Apher Sci. 2018 Dec;57(6):713-6.
Isolated communities in the Canadian province of Newfoundland and Labrador have an “unusual prevalence” of certain hereditary bleeding disorders, a fact attributable to the province’s unique topography and settlement patterns, according to a new study.
The prevalence of hemophilia A in Newfoundland and Labrador (NL) is 2.89 times higher than in the rest of Canada. Deficiencies in Factors V, XI, and XIII are 4.54, 5.44, and 9.22 times more prevalent in NL than mainland Canada, respectively. The study also found more cases than expected of the extremely rare hereditary bleeding disorder, Glanzmann thrombasthenia (n = 4). One case of Bernard-Soulier syndrome was also seen, the investigators reported in Transfusion and Apheresis Science.
“This comparatively high prevalence provides a potential pool of patients for genotype/phenotype research,” wrote Mary-Frances Scully, MD, a hematologist at Memorial University, St. John’s, Nfld., and her associates.
In addition to founding populations of indigenous Innu, Inuit, and Mi’kmaq populations, present-day residents of Canada’s easternmost province trace their lineages to about 28,000 settlers who came from southwest England and southeast Ireland for the area’s rich fisheries, explained Dr. Scully and her coauthors. The overall population density of NL is still very low, at about 1.38 individuals per square kilometer, less than half that of Canada overall and far less than the United States’ 36 per square kilometer.
Overall, the investigators reviewed records for 180 patients with hereditary bleeding disorders who were receiving specialty care in St. John’s. Most (n = 127) had hemophilia A; of these patients, those who had mutation testing primarily had the Val 2016A1 mutation. This was particularly true for patients with mild hemophilia A. More than 73% (83/111 patients) carried this mutation, demonstrating a founder effect, wrote Dr. Scully and her coauthors. The next most common hereditary bleeding disorder was Factor XI deficiency, seen in 29 patients.
Additionally, of the seven patients with Factor XIII deficiency, five were homozygous for the c.691-1 G greater than A mutation.
More males in NL than in global comparator data had Factor V deficiency and Glanzmann thrombasthenia, though Dr. Scully and her colleagues acknowledged that the numbers were low overall.
Coagulation tests performed at the time of diagnosis and before treatment initiation were used, when available, to ascertain the severity of the bleeding disorder. Patients were included whether they were heterozygous or homozygous for hereditary bleeding disorders, so long as their baseline coagulation factor levels were below predetermined cutoff levels.
Comparing the prevalence of all the hereditary bleeding disorders identified in the NL population against mainland Canada and that of four other reference countries – Iran, Ireland, the United Kingdom, and the United States – the increased prevalence rates in NL were highly statistically significant (P less than .0001) for all but the single case of Bernard-Soulier syndrome.
Hemophilia B was the only hereditary bleeding disorder seen less frequently in the NL population than in Canada or the other reference populations.
“These results show that NL’s unique geography and population distribution led to a genetic drift that increased the prevalence of some rare factor deficiencies,” wrote Dr. Scully and her colleagues.
The investigators plan to continue investigating and reporting genotype and phenotype correlations among their patient population; they also invite broader international collaboration into the prevalence of rare hereditary bleeding disorders in isolated populations.
The authors reported having no conflicts of interest and no outside sources of funding.
SOURCE: Scully M-F et al. Transfus Apher Sci. 2018 Dec;57(6):713-6.
FROM TRANSFUSION AND APHERESIS SCIENCE
Key clinical point:
Major finding: Hemophilia A is 2.89 times more common in Newfoundland and Labrador than in the rest of Canada.
Study details: A study of 180 patients with hereditary bleeding disorders receiving specialty care in Newfoundland and Labrador.
Disclosures: The authors reported that they had no conflicts of interest and no outside sources of funding.
Source: Scully M-F et al. Transfus Apher Sci. 2018 Dec;57(6):713-6.
Postdiagnosis statin use lowers mortality rate for patients with HCC
Statin use after a diagnosis of hepatocellular carcinoma (HCC) was associated with a reduced risk of all-cause and cancer-specific mortality, according to recent research published in Clinical Gastroenterology and Hepatology.
“Our current findings are biologically plausible since statins inhibit not only cholesterol synthesis but also reduce other important downstream products, including membrane integrity maintenance, cell signaling, protein synthesis, and cell-cycle progression,” wrote Aaron P. Thrift, PhD, of the section of epidemiology and population sciences and department of medicine at Baylor College of Medicine in Houston, and his colleagues. “Not only can statins have a direct impact on cancer cells through inhibition of the mevalonate pathway within the cancer cells, but the reduction of circulating cholesterol levels through hepatic pathways is indeed considered important.”
Dr. Thrift and his colleagues performed a retrospective cohort analysis of data from 15,422 patients with HCC in the VA Central Cancer Registry who were diagnosed between 2002 and 2016 and filled a prescription for statins. The researchers looked at statin prescriptions filled prior to and after diagnosis, following patients from diagnosis up to a 3-month lag period. The statins analyzed included atorvastatin, fluvastatin, lovastatin, pravastatin, rosuvastatin, and simvastatin.
Overall, 78.8% of patients died during 26,680 person-years of follow-up and the median survival time was 17.24 months. The researchers found 14.9% of patients (2,293 patients) with HCC filled prescriptions for statins after their cancer diagnosis. The median time to begin statins after diagnosis was 2.37 months, and patients who used statins after diagnosis had a median survival time of 26.38 months compared with 15.67 months for patients who did not use statins after diagnosis. For HCC patients who used statins, there was a decreased risk of all-cause mortality (hazard ratio, 0.89; 95% confidence interval, 0.83-0.95) and cancer-specific mortality (adjusted HR, 0.85; 95% CI, 0.77-0.93), which was consistent for both high-dose and low-dose statins and for lag periods between 0 months and 12 months after diagnosis.
Limitations in the study were the exclusion of any statins filled at non-VA pharmacies, baseline differences in statin users and nonstatin users that could have affected results, potential misclassification of cirrhosis in the registry, and the lack of generalization to other populations due to a veteran-specific patient cohort.
This study was funded by the National Institutes of Health and VA Health Services Research and Development Service Center for Innovations in Quality, Effectiveness, and Safety. The authors report having no conflicts of interest.
SOURCE: Thrift AP et al. Clin Gastroenterol Hepatol. 2019. doi: 10.1016/j.cgh.2018.12.046.
Statin use after a diagnosis of hepatocellular carcinoma (HCC) was associated with a reduced risk of all-cause and cancer-specific mortality, according to recent research published in Clinical Gastroenterology and Hepatology.
“Our current findings are biologically plausible since statins inhibit not only cholesterol synthesis but also reduce other important downstream products, including membrane integrity maintenance, cell signaling, protein synthesis, and cell-cycle progression,” wrote Aaron P. Thrift, PhD, of the section of epidemiology and population sciences and department of medicine at Baylor College of Medicine in Houston, and his colleagues. “Not only can statins have a direct impact on cancer cells through inhibition of the mevalonate pathway within the cancer cells, but the reduction of circulating cholesterol levels through hepatic pathways is indeed considered important.”
Dr. Thrift and his colleagues performed a retrospective cohort analysis of data from 15,422 patients with HCC in the VA Central Cancer Registry who were diagnosed between 2002 and 2016 and filled a prescription for statins. The researchers looked at statin prescriptions filled prior to and after diagnosis, following patients from diagnosis up to a 3-month lag period. The statins analyzed included atorvastatin, fluvastatin, lovastatin, pravastatin, rosuvastatin, and simvastatin.
Overall, 78.8% of patients died during 26,680 person-years of follow-up and the median survival time was 17.24 months. The researchers found 14.9% of patients (2,293 patients) with HCC filled prescriptions for statins after their cancer diagnosis. The median time to begin statins after diagnosis was 2.37 months, and patients who used statins after diagnosis had a median survival time of 26.38 months compared with 15.67 months for patients who did not use statins after diagnosis. For HCC patients who used statins, there was a decreased risk of all-cause mortality (hazard ratio, 0.89; 95% confidence interval, 0.83-0.95) and cancer-specific mortality (adjusted HR, 0.85; 95% CI, 0.77-0.93), which was consistent for both high-dose and low-dose statins and for lag periods between 0 months and 12 months after diagnosis.
Limitations in the study were the exclusion of any statins filled at non-VA pharmacies, baseline differences in statin users and nonstatin users that could have affected results, potential misclassification of cirrhosis in the registry, and the lack of generalization to other populations due to a veteran-specific patient cohort.
This study was funded by the National Institutes of Health and VA Health Services Research and Development Service Center for Innovations in Quality, Effectiveness, and Safety. The authors report having no conflicts of interest.
SOURCE: Thrift AP et al. Clin Gastroenterol Hepatol. 2019. doi: 10.1016/j.cgh.2018.12.046.
Statin use after a diagnosis of hepatocellular carcinoma (HCC) was associated with a reduced risk of all-cause and cancer-specific mortality, according to recent research published in Clinical Gastroenterology and Hepatology.
“Our current findings are biologically plausible since statins inhibit not only cholesterol synthesis but also reduce other important downstream products, including membrane integrity maintenance, cell signaling, protein synthesis, and cell-cycle progression,” wrote Aaron P. Thrift, PhD, of the section of epidemiology and population sciences and department of medicine at Baylor College of Medicine in Houston, and his colleagues. “Not only can statins have a direct impact on cancer cells through inhibition of the mevalonate pathway within the cancer cells, but the reduction of circulating cholesterol levels through hepatic pathways is indeed considered important.”
Dr. Thrift and his colleagues performed a retrospective cohort analysis of data from 15,422 patients with HCC in the VA Central Cancer Registry who were diagnosed between 2002 and 2016 and filled a prescription for statins. The researchers looked at statin prescriptions filled prior to and after diagnosis, following patients from diagnosis up to a 3-month lag period. The statins analyzed included atorvastatin, fluvastatin, lovastatin, pravastatin, rosuvastatin, and simvastatin.
Overall, 78.8% of patients died during 26,680 person-years of follow-up and the median survival time was 17.24 months. The researchers found 14.9% of patients (2,293 patients) with HCC filled prescriptions for statins after their cancer diagnosis. The median time to begin statins after diagnosis was 2.37 months, and patients who used statins after diagnosis had a median survival time of 26.38 months compared with 15.67 months for patients who did not use statins after diagnosis. For HCC patients who used statins, there was a decreased risk of all-cause mortality (hazard ratio, 0.89; 95% confidence interval, 0.83-0.95) and cancer-specific mortality (adjusted HR, 0.85; 95% CI, 0.77-0.93), which was consistent for both high-dose and low-dose statins and for lag periods between 0 months and 12 months after diagnosis.
Limitations in the study were the exclusion of any statins filled at non-VA pharmacies, baseline differences in statin users and nonstatin users that could have affected results, potential misclassification of cirrhosis in the registry, and the lack of generalization to other populations due to a veteran-specific patient cohort.
This study was funded by the National Institutes of Health and VA Health Services Research and Development Service Center for Innovations in Quality, Effectiveness, and Safety. The authors report having no conflicts of interest.
SOURCE: Thrift AP et al. Clin Gastroenterol Hepatol. 2019. doi: 10.1016/j.cgh.2018.12.046.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Key clinical point: The use of statins after diagnosis of hepatocellular carcinoma was associated with a lower risk of death.
Major finding: In 14.9% of patients who used statins after diagnosis, the rate of all-cause mortality (hazard ratio, 0.89; 95% confidence interval, 0.83-0.95) and cancer-specific mortality (adjusted HR, 0.85; 95% CI, 0.77-0.93) was lower, and was consistent for both high-dose and low-dose statins.
Study details: A retrospective analysis of 15,422 patients with hepatocellular carcinoma in the VA Central Cancer Registry between 2002 and 2016.
Disclosures: This study was funded by the National Institutes of Health and VA Health Services Research and Development Service Center for Innovations in Quality, Effectiveness, and Safety. The authors report having no conflicts of interest.
Source: Thrift AP et al. Clin Gastroenterol Hepatol. 2018. doi: 10.1016/j.cgh.2018.12.046.
Chronic infections such as HCV, HIV, and TB cause unique problems for psoriasis patients
In a review of therapeutic issues for psoriasis patients who have such chronic infections as hepatitis, HIV, or latent tuberculosis infection (LTBI) or those who fall into the category of special populations (pregnant women or children), significant concerns were directly tied to the mode of action of the drugs involved.

In particular, “Most systemic agents for psoriasis are immunosuppressive, which poses a unique treatment challenge in patients with psoriasis with chronic infections because they are already immunosuppressed,” according to Shivani B. Kaushik, MD, a resident in the department of dermatology at the Icahn School of Medicine at Mount Sinai, New York, and her colleague Mark G. Lebwohl, MD, professor and system chair of the department.
For example, the reviewers detailed a report of hepatitis B virus (HBV) and hepatitis C virus (HCV) reactivation in patients with psoriasis who were taking biologics. Virus reactivation was noted in 2/175 patients who were positive for anti-HBc antibody, 3/97 patients with HCV infection, and 8/40 patients who were positive for HBsAg (the surface antigen of HBV). From this, they concluded that “biologics pose minimal risk for viral reactivation in patients with anti-HCV or anti-HBc antibodies, but they are of considerable risk in HBsAg-positive patients.” (J Amer Acad Derm. 2019 Jan;80:43-53).
Giving a specific example, Dr. Kaushik and her colleague pointed out that the safety of ustekinumab in patients with psoriasis with concurrent HCV and HBV infection was not clear. Viral reactivation and hepatocellular cancer were reported in one of four patients with HCV and in two of seven HBsAg-positive patients; and yet, another study showed that the successful use of ustekinumab for psoriasis had no impact on liver function or viral load in a patient with coexisting HCV.
Overall, “Patients should not be treated with immunosuppressive therapies during the acute stage. However, biologic treatment can be initiated in patients with chronic or resolved hepatitis under close monitoring and collaboration with a gastroenterologist,” the researchers stated.
In addition, they pointed out that methotrexate, another commonly prescribed drug for psoriasis, is absolutely contraindicated, although the use of cyclosporine remains controversial for those patients who are HCV-antibody positive.
“Most systemic agents used in psoriasis are immunosuppressive and require appropriate screening, monitoring, and prophylaxis when used in [psoriasis] patients with chronic infections, such as hepatitis, HIV, and LTBI,” the authors concluded.
The authors reported receiving funding from a number of pharmaceutical companies.
SOURCE: Kaushik BS et al. J Amer Acad Derm. 2019;80:43-53.
In a review of therapeutic issues for psoriasis patients who have such chronic infections as hepatitis, HIV, or latent tuberculosis infection (LTBI) or those who fall into the category of special populations (pregnant women or children), significant concerns were directly tied to the mode of action of the drugs involved.
In particular, “Most systemic agents for psoriasis are immunosuppressive, which poses a unique treatment challenge in patients with psoriasis with chronic infections because they are already immunosuppressed,” according to Shivani B. Kaushik, MD, a resident in the department of dermatology at the Icahn School of Medicine at Mount Sinai, New York, and her colleague Mark G. Lebwohl, MD, professor and system chair of the department.
For example, the reviewers detailed a report of hepatitis B virus (HBV) and hepatitis C virus (HCV) reactivation in patients with psoriasis who were taking biologics. Virus reactivation was noted in 2/175 patients who were positive for anti-HBc antibody, 3/97 patients with HCV infection, and 8/40 patients who were positive for HBsAg (the surface antigen of HBV). From this, they concluded that “biologics pose minimal risk for viral reactivation in patients with anti-HCV or anti-HBc antibodies, but they are of considerable risk in HBsAg-positive patients.” (J Amer Acad Derm. 2019 Jan;80:43-53).
Giving a specific example, Dr. Kaushik and her colleague pointed out that the safety of ustekinumab in patients with psoriasis with concurrent HCV and HBV infection was not clear. Viral reactivation and hepatocellular cancer were reported in one of four patients with HCV and in two of seven HBsAg-positive patients; and yet, another study showed that the successful use of ustekinumab for psoriasis had no impact on liver function or viral load in a patient with coexisting HCV.
Overall, “Patients should not be treated with immunosuppressive therapies during the acute stage. However, biologic treatment can be initiated in patients with chronic or resolved hepatitis under close monitoring and collaboration with a gastroenterologist,” the researchers stated.
In addition, they pointed out that methotrexate, another commonly prescribed drug for psoriasis, is absolutely contraindicated, although the use of cyclosporine remains controversial for those patients who are HCV-antibody positive.
“Most systemic agents used in psoriasis are immunosuppressive and require appropriate screening, monitoring, and prophylaxis when used in [psoriasis] patients with chronic infections, such as hepatitis, HIV, and LTBI,” the authors concluded.
The authors reported receiving funding from a number of pharmaceutical companies.
SOURCE: Kaushik BS et al. J Amer Acad Derm. 2019;80:43-53.
In a review of therapeutic issues for psoriasis patients who have such chronic infections as hepatitis, HIV, or latent tuberculosis infection (LTBI) or those who fall into the category of special populations (pregnant women or children), significant concerns were directly tied to the mode of action of the drugs involved.
In particular, “Most systemic agents for psoriasis are immunosuppressive, which poses a unique treatment challenge in patients with psoriasis with chronic infections because they are already immunosuppressed,” according to Shivani B. Kaushik, MD, a resident in the department of dermatology at the Icahn School of Medicine at Mount Sinai, New York, and her colleague Mark G. Lebwohl, MD, professor and system chair of the department.
For example, the reviewers detailed a report of hepatitis B virus (HBV) and hepatitis C virus (HCV) reactivation in patients with psoriasis who were taking biologics. Virus reactivation was noted in 2/175 patients who were positive for anti-HBc antibody, 3/97 patients with HCV infection, and 8/40 patients who were positive for HBsAg (the surface antigen of HBV). From this, they concluded that “biologics pose minimal risk for viral reactivation in patients with anti-HCV or anti-HBc antibodies, but they are of considerable risk in HBsAg-positive patients.” (J Amer Acad Derm. 2019 Jan;80:43-53).
Giving a specific example, Dr. Kaushik and her colleague pointed out that the safety of ustekinumab in patients with psoriasis with concurrent HCV and HBV infection was not clear. Viral reactivation and hepatocellular cancer were reported in one of four patients with HCV and in two of seven HBsAg-positive patients; and yet, another study showed that the successful use of ustekinumab for psoriasis had no impact on liver function or viral load in a patient with coexisting HCV.
Overall, “Patients should not be treated with immunosuppressive therapies during the acute stage. However, biologic treatment can be initiated in patients with chronic or resolved hepatitis under close monitoring and collaboration with a gastroenterologist,” the researchers stated.
In addition, they pointed out that methotrexate, another commonly prescribed drug for psoriasis, is absolutely contraindicated, although the use of cyclosporine remains controversial for those patients who are HCV-antibody positive.
“Most systemic agents used in psoriasis are immunosuppressive and require appropriate screening, monitoring, and prophylaxis when used in [psoriasis] patients with chronic infections, such as hepatitis, HIV, and LTBI,” the authors concluded.
The authors reported receiving funding from a number of pharmaceutical companies.
SOURCE: Kaushik BS et al. J Amer Acad Derm. 2019;80:43-53.
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY