User login
Adding mechanical to pharma prophylaxis does not cut DVT incidence
Background: Critically ill patients have a high risk of venous thromboembolism (VTE) during their hospitalizations, and it is standard of care to prophylax against this complication by either pharmacological or mechanical means.
Study design: Prospective, randomized, controlled trial (Pneumatic Compression for Preventing Venous Thromboembolism [PREVENT]).
Setting: Multicenter study involving 20 ICUs in Saudi Arabia, Canada, Australia, and India.
Synopsis: The study monitored 2,003 medical and surgical ICU patients on pharmacological thromboprophylaxis (unfractionated or low-molecular-weight heparin) after receiving either adjunctive pneumatic compression or pharmacological thromboprophylaxis alone. The primary outcome was incident (newly diagnosed) proximal lower-limb DVT detected by twice-weekly venous ultrasonography until ICU discharge, death, attainment of full mobility, or trial day 28, whichever occurred first. Key secondary outcomes included the occurrence of any lower-limb DVTs and pulmonary embolism. Intermittent pneumatic compression was used a median of 22 hours daily. The incidence of proximal lower limb DVT did not differ in the two groups and was relatively low (4%) in the control group. There were also no differences in the groups in the composite VTE, death at 28 days, or any other secondary outcomes studied.
The main limitation of the study was the low incidence of primary outcomes in the control group, which reduced the power of the study.
Bottom line: Based on the PREVENT trial, adjunctive intermittent pneumatic compression provided no additional benefit to pharmacological prophylaxis in the prevention of incident proximal lower-limb DVT.
Citation: Arabi Y et al. Adjunctive intermittent pneumatic compression for venous thromboprophylaxis. N Eng J Med. 2019 Feb 18. doi: 10.1056/NEJMoa1816150.
Dr. Sekaran is a hospitalist at Massachusetts General Hospital.
Background: Critically ill patients have a high risk of venous thromboembolism (VTE) during their hospitalizations, and it is standard of care to prophylax against this complication by either pharmacological or mechanical means.
Study design: Prospective, randomized, controlled trial (Pneumatic Compression for Preventing Venous Thromboembolism [PREVENT]).
Setting: Multicenter study involving 20 ICUs in Saudi Arabia, Canada, Australia, and India.
Synopsis: The study monitored 2,003 medical and surgical ICU patients on pharmacological thromboprophylaxis (unfractionated or low-molecular-weight heparin) after receiving either adjunctive pneumatic compression or pharmacological thromboprophylaxis alone. The primary outcome was incident (newly diagnosed) proximal lower-limb DVT detected by twice-weekly venous ultrasonography until ICU discharge, death, attainment of full mobility, or trial day 28, whichever occurred first. Key secondary outcomes included the occurrence of any lower-limb DVTs and pulmonary embolism. Intermittent pneumatic compression was used a median of 22 hours daily. The incidence of proximal lower limb DVT did not differ in the two groups and was relatively low (4%) in the control group. There were also no differences in the groups in the composite VTE, death at 28 days, or any other secondary outcomes studied.
The main limitation of the study was the low incidence of primary outcomes in the control group, which reduced the power of the study.
Bottom line: Based on the PREVENT trial, adjunctive intermittent pneumatic compression provided no additional benefit to pharmacological prophylaxis in the prevention of incident proximal lower-limb DVT.
Citation: Arabi Y et al. Adjunctive intermittent pneumatic compression for venous thromboprophylaxis. N Eng J Med. 2019 Feb 18. doi: 10.1056/NEJMoa1816150.
Dr. Sekaran is a hospitalist at Massachusetts General Hospital.
Background: Critically ill patients have a high risk of venous thromboembolism (VTE) during their hospitalizations, and it is standard of care to prophylax against this complication by either pharmacological or mechanical means.
Study design: Prospective, randomized, controlled trial (Pneumatic Compression for Preventing Venous Thromboembolism [PREVENT]).
Setting: Multicenter study involving 20 ICUs in Saudi Arabia, Canada, Australia, and India.
Synopsis: The study monitored 2,003 medical and surgical ICU patients on pharmacological thromboprophylaxis (unfractionated or low-molecular-weight heparin) after receiving either adjunctive pneumatic compression or pharmacological thromboprophylaxis alone. The primary outcome was incident (newly diagnosed) proximal lower-limb DVT detected by twice-weekly venous ultrasonography until ICU discharge, death, attainment of full mobility, or trial day 28, whichever occurred first. Key secondary outcomes included the occurrence of any lower-limb DVTs and pulmonary embolism. Intermittent pneumatic compression was used a median of 22 hours daily. The incidence of proximal lower limb DVT did not differ in the two groups and was relatively low (4%) in the control group. There were also no differences in the groups in the composite VTE, death at 28 days, or any other secondary outcomes studied.
The main limitation of the study was the low incidence of primary outcomes in the control group, which reduced the power of the study.
Bottom line: Based on the PREVENT trial, adjunctive intermittent pneumatic compression provided no additional benefit to pharmacological prophylaxis in the prevention of incident proximal lower-limb DVT.
Citation: Arabi Y et al. Adjunctive intermittent pneumatic compression for venous thromboprophylaxis. N Eng J Med. 2019 Feb 18. doi: 10.1056/NEJMoa1816150.
Dr. Sekaran is a hospitalist at Massachusetts General Hospital.
FOURIER: Evolocumab follow-up shows no cognitive adverse effects
Treatment with a PCSK9 inhibitor, as well as achieving dramatically lowered cholesterol levels, did not mess with patients’ minds. Results from a cognition self-assessment completed by more than 22,000 patients when they finished participation in the FOURIER pivotal outcomes trial for evolocumab showed no signal of mental harm from either treatment with this PCSK9 inhibitor or from reaching a serum level of low-density lipoprotein cholesterol (LDL-C) of less than 20 mg/dL.
“We observed that patients treated with evolocumab, as well as those who achieved progressively very low LDL-C at 4 weeks in the FOURIER trial, had similar self-reported cognition in comparison with those receiving placebo and those with higher achieved LDL-C levels,” wrote a team of researchers from the trial in an article published online on May 4 (J Am Coll Cardiol. 2020 May 12;75[18]: 2283-93). “These data confirm the neurocognitive safety of intensive LDL-C reduction with evolocumab while reducing recurrent CV [cardiovascular] events in high-risk patients, and suggest that very low achieved LDL-C levels may be safely targeted for high-risk patients.”
The findings added to prior results documenting the cognitive safety of evolocumab (Repatha) from a much smaller FOURIER substudy that involved more intensive testing, the EBBINGHAUS (Evaluating PCSK9 Binding Antibody Influence on Cognitive Health in High Cardiovascular Risk Subjects) study with 1,204 patients drawn from the broader study and tested after a median 19 months on treatment (N Engl J Med. 2017 Aug 17;377[17]: 633-43), as well as reports of neurocognitive safety for the other U.S. approved PCSK9 (proprotein convertase subtilisin kexin 9) inhibitor, alirocumab (Praluent) (N Engl J Med. 2015 Apr 16;372[16]:1489-99), various statins (J Gen Intern Med. 2015 Mar;30[3]: 348-58), and a third type of LDL-C–lowering agent, ezetimibe (JAMA Cardiol. 2017 May;2[5]:547-55).
Despite this evidence from across several drug classes that all cut LDL-C a long-standing but unsubstantiated belief persists among some that lipid lowering, especially by statins, blunts mental function, misinformation that’s easy to find on the Internet. “I estimate that about 20% of patients prescribed a statin won’t take it because of something they’ve heard” including that statins make you stupid. “It’s hard to undo that,” said Robert P. Giugliano, MD, a cardiologist at Brigham and Women’s Hospital in Boston and senior author for the new FOURIER study as well as for EBBINGHAUS. The same stigma has not gained nearly as much traction for PCSK9 inhibitors, however, and Dr. Giugliano said he has also recently sensed what may be a downtrend in statin apprehension.
“The information added by this study is very important,” commented Massimo R. Mannarino, MD, an atherosclerotic disease researcher at the University of Perugia (Italy). “The prejudice and misinformation regarding possible side effects of statins among patients and also some physicians unfortunately remains very strong today,” he said in an interview. “My impression is that PCSK9 inhibitors are less affected by this negative bias and are seen as a safer alternative to statins.” Concerns about PCSK9 inhibitors have especially focused on “the possible risks from very low cholesterol levels on the brain.” The evidence from both studies and clinical experience “allows for a very positive opinion about the efficacy and safety of PCSK9 inhibitors, although the long-term effects still require a few more years of observation,” said Dr. Mannarino, who led a review of the evidence that clears this class from links to neurocognitive loss (J Clin Lipid. 2018 Sep 1;12[5]:1123-32).
FOURIER (Further Cardiovascular Outcomes Research With PCSK9 Inhibition in Subjects With Elevated Risk) randomized 27,564 patients with atherosclerotic cardiovascular disease and elevated LDL cholesterol despite maximally tolerated standard treatment. Treatment with evolocumab for a median of 2.2 years resulted in a statistically significant 15% reduction in the study’s primary efficacy endpoint, compared with placebo (N Engl J Med. 2017 May 4;376[18]:1713-22), and led to the drug receiving an indication for lowering rates of MI, stroke, and symptom-driven coronary revascularization.
The prespecified substudy reported by Dr. Giugliano and his associates focused on a 23-question, validated, self-assessment survey of cognitive function completed by 22,655 of the FOURIER patients (82%). The more than 4,900 other patients in the study who did not complete the survey had modestly higher prevalence rates of various comorbidities at baseline, and also higher rates of adverse outcomes during follow-up, and in many cases these adverse outcome may have contributed to these patients not being able to complete their end-of-study cognitive assessment. For example, almost a quarter of the patients who did not complete their end-of-study cognitive assessment failed to do so because they had already died.
Overall, the prevalence of patients indicating a cognitive decline was virtually identical among 11,363 patients who had been maintained on evolocumab, with a 3.7% rate, and the 11,292 patients in the placebo group, with a 3.6% rate. When analyzed by achieved level of LDL-C after 4 weeks on treatment, the 2,338 patients with a level below 20 mg/dL had a 3.8% rate of self-reported cognitive loss, compared with a 4.5% rate among 3,613 patients who had an LDL-C level of at least 100 mg/dL when measured 4 weeks into the study.
One of the strengths of the new cognitive analysis is that, although it did not use the more sophisticated assessment tests employed on fewer patients in the EBBINGHAUS substudy, it used the Everyday Cognition scale (Neuropsychiatry. 2008 Jul;22[4]: 531-44). “We asked patients what they have experienced, and in the end that is what’s important, so this adds to the neurocognitive testing,” run in EBBINGHAUS, Dr. Giugliano said in an interview.
“The neurocognitive results in the present study were self-reported, and that might be a limitation, as it is less specific and objective, but it is also a strength, as it could be more sensitive” especially for a “nocebo effect common to all lipid-lowering drugs linked to the bad reputation historically attributed to statins,” Dr. Mannarino said.
Should the new FOURIER data “be interpreted as definitive evidence that intensive LDL-C lowering with PCSK9 monoclonal antibodies has no major harmful cognitive effects, at least over a period of 3 years? The answer appears to be a qualified yes, but with three important caveats,” Jennifer G. Robinson, MD, a professor of epidemiology at the University of Iowa College of Public Health in Iowa City, said in an editorial that accompanied the new report (J Am Coll Cardiol. 2020 May 12;75[18]:2294-6). Her three caveats are the missing 18% of patients who never took the end-of-study assessment, the relative paucity of patients at very advanced age in FOURIER, in which patients averaged 62.5 years old, and the exclusion from FOURIER of patients with a history of hemorrhagic stroke. Dr. Robinson also cited the 2.2 year median follow-up as leaving unsettled the potential cognitive impact of longer treatment.
In response, Dr. Giugliano noted that the very large size of FOURIER and the 22,655 patients who completed their survey provided substantial numbers of patients to address some of these concerns in robust subgroup analyses. For example, the new report showed no signal of excess cognitive complaints with evolocumab treatment among 1,999 patients who were at least 75 years old when entering the study, or in more than 5,000 patients with a history of cerebrovascular disease at baseline, or in 1,990 patients with a history of a nonstroke neurologic disease. In addition, while he conceded that the 18% of patients not accounted for in the new study placed some limits on generalizability of the findings, he also maintained that this unavoidable failure to collect data from a modest percentage of patients doesn’t scuttle the overarching signal of cognitive safety for most patients. And regarding the duration of treatment monitored, he noted that 5-year follow-up cognitive assessments are planned.
FOURIER was sponsored by Amgen, the company that markets evolocumab (Repatha). Dr. Giugliano has received personal fees and research support from Amgen and from several other companies. Dr. Mannarino had no disclosures. Dr. Robinson has been a consultant to The Medicines Company, Novartis, and Pfizer, and she has received research funding to her institution from Amgen and several other companies.
SOURCE: Gencer B et al. J Am Coll Cardiol. 2020 May 12;75[18]:2283-93.
Correction: Dr. Giugliano's name was misspelled in an earlier version of this article.
Treatment with a PCSK9 inhibitor, as well as achieving dramatically lowered cholesterol levels, did not mess with patients’ minds. Results from a cognition self-assessment completed by more than 22,000 patients when they finished participation in the FOURIER pivotal outcomes trial for evolocumab showed no signal of mental harm from either treatment with this PCSK9 inhibitor or from reaching a serum level of low-density lipoprotein cholesterol (LDL-C) of less than 20 mg/dL.
“We observed that patients treated with evolocumab, as well as those who achieved progressively very low LDL-C at 4 weeks in the FOURIER trial, had similar self-reported cognition in comparison with those receiving placebo and those with higher achieved LDL-C levels,” wrote a team of researchers from the trial in an article published online on May 4 (J Am Coll Cardiol. 2020 May 12;75[18]: 2283-93). “These data confirm the neurocognitive safety of intensive LDL-C reduction with evolocumab while reducing recurrent CV [cardiovascular] events in high-risk patients, and suggest that very low achieved LDL-C levels may be safely targeted for high-risk patients.”
The findings added to prior results documenting the cognitive safety of evolocumab (Repatha) from a much smaller FOURIER substudy that involved more intensive testing, the EBBINGHAUS (Evaluating PCSK9 Binding Antibody Influence on Cognitive Health in High Cardiovascular Risk Subjects) study with 1,204 patients drawn from the broader study and tested after a median 19 months on treatment (N Engl J Med. 2017 Aug 17;377[17]: 633-43), as well as reports of neurocognitive safety for the other U.S. approved PCSK9 (proprotein convertase subtilisin kexin 9) inhibitor, alirocumab (Praluent) (N Engl J Med. 2015 Apr 16;372[16]:1489-99), various statins (J Gen Intern Med. 2015 Mar;30[3]: 348-58), and a third type of LDL-C–lowering agent, ezetimibe (JAMA Cardiol. 2017 May;2[5]:547-55).
Despite this evidence from across several drug classes that all cut LDL-C a long-standing but unsubstantiated belief persists among some that lipid lowering, especially by statins, blunts mental function, misinformation that’s easy to find on the Internet. “I estimate that about 20% of patients prescribed a statin won’t take it because of something they’ve heard” including that statins make you stupid. “It’s hard to undo that,” said Robert P. Giugliano, MD, a cardiologist at Brigham and Women’s Hospital in Boston and senior author for the new FOURIER study as well as for EBBINGHAUS. The same stigma has not gained nearly as much traction for PCSK9 inhibitors, however, and Dr. Giugliano said he has also recently sensed what may be a downtrend in statin apprehension.
“The information added by this study is very important,” commented Massimo R. Mannarino, MD, an atherosclerotic disease researcher at the University of Perugia (Italy). “The prejudice and misinformation regarding possible side effects of statins among patients and also some physicians unfortunately remains very strong today,” he said in an interview. “My impression is that PCSK9 inhibitors are less affected by this negative bias and are seen as a safer alternative to statins.” Concerns about PCSK9 inhibitors have especially focused on “the possible risks from very low cholesterol levels on the brain.” The evidence from both studies and clinical experience “allows for a very positive opinion about the efficacy and safety of PCSK9 inhibitors, although the long-term effects still require a few more years of observation,” said Dr. Mannarino, who led a review of the evidence that clears this class from links to neurocognitive loss (J Clin Lipid. 2018 Sep 1;12[5]:1123-32).
FOURIER (Further Cardiovascular Outcomes Research With PCSK9 Inhibition in Subjects With Elevated Risk) randomized 27,564 patients with atherosclerotic cardiovascular disease and elevated LDL cholesterol despite maximally tolerated standard treatment. Treatment with evolocumab for a median of 2.2 years resulted in a statistically significant 15% reduction in the study’s primary efficacy endpoint, compared with placebo (N Engl J Med. 2017 May 4;376[18]:1713-22), and led to the drug receiving an indication for lowering rates of MI, stroke, and symptom-driven coronary revascularization.
The prespecified substudy reported by Dr. Giugliano and his associates focused on a 23-question, validated, self-assessment survey of cognitive function completed by 22,655 of the FOURIER patients (82%). The more than 4,900 other patients in the study who did not complete the survey had modestly higher prevalence rates of various comorbidities at baseline, and also higher rates of adverse outcomes during follow-up, and in many cases these adverse outcome may have contributed to these patients not being able to complete their end-of-study cognitive assessment. For example, almost a quarter of the patients who did not complete their end-of-study cognitive assessment failed to do so because they had already died.
Overall, the prevalence of patients indicating a cognitive decline was virtually identical among 11,363 patients who had been maintained on evolocumab, with a 3.7% rate, and the 11,292 patients in the placebo group, with a 3.6% rate. When analyzed by achieved level of LDL-C after 4 weeks on treatment, the 2,338 patients with a level below 20 mg/dL had a 3.8% rate of self-reported cognitive loss, compared with a 4.5% rate among 3,613 patients who had an LDL-C level of at least 100 mg/dL when measured 4 weeks into the study.
One of the strengths of the new cognitive analysis is that, although it did not use the more sophisticated assessment tests employed on fewer patients in the EBBINGHAUS substudy, it used the Everyday Cognition scale (Neuropsychiatry. 2008 Jul;22[4]: 531-44). “We asked patients what they have experienced, and in the end that is what’s important, so this adds to the neurocognitive testing,” run in EBBINGHAUS, Dr. Giugliano said in an interview.
“The neurocognitive results in the present study were self-reported, and that might be a limitation, as it is less specific and objective, but it is also a strength, as it could be more sensitive” especially for a “nocebo effect common to all lipid-lowering drugs linked to the bad reputation historically attributed to statins,” Dr. Mannarino said.
Should the new FOURIER data “be interpreted as definitive evidence that intensive LDL-C lowering with PCSK9 monoclonal antibodies has no major harmful cognitive effects, at least over a period of 3 years? The answer appears to be a qualified yes, but with three important caveats,” Jennifer G. Robinson, MD, a professor of epidemiology at the University of Iowa College of Public Health in Iowa City, said in an editorial that accompanied the new report (J Am Coll Cardiol. 2020 May 12;75[18]:2294-6). Her three caveats are the missing 18% of patients who never took the end-of-study assessment, the relative paucity of patients at very advanced age in FOURIER, in which patients averaged 62.5 years old, and the exclusion from FOURIER of patients with a history of hemorrhagic stroke. Dr. Robinson also cited the 2.2 year median follow-up as leaving unsettled the potential cognitive impact of longer treatment.
In response, Dr. Giugliano noted that the very large size of FOURIER and the 22,655 patients who completed their survey provided substantial numbers of patients to address some of these concerns in robust subgroup analyses. For example, the new report showed no signal of excess cognitive complaints with evolocumab treatment among 1,999 patients who were at least 75 years old when entering the study, or in more than 5,000 patients with a history of cerebrovascular disease at baseline, or in 1,990 patients with a history of a nonstroke neurologic disease. In addition, while he conceded that the 18% of patients not accounted for in the new study placed some limits on generalizability of the findings, he also maintained that this unavoidable failure to collect data from a modest percentage of patients doesn’t scuttle the overarching signal of cognitive safety for most patients. And regarding the duration of treatment monitored, he noted that 5-year follow-up cognitive assessments are planned.
FOURIER was sponsored by Amgen, the company that markets evolocumab (Repatha). Dr. Giugliano has received personal fees and research support from Amgen and from several other companies. Dr. Mannarino had no disclosures. Dr. Robinson has been a consultant to The Medicines Company, Novartis, and Pfizer, and she has received research funding to her institution from Amgen and several other companies.
SOURCE: Gencer B et al. J Am Coll Cardiol. 2020 May 12;75[18]:2283-93.
Correction: Dr. Giugliano's name was misspelled in an earlier version of this article.
Treatment with a PCSK9 inhibitor, as well as achieving dramatically lowered cholesterol levels, did not mess with patients’ minds. Results from a cognition self-assessment completed by more than 22,000 patients when they finished participation in the FOURIER pivotal outcomes trial for evolocumab showed no signal of mental harm from either treatment with this PCSK9 inhibitor or from reaching a serum level of low-density lipoprotein cholesterol (LDL-C) of less than 20 mg/dL.
“We observed that patients treated with evolocumab, as well as those who achieved progressively very low LDL-C at 4 weeks in the FOURIER trial, had similar self-reported cognition in comparison with those receiving placebo and those with higher achieved LDL-C levels,” wrote a team of researchers from the trial in an article published online on May 4 (J Am Coll Cardiol. 2020 May 12;75[18]: 2283-93). “These data confirm the neurocognitive safety of intensive LDL-C reduction with evolocumab while reducing recurrent CV [cardiovascular] events in high-risk patients, and suggest that very low achieved LDL-C levels may be safely targeted for high-risk patients.”
The findings added to prior results documenting the cognitive safety of evolocumab (Repatha) from a much smaller FOURIER substudy that involved more intensive testing, the EBBINGHAUS (Evaluating PCSK9 Binding Antibody Influence on Cognitive Health in High Cardiovascular Risk Subjects) study with 1,204 patients drawn from the broader study and tested after a median 19 months on treatment (N Engl J Med. 2017 Aug 17;377[17]: 633-43), as well as reports of neurocognitive safety for the other U.S. approved PCSK9 (proprotein convertase subtilisin kexin 9) inhibitor, alirocumab (Praluent) (N Engl J Med. 2015 Apr 16;372[16]:1489-99), various statins (J Gen Intern Med. 2015 Mar;30[3]: 348-58), and a third type of LDL-C–lowering agent, ezetimibe (JAMA Cardiol. 2017 May;2[5]:547-55).
Despite this evidence from across several drug classes that all cut LDL-C a long-standing but unsubstantiated belief persists among some that lipid lowering, especially by statins, blunts mental function, misinformation that’s easy to find on the Internet. “I estimate that about 20% of patients prescribed a statin won’t take it because of something they’ve heard” including that statins make you stupid. “It’s hard to undo that,” said Robert P. Giugliano, MD, a cardiologist at Brigham and Women’s Hospital in Boston and senior author for the new FOURIER study as well as for EBBINGHAUS. The same stigma has not gained nearly as much traction for PCSK9 inhibitors, however, and Dr. Giugliano said he has also recently sensed what may be a downtrend in statin apprehension.
“The information added by this study is very important,” commented Massimo R. Mannarino, MD, an atherosclerotic disease researcher at the University of Perugia (Italy). “The prejudice and misinformation regarding possible side effects of statins among patients and also some physicians unfortunately remains very strong today,” he said in an interview. “My impression is that PCSK9 inhibitors are less affected by this negative bias and are seen as a safer alternative to statins.” Concerns about PCSK9 inhibitors have especially focused on “the possible risks from very low cholesterol levels on the brain.” The evidence from both studies and clinical experience “allows for a very positive opinion about the efficacy and safety of PCSK9 inhibitors, although the long-term effects still require a few more years of observation,” said Dr. Mannarino, who led a review of the evidence that clears this class from links to neurocognitive loss (J Clin Lipid. 2018 Sep 1;12[5]:1123-32).
FOURIER (Further Cardiovascular Outcomes Research With PCSK9 Inhibition in Subjects With Elevated Risk) randomized 27,564 patients with atherosclerotic cardiovascular disease and elevated LDL cholesterol despite maximally tolerated standard treatment. Treatment with evolocumab for a median of 2.2 years resulted in a statistically significant 15% reduction in the study’s primary efficacy endpoint, compared with placebo (N Engl J Med. 2017 May 4;376[18]:1713-22), and led to the drug receiving an indication for lowering rates of MI, stroke, and symptom-driven coronary revascularization.
The prespecified substudy reported by Dr. Giugliano and his associates focused on a 23-question, validated, self-assessment survey of cognitive function completed by 22,655 of the FOURIER patients (82%). The more than 4,900 other patients in the study who did not complete the survey had modestly higher prevalence rates of various comorbidities at baseline, and also higher rates of adverse outcomes during follow-up, and in many cases these adverse outcome may have contributed to these patients not being able to complete their end-of-study cognitive assessment. For example, almost a quarter of the patients who did not complete their end-of-study cognitive assessment failed to do so because they had already died.
Overall, the prevalence of patients indicating a cognitive decline was virtually identical among 11,363 patients who had been maintained on evolocumab, with a 3.7% rate, and the 11,292 patients in the placebo group, with a 3.6% rate. When analyzed by achieved level of LDL-C after 4 weeks on treatment, the 2,338 patients with a level below 20 mg/dL had a 3.8% rate of self-reported cognitive loss, compared with a 4.5% rate among 3,613 patients who had an LDL-C level of at least 100 mg/dL when measured 4 weeks into the study.
One of the strengths of the new cognitive analysis is that, although it did not use the more sophisticated assessment tests employed on fewer patients in the EBBINGHAUS substudy, it used the Everyday Cognition scale (Neuropsychiatry. 2008 Jul;22[4]: 531-44). “We asked patients what they have experienced, and in the end that is what’s important, so this adds to the neurocognitive testing,” run in EBBINGHAUS, Dr. Giugliano said in an interview.
“The neurocognitive results in the present study were self-reported, and that might be a limitation, as it is less specific and objective, but it is also a strength, as it could be more sensitive” especially for a “nocebo effect common to all lipid-lowering drugs linked to the bad reputation historically attributed to statins,” Dr. Mannarino said.
Should the new FOURIER data “be interpreted as definitive evidence that intensive LDL-C lowering with PCSK9 monoclonal antibodies has no major harmful cognitive effects, at least over a period of 3 years? The answer appears to be a qualified yes, but with three important caveats,” Jennifer G. Robinson, MD, a professor of epidemiology at the University of Iowa College of Public Health in Iowa City, said in an editorial that accompanied the new report (J Am Coll Cardiol. 2020 May 12;75[18]:2294-6). Her three caveats are the missing 18% of patients who never took the end-of-study assessment, the relative paucity of patients at very advanced age in FOURIER, in which patients averaged 62.5 years old, and the exclusion from FOURIER of patients with a history of hemorrhagic stroke. Dr. Robinson also cited the 2.2 year median follow-up as leaving unsettled the potential cognitive impact of longer treatment.
In response, Dr. Giugliano noted that the very large size of FOURIER and the 22,655 patients who completed their survey provided substantial numbers of patients to address some of these concerns in robust subgroup analyses. For example, the new report showed no signal of excess cognitive complaints with evolocumab treatment among 1,999 patients who were at least 75 years old when entering the study, or in more than 5,000 patients with a history of cerebrovascular disease at baseline, or in 1,990 patients with a history of a nonstroke neurologic disease. In addition, while he conceded that the 18% of patients not accounted for in the new study placed some limits on generalizability of the findings, he also maintained that this unavoidable failure to collect data from a modest percentage of patients doesn’t scuttle the overarching signal of cognitive safety for most patients. And regarding the duration of treatment monitored, he noted that 5-year follow-up cognitive assessments are planned.
FOURIER was sponsored by Amgen, the company that markets evolocumab (Repatha). Dr. Giugliano has received personal fees and research support from Amgen and from several other companies. Dr. Mannarino had no disclosures. Dr. Robinson has been a consultant to The Medicines Company, Novartis, and Pfizer, and she has received research funding to her institution from Amgen and several other companies.
SOURCE: Gencer B et al. J Am Coll Cardiol. 2020 May 12;75[18]:2283-93.
Correction: Dr. Giugliano's name was misspelled in an earlier version of this article.
FROM JACC
Key clinical point: A cognition survey of a large number of trial participants showed no signal of adverse effects from evolocumab treatment.
Major finding: Survey results showed cognitive compromise in 3.7% of patients on evolocumab and in 3.6% control patients on placebo.
Study details:
Disclosures: FOURIER was sponsored by Amgen, the company that markets evolocumab (Repatha). Dr. Guigliano has received personal fees and research support from Amgen and from several other companies.
Source: Gencer B et al. J Am Coll Cardiol. 2020 May 12;75[18]:2283-93.
Hydroxychloroquine-triggered QTc-interval prolongations mount in COVID-19 patients
The potential for serious arrhythmias from hydroxychloroquine treatment of COVID-19 patients received further documentation from a pair of studies released on May 1, casting further doubt on whether the uncertain benefit from this or related drugs to infected patients is worth the clear risks the agents pose.

A report from 90 confirmed COVID-19 patients treated with hydroxychloroquine at one Boston hospital during March-April 2020 identified a significantly prolonged, corrected QT (QTc) interval of at least 500 msec in 18 patients (20%), which included 10 patients whose QTc rose by at least 60 msec above baseline, and a total of 21 patients (23%) having a notable prolongation (JAMA Cardiol. 2020 May 4. doi: 10.1001/jamacardio.2020.1834). This series included one patient who developed torsades de pointes following treatment with hydroxychloroquine and azithromycin, “which to our knowledge has yet to be reported elsewhere in the literature,” the report said.
The second report, from a single center in Lyon, France, included 40 confirmed COVID-19 patients treated with hydroxychloroquine during 2 weeks in late March, and found that 37 (93%) had some increase in the QTc interval, including 14 patients (36%) with an increase of at least 60 msec, and 7 patients (18%) whose QTc rose to at least 500 msec (JAMA Cardiol. 2020 May. doi: 10.1001/jamacardio.2020.1787). However, none of the 40 patients in this series developed an identified ventricular arrhythmia. All patients in both studies received hydroxychloroquine for at least 1 day, and roughly half the patients in each series also received concurrent azithromycin, another drug that can prolong the QTc interval and that has been frequently used in combination with hydroxychloroquine as an unproven COVID-19 treatment cocktail.
These two reports, as well as prior report from Brazil on COVID-19 patients treated with chloroquine diphosphate (JAMA Netw Open. 2020;3[4]:e208857), “underscore the potential risk associated with widespread use of hydroxychloroquine and the combination of hydroxychloroquine and azithromycin in ambulatory patients with known or suspected COVID-19. Understanding whether this risk is worth taking in the absence of evidence of therapeutic efficacy creates a knowledge gap that needs to be addressed,” wrote Robert O. Bonow, MD, a professor of medicine at Northwestern University in Chicago, and coauthors in an editorial that accompanied the two reports (JAMA Cardiol. 2020 May 4;doi: 10.1001/jamacardio.2020.1782). The editorial cited two recently-begun prospective trials, ORCHID and RECOVERY, that are more systematically assessing the safety and efficacy of hydroxychloroquine treatment in COVID-19 patients.
The findings lend further support to a Safety Communication from the U.S. Food and Drug Administration on April 24 that reminded clinicians that the Emergency Use Authorization for hydroxychloroquine and chloroquine in COVID-19 patients that the FDA issued on March 28 applied to only certain hospitalized patients or those enrolled in clinical trials. The Safety Communication also said that agency was aware of reports of adverse arrhythmia events when COVID-19 patients received these drugs outside a hospital setting as well as uninfected people who had received one of these drugs for preventing infection.
In addition, leaders of the American College of Cardiology, the American Heart Association, and the Heart Rhythm Society on April 10 issued a summary of considerations when using hydroxychloroquine and azithromycin to treat COVID-19 patients, and noted that a way to minimized the risk from these drugs is to withhold them from patients with a QTc interval of 500 msec or greater at baseline (J Am Coll Cardiol. 2020 Apr 10. doi: 10.1016/j.jacc.2020.04.016). The summary also highlighted the need for regular ECG monitoring of COVID-19 patients who receive drugs that can prolong the QTc interval, and recommended withdrawing treatment from patients when their QTc exceeds the 500 msec threshold.
None of the authors of the two reports and editorial had relevant commercial disclosures.
The potential for serious arrhythmias from hydroxychloroquine treatment of COVID-19 patients received further documentation from a pair of studies released on May 1, casting further doubt on whether the uncertain benefit from this or related drugs to infected patients is worth the clear risks the agents pose.
A report from 90 confirmed COVID-19 patients treated with hydroxychloroquine at one Boston hospital during March-April 2020 identified a significantly prolonged, corrected QT (QTc) interval of at least 500 msec in 18 patients (20%), which included 10 patients whose QTc rose by at least 60 msec above baseline, and a total of 21 patients (23%) having a notable prolongation (JAMA Cardiol. 2020 May 4. doi: 10.1001/jamacardio.2020.1834). This series included one patient who developed torsades de pointes following treatment with hydroxychloroquine and azithromycin, “which to our knowledge has yet to be reported elsewhere in the literature,” the report said.
The second report, from a single center in Lyon, France, included 40 confirmed COVID-19 patients treated with hydroxychloroquine during 2 weeks in late March, and found that 37 (93%) had some increase in the QTc interval, including 14 patients (36%) with an increase of at least 60 msec, and 7 patients (18%) whose QTc rose to at least 500 msec (JAMA Cardiol. 2020 May. doi: 10.1001/jamacardio.2020.1787). However, none of the 40 patients in this series developed an identified ventricular arrhythmia. All patients in both studies received hydroxychloroquine for at least 1 day, and roughly half the patients in each series also received concurrent azithromycin, another drug that can prolong the QTc interval and that has been frequently used in combination with hydroxychloroquine as an unproven COVID-19 treatment cocktail.
These two reports, as well as prior report from Brazil on COVID-19 patients treated with chloroquine diphosphate (JAMA Netw Open. 2020;3[4]:e208857), “underscore the potential risk associated with widespread use of hydroxychloroquine and the combination of hydroxychloroquine and azithromycin in ambulatory patients with known or suspected COVID-19. Understanding whether this risk is worth taking in the absence of evidence of therapeutic efficacy creates a knowledge gap that needs to be addressed,” wrote Robert O. Bonow, MD, a professor of medicine at Northwestern University in Chicago, and coauthors in an editorial that accompanied the two reports (JAMA Cardiol. 2020 May 4;doi: 10.1001/jamacardio.2020.1782). The editorial cited two recently-begun prospective trials, ORCHID and RECOVERY, that are more systematically assessing the safety and efficacy of hydroxychloroquine treatment in COVID-19 patients.
The findings lend further support to a Safety Communication from the U.S. Food and Drug Administration on April 24 that reminded clinicians that the Emergency Use Authorization for hydroxychloroquine and chloroquine in COVID-19 patients that the FDA issued on March 28 applied to only certain hospitalized patients or those enrolled in clinical trials. The Safety Communication also said that agency was aware of reports of adverse arrhythmia events when COVID-19 patients received these drugs outside a hospital setting as well as uninfected people who had received one of these drugs for preventing infection.
In addition, leaders of the American College of Cardiology, the American Heart Association, and the Heart Rhythm Society on April 10 issued a summary of considerations when using hydroxychloroquine and azithromycin to treat COVID-19 patients, and noted that a way to minimized the risk from these drugs is to withhold them from patients with a QTc interval of 500 msec or greater at baseline (J Am Coll Cardiol. 2020 Apr 10. doi: 10.1016/j.jacc.2020.04.016). The summary also highlighted the need for regular ECG monitoring of COVID-19 patients who receive drugs that can prolong the QTc interval, and recommended withdrawing treatment from patients when their QTc exceeds the 500 msec threshold.
None of the authors of the two reports and editorial had relevant commercial disclosures.
The potential for serious arrhythmias from hydroxychloroquine treatment of COVID-19 patients received further documentation from a pair of studies released on May 1, casting further doubt on whether the uncertain benefit from this or related drugs to infected patients is worth the clear risks the agents pose.
A report from 90 confirmed COVID-19 patients treated with hydroxychloroquine at one Boston hospital during March-April 2020 identified a significantly prolonged, corrected QT (QTc) interval of at least 500 msec in 18 patients (20%), which included 10 patients whose QTc rose by at least 60 msec above baseline, and a total of 21 patients (23%) having a notable prolongation (JAMA Cardiol. 2020 May 4. doi: 10.1001/jamacardio.2020.1834). This series included one patient who developed torsades de pointes following treatment with hydroxychloroquine and azithromycin, “which to our knowledge has yet to be reported elsewhere in the literature,” the report said.
The second report, from a single center in Lyon, France, included 40 confirmed COVID-19 patients treated with hydroxychloroquine during 2 weeks in late March, and found that 37 (93%) had some increase in the QTc interval, including 14 patients (36%) with an increase of at least 60 msec, and 7 patients (18%) whose QTc rose to at least 500 msec (JAMA Cardiol. 2020 May. doi: 10.1001/jamacardio.2020.1787). However, none of the 40 patients in this series developed an identified ventricular arrhythmia. All patients in both studies received hydroxychloroquine for at least 1 day, and roughly half the patients in each series also received concurrent azithromycin, another drug that can prolong the QTc interval and that has been frequently used in combination with hydroxychloroquine as an unproven COVID-19 treatment cocktail.
These two reports, as well as prior report from Brazil on COVID-19 patients treated with chloroquine diphosphate (JAMA Netw Open. 2020;3[4]:e208857), “underscore the potential risk associated with widespread use of hydroxychloroquine and the combination of hydroxychloroquine and azithromycin in ambulatory patients with known or suspected COVID-19. Understanding whether this risk is worth taking in the absence of evidence of therapeutic efficacy creates a knowledge gap that needs to be addressed,” wrote Robert O. Bonow, MD, a professor of medicine at Northwestern University in Chicago, and coauthors in an editorial that accompanied the two reports (JAMA Cardiol. 2020 May 4;doi: 10.1001/jamacardio.2020.1782). The editorial cited two recently-begun prospective trials, ORCHID and RECOVERY, that are more systematically assessing the safety and efficacy of hydroxychloroquine treatment in COVID-19 patients.
The findings lend further support to a Safety Communication from the U.S. Food and Drug Administration on April 24 that reminded clinicians that the Emergency Use Authorization for hydroxychloroquine and chloroquine in COVID-19 patients that the FDA issued on March 28 applied to only certain hospitalized patients or those enrolled in clinical trials. The Safety Communication also said that agency was aware of reports of adverse arrhythmia events when COVID-19 patients received these drugs outside a hospital setting as well as uninfected people who had received one of these drugs for preventing infection.
In addition, leaders of the American College of Cardiology, the American Heart Association, and the Heart Rhythm Society on April 10 issued a summary of considerations when using hydroxychloroquine and azithromycin to treat COVID-19 patients, and noted that a way to minimized the risk from these drugs is to withhold them from patients with a QTc interval of 500 msec or greater at baseline (J Am Coll Cardiol. 2020 Apr 10. doi: 10.1016/j.jacc.2020.04.016). The summary also highlighted the need for regular ECG monitoring of COVID-19 patients who receive drugs that can prolong the QTc interval, and recommended withdrawing treatment from patients when their QTc exceeds the 500 msec threshold.
None of the authors of the two reports and editorial had relevant commercial disclosures.
FROM JAMA CARDIOLOGY
COVID-19: Social distancing with young children
Emma just celebrated her second birthday, and she has been working on the usual things that children start to master at this age: potty training, making friends, exerting her will through both actions and words, and generally enjoying life as the center of attention for both her parents and grandparents. Like everyone else in Maryland, Emma’s life changed suddenly with the coronavirus stay-at-home order that was issued on March 30. There is no more day care and her parents work from home while caring for her. Her grandparents visit, but only outside and only from a distance – there are no more hugs and there is no more sitting in her grandfather’s lap while he reads stories.

One afternoon a few weeks ago, Emma was looking out the window when she saw her friend, Max, walk by with his parents. Before her parents could stop her, Emma bolted out the door, and she and little Max wrapped each other in a tight embrace. Their parents snapped a photo of the smiling toddlers hugging before they separated the children. The photo is adorable, but as all struggle with social distancing, the poignance of two innocent toddlers in a forbidden embrace is a bit heartbreaking.
Everyone who has ever observed children knows that social distancing is not in their nature. Children play, they hug, they wrestle and tackle and poke, and sometimes even bite. And every student of social psychology has been taught about Harry Harlow’s experiments with rhesus macaques who were separated from their mothers and given access to an inanimate object to serve as a surrogate mother. The Harlow studies, while controversial, were revolutionary in demonstrating that early interactions with both a mother and with playmates were essential in the development of normal social relationships.
Regine Galanti, PhD, is a clinical psychologist at Long Island Behavioral Psychology, Cedarhurst, N.Y., who specializes in the treatment of anxiety and behavior problems. With young children she uses parent-child interaction therapy (PCIT) to help build relationships and discipline. Dr. Galanti said: “I don’t think we’re well prepared as a field to answer questions about the long-term effects of social distancing. If you need young children to socially distance, the responsibility has to fall on the adults. It’s important to explain to children what’s going on and to be honest in a developmentally appropriate way.”
Dr. Galanti has noticed that the issues that people had before COVID-19 are exacerbated by the stress of the current situation. What we do know is that young children thrive on structure.”
Tovah P. Klein, PhD, is the author of “How Toddlers Thrive” (Touchstone, 2015) and is the director of the Barnard College Center for Toddler Development in Manhattan. “When this started, we thought we would be closed for a few weeks,” Dr. Klein said. “We wanted to maintain a connection to the children, so we made videos for the parents to show to the kids, just to say ‘We’re still here.’ But as time went on and we realized it was going to be a while, we felt it was important to provide connection, so we launched a virtual program.”
Dr. Klein said that the teachers meet with their classes of 13 2-year-olds over Zoom, and when they first started, she asked the teachers to try to meet for 10 minutes. They are now meeting for 40 minutes twice a week. The children like seeing their teachers in their homes and they like seeing each other. In addition, the teachers make videos to send home and they are currently working on one to demystify masks. “We’re working on normalizing masks and showing children that when you put the mask on, you’re still there underneath.”
The center has existed for 48 years. There have been struggles for some of the children who attend; some of the parents have been hospitalized with the virus, and some work on the front line and so parents may be living away from a child.
“We’ve seen more challenging behaviors during this time, more tantrums, toileting issues, night awakenings, and more fragility. But as the new normal takes hold, things are settling in. Parents have been good about getting new routines and it helps if parents can handle their own stress,” Dr. Klein said. She also pointed out that for parents working at home while caring for their children, this can be particularly difficult on a young child. “The child knows the parent is home, but isn’t spending time with him, and he sees it as a rejection.”
Margaret Adams, MD, is a child psychiatrist in Maryland who works with very young children and their parents. She says that some of the children are thriving with the extra attention from their parents. “I often have seen difficulties with readjustment to the routine of separations to day care after a family vacation of a week, or sometimes even a weekend, even for those young ones who seem to love the social aspects of day care. I think it is likely a big impact will come upon return, depending on the developmental stage of the child,” Dr. Adams noted.
Despite the hardships of the moment, all three experts expressed hopefulness about the future for these children.
“Young children are super-resilient and that’s the blessing of this,” Dr. Galanti said. “I think they will be okay.”
Emma is home for now with her parents, who are expecting another child soon. Her mother notes: “The days are long and balancing work is an impossible challenge, but being with Emma has been a total blessing, and when would I ever have this much time to spend with my kid? She’s at such a fun age – so curious and adventurous – it’s amazing to watch her language and skills progress. I wish we weren’t in the midst of a pandemic, but Emma is definitely the bright spot.”
Dr. Miller is coauthor with Annette Hanson, MD, of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins, both in Baltimore. Dr. Miller has no disclosures.
Emma just celebrated her second birthday, and she has been working on the usual things that children start to master at this age: potty training, making friends, exerting her will through both actions and words, and generally enjoying life as the center of attention for both her parents and grandparents. Like everyone else in Maryland, Emma’s life changed suddenly with the coronavirus stay-at-home order that was issued on March 30. There is no more day care and her parents work from home while caring for her. Her grandparents visit, but only outside and only from a distance – there are no more hugs and there is no more sitting in her grandfather’s lap while he reads stories.
One afternoon a few weeks ago, Emma was looking out the window when she saw her friend, Max, walk by with his parents. Before her parents could stop her, Emma bolted out the door, and she and little Max wrapped each other in a tight embrace. Their parents snapped a photo of the smiling toddlers hugging before they separated the children. The photo is adorable, but as all struggle with social distancing, the poignance of two innocent toddlers in a forbidden embrace is a bit heartbreaking.
Everyone who has ever observed children knows that social distancing is not in their nature. Children play, they hug, they wrestle and tackle and poke, and sometimes even bite. And every student of social psychology has been taught about Harry Harlow’s experiments with rhesus macaques who were separated from their mothers and given access to an inanimate object to serve as a surrogate mother. The Harlow studies, while controversial, were revolutionary in demonstrating that early interactions with both a mother and with playmates were essential in the development of normal social relationships.
Regine Galanti, PhD, is a clinical psychologist at Long Island Behavioral Psychology, Cedarhurst, N.Y., who specializes in the treatment of anxiety and behavior problems. With young children she uses parent-child interaction therapy (PCIT) to help build relationships and discipline. Dr. Galanti said: “I don’t think we’re well prepared as a field to answer questions about the long-term effects of social distancing. If you need young children to socially distance, the responsibility has to fall on the adults. It’s important to explain to children what’s going on and to be honest in a developmentally appropriate way.”
Dr. Galanti has noticed that the issues that people had before COVID-19 are exacerbated by the stress of the current situation. What we do know is that young children thrive on structure.”
Tovah P. Klein, PhD, is the author of “How Toddlers Thrive” (Touchstone, 2015) and is the director of the Barnard College Center for Toddler Development in Manhattan. “When this started, we thought we would be closed for a few weeks,” Dr. Klein said. “We wanted to maintain a connection to the children, so we made videos for the parents to show to the kids, just to say ‘We’re still here.’ But as time went on and we realized it was going to be a while, we felt it was important to provide connection, so we launched a virtual program.”
Dr. Klein said that the teachers meet with their classes of 13 2-year-olds over Zoom, and when they first started, she asked the teachers to try to meet for 10 minutes. They are now meeting for 40 minutes twice a week. The children like seeing their teachers in their homes and they like seeing each other. In addition, the teachers make videos to send home and they are currently working on one to demystify masks. “We’re working on normalizing masks and showing children that when you put the mask on, you’re still there underneath.”
The center has existed for 48 years. There have been struggles for some of the children who attend; some of the parents have been hospitalized with the virus, and some work on the front line and so parents may be living away from a child.
“We’ve seen more challenging behaviors during this time, more tantrums, toileting issues, night awakenings, and more fragility. But as the new normal takes hold, things are settling in. Parents have been good about getting new routines and it helps if parents can handle their own stress,” Dr. Klein said. She also pointed out that for parents working at home while caring for their children, this can be particularly difficult on a young child. “The child knows the parent is home, but isn’t spending time with him, and he sees it as a rejection.”
Margaret Adams, MD, is a child psychiatrist in Maryland who works with very young children and their parents. She says that some of the children are thriving with the extra attention from their parents. “I often have seen difficulties with readjustment to the routine of separations to day care after a family vacation of a week, or sometimes even a weekend, even for those young ones who seem to love the social aspects of day care. I think it is likely a big impact will come upon return, depending on the developmental stage of the child,” Dr. Adams noted.
Despite the hardships of the moment, all three experts expressed hopefulness about the future for these children.
“Young children are super-resilient and that’s the blessing of this,” Dr. Galanti said. “I think they will be okay.”
Emma is home for now with her parents, who are expecting another child soon. Her mother notes: “The days are long and balancing work is an impossible challenge, but being with Emma has been a total blessing, and when would I ever have this much time to spend with my kid? She’s at such a fun age – so curious and adventurous – it’s amazing to watch her language and skills progress. I wish we weren’t in the midst of a pandemic, but Emma is definitely the bright spot.”
Dr. Miller is coauthor with Annette Hanson, MD, of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins, both in Baltimore. Dr. Miller has no disclosures.
Emma just celebrated her second birthday, and she has been working on the usual things that children start to master at this age: potty training, making friends, exerting her will through both actions and words, and generally enjoying life as the center of attention for both her parents and grandparents. Like everyone else in Maryland, Emma’s life changed suddenly with the coronavirus stay-at-home order that was issued on March 30. There is no more day care and her parents work from home while caring for her. Her grandparents visit, but only outside and only from a distance – there are no more hugs and there is no more sitting in her grandfather’s lap while he reads stories.
One afternoon a few weeks ago, Emma was looking out the window when she saw her friend, Max, walk by with his parents. Before her parents could stop her, Emma bolted out the door, and she and little Max wrapped each other in a tight embrace. Their parents snapped a photo of the smiling toddlers hugging before they separated the children. The photo is adorable, but as all struggle with social distancing, the poignance of two innocent toddlers in a forbidden embrace is a bit heartbreaking.
Everyone who has ever observed children knows that social distancing is not in their nature. Children play, they hug, they wrestle and tackle and poke, and sometimes even bite. And every student of social psychology has been taught about Harry Harlow’s experiments with rhesus macaques who were separated from their mothers and given access to an inanimate object to serve as a surrogate mother. The Harlow studies, while controversial, were revolutionary in demonstrating that early interactions with both a mother and with playmates were essential in the development of normal social relationships.
Regine Galanti, PhD, is a clinical psychologist at Long Island Behavioral Psychology, Cedarhurst, N.Y., who specializes in the treatment of anxiety and behavior problems. With young children she uses parent-child interaction therapy (PCIT) to help build relationships and discipline. Dr. Galanti said: “I don’t think we’re well prepared as a field to answer questions about the long-term effects of social distancing. If you need young children to socially distance, the responsibility has to fall on the adults. It’s important to explain to children what’s going on and to be honest in a developmentally appropriate way.”
Dr. Galanti has noticed that the issues that people had before COVID-19 are exacerbated by the stress of the current situation. What we do know is that young children thrive on structure.”
Tovah P. Klein, PhD, is the author of “How Toddlers Thrive” (Touchstone, 2015) and is the director of the Barnard College Center for Toddler Development in Manhattan. “When this started, we thought we would be closed for a few weeks,” Dr. Klein said. “We wanted to maintain a connection to the children, so we made videos for the parents to show to the kids, just to say ‘We’re still here.’ But as time went on and we realized it was going to be a while, we felt it was important to provide connection, so we launched a virtual program.”
Dr. Klein said that the teachers meet with their classes of 13 2-year-olds over Zoom, and when they first started, she asked the teachers to try to meet for 10 minutes. They are now meeting for 40 minutes twice a week. The children like seeing their teachers in their homes and they like seeing each other. In addition, the teachers make videos to send home and they are currently working on one to demystify masks. “We’re working on normalizing masks and showing children that when you put the mask on, you’re still there underneath.”
The center has existed for 48 years. There have been struggles for some of the children who attend; some of the parents have been hospitalized with the virus, and some work on the front line and so parents may be living away from a child.
“We’ve seen more challenging behaviors during this time, more tantrums, toileting issues, night awakenings, and more fragility. But as the new normal takes hold, things are settling in. Parents have been good about getting new routines and it helps if parents can handle their own stress,” Dr. Klein said. She also pointed out that for parents working at home while caring for their children, this can be particularly difficult on a young child. “The child knows the parent is home, but isn’t spending time with him, and he sees it as a rejection.”
Margaret Adams, MD, is a child psychiatrist in Maryland who works with very young children and their parents. She says that some of the children are thriving with the extra attention from their parents. “I often have seen difficulties with readjustment to the routine of separations to day care after a family vacation of a week, or sometimes even a weekend, even for those young ones who seem to love the social aspects of day care. I think it is likely a big impact will come upon return, depending on the developmental stage of the child,” Dr. Adams noted.
Despite the hardships of the moment, all three experts expressed hopefulness about the future for these children.
“Young children are super-resilient and that’s the blessing of this,” Dr. Galanti said. “I think they will be okay.”
Emma is home for now with her parents, who are expecting another child soon. Her mother notes: “The days are long and balancing work is an impossible challenge, but being with Emma has been a total blessing, and when would I ever have this much time to spend with my kid? She’s at such a fun age – so curious and adventurous – it’s amazing to watch her language and skills progress. I wish we weren’t in the midst of a pandemic, but Emma is definitely the bright spot.”
Dr. Miller is coauthor with Annette Hanson, MD, of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins, both in Baltimore. Dr. Miller has no disclosures.
Shoulder arthroplasty template data require careful interpretation
Proprietary templating software to guide the positioning of total shoulder arthroplasty (TSA) generate very different measures for inclination and version, according to a study that compared four programs and reported in an abstract scheduled for release at the annual meeting of the American Academy of Orthopaedic Surgeons. The meeting was canceled due to COVID-19.
“It is not a question of one software being better than another. They are just different, and they are device specific,” reported Brent B. Wiesel, MD, chief of the shoulder service at the MedStar Georgetown Orthopaedic Institute, Washington.
The variations were substantial and clinically relevant, suggesting that surgeons need to be aware of these differences when switching between the devices, according to Dr. Wiesel. He said that there is no gold standard for positioning total shoulder arthroplasty, which prevents any conclusion about the superiority of one over the other.
In this study, 76 CT scans obtained from shoulders of patients with glenohumeral arthritis were analyzed for native glenoid version and inclination by the ArthrexVIP, Tornier BluePrint, Stryker TrueSight, and ExactechGPS software programs. Dr. Wiesel explained that these are among the most commonly used programs, but there are others.
After extracting the recommended version and inclination measures from each software program, agreement between measures was calculated with an analysis of variance (ANOVA) test. The variance across programs was highly significant for both native glenoid version and inclination (P < .001).
Inter-rater reliability of the software outputs analyzed with Krippendorff’s alpha, for which a value of 1.0 signals perfect agreement and a value of 0 signals complete disagreement, reinforced the discord. For the 76 scans, the values for version and inclination were 0.272 and 0.303, respectively. Both are extremely low.
“The suggested threshold for high reliability is a value of 0.8 or greater,” said Dr. Wiesel, who was contacted about these data after the AAOS annual meeting was canceled. “The lowest acceptable limit for reliability is 0.667 or greater.”
There was disagreement across all programs. The only agreement to reach an acceptable Krippendorff’s alpha was generated by the Tornier BluePrint and Stryker TrueSight programs. These programs modestly agreed on version (0.706 on the Krippendorff’s alpha), but agreement on inclination was below the acceptable threshold.
“In other words, if you take the same scan from the same patient, you will get different angles from these different templating software programs,” Dr. Wiesel said.
There are several messages from these data, according to Dr. Wiesel. In addition to demonstrating the programs generate outputs that do not agree, he suggested that the values provided by the programs should not be considered absolute. Rather, the software values should be interpreted in the context of the individual patient.
“It is easy to get lazy, but it is important to remember that the software is a tool rather than something that will do the procedure for you,” Dr. Wiesel said. He reported that when the software guidance is not consistent with his own experience, he proceeds cautiously.
“On several occasions when the software has provided measures that are not consistent with my own perception, I have not been happy when I went with the software,” he said. “So typically I go with my gut when there is a discrepancy, and the data from this study supports that.”
Because of the difficulty in creating a gold standard for templating when there are multiple variables that influence optimal positioning of components, Dr. Wiesel suggested that “crowd thinking” might eventually determine the values that produce the best results. By crowd thinking, he was referring to Big Data analysis, collating data from a large number of cases performed by a large number of surgeons.
“All of these software programs provide reasonable guidance, but each has different advantages and disadvantages, and it is important to be aware that they are different,” Dr. Wiesel reported.
There are differences in the templating software, and they should be taken into consideration, according to another expert who has looked at this issue. Senior author of a randomized trial evaluating planning strategies for total shoulder arthroplasty ( J Bone Joint Surg AM. 2019:101;446-57), Eric T. Ricchetti, MD, an orthopedic surgeon and director of the shoulder center at the Cleveland Clinic, offered a similar perspective on templating.
“I agree that surgeons should be familiar with the differences that exist in templating software,” Dr. Ricchetti said. Basing his remarks on his own experience and reiterating the conclusion of the AAOS study, he added, “the methods that are used to identify the bone anatomy of the shoulder can vary across software programs, potentially resulting in differences in subsequent measures of glenoid pathology, such as version and inclination, that may impact surgical decision making.”
Dr. Wiesel reports no potential conflicts of interest.
SOURCE: Wiesel B et al. AAOS 2020. Abstract 212.
Proprietary templating software to guide the positioning of total shoulder arthroplasty (TSA) generate very different measures for inclination and version, according to a study that compared four programs and reported in an abstract scheduled for release at the annual meeting of the American Academy of Orthopaedic Surgeons. The meeting was canceled due to COVID-19.
“It is not a question of one software being better than another. They are just different, and they are device specific,” reported Brent B. Wiesel, MD, chief of the shoulder service at the MedStar Georgetown Orthopaedic Institute, Washington.
The variations were substantial and clinically relevant, suggesting that surgeons need to be aware of these differences when switching between the devices, according to Dr. Wiesel. He said that there is no gold standard for positioning total shoulder arthroplasty, which prevents any conclusion about the superiority of one over the other.
In this study, 76 CT scans obtained from shoulders of patients with glenohumeral arthritis were analyzed for native glenoid version and inclination by the ArthrexVIP, Tornier BluePrint, Stryker TrueSight, and ExactechGPS software programs. Dr. Wiesel explained that these are among the most commonly used programs, but there are others.
After extracting the recommended version and inclination measures from each software program, agreement between measures was calculated with an analysis of variance (ANOVA) test. The variance across programs was highly significant for both native glenoid version and inclination (P < .001).
Inter-rater reliability of the software outputs analyzed with Krippendorff’s alpha, for which a value of 1.0 signals perfect agreement and a value of 0 signals complete disagreement, reinforced the discord. For the 76 scans, the values for version and inclination were 0.272 and 0.303, respectively. Both are extremely low.
“The suggested threshold for high reliability is a value of 0.8 or greater,” said Dr. Wiesel, who was contacted about these data after the AAOS annual meeting was canceled. “The lowest acceptable limit for reliability is 0.667 or greater.”
There was disagreement across all programs. The only agreement to reach an acceptable Krippendorff’s alpha was generated by the Tornier BluePrint and Stryker TrueSight programs. These programs modestly agreed on version (0.706 on the Krippendorff’s alpha), but agreement on inclination was below the acceptable threshold.
“In other words, if you take the same scan from the same patient, you will get different angles from these different templating software programs,” Dr. Wiesel said.
There are several messages from these data, according to Dr. Wiesel. In addition to demonstrating the programs generate outputs that do not agree, he suggested that the values provided by the programs should not be considered absolute. Rather, the software values should be interpreted in the context of the individual patient.
“It is easy to get lazy, but it is important to remember that the software is a tool rather than something that will do the procedure for you,” Dr. Wiesel said. He reported that when the software guidance is not consistent with his own experience, he proceeds cautiously.
“On several occasions when the software has provided measures that are not consistent with my own perception, I have not been happy when I went with the software,” he said. “So typically I go with my gut when there is a discrepancy, and the data from this study supports that.”
Because of the difficulty in creating a gold standard for templating when there are multiple variables that influence optimal positioning of components, Dr. Wiesel suggested that “crowd thinking” might eventually determine the values that produce the best results. By crowd thinking, he was referring to Big Data analysis, collating data from a large number of cases performed by a large number of surgeons.
“All of these software programs provide reasonable guidance, but each has different advantages and disadvantages, and it is important to be aware that they are different,” Dr. Wiesel reported.
There are differences in the templating software, and they should be taken into consideration, according to another expert who has looked at this issue. Senior author of a randomized trial evaluating planning strategies for total shoulder arthroplasty ( J Bone Joint Surg AM. 2019:101;446-57), Eric T. Ricchetti, MD, an orthopedic surgeon and director of the shoulder center at the Cleveland Clinic, offered a similar perspective on templating.
“I agree that surgeons should be familiar with the differences that exist in templating software,” Dr. Ricchetti said. Basing his remarks on his own experience and reiterating the conclusion of the AAOS study, he added, “the methods that are used to identify the bone anatomy of the shoulder can vary across software programs, potentially resulting in differences in subsequent measures of glenoid pathology, such as version and inclination, that may impact surgical decision making.”
Dr. Wiesel reports no potential conflicts of interest.
SOURCE: Wiesel B et al. AAOS 2020. Abstract 212.
Proprietary templating software to guide the positioning of total shoulder arthroplasty (TSA) generate very different measures for inclination and version, according to a study that compared four programs and reported in an abstract scheduled for release at the annual meeting of the American Academy of Orthopaedic Surgeons. The meeting was canceled due to COVID-19.
“It is not a question of one software being better than another. They are just different, and they are device specific,” reported Brent B. Wiesel, MD, chief of the shoulder service at the MedStar Georgetown Orthopaedic Institute, Washington.
The variations were substantial and clinically relevant, suggesting that surgeons need to be aware of these differences when switching between the devices, according to Dr. Wiesel. He said that there is no gold standard for positioning total shoulder arthroplasty, which prevents any conclusion about the superiority of one over the other.
In this study, 76 CT scans obtained from shoulders of patients with glenohumeral arthritis were analyzed for native glenoid version and inclination by the ArthrexVIP, Tornier BluePrint, Stryker TrueSight, and ExactechGPS software programs. Dr. Wiesel explained that these are among the most commonly used programs, but there are others.
After extracting the recommended version and inclination measures from each software program, agreement between measures was calculated with an analysis of variance (ANOVA) test. The variance across programs was highly significant for both native glenoid version and inclination (P < .001).
Inter-rater reliability of the software outputs analyzed with Krippendorff’s alpha, for which a value of 1.0 signals perfect agreement and a value of 0 signals complete disagreement, reinforced the discord. For the 76 scans, the values for version and inclination were 0.272 and 0.303, respectively. Both are extremely low.
“The suggested threshold for high reliability is a value of 0.8 or greater,” said Dr. Wiesel, who was contacted about these data after the AAOS annual meeting was canceled. “The lowest acceptable limit for reliability is 0.667 or greater.”
There was disagreement across all programs. The only agreement to reach an acceptable Krippendorff’s alpha was generated by the Tornier BluePrint and Stryker TrueSight programs. These programs modestly agreed on version (0.706 on the Krippendorff’s alpha), but agreement on inclination was below the acceptable threshold.
“In other words, if you take the same scan from the same patient, you will get different angles from these different templating software programs,” Dr. Wiesel said.
There are several messages from these data, according to Dr. Wiesel. In addition to demonstrating the programs generate outputs that do not agree, he suggested that the values provided by the programs should not be considered absolute. Rather, the software values should be interpreted in the context of the individual patient.
“It is easy to get lazy, but it is important to remember that the software is a tool rather than something that will do the procedure for you,” Dr. Wiesel said. He reported that when the software guidance is not consistent with his own experience, he proceeds cautiously.
“On several occasions when the software has provided measures that are not consistent with my own perception, I have not been happy when I went with the software,” he said. “So typically I go with my gut when there is a discrepancy, and the data from this study supports that.”
Because of the difficulty in creating a gold standard for templating when there are multiple variables that influence optimal positioning of components, Dr. Wiesel suggested that “crowd thinking” might eventually determine the values that produce the best results. By crowd thinking, he was referring to Big Data analysis, collating data from a large number of cases performed by a large number of surgeons.
“All of these software programs provide reasonable guidance, but each has different advantages and disadvantages, and it is important to be aware that they are different,” Dr. Wiesel reported.
There are differences in the templating software, and they should be taken into consideration, according to another expert who has looked at this issue. Senior author of a randomized trial evaluating planning strategies for total shoulder arthroplasty ( J Bone Joint Surg AM. 2019:101;446-57), Eric T. Ricchetti, MD, an orthopedic surgeon and director of the shoulder center at the Cleveland Clinic, offered a similar perspective on templating.
“I agree that surgeons should be familiar with the differences that exist in templating software,” Dr. Ricchetti said. Basing his remarks on his own experience and reiterating the conclusion of the AAOS study, he added, “the methods that are used to identify the bone anatomy of the shoulder can vary across software programs, potentially resulting in differences in subsequent measures of glenoid pathology, such as version and inclination, that may impact surgical decision making.”
Dr. Wiesel reports no potential conflicts of interest.
SOURCE: Wiesel B et al. AAOS 2020. Abstract 212.
FROM AAOS 2020
COVID-19: To have and to hold ... in quarantine
Tips for marriage survival during a pandemic
Most married couples vowed to stay with their partners during sickness and health, but none of us vowed to remain trapped with our loved ones behind the same four walls, all day, every day, for an unknown period of time. We didn’t sign up for this! Some romantics may be titillated by the prospect, while more independent partners may panic at the mere thought of spending all day and night with their loved ones.

Because of the swift implementation of the lifestyle-altering restrictions, couples did not have ample time to mentally and physically prepare. A lack of preparation and loss of control heightens our emotions. It can make couples more susceptible to engage in unhealthy styles of communication and destructive behaviors that are harmful to their relationships.
There are psychological reasons that “absence makes the heart grow fonder.” Distance from your partner is not just a clever way to make your partner appreciate and desire you more. It is human nature to habituate to what is part of your daily life. For instance, when your partner is away from you while on a work trip, you may find the first night or two alone relaxing; but by day 3, you begin to miss your partner’s hugs and kisses, smell, and touch. And after many days apart, you may even miss the incessant nagging that secretly motivates you. Physical distance from our partners essentially gives us the ability to long for and appreciate each other. Our brains are wired to pay more attention to things that are novel and exciting and less interested in what is in our everyday lives.
Separation gives us the ability to miss our partners, while quarantine does the complete opposite.
To avoid contemplating how to murder one’s spouse before quarantine ends, partners can strengthen their relationships by using the strategies I’ve outlined below, which are loosely based on dialectical behavior therapy (DBT). These strategies can be useful for anyone – providers and patients alike – going through these struggles.
Dialectical behavior therapy was developed by psychologist Marsha Linehan PhD, to help regulate emotions for people diagnosed with borderline personality disorder. These skills help to identify thoughts and feelings, to accept one’s inner emotional world and outward behaviors. The idea is that, once you can recognize and accept, then change is possible. The “dialectic” in dialectical behavior therapy implies that one is attempting to find a balance between acceptance and change. All of us can benefit from these skills, especially emotionally volatile couples who are trapped together in quarantine.
Radically accept what is uncertain in your lives
Radical acceptance is a practice used in DBT in situations that are out of our control, such as the COVID-19 pandemic. Radically accept that you and your partner are trapped in quarantine without attempting to place blame on our government, your spouse, your boss, and even yourself. Radical acceptance is exactly what the name implies. Accept your current situation for what it is and not what you hoped it to be.
Accept the unknown and unanswered questions such as when will this quarantine end? Will there be a summer camp? Will I get back to my office this summer? Will my children even return to school in the fall? The acceptance of what is out of your control will ultimately decrease your mental time spent worrying and obsessing about the uncertainties of your post-quarantine life and instead provide you more time to be present with your spouse.
Remain mindful during all communication with your spouse. To stay in the moment, you need to be aware of your bodily reactions to distress and notice when your heart rate increases, breathing becomes more shallow, stomach muscles tighten, and when your thoughts become more negative. Mindfulness skills enable us to use physiological changes in our body to become aware of our emotions. You can use your partner’s nonverbal body language and tone of voice to gauge that person’s emotional reactivity.
The practice of mindfulness leads to an increased emotional intelligence. The goal is to have enough self-awareness and emotional understanding of your partner and enough empathy to know when a conversation is becoming too emotionally charged and to let it go and back off. Mindfulness is not nagging your partner to remember to change the heating unit filters with a reminder of what happened years ago when this wasn’t done promptly – without first checking in to make sure your partner is emotionally ready for this type of conversation.
When we have strong emotions, we are using the more primitive parts of our brain that induce a fight or flight reaction. These emotional reactions overshadow the more advanced prefrontal region of our brain that stores our rational thoughts and reasoning skills, a concept identified by psychologist Daniel Goleman as “emotional hijacking.”
Use distress tolerance skills to deal with negative emotions
Distress tolerance is an individual’s ability to manage feelings in response to stress. Distress tolerance skills are aimed at helping one manage intense emotions without worsening a situation by engaging in behaviors that are destructive and may exacerbate the problem. The goal is to tolerate the stress while with your partner and not respond negatively or in a way that is harmful to the integrity of your relationship.
To prioritize your relationship, this may mean that you choose not to react negatively when your partner makes a passive-aggressive comment on how you spent your day during quarantine since you still have a pile of laundry on your bedroom floor and overflowing dishes in the kitchen sink. A high level of distress tolerance will enable you to not overreact or withdraw from your spouse when flooded with emotions of anger or sadness.
Distraction techniques are a type of distress tolerance skill. You can engage in activities that keep you distracted and require your full attention. When things get heated between you and your spouse during quarantine, try to obtain some distance from each other to cool down and engage in an activity that involves your full concentration.
Many of us have been surprised by our hidden talents that were discovered during the quarantine. Use the time away from your partner to distract yourself with your new passion for writing, baking, organizing, and even your newfound love of balloon artistry. Do an activity that engages your mind and provides you the necessary physical and mental time away from your partner to deescalate. You can always revisit the initial cause of the conflict when both you and your partner are not emotionally charged. You can also distract yourself with self-soothing tactics such as taking a warm bath or a reading good book. Perhaps distract yourself by giving back to others and spending time planning a drive-by surprise party for your sister’s birthday next month. It can be helpful to distract yourself by comparing yourself to others less fortunate than you or a time in your life when you and your partner were struggling much worse than now, to provide perspective. The goal is not to add to your distress but instead, provide yourself a sense of perspective.
Use interpersonal effectiveness skills to establish a healthy relationship
Be gentle in all your communications with your partner, think about your spouse’s perspective, show empathy and interest in what your partner has to say by your verbal communication or body language, such as maintaining eye contact, and offer recognitional cues, such as “uh-huh” and “oh, really.” Avoid communication that is at all invalidating. Never start a sentence with “YOU” while having heated conversations with your spouse; instead, use “I feel” statements. This type of communication avoids the blame game that gets many couples into trouble.
Instead, communicate how you feel while not necessarily blaming your spouse but rather expressing your emotions. This will ultimately lead to less defensive communication from your partner. Remember that not all communication is for the sole purpose of communicating. Much of the time, communication is used as an attempt for one partner to connect with the other partner. Couples may say that they have difficulty with communication when it is not the communication that is the issue but instead the underlying disconnect of the couple.
This disconnect usually manifests while couples are communicating, and therefore, can be misconstrued as solely a communication issue by the couple. When your partner asks you to stop staring at your phone during dinner, it is not necessarily that your spouse is attempting to control you or wants to engage in some deep conversation, but more likely a bid to try to connect with you. Your partner is attempting to tell you that he or she feels disconnected, misses you, and wants to reconnect.
Provide validation and acceptance to your partner
Focus on your partner’s strengths and accept the weaknesses. Accept that your partner is scattered, disorganized, and takes at least 20 minutes to find the phone and keys every morning. Remember that during your courtship days, you found your partner’s flighty attributes to be endearing. Do the same for your strengths and weaknesses.
Accept that the pandemic is unpredictable and that you may need to strengthen your ability to be flexible and more adaptable. This will ultimately lead to feeling less disappointment by your partner and more accepting of shortcomings. Acceptance of your imperfections will improve your sense of worth and confidence and lessen negative emotions, such as guilt, regret, and shame.
Accept the fact that, as similar as we all are, we use different methods to recharge ourselves. In contrast, your spouse needs alone time without distractions to reboot mentally and prepare for the following day. In the pre-pandemic world, if there were a mismatch in what a couple needed to feel rejuvenated, they could independently compensate and search for fulfillment outside of the home. Before stay-at-home orders were rolled out throughout the country, spouses had ample opportunities to spend time away from their partners at work, dinner with friends, or while squeezing in a 7 p.m. yoga sculpt class – barely getting home in time to kiss our children goodnight – with a few minutes to spare to engage in mundane conversation with our partners before our nighttime routine of TV commenced. Unfortunately, COVID-19 has made it very hard for couples to carve out that time for compensatory activities outside of the home.
Remember that you are a team
Remind yourself of the reason why you initially fell in love with your partner. Teammates do not keep score or compete with one another. They support each other when one player is not feeling well, and they make sacrifices for the betterment of the team.
Your marriage vows included “through sickness and health” and now should include “through quarantine.”
Dr. Abraham is a psychiatrist in private practice in Philadelphia. She has no disclosures.
Tips for marriage survival during a pandemic
Tips for marriage survival during a pandemic
Most married couples vowed to stay with their partners during sickness and health, but none of us vowed to remain trapped with our loved ones behind the same four walls, all day, every day, for an unknown period of time. We didn’t sign up for this! Some romantics may be titillated by the prospect, while more independent partners may panic at the mere thought of spending all day and night with their loved ones.
Because of the swift implementation of the lifestyle-altering restrictions, couples did not have ample time to mentally and physically prepare. A lack of preparation and loss of control heightens our emotions. It can make couples more susceptible to engage in unhealthy styles of communication and destructive behaviors that are harmful to their relationships.
There are psychological reasons that “absence makes the heart grow fonder.” Distance from your partner is not just a clever way to make your partner appreciate and desire you more. It is human nature to habituate to what is part of your daily life. For instance, when your partner is away from you while on a work trip, you may find the first night or two alone relaxing; but by day 3, you begin to miss your partner’s hugs and kisses, smell, and touch. And after many days apart, you may even miss the incessant nagging that secretly motivates you. Physical distance from our partners essentially gives us the ability to long for and appreciate each other. Our brains are wired to pay more attention to things that are novel and exciting and less interested in what is in our everyday lives.
Separation gives us the ability to miss our partners, while quarantine does the complete opposite.
To avoid contemplating how to murder one’s spouse before quarantine ends, partners can strengthen their relationships by using the strategies I’ve outlined below, which are loosely based on dialectical behavior therapy (DBT). These strategies can be useful for anyone – providers and patients alike – going through these struggles.
Dialectical behavior therapy was developed by psychologist Marsha Linehan PhD, to help regulate emotions for people diagnosed with borderline personality disorder. These skills help to identify thoughts and feelings, to accept one’s inner emotional world and outward behaviors. The idea is that, once you can recognize and accept, then change is possible. The “dialectic” in dialectical behavior therapy implies that one is attempting to find a balance between acceptance and change. All of us can benefit from these skills, especially emotionally volatile couples who are trapped together in quarantine.
Radically accept what is uncertain in your lives
Radical acceptance is a practice used in DBT in situations that are out of our control, such as the COVID-19 pandemic. Radically accept that you and your partner are trapped in quarantine without attempting to place blame on our government, your spouse, your boss, and even yourself. Radical acceptance is exactly what the name implies. Accept your current situation for what it is and not what you hoped it to be.
Accept the unknown and unanswered questions such as when will this quarantine end? Will there be a summer camp? Will I get back to my office this summer? Will my children even return to school in the fall? The acceptance of what is out of your control will ultimately decrease your mental time spent worrying and obsessing about the uncertainties of your post-quarantine life and instead provide you more time to be present with your spouse.
Remain mindful during all communication with your spouse. To stay in the moment, you need to be aware of your bodily reactions to distress and notice when your heart rate increases, breathing becomes more shallow, stomach muscles tighten, and when your thoughts become more negative. Mindfulness skills enable us to use physiological changes in our body to become aware of our emotions. You can use your partner’s nonverbal body language and tone of voice to gauge that person’s emotional reactivity.
The practice of mindfulness leads to an increased emotional intelligence. The goal is to have enough self-awareness and emotional understanding of your partner and enough empathy to know when a conversation is becoming too emotionally charged and to let it go and back off. Mindfulness is not nagging your partner to remember to change the heating unit filters with a reminder of what happened years ago when this wasn’t done promptly – without first checking in to make sure your partner is emotionally ready for this type of conversation.
When we have strong emotions, we are using the more primitive parts of our brain that induce a fight or flight reaction. These emotional reactions overshadow the more advanced prefrontal region of our brain that stores our rational thoughts and reasoning skills, a concept identified by psychologist Daniel Goleman as “emotional hijacking.”
Use distress tolerance skills to deal with negative emotions
Distress tolerance is an individual’s ability to manage feelings in response to stress. Distress tolerance skills are aimed at helping one manage intense emotions without worsening a situation by engaging in behaviors that are destructive and may exacerbate the problem. The goal is to tolerate the stress while with your partner and not respond negatively or in a way that is harmful to the integrity of your relationship.
To prioritize your relationship, this may mean that you choose not to react negatively when your partner makes a passive-aggressive comment on how you spent your day during quarantine since you still have a pile of laundry on your bedroom floor and overflowing dishes in the kitchen sink. A high level of distress tolerance will enable you to not overreact or withdraw from your spouse when flooded with emotions of anger or sadness.
Distraction techniques are a type of distress tolerance skill. You can engage in activities that keep you distracted and require your full attention. When things get heated between you and your spouse during quarantine, try to obtain some distance from each other to cool down and engage in an activity that involves your full concentration.
Many of us have been surprised by our hidden talents that were discovered during the quarantine. Use the time away from your partner to distract yourself with your new passion for writing, baking, organizing, and even your newfound love of balloon artistry. Do an activity that engages your mind and provides you the necessary physical and mental time away from your partner to deescalate. You can always revisit the initial cause of the conflict when both you and your partner are not emotionally charged. You can also distract yourself with self-soothing tactics such as taking a warm bath or a reading good book. Perhaps distract yourself by giving back to others and spending time planning a drive-by surprise party for your sister’s birthday next month. It can be helpful to distract yourself by comparing yourself to others less fortunate than you or a time in your life when you and your partner were struggling much worse than now, to provide perspective. The goal is not to add to your distress but instead, provide yourself a sense of perspective.
Use interpersonal effectiveness skills to establish a healthy relationship
Be gentle in all your communications with your partner, think about your spouse’s perspective, show empathy and interest in what your partner has to say by your verbal communication or body language, such as maintaining eye contact, and offer recognitional cues, such as “uh-huh” and “oh, really.” Avoid communication that is at all invalidating. Never start a sentence with “YOU” while having heated conversations with your spouse; instead, use “I feel” statements. This type of communication avoids the blame game that gets many couples into trouble.
Instead, communicate how you feel while not necessarily blaming your spouse but rather expressing your emotions. This will ultimately lead to less defensive communication from your partner. Remember that not all communication is for the sole purpose of communicating. Much of the time, communication is used as an attempt for one partner to connect with the other partner. Couples may say that they have difficulty with communication when it is not the communication that is the issue but instead the underlying disconnect of the couple.
This disconnect usually manifests while couples are communicating, and therefore, can be misconstrued as solely a communication issue by the couple. When your partner asks you to stop staring at your phone during dinner, it is not necessarily that your spouse is attempting to control you or wants to engage in some deep conversation, but more likely a bid to try to connect with you. Your partner is attempting to tell you that he or she feels disconnected, misses you, and wants to reconnect.
Provide validation and acceptance to your partner
Focus on your partner’s strengths and accept the weaknesses. Accept that your partner is scattered, disorganized, and takes at least 20 minutes to find the phone and keys every morning. Remember that during your courtship days, you found your partner’s flighty attributes to be endearing. Do the same for your strengths and weaknesses.
Accept that the pandemic is unpredictable and that you may need to strengthen your ability to be flexible and more adaptable. This will ultimately lead to feeling less disappointment by your partner and more accepting of shortcomings. Acceptance of your imperfections will improve your sense of worth and confidence and lessen negative emotions, such as guilt, regret, and shame.
Accept the fact that, as similar as we all are, we use different methods to recharge ourselves. In contrast, your spouse needs alone time without distractions to reboot mentally and prepare for the following day. In the pre-pandemic world, if there were a mismatch in what a couple needed to feel rejuvenated, they could independently compensate and search for fulfillment outside of the home. Before stay-at-home orders were rolled out throughout the country, spouses had ample opportunities to spend time away from their partners at work, dinner with friends, or while squeezing in a 7 p.m. yoga sculpt class – barely getting home in time to kiss our children goodnight – with a few minutes to spare to engage in mundane conversation with our partners before our nighttime routine of TV commenced. Unfortunately, COVID-19 has made it very hard for couples to carve out that time for compensatory activities outside of the home.
Remember that you are a team
Remind yourself of the reason why you initially fell in love with your partner. Teammates do not keep score or compete with one another. They support each other when one player is not feeling well, and they make sacrifices for the betterment of the team.
Your marriage vows included “through sickness and health” and now should include “through quarantine.”
Dr. Abraham is a psychiatrist in private practice in Philadelphia. She has no disclosures.
Most married couples vowed to stay with their partners during sickness and health, but none of us vowed to remain trapped with our loved ones behind the same four walls, all day, every day, for an unknown period of time. We didn’t sign up for this! Some romantics may be titillated by the prospect, while more independent partners may panic at the mere thought of spending all day and night with their loved ones.
Because of the swift implementation of the lifestyle-altering restrictions, couples did not have ample time to mentally and physically prepare. A lack of preparation and loss of control heightens our emotions. It can make couples more susceptible to engage in unhealthy styles of communication and destructive behaviors that are harmful to their relationships.
There are psychological reasons that “absence makes the heart grow fonder.” Distance from your partner is not just a clever way to make your partner appreciate and desire you more. It is human nature to habituate to what is part of your daily life. For instance, when your partner is away from you while on a work trip, you may find the first night or two alone relaxing; but by day 3, you begin to miss your partner’s hugs and kisses, smell, and touch. And after many days apart, you may even miss the incessant nagging that secretly motivates you. Physical distance from our partners essentially gives us the ability to long for and appreciate each other. Our brains are wired to pay more attention to things that are novel and exciting and less interested in what is in our everyday lives.
Separation gives us the ability to miss our partners, while quarantine does the complete opposite.
To avoid contemplating how to murder one’s spouse before quarantine ends, partners can strengthen their relationships by using the strategies I’ve outlined below, which are loosely based on dialectical behavior therapy (DBT). These strategies can be useful for anyone – providers and patients alike – going through these struggles.
Dialectical behavior therapy was developed by psychologist Marsha Linehan PhD, to help regulate emotions for people diagnosed with borderline personality disorder. These skills help to identify thoughts and feelings, to accept one’s inner emotional world and outward behaviors. The idea is that, once you can recognize and accept, then change is possible. The “dialectic” in dialectical behavior therapy implies that one is attempting to find a balance between acceptance and change. All of us can benefit from these skills, especially emotionally volatile couples who are trapped together in quarantine.
Radically accept what is uncertain in your lives
Radical acceptance is a practice used in DBT in situations that are out of our control, such as the COVID-19 pandemic. Radically accept that you and your partner are trapped in quarantine without attempting to place blame on our government, your spouse, your boss, and even yourself. Radical acceptance is exactly what the name implies. Accept your current situation for what it is and not what you hoped it to be.
Accept the unknown and unanswered questions such as when will this quarantine end? Will there be a summer camp? Will I get back to my office this summer? Will my children even return to school in the fall? The acceptance of what is out of your control will ultimately decrease your mental time spent worrying and obsessing about the uncertainties of your post-quarantine life and instead provide you more time to be present with your spouse.
Remain mindful during all communication with your spouse. To stay in the moment, you need to be aware of your bodily reactions to distress and notice when your heart rate increases, breathing becomes more shallow, stomach muscles tighten, and when your thoughts become more negative. Mindfulness skills enable us to use physiological changes in our body to become aware of our emotions. You can use your partner’s nonverbal body language and tone of voice to gauge that person’s emotional reactivity.
The practice of mindfulness leads to an increased emotional intelligence. The goal is to have enough self-awareness and emotional understanding of your partner and enough empathy to know when a conversation is becoming too emotionally charged and to let it go and back off. Mindfulness is not nagging your partner to remember to change the heating unit filters with a reminder of what happened years ago when this wasn’t done promptly – without first checking in to make sure your partner is emotionally ready for this type of conversation.
When we have strong emotions, we are using the more primitive parts of our brain that induce a fight or flight reaction. These emotional reactions overshadow the more advanced prefrontal region of our brain that stores our rational thoughts and reasoning skills, a concept identified by psychologist Daniel Goleman as “emotional hijacking.”
Use distress tolerance skills to deal with negative emotions
Distress tolerance is an individual’s ability to manage feelings in response to stress. Distress tolerance skills are aimed at helping one manage intense emotions without worsening a situation by engaging in behaviors that are destructive and may exacerbate the problem. The goal is to tolerate the stress while with your partner and not respond negatively or in a way that is harmful to the integrity of your relationship.
To prioritize your relationship, this may mean that you choose not to react negatively when your partner makes a passive-aggressive comment on how you spent your day during quarantine since you still have a pile of laundry on your bedroom floor and overflowing dishes in the kitchen sink. A high level of distress tolerance will enable you to not overreact or withdraw from your spouse when flooded with emotions of anger or sadness.
Distraction techniques are a type of distress tolerance skill. You can engage in activities that keep you distracted and require your full attention. When things get heated between you and your spouse during quarantine, try to obtain some distance from each other to cool down and engage in an activity that involves your full concentration.
Many of us have been surprised by our hidden talents that were discovered during the quarantine. Use the time away from your partner to distract yourself with your new passion for writing, baking, organizing, and even your newfound love of balloon artistry. Do an activity that engages your mind and provides you the necessary physical and mental time away from your partner to deescalate. You can always revisit the initial cause of the conflict when both you and your partner are not emotionally charged. You can also distract yourself with self-soothing tactics such as taking a warm bath or a reading good book. Perhaps distract yourself by giving back to others and spending time planning a drive-by surprise party for your sister’s birthday next month. It can be helpful to distract yourself by comparing yourself to others less fortunate than you or a time in your life when you and your partner were struggling much worse than now, to provide perspective. The goal is not to add to your distress but instead, provide yourself a sense of perspective.
Use interpersonal effectiveness skills to establish a healthy relationship
Be gentle in all your communications with your partner, think about your spouse’s perspective, show empathy and interest in what your partner has to say by your verbal communication or body language, such as maintaining eye contact, and offer recognitional cues, such as “uh-huh” and “oh, really.” Avoid communication that is at all invalidating. Never start a sentence with “YOU” while having heated conversations with your spouse; instead, use “I feel” statements. This type of communication avoids the blame game that gets many couples into trouble.
Instead, communicate how you feel while not necessarily blaming your spouse but rather expressing your emotions. This will ultimately lead to less defensive communication from your partner. Remember that not all communication is for the sole purpose of communicating. Much of the time, communication is used as an attempt for one partner to connect with the other partner. Couples may say that they have difficulty with communication when it is not the communication that is the issue but instead the underlying disconnect of the couple.
This disconnect usually manifests while couples are communicating, and therefore, can be misconstrued as solely a communication issue by the couple. When your partner asks you to stop staring at your phone during dinner, it is not necessarily that your spouse is attempting to control you or wants to engage in some deep conversation, but more likely a bid to try to connect with you. Your partner is attempting to tell you that he or she feels disconnected, misses you, and wants to reconnect.
Provide validation and acceptance to your partner
Focus on your partner’s strengths and accept the weaknesses. Accept that your partner is scattered, disorganized, and takes at least 20 minutes to find the phone and keys every morning. Remember that during your courtship days, you found your partner’s flighty attributes to be endearing. Do the same for your strengths and weaknesses.
Accept that the pandemic is unpredictable and that you may need to strengthen your ability to be flexible and more adaptable. This will ultimately lead to feeling less disappointment by your partner and more accepting of shortcomings. Acceptance of your imperfections will improve your sense of worth and confidence and lessen negative emotions, such as guilt, regret, and shame.
Accept the fact that, as similar as we all are, we use different methods to recharge ourselves. In contrast, your spouse needs alone time without distractions to reboot mentally and prepare for the following day. In the pre-pandemic world, if there were a mismatch in what a couple needed to feel rejuvenated, they could independently compensate and search for fulfillment outside of the home. Before stay-at-home orders were rolled out throughout the country, spouses had ample opportunities to spend time away from their partners at work, dinner with friends, or while squeezing in a 7 p.m. yoga sculpt class – barely getting home in time to kiss our children goodnight – with a few minutes to spare to engage in mundane conversation with our partners before our nighttime routine of TV commenced. Unfortunately, COVID-19 has made it very hard for couples to carve out that time for compensatory activities outside of the home.
Remember that you are a team
Remind yourself of the reason why you initially fell in love with your partner. Teammates do not keep score or compete with one another. They support each other when one player is not feeling well, and they make sacrifices for the betterment of the team.
Your marriage vows included “through sickness and health” and now should include “through quarantine.”
Dr. Abraham is a psychiatrist in private practice in Philadelphia. She has no disclosures.
High rate of fatty liver disease found among 9/11 first responders
First responders to the site of the 2001 World Trade Center attack may have an elevated risk of nonalcoholic fatty liver disease (NAFLD), according to investigators.
In a retrospective look at 236 first responders presenting with gastrointestinal symptoms to the World Trade Center Health Program, 195 (82.6%) had NAFLD, compared with 24%-45% of the general population, reported lead author Mishal Reja, MD, of Robert Wood Johnson University Hospital, New Brunswick, N.J.
The increased rate of NAFLD among first responders is likely because of toxin exposure at ground zero, which can cause a subtype of NAFLD known as toxin-associated fatty liver disease (TAFLD), Dr. Reja wrote in an abstract released as part of the annual Digestive Disease Week®, which was canceled because of COVID-19.
“I was not surprised [by these findings],” Dr. Reja said during a virtual press conference. “In the prior literature that did examine TAFLD, it did show that populations exposed to these specific chemicals ... at the ground zero site had extremely high rates – consistent with the rates we found in our study – of fatty liver disease.”
Dr. Reja said that 9/11 first responders were exposed to “many common toxins that are consistently in occupational and environmental toxicant literature.” In particular, he named polycyclic aromatic hydrocarbons and vinyl chloride.
“A lot of these toxins are ... included in industrial solvents as well as building demolition,” Dr. Reja said. “So they’ve been around for so long, and they’ve been studied for so long, [that we have] literature that shows these toxins are associated with fatty liver disease, which is how we arrived at the hypothesis in the first place.”
The first responders were stratified by roles, which were associated with varying levels of exposure. About 40% of individuals in the study were involved in moving debris from the site, a small group (4%) were involved in clean-up and maintenance, while approximately 30%-40% worked in more protected, administrative roles.
Comparing individuals in the study with TAFLD versus those without TAFLD revealed additional risk factors. Multivariate logistical regression analysis showed that obese individuals had a significantly increased risk of fatty liver disease, suggesting a synergistic effect.
“If you were exposed to these toxins in the World Trade Center, and you were obese, [then] you are actually between two to three times more likely to get [TAFLD],” Dr. Reja said, noting that hypertension and diabetes were also identified as independent risk factors.
Dr. Reja and colleagues are planning a prospective trial to investigate further. The study will likely involve 100-200 first responders with TAFLD, a similar number of individuals with NAFLD, and another group without liver disease.
The investigators reported no outside funding or conflicts of interest.
SOURCE: Reja M et al. DDW 2020, Abstracts available online May 2.
First responders to the site of the 2001 World Trade Center attack may have an elevated risk of nonalcoholic fatty liver disease (NAFLD), according to investigators.
In a retrospective look at 236 first responders presenting with gastrointestinal symptoms to the World Trade Center Health Program, 195 (82.6%) had NAFLD, compared with 24%-45% of the general population, reported lead author Mishal Reja, MD, of Robert Wood Johnson University Hospital, New Brunswick, N.J.
The increased rate of NAFLD among first responders is likely because of toxin exposure at ground zero, which can cause a subtype of NAFLD known as toxin-associated fatty liver disease (TAFLD), Dr. Reja wrote in an abstract released as part of the annual Digestive Disease Week®, which was canceled because of COVID-19.
“I was not surprised [by these findings],” Dr. Reja said during a virtual press conference. “In the prior literature that did examine TAFLD, it did show that populations exposed to these specific chemicals ... at the ground zero site had extremely high rates – consistent with the rates we found in our study – of fatty liver disease.”
Dr. Reja said that 9/11 first responders were exposed to “many common toxins that are consistently in occupational and environmental toxicant literature.” In particular, he named polycyclic aromatic hydrocarbons and vinyl chloride.
“A lot of these toxins are ... included in industrial solvents as well as building demolition,” Dr. Reja said. “So they’ve been around for so long, and they’ve been studied for so long, [that we have] literature that shows these toxins are associated with fatty liver disease, which is how we arrived at the hypothesis in the first place.”
The first responders were stratified by roles, which were associated with varying levels of exposure. About 40% of individuals in the study were involved in moving debris from the site, a small group (4%) were involved in clean-up and maintenance, while approximately 30%-40% worked in more protected, administrative roles.
Comparing individuals in the study with TAFLD versus those without TAFLD revealed additional risk factors. Multivariate logistical regression analysis showed that obese individuals had a significantly increased risk of fatty liver disease, suggesting a synergistic effect.
“If you were exposed to these toxins in the World Trade Center, and you were obese, [then] you are actually between two to three times more likely to get [TAFLD],” Dr. Reja said, noting that hypertension and diabetes were also identified as independent risk factors.
Dr. Reja and colleagues are planning a prospective trial to investigate further. The study will likely involve 100-200 first responders with TAFLD, a similar number of individuals with NAFLD, and another group without liver disease.
The investigators reported no outside funding or conflicts of interest.
SOURCE: Reja M et al. DDW 2020, Abstracts available online May 2.
First responders to the site of the 2001 World Trade Center attack may have an elevated risk of nonalcoholic fatty liver disease (NAFLD), according to investigators.
In a retrospective look at 236 first responders presenting with gastrointestinal symptoms to the World Trade Center Health Program, 195 (82.6%) had NAFLD, compared with 24%-45% of the general population, reported lead author Mishal Reja, MD, of Robert Wood Johnson University Hospital, New Brunswick, N.J.
The increased rate of NAFLD among first responders is likely because of toxin exposure at ground zero, which can cause a subtype of NAFLD known as toxin-associated fatty liver disease (TAFLD), Dr. Reja wrote in an abstract released as part of the annual Digestive Disease Week®, which was canceled because of COVID-19.
“I was not surprised [by these findings],” Dr. Reja said during a virtual press conference. “In the prior literature that did examine TAFLD, it did show that populations exposed to these specific chemicals ... at the ground zero site had extremely high rates – consistent with the rates we found in our study – of fatty liver disease.”
Dr. Reja said that 9/11 first responders were exposed to “many common toxins that are consistently in occupational and environmental toxicant literature.” In particular, he named polycyclic aromatic hydrocarbons and vinyl chloride.
“A lot of these toxins are ... included in industrial solvents as well as building demolition,” Dr. Reja said. “So they’ve been around for so long, and they’ve been studied for so long, [that we have] literature that shows these toxins are associated with fatty liver disease, which is how we arrived at the hypothesis in the first place.”
The first responders were stratified by roles, which were associated with varying levels of exposure. About 40% of individuals in the study were involved in moving debris from the site, a small group (4%) were involved in clean-up and maintenance, while approximately 30%-40% worked in more protected, administrative roles.
Comparing individuals in the study with TAFLD versus those without TAFLD revealed additional risk factors. Multivariate logistical regression analysis showed that obese individuals had a significantly increased risk of fatty liver disease, suggesting a synergistic effect.
“If you were exposed to these toxins in the World Trade Center, and you were obese, [then] you are actually between two to three times more likely to get [TAFLD],” Dr. Reja said, noting that hypertension and diabetes were also identified as independent risk factors.
Dr. Reja and colleagues are planning a prospective trial to investigate further. The study will likely involve 100-200 first responders with TAFLD, a similar number of individuals with NAFLD, and another group without liver disease.
The investigators reported no outside funding or conflicts of interest.
SOURCE: Reja M et al. DDW 2020, Abstracts available online May 2.
FROM DDW 2020
Key clinical point: First responders to the site of the 2001 World Trade Center attack may have a higher risk of fatty liver disease.
Major finding: Eighty-three percent of first responders presenting with gastrointestinal symptoms had toxin-associated fatty liver disease (TAFLD), a subtype of nonalcoholic fatty liver disease (NAFLD).
Study details: A retrospective study involving 236 first responders presenting with gastrointestinal symptoms to the World Trade Center Health Program between January 2014 and August 2019.
Disclosures: The investigators reported no outside funding or conflicts of interest.
Source: Reja M et al. DDW 2020, Abstracts available online May 2.
Advances in Hematology and Oncology (May 2020)
Click here to access May 2020 Advances in Hematology and Oncology
Table of Contents
- Distress and Factors Associated with Suicidal Ideation in Veterans Living with Cancer
- Incidental Findings of Pulmonary and Hilar Malignancy by Low-Resolution Computed Tomography Used in Perfusion Imaging
- Applying a Text-Search Algorithm to Radiology Reports Can Find More Patients With Pulmonary Nodules Than Radiology Coding Alone
- Radiotherapeutic Care of Patients With Stage IV Lung Cancer and Thoracic Symptoms in the Veterans Health Administration
- Atrial Fibrillation and Bleeding in Chronic Lymphocytic Leukemia Patients Treated with Ibrutinib in the Veterans Health Administration

Click here to access May 2020 Advances in Hematology and Oncology
Table of Contents
- Distress and Factors Associated with Suicidal Ideation in Veterans Living with Cancer
- Incidental Findings of Pulmonary and Hilar Malignancy by Low-Resolution Computed Tomography Used in Perfusion Imaging
- Applying a Text-Search Algorithm to Radiology Reports Can Find More Patients With Pulmonary Nodules Than Radiology Coding Alone
- Radiotherapeutic Care of Patients With Stage IV Lung Cancer and Thoracic Symptoms in the Veterans Health Administration
- Atrial Fibrillation and Bleeding in Chronic Lymphocytic Leukemia Patients Treated with Ibrutinib in the Veterans Health Administration
Click here to access May 2020 Advances in Hematology and Oncology
Table of Contents
- Distress and Factors Associated with Suicidal Ideation in Veterans Living with Cancer
- Incidental Findings of Pulmonary and Hilar Malignancy by Low-Resolution Computed Tomography Used in Perfusion Imaging
- Applying a Text-Search Algorithm to Radiology Reports Can Find More Patients With Pulmonary Nodules Than Radiology Coding Alone
- Radiotherapeutic Care of Patients With Stage IV Lung Cancer and Thoracic Symptoms in the Veterans Health Administration
- Atrial Fibrillation and Bleeding in Chronic Lymphocytic Leukemia Patients Treated with Ibrutinib in the Veterans Health Administration

Testicular Swelling as an Initial Presentation of a Patient With Metastatic Gastric Cancer (FULL)
Gastric cancer is one of the most common cancers and the second most common cause of cancer-related death worldwide.1 Patients with an early-stage gastric cancer are often asymptomatic, and about 30% to 40% of patients present with distant metastases.2 The most common sites of metastasis are the liver, peritoneum, and the lymph nodes. In more advanced stages, gastric cancers spread to the lungs, brain, bones, soft tissues, and other sites. Krukenberg tumors are classic but rare occurrences of gastric cancer metastasis to ovaries in females. In men, it is rare for gastric cancer to metastasize to the testes. Only a few cases of testicular metastasis from gastric cancer have been reported in the literature.3-5
Primary testicular neoplasms typically present with unilateral testicular swelling. In rare instances, testicular swelling can be an initial presentation of a metastatic cancer. In this article, we report a man who initially presented with right testicular swelling and was eventually diagnosed with a secondary testicular cancer from an aggressive metastatic gastric adenocarcinoma.
Case Presentation
A 43-year-old male presented to his primary care physician with a 6-month history of right testicular swelling and unintentional weight loss of 33 pounds. An ultrasound of the scrotum and the testes showed a 4.5-cm hypoechoic and predominantly cystic mass in the right testis. Serum levels of β-human chorionic gonadotropin, α-feto protein and lactate dehydrogenase were within normal limits.
A primary testicular neoplasm was suspected. The patient underwent a right-sided inguinal orchiectomy. The pathology of the resected testis revealed an intestinal type adenocarcinoma with mucinous and signet-ring cell features (Figure). 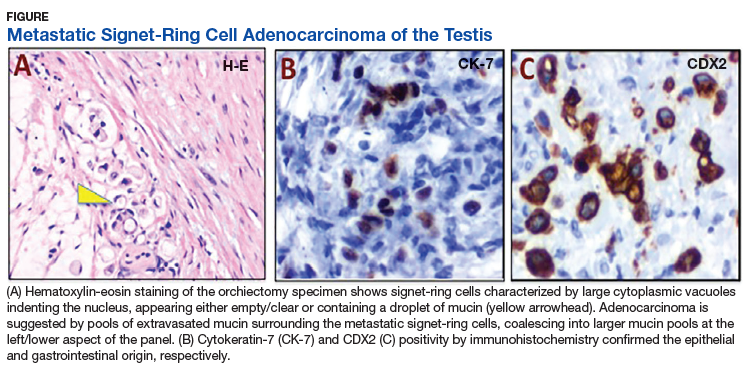
A staging Fluorine-18 fluorodeoxyglucose positron emission tomography scan revealed extensive hypermetabolic peritoneal nodules consistent with peritoneal carcinomatosis. The patient started palliative chemotherapy with 5-fluorouracil and oxaliplatin but rapidly declined with progressive abdominal symptoms after completion of 2 cycles. He discontinued chemotherapy and eventually opted for supportive care focusing on comfort.
Discussion
Testicular neoplasm is the most common solid tumor in men aged 20 to 34 years in the US.6 More than 90% of testicular neoplasms are germ-cell tumors and originate from the testes.6 Secondary neoplasms of the testes from solid tumors are rare. In an autopsy series, secondary neoplasms from solid tumors represented 4.6% of all testicular neoplasms.7 The reported frequencies of primary sites of origin vary based on the report. In a relatively large series, the most common solid tumors of origin were the prostate (35%) and lungs (20%).8 Among hematologic malignancies, lymphomas may originate from or secondarily involve the testes. Primary testicular lymphomas account for approximately 5% of testicular neoplasms and commonly occur in men aged > 60 years.9 Testicular involvement of acute myeloid or lymphoid leukemia may happen at diagnosis, but relapses of acute leukemia in a testicular site are more common and well recognized.10,11
Our report shows a rare occurrence of a testicular swelling as an initial presentation of an aggressive metastatic gastric adenocarcinoma. When a patient presents with a testicular swelling, a testicular neoplasm is suspected based on the clinical examination, serum tumor markers, and ultrasonographic examination of the testes. Inguinal orchiectomy is the initial standard of care, and pathologic examination of a resected testis renders the confirmatory diagnosis. The overwhelming majority of these patients have primary testicular neoplasms, predominantly testicular germ-cell tumors. A small group may have atypical and rare tumors requiring additional workup to establish a diagnosis.
Metastatic spread of a solid tumor to a testicular site is rare. A testis is somewhat protected by the distinct anatomy that is offered by the blood-testis barrier. The tunica vaginalis, an external fibrous covering sheath of the testis, separates the testis from the peritoneal cavity and provides additional protection. Nevertheless, possible routes of secondary metastatic spread may include hematogenous and lymphovascular spread, cavitary dissemination and peritoneal seeding. Among gastric cancers, diffuse gastric cancer subtype is commonly associated with signet-ring cells. These cells lack adhesion and invade as single cells or small groups, leading to scattered tumor cells and a higher probability of seeding.
Our patient exhibited extensive peritoneal carcinomatosis, so peritoneal seeding likely played a dominant role in disseminating the cancer to the testis. It should be noted that possible primary sites of signet-ring cell metastatic adenocarcinomas are broad and may include the stomach and other GI and pancreaticobiliary sites, as well as the lung, bladder, breast, and gynecologic tract. Immunohistochemistry is often of limited value in establishing the primary site. Diagnosis is best established on clinical grounds, as was done in our patient.
When signet-ring cells are encountered in an orchiectomy specimen and a primary extratesticular site of origin cannot be identified, it is important to consider rare variants of primary testicular tumors in the differential diagnosis. A number of primary testicular tumors have signetring morphology. These include primary signetring cell stromal tumor of the testis (PSRST),12 seminoma with signet-ring cell predominance,13 and a primary signet-ring cell germ-cell carcinoma of the testes (PSRGCT).14
Seminoma and PSRST variants generally are differentiated from adenocarcinoma by a lack of mucin production and the absence of keratin expression. PSRGCT is considered a
malignant somatic-type transformation of a testicular germ-cell tumor and germ-cell clonality is established by abnormal 12p chromosome through fluorescent in situ hybridization testing.13 PSRST is a benign tumor with excellent prognosis. Seminoma variants with signet-ring cell predominance and PSRGCT are managed as germ-cell tumors and are also considered to have good outcome. In contrast, testicular involvements from metastatic adenocarcinomas, including gastric cancers, are managed with multidisciplinary approach, including systemic chemotherapy. Despite this, patients have a poor outcome with a median survival of about 1 year.2
Conclusion
Advanced gastric adenocarcinoma can metastasize to the testes, and patients may present with a testicular swelling as an initial presentation. It is important to differentiate secondary testicular cancers from rare variants of primary testicular tumors because the prognosis and management vary substantially.
1. Global Burden of Disease Cancer Collaboration, Fitzmaurice C, Dicker D, et al. The global burden of cancer 2013. JAMA Oncol. 2015;1(4):505-527.
2. Van Cutsem E, Sagaert X, Topal B, Haustermans K, Prenen H. Gastric cancer. Lancet. 2016;388(10060):2654-2664.
3. Qazi HA, Manikandan R, Foster CS, Fordham MV. Testicular metastasis from gastric carcinoma. Urology. 2006;68(4):890.e7-e8.
4. Civelek B, Aksoy S, Kos T, et al. Isolated testicular metastasis of gastric cancer. J Gastrointest Canc. 2012;43(suppl 1):S64-S66.
5. Li B, Cai H, Kang ZC, et al. Testicular metastasis from gastric carcinoma: a case report. World J of Gastroenterol. 2015;21(21):6764-6768.
6. National Cancer Institute Surveillance, Epidemiology, and End Results Program. Cancer stat facts: testicular cancer. https://seer.cancer.gov/statfacts/html/testis.html. Updated September 10, 2018. Accessed April 10, 2019.
7. Dutt N, Bates AW, Baithun SI. Secondary neoplasms of the male genital tract with different patterns of involvement in adults and children. Histopathology. 2000;37(4):323-331.
8. Haupt HM, Mann RB, Trump DL, Abeloff MD. Metastatic carcinoma involving the testis. Clinical and pathologic distinction from primary testicular neoplasms. Cancer.1984;54 (4):709-714.
9. Cheah CY, Wirth A, Seymour JF. Primary testicular lymphoma. Blood. 2014;123(4):486-493.
10. Kawamoto K, Miyoshi H, Yoshida N, Takizawa J, Sone H, Ohshima K. Clinicopathological, cytogenetic, and prognostic analysis of 131 myeloid sarcoma patients. Am J Surg Pathol. 2016;40(11):1473-1483.
11. Kulkarni KP, Marwaha RK, Trehan A, Bansal D. Testicular relapse in childhood acute lymphoblastic leukemia: the challenges and lessons. Indian J Cancer. 2010;47(2):134-138.
12. Kuo CY, Wen MC, Wang J, Jan YJ. Signet-ring stromal tumor of the testis: a case report and literature review. Hum Pathol. 2009;40(4):584-587.
13. Ulbright TM, Young RH. Seminoma with conspicuous signet ring cells: a rare, previously uncharacterized morphologic variant. Am J Surg Pathol. 2008;32(8):1175-1181.
14. Williamson SR, Kum JB, Shah SR, et al. Signet ring cell carcinoma of the testis: clinicopathologic and molecular evidence for germ cell tumor origin—a case report. Am J
Surg Pathol. 2012;36(2):311-315.
Gastric cancer is one of the most common cancers and the second most common cause of cancer-related death worldwide.1 Patients with an early-stage gastric cancer are often asymptomatic, and about 30% to 40% of patients present with distant metastases.2 The most common sites of metastasis are the liver, peritoneum, and the lymph nodes. In more advanced stages, gastric cancers spread to the lungs, brain, bones, soft tissues, and other sites. Krukenberg tumors are classic but rare occurrences of gastric cancer metastasis to ovaries in females. In men, it is rare for gastric cancer to metastasize to the testes. Only a few cases of testicular metastasis from gastric cancer have been reported in the literature.3-5
Primary testicular neoplasms typically present with unilateral testicular swelling. In rare instances, testicular swelling can be an initial presentation of a metastatic cancer. In this article, we report a man who initially presented with right testicular swelling and was eventually diagnosed with a secondary testicular cancer from an aggressive metastatic gastric adenocarcinoma.
Case Presentation
A 43-year-old male presented to his primary care physician with a 6-month history of right testicular swelling and unintentional weight loss of 33 pounds. An ultrasound of the scrotum and the testes showed a 4.5-cm hypoechoic and predominantly cystic mass in the right testis. Serum levels of β-human chorionic gonadotropin, α-feto protein and lactate dehydrogenase were within normal limits.
A primary testicular neoplasm was suspected. The patient underwent a right-sided inguinal orchiectomy. The pathology of the resected testis revealed an intestinal type adenocarcinoma with mucinous and signet-ring cell features (Figure).
A staging Fluorine-18 fluorodeoxyglucose positron emission tomography scan revealed extensive hypermetabolic peritoneal nodules consistent with peritoneal carcinomatosis. The patient started palliative chemotherapy with 5-fluorouracil and oxaliplatin but rapidly declined with progressive abdominal symptoms after completion of 2 cycles. He discontinued chemotherapy and eventually opted for supportive care focusing on comfort.
Discussion
Testicular neoplasm is the most common solid tumor in men aged 20 to 34 years in the US.6 More than 90% of testicular neoplasms are germ-cell tumors and originate from the testes.6 Secondary neoplasms of the testes from solid tumors are rare. In an autopsy series, secondary neoplasms from solid tumors represented 4.6% of all testicular neoplasms.7 The reported frequencies of primary sites of origin vary based on the report. In a relatively large series, the most common solid tumors of origin were the prostate (35%) and lungs (20%).8 Among hematologic malignancies, lymphomas may originate from or secondarily involve the testes. Primary testicular lymphomas account for approximately 5% of testicular neoplasms and commonly occur in men aged > 60 years.9 Testicular involvement of acute myeloid or lymphoid leukemia may happen at diagnosis, but relapses of acute leukemia in a testicular site are more common and well recognized.10,11
Our report shows a rare occurrence of a testicular swelling as an initial presentation of an aggressive metastatic gastric adenocarcinoma. When a patient presents with a testicular swelling, a testicular neoplasm is suspected based on the clinical examination, serum tumor markers, and ultrasonographic examination of the testes. Inguinal orchiectomy is the initial standard of care, and pathologic examination of a resected testis renders the confirmatory diagnosis. The overwhelming majority of these patients have primary testicular neoplasms, predominantly testicular germ-cell tumors. A small group may have atypical and rare tumors requiring additional workup to establish a diagnosis.
Metastatic spread of a solid tumor to a testicular site is rare. A testis is somewhat protected by the distinct anatomy that is offered by the blood-testis barrier. The tunica vaginalis, an external fibrous covering sheath of the testis, separates the testis from the peritoneal cavity and provides additional protection. Nevertheless, possible routes of secondary metastatic spread may include hematogenous and lymphovascular spread, cavitary dissemination and peritoneal seeding. Among gastric cancers, diffuse gastric cancer subtype is commonly associated with signet-ring cells. These cells lack adhesion and invade as single cells or small groups, leading to scattered tumor cells and a higher probability of seeding.
Our patient exhibited extensive peritoneal carcinomatosis, so peritoneal seeding likely played a dominant role in disseminating the cancer to the testis. It should be noted that possible primary sites of signet-ring cell metastatic adenocarcinomas are broad and may include the stomach and other GI and pancreaticobiliary sites, as well as the lung, bladder, breast, and gynecologic tract. Immunohistochemistry is often of limited value in establishing the primary site. Diagnosis is best established on clinical grounds, as was done in our patient.
When signet-ring cells are encountered in an orchiectomy specimen and a primary extratesticular site of origin cannot be identified, it is important to consider rare variants of primary testicular tumors in the differential diagnosis. A number of primary testicular tumors have signetring morphology. These include primary signetring cell stromal tumor of the testis (PSRST),12 seminoma with signet-ring cell predominance,13 and a primary signet-ring cell germ-cell carcinoma of the testes (PSRGCT).14
Seminoma and PSRST variants generally are differentiated from adenocarcinoma by a lack of mucin production and the absence of keratin expression. PSRGCT is considered a
malignant somatic-type transformation of a testicular germ-cell tumor and germ-cell clonality is established by abnormal 12p chromosome through fluorescent in situ hybridization testing.13 PSRST is a benign tumor with excellent prognosis. Seminoma variants with signet-ring cell predominance and PSRGCT are managed as germ-cell tumors and are also considered to have good outcome. In contrast, testicular involvements from metastatic adenocarcinomas, including gastric cancers, are managed with multidisciplinary approach, including systemic chemotherapy. Despite this, patients have a poor outcome with a median survival of about 1 year.2
Conclusion
Advanced gastric adenocarcinoma can metastasize to the testes, and patients may present with a testicular swelling as an initial presentation. It is important to differentiate secondary testicular cancers from rare variants of primary testicular tumors because the prognosis and management vary substantially.
Gastric cancer is one of the most common cancers and the second most common cause of cancer-related death worldwide.1 Patients with an early-stage gastric cancer are often asymptomatic, and about 30% to 40% of patients present with distant metastases.2 The most common sites of metastasis are the liver, peritoneum, and the lymph nodes. In more advanced stages, gastric cancers spread to the lungs, brain, bones, soft tissues, and other sites. Krukenberg tumors are classic but rare occurrences of gastric cancer metastasis to ovaries in females. In men, it is rare for gastric cancer to metastasize to the testes. Only a few cases of testicular metastasis from gastric cancer have been reported in the literature.3-5
Primary testicular neoplasms typically present with unilateral testicular swelling. In rare instances, testicular swelling can be an initial presentation of a metastatic cancer. In this article, we report a man who initially presented with right testicular swelling and was eventually diagnosed with a secondary testicular cancer from an aggressive metastatic gastric adenocarcinoma.
Case Presentation
A 43-year-old male presented to his primary care physician with a 6-month history of right testicular swelling and unintentional weight loss of 33 pounds. An ultrasound of the scrotum and the testes showed a 4.5-cm hypoechoic and predominantly cystic mass in the right testis. Serum levels of β-human chorionic gonadotropin, α-feto protein and lactate dehydrogenase were within normal limits.
A primary testicular neoplasm was suspected. The patient underwent a right-sided inguinal orchiectomy. The pathology of the resected testis revealed an intestinal type adenocarcinoma with mucinous and signet-ring cell features (Figure).
A staging Fluorine-18 fluorodeoxyglucose positron emission tomography scan revealed extensive hypermetabolic peritoneal nodules consistent with peritoneal carcinomatosis. The patient started palliative chemotherapy with 5-fluorouracil and oxaliplatin but rapidly declined with progressive abdominal symptoms after completion of 2 cycles. He discontinued chemotherapy and eventually opted for supportive care focusing on comfort.
Discussion
Testicular neoplasm is the most common solid tumor in men aged 20 to 34 years in the US.6 More than 90% of testicular neoplasms are germ-cell tumors and originate from the testes.6 Secondary neoplasms of the testes from solid tumors are rare. In an autopsy series, secondary neoplasms from solid tumors represented 4.6% of all testicular neoplasms.7 The reported frequencies of primary sites of origin vary based on the report. In a relatively large series, the most common solid tumors of origin were the prostate (35%) and lungs (20%).8 Among hematologic malignancies, lymphomas may originate from or secondarily involve the testes. Primary testicular lymphomas account for approximately 5% of testicular neoplasms and commonly occur in men aged > 60 years.9 Testicular involvement of acute myeloid or lymphoid leukemia may happen at diagnosis, but relapses of acute leukemia in a testicular site are more common and well recognized.10,11
Our report shows a rare occurrence of a testicular swelling as an initial presentation of an aggressive metastatic gastric adenocarcinoma. When a patient presents with a testicular swelling, a testicular neoplasm is suspected based on the clinical examination, serum tumor markers, and ultrasonographic examination of the testes. Inguinal orchiectomy is the initial standard of care, and pathologic examination of a resected testis renders the confirmatory diagnosis. The overwhelming majority of these patients have primary testicular neoplasms, predominantly testicular germ-cell tumors. A small group may have atypical and rare tumors requiring additional workup to establish a diagnosis.
Metastatic spread of a solid tumor to a testicular site is rare. A testis is somewhat protected by the distinct anatomy that is offered by the blood-testis barrier. The tunica vaginalis, an external fibrous covering sheath of the testis, separates the testis from the peritoneal cavity and provides additional protection. Nevertheless, possible routes of secondary metastatic spread may include hematogenous and lymphovascular spread, cavitary dissemination and peritoneal seeding. Among gastric cancers, diffuse gastric cancer subtype is commonly associated with signet-ring cells. These cells lack adhesion and invade as single cells or small groups, leading to scattered tumor cells and a higher probability of seeding.
Our patient exhibited extensive peritoneal carcinomatosis, so peritoneal seeding likely played a dominant role in disseminating the cancer to the testis. It should be noted that possible primary sites of signet-ring cell metastatic adenocarcinomas are broad and may include the stomach and other GI and pancreaticobiliary sites, as well as the lung, bladder, breast, and gynecologic tract. Immunohistochemistry is often of limited value in establishing the primary site. Diagnosis is best established on clinical grounds, as was done in our patient.
When signet-ring cells are encountered in an orchiectomy specimen and a primary extratesticular site of origin cannot be identified, it is important to consider rare variants of primary testicular tumors in the differential diagnosis. A number of primary testicular tumors have signetring morphology. These include primary signetring cell stromal tumor of the testis (PSRST),12 seminoma with signet-ring cell predominance,13 and a primary signet-ring cell germ-cell carcinoma of the testes (PSRGCT).14
Seminoma and PSRST variants generally are differentiated from adenocarcinoma by a lack of mucin production and the absence of keratin expression. PSRGCT is considered a
malignant somatic-type transformation of a testicular germ-cell tumor and germ-cell clonality is established by abnormal 12p chromosome through fluorescent in situ hybridization testing.13 PSRST is a benign tumor with excellent prognosis. Seminoma variants with signet-ring cell predominance and PSRGCT are managed as germ-cell tumors and are also considered to have good outcome. In contrast, testicular involvements from metastatic adenocarcinomas, including gastric cancers, are managed with multidisciplinary approach, including systemic chemotherapy. Despite this, patients have a poor outcome with a median survival of about 1 year.2
Conclusion
Advanced gastric adenocarcinoma can metastasize to the testes, and patients may present with a testicular swelling as an initial presentation. It is important to differentiate secondary testicular cancers from rare variants of primary testicular tumors because the prognosis and management vary substantially.
1. Global Burden of Disease Cancer Collaboration, Fitzmaurice C, Dicker D, et al. The global burden of cancer 2013. JAMA Oncol. 2015;1(4):505-527.
2. Van Cutsem E, Sagaert X, Topal B, Haustermans K, Prenen H. Gastric cancer. Lancet. 2016;388(10060):2654-2664.
3. Qazi HA, Manikandan R, Foster CS, Fordham MV. Testicular metastasis from gastric carcinoma. Urology. 2006;68(4):890.e7-e8.
4. Civelek B, Aksoy S, Kos T, et al. Isolated testicular metastasis of gastric cancer. J Gastrointest Canc. 2012;43(suppl 1):S64-S66.
5. Li B, Cai H, Kang ZC, et al. Testicular metastasis from gastric carcinoma: a case report. World J of Gastroenterol. 2015;21(21):6764-6768.
6. National Cancer Institute Surveillance, Epidemiology, and End Results Program. Cancer stat facts: testicular cancer. https://seer.cancer.gov/statfacts/html/testis.html. Updated September 10, 2018. Accessed April 10, 2019.
7. Dutt N, Bates AW, Baithun SI. Secondary neoplasms of the male genital tract with different patterns of involvement in adults and children. Histopathology. 2000;37(4):323-331.
8. Haupt HM, Mann RB, Trump DL, Abeloff MD. Metastatic carcinoma involving the testis. Clinical and pathologic distinction from primary testicular neoplasms. Cancer.1984;54 (4):709-714.
9. Cheah CY, Wirth A, Seymour JF. Primary testicular lymphoma. Blood. 2014;123(4):486-493.
10. Kawamoto K, Miyoshi H, Yoshida N, Takizawa J, Sone H, Ohshima K. Clinicopathological, cytogenetic, and prognostic analysis of 131 myeloid sarcoma patients. Am J Surg Pathol. 2016;40(11):1473-1483.
11. Kulkarni KP, Marwaha RK, Trehan A, Bansal D. Testicular relapse in childhood acute lymphoblastic leukemia: the challenges and lessons. Indian J Cancer. 2010;47(2):134-138.
12. Kuo CY, Wen MC, Wang J, Jan YJ. Signet-ring stromal tumor of the testis: a case report and literature review. Hum Pathol. 2009;40(4):584-587.
13. Ulbright TM, Young RH. Seminoma with conspicuous signet ring cells: a rare, previously uncharacterized morphologic variant. Am J Surg Pathol. 2008;32(8):1175-1181.
14. Williamson SR, Kum JB, Shah SR, et al. Signet ring cell carcinoma of the testis: clinicopathologic and molecular evidence for germ cell tumor origin—a case report. Am J
Surg Pathol. 2012;36(2):311-315.
1. Global Burden of Disease Cancer Collaboration, Fitzmaurice C, Dicker D, et al. The global burden of cancer 2013. JAMA Oncol. 2015;1(4):505-527.
2. Van Cutsem E, Sagaert X, Topal B, Haustermans K, Prenen H. Gastric cancer. Lancet. 2016;388(10060):2654-2664.
3. Qazi HA, Manikandan R, Foster CS, Fordham MV. Testicular metastasis from gastric carcinoma. Urology. 2006;68(4):890.e7-e8.
4. Civelek B, Aksoy S, Kos T, et al. Isolated testicular metastasis of gastric cancer. J Gastrointest Canc. 2012;43(suppl 1):S64-S66.
5. Li B, Cai H, Kang ZC, et al. Testicular metastasis from gastric carcinoma: a case report. World J of Gastroenterol. 2015;21(21):6764-6768.
6. National Cancer Institute Surveillance, Epidemiology, and End Results Program. Cancer stat facts: testicular cancer. https://seer.cancer.gov/statfacts/html/testis.html. Updated September 10, 2018. Accessed April 10, 2019.
7. Dutt N, Bates AW, Baithun SI. Secondary neoplasms of the male genital tract with different patterns of involvement in adults and children. Histopathology. 2000;37(4):323-331.
8. Haupt HM, Mann RB, Trump DL, Abeloff MD. Metastatic carcinoma involving the testis. Clinical and pathologic distinction from primary testicular neoplasms. Cancer.1984;54 (4):709-714.
9. Cheah CY, Wirth A, Seymour JF. Primary testicular lymphoma. Blood. 2014;123(4):486-493.
10. Kawamoto K, Miyoshi H, Yoshida N, Takizawa J, Sone H, Ohshima K. Clinicopathological, cytogenetic, and prognostic analysis of 131 myeloid sarcoma patients. Am J Surg Pathol. 2016;40(11):1473-1483.
11. Kulkarni KP, Marwaha RK, Trehan A, Bansal D. Testicular relapse in childhood acute lymphoblastic leukemia: the challenges and lessons. Indian J Cancer. 2010;47(2):134-138.
12. Kuo CY, Wen MC, Wang J, Jan YJ. Signet-ring stromal tumor of the testis: a case report and literature review. Hum Pathol. 2009;40(4):584-587.
13. Ulbright TM, Young RH. Seminoma with conspicuous signet ring cells: a rare, previously uncharacterized morphologic variant. Am J Surg Pathol. 2008;32(8):1175-1181.
14. Williamson SR, Kum JB, Shah SR, et al. Signet ring cell carcinoma of the testis: clinicopathologic and molecular evidence for germ cell tumor origin—a case report. Am J
Surg Pathol. 2012;36(2):311-315.
The Diagnosis and Management of Cutaneous T-Cell Lymphomas (FULL)
John Zic, MD. Let’s start by defining cutaneous T-cell lymphomas (CTCLs) and how they differ from other non-Hodgkin lymphomas. We also should discuss classification, which can be very confusing and epidemiology as it relates to the veteran population. Then I think we should dive into challenges with diagnosis and when should a VA or any provider consider mycosis fungoides (MF) and Sézary syndrome—the 2 most common variants of CTCLs.
I like to define the primary CTCLs as malignancies of the T-cell where the primary organ of involvement is the skin. However, this disease can spread to lymph nodes and visceral organs and the blood compartment in more advanced patients. Alejandro, could you provide some highlights about how CTCLs are classified?
Alejandro Ariel Gru, MD. Lymphomas are divided in the general hematology/oncology practice as Hodgkin and non-Hodgkin lymphomas. Traditionally all lymphomas that occur on the skin are non-Hodgkin lymphoma subtypes. That has specific connotations in terms of diagnosis, prognosis, and therapy. Because the T cells are one of the main residents of the subtypes of lymphocytes you encounter on the skin, most lymphomas that occur on the skin are derived of T-cell origin. B-cell lymphomas, in general, tend to be relatively uncommon or more infrequent.
There are 3 main subtypes of CTCL that present on the skin.1 MF is, by far, the most common subtype of CTCL. The disease tends to present in patients who are usually aged > 60 years and is more frequent in white males. It’s a lymphoma that is particularly relevant to the veteran population. The second subtype has many similarities to MF but shows substantial peripheral blood involvement and is referred to as Sézary syndrome. The third group is encompassed under the term CD30-positive lymphoproliferative disorders. This group includes 2 main subtypes: primary cutaneous anaplastic large-cell lymphoma and lymphomatoid papulosis. Some cases of MF develop progression to what we call large cell transformation, which implies cytologic transformation to a more aggressive lymphoma.
There are other cutaneous lymphomas that are far less common. Some are indolent and others can be more aggressive, but they represent < 5% of all CTCL subtypes.
Lauren Pinter-Brown, MD. That was a great summary about these non-Hodgkin lymphomas. In the veteran population, it’s wise to remember that there are many kinds of non-Hodgkin lymphomas. Because of the action that they have seen, some people, such as Vietnam veterans, might be more susceptible to non-Hodgkin lymphomas than others.
John Zic. That’s a good point because certainly non-Hodgkin lymphomas are listed as one of the potential disease associations with exposure to Agent Orange.
I’d like to move on to epidemiology and the incidence of MF and Sézary syndrome. An article that came out of Emory University in 2013 is one of the more up-to-date articles to examine the incidence and survival patterns of CTCL.2 The authors looked at patients from 2005 to 2008 and identified 2,273 patients in the Surveillance, Epidemiology, and End Results registry. They estimated that the incidence of MF in the US population is about 5.5 per 1,000,000 per year, which certainly makes it a rare disease. The incidence of Sézary syndrome was 0.1 per 1,000,000 per year, which comes out to about 1 per 10 million per year.
However, the MF incidence needs to be contrasted to the estimated incidence in the veteran population. In 2016, Larisa Geskin and colleagues from Columbia University and the Bronx US Department of Veterans Affairs (VA) Medical Center examined the VA database of patients with diagnoses of MF and Sézary syndrome.3 They combined them, but I have a feeling that the amount of Sézary syndrome patients was much less than those with MF. They estimated an incidence per million of 62 to 79 cases per 1,000,000 per year. The conclusion of Dr. Geskin’s study stated that the incidence of CTCL in the veteran population appears to be anywhere from 6 to 8 times higher. But if we use the most recent US incidence rates, it’s more than 10 times higher.
Those of you who have worked with veterans, either at the VA or in your private practice, do you have any ideas about why that might be?
Lauren Pinter-Brown. As you previously discussed, this is an illness of older people, and Vietnam veterans now are in their 60s and 70s. They may account for a lot of these diagnoses.
John Zic. That’s a good point. There’s quite a bit of talk about exposure to Agent Orange. But honestly, we really don’t know the cause of any of the CTCLs. We have not been able to identify a single cause. There are some risk factors. A 2014 article from the Journal of the National Cancer Institute looked at 324 cases of CTCL and compared it with 17,000 controls.4 They showed some interesting risk factors, such as body mass index (BMI) > 30 and smoking > 40 years. Similar to previous European studies, they showed that occupations like being a farmer, a painter, a woodworker, or a carpenter may carry additional risk.I wonder whether or not veterans were more likely to have some of these risk factors that this epidemiologic study picked up in addition to exposures that they may have encountered during their active-duty service. Interestingly, a decreased risk factor for developing MF was moderate physical activity. Clearly though, there are a large number of patients with CTCL in the veteran population.
I’d like to turn now to some of the challenges with diagnosis. Marianne, could you share some of your experience with early-stage disease and about how long it took them to be diagnosed?
Marianne Tawa, RN, MSN, ANP. Speaking specifically about early-stage disease, patients often share a history of waxing and waning rash that may not be particularly itchy. Confounding the picture, the distribution of early patch or plaque stage CTCL rash frequently occurs in covered areas. Many patients miss out on complete skin examinations by providers, thus early-stage CTCL may not be appreciated in a timely manner.
In certain scenarios, it may take upward of 5 to 7 years before the CTCL diagnosis is rendered. This is not because the patient delayed care. Nor is it because a skin biopsy was not performed. The progression of the disease and meeting the classic features of histology under the microscope can require clinical observation over time and repeated skin biopsies. We recommend patients refrain from topical steroid applications for 2 to 4 weeks prior to skin biopsy if we have a strong suspicion of CTCL. Many patients will report having a chronic eczematous process. Some patients may have a history of parapsoriasis, and they’re on the continuum for CTCL. That’s a common story for CTCL patients.
John Zic. What is the role of a skin biopsy in the diagnosis of CTCL? We see many patients who have had multiple skin biopsies who often wonder whether or not the diagnosis was missed by either the clinician or the pathologist.
Alejandro Ariel Gru. That is a great area of challenge in terms of pathologic diagnosis of early MF. A study led by Julia Scarisbrick, from an international registry data (PROCLIPI) on the early stages of the disease, showed a median delay of diagnosis of early MF of approximately 36 months.5 For all physicians involved in the diagnosis and care of patients with MF, the delay is probably significantly higher than that. We’ve seen patients who have lived without a diagnosis for a period of 10 or sometimes 15 years. That suggests that many cases are behaving in an indolent fashion, and patients are not progressing through the ‘natural’ stages of the disease and remain at the early stage. There also is the potential that other chronic inflammatory conditions, particularly psoriasis or parapsoriasis, can be confused with this entity. The diagnosis of certain types of parapsoriasis, can belong to the same spectrum of MF and can be treated in a similar way than patients with early stage MF are, such as phototherapy or methotrexate.
The diagnosis of MF relies on a combination of clinical, pathologic, and immunophenotypic findings where it is desired or preferred that at least 2 biopsies are done from different sides of the body. In addition to having a good clinical history that supports the diagnosis, a history of patches, plaques, and sometimes tumors in advanced stages in particular locations that are covered from the light (eg, trunk, buttocks, upper thighs, etc) combined with specific histopathologic criteria are capital to establish an accurate diagnosis.
In the biopsies, we look particularly for a lymphoid infiltrate that shows extension to the epidermis. We use the term epidermotropism to imply that these abnormal or neoplastic lymphocytes extend into the epidermis. They are also cytologically atypical. We see variations in the nucleus. In the size, we see a different character of the chromatin where they can be hyperchromatic. We also look for immunophenotypic aberrations, and particularly we analyze for patterns of expression of T-cell markers. Most cases of MF belong to a subset of T cells that are called CD4-positive or T-helper cells. We look for a patterned ratio of the CD4 and CD8 between the epidermis and an aberrant loss of the CD7 T-cell marker. Once we establish that we can see significant loss of these markers, we can tell where there is something wrong with that T-cell population, and likely belong to a neoplastic category.
In addition, we also rely on the molecular evaluation and search of a clonal population of T cells, by means of a T-cell receptor gene rearrangement study. Ideally, we like to see the establishment of a single clone of T cells that is matched in different biopsy sites. Proving that the same clone is present in 2 separate biopsies in 2 separate sites is the gold standard for diagnosis.6
John Zic. To recap, a biopsy is indicated for patients who have patches or plaques (that are slightly raised above the skin) in sun-protected areas that are fixed; rather than completely go away in the summer and come back in the winter, they are fixed if they have been present > 6 to 12 months. Many of these patients are diagnosed with eczema, psoriasis, allergic contact dermatitis, and other skin diseases before the clinician starts to think about other diagnoses, such as CTCL.
I agree that I would not rule out the diagnosis with 1 biopsy that does not show classic histologic changes. Also, I think that it’s important to alert the pathologist that you’re considering a diagnosis of T-cell lymphoma, either MF or some of the other subtypes, because that will certainly alert them to look a little closer at the infiltrating cells and perhaps do some of the other testing that was mentioned. Once we establish the MF diagnosis, staging studies may be indicated.
Lauren Pinter-Brown. Early stage would be patients with patches or plaques. Stage IA would be < 10% body surface area, and stage IB would be > 10%. I don’t perform scans for early-stage patients, but I do a very thorough physical and perform blood tests. For patients that have more advanced disease, such as tumors, erythroderma, or Sézary syndrome, I would conduct the same thorough examination and blood tests and scan the patient either with a computed tomography (CT) or a positron emission tomography (PET)/CT to detect adenopathy. We have to recognize that most of the adenopathy that is detected in these patients is peripheral, and we can feel it on physical examination.
John Zic. Do you prefer one imaging modality over the other? CT scan with IV contrast vs PET/CT?
Lauren Pinter-Brown. I tend to use PET/CT because it illuminates extranodal sites as well. I have to admit that sometimes it’s a problem to get that approved with insurance.
John Zic. In the federal system, many PET/CT scans are performed at other facilities. That would be an extra step in getting approval.
You mentioned Sézary syndrome. We should consider a diagnosis of Sézary syndrome when you have a patient with erythroderma, which means that they have > 80% of the skin covered in redness and scaling.
Lauren Pinter-Brown. The first step is to do a complete blood count (CBC) and see if there’s a lymphocytosis. Sometimes that really isn’t very sensitive, so my go-to test is flow cytometry. We are looking for an abnormal population of cells that, unlike normal T cells, often lack certain T-cell antigens. The most common would be CD7. We can confirm that this is a clone by T-cell gene rearrangement, and often in Sézary we like to compare the gene rearrangement seen in blood with what might be seen in the skin biopsy to confirm that they’re the same clone.
John Zic. That’s an excellent point. I know there are specific criteria to meet significant blood involvement. That is a topic of conversation among CTCL experts and something that might be changing over the next few years. But I think as it stands right now, having a lymphocytosis or at least an elevated CD4 count along with having a clone in the blood matching the clone in the skin are the first 2 steps in assessing blood involvement. However, the flow cytometry is very important. Not all medical centers are going to do flow cytometry—looking specifically for a drop of the CD7 or CD26 antigen among the CD4 population. But that is one of the major criteria that we look for in those patients with suspected blood involvement.
Marianne Tawa. Additionally, we would advise obtaining flow cytometry on patients that look like they have a robust skin burden with lots of patches, plaques, or tumors. We also perform lactate dehydrogenase (LDH) with staging.
John Zic. What do you usually tell patients with early-stage disease, those that have patches and plaques?
Marianne Tawa. For patients with stage IA disease, we are very optimistic about their prospects. We explain that the likelihood that early-stage disease will progress to a more advanced stage or rare variant is unlikely. This is very much a chronic disease, and the goal is to manage appropriately, palliate symptoms, and preserve quality of life (QOL).
Lauren Pinter-Brown. I often refer to a landmark paper by Youn H. Kim and colleagues that shows us that patients with IA disease who are at least treated usually have a normal lifespan.7 I encourage patients by sharing that data with them.
John Zic. Sean Whittaker and colleagues in the United Kingdom identified 5 risk factors for early-stage patients that may put them at higher risk for progressing: aged > 60 years; having a variant called folliculotropic MF; having palpable lymph nodes even if they’re reactive on biopsy, having plaques, and male sex.8 For staging of lymph nodes, what’s your usual approach when you see a patient with palpable lymph nodes?
Lauren Pinter-Brown. Many patients, particularly those with advanced skin disease, may have palpable lymph nodes that are reacting to their skin disease and on pathology would be dermatopathic. That would not change my management. I pay attention to the quality of the lymph node—if it’s very firm, if it’s > 2 cm, if it is persistent—before I biopsy. These patients have a higher incidence of wound infection after excisional biopsy. If the patient has pathologic lymph node involvement and effacement of the node with malignant cells, I would change my management. I do need to know that sort of information.
John Zic. Alejandro, as a hematopathologist can you comment on the debate about whether or not we actually do need an excisional biopsy or whether or not we can get a core lymph node biopsy to give you all the information that you need to grade it?
Alejandro Ariel Gru. There are 2 main modalities of biopsies we typically see for lymph nodes for evaluation and staging for involvement of CTCL. One is the traditional excisional biopsy that for the most part requires surgery with general anesthesia and has all the major implications that that type of procedure has. Many centers are looking at less invasive types of procedures, and needle core biopsies have become one of the most common forms of biopsy for all lymphoma subtypes. Excisional biopsies have the advantage of being able to see the whole lymph node, so you can determine and evaluate the architecture very well. Whereas needle core biopsies typically use a small needle to obtain a small piece of the tissue.
The likelihood of a successful diagnosis and accurate staging was compared recently in the British Journal of Dermatology.9 They were able to perform accurate staging in needle core biopsies of patients with MF. However, this is still a matter of debate; many people feel they are more likely to get enough information from an excisional biopsy. As we know, excisional biopsies sometimes can be hard, particularly if the large lymph node is located in an area that is difficult to access, for example, a retroperitoneal lymph node.
There are many staging categories that are used in the pathologic evaluation of lymph node involvement. On one hand, we could see the so-called dermatopathic changes, which is a reactive form of lymphadenopathy that typically happens in patients who have skin rashes and where there is no evidence of direct involvement by the disease (although there are some patients who can have T-cell clones by molecular methods). The patients who have clonal T cells perhaps might not do as well as the ones who do not. On the other hand, we have patients for whom the whole architecture of the lymph node is effaced or replaced by neoplastic malignant cells. Those patients are probably going to need more aggressive forms of therapy.10
John Zic. The type of lymph node biopsy has been a hot topic. If patients have palpable lymph nodes in the cervical, axillary, and inguinal area, I don’t know if it’s a consensus, but the recommendation right now is to consider performing a lymph node biopsy of the cervical lymph nodes first, axillary second, and inguinal lymph nodes third. That might have to do with the complication rates for those different areas.
I’d like to switch to a discussion to more advanced disease. CTCL tumors are defined as a dome-shaped nodule > 1 cm. They don’t have to be very big before we label it a tumor, and the disease is considered more advanced. For patients with a few tumors, what does your prognosis discussion sound like?
Marianne Tawa. Certainly, the prognosis discussion can become slightly more complicated when you move into the realm of tumor-stage development. This is especially true if a CTCL patient has lived with and managed indolent patches or plaques for several years. We approach these patients with optimism and with the goal of managing their tumors, whether it be with a skin-directed option, such as localized radiation or a host of approved systemic therapies. Patients presenting with or developing tumor-stage disease over time will require additional staging workup compared with early-stage disease staging practice. Patients are counseled on imaging use in tumor-stage disease and why flow cytometry may be requested to rule in or rule out accompanying peripheral blood involvement. Patients are exposed to a myriad of pictures, stories, and survival statistics from Internet research. It becomes our task to inform them of their unique presentation and tailored treatment plan, which thankfully may produce more favorable responses than those presented online.
Lauren Pinter-Brown. One thing that we focus on is the idea that a statistic regarding prognosis isn’t predictive for an individual patient. When patients go online, we caution them that many of the statistics are really old. There’s been a lot of new therapies in the past 10 years. Just looking at my patients, my feeling is that their prognosis has continued to improve over the decades that I’ve been involved in this area.
We have to take the statistics with a grain of salt, though certainly someone that has Sézary syndrome or someone that has nodal involvement or tumors is not going to fare as well as the patients that we talked about with stage I disease. However, if we all continue to do our jobs and have more and more treatment options for patients, that’s certainly going to change over time as it has with other non-Hodgkin lymphomas.
John Zic. We’ve all treated advanced patients with disease and some, of course, have died of the disease. When patients die of advanced CTCL, what are the things that lead to their demise?
Lauren Pinter-Brown. Probably the most common would be infections because their skin barrier has been broken. As the disease advances, their immune system also deteriorates. We may contribute to that sometimes with some of the therapies that we use, although we try and be judicious. First and foremost, the primary cause of death remains infection and sometimes inanition.
Marianne Tawa. I agree, infection or just the unfortunate progression of their lymphoma through the various armamentarium of treatments would be the 2 reasons.
John Zic. Let’s dive into therapy. I want to start with early stage. While, I don’t think there’s a role for systemic anticancer agents, certainly the IV agents for most patients with early-stage disease Marianne, you mentioned phototherapy. What are the types of phototherapy that you offer?
Marianne Tawa. We would start out with narrow band UVB therapy for patients with > 10% body surface area involvement. When applying topical corticosteroids to wider surface areas of the patient’s body is no longer feasible or effective, we recommend the initiation of narrow band UVB phototherapy. This is preferred because of its lessor adverse effect (AE) profile as far as nonmelanoma skin cancer risk. Patients commence narrow band UVB 3 times per week, with a goal of getting the patient into remission over a matter of months and then slowly tapering the phototherapy so that they get to a maintenance of once weekly.
Realizing that narrow band UVB may not penetrate deeper plaques or effectively reach folliculotropic variant of CTCL, we would employ PUVA, (psoralen and UVA). Patients are expected to protect their eyes with UVA glasses and remain out of the sun 24 hours following PUVA treatments. The cost of the methoxsalen can be an issue for some patients. Nonmelanoma skin cancer risks are increased in patients undergoing long-term PUVA treatments. Routine skin cancer surveillance is key.
There are monetary, time, and travel demands for patients receiving phototherapy. Thus, many CTCL patients are moving toward home-based narrow band UVB units supervised by their treating dermatologist. Other skin-directed treatment options, aside from topical corticosteroids and phototherapy, would include topical nitrogen mustard, imiquimod, and localized or total skin electron beam radiation.
John Zic. Here in Nashville, some of our veterans travel hundreds of miles to get to our center. It’s not practical for them to come here for the narrow band UVB phototherapy. Veterans can get approval through the VA Choice programs to have phototherapy performed by a local dermatologist closer to home. We also have had many veterans who choose to get home narrow band UVB phototherapy, which can be quite effective. Narrow band UVB phototherapy is among the most effective therapies for patients with generalized patches in particular, and maybe some with just a few plaques.
Medium potency topical steroids are not as helpful as superpotent topical steroids such as clobetasol, dipropionate ointment, or betamethasone dipropionate ointment. Usually, I tell patients to apply it twice a day for 8 weeks. You must be careful because these high-potency topical steroids can cause thinning of the skin, but it’s rarely seen, even in patients that may use them for 8 weeks if they’re applying them just to their patches and thin plaques. There are a few other topicals. There’s bexarotene gel, which is a topical retinoid, and mechlorethamine or nitrogen mustard gel that are available as topicals. Both of those can be helpful if patients have < 10% body surface area of patches or plaques because they can apply that at home.
Because of the excellent prognosis for patients in early stages, this is an area we want to try to avoid doing harm. For patients with advanced disease, what are some of the decisions that you think about in recommending a patient to get radiation therapy?
Lauren Pinter-Brown. I use radiation therapy sparingly and primarily for patients who either have only 1 tumor and the rest of their disease is patch and plaque or for patients who have very large tumors that are either cosmetically unacceptable or creating infection or pain. I treat people with systemic therapies primarily to prevent the formation of tumors.
John Zic. There probably is a role for total skin electron beam radiotherapy in patients who have failed multiple other skin-directed therapies and are progressing and then perhaps a role for more advanced patients who have multiple tumors where you’re trying to get some control of the disease. Are there any other situations where you might consider total skin electron beam?
Marianne Tawa. Yes, those are 2 scenarios. A third scenario would be in patients preparing for stem cell transplant. We typically do a modified 12 Gy regimen of total skin electron beam for palliation and up to 24 Gy regimen for patients who are in earnest preparing for a stem cell transplant.
John Zic. Systemic therapies also treat this disease. There are 2 oral agents. One is bexarotene capsules, a retinoid that binds to the RXR receptor and has a multitude of effects on different organ systems. It is probably the best tolerated oral agent we have. The other FDA-approved agent is vorinostat, a histone deacetylase inhibitor, but it has more gastrointestinal AEs than does bexarotene. Bexarotene has AEs as well, including hypertriglyceridemia and central hypothyroidism, which can throw a curveball to unsuspecting primary care physicians who might check thyroid function studies in these patients.
We certainly need to know about those AEs. There are many patients who have tumor-stage disease that can have radiotherapy to several tumors, then go on a drug like bexarotene capsules and may be able to maintain the remission for years. In my experience, it’s a drug that patients usually stay on. They can be weaned to a very low dose, but I’ve had several patients who come off of bexarotene only to suffer relapses.
Lauren, what are some of the things that you think about when you declare someone as having failed bexarotene or vorinostat and you’re thinking about IV therapies?
Lauren Pinter-Brown. Patient comorbidities and the particular compartment of their body that is involved are important factors. Do they have blood involvement, or not? Do they have nodal involvement, or not? Another concern is both acute and chronic toxicities that need to be discussed with the patient to determine an acceptable QOL. Finally, the schedule that you’re giving the drug. Some people may not be able to come in frequently. There are a lot of variables that go into making an individual decision at a particular time for a specific patient who will be using parenteral therapies.
John Zic. If we have a patient with advanced MF, tumors, and perhaps lymph node involvement, what are some of the systemic options that you would consider?
Lauren Pinter-Brown. With nodal involvement, an attractive option is something like IV romidepsin because we know that it treats peripheral T-cell lymphomas, which are aggressive nodal T-cell lymphomas. It’s FDA approved and also treats CTCL. Another is brentuximab vedotin if there is significant CD30 expression. It also is FDA approved for CTCL and has a long track record of treating certain peripheral T-cell lymphomas like anaplastic large cell.
John Zic. When would the stem cell transplant discussion start at your institution?
Lauren Pinter-Brown. It starts earlier for a younger patient because even though we do have lots of treatment if someone is aged 20 or30 years, I don’t really have any illusions that I have enough treatment options for them to live a normal lifespan if they have advanced disease. It’s a possibility for any patient when I see that the future options are dwindling, and that I am not going to be able to control the patient’s disease for much longer. Having said that, patients who have tumor-stage disease are among those that don’t do quite as well with allogeneic transplantation; ironically, patients with Sézary syndrome or erythroderma might do a little bit better.
John Zic. Before considering a stem cell transplant for patients with Sézary syndrome, that is erythroderma with significant blood involvement, what other treatment options would you offer?
Marianne Tawa. For low blood-burden disease, we might look at extracorporeal photopheresis as monotherapy or in combination with interferon or bexarotene. For patients with higher blood burden we might recommend low-dose alemtuzumab, especially if they have abundant CD52 expression. We also consider the newly FDA-approved anti-CCR4 antibody treatment, mogamulizumab, for patients presenting with Sézary syndrome. It is generally well tolerated but does have the potential for producing infusion reactions or drug rash.
Romidepsin has efficacy in blood, lymph node, and skin compartments. The primary considerations for patients considering romidepsin are prolonged infusion times and QOL AEs with gastrointestinal and taste disturbances and fatigue.
John Zic. Both of you have brought up an excellent point. This is a disease that while we do not have a good chance of curing, we have a pretty fair chance of controlling, especially if it’s early stage. The data from the stem cell transplant literature indicate that stem cell transplant may be one of the few modalities that we have that may offer a cure.11
Lauren Pinter-Brown. There are patients who are cured with allogeneic transplants; and the very first allogeneic transplants were performed well over 20 years ago. Many patients, even some in my practice, who were among those patients and continue to do extremely well without any evidence of disease. Sometimes when people have allogeneic transplantation, their disease relapse may be in a more indolent form that’s much easier to deal with than their original disease. Even if they’re not cured, the fact that the aggressive disease seems to be at bay may make them much easier to treat.
John Zic. Those are excellent points. You brought up photopheresis as a treatment modality for patients with evolving or early Sézary syndrome and patients with erythrodermic MF can also respond. We have a lot of experience with that at the Nashville VA medical center. We’re one of the few VA hospitals in the US that has a photopheresis unit. But the modality is available at many academic medical centers because it’s a treatment for graft-vs-host disease.
We tend to also consider photopheresis in patients who may have had an excellent response to another systemic agent. There are some data that patients who received photopheresis, after total skin electron beam therapy vs those who received chemotherapy after radiation, had a longer disease-free survival.12
I’d like to end with a discussion of something that’s very important, which is managing QOL issues for patients with CTCL. Itch is among some of the worst symptoms that can cause suffering in patients. But it is sometimes not a problem at all for patients who have a few patches or plaques. That’s one reason why they might ignore their rash. Certainly, as the disease progresses, especially those patients with erythroderma, the itch can be intractable and can have a major impact on their life. What are some approaches to managing itch at your institutions?
Lauren Pinter-Brown. One thing to be aware of is that the itch is not usually mediated by histamine, though people will often put the patients on a lot of antihistamines. I don’t find those to be the most effective treatments. I think of the itch in these patients as more of a neuropathic condition and would tend to treat more with things that you might use for neuropathy, such as gabapentin or doxepin or antidepressants. There’s a whole host of other treatments, such as aprepitant, something that I would use as an antiemetic, that might also be helpful for pruritus in this patient population.
John Zic. That’s my experience as well. I have found gabapentin to be helpful for patients with itch, though not universally.
Marianne Tawa. I consider itch a huge QOL concern for a large majority of our patients with a CTCL diagnosis. It’s on par with pain. In early-stage disease, pruritus levels improve as the cutaneous burden is reduced with skin-directed therapies such as, topical corticosteroid or phototherapy.
SSRI agents could also be considered for select patients. The antiemetic agent, aprepitant has been useful for addressing itch in a subset of our patients with Sézary syndrome. Patients will also seek out complementary modalities such acupuncture, hypnosis, and guided imagery.
John Zic. Because the disease itself affects the skin and can lead to dryness, patients often suffer with dry skin. When I trained in Chicago, that was the foundation of our treatment, making sure that patients are using a super fatted soap such as Dove (Unilever, London, United Kingdom) or Cetaphil (Galderma Laboratories; Fort Worth, TX), making sure that they’re lubricating their skin frequently with something perhaps in the wintertime as thick as petroleum jelly. And then in the summertime perhaps with Sarna lotion (Crown Laboratories; Johnson City, TN), which has menthol. It’s important to note that when the patient’s skin is infected, the itch can skyrocket. Being aware and monitoring the skin for signs of infection such as crusting and impetigo-like findings can be helpful.
I also wanted to touch on fatigue. Patients can have fatigue for many reasons. Sometimes it’s because the itch is interfering with their sleep. How do you approach managing fatigue?
Lauren Pinter-Brown. There have been many studies about cancer fatigue, and it appears that one of the cheapest and easiest modalities is for patients to walk. We often suggest that our patients go on walks, however much they can do, because that has been seen over and over again in studies of cancer fatigue to be beneficial.
John Zic. Do you have any advice for nurses that might be helping to manage patients in a cutaneous lymphoma clinic?
Marianne Tawa. As this is a rare disease, nursing encounters with patients carrying a diagnosis of CTCL in both oncology and dermatology settings may be few and far between. I recommend nurses familiarize themselves with articles published on CTCL topics found in both dermatology and oncology peer review journals. Another avenue for gaining insight and education would be through continuing education courses. Resources can also be found for nurses, patients, and caregivers through advocacy foundations such as the Cutaneous Lymphoma Foundation (www.clfoundation.org) and the Lymphoma Research Foundation (LRF@lymphma.org).
John Zic. Is there anything else that anyone would like to add to our discussion?
Lauren Pinter-Brown. One thing that we touched upon, but I was concerned that we didn’t emphasize, was the use of flow cytometry as a diagnostic tool in a patient with erythroderma. Sometimes biopsies of patients with erythroderma are not diagnostic, so clinicians need to be aware that there are other ways of diagnosing patients—nodal biopsy or flow cytometry. They should not only think of it as a staging tool but sometimes as a diagnostic tool.
Alejandro Ariel Gru. I agree. Particularly in patients who have Sézary syndrome or MF with peripheral blood involvement, sometimes the findings on the biopsy show a dissociation between how impressive the clinical presentation of the patient might be and how very few findings you might encounter on the skin biopsy. Therefore, relying on flow cytometry as a diagnostic tool is capital. Lauren, you briefly mentioned the criteria, which is looking for an abnormal CD4 to CD8 ratio of > 10%, abnormal loss of CD7, > 40%, or abnormal loss of CD26 of > 30%.
In addition, there are new markers that are now undergoing validation in the diagnosis of Sézary syndrome. One is KIR3DL2, which is a natural killer receptor that has been shown to be significantly upregulated in Sézary syndrome and appears to be both more sensitive and specific. With that also comes therapies that target the KIR3DL2 molecule.
John Zic. One of the first things we teach our dermatology residents to work up patients with erythroderma is that they shouldn’t expect the skin biopsy to help them sort out the cause of the erythroderma. As you mentioned, Lauren, the flow cytometry of peripheral blood should always be accompanied by a CBC with differential and platelets. And if the patients do have lymph nodes, consider a biopsy because sometimes that’s where you can make the firmest diagnosis of a T-cell lymphoma.
Acknowledgmentszz
The participants and Federal Practitioner would like to thank Susan Thornton, CEO of the Cutaneous Lymphoma Foundation for helping to arrange this roundtable discussion.
1. Willemze R, Cerroni L, Kempf W, et al. The 2018 update of the WHO-EORTC classification for primary cutaneous lymphomas. Blood. 2019;133(16):1703-1714.
2. Imam MH, Shenoy PJ, Flowers CR, Phillips A, Lechowicz MJ. Incidence and survival patterns of cutaneous T-cell lymphomas in the United States. Leuk Lymphoma. 2013;54(4):752-759.
3. Del Guzzo C, Levin A, Dana A, et al. The incidence of cutaneous T-Cell lymphoma in the veteran population. Abstract 133. J Invest Dermatol. 2016;136(5 suppl 1):S24.
4. Aschebrook-Kilfoy B, Cocco P, La Vecchia C, et al. Medical history, lifestyle, family history, and occupational risk factors for mycosis fungoides and Sèzary syndrome: the InterLymph Non-Hodgkin lymphoma subtypes project. J Natl Cancer Inst Monogr. 2014;48:98-105.
5. Scarisbrick JJ, Quaglino P, Prince HM, et al. The PROCLIPI international registry of early-stage mycosis fungoides identifies substantial diagnostic delay in most patients. Br J Dermatol. 2018. [Epub ahead of print.]
6. Thurber SE, Zhang B, Kim YH, Schrijver I, Zehnder J, Kohler S. T-cell clonality analysis in biopsy specimens from two different skin sites shows high specificity in the diagnosis of patients with suggested mycosis fungoides. J Am Acad Dermatol. 2007;57(5):782-790.
7. Kim YH, Jensen RA, Watanabe GL, Varghese A, Hoppe RT. Clinical stage IA (limited patch and plaque) mycosis fungoides. A long-term outcome analysis. Arch Dermatol. 1996;132(11):1309-1313.
8. Benton EC, Crichton S, Talpur R, et al. A cutaneous lymphoma international prognostic index (CLIPi) for mycosis fungoides and Sézary syndrome. Eur J Cancer. 2013; 49(13):2859-2868.
9. Battistella M, Sallé de Chou C, de Bazelaire C, et al. Lymph node image-guided core-needle biopsy for cutaneous T-cell lymphoma staging. Br J Dermatol. 2016;175(6):1397-1400.
10. Johnson WT, Mukherji R, Kartan S, Nikbakht N, Porcu P, Alpdogan O. Allogeneic hematopoietic stem cell transplantation in advanced stage mycosis fungoides and Sézary syndrome: a concise review. Chin Clin Oncol. 2019;8(1):12.
11. Johnson WT, Mukherji R, Kartan S, Nikbakht N, Porcu P, Alpdogan O. Allogeneic hematopoietic stem cell transplantation in advanced stage mycosis fungoides and Sézary syndrome: a concise review. Chin Clin Oncol. 2019;8(1):12.
12. Wilson LD, Jones GW, Kim D, et al. Experience with total skin electron beam therapy in combination with extracorporeal photopheresis in the management of patients with erythrodermic (T4) mycosis fungoides. J Am Acad Dermatol. 2000;43(1 Pt 1):54-60.
John Zic, MD. Let’s start by defining cutaneous T-cell lymphomas (CTCLs) and how they differ from other non-Hodgkin lymphomas. We also should discuss classification, which can be very confusing and epidemiology as it relates to the veteran population. Then I think we should dive into challenges with diagnosis and when should a VA or any provider consider mycosis fungoides (MF) and Sézary syndrome—the 2 most common variants of CTCLs.
I like to define the primary CTCLs as malignancies of the T-cell where the primary organ of involvement is the skin. However, this disease can spread to lymph nodes and visceral organs and the blood compartment in more advanced patients. Alejandro, could you provide some highlights about how CTCLs are classified?
Alejandro Ariel Gru, MD. Lymphomas are divided in the general hematology/oncology practice as Hodgkin and non-Hodgkin lymphomas. Traditionally all lymphomas that occur on the skin are non-Hodgkin lymphoma subtypes. That has specific connotations in terms of diagnosis, prognosis, and therapy. Because the T cells are one of the main residents of the subtypes of lymphocytes you encounter on the skin, most lymphomas that occur on the skin are derived of T-cell origin. B-cell lymphomas, in general, tend to be relatively uncommon or more infrequent.
There are 3 main subtypes of CTCL that present on the skin.1 MF is, by far, the most common subtype of CTCL. The disease tends to present in patients who are usually aged > 60 years and is more frequent in white males. It’s a lymphoma that is particularly relevant to the veteran population. The second subtype has many similarities to MF but shows substantial peripheral blood involvement and is referred to as Sézary syndrome. The third group is encompassed under the term CD30-positive lymphoproliferative disorders. This group includes 2 main subtypes: primary cutaneous anaplastic large-cell lymphoma and lymphomatoid papulosis. Some cases of MF develop progression to what we call large cell transformation, which implies cytologic transformation to a more aggressive lymphoma.
There are other cutaneous lymphomas that are far less common. Some are indolent and others can be more aggressive, but they represent < 5% of all CTCL subtypes.
Lauren Pinter-Brown, MD. That was a great summary about these non-Hodgkin lymphomas. In the veteran population, it’s wise to remember that there are many kinds of non-Hodgkin lymphomas. Because of the action that they have seen, some people, such as Vietnam veterans, might be more susceptible to non-Hodgkin lymphomas than others.
John Zic. That’s a good point because certainly non-Hodgkin lymphomas are listed as one of the potential disease associations with exposure to Agent Orange.
I’d like to move on to epidemiology and the incidence of MF and Sézary syndrome. An article that came out of Emory University in 2013 is one of the more up-to-date articles to examine the incidence and survival patterns of CTCL.2 The authors looked at patients from 2005 to 2008 and identified 2,273 patients in the Surveillance, Epidemiology, and End Results registry. They estimated that the incidence of MF in the US population is about 5.5 per 1,000,000 per year, which certainly makes it a rare disease. The incidence of Sézary syndrome was 0.1 per 1,000,000 per year, which comes out to about 1 per 10 million per year.
However, the MF incidence needs to be contrasted to the estimated incidence in the veteran population. In 2016, Larisa Geskin and colleagues from Columbia University and the Bronx US Department of Veterans Affairs (VA) Medical Center examined the VA database of patients with diagnoses of MF and Sézary syndrome.3 They combined them, but I have a feeling that the amount of Sézary syndrome patients was much less than those with MF. They estimated an incidence per million of 62 to 79 cases per 1,000,000 per year. The conclusion of Dr. Geskin’s study stated that the incidence of CTCL in the veteran population appears to be anywhere from 6 to 8 times higher. But if we use the most recent US incidence rates, it’s more than 10 times higher.
Those of you who have worked with veterans, either at the VA or in your private practice, do you have any ideas about why that might be?
Lauren Pinter-Brown. As you previously discussed, this is an illness of older people, and Vietnam veterans now are in their 60s and 70s. They may account for a lot of these diagnoses.
John Zic. That’s a good point. There’s quite a bit of talk about exposure to Agent Orange. But honestly, we really don’t know the cause of any of the CTCLs. We have not been able to identify a single cause. There are some risk factors. A 2014 article from the Journal of the National Cancer Institute looked at 324 cases of CTCL and compared it with 17,000 controls.4 They showed some interesting risk factors, such as body mass index (BMI) > 30 and smoking > 40 years. Similar to previous European studies, they showed that occupations like being a farmer, a painter, a woodworker, or a carpenter may carry additional risk.I wonder whether or not veterans were more likely to have some of these risk factors that this epidemiologic study picked up in addition to exposures that they may have encountered during their active-duty service. Interestingly, a decreased risk factor for developing MF was moderate physical activity. Clearly though, there are a large number of patients with CTCL in the veteran population.
I’d like to turn now to some of the challenges with diagnosis. Marianne, could you share some of your experience with early-stage disease and about how long it took them to be diagnosed?
Marianne Tawa, RN, MSN, ANP. Speaking specifically about early-stage disease, patients often share a history of waxing and waning rash that may not be particularly itchy. Confounding the picture, the distribution of early patch or plaque stage CTCL rash frequently occurs in covered areas. Many patients miss out on complete skin examinations by providers, thus early-stage CTCL may not be appreciated in a timely manner.
In certain scenarios, it may take upward of 5 to 7 years before the CTCL diagnosis is rendered. This is not because the patient delayed care. Nor is it because a skin biopsy was not performed. The progression of the disease and meeting the classic features of histology under the microscope can require clinical observation over time and repeated skin biopsies. We recommend patients refrain from topical steroid applications for 2 to 4 weeks prior to skin biopsy if we have a strong suspicion of CTCL. Many patients will report having a chronic eczematous process. Some patients may have a history of parapsoriasis, and they’re on the continuum for CTCL. That’s a common story for CTCL patients.
John Zic. What is the role of a skin biopsy in the diagnosis of CTCL? We see many patients who have had multiple skin biopsies who often wonder whether or not the diagnosis was missed by either the clinician or the pathologist.
Alejandro Ariel Gru. That is a great area of challenge in terms of pathologic diagnosis of early MF. A study led by Julia Scarisbrick, from an international registry data (PROCLIPI) on the early stages of the disease, showed a median delay of diagnosis of early MF of approximately 36 months.5 For all physicians involved in the diagnosis and care of patients with MF, the delay is probably significantly higher than that. We’ve seen patients who have lived without a diagnosis for a period of 10 or sometimes 15 years. That suggests that many cases are behaving in an indolent fashion, and patients are not progressing through the ‘natural’ stages of the disease and remain at the early stage. There also is the potential that other chronic inflammatory conditions, particularly psoriasis or parapsoriasis, can be confused with this entity. The diagnosis of certain types of parapsoriasis, can belong to the same spectrum of MF and can be treated in a similar way than patients with early stage MF are, such as phototherapy or methotrexate.
The diagnosis of MF relies on a combination of clinical, pathologic, and immunophenotypic findings where it is desired or preferred that at least 2 biopsies are done from different sides of the body. In addition to having a good clinical history that supports the diagnosis, a history of patches, plaques, and sometimes tumors in advanced stages in particular locations that are covered from the light (eg, trunk, buttocks, upper thighs, etc) combined with specific histopathologic criteria are capital to establish an accurate diagnosis.
In the biopsies, we look particularly for a lymphoid infiltrate that shows extension to the epidermis. We use the term epidermotropism to imply that these abnormal or neoplastic lymphocytes extend into the epidermis. They are also cytologically atypical. We see variations in the nucleus. In the size, we see a different character of the chromatin where they can be hyperchromatic. We also look for immunophenotypic aberrations, and particularly we analyze for patterns of expression of T-cell markers. Most cases of MF belong to a subset of T cells that are called CD4-positive or T-helper cells. We look for a patterned ratio of the CD4 and CD8 between the epidermis and an aberrant loss of the CD7 T-cell marker. Once we establish that we can see significant loss of these markers, we can tell where there is something wrong with that T-cell population, and likely belong to a neoplastic category.
In addition, we also rely on the molecular evaluation and search of a clonal population of T cells, by means of a T-cell receptor gene rearrangement study. Ideally, we like to see the establishment of a single clone of T cells that is matched in different biopsy sites. Proving that the same clone is present in 2 separate biopsies in 2 separate sites is the gold standard for diagnosis.6
John Zic. To recap, a biopsy is indicated for patients who have patches or plaques (that are slightly raised above the skin) in sun-protected areas that are fixed; rather than completely go away in the summer and come back in the winter, they are fixed if they have been present > 6 to 12 months. Many of these patients are diagnosed with eczema, psoriasis, allergic contact dermatitis, and other skin diseases before the clinician starts to think about other diagnoses, such as CTCL.
I agree that I would not rule out the diagnosis with 1 biopsy that does not show classic histologic changes. Also, I think that it’s important to alert the pathologist that you’re considering a diagnosis of T-cell lymphoma, either MF or some of the other subtypes, because that will certainly alert them to look a little closer at the infiltrating cells and perhaps do some of the other testing that was mentioned. Once we establish the MF diagnosis, staging studies may be indicated.
Lauren Pinter-Brown. Early stage would be patients with patches or plaques. Stage IA would be < 10% body surface area, and stage IB would be > 10%. I don’t perform scans for early-stage patients, but I do a very thorough physical and perform blood tests. For patients that have more advanced disease, such as tumors, erythroderma, or Sézary syndrome, I would conduct the same thorough examination and blood tests and scan the patient either with a computed tomography (CT) or a positron emission tomography (PET)/CT to detect adenopathy. We have to recognize that most of the adenopathy that is detected in these patients is peripheral, and we can feel it on physical examination.
John Zic. Do you prefer one imaging modality over the other? CT scan with IV contrast vs PET/CT?
Lauren Pinter-Brown. I tend to use PET/CT because it illuminates extranodal sites as well. I have to admit that sometimes it’s a problem to get that approved with insurance.
John Zic. In the federal system, many PET/CT scans are performed at other facilities. That would be an extra step in getting approval.
You mentioned Sézary syndrome. We should consider a diagnosis of Sézary syndrome when you have a patient with erythroderma, which means that they have > 80% of the skin covered in redness and scaling.
Lauren Pinter-Brown. The first step is to do a complete blood count (CBC) and see if there’s a lymphocytosis. Sometimes that really isn’t very sensitive, so my go-to test is flow cytometry. We are looking for an abnormal population of cells that, unlike normal T cells, often lack certain T-cell antigens. The most common would be CD7. We can confirm that this is a clone by T-cell gene rearrangement, and often in Sézary we like to compare the gene rearrangement seen in blood with what might be seen in the skin biopsy to confirm that they’re the same clone.
John Zic. That’s an excellent point. I know there are specific criteria to meet significant blood involvement. That is a topic of conversation among CTCL experts and something that might be changing over the next few years. But I think as it stands right now, having a lymphocytosis or at least an elevated CD4 count along with having a clone in the blood matching the clone in the skin are the first 2 steps in assessing blood involvement. However, the flow cytometry is very important. Not all medical centers are going to do flow cytometry—looking specifically for a drop of the CD7 or CD26 antigen among the CD4 population. But that is one of the major criteria that we look for in those patients with suspected blood involvement.
Marianne Tawa. Additionally, we would advise obtaining flow cytometry on patients that look like they have a robust skin burden with lots of patches, plaques, or tumors. We also perform lactate dehydrogenase (LDH) with staging.
John Zic. What do you usually tell patients with early-stage disease, those that have patches and plaques?
Marianne Tawa. For patients with stage IA disease, we are very optimistic about their prospects. We explain that the likelihood that early-stage disease will progress to a more advanced stage or rare variant is unlikely. This is very much a chronic disease, and the goal is to manage appropriately, palliate symptoms, and preserve quality of life (QOL).
Lauren Pinter-Brown. I often refer to a landmark paper by Youn H. Kim and colleagues that shows us that patients with IA disease who are at least treated usually have a normal lifespan.7 I encourage patients by sharing that data with them.
John Zic. Sean Whittaker and colleagues in the United Kingdom identified 5 risk factors for early-stage patients that may put them at higher risk for progressing: aged > 60 years; having a variant called folliculotropic MF; having palpable lymph nodes even if they’re reactive on biopsy, having plaques, and male sex.8 For staging of lymph nodes, what’s your usual approach when you see a patient with palpable lymph nodes?
Lauren Pinter-Brown. Many patients, particularly those with advanced skin disease, may have palpable lymph nodes that are reacting to their skin disease and on pathology would be dermatopathic. That would not change my management. I pay attention to the quality of the lymph node—if it’s very firm, if it’s > 2 cm, if it is persistent—before I biopsy. These patients have a higher incidence of wound infection after excisional biopsy. If the patient has pathologic lymph node involvement and effacement of the node with malignant cells, I would change my management. I do need to know that sort of information.
John Zic. Alejandro, as a hematopathologist can you comment on the debate about whether or not we actually do need an excisional biopsy or whether or not we can get a core lymph node biopsy to give you all the information that you need to grade it?
Alejandro Ariel Gru. There are 2 main modalities of biopsies we typically see for lymph nodes for evaluation and staging for involvement of CTCL. One is the traditional excisional biopsy that for the most part requires surgery with general anesthesia and has all the major implications that that type of procedure has. Many centers are looking at less invasive types of procedures, and needle core biopsies have become one of the most common forms of biopsy for all lymphoma subtypes. Excisional biopsies have the advantage of being able to see the whole lymph node, so you can determine and evaluate the architecture very well. Whereas needle core biopsies typically use a small needle to obtain a small piece of the tissue.
The likelihood of a successful diagnosis and accurate staging was compared recently in the British Journal of Dermatology.9 They were able to perform accurate staging in needle core biopsies of patients with MF. However, this is still a matter of debate; many people feel they are more likely to get enough information from an excisional biopsy. As we know, excisional biopsies sometimes can be hard, particularly if the large lymph node is located in an area that is difficult to access, for example, a retroperitoneal lymph node.
There are many staging categories that are used in the pathologic evaluation of lymph node involvement. On one hand, we could see the so-called dermatopathic changes, which is a reactive form of lymphadenopathy that typically happens in patients who have skin rashes and where there is no evidence of direct involvement by the disease (although there are some patients who can have T-cell clones by molecular methods). The patients who have clonal T cells perhaps might not do as well as the ones who do not. On the other hand, we have patients for whom the whole architecture of the lymph node is effaced or replaced by neoplastic malignant cells. Those patients are probably going to need more aggressive forms of therapy.10
John Zic. The type of lymph node biopsy has been a hot topic. If patients have palpable lymph nodes in the cervical, axillary, and inguinal area, I don’t know if it’s a consensus, but the recommendation right now is to consider performing a lymph node biopsy of the cervical lymph nodes first, axillary second, and inguinal lymph nodes third. That might have to do with the complication rates for those different areas.
I’d like to switch to a discussion to more advanced disease. CTCL tumors are defined as a dome-shaped nodule > 1 cm. They don’t have to be very big before we label it a tumor, and the disease is considered more advanced. For patients with a few tumors, what does your prognosis discussion sound like?
Marianne Tawa. Certainly, the prognosis discussion can become slightly more complicated when you move into the realm of tumor-stage development. This is especially true if a CTCL patient has lived with and managed indolent patches or plaques for several years. We approach these patients with optimism and with the goal of managing their tumors, whether it be with a skin-directed option, such as localized radiation or a host of approved systemic therapies. Patients presenting with or developing tumor-stage disease over time will require additional staging workup compared with early-stage disease staging practice. Patients are counseled on imaging use in tumor-stage disease and why flow cytometry may be requested to rule in or rule out accompanying peripheral blood involvement. Patients are exposed to a myriad of pictures, stories, and survival statistics from Internet research. It becomes our task to inform them of their unique presentation and tailored treatment plan, which thankfully may produce more favorable responses than those presented online.
Lauren Pinter-Brown. One thing that we focus on is the idea that a statistic regarding prognosis isn’t predictive for an individual patient. When patients go online, we caution them that many of the statistics are really old. There’s been a lot of new therapies in the past 10 years. Just looking at my patients, my feeling is that their prognosis has continued to improve over the decades that I’ve been involved in this area.
We have to take the statistics with a grain of salt, though certainly someone that has Sézary syndrome or someone that has nodal involvement or tumors is not going to fare as well as the patients that we talked about with stage I disease. However, if we all continue to do our jobs and have more and more treatment options for patients, that’s certainly going to change over time as it has with other non-Hodgkin lymphomas.
John Zic. We’ve all treated advanced patients with disease and some, of course, have died of the disease. When patients die of advanced CTCL, what are the things that lead to their demise?
Lauren Pinter-Brown. Probably the most common would be infections because their skin barrier has been broken. As the disease advances, their immune system also deteriorates. We may contribute to that sometimes with some of the therapies that we use, although we try and be judicious. First and foremost, the primary cause of death remains infection and sometimes inanition.
Marianne Tawa. I agree, infection or just the unfortunate progression of their lymphoma through the various armamentarium of treatments would be the 2 reasons.
John Zic. Let’s dive into therapy. I want to start with early stage. While, I don’t think there’s a role for systemic anticancer agents, certainly the IV agents for most patients with early-stage disease Marianne, you mentioned phototherapy. What are the types of phototherapy that you offer?
Marianne Tawa. We would start out with narrow band UVB therapy for patients with > 10% body surface area involvement. When applying topical corticosteroids to wider surface areas of the patient’s body is no longer feasible or effective, we recommend the initiation of narrow band UVB phototherapy. This is preferred because of its lessor adverse effect (AE) profile as far as nonmelanoma skin cancer risk. Patients commence narrow band UVB 3 times per week, with a goal of getting the patient into remission over a matter of months and then slowly tapering the phototherapy so that they get to a maintenance of once weekly.
Realizing that narrow band UVB may not penetrate deeper plaques or effectively reach folliculotropic variant of CTCL, we would employ PUVA, (psoralen and UVA). Patients are expected to protect their eyes with UVA glasses and remain out of the sun 24 hours following PUVA treatments. The cost of the methoxsalen can be an issue for some patients. Nonmelanoma skin cancer risks are increased in patients undergoing long-term PUVA treatments. Routine skin cancer surveillance is key.
There are monetary, time, and travel demands for patients receiving phototherapy. Thus, many CTCL patients are moving toward home-based narrow band UVB units supervised by their treating dermatologist. Other skin-directed treatment options, aside from topical corticosteroids and phototherapy, would include topical nitrogen mustard, imiquimod, and localized or total skin electron beam radiation.
John Zic. Here in Nashville, some of our veterans travel hundreds of miles to get to our center. It’s not practical for them to come here for the narrow band UVB phototherapy. Veterans can get approval through the VA Choice programs to have phototherapy performed by a local dermatologist closer to home. We also have had many veterans who choose to get home narrow band UVB phototherapy, which can be quite effective. Narrow band UVB phototherapy is among the most effective therapies for patients with generalized patches in particular, and maybe some with just a few plaques.
Medium potency topical steroids are not as helpful as superpotent topical steroids such as clobetasol, dipropionate ointment, or betamethasone dipropionate ointment. Usually, I tell patients to apply it twice a day for 8 weeks. You must be careful because these high-potency topical steroids can cause thinning of the skin, but it’s rarely seen, even in patients that may use them for 8 weeks if they’re applying them just to their patches and thin plaques. There are a few other topicals. There’s bexarotene gel, which is a topical retinoid, and mechlorethamine or nitrogen mustard gel that are available as topicals. Both of those can be helpful if patients have < 10% body surface area of patches or plaques because they can apply that at home.
Because of the excellent prognosis for patients in early stages, this is an area we want to try to avoid doing harm. For patients with advanced disease, what are some of the decisions that you think about in recommending a patient to get radiation therapy?
Lauren Pinter-Brown. I use radiation therapy sparingly and primarily for patients who either have only 1 tumor and the rest of their disease is patch and plaque or for patients who have very large tumors that are either cosmetically unacceptable or creating infection or pain. I treat people with systemic therapies primarily to prevent the formation of tumors.
John Zic. There probably is a role for total skin electron beam radiotherapy in patients who have failed multiple other skin-directed therapies and are progressing and then perhaps a role for more advanced patients who have multiple tumors where you’re trying to get some control of the disease. Are there any other situations where you might consider total skin electron beam?
Marianne Tawa. Yes, those are 2 scenarios. A third scenario would be in patients preparing for stem cell transplant. We typically do a modified 12 Gy regimen of total skin electron beam for palliation and up to 24 Gy regimen for patients who are in earnest preparing for a stem cell transplant.
John Zic. Systemic therapies also treat this disease. There are 2 oral agents. One is bexarotene capsules, a retinoid that binds to the RXR receptor and has a multitude of effects on different organ systems. It is probably the best tolerated oral agent we have. The other FDA-approved agent is vorinostat, a histone deacetylase inhibitor, but it has more gastrointestinal AEs than does bexarotene. Bexarotene has AEs as well, including hypertriglyceridemia and central hypothyroidism, which can throw a curveball to unsuspecting primary care physicians who might check thyroid function studies in these patients.
We certainly need to know about those AEs. There are many patients who have tumor-stage disease that can have radiotherapy to several tumors, then go on a drug like bexarotene capsules and may be able to maintain the remission for years. In my experience, it’s a drug that patients usually stay on. They can be weaned to a very low dose, but I’ve had several patients who come off of bexarotene only to suffer relapses.
Lauren, what are some of the things that you think about when you declare someone as having failed bexarotene or vorinostat and you’re thinking about IV therapies?
Lauren Pinter-Brown. Patient comorbidities and the particular compartment of their body that is involved are important factors. Do they have blood involvement, or not? Do they have nodal involvement, or not? Another concern is both acute and chronic toxicities that need to be discussed with the patient to determine an acceptable QOL. Finally, the schedule that you’re giving the drug. Some people may not be able to come in frequently. There are a lot of variables that go into making an individual decision at a particular time for a specific patient who will be using parenteral therapies.
John Zic. If we have a patient with advanced MF, tumors, and perhaps lymph node involvement, what are some of the systemic options that you would consider?
Lauren Pinter-Brown. With nodal involvement, an attractive option is something like IV romidepsin because we know that it treats peripheral T-cell lymphomas, which are aggressive nodal T-cell lymphomas. It’s FDA approved and also treats CTCL. Another is brentuximab vedotin if there is significant CD30 expression. It also is FDA approved for CTCL and has a long track record of treating certain peripheral T-cell lymphomas like anaplastic large cell.
John Zic. When would the stem cell transplant discussion start at your institution?
Lauren Pinter-Brown. It starts earlier for a younger patient because even though we do have lots of treatment if someone is aged 20 or30 years, I don’t really have any illusions that I have enough treatment options for them to live a normal lifespan if they have advanced disease. It’s a possibility for any patient when I see that the future options are dwindling, and that I am not going to be able to control the patient’s disease for much longer. Having said that, patients who have tumor-stage disease are among those that don’t do quite as well with allogeneic transplantation; ironically, patients with Sézary syndrome or erythroderma might do a little bit better.
John Zic. Before considering a stem cell transplant for patients with Sézary syndrome, that is erythroderma with significant blood involvement, what other treatment options would you offer?
Marianne Tawa. For low blood-burden disease, we might look at extracorporeal photopheresis as monotherapy or in combination with interferon or bexarotene. For patients with higher blood burden we might recommend low-dose alemtuzumab, especially if they have abundant CD52 expression. We also consider the newly FDA-approved anti-CCR4 antibody treatment, mogamulizumab, for patients presenting with Sézary syndrome. It is generally well tolerated but does have the potential for producing infusion reactions or drug rash.
Romidepsin has efficacy in blood, lymph node, and skin compartments. The primary considerations for patients considering romidepsin are prolonged infusion times and QOL AEs with gastrointestinal and taste disturbances and fatigue.
John Zic. Both of you have brought up an excellent point. This is a disease that while we do not have a good chance of curing, we have a pretty fair chance of controlling, especially if it’s early stage. The data from the stem cell transplant literature indicate that stem cell transplant may be one of the few modalities that we have that may offer a cure.11
Lauren Pinter-Brown. There are patients who are cured with allogeneic transplants; and the very first allogeneic transplants were performed well over 20 years ago. Many patients, even some in my practice, who were among those patients and continue to do extremely well without any evidence of disease. Sometimes when people have allogeneic transplantation, their disease relapse may be in a more indolent form that’s much easier to deal with than their original disease. Even if they’re not cured, the fact that the aggressive disease seems to be at bay may make them much easier to treat.
John Zic. Those are excellent points. You brought up photopheresis as a treatment modality for patients with evolving or early Sézary syndrome and patients with erythrodermic MF can also respond. We have a lot of experience with that at the Nashville VA medical center. We’re one of the few VA hospitals in the US that has a photopheresis unit. But the modality is available at many academic medical centers because it’s a treatment for graft-vs-host disease.
We tend to also consider photopheresis in patients who may have had an excellent response to another systemic agent. There are some data that patients who received photopheresis, after total skin electron beam therapy vs those who received chemotherapy after radiation, had a longer disease-free survival.12
I’d like to end with a discussion of something that’s very important, which is managing QOL issues for patients with CTCL. Itch is among some of the worst symptoms that can cause suffering in patients. But it is sometimes not a problem at all for patients who have a few patches or plaques. That’s one reason why they might ignore their rash. Certainly, as the disease progresses, especially those patients with erythroderma, the itch can be intractable and can have a major impact on their life. What are some approaches to managing itch at your institutions?
Lauren Pinter-Brown. One thing to be aware of is that the itch is not usually mediated by histamine, though people will often put the patients on a lot of antihistamines. I don’t find those to be the most effective treatments. I think of the itch in these patients as more of a neuropathic condition and would tend to treat more with things that you might use for neuropathy, such as gabapentin or doxepin or antidepressants. There’s a whole host of other treatments, such as aprepitant, something that I would use as an antiemetic, that might also be helpful for pruritus in this patient population.
John Zic. That’s my experience as well. I have found gabapentin to be helpful for patients with itch, though not universally.
Marianne Tawa. I consider itch a huge QOL concern for a large majority of our patients with a CTCL diagnosis. It’s on par with pain. In early-stage disease, pruritus levels improve as the cutaneous burden is reduced with skin-directed therapies such as, topical corticosteroid or phototherapy.
SSRI agents could also be considered for select patients. The antiemetic agent, aprepitant has been useful for addressing itch in a subset of our patients with Sézary syndrome. Patients will also seek out complementary modalities such acupuncture, hypnosis, and guided imagery.
John Zic. Because the disease itself affects the skin and can lead to dryness, patients often suffer with dry skin. When I trained in Chicago, that was the foundation of our treatment, making sure that patients are using a super fatted soap such as Dove (Unilever, London, United Kingdom) or Cetaphil (Galderma Laboratories; Fort Worth, TX), making sure that they’re lubricating their skin frequently with something perhaps in the wintertime as thick as petroleum jelly. And then in the summertime perhaps with Sarna lotion (Crown Laboratories; Johnson City, TN), which has menthol. It’s important to note that when the patient’s skin is infected, the itch can skyrocket. Being aware and monitoring the skin for signs of infection such as crusting and impetigo-like findings can be helpful.
I also wanted to touch on fatigue. Patients can have fatigue for many reasons. Sometimes it’s because the itch is interfering with their sleep. How do you approach managing fatigue?
Lauren Pinter-Brown. There have been many studies about cancer fatigue, and it appears that one of the cheapest and easiest modalities is for patients to walk. We often suggest that our patients go on walks, however much they can do, because that has been seen over and over again in studies of cancer fatigue to be beneficial.
John Zic. Do you have any advice for nurses that might be helping to manage patients in a cutaneous lymphoma clinic?
Marianne Tawa. As this is a rare disease, nursing encounters with patients carrying a diagnosis of CTCL in both oncology and dermatology settings may be few and far between. I recommend nurses familiarize themselves with articles published on CTCL topics found in both dermatology and oncology peer review journals. Another avenue for gaining insight and education would be through continuing education courses. Resources can also be found for nurses, patients, and caregivers through advocacy foundations such as the Cutaneous Lymphoma Foundation (www.clfoundation.org) and the Lymphoma Research Foundation (LRF@lymphma.org).
John Zic. Is there anything else that anyone would like to add to our discussion?
Lauren Pinter-Brown. One thing that we touched upon, but I was concerned that we didn’t emphasize, was the use of flow cytometry as a diagnostic tool in a patient with erythroderma. Sometimes biopsies of patients with erythroderma are not diagnostic, so clinicians need to be aware that there are other ways of diagnosing patients—nodal biopsy or flow cytometry. They should not only think of it as a staging tool but sometimes as a diagnostic tool.
Alejandro Ariel Gru. I agree. Particularly in patients who have Sézary syndrome or MF with peripheral blood involvement, sometimes the findings on the biopsy show a dissociation between how impressive the clinical presentation of the patient might be and how very few findings you might encounter on the skin biopsy. Therefore, relying on flow cytometry as a diagnostic tool is capital. Lauren, you briefly mentioned the criteria, which is looking for an abnormal CD4 to CD8 ratio of > 10%, abnormal loss of CD7, > 40%, or abnormal loss of CD26 of > 30%.
In addition, there are new markers that are now undergoing validation in the diagnosis of Sézary syndrome. One is KIR3DL2, which is a natural killer receptor that has been shown to be significantly upregulated in Sézary syndrome and appears to be both more sensitive and specific. With that also comes therapies that target the KIR3DL2 molecule.
John Zic. One of the first things we teach our dermatology residents to work up patients with erythroderma is that they shouldn’t expect the skin biopsy to help them sort out the cause of the erythroderma. As you mentioned, Lauren, the flow cytometry of peripheral blood should always be accompanied by a CBC with differential and platelets. And if the patients do have lymph nodes, consider a biopsy because sometimes that’s where you can make the firmest diagnosis of a T-cell lymphoma.
Acknowledgmentszz
The participants and Federal Practitioner would like to thank Susan Thornton, CEO of the Cutaneous Lymphoma Foundation for helping to arrange this roundtable discussion.
John Zic, MD. Let’s start by defining cutaneous T-cell lymphomas (CTCLs) and how they differ from other non-Hodgkin lymphomas. We also should discuss classification, which can be very confusing and epidemiology as it relates to the veteran population. Then I think we should dive into challenges with diagnosis and when should a VA or any provider consider mycosis fungoides (MF) and Sézary syndrome—the 2 most common variants of CTCLs.
I like to define the primary CTCLs as malignancies of the T-cell where the primary organ of involvement is the skin. However, this disease can spread to lymph nodes and visceral organs and the blood compartment in more advanced patients. Alejandro, could you provide some highlights about how CTCLs are classified?
Alejandro Ariel Gru, MD. Lymphomas are divided in the general hematology/oncology practice as Hodgkin and non-Hodgkin lymphomas. Traditionally all lymphomas that occur on the skin are non-Hodgkin lymphoma subtypes. That has specific connotations in terms of diagnosis, prognosis, and therapy. Because the T cells are one of the main residents of the subtypes of lymphocytes you encounter on the skin, most lymphomas that occur on the skin are derived of T-cell origin. B-cell lymphomas, in general, tend to be relatively uncommon or more infrequent.
There are 3 main subtypes of CTCL that present on the skin.1 MF is, by far, the most common subtype of CTCL. The disease tends to present in patients who are usually aged > 60 years and is more frequent in white males. It’s a lymphoma that is particularly relevant to the veteran population. The second subtype has many similarities to MF but shows substantial peripheral blood involvement and is referred to as Sézary syndrome. The third group is encompassed under the term CD30-positive lymphoproliferative disorders. This group includes 2 main subtypes: primary cutaneous anaplastic large-cell lymphoma and lymphomatoid papulosis. Some cases of MF develop progression to what we call large cell transformation, which implies cytologic transformation to a more aggressive lymphoma.
There are other cutaneous lymphomas that are far less common. Some are indolent and others can be more aggressive, but they represent < 5% of all CTCL subtypes.
Lauren Pinter-Brown, MD. That was a great summary about these non-Hodgkin lymphomas. In the veteran population, it’s wise to remember that there are many kinds of non-Hodgkin lymphomas. Because of the action that they have seen, some people, such as Vietnam veterans, might be more susceptible to non-Hodgkin lymphomas than others.
John Zic. That’s a good point because certainly non-Hodgkin lymphomas are listed as one of the potential disease associations with exposure to Agent Orange.
I’d like to move on to epidemiology and the incidence of MF and Sézary syndrome. An article that came out of Emory University in 2013 is one of the more up-to-date articles to examine the incidence and survival patterns of CTCL.2 The authors looked at patients from 2005 to 2008 and identified 2,273 patients in the Surveillance, Epidemiology, and End Results registry. They estimated that the incidence of MF in the US population is about 5.5 per 1,000,000 per year, which certainly makes it a rare disease. The incidence of Sézary syndrome was 0.1 per 1,000,000 per year, which comes out to about 1 per 10 million per year.
However, the MF incidence needs to be contrasted to the estimated incidence in the veteran population. In 2016, Larisa Geskin and colleagues from Columbia University and the Bronx US Department of Veterans Affairs (VA) Medical Center examined the VA database of patients with diagnoses of MF and Sézary syndrome.3 They combined them, but I have a feeling that the amount of Sézary syndrome patients was much less than those with MF. They estimated an incidence per million of 62 to 79 cases per 1,000,000 per year. The conclusion of Dr. Geskin’s study stated that the incidence of CTCL in the veteran population appears to be anywhere from 6 to 8 times higher. But if we use the most recent US incidence rates, it’s more than 10 times higher.
Those of you who have worked with veterans, either at the VA or in your private practice, do you have any ideas about why that might be?
Lauren Pinter-Brown. As you previously discussed, this is an illness of older people, and Vietnam veterans now are in their 60s and 70s. They may account for a lot of these diagnoses.
John Zic. That’s a good point. There’s quite a bit of talk about exposure to Agent Orange. But honestly, we really don’t know the cause of any of the CTCLs. We have not been able to identify a single cause. There are some risk factors. A 2014 article from the Journal of the National Cancer Institute looked at 324 cases of CTCL and compared it with 17,000 controls.4 They showed some interesting risk factors, such as body mass index (BMI) > 30 and smoking > 40 years. Similar to previous European studies, they showed that occupations like being a farmer, a painter, a woodworker, or a carpenter may carry additional risk.I wonder whether or not veterans were more likely to have some of these risk factors that this epidemiologic study picked up in addition to exposures that they may have encountered during their active-duty service. Interestingly, a decreased risk factor for developing MF was moderate physical activity. Clearly though, there are a large number of patients with CTCL in the veteran population.
I’d like to turn now to some of the challenges with diagnosis. Marianne, could you share some of your experience with early-stage disease and about how long it took them to be diagnosed?
Marianne Tawa, RN, MSN, ANP. Speaking specifically about early-stage disease, patients often share a history of waxing and waning rash that may not be particularly itchy. Confounding the picture, the distribution of early patch or plaque stage CTCL rash frequently occurs in covered areas. Many patients miss out on complete skin examinations by providers, thus early-stage CTCL may not be appreciated in a timely manner.
In certain scenarios, it may take upward of 5 to 7 years before the CTCL diagnosis is rendered. This is not because the patient delayed care. Nor is it because a skin biopsy was not performed. The progression of the disease and meeting the classic features of histology under the microscope can require clinical observation over time and repeated skin biopsies. We recommend patients refrain from topical steroid applications for 2 to 4 weeks prior to skin biopsy if we have a strong suspicion of CTCL. Many patients will report having a chronic eczematous process. Some patients may have a history of parapsoriasis, and they’re on the continuum for CTCL. That’s a common story for CTCL patients.
John Zic. What is the role of a skin biopsy in the diagnosis of CTCL? We see many patients who have had multiple skin biopsies who often wonder whether or not the diagnosis was missed by either the clinician or the pathologist.
Alejandro Ariel Gru. That is a great area of challenge in terms of pathologic diagnosis of early MF. A study led by Julia Scarisbrick, from an international registry data (PROCLIPI) on the early stages of the disease, showed a median delay of diagnosis of early MF of approximately 36 months.5 For all physicians involved in the diagnosis and care of patients with MF, the delay is probably significantly higher than that. We’ve seen patients who have lived without a diagnosis for a period of 10 or sometimes 15 years. That suggests that many cases are behaving in an indolent fashion, and patients are not progressing through the ‘natural’ stages of the disease and remain at the early stage. There also is the potential that other chronic inflammatory conditions, particularly psoriasis or parapsoriasis, can be confused with this entity. The diagnosis of certain types of parapsoriasis, can belong to the same spectrum of MF and can be treated in a similar way than patients with early stage MF are, such as phototherapy or methotrexate.
The diagnosis of MF relies on a combination of clinical, pathologic, and immunophenotypic findings where it is desired or preferred that at least 2 biopsies are done from different sides of the body. In addition to having a good clinical history that supports the diagnosis, a history of patches, plaques, and sometimes tumors in advanced stages in particular locations that are covered from the light (eg, trunk, buttocks, upper thighs, etc) combined with specific histopathologic criteria are capital to establish an accurate diagnosis.
In the biopsies, we look particularly for a lymphoid infiltrate that shows extension to the epidermis. We use the term epidermotropism to imply that these abnormal or neoplastic lymphocytes extend into the epidermis. They are also cytologically atypical. We see variations in the nucleus. In the size, we see a different character of the chromatin where they can be hyperchromatic. We also look for immunophenotypic aberrations, and particularly we analyze for patterns of expression of T-cell markers. Most cases of MF belong to a subset of T cells that are called CD4-positive or T-helper cells. We look for a patterned ratio of the CD4 and CD8 between the epidermis and an aberrant loss of the CD7 T-cell marker. Once we establish that we can see significant loss of these markers, we can tell where there is something wrong with that T-cell population, and likely belong to a neoplastic category.
In addition, we also rely on the molecular evaluation and search of a clonal population of T cells, by means of a T-cell receptor gene rearrangement study. Ideally, we like to see the establishment of a single clone of T cells that is matched in different biopsy sites. Proving that the same clone is present in 2 separate biopsies in 2 separate sites is the gold standard for diagnosis.6
John Zic. To recap, a biopsy is indicated for patients who have patches or plaques (that are slightly raised above the skin) in sun-protected areas that are fixed; rather than completely go away in the summer and come back in the winter, they are fixed if they have been present > 6 to 12 months. Many of these patients are diagnosed with eczema, psoriasis, allergic contact dermatitis, and other skin diseases before the clinician starts to think about other diagnoses, such as CTCL.
I agree that I would not rule out the diagnosis with 1 biopsy that does not show classic histologic changes. Also, I think that it’s important to alert the pathologist that you’re considering a diagnosis of T-cell lymphoma, either MF or some of the other subtypes, because that will certainly alert them to look a little closer at the infiltrating cells and perhaps do some of the other testing that was mentioned. Once we establish the MF diagnosis, staging studies may be indicated.
Lauren Pinter-Brown. Early stage would be patients with patches or plaques. Stage IA would be < 10% body surface area, and stage IB would be > 10%. I don’t perform scans for early-stage patients, but I do a very thorough physical and perform blood tests. For patients that have more advanced disease, such as tumors, erythroderma, or Sézary syndrome, I would conduct the same thorough examination and blood tests and scan the patient either with a computed tomography (CT) or a positron emission tomography (PET)/CT to detect adenopathy. We have to recognize that most of the adenopathy that is detected in these patients is peripheral, and we can feel it on physical examination.
John Zic. Do you prefer one imaging modality over the other? CT scan with IV contrast vs PET/CT?
Lauren Pinter-Brown. I tend to use PET/CT because it illuminates extranodal sites as well. I have to admit that sometimes it’s a problem to get that approved with insurance.
John Zic. In the federal system, many PET/CT scans are performed at other facilities. That would be an extra step in getting approval.
You mentioned Sézary syndrome. We should consider a diagnosis of Sézary syndrome when you have a patient with erythroderma, which means that they have > 80% of the skin covered in redness and scaling.
Lauren Pinter-Brown. The first step is to do a complete blood count (CBC) and see if there’s a lymphocytosis. Sometimes that really isn’t very sensitive, so my go-to test is flow cytometry. We are looking for an abnormal population of cells that, unlike normal T cells, often lack certain T-cell antigens. The most common would be CD7. We can confirm that this is a clone by T-cell gene rearrangement, and often in Sézary we like to compare the gene rearrangement seen in blood with what might be seen in the skin biopsy to confirm that they’re the same clone.
John Zic. That’s an excellent point. I know there are specific criteria to meet significant blood involvement. That is a topic of conversation among CTCL experts and something that might be changing over the next few years. But I think as it stands right now, having a lymphocytosis or at least an elevated CD4 count along with having a clone in the blood matching the clone in the skin are the first 2 steps in assessing blood involvement. However, the flow cytometry is very important. Not all medical centers are going to do flow cytometry—looking specifically for a drop of the CD7 or CD26 antigen among the CD4 population. But that is one of the major criteria that we look for in those patients with suspected blood involvement.
Marianne Tawa. Additionally, we would advise obtaining flow cytometry on patients that look like they have a robust skin burden with lots of patches, plaques, or tumors. We also perform lactate dehydrogenase (LDH) with staging.
John Zic. What do you usually tell patients with early-stage disease, those that have patches and plaques?
Marianne Tawa. For patients with stage IA disease, we are very optimistic about their prospects. We explain that the likelihood that early-stage disease will progress to a more advanced stage or rare variant is unlikely. This is very much a chronic disease, and the goal is to manage appropriately, palliate symptoms, and preserve quality of life (QOL).
Lauren Pinter-Brown. I often refer to a landmark paper by Youn H. Kim and colleagues that shows us that patients with IA disease who are at least treated usually have a normal lifespan.7 I encourage patients by sharing that data with them.
John Zic. Sean Whittaker and colleagues in the United Kingdom identified 5 risk factors for early-stage patients that may put them at higher risk for progressing: aged > 60 years; having a variant called folliculotropic MF; having palpable lymph nodes even if they’re reactive on biopsy, having plaques, and male sex.8 For staging of lymph nodes, what’s your usual approach when you see a patient with palpable lymph nodes?
Lauren Pinter-Brown. Many patients, particularly those with advanced skin disease, may have palpable lymph nodes that are reacting to their skin disease and on pathology would be dermatopathic. That would not change my management. I pay attention to the quality of the lymph node—if it’s very firm, if it’s > 2 cm, if it is persistent—before I biopsy. These patients have a higher incidence of wound infection after excisional biopsy. If the patient has pathologic lymph node involvement and effacement of the node with malignant cells, I would change my management. I do need to know that sort of information.
John Zic. Alejandro, as a hematopathologist can you comment on the debate about whether or not we actually do need an excisional biopsy or whether or not we can get a core lymph node biopsy to give you all the information that you need to grade it?
Alejandro Ariel Gru. There are 2 main modalities of biopsies we typically see for lymph nodes for evaluation and staging for involvement of CTCL. One is the traditional excisional biopsy that for the most part requires surgery with general anesthesia and has all the major implications that that type of procedure has. Many centers are looking at less invasive types of procedures, and needle core biopsies have become one of the most common forms of biopsy for all lymphoma subtypes. Excisional biopsies have the advantage of being able to see the whole lymph node, so you can determine and evaluate the architecture very well. Whereas needle core biopsies typically use a small needle to obtain a small piece of the tissue.
The likelihood of a successful diagnosis and accurate staging was compared recently in the British Journal of Dermatology.9 They were able to perform accurate staging in needle core biopsies of patients with MF. However, this is still a matter of debate; many people feel they are more likely to get enough information from an excisional biopsy. As we know, excisional biopsies sometimes can be hard, particularly if the large lymph node is located in an area that is difficult to access, for example, a retroperitoneal lymph node.
There are many staging categories that are used in the pathologic evaluation of lymph node involvement. On one hand, we could see the so-called dermatopathic changes, which is a reactive form of lymphadenopathy that typically happens in patients who have skin rashes and where there is no evidence of direct involvement by the disease (although there are some patients who can have T-cell clones by molecular methods). The patients who have clonal T cells perhaps might not do as well as the ones who do not. On the other hand, we have patients for whom the whole architecture of the lymph node is effaced or replaced by neoplastic malignant cells. Those patients are probably going to need more aggressive forms of therapy.10
John Zic. The type of lymph node biopsy has been a hot topic. If patients have palpable lymph nodes in the cervical, axillary, and inguinal area, I don’t know if it’s a consensus, but the recommendation right now is to consider performing a lymph node biopsy of the cervical lymph nodes first, axillary second, and inguinal lymph nodes third. That might have to do with the complication rates for those different areas.
I’d like to switch to a discussion to more advanced disease. CTCL tumors are defined as a dome-shaped nodule > 1 cm. They don’t have to be very big before we label it a tumor, and the disease is considered more advanced. For patients with a few tumors, what does your prognosis discussion sound like?
Marianne Tawa. Certainly, the prognosis discussion can become slightly more complicated when you move into the realm of tumor-stage development. This is especially true if a CTCL patient has lived with and managed indolent patches or plaques for several years. We approach these patients with optimism and with the goal of managing their tumors, whether it be with a skin-directed option, such as localized radiation or a host of approved systemic therapies. Patients presenting with or developing tumor-stage disease over time will require additional staging workup compared with early-stage disease staging practice. Patients are counseled on imaging use in tumor-stage disease and why flow cytometry may be requested to rule in or rule out accompanying peripheral blood involvement. Patients are exposed to a myriad of pictures, stories, and survival statistics from Internet research. It becomes our task to inform them of their unique presentation and tailored treatment plan, which thankfully may produce more favorable responses than those presented online.
Lauren Pinter-Brown. One thing that we focus on is the idea that a statistic regarding prognosis isn’t predictive for an individual patient. When patients go online, we caution them that many of the statistics are really old. There’s been a lot of new therapies in the past 10 years. Just looking at my patients, my feeling is that their prognosis has continued to improve over the decades that I’ve been involved in this area.
We have to take the statistics with a grain of salt, though certainly someone that has Sézary syndrome or someone that has nodal involvement or tumors is not going to fare as well as the patients that we talked about with stage I disease. However, if we all continue to do our jobs and have more and more treatment options for patients, that’s certainly going to change over time as it has with other non-Hodgkin lymphomas.
John Zic. We’ve all treated advanced patients with disease and some, of course, have died of the disease. When patients die of advanced CTCL, what are the things that lead to their demise?
Lauren Pinter-Brown. Probably the most common would be infections because their skin barrier has been broken. As the disease advances, their immune system also deteriorates. We may contribute to that sometimes with some of the therapies that we use, although we try and be judicious. First and foremost, the primary cause of death remains infection and sometimes inanition.
Marianne Tawa. I agree, infection or just the unfortunate progression of their lymphoma through the various armamentarium of treatments would be the 2 reasons.
John Zic. Let’s dive into therapy. I want to start with early stage. While, I don’t think there’s a role for systemic anticancer agents, certainly the IV agents for most patients with early-stage disease Marianne, you mentioned phototherapy. What are the types of phototherapy that you offer?
Marianne Tawa. We would start out with narrow band UVB therapy for patients with > 10% body surface area involvement. When applying topical corticosteroids to wider surface areas of the patient’s body is no longer feasible or effective, we recommend the initiation of narrow band UVB phototherapy. This is preferred because of its lessor adverse effect (AE) profile as far as nonmelanoma skin cancer risk. Patients commence narrow band UVB 3 times per week, with a goal of getting the patient into remission over a matter of months and then slowly tapering the phototherapy so that they get to a maintenance of once weekly.
Realizing that narrow band UVB may not penetrate deeper plaques or effectively reach folliculotropic variant of CTCL, we would employ PUVA, (psoralen and UVA). Patients are expected to protect their eyes with UVA glasses and remain out of the sun 24 hours following PUVA treatments. The cost of the methoxsalen can be an issue for some patients. Nonmelanoma skin cancer risks are increased in patients undergoing long-term PUVA treatments. Routine skin cancer surveillance is key.
There are monetary, time, and travel demands for patients receiving phototherapy. Thus, many CTCL patients are moving toward home-based narrow band UVB units supervised by their treating dermatologist. Other skin-directed treatment options, aside from topical corticosteroids and phototherapy, would include topical nitrogen mustard, imiquimod, and localized or total skin electron beam radiation.
John Zic. Here in Nashville, some of our veterans travel hundreds of miles to get to our center. It’s not practical for them to come here for the narrow band UVB phototherapy. Veterans can get approval through the VA Choice programs to have phototherapy performed by a local dermatologist closer to home. We also have had many veterans who choose to get home narrow band UVB phototherapy, which can be quite effective. Narrow band UVB phototherapy is among the most effective therapies for patients with generalized patches in particular, and maybe some with just a few plaques.
Medium potency topical steroids are not as helpful as superpotent topical steroids such as clobetasol, dipropionate ointment, or betamethasone dipropionate ointment. Usually, I tell patients to apply it twice a day for 8 weeks. You must be careful because these high-potency topical steroids can cause thinning of the skin, but it’s rarely seen, even in patients that may use them for 8 weeks if they’re applying them just to their patches and thin plaques. There are a few other topicals. There’s bexarotene gel, which is a topical retinoid, and mechlorethamine or nitrogen mustard gel that are available as topicals. Both of those can be helpful if patients have < 10% body surface area of patches or plaques because they can apply that at home.
Because of the excellent prognosis for patients in early stages, this is an area we want to try to avoid doing harm. For patients with advanced disease, what are some of the decisions that you think about in recommending a patient to get radiation therapy?
Lauren Pinter-Brown. I use radiation therapy sparingly and primarily for patients who either have only 1 tumor and the rest of their disease is patch and plaque or for patients who have very large tumors that are either cosmetically unacceptable or creating infection or pain. I treat people with systemic therapies primarily to prevent the formation of tumors.
John Zic. There probably is a role for total skin electron beam radiotherapy in patients who have failed multiple other skin-directed therapies and are progressing and then perhaps a role for more advanced patients who have multiple tumors where you’re trying to get some control of the disease. Are there any other situations where you might consider total skin electron beam?
Marianne Tawa. Yes, those are 2 scenarios. A third scenario would be in patients preparing for stem cell transplant. We typically do a modified 12 Gy regimen of total skin electron beam for palliation and up to 24 Gy regimen for patients who are in earnest preparing for a stem cell transplant.
John Zic. Systemic therapies also treat this disease. There are 2 oral agents. One is bexarotene capsules, a retinoid that binds to the RXR receptor and has a multitude of effects on different organ systems. It is probably the best tolerated oral agent we have. The other FDA-approved agent is vorinostat, a histone deacetylase inhibitor, but it has more gastrointestinal AEs than does bexarotene. Bexarotene has AEs as well, including hypertriglyceridemia and central hypothyroidism, which can throw a curveball to unsuspecting primary care physicians who might check thyroid function studies in these patients.
We certainly need to know about those AEs. There are many patients who have tumor-stage disease that can have radiotherapy to several tumors, then go on a drug like bexarotene capsules and may be able to maintain the remission for years. In my experience, it’s a drug that patients usually stay on. They can be weaned to a very low dose, but I’ve had several patients who come off of bexarotene only to suffer relapses.
Lauren, what are some of the things that you think about when you declare someone as having failed bexarotene or vorinostat and you’re thinking about IV therapies?
Lauren Pinter-Brown. Patient comorbidities and the particular compartment of their body that is involved are important factors. Do they have blood involvement, or not? Do they have nodal involvement, or not? Another concern is both acute and chronic toxicities that need to be discussed with the patient to determine an acceptable QOL. Finally, the schedule that you’re giving the drug. Some people may not be able to come in frequently. There are a lot of variables that go into making an individual decision at a particular time for a specific patient who will be using parenteral therapies.
John Zic. If we have a patient with advanced MF, tumors, and perhaps lymph node involvement, what are some of the systemic options that you would consider?
Lauren Pinter-Brown. With nodal involvement, an attractive option is something like IV romidepsin because we know that it treats peripheral T-cell lymphomas, which are aggressive nodal T-cell lymphomas. It’s FDA approved and also treats CTCL. Another is brentuximab vedotin if there is significant CD30 expression. It also is FDA approved for CTCL and has a long track record of treating certain peripheral T-cell lymphomas like anaplastic large cell.
John Zic. When would the stem cell transplant discussion start at your institution?
Lauren Pinter-Brown. It starts earlier for a younger patient because even though we do have lots of treatment if someone is aged 20 or30 years, I don’t really have any illusions that I have enough treatment options for them to live a normal lifespan if they have advanced disease. It’s a possibility for any patient when I see that the future options are dwindling, and that I am not going to be able to control the patient’s disease for much longer. Having said that, patients who have tumor-stage disease are among those that don’t do quite as well with allogeneic transplantation; ironically, patients with Sézary syndrome or erythroderma might do a little bit better.
John Zic. Before considering a stem cell transplant for patients with Sézary syndrome, that is erythroderma with significant blood involvement, what other treatment options would you offer?
Marianne Tawa. For low blood-burden disease, we might look at extracorporeal photopheresis as monotherapy or in combination with interferon or bexarotene. For patients with higher blood burden we might recommend low-dose alemtuzumab, especially if they have abundant CD52 expression. We also consider the newly FDA-approved anti-CCR4 antibody treatment, mogamulizumab, for patients presenting with Sézary syndrome. It is generally well tolerated but does have the potential for producing infusion reactions or drug rash.
Romidepsin has efficacy in blood, lymph node, and skin compartments. The primary considerations for patients considering romidepsin are prolonged infusion times and QOL AEs with gastrointestinal and taste disturbances and fatigue.
John Zic. Both of you have brought up an excellent point. This is a disease that while we do not have a good chance of curing, we have a pretty fair chance of controlling, especially if it’s early stage. The data from the stem cell transplant literature indicate that stem cell transplant may be one of the few modalities that we have that may offer a cure.11
Lauren Pinter-Brown. There are patients who are cured with allogeneic transplants; and the very first allogeneic transplants were performed well over 20 years ago. Many patients, even some in my practice, who were among those patients and continue to do extremely well without any evidence of disease. Sometimes when people have allogeneic transplantation, their disease relapse may be in a more indolent form that’s much easier to deal with than their original disease. Even if they’re not cured, the fact that the aggressive disease seems to be at bay may make them much easier to treat.
John Zic. Those are excellent points. You brought up photopheresis as a treatment modality for patients with evolving or early Sézary syndrome and patients with erythrodermic MF can also respond. We have a lot of experience with that at the Nashville VA medical center. We’re one of the few VA hospitals in the US that has a photopheresis unit. But the modality is available at many academic medical centers because it’s a treatment for graft-vs-host disease.
We tend to also consider photopheresis in patients who may have had an excellent response to another systemic agent. There are some data that patients who received photopheresis, after total skin electron beam therapy vs those who received chemotherapy after radiation, had a longer disease-free survival.12
I’d like to end with a discussion of something that’s very important, which is managing QOL issues for patients with CTCL. Itch is among some of the worst symptoms that can cause suffering in patients. But it is sometimes not a problem at all for patients who have a few patches or plaques. That’s one reason why they might ignore their rash. Certainly, as the disease progresses, especially those patients with erythroderma, the itch can be intractable and can have a major impact on their life. What are some approaches to managing itch at your institutions?
Lauren Pinter-Brown. One thing to be aware of is that the itch is not usually mediated by histamine, though people will often put the patients on a lot of antihistamines. I don’t find those to be the most effective treatments. I think of the itch in these patients as more of a neuropathic condition and would tend to treat more with things that you might use for neuropathy, such as gabapentin or doxepin or antidepressants. There’s a whole host of other treatments, such as aprepitant, something that I would use as an antiemetic, that might also be helpful for pruritus in this patient population.
John Zic. That’s my experience as well. I have found gabapentin to be helpful for patients with itch, though not universally.
Marianne Tawa. I consider itch a huge QOL concern for a large majority of our patients with a CTCL diagnosis. It’s on par with pain. In early-stage disease, pruritus levels improve as the cutaneous burden is reduced with skin-directed therapies such as, topical corticosteroid or phototherapy.
SSRI agents could also be considered for select patients. The antiemetic agent, aprepitant has been useful for addressing itch in a subset of our patients with Sézary syndrome. Patients will also seek out complementary modalities such acupuncture, hypnosis, and guided imagery.
John Zic. Because the disease itself affects the skin and can lead to dryness, patients often suffer with dry skin. When I trained in Chicago, that was the foundation of our treatment, making sure that patients are using a super fatted soap such as Dove (Unilever, London, United Kingdom) or Cetaphil (Galderma Laboratories; Fort Worth, TX), making sure that they’re lubricating their skin frequently with something perhaps in the wintertime as thick as petroleum jelly. And then in the summertime perhaps with Sarna lotion (Crown Laboratories; Johnson City, TN), which has menthol. It’s important to note that when the patient’s skin is infected, the itch can skyrocket. Being aware and monitoring the skin for signs of infection such as crusting and impetigo-like findings can be helpful.
I also wanted to touch on fatigue. Patients can have fatigue for many reasons. Sometimes it’s because the itch is interfering with their sleep. How do you approach managing fatigue?
Lauren Pinter-Brown. There have been many studies about cancer fatigue, and it appears that one of the cheapest and easiest modalities is for patients to walk. We often suggest that our patients go on walks, however much they can do, because that has been seen over and over again in studies of cancer fatigue to be beneficial.
John Zic. Do you have any advice for nurses that might be helping to manage patients in a cutaneous lymphoma clinic?
Marianne Tawa. As this is a rare disease, nursing encounters with patients carrying a diagnosis of CTCL in both oncology and dermatology settings may be few and far between. I recommend nurses familiarize themselves with articles published on CTCL topics found in both dermatology and oncology peer review journals. Another avenue for gaining insight and education would be through continuing education courses. Resources can also be found for nurses, patients, and caregivers through advocacy foundations such as the Cutaneous Lymphoma Foundation (www.clfoundation.org) and the Lymphoma Research Foundation (LRF@lymphma.org).
John Zic. Is there anything else that anyone would like to add to our discussion?
Lauren Pinter-Brown. One thing that we touched upon, but I was concerned that we didn’t emphasize, was the use of flow cytometry as a diagnostic tool in a patient with erythroderma. Sometimes biopsies of patients with erythroderma are not diagnostic, so clinicians need to be aware that there are other ways of diagnosing patients—nodal biopsy or flow cytometry. They should not only think of it as a staging tool but sometimes as a diagnostic tool.
Alejandro Ariel Gru. I agree. Particularly in patients who have Sézary syndrome or MF with peripheral blood involvement, sometimes the findings on the biopsy show a dissociation between how impressive the clinical presentation of the patient might be and how very few findings you might encounter on the skin biopsy. Therefore, relying on flow cytometry as a diagnostic tool is capital. Lauren, you briefly mentioned the criteria, which is looking for an abnormal CD4 to CD8 ratio of > 10%, abnormal loss of CD7, > 40%, or abnormal loss of CD26 of > 30%.
In addition, there are new markers that are now undergoing validation in the diagnosis of Sézary syndrome. One is KIR3DL2, which is a natural killer receptor that has been shown to be significantly upregulated in Sézary syndrome and appears to be both more sensitive and specific. With that also comes therapies that target the KIR3DL2 molecule.
John Zic. One of the first things we teach our dermatology residents to work up patients with erythroderma is that they shouldn’t expect the skin biopsy to help them sort out the cause of the erythroderma. As you mentioned, Lauren, the flow cytometry of peripheral blood should always be accompanied by a CBC with differential and platelets. And if the patients do have lymph nodes, consider a biopsy because sometimes that’s where you can make the firmest diagnosis of a T-cell lymphoma.
Acknowledgmentszz
The participants and Federal Practitioner would like to thank Susan Thornton, CEO of the Cutaneous Lymphoma Foundation for helping to arrange this roundtable discussion.
1. Willemze R, Cerroni L, Kempf W, et al. The 2018 update of the WHO-EORTC classification for primary cutaneous lymphomas. Blood. 2019;133(16):1703-1714.
2. Imam MH, Shenoy PJ, Flowers CR, Phillips A, Lechowicz MJ. Incidence and survival patterns of cutaneous T-cell lymphomas in the United States. Leuk Lymphoma. 2013;54(4):752-759.
3. Del Guzzo C, Levin A, Dana A, et al. The incidence of cutaneous T-Cell lymphoma in the veteran population. Abstract 133. J Invest Dermatol. 2016;136(5 suppl 1):S24.
4. Aschebrook-Kilfoy B, Cocco P, La Vecchia C, et al. Medical history, lifestyle, family history, and occupational risk factors for mycosis fungoides and Sèzary syndrome: the InterLymph Non-Hodgkin lymphoma subtypes project. J Natl Cancer Inst Monogr. 2014;48:98-105.
5. Scarisbrick JJ, Quaglino P, Prince HM, et al. The PROCLIPI international registry of early-stage mycosis fungoides identifies substantial diagnostic delay in most patients. Br J Dermatol. 2018. [Epub ahead of print.]
6. Thurber SE, Zhang B, Kim YH, Schrijver I, Zehnder J, Kohler S. T-cell clonality analysis in biopsy specimens from two different skin sites shows high specificity in the diagnosis of patients with suggested mycosis fungoides. J Am Acad Dermatol. 2007;57(5):782-790.
7. Kim YH, Jensen RA, Watanabe GL, Varghese A, Hoppe RT. Clinical stage IA (limited patch and plaque) mycosis fungoides. A long-term outcome analysis. Arch Dermatol. 1996;132(11):1309-1313.
8. Benton EC, Crichton S, Talpur R, et al. A cutaneous lymphoma international prognostic index (CLIPi) for mycosis fungoides and Sézary syndrome. Eur J Cancer. 2013; 49(13):2859-2868.
9. Battistella M, Sallé de Chou C, de Bazelaire C, et al. Lymph node image-guided core-needle biopsy for cutaneous T-cell lymphoma staging. Br J Dermatol. 2016;175(6):1397-1400.
10. Johnson WT, Mukherji R, Kartan S, Nikbakht N, Porcu P, Alpdogan O. Allogeneic hematopoietic stem cell transplantation in advanced stage mycosis fungoides and Sézary syndrome: a concise review. Chin Clin Oncol. 2019;8(1):12.
11. Johnson WT, Mukherji R, Kartan S, Nikbakht N, Porcu P, Alpdogan O. Allogeneic hematopoietic stem cell transplantation in advanced stage mycosis fungoides and Sézary syndrome: a concise review. Chin Clin Oncol. 2019;8(1):12.
12. Wilson LD, Jones GW, Kim D, et al. Experience with total skin electron beam therapy in combination with extracorporeal photopheresis in the management of patients with erythrodermic (T4) mycosis fungoides. J Am Acad Dermatol. 2000;43(1 Pt 1):54-60.
1. Willemze R, Cerroni L, Kempf W, et al. The 2018 update of the WHO-EORTC classification for primary cutaneous lymphomas. Blood. 2019;133(16):1703-1714.
2. Imam MH, Shenoy PJ, Flowers CR, Phillips A, Lechowicz MJ. Incidence and survival patterns of cutaneous T-cell lymphomas in the United States. Leuk Lymphoma. 2013;54(4):752-759.
3. Del Guzzo C, Levin A, Dana A, et al. The incidence of cutaneous T-Cell lymphoma in the veteran population. Abstract 133. J Invest Dermatol. 2016;136(5 suppl 1):S24.
4. Aschebrook-Kilfoy B, Cocco P, La Vecchia C, et al. Medical history, lifestyle, family history, and occupational risk factors for mycosis fungoides and Sèzary syndrome: the InterLymph Non-Hodgkin lymphoma subtypes project. J Natl Cancer Inst Monogr. 2014;48:98-105.
5. Scarisbrick JJ, Quaglino P, Prince HM, et al. The PROCLIPI international registry of early-stage mycosis fungoides identifies substantial diagnostic delay in most patients. Br J Dermatol. 2018. [Epub ahead of print.]
6. Thurber SE, Zhang B, Kim YH, Schrijver I, Zehnder J, Kohler S. T-cell clonality analysis in biopsy specimens from two different skin sites shows high specificity in the diagnosis of patients with suggested mycosis fungoides. J Am Acad Dermatol. 2007;57(5):782-790.
7. Kim YH, Jensen RA, Watanabe GL, Varghese A, Hoppe RT. Clinical stage IA (limited patch and plaque) mycosis fungoides. A long-term outcome analysis. Arch Dermatol. 1996;132(11):1309-1313.
8. Benton EC, Crichton S, Talpur R, et al. A cutaneous lymphoma international prognostic index (CLIPi) for mycosis fungoides and Sézary syndrome. Eur J Cancer. 2013; 49(13):2859-2868.
9. Battistella M, Sallé de Chou C, de Bazelaire C, et al. Lymph node image-guided core-needle biopsy for cutaneous T-cell lymphoma staging. Br J Dermatol. 2016;175(6):1397-1400.
10. Johnson WT, Mukherji R, Kartan S, Nikbakht N, Porcu P, Alpdogan O. Allogeneic hematopoietic stem cell transplantation in advanced stage mycosis fungoides and Sézary syndrome: a concise review. Chin Clin Oncol. 2019;8(1):12.
11. Johnson WT, Mukherji R, Kartan S, Nikbakht N, Porcu P, Alpdogan O. Allogeneic hematopoietic stem cell transplantation in advanced stage mycosis fungoides and Sézary syndrome: a concise review. Chin Clin Oncol. 2019;8(1):12.
12. Wilson LD, Jones GW, Kim D, et al. Experience with total skin electron beam therapy in combination with extracorporeal photopheresis in the management of patients with erythrodermic (T4) mycosis fungoides. J Am Acad Dermatol. 2000;43(1 Pt 1):54-60.